Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Impact of a Multi-Component Preventive Oral Health Program on Dental Plaque Scores for Individuals with Special Health Care Needs
Authors Alrazooq WS, Alhurishi SA ![]() , Shah AH
, Shah AH ![]()
Received 12 December 2025
Accepted for publication 16 June 2026
Published 30 June 2026 Volume 2026:18 584289
DOI https://doi.org/10.2147/CCIDE.S584289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Christopher E. Okunseri
Wejdan Saad Alrazooq1, Sultana A Alhurishi2, Altaf H Shah3
1Department of Dental Hygiene, University Dental Hospital, King Saud University Medical City, Riyadh, Saudi Arabia; 2Community Health Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 3Community Dental Sciences Department, Marquette University School of Dentistry, Milwaukee, WI, USA
Correspondence: Dr. Altaf H Shah, Marquette University School of Dentistry, Room No. 141T, Delta Dental Urgent and Special Care Clinic, Community Dental Sciences Department, 1801 W Wisconsin Avenue, Milwaukee, WI, 53233, USA, Tel +1-4142886920, Email [email protected]
Purpose: Plaque accumulation is considered to be one of the main factors in various oral diseases. This study aimed to evaluate the effect of oral health counselling on plaque scores for Individuals with Special Health Care Needs (ISHCN) attending special care dentistry clinics.
Patients and Methods: A prospective observational study was designed and consecutive sampling was used among the adult patients attending special care dentistry clinics at a University Dental Hospital. A total of 120 participants (61 males and 59 females between) aged between 16 and 69 years were enrolled in the study. Participation was voluntary, and recruits were selected after the application of a set of inclusion and exclusion criteria. The participants were categorized according to their specific health care needs. The subjects were assessed for plaque scores using the Silness–Löe Plaque Index for a period of six months. The first observation was noted at baseline and then every two weeks until the next three months. Finally, monthly plaque scores were recorded for the subsequent three months. Ten observations were recorded for each participant. All data were entered and analyzed using Statistical Package for Social Sciences (SPSS v.22) software.
Results: The majority of the sample was comprised of the “Medically compromised group”, followed by the “Intellectual disability” group. The overall baseline mean plaque index score was 2.68, which reduced significantly (p = 0.01) at the completion of 6 months period.
Conclusion: The multi-component preventive oral health program and repeated follow up was associated with significant reduction in dental plaque scores among individuals with special health care need over six months.
Keywords: education, prevention, disability, tooth brushing, oral disease, oral health promotion
Introduction
Oral Health is an important aspect of overall health and well-being. The active engagement of oral health professionals should be an integral component of health promotion strategies.1 Oral healthcare is one of the challenging areas for Individuals with Special Health Care Needs (ISHCN)2 who are more susceptible to oral diseases and conditions, particularly periodontal disease.3 It has been demonstrated that ISHCN have higher unmet oral need and experience challenges in accessing dental care.4 The apparent reasons for the higher unmet oral health need are the barriers to access as well as the lack of attitude, training and unwillingness of the oral health care providers5,6 A recent study in Saudi Arabia has also indicated poor oral health and suboptimal oral health behavior in this population.7
Poor oral health behaviors negatively affect oral health outcomes, whereas effective oral hygiene practices have beneficial effects not only on oral health but also on overall general health.8 Therefore, the implementation of structured oral hygiene education programs and dental plaque control measures are essential to promote preventive behaviors thereby reducing the oral disease burden in this population.9 Evidence indicates that oral health promotion strategies, particularly those incorporating oral health education, are effective in enhancing oral health behaviors.10 Obtaining a health gain like improving oral health for ISHCN can be possible mainly through community based initiatives.11 Prevention of oral diseases in this group has more significance owing to the limited resources available as well as the barriers to access for oral health services.12,13 Oral health counselling is an element of oral health education where the oral health care education is delivered to the person taking into consideration the circumstances associated with the person. However, it has to be repeated and continued for effective oral health benefits.14
Little is known about the effect of context-specific oral health counselling on plaque scores for ISHCN attending special care dentistry clinics. There is limited evidence regarding its effectiveness among individuals with ISHCN. Therefore, there is a need to initiate specialized oral health care programs for ISHCN. This study assessed the impact of a multi-component oral health preventive program on dental plaque control among ISHCN. We hypothesized that plaque scores would reduce following the multi-component oral health preventive program which would eventually enable ISHCN to have a reduced risk for oral diseases.
Material and Methods
Ethical Approval
This project is covered under “Research on Human subjects.” The study complied with the Declaration of Helsinki.15 No introduction of new materials or items was proposed, and at no stage was the study intended to be interventional. The project proposal was presented to the Institutional Review Board (IRB) and the Chair of the Research Ethics Committee of King Saud University. After fulfilling all requirements and in accordance with the International Guidelines for individuals who lack capacity, formal ethical approval was granted (approval number IRB #E-22-6764, dated 27th March 2022). A formal informed written consent was taken from all participants explaining in detail the rationale and the role of their participation in the study. Formal written consent was taken from parents/guardians and/or caregivers of ISHCN aged between 16 to 18 years as well as for those who lacked the capacity to understand, process or retain the information given during the research.
Study Design
A prospective study design was employed to enroll patients attending the special care dentistry clinics and follow-up was done with participants who met the selection criteria and agreed to complete the study. Data were collected from April 2022 to December 2022.
Study Sample and Location
Consecutive sampling was used to recruit participants. The participants were approached to participate when they sought dental treatment at the Special Care Dentistry Clinics of the University Dental Hospital. The selection criteria were set based on the inclusion and exclusion criteria. A total of 160 participants were initially recruited after providing informed consent and meeting the selection criteria. However, the total number of participants who completed the study was 120 after 40 participants dropped out of the study at various stages because of non-attendance for various reasons. Most of the drop outs were related to personal reasons unrelated to the consequences resulting from the multi-component preventive measures.
Inclusion Criteria
- Patients with > or = 20 permanent dentition.
- Patients who had the capacity to consent and perform self-tooth brushing.
Exclusion Criteria
- Children below the age of 16 years.
- Patients who are dependent on caregivers for brushing and other oral hygiene measures.
- Patients with retained teeth or mixed dentition.
- Patients with supernumerary teeth.
- Removable prostheses or orthodontic appliances that may affect plaque accumulation.
- Acute oral infections or untreated severe oral disease.
Multi-Component Oral Health Preventive Program
A structured, multicomponent oral health preventive program was implemented for all participants. The program comprised four integrated components:
- Baseline assessment and professional prophylaxis: Participants attended an initial appointment with a dental hygienist, during which plaque levels were recorded using the Silness–Löe Plaque Index.16 Following the assessment, full-mouth professional prophylaxis was performed by the same hygienist to standardize baseline oral hygiene status.
- Oral health education: A standardized 15-minute educational session was delivered using a jaw model and a powered toothbrush demonstration.
- Provision of powered toothbrushes: To support adherence and reinforce instruction, each participant received a powered toothbrush after completion of the educational session. All participants received the same type of powered toothbrush and a commercially available 1450 ppm fluoride toothpaste for use at home.
- Scheduled follow-up and reinforcement: Participants were scheduled for follow-up visits to reassess plaque scores and reinforce oral hygiene instructions.
Participants were subjected to complete oral prophylaxis to achieve a score of 0. Following the oral prophylaxis session, individualized oral health counselling was provided to each participant recruited in the study. Each participant was instructed about correct toothbrushing at home twice daily for two minutes as shown during the session. Once at night, before sleeping, and at any other time during the day. Each participant was followed-up for six months. Plaque scores were recorded ten times for each participant during the study period according to the following schedule.
The baseline assessment (Month 0) was conducted during the participant’s first appointment with the dental hygienist, during which the initial plaque recording was performed. Following baseline, plaque levels were assessed every two weeks for the first three months, resulting in six biweekly assessments at Weeks 2, 4, 6, 8, 10, and 12. Participants underwent monthly plaque assessments for the subsequent three months, specifically at Months 4, 5, and 6.
During each follow-up visit, participants were asked about their compliance with powered toothbrushing at home and their brushing technique. Guidance was provided when necessary. The counselling was adapted informally according to the participant’s functional profiles and no formal protocol differentiation across disability subgroups was pre-specified. The degree of adaptation across the subgroups was not independently recorded.
Participants enrolled in the study performed oral hygiene themselves when physically able. The researcher assessed participants’ plaque scores and delivered the intervention to ensure consistent implementation across all participants. The researcher also documented the delivery of all program components. Plaque score recordings were documented separately at each scheduled visit.
Plaque Scores
The Silness–Löe Plaque Index was used to measure the effectiveness of plaque removal. Plaque accumulation was assessed on four surfaces—distal, mesial, facial, and lingual/palatal—of the first molars and central incisors in each quadrant. Plaque was scored on a scale from 0 to 3, For each participant, an average plaque index score was calculated across all assessed teeth. A William’s periodontal probe, a mouth mirror and sterile gauze were used to collect and record plaque when present, ensuring consistent and accurate measurement. Table 1 shows the plaque scores and their respective interpretation.
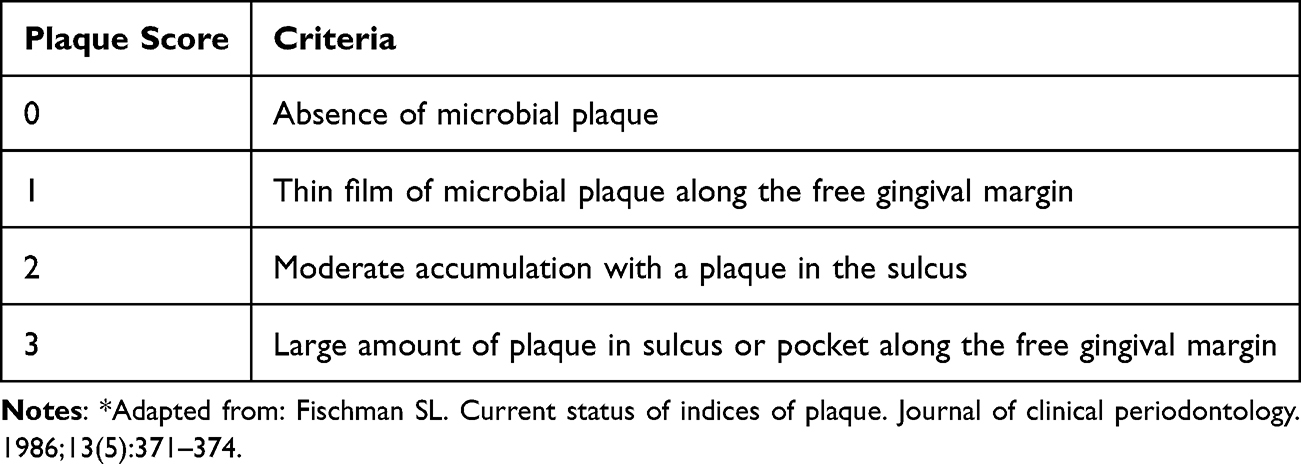 |
Table 1 Silness–Löe Plaque Index* |
Variables
Participants were grouped according to their specific special need into four categories: Intellectual Disability, Medically Compromised, Physical Disability and Syndromes /Multiple disabilities.
Statistical Analysis
The recorded data were compiled and entered into a computer using Statistical Package for Social Sciences software (SPSS) version 22.0 software (Chicago, IL, USA). One-way ANOVA and Chi-square tests, as well as the Bonferroni test for the adjustment of multiple comparisons, were used. A p value of < 0.05 was considered statistically significant.
Results
A total of 120 participants completed the study. The participants were 61 males and 59 females. The participants were aged between 16 and 69 years old. The majority were medically compromised (33.3%), followed by those with intellectual disabilities (26.7%). Participants with syndromes or multiple disabilities accounted for 23.3%, whereas 16.7% had physical disabilities (Table 2).
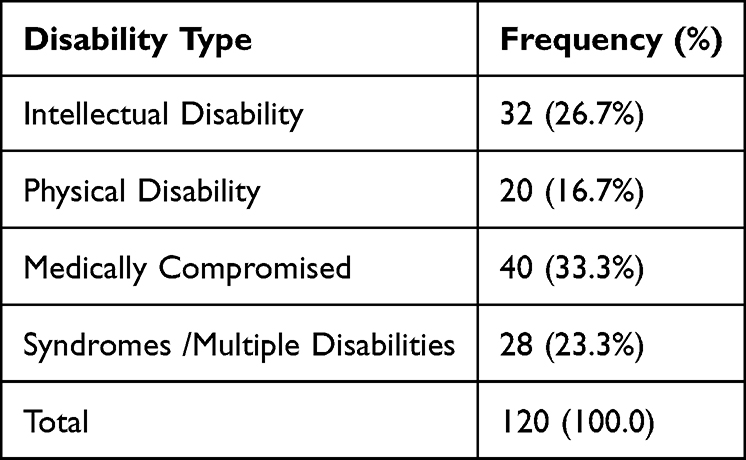 |
Table 2 Description of the Study Participants According to Their Disability (n=120) |
Figure 1 shows that participants aged 21–25 years accounted for 42.5%, whereas those above 60 years consisted of only 2.5% of the participant group. Baseline plaque scores via the Silness–Löe Plaque Index were obtained for each individual and the overall mean scores were calculated. Figure 2 presents the mean plaque index scores stratified according to specific health care need. Comparisons between groups indicated that participants with intellectual disabilities had the highest mean plaque score (2.91).
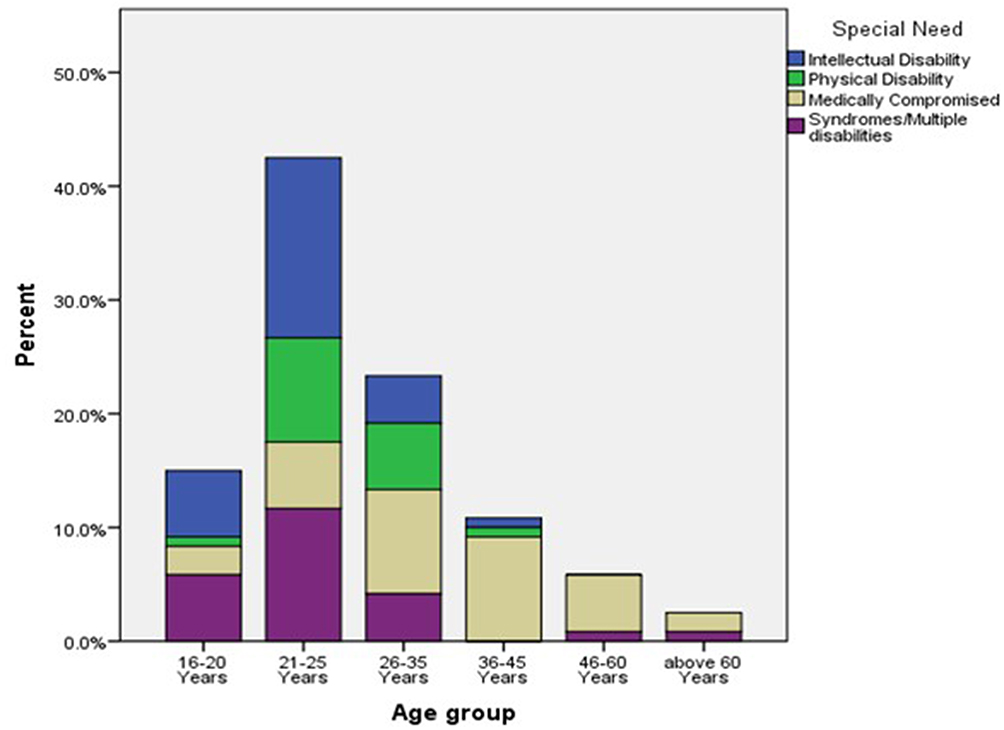 |
Figure 1 Distribution of Special health care needs by age group. |
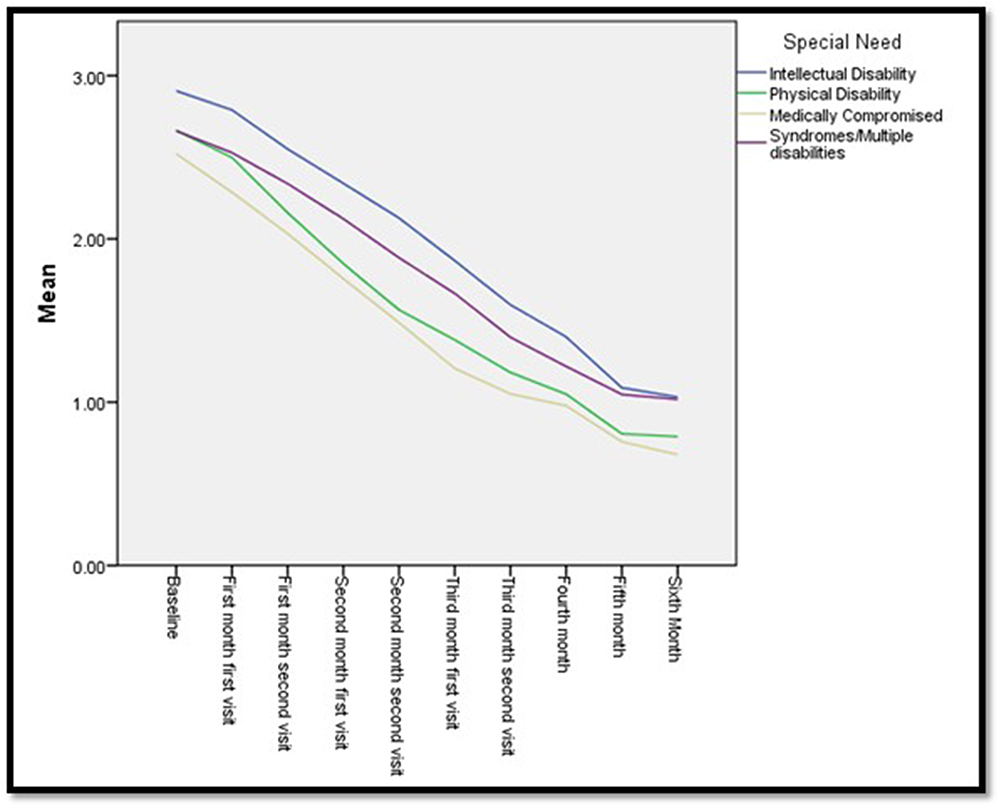 |
Figure 2 Mean plaque index scores over 6 months. |
Table 3 presents the mean plaque index scores for each group of special health care needs, along with the overall mean. Significant reductions in plaque scores were observed across all groups (p < 0.05), with the medically compromised group showing the greatest reduction. No significant differences were found between genders (p > 0.05).
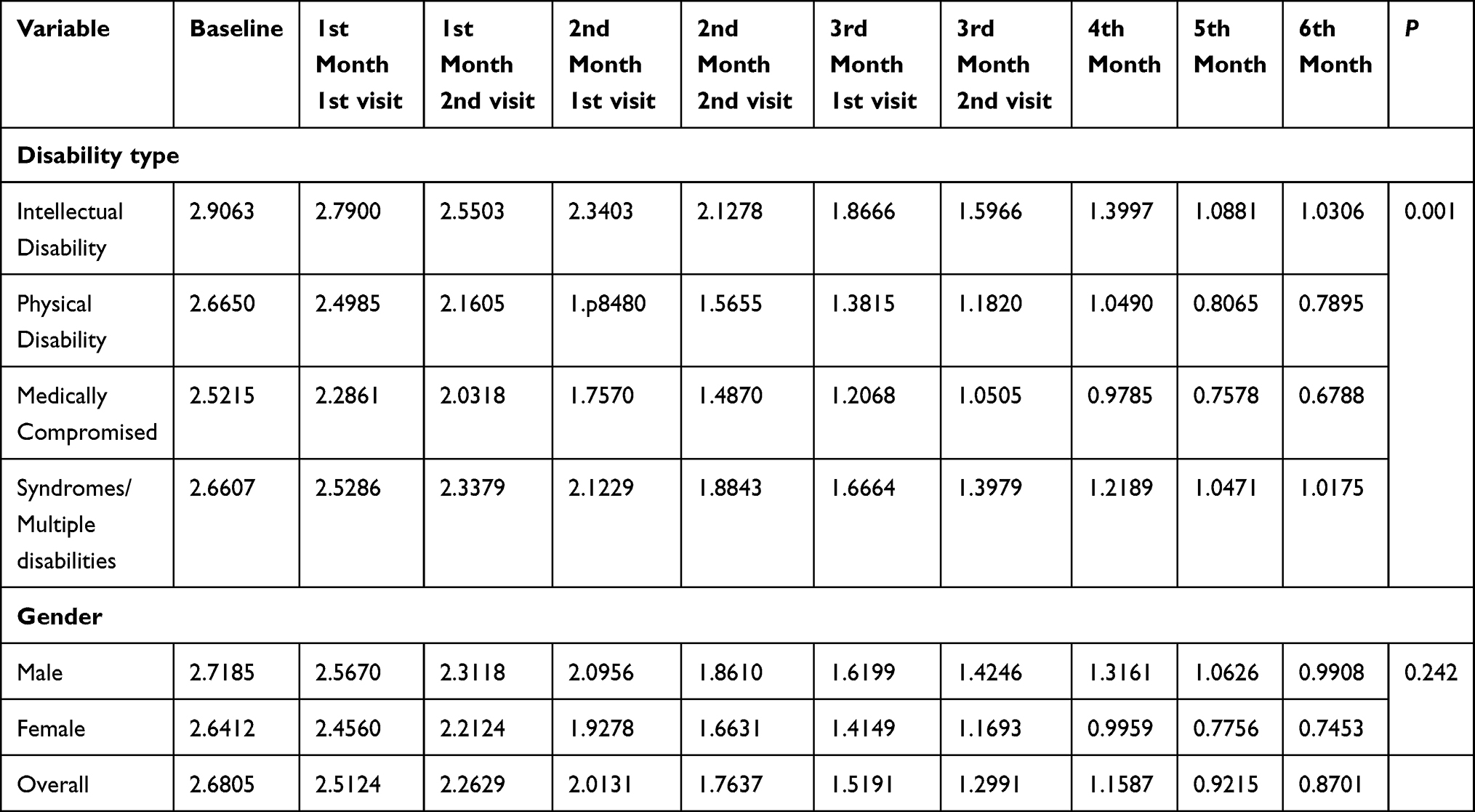 |
Table 3 Mean Plaque Scores at Various Time Intervals During the Study |
Comparisons over time showed a consistent decrease in mean plaque scores at monthly intervals. Table 4 summarizes the comparisons between baseline and follow-up mean plaque scores, with statistically significant reductions observed at all time points.
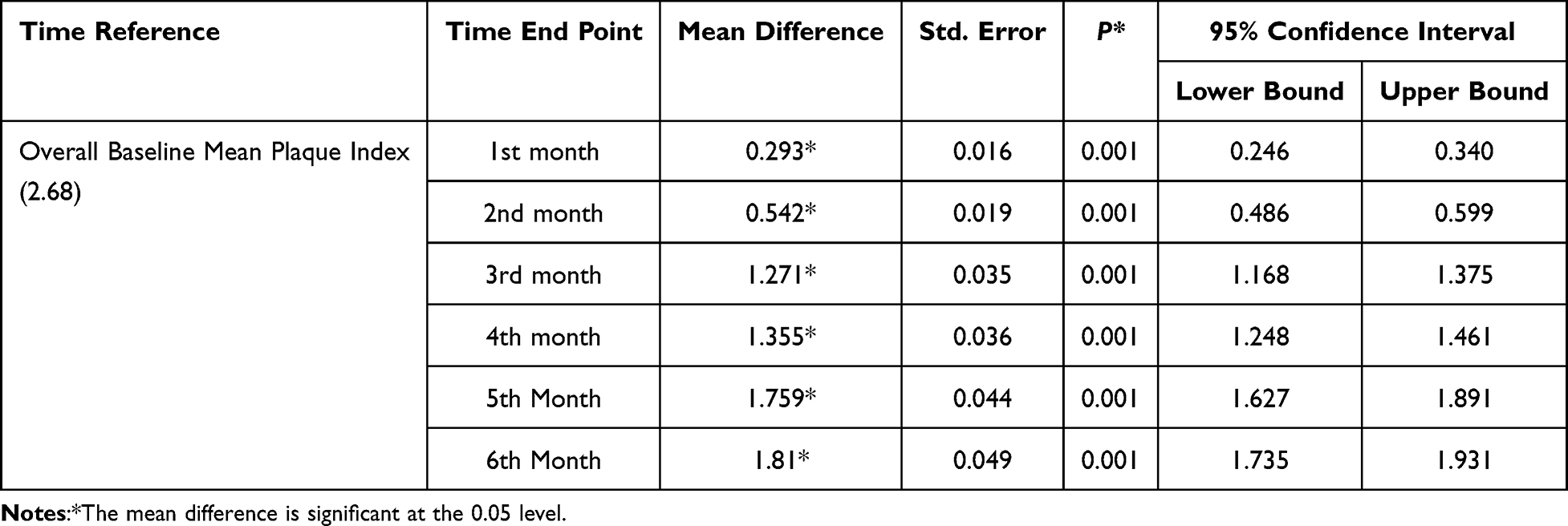 |
Table 4 Pairwise Comparisons of Mean Plaque Index Between Baseline and Follow-Up Months (Bonferroni-Adjusted) |
Discussion
Maintaining good oral health is a challenge for many ISHCN, who are also more susceptible to oral disease than the general population.17–19 Poor oral hygiene in ISHCN may be attributed to reduced intellectual and physical abilities that hinder effective toothbrushing.10,20,21 Oral health is further compromised by limited awareness of its importance and inadequate oral hygiene practices.3,22 In this context, structured oral health promotion programs may play a key role in improving the oral health among ISHCN by improving their knowledge and supporting the development of effective self-care behaviours through education, caregiver involvement, and regular reinforcement.3,23–25 There is limited evidence on interventions from Saudi Arabia to support oral health promotion among ISHCN.26,27
This study was conducted as a single group evaluation within the routine clinical services of the Special Care Dentistry Clinics. In such a setting, a structured preventive programme for all eligible patients is consistent with standard of care obligations, and assigning patients to separate intervention and control groups was not feasible. A multicomponent preventive oral health strategy was implemented that included baseline assessment and professional cleaning, provision of powered toothbrushes, oral health education, and scheduled follow-up appointments. Offering systematic guidance, follow-up, and reinforcements has shown to have an influence on tooth brushing behavior among people with intellectual disabilities.23,25,28
In the present study, the higher plaque score at baseline confirms poor oral hygiene in ISHCN, which is similar to the previous studies.10,21,26 The overall mean plaque index score at the baseline was 2.68; which reduced significantly to 1.5 at 3 months and finally to 0.87 at six months (p < 0.001). These results are in line with the previously conducted studies in other settings.25,29 This provides empirical support for the effectiveness of a multicomponent preventive program comprising professional prophylaxis, oral health education, provision of powered toothbrushes, and scheduled follow-up in this underserved population;
The sample consisted of medically compromised individuals, those with physical disabilities, and intellectual disabilities as well as those with syndromes or multiple disabilities. Among the four disability groups, the medically compromised group demonstrated the greatest reduction in plaque scores over the study period, while the intellectual disability group, despite beginning with the highest baseline mean (2.91), showed comparatively less reduction. It is noteworthy that the study participants had a wide range of special needs. Studies among similar groups have found inconsistency in participants’ recruitment as well as oral health outcomes for people with intellectual disabilities.27,30
There was no statistically significant difference in plaque score reduction among gender which suggests that the program was equally effective across sexes. This finding may be due to the structured and standardized nature of the intervention and similar result was reported by Shyama et al in a study conducted in Kuwait.25
A formal sensitivity analysis distinguishing the early plaque reduction attributable to baseline prophylaxis from the sustained reduction reflecting behavioural change was not conducted. However, pairwise comparison of mean plaque index shows a progressive and sustained decline in plaque scores over time, with mean differences increasing from 0.293 at 1 month to 1.81 at 6 months, all statistically significant (p < 0.001). This suggests that the observed improvements were not limited to the immediate post-prophylaxis but were maintained over time, likely reflecting continued behavioural change. Studies have emphasized the need of continued oral health promotion for a notable benefit.27,29,31–33
Limitations
Limitations of the study should be considered when interpreting the findings. The absence of a control group limits causal attribution to any specific component of the intervention; future studies with factorial designs would identify the independent contribution of each element. Absence of a prior sample size calculation introduces uncertainty regarding statistical power and the potential for Type I and II errors. The attrition rate of 25% is a notable limitation and the dropouts were attributed to scheduling conflicts and personal reasons unrelated to the preventive program; although available clinical data suggest that those who withdrew were broadly comparable to completers. A formal attrition bias analysis should be performed in future studies. Compliance was assessed informally through follow-up attendance rather than validated measures, and cognitive or functional differences among participants were not evaluated, potentially confounding observed outcomes. Additionally, analysis for subgroups were not stratified, which limited the granularity of the findings. Future studies should do subgroup analysis to report specific effects.
From a methodological perspective, the use of repeated-measures ANOVA does not account for within-subject correlations or missing data; a mixed-effects modelling approach would have been more appropriate and is recommended for future studies. Finally, the scalability and sustainability of the multicomponent preventive oral health program remain uncertain, given its reliance on trained personnel, provision of powered toothbrushes, and multiple follow-up visits, which may be challenging to replicate in routine or resource-limited settings.
Despite these limitations, the study contributes to an important step to close the gap in the literature concerning oral health promotion for ISHCN in Saudi Arabia. The findings of this study carry implications for the ongoing transformation of healthcare in Saudi Arabia.34,35 The present study demonstrates that structured, clinic-based oral health promotion is feasible and effective within existing dental services and can meaningfully reduce the oral health burden in this population. Future controlled studies incorporating validated behavioural measures, caregiver involvement assessments, and longer follow-up durations are needed for evidence-based guidelines.
Conclusions
Engagement in a multicomponent oral health preventive program was linked to improvements in plaque scores among Individuals with special health care needs. These findings support the effectiveness of structured preventive approaches with groups having special needs for oral health gain.
Recommendations
Implementation of preventive programs for ISHCN is likely to result in significant oral health benefits. Oral health counselling can be considered an important preventive oral health measure for ISHCN.
Data Sharing Statement
Data from this research is available upon reasonable request to the corresponding author.
Acknowledgments
The authors would like to thank the University Dental Hospital at King Saud University for the support and cooperation.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Barranca-Enríquez A, Romo-González T. Your health is in your mouth: a comprehensive view to promote general wellness. Front Oral Health. 2022;3:971223. doi:10.3389/froh.2022.971223
2. Waldman HB, Rader R, Perlman SP. Health related issues for individuals with special health care needs. Dental Clin North America. 2009;53(2):183–10. doi:10.1016/j.cden.2008.12.008
3. Brown LF, Ford PJ, Symons AL. Periodontal disease and the special needs patient. Periodontology. 2017;74(1):182–193. doi:10.1111/prd.12198
4. Khan AJ, Sabri BAM, Ahmad MS. Factors affecting provision of oral health care for people with special health care needs: a systematic review. Saudi Dental J. 2022;34(7):527–537. doi:10.1016/j.sdentj.2022.08.008
5. Lewis C, Robertson AS, Phelps S. Unmet dental care needs among children with special health care needs: implications for the medical home. Pediatrics. 2005;116(3):e426–e431. doi:10.1542/peds.2005-0390
6. Shah AH, Fateel A, Al-Nakhli O. Dentists and dental students opinion regarding dental treatment of patients with special needs. JPDA. 2011;20(2):98–104.
7. Asiri FYI, Tennant M, Kruger E. Disabilities and disparities in oral health-related quality of life: a systematic review and meta-analysis in Saudi Arabia. Medicina. 2024;60(12):2005. doi:10.3390/medicina60122005
8. Kane SF. The effects of oral health on systemic health. General Dentistry. 2017;65(6):30–34.
9. Gabre P. Strategies for the prevention of dental caries in people with disabilities: a review of risk factors, adapted preventive measures and cognitive support. J Disability Oral Health. 2009;10(4):184.
10. Anders PL, Davis EL. Oral health of patients with intellectual disabilities: a systematic review. Special Care Dentistry. 2010;30(3):110–117. doi:10.1111/j.1754-4505.2010.00136.x
11. McPherson M, Weissman G, Strickland BB, PCv D, Blumberg SJ, Newacheck PW. Implementing community-based systems of services for children and youths with special health care needs: how well are we doing? Pediatrics. 2004;113(Supplement_4):1538–1544. doi:10.1542/peds.113.S4.1538
12. Naseem M, Shah AH, Khiyani MF, et al. Access to oral health care services among adults with learning disabilities: a scoping review. Annali di stomatologia. 2016;7(3):52. doi:10.11138/ads/2016.7.3.052
13. Al Agili DE, Roseman J, Pass MA, Thornton JB, Chavers LS. Access to dental care in Alabama for children with special needs: parents’ perspectives. J Am Dent Assoc. 2004;135(4):490–495. doi:10.14219/jada.archive.2004.0216
14. Lalic M, Aleksic E, Gajic M, Milic J, Malesevic D. Does oral health counseling effectively improve oral hygiene of orthodontic patients? Eur J Paediatric Dent. 2012;13(3):181–186.
15. Williams JR. The Declaration of Helsinki and public health. Bulletin World Health Organization. 2008;86(8):650–652. doi:10.2471/BLT.08.050955
16. Fischman SL. Current status of indices of plaque. J Clinical Periodontol. 1986;13(5):371–374. doi:10.1111/j.1600-051X.1986.tb01475.x
17. Thikkurissy S, Lal S. Oral health burden in children with systemic diseases. Dental Clin North America. 2009;53(2):351–357. doi:10.1016/j.cden.2008.12.004
18. Zhou N, Wong HM, Wen YF, Mcgrath C. Oral health status of children and adolescents with intellectual disabilities: a systematic review and meta-analysis. Dev Med Child Neurol. 2017;59(10):1019–1026. doi:10.1111/dmcn.13486
19. Carter A, Clarke L, Stevens C. Dental health for children with special educational needs and disability. Paediatrics Child Health. 2022;32(8):290–296. doi:10.1016/j.paed.2022.05.003
20. Murshid EZ. Oral health status, dental needs, habits and behavioral attitude towards dental treatment of a group of autistic children in Riyadh, Saudi Arabia. Saudi Dent J. 2005;17(3):132–139.
21. Mehta V, Tripathy S, Merchant Y, et al. Oral health status of children with intellectual and developmental disabilities in India: a systematic review and meta-analysis. BMC Pediatric. 2024;24(1):748. doi:10.1186/s12887-024-05242-8
22. Faulks D, Hennequin M. Evaluation of a long-term oral health program by carers of children and adults with intellectual disabilities. Special Care Dentistry. 2000;20(5):199–208. doi:10.1111/j.1754-4505.2000.tb00020.x
23. Shah AH, Wyne AH, Asiri FY, et al. Effectiveness of Preventive Oral Health Measures among Special Care School Children (boys) in Al-Kharj, Saudi Arabia. J Clin Diagn Res. 2020;14(8):1.
24. Shah AH, Wyne AH, Gulzar S, et al. Effectiveness of Oral Health Promotion among Teachers and Parents of Special Care School Children in Al-Kharj, Kingdom of Saudi Arabia. World. 2020;11(6):483.
25. Shyama M, Al-Mutawa SA, Honkala S, Honkala E. Supervised toothbrushing and oral health education program in Kuwait for children and young adults with Down syndrome. Special Care Dentistry. 2003;23(3):94–99. doi:10.1111/j.1754-4505.2003.tb01668.x
26. Shah A, Bindayel N, AlOlaywi F, Sheehan S, AlQahtani H, AlShalwi A. Oral health status of a group at a special needs centre in AlKharj, Saudi Arabia. J Disabil Oral Health. 2015;16(3):79–85.
27. AlJameel AH, Gulzar S, Gupta M, et al. Oral health promotion among individuals with intellectual disabilities: a systematic review. Eur J Dent. 2024;18(01):055–064. doi:10.1055/s-0043-1768151
28. Borromeo G, Bramante G, Betar D, Bhikha C, Cai Y, Cajili C. Transitioning of special needs paediatric patients to adult special needs dental services. Aus Dent J. 2014;59(3):360–365. doi:10.1111/adj.12197
29. Catteau C, Faulks D, Pereira B, Hennequin M. Could a national oral health promotion program improve the oral hygiene of persons attending special care establishments in France? Evaluation of a pilot program. Special Care Dentistry. 2019;39(1):10–19. doi:10.1111/scd.12338
30. AlJameell A. Oral health-related quality of life outcomes for individuals with disabilities: a review. J Clin Diagn. 2020;14:1–6.
31. da Fonseca MA, Hong C. Improving oral health for individuals with special health care needs. Pediatric Dentistry. 2007;29(2):98–104.
32. Shah AH, Al Refeai M, Alolaywi FM, Gulzar S, Asiri FY, Al Jameel AB. Satisfaction of Oral Health Education among Parents and Caregivers Regarding Children with Special Healthcare Needs in Riyadh, Saudi Arabia. J Contemporary Dental Pract. 2021;22(8):894–899. doi:10.5005/jp-journals-10024-3141
33. Al-Mashhadani S, Nasser M, Alsalami A, Burns L, Paisi M. Barriers and facilitators to dental care services utilization among children with disabilities: a systematic review and thematic synthesis. Health Expectations. 2024;27(5):e70049. doi:10.1111/hex.70049
34. Alharbi MF. An analysis of the Saudi health-care system’s readiness to change in the context of the Saudi National Health-care Plan in Vision 2030. Int J Health Sci. 2018;12(3):83.
35. Chowdhury S, Mok D, Leenen L. Transformation of health care and the new model of care in Saudi Arabia: kingdom’s Vision 2030. J Med Life. 2021;14(3):347. doi:10.25122/jml-2021-0070
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acceptance of Students with Physical Disabilities in Medical Schools in Saudi Arabia: Perception, Experience, and Recommendation
Batarfi M, Alraddadi A
Advances in Medical Education and Practice 2024, 15:231-241
Published Date: 26 March 2024