Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Impact of a Heating Voucher on Health Outcomes in COPD Patients: A Randomised Controlled Trial
Authors Viggers HE ![]() , Ingham TR
, Ingham TR ![]() , Chapman RB
, Chapman RB ![]() , Crane J, Currie AB, Davies C, Keall M, Howden-Chapman PL
, Crane J, Currie AB, Davies C, Keall M, Howden-Chapman PL
Received 21 October 2024
Accepted for publication 7 March 2025
Published 16 April 2025 Volume 2025:20 Pages 1097—1109
DOI https://doi.org/10.2147/COPD.S483194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Helen Elizabeth Viggers,1 Tristram Richard Ingham,2 Ralph Brougham Chapman,3 Julian Crane,2 Ann Beatrice Currie,4 Cheryl Davies,5 Michael Keall,1 Philippa Lynne Howden-Chapman1
1Department of Public Health, University of Otago, Wellington, New Zealand; 2Department of Medicine, University of Otago, Wellington, New Zealand; 3Environmental Studies, Victoria University of Wellington, Wellington, New Zealand; 4Community and Public Health, Canterbury District Health Board, Christchurch, New Zealand; 5Tū Kotahi Māori Asthma Trust, Lower Hutt, New Zealand
Correspondence: Helen Elizabeth Viggers, Department of Public Health, University of Otago, P.O. Box 7343, Wellington South, 6242, New Zealand, Email [email protected]
Purpose: Aotearoa New Zealand (NZ) homes are cold by international standards, with many failing to achieve temperatures recommended by WHO housing and health guidelines. Despite strong evidence of seasonal exacerbations in Chronic Obstructive Pulmonary Disease (COPD), there has been little examination of the effect of household warmth, or housing quality on COPD outcomes. The Warm Homes for Elder New Zealanders (WHEZ) study aimed to see if subsidising electricity costs would improve the health outcomes of older people with COPD. Previous analysis showed a modest, typically 2– 10% dependent on prior usage, increase in electricity use among the subsidised households.
Patients and Methods: Participants aged over 55 with doctor-diagnosed COPD were recruited from three regional centres, and where possible their dwelling was insulated after enrolment. A single-blinded randomised controlled trial of the effect of an electricity voucher (NZ$500) on health care usage during winter was carried out in three locations across New Zealand. The primary outcome was exacerbations treated with antibiotics, and/or corticosteroids. The Clinical Trial Registration is NCT01627418. Of the 520 participants assigned to a wave, partial or better data was achieved for 424; 215 of those were randomised to the early intervention group, and 209 to receive the intervention later.
Results: Despite the modest increase in energy use by study households, reported previously, there was no significant difference between study arms in the frequency of exacerbation of COPD (0.089, p=0.5875, 95% CI − 1.406– 1.584) nor hospitalisations. An exploratory analysis suggested a lower mortality among participants assigned to receive the intervention first (OR 0.310, p=0.0175, 95% CI 0.118– 0.815).
Conclusion: This study showed little effect of winter electricity vouchers on exacerbations of COPD. However, such vouchers increased energy use and may have reduced overall mortality. A larger study, particularly with susceptible subpopulations, is recommended to examine this mortality impact further.
Plain Language Summary: For many people COPD is worse in winter, but little is known about the relationship between flare-ups and indoor temperature, so we conducted a randomised controlled trial in the community. We enrolled people aged over 55 who had COPD before winter. We gave half of the participants a voucher to help with electricity bills in their first winter in the study. The second winter we gave the other half the electricity voucher. We measured electricity use, home temperature and health outcomes in both winters. We did not find an effect on COPD flare-up symptoms from giving an electricity voucher to older people with COPD. However, we did find a reduced death rate both winters among those who received the voucher their first winter. This may have been a chance finding as the study was not designed to find a reduction in death rates and that analysis was not prespecified. We conclude that more research should be done to explore this result.
Keywords: housing, respiratory, energy, older people
Introduction
One percent (0.85%) of the NZ population are estimated to have severe COPD, characterised by chronic and progressive airflow limitation and respiratory symptoms, with age-standardised prevalence for those over the age of 45 of 2.0% for all, 5.7% for indigenous Māori, and 4.6% for Pacific peoples.1 Age-adjusted mortality rates for those aged over 45 are similarly patterned; 77.0 per 100,000 for all, 169.0 per 100,000 for Māori, and 72.5 for Pacific peoples. There are strong ethnic and socioeconomic patterns of COPD hospitalisation: the most deprived quintile of the population had rates 5.17 times that of the least deprived quintile. The reasons for the association of COPD hospitalisation with lower socio-economic status are unclear.
Most syntheses of information on COPD2–4 pay little attention to indoor temperature. Nevertheless, considerable research on the relationship between outdoor temperature and COPD has found worse outcomes in winter5–7 and significant lags between cold temperatures and peak health effects.8,9 The outdoor temperature of minimum morbidity reported is typically somewhere between 22°C10 and 27°C.11 Studies have found a stronger relationship between spirometry results and bedroom temperature than for outdoor temperature,12 emphasising the importance of the indoor environment. Threshold temperatures have been suggested for increased COPD symptoms; in the USA13 when the median daily indoor temperature was below 21°C, in Scotland14 when the temperature in the living room was below 21°C for more than 9hr per day, and in China15 with temperatures below 18.2°C. Systematic reviews of the effect of indoor temperature in temperate climates on a variety of health outcomes have found that typically colder indoor temperatures were associated with worse respiratory,16,17 cardiovascular,16,17 sleep17 and general health.17 The World Health Organization (WHO) Housing and health guidelines18 suggest an appropriate minimum indoor temperature for general populations of 18°C. NZ housing is often cold by international standards.19. A survey of NZ spot temperatures found that during winter a third of dwellings (33%) had temperatures below 18°C.20 This is consistent with data from other NZ studies, which have found average dwelling temperatures ranging from 13.2 °C to 17.9°C during winter.21–25
How to reduce exacerbations was recently identified as the most pressing research need for COPD.26 Indoor temperatures can be altered by heating, as well as dwelling design, and therefore are potentially amenable to improvement through heating behaviour change. However, the cost of heating can force “heat or eat” decisions to be made by households; the proportion of household income spent on food went down during extreme cold events among the poorest householders over the period 1974–2007 in Britain.27 A Scottish study examined the effect of housing energy efficiency improvements on older COPD patients;28 the intention-to-treat analysis found no significant effects, but a pragmatic analysis found improvement in self-reported respiratory symptom scores among those who received the intervention.
Context for Current Analysis
Previous work by our group has examined the importance of indoor conditions for respiratory disease outcomes.22,29–31 The study this paper reports on was designed to examine the effect of an energy intervention on home warmth, and health outcomes. It focused on participants with COPD as they are a group with large potential for health improvement.
From 2009 to 2011, participants who had doctor-diagnosed COPD were enrolled in the Warm Homes for Elder New Zealanders study (WHEZ).32 The study aimed to test whether paying a NZ$500 (approximately US $335, £250, €300) supplement directly into participants’ electricity accounts improved their health outcomes. The amount and mode of intervention was chosen as a plausible government policy. We have previously reported on electricity use among participating households,33 which found that electricity use increased slightly overall, mostly among those using less electricity prior to enrolment in the study. Analyses of hospitalisations and mortality, measured through the New Zealand Health Information Service (NZHIS), self-reported exacerbations, and home temperatures are presented here.
Method
Intervention Rollout/Timing
The prospective randomised controlled trial used a staggered “wave” rollout to aid recruitment (Figure S1); it was conducted in the 2010–2012 winters in three geographically and demographically distinct regions of New Zealand: Whanganui, Wellington, and Christchurch. Where appropriate, insulation was retrofitted in ceilings and under floors, co-funded by a government subsidy and an insulation company.
As some of the most severe COPD patients were less likely to survive a baseline year of data collection, we designed the study with an initial autumn-baseline questionnaire, and then randomised so that half the participants received the intervention that winter (“early”), and half the following winter (“late”). Thus the “late” group was able to act as controls for the “early” group. All participants received the voucher at some stage (“early” or “late”), which we considered an ethical way of conducting the trial. The follow-up data were collected in the subsequent spring. The $500 intervention was delivered directly into the participants’ electricity accounts in early winter, and those receiving the intervention were sent a pamphlet, “How much heat can you buy for $500?” An external researcher conducted the randomisation, blocking by area and wave. Interviewers were blinded to the intervention and instructed not to ask the participants their status. Interview timings were dependent on interviewer and participant availability. Temperatures were measured in the living room, and some bedrooms (Hobo and ibutton® dataloggers). Dataloggers were run through a sequence in a temperature and humidity controlled oven and checked that their outputs were inside tolerance before deployment.
Participants
Participants were recruited through multiple health care channels including: mail-outs to previously hospitalised patients; patients enrolled with selected health-care practitioners; visits to COPD or pulmonary rehabilitation support groups; or word-of-mouth. Inclusion criteria were: age over 55 years; location in one of the three study areas; household responsible for paying its own electricity bill; not expecting to move; self-reported doctor-diagnosed COPD resulting in a hospitalisation or prescription for antibiotics or steroids in the last three years; and wishing to take part in research. Only one participant was accepted from each household. Some people who applied withdrew before they were accepted. Figure 1 shows the participant flow.
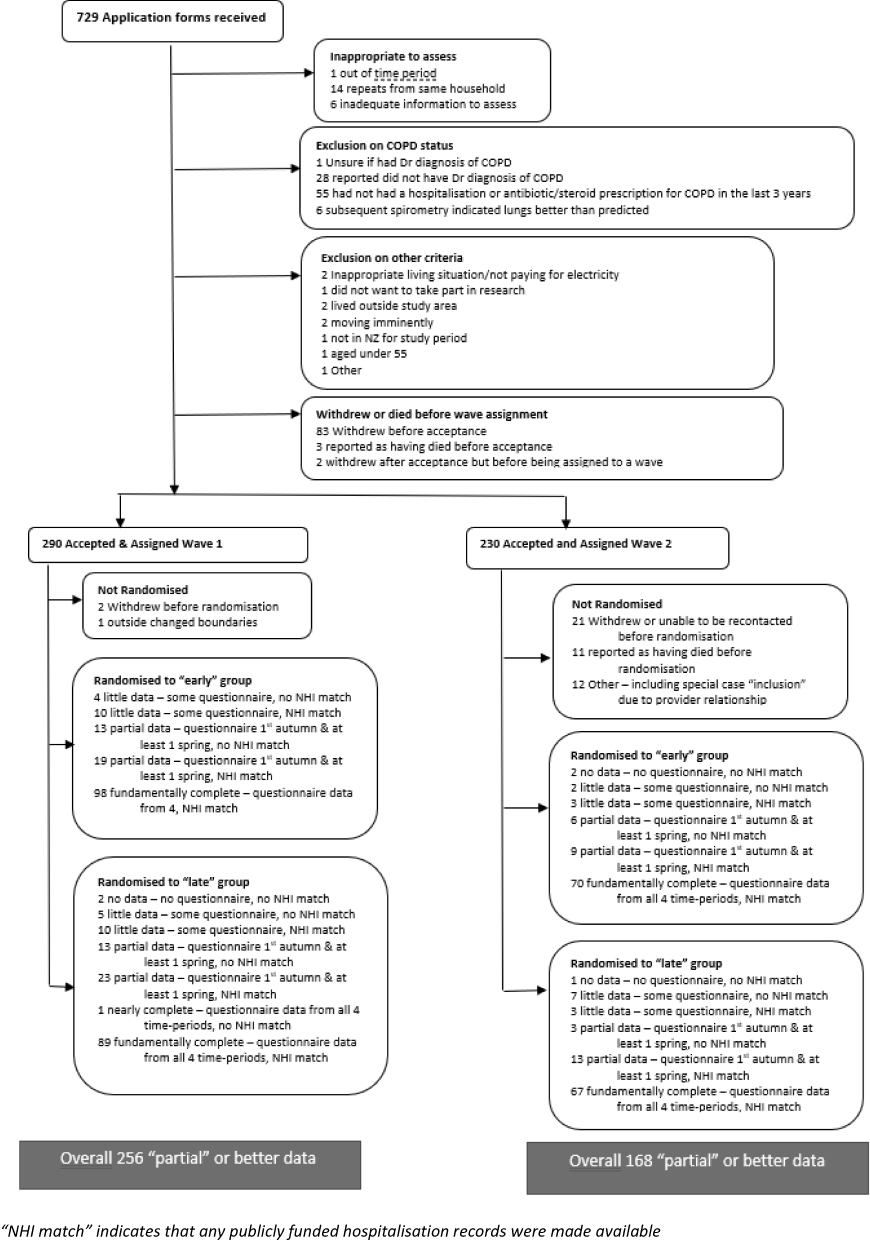 |
Figure 1 Participant flow through the WHEZ study. |
Ethics
Ethical consent was obtained from the NZ Multi-Region Ethics Committee MEC/07/05/062. The Clinical Trial Registration is NCT01627418. Written informed consent was gained from participants. The study followed the principles of the Declaration of Helsinki.34
Patient and Public Involvement
Although there was no direct patient or public involvement in the design of this research, the focus of the trial was chosen after discussions with the kaimahi (Māori healthcare workers) at Tū Kotahi Māori Asthma Trust, a grassroots healthcare organisation serving an ethnically diverse community in the Wellington region. The kaimahi identified the home warmth needs of whānau (families) with COPD as of pressing concern.
Sample Size
Sample size was calculated using results from previous studies. Our baseline hypothesis was that this intervention would achieve a similar reduction in exacerbation rates as the pharmaceutical intervention of the TORCH COPD study which used long-acting beta-agonist and inhaled corticosteroid (LABA/ICS) combination therapy,35 with the negative binomial parameters of exacerbation counts found from the TRISTAN COPD study reanalysis.36 From these, we estimated a required sample size of 478, so allowing for a 15% dropout rate, 560 participants were required. Five hundred and twenty households were recruited and assigned to a wave; however, the dropout rate was greater than anticipated and only 324 people fully completed the study.
Research Question /Outcomes
The primary research question was whether the provision of an electricity subsidy reduces the incidence of self-reported moderate or severe exacerbations of COPD. Following the TORCH COPD Study37 self-reported exacerbations were defined as an increase in usual symptoms of COPD with subclassification by severity: those requiring hospitalisation (severe); treatment with corticosteroids and/or antibiotics (moderate); those requiring any healthcare intervention; those not requiring any healthcare intervention.
We also collected hospitalisation data and International Classification of Diseases (ICD) codes from national administrative datasets. Pre-specified secondary questions relating to the hospitalisation and self-report data included severe exacerbations requiring hospitalisation, all-cause hospitalisation, and death.
Analysis
The primary analysis directly compares the intervention and control groups during the first study winter. We carried out further analyses, including data from both study winters but effectively altering the assumptions about the effect of the intervention timing, as if it were: (i) a cross-over study, thus assuming the intervention only had an effect the winter it was received; (ii) a wedge analysis, thus assuming the intervention had an effect the winter it was received and the following winter; and (iii) a continuation analysis, thus assuming that the intervention effect of the first winter continued directly into the second winter (Figure S2). This was broadly consistent with our published analysis of electricity consumed in response to the intervention.33 The “first study winter” was 2010 for wave 1, and 2011 for wave 2.
The primary outcome was number of moderate or severe exacerbations in the self-reported data. We used negative binomial models. Additional sensitivity analyses considered both binary models and three other post-hoc levels of exacerbation. We also accessed validated hospitalisation data from the national minimum dataset for publicly funded hospitalisations, using direct matching based on name, date of birth, sex and address. Missing data were not imputed, but where possible data from participants who did not remain in the study for the entire duration were included as excluding participants withdrawing due to increasing infirmity or death could bias the results of the study. We pre-specified secondary analyses of: hospitalisations for severe COPD exacerbations (main code J44), hospitalisations for key lower respiratory tract illnesses (J40-J47), all-cause hospitalisations, and deaths. We also included a post-hoc analysis of hospitalisations for circulatory conditions. Adjusted models included age-band, gender, ethnicity, the study area, and a binary variable indicating if the exacerbation level of interest had been reported in the period prior to the study commencing. Further adjustments were used for the ancillary variables of study wave, year in the study, and whether the data was collected from post-earthquake Christchurch. Due to the rarer outcome, a reduced set of adjustments were used on the mortality analyses. It was initially intended to include household insulation status in the analysis, however this proved impossible due to data collection difficulties.
We analysed hourly home living room temperatures during August (Southern Hemisphere winter), as this was the month for which data was most complete, both overall and at different times of day examining both average temperature and the exposure to temperatures below set thresholds.
A series of large earthquakes in the Christchurch region during the study caused significant disruption in many ways, including displacing participants and damaging their homes, and led us to modify inclusion criteria.32 We accounted for the earthquake disruption in the analysis in two ways: by conducting a sensitivity analysis where data collected for participants from Christchurch for winters after the earthquakes were excluded from the analysis, and by including a term in the models to indicate that the data were for post-earthquake Christchurch.
Total ethnicity was reported, as is standard for NZ: 29 (6%) of the participants reported more than one ethnicity. Owing to the ethnic distribution of the participants, ethnicity was categorised into NZ Māori and Other (predominantly a NZ European group).
Data were analysed using SAS 9.4 using the GLIMMIX procedure for generalised linear mixed models formulated with G-side random effects to adjust for any differences between the study arms and, in the relevant analyses, clustering. We followed CONSORT reporting guidelines.38
Results
Following randomisation, the baseline characteristics were appropriately distributed between the treatment and control groups (Table S1). Only rates of liver disease were significantly different at the p=0.05 level, however as 27 characteristics were considered, at least one would be expected to be significant at this level when two populations are identical. The raw counts and rates for the main outcome measure of exacerbations, treated with antibiotics or corticosteroids, are shown in Table 1. Similar information for other severities of self-reported exacerbation is reported in Table S2.
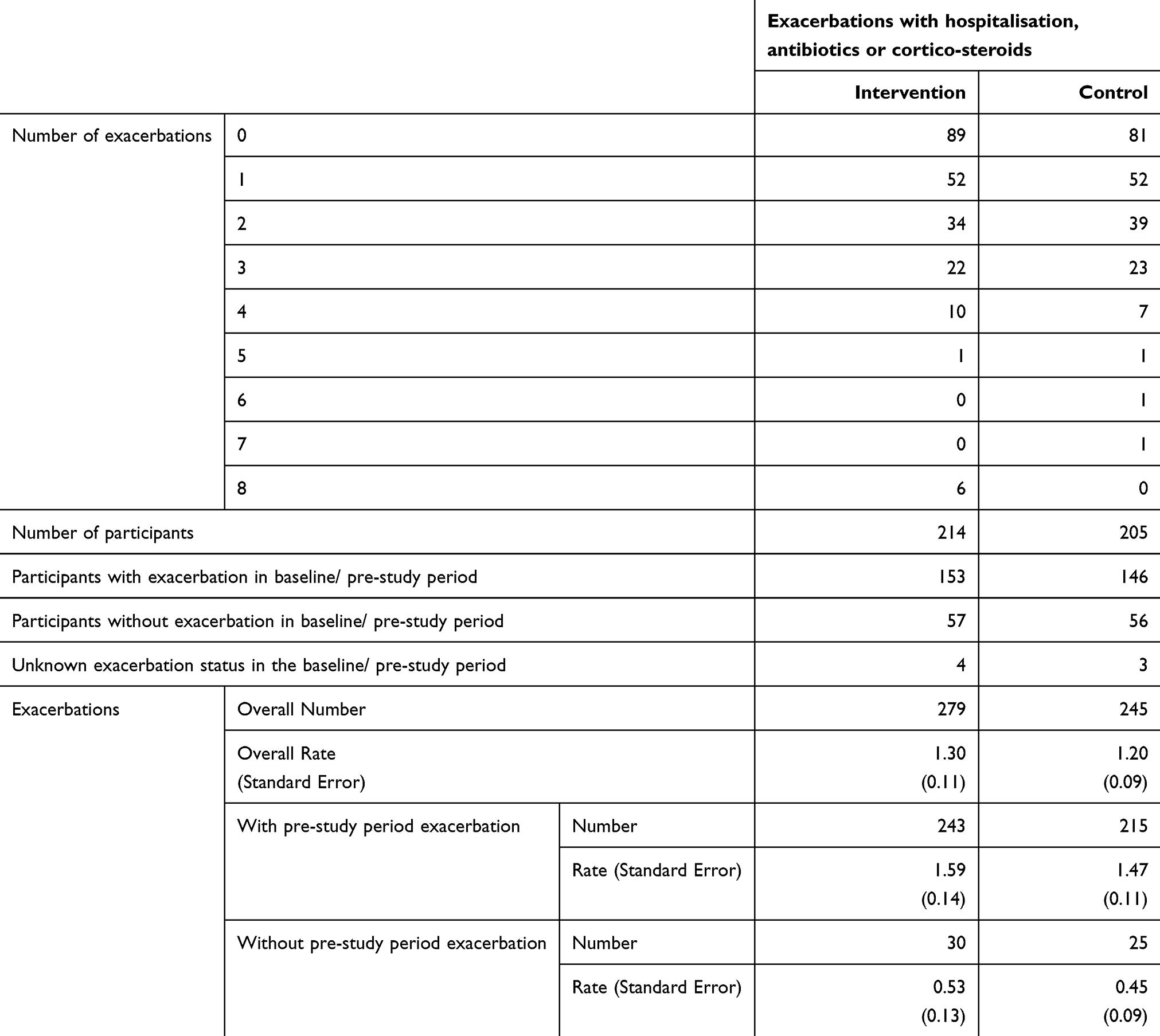 |
Table 1 Raw Numbers of Self-Reported Data for First Winter of Study |
Table 2 shows the coefficients for self-reported exacerbations analysed using negative binomial modelling. None of the results approach statistical significance. Positive coefficients indicate increased rates (worse outcomes) modelled for the intervention group. Similar effect sizes and p-values were found in the univariate analysis and analyses where other relevant variables were included in the regression. The sensitivity analyses of other severities of exacerbation, and considering binary outcomes showed a similar lack of statistical significance (Table S3a). The best predictor of exacerbations (data not shown – DNS) was a prior exacerbation. A sensitivity analysis for the effect of the earthquake (Table S3b) and other model formulations (Table S3c) show similar small effect sizes and lack of statistical significance.
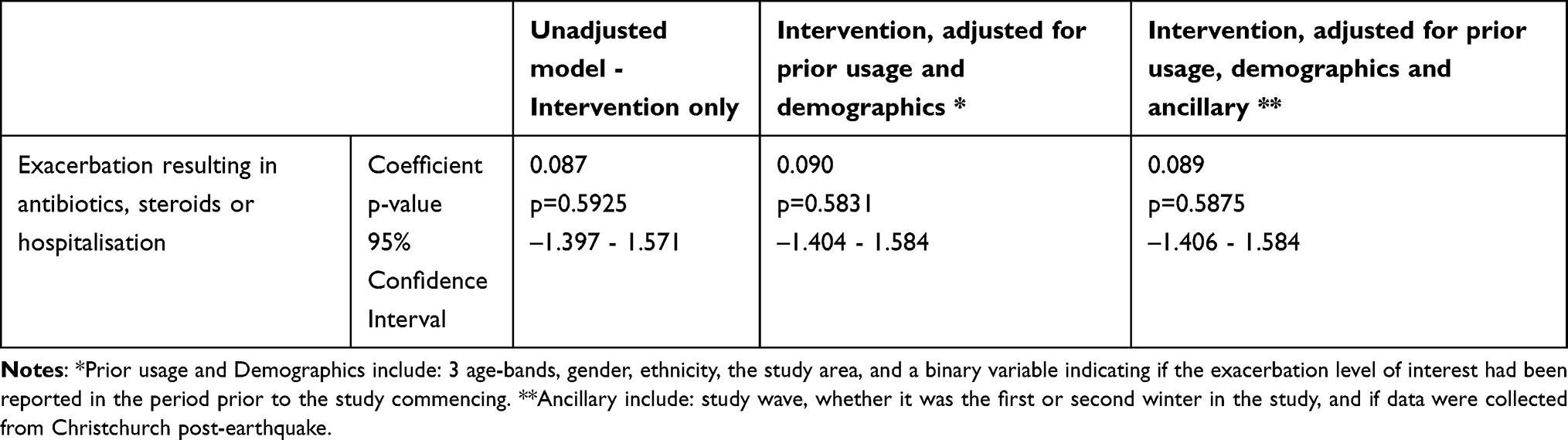 |
Table 2 Self-Reported Exacerbations – First Winter Only – Negative Binomial Model |
We analysed National Health Index (NHI) data on hospital admissions for 413 participants. Owing to the pre-existing serious illness of the study population, a pre-specified secondary analysis considered death. We considered participant survival during the winter (June to September inclusive), or “long winter” (six-month winter/spring period – June to December inclusive) (Table 3). Participants who received the intervention the first winter of the study had lower odds of dying that winter, although the effect was not statistically significant, and lower odds of dying during that “long winter”, with borderline statistical significance. Further exploratory analysis showed that the effect continued in the second winter, with those receiving the intervention early (during the first winter) continuing to have lower death rates than those who received the intervention late (the second winter).
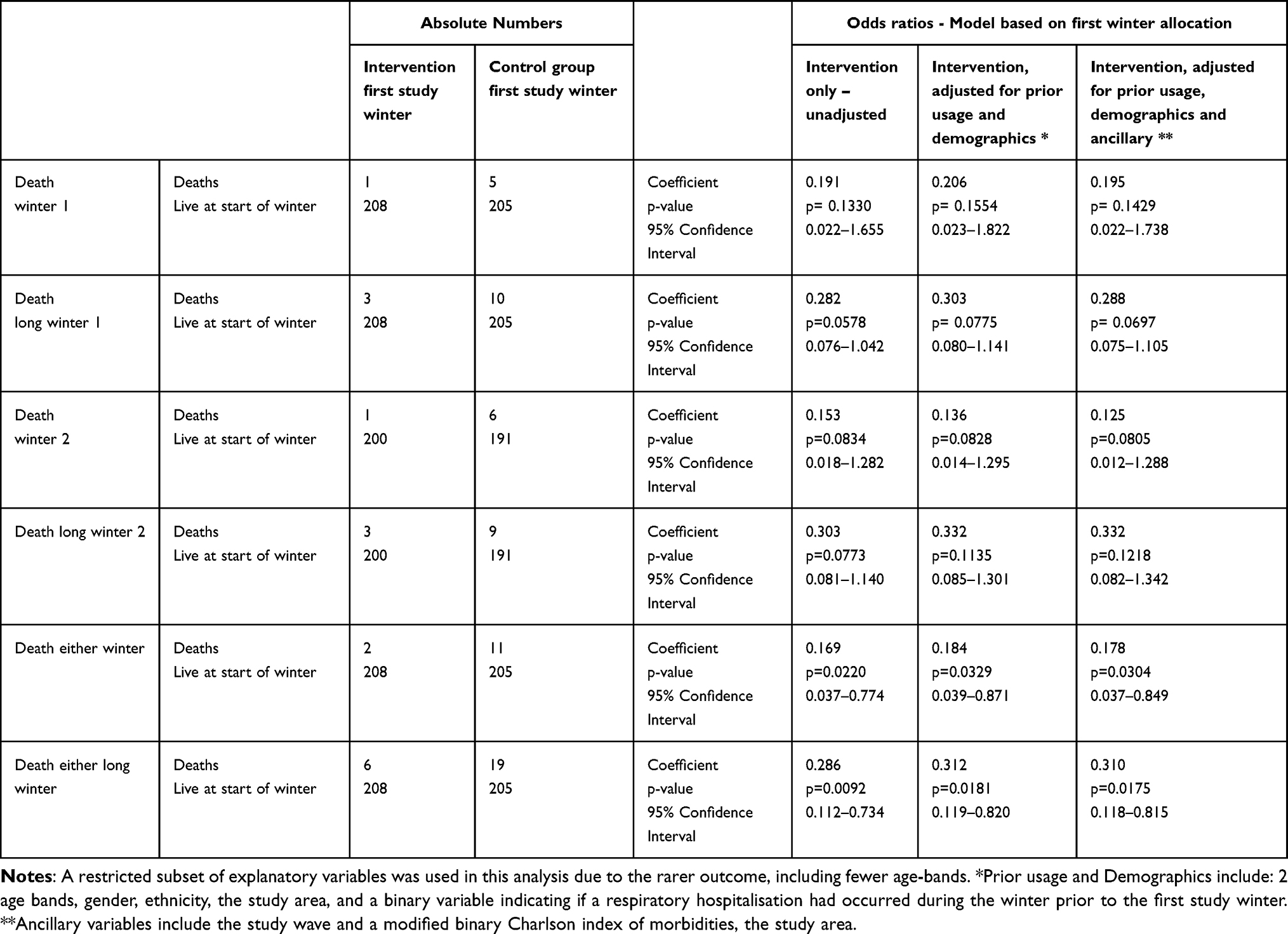 |
Table 3 Absolute Numbers of Participant Death and Odds Ratios |
These effects were of borderline statistical significance, but the lower odds of death associated with receiving the intervention first were, for either study winter, statistically significant. Assumptions about the effect of continuing study enrolment led to different ways of analysing data from the second winter (Figure S2). A continuation analysis showed a substantial reduction in the odds of death, but a cross-over analysis showed no effect, and although the effect sizes for a wedge analysis indicated a substantial reduction, the results were not statistically significant (Table S4). Similar numbers of participants from both study groups died during summer between the study winters, when the intervention was unlikely to be affecting heating behaviours.
We categorised hospitalisations by three-digit ICD code (ICD-10-AM). Table S5 shows the total counts and the numbers of participants hospitalised over the study. Over half (96/187) of all-cause hospitalisations during the study winters were for exacerbation of COPD (J44). The mean number of hospitalisations in the first winter was 0.20 for all-cause hospitalisations, 0.10 for any lower respiratory tract illness (J40-J47), 0.10 for exacerbation of COPD (J44), and 0.03 for all circulatory disorders (I00-I99).
We pre-specified secondary analyses of hospitalisation: COPD exacerbations; lower respiratory tract illnesses; and all-cause hospitalisation. Post-hoc we also considered hospitalisations for circulatory conditions. Table 4 shows these results; none were statistically significant. Sensitivity analyses (Table S6a to S6c) largely showed similar lack of effect.
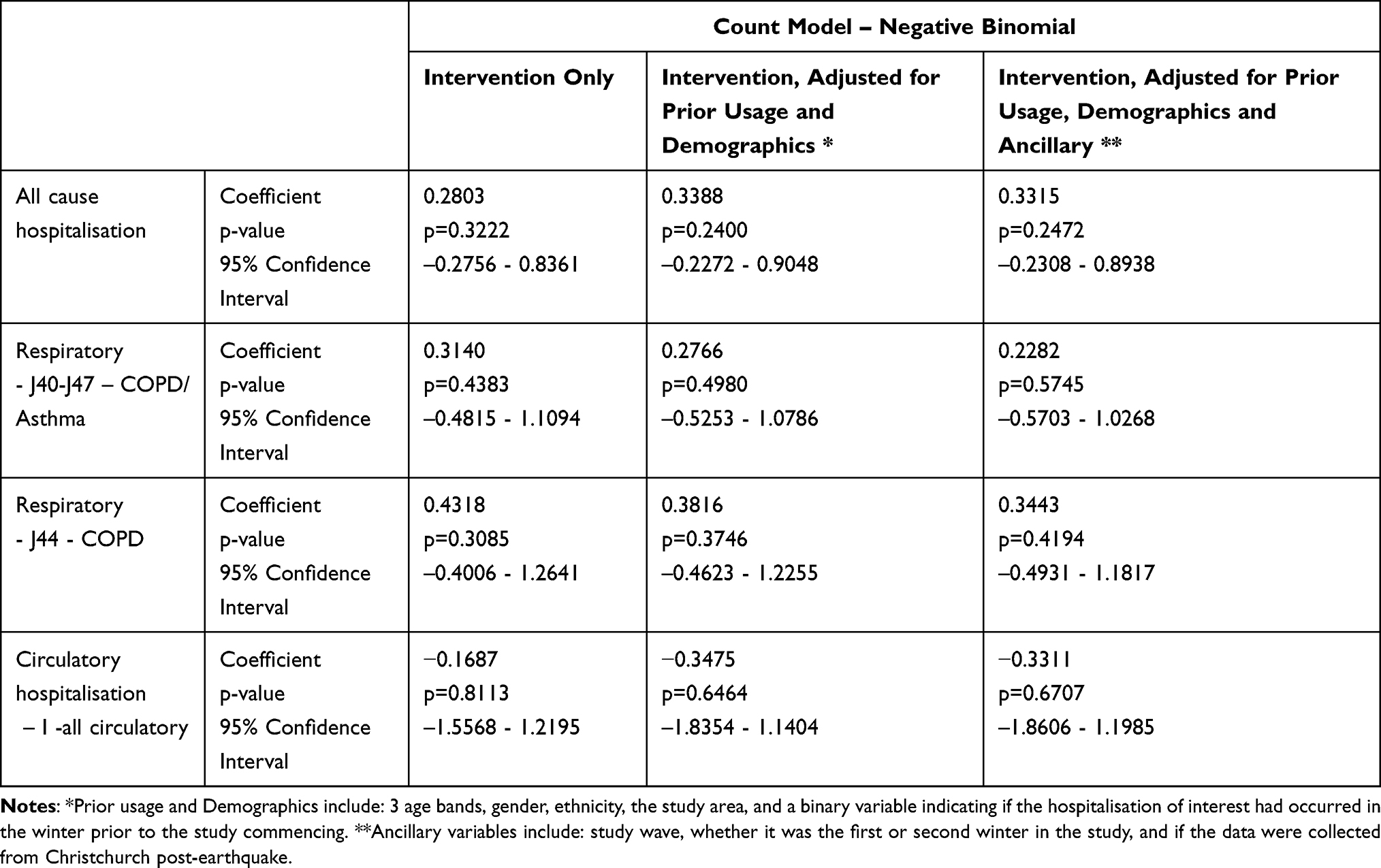 |
Table 4 Hospitalisation During First Winter From NHI Records – Count Model Negative Binomial |
The temperature analysis of first winter data showed no significant difference between the intervention and control groups (Table S7). Secondary analyses using the same crossover, wedge, and continuation analyses, found an effect only for the wedge analyses where dwellings in the wedge had less exposure to very cold temperatures (below both 12°C and 15°C). In models which included actual electricity use, greater electricity use was highly statistically significantly associated with warmer temperatures (DNS).
Discussion
Findings
The main analysis found no statistically significant benefit in the primary health outcome, ie moderate or severe exacerbations of COPD, for older people with COPD receiving a voucher for electricity to assist with heating.
As the intervention, a heating voucher and pamphlet about the benefits of heating, constituted a behavioural nudge,39 and were necessarily unblinded to the participants, we conducted secondary analyses to test whether the intervention timing had any effect. There was little evidence of a timing effect on the main and most secondary health outcomes. However, despite the short length of the study, there was a strong effect on the odds of dying, which was a pre-specified secondary outcome. The continuation analysis showed that over both winters participants who received the intervention in the first winter of the study had lower odds of dying than those randomised to receive it the second winter. The wedge analysis showed a similar effect direction but was not statistically significant. We considered death both during the study winters (OR 0.178 p=0.03) and “long winters” (winter and subsequent spring, OR 0.310 p=0.02), because of the substantial evidence showing delayed effects of low temperature.8,9,40 This lower death rate is difficult to interpret as it may be a chance effect of small numbers. We also examined the causes of hospitalisation for those who died during, or within two weeks of, a hospitalisation; however there was not a statistically significant difference (DNS).
The temperature analysis (Table S7) also showed a lack of clear effect. The most significant effects were for lower odds of exposure to very cold temperatures (less than 12°C) overnight and in the morning for the wedge analysis, and to a smaller extent less exposure to cold temperatures (less than 18°C) overnight also for the wedge analysis. Examination showed that most of the temperature difference in the wedge analysis was caused by both groups of dwellings having increased temperatures in the second year. Dwellings in which more electricity was used tended to be warmer (DNS). The associated electricity analysis previously published found there was only a small increase, 2–10%, in electricity use.33 The effect sizes indicated that to increase the average living room temperature by 1°C each month would have required approximately the entire voucher to be spent on additional energy over three months (DNS).
Strengths and Limitations
Dwellings were insulated where necessary and feasible as our prior work had identified this as a mechanism to improve home warmth and health30 and it was ethically appropriate. However, installing insulation had the potential to blunt the effect of the intervention, as both control and intervention households received it and may have already felt warmer. Although participants were referred to the insulation programme as soon as feasible after enrolment, installation took longer to occur. It was initially intended to include household insulation status as a factor in the analysis, but this proved impossible despite strong and persistent efforts at data collection, due to the devolved structure of the insulation crews. The variably delayed rollout may also have blunted the intervention effect.
Possibly those participants with disposable income and allocated to the later intervention group were in some cases prompted to “borrow” the intervention dollar amount from their savings, and heated their homes more, knowing from when they consented to be part of the study that their electricity account would be credited the following year providing they stayed enrolled.
Perhaps because of the recruitment methods, the study population was well connected to health care: over 80% had received a recent flu vaccination, similar numbers had seen a GP for their COPD in the recent past. There was a borderline statistically significant tendency in the winter prior to study enrolment, for lower health care usage in the group with the lowest levels of electricity use (Table S8). Participants with ready resources who had experienced an exacerbation may have already increased their electricity usage prior to enrolment, thereby reducing the ability of the study to capture health or temperature benefits of any behavioural change that had already occurred. Participants’ self-report of baseline conditions occurred before the randomisation; therefore, association between prior electricity use and prior health care use is unlikely to be a result of reporting biases. Baseline heating habits were not explicitly addressed in the analysis.
This study differs from other studies of COPD sufferers in that recruited people were over the age of 55, rather than 65. This was to facilitate Māori enrolment, to be explicitly pro-equity. Māori experience significant inequities with respect to COPD, including higher rates of smoking, earlier onset of COPD, higher incidence, higher prevalence, and higher mortality rates.41,42 Another feature of this study was the inclusion in the analysis of participants who did not remain in the study for the entire duration. Recognising that participants withdrawing due to increasing infirmity or death could bias the results of the study, we made the decision to include as many as possible in the analysis. The higher than anticipated drop-out rate reduced the statistical power of the study to explore many outcomes. Many of the participants who dropped out died several months later, although after the point when the next phase of data collection would have occurred. Despite our community workers’ strong efforts, we were not always able to collect the reasons for participants’ withdrawal.
The intervention amount (NZ$500) was calculated as sufficient to run a 2.4kW electric heater for 12 weeks for up to 10 hours per day. Although it was anticipated that this could substantially increase temperature in one room, in practice the effect sizes indicated that it would only have increased the living room temperatures by 1°C if the entire voucher had been spent on electricity, and this did not typically happen. Without a significant increase in indoor temperatures, few health effects were likely to be observed.
Baseline characteristics were appropriately distributed across the randomisation groups. Although slightly more participants in the later intervention group reported liver disease (p=0.0357; 5 cf 14), the groups were similar when analysed by number of participant co-morbidities (p=0.4811), by number of participant exacerbations (p=0.3072) and by participant exacerbations requiring antibiotics, cortico-steriods or hospitalisation (p=0.3415). Therefore, the study results are unlikely to be affected by obvious differences between the groups.
Study Meaning, Implications and Future Work
The causal pathway that was being examined required the participants to change their heating behaviour to have a warmer home. It was hypothesised that warmer home temperatures either directly, or through other changes in the in-home environment such as humidity or mould growth, would affect the participants’ respiratory, circulatory, physio-social, or other health.
There is no obvious causal pathway that would reduce mortality without also reducing exacerbations, therefore it is surprising to find a reduction in mortality when we did not identify a reduction in exacerbations, and notable that the reduction in mortality, in both years of the study, was for those who received the intervention in the first year of the study. Thus, the reduction in mortality may have occurred through a pathway other than the direct effect of the payment. One plausible pathway is that those who were assigned to receive the intervention “early” were motivated by their assignment to improve their health to an extent that those receiving the money “late” were not. This suggests that the “nudge”39 effect of study enrolment and the materials around it may themselves have been a crucial mechanism. It is also possible that the reduced exposure to low temperatures found in the wedge analysis indicated that some households continued heating even after the end of their intervention winter; and that the non-statistically significant reduction in mortality for the wedge analysis is a real consequence of this. However, it is also possible that results for the mortality analysis could have been either caused by some unmeasured co-morbidities or aspect of disease severity, or were significant only by chance: the study was not powered for an expected reduction in mortality, and the results were statistically significant in only one non-pre-specified secondary analysis.
Many interrelated housing factors can plausibly affect health including: dwelling temperature, dampness, thermal efficiency, ventilation, indoor pollutants, and mould. Likewise, all people with COPD have different life and health histories, income, and expenses. The utility of the randomised controlled trial design is that the randomisation process, used correctly, will balance these factors. This research addresses the very small number of trials investigating the links between home warmth and health outcomes for people with COPD. A Scottish study28 investigated the effects of improved home energy efficiency whereas this study investigated fuel vouchers. Neither found any difference in symptoms in an intention-to-treat analysis, although the Scottish study did find symptom differences in a secondary analysis. Both studies relied on participants to change their behaviour in some way and had some similar findings: both found it was challenging to create or maintain different in-home conditions between the study groups; both found some evidence that participants’ health before the study commenced may have changed their behaviour during it, and both finished under-powered. The results of these studies highlight the difficulty of conducting adequately powered trials which are needed to investigate the effect of indoor warmth on this serious condition.
Analyses of the effect of the UK Winter Fuel Payment, although not specific to COPD, have shown an increase in the amount spent on fuel43,44, and improved health including a decrease in excess winter mortality45 and a tendency for reduced disease markers in eligible households.46 In our study, the intervention amount (NZ$500) was calculated as both politically feasible to implement on a larger scale, somewhat similar to the UK Winter Fuel Payment, and sufficient to run a 2.4kW electric heater for 12 weeks for up to 10 hours per day, which could substantially increase temperature in one room. Thus, the present study addressed cold homes as a relevant policy problem, with voucher rollout being a plausible policy solution.
Since this study was carried out, NZ has introduced a “Winter Energy Payment” for elder New Zealanders receiving national superannuation payments, and some younger people receiving income support, but the effects of this are yet to be evaluated. The present study’s results suggest that the framing of the payment may be important to ensure that desirable behavioural responses and health outcomes are achieved.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; DNS, Data not shown; NZ, Aotearoa New Zealand; WHEZ, Warm Homes for Elder New Zealanders.
Data Sharing Statement
Please contact the corresponding author.
Acknowledgments
The authors would like to gratefully acknowledge the help of all the study participants, the people who worked on the study including interviewers and data-entry and data-cleaning staff, the NZ Ministry of Health, and electricity retailers that took part: Contact, Empower, EnergyDirect, Energy Online, Genesis, Just Energy, Mercury, Meridian, Nova Energy, Powershop, Pulse Utilities, and Trustpower. We valued the organisations we worked with in the study centres: Community and Public Health, Canterbury District Health Board in Christchurch; Tu Kotahi Māori Asthma Trust, Capital and Coast District Health Board in Wellington; Te Oranganui Iwi Health Authority, Whanganui Regional Primary Health Organisation, MidCentral District Health Board, Whanganui District Health Board in Whanganui.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received financial support from Autex Industries Ltd/GreenStuf ®, the Energy Efficiency and Conservation Authority, the Health Research Council of NZ (HRC 09/071) and the NZ Lottery Grants Board (250849).
Disclosure
HV and PLHC report data from the New Zealand Ministry of Health and Electricity companies; assistance with insulating dwellings from the Energy Efficiency and Conservation Authority and Autex/Greenstuf®. PLHC reports board membership of Kāinga Ora – Homes and Communities. The authors report no other conflicts of interest in this work.
References
1. Telfar-Barnard L, Zhang J. The Impact of Respiratory Disease in New Zealand: 2023 Update. University of Otago: Asthma and Respiratory Foundation NZ; 2024.
2. Jordan RE, Majothi S, Heneghan NR, et al. Supported self-management for patients with moderate to severe chronic obstructive pulmonary disease (COPD): an evidence synthesis and economic analysis. Health Technol Assess. 2015;19(36):1–516.
3. Ko FW, Cheung NK, Rainer TH, Lum C, Wong I, Hui DS. Comprehensive care programme for patients with chronic obstructive pulmonary disease: a randomised controlled trial. Thorax. 2017;72(2):122–128.
4. Korpershoek YJG, Bruins Slot JC, Effing TW, Schuurmans MJ, Trappenburg JCA. Self-management behaviors to reduce exacerbation impact in COPD patients: a Delphi study. Int J Chronic Obstr. 2017;12:2735–2746.
5. Jenkins CR, Celli B, Anderson JA, et al. Seasonality and determinants of moderate and severe COPD exacerbations in the TORCH study. Eur Respir J. 2012;39(1):38–45.
6. Rabe KF, Fabbri LM, Vogelmeier C, et al. Seasonal distribution of COPD exacerbations in the prevention of exacerbations with tiotropium in COPD trial. Chest. 2013;143(3):711–719.
7. Wise RA, Calverley PM, Carter K, Clerisme-Beaty E, Metzdorf N, Anzueto A. Seasonal variations in exacerbations and deaths in patients with COPD during the TIOSPIR((R)) trial. Int J Chronic Obstr. 2018;13:605–616.
8. Chen J, Yang J, Zhou M, et al. Cold spell and mortality in 31 Chinese capital cities: definitions, vulnerability and implications. Environ Int. 2019;128:271–278.
9. Monteiro A, Carvalho V, Gois J, Sousa C. Use of “Cold Spell” indices to quantify excess chronic obstructive pulmonary disease (COPD) morbidity during winter (November to March 2000-2007): case study in Porto. Int J Biometeorol. 2013;57(6):857–870.
10. Song G, Chen G, Jiang L, et al. Diurnal temperature range as a novel risk factor for COPD death. Respirology. 2008;13(7):1066–1069. doi:10.1111/j.1440-1843.2008.01401.x
11. Wang YC, Lin YK. Association between temperature and emergency room visits for cardiorespiratory diseases, metabolic syndrome-related diseases, and accidents in metropolitan Taipei. PLoS One. 2014;9(6):e99599.
12. Donaldson GC, Seemungal T, Jeffries DJ, Wedzicha JA. Effect of temperature on lung function and symptoms in chronic obstructive pulmonary disease. Eur Respir J. 1999;13:844–849.
13. McCormack MC, Paulin LM, Gummerson CE, Peng RD, Diette GB, Hansel NN. Colder temperature is associated with increased COPD morbidity. Eur Respir J. 2017;49(6)1601501.
14. Osman LM, Ayres JG, Garden C, Reglitz K, Lyon J, Douglas JG. Home warmth and health status of COPD patients. Eur J Public Health. 2008;18(4):399–405.
15. Zhe M, Chen P-L, Geng F-H, et al. Synergistic effects of temperature and humidity on the symptoms of COPD patients. Int J Biometeorol. 2017;61(11):1919–1925.
16. Jevons R, Carmichael C, Crossley A, Bone A. Minimum indoor temperature threshold recommendations for English homes in winter - A systematic review. Public Health. 2016;136:4–12.
17. Janssen H, Ford K, Gascoyne B, et al. Cold indoor temperatures and their association with health and well-being: a systematic literature review. Public Health. 2023;224:185–194.
18. World Health Organization. WHO Housing and Health Guidelines. Geneva: World Health Organization; 2018.
19. Howden-Chapman P, Viggers H, Chapman R, O’Dea D, Free S, O’Sullivan K. Warm homes: drivers of the demand for heating in the residential sector in New Zealand. Energy Policy. 2009;37(9):3387–3399.
20. Statistics New Zealand. Housing in-Aotearoa2020. 2020.
21. Howden-Chapman P, Crane J, Matheson A, et al. Retrofitting houses with insulation to reduce health inequalities: aims and methods of a clustered, randomised community-based trial. Soc Sci Med. 2005;61(12):2600–2610.
22. Howden-Chapman P, Pierse N, Nicholls S, et al. Effects of improved home heating on asthma in community dwelling children: randomised controlled trial. Br Med J. 2008;337(7674):337.
23. Isaacs N, Camilleri M, Burrough L, et al. Energy use in New Zealand households: final report on the household energy end-use project (HEEP). BRANZ;2010.
24. Rangiwhetu L, Pierse N, Howden-Chapman P. Effects of minor household interventions to block draughts on social housing temperatures: a before and after study. Kotuitui. 2017;12(2):235–245.
25. Rangiwhetu L, Pierse N, Viggers H, Howden-Chapman P. Cold New Zealand Council Housing getting an Upgrade. Policy Quarterly. 2018;14(2):65–73.
26. Alqahtani JS, Aquilina J, Bafadhel M, et al. Research priorities for exacerbations of COPD. Lancet Respir Med. 2021;9(8):824–6.
27. Beatty TKM, Blow L, Crossley TF. Is there a ‘heat-or-eat’ trade-off in the UK? J Royal Stat Society Series a-Stat Society. 2014;177(1):281–294.
28. Osman LM, Ayres JG, Garden C, Reglitz K, Lyon J, Douglas JG. A randomised trial of home energy efficiency improvement in the homes of elderly COPD patients. Eur Respir J. 2010;35(2):303–309.
29. Free S, Howden-Chapman P, Pierse N, Viggers H, Housing Heating Hlth Study R. More effective home heating reduces school absences for children with asthma. J Epidemiol Community Health. 2010;64(5):379–386.
30. Howden-Chapman P, Matheson A, Crane J, et al. Effect of insulating existing houses on health inequality: cluster randomised study in the community. Br Med J. 2007;334(7591):460–464.
31. Woodcock A. Moulds and asthma: time for indoor climate change? Thorax. 2007;62(9):745–746.
32. Viggers H, Howden-Chapman P, Ingham T, et al. Warm homes for older people: aims and methods of a randomised community-based trial for people with COPD. BMC Public Health. 2013;13(176):1–2.
33. Viggers H, Keall M, Howden-Chapman P, et al. Effect of an electricity voucher on electricity use. Energy Policy. 2019;134:110985.
34. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
35. Calverley PMA, Anderson JA, Celli B, et al. Supplementary Appendix 1 to Calverley PMA, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–789.
36. Keene ON, Jones MRK, Lane PW, Anderson J. Analysis of exacerbation rates in asthma and chronic obstructive pulmonary disease: example from the TRISTAN study. Pharm Stat. 2007;6:89–97.
37. Vestbo J, Study Group T. The TORCH (towards a revolution in COPD health) survival study protocol. Eur Respir J. 2004;24(2):206–210.
38. Schulz KF, Altman DG, Moher D, Group CCONSORT. Statement: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010;63(8):834–840.
39. Thaler RH, Sunstein CR. Nudge: Improving Decisions About Health, Wealth and Happiness. New Haven: Yale University Press; 2008.
40. Pierse N, Arnold R, Keall M, et al. Modelling the effects of low indoor temperatures on the lung function of children with asthma. J Epidemiol Community Health. 2013;67(11):918–925.
41. Telfar Barnard L, Zhang J. The Impact of Respiratory Disease in New Zealand: 2020 Update. Asthma and Respiratory Foundation NZ; 2021.
42. Ministry of Health. Tatau Kahukura Māori Health Chart Book 2015.
43. Beatty TKM, Blow L, Crossley TF, O’Dea C. Cash by any other name? Evidence on labeling from the UK winter fuel payment. J Public Econ. 2014;118:86–96.
44. Munro A, Walker I, Zhu Y Ostensible hypothecation: the effect on fuel expenditure of cash transfers to the elderly for fuel.
45. Iparraguirre J. Have winter fuel payments reduced excess winter mortality in England and Wales? J Public Health. 2015;37(1):26–33.
46. Crossley TF, Zilio F. The Health Benefits of a Targeted Cash Transfer: The UK Winter Fuel Payment. Institute for Fiscal Studies; 2017.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.