Back to Journals » OncoTargets and Therapy » Volume 14
Immunotherapy-Related Cardiotoxicity Re-Emergence in Non-Small Cell Lung Cancer – A Case Report
Authors Li Y, Hu Y, Yang B, Jin C, Ren H, Wu J, Wang Z, Wei Y, Yang L, Hu Y
Received 14 August 2021
Accepted for publication 29 October 2021
Published 23 November 2021 Volume 2021:14 Pages 5309—5314
DOI https://doi.org/10.2147/OTT.S333242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Yuanxiang Li,* Yang Hu,* Bin Yang, Caibao Jin, Hui Ren, Jingyi Wu, Zhijun Wang, Youying Wei, Ling Yang, Yanping Hu
Department of Oncology, Hubei Cancer Hospital, TongJi Medical College, Huazhong University of Science and Technology, Wuhan, 430079, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanping Hu
Department of Oncology, Hubei Cancer Hospital, TongJi Medical College, Huazhong University of Science and Technology, Wuhan, 430079, Hubei, People’s Republic of China
Email [email protected]
Abstract: PD-1/PD-L1 inhibitors activate immunological response and have become one of the main modalities of cancer treatment. However, they may result in the immune-related adverse events (irAEs). Immune-related cardiotoxicity is relatively rare but may become fatal. We will present a case of a male patient who experienced immunotherapy-related cardiotoxicity one year after received pembrolizumab treatment. The patient had atypical symptom presentation initially, but his condition deteriorated worsened rapidly and he developed severe cardiac disease. The patient experienced significant relief after corticosteroid treatment. Unfortunately, he experienced a reoccurence of the severe adverse event when discontinuing the use of corticosteroids. Ultimately, larger doses and longer courses of corticosteroid treatment cured the heart damage. Fortunately, we observed that lesions were stable and maintained for a long time after cessation of using pembrolizumab for eight months.
Keywords: PD-1/PD-L1 inhibitors, immune-related cardiotoxicity, non-small cell lung cancer
Introduction
Programmed death ligand-1 (PD-L1), which is expressed on tumor cells, combines to programmed death receptor-1 (PD-1) on T lymphocyte, thus results in the ineffectiveness of lymphocyte and is involved in immune escape and tumor progression.1–3 PD-1/PD-L1 inhibitors can activate immunological response and enhance therapeutic activity via blocking the combination of PD-L1 and PD-1.4,5 Accordingly, PD-1/PD-L1 inhibitors have become one of the main modalities of cancer treatment.6
Despite the success of PD-1/PD-L1 inhibitors on activating anti-tumor immunity, the immune-related adverse events (irAEs) caused by abnormal activation of immunity response cannot be ignored.7,8 They may cause various toxicities in skin, gastrointestinal tract, liver, and lungs.9,10 Although the immune-related cardiotoxicity is relatively rare, it may induce potentially fatal consequence.11 The mechanism may be that T lymphocytes can recognise the common antigens in heart tissues and further contribute to cardiac damage.12 The symptoms of immune-related cardiotoxicity vary from asymptomatic elevation of cardiac markers and electrocardiograph (ECG) abnormalities, shortness of breath, angina pectoris, heart failure, and arrhythmias to cardiogenic shock.13–16 Corticosteroids were the main treatment alternative in dealing with immunotherapy-induced cardiotoxicity.17 Here, we report a case in which the patient developed cardiotoxicity resulted from application of pembrolizumab and relieved with corticosteroid treatment, while the disease symptoms reappears after discontinuation of corticosteroid. Treatment with larger doses and longer courses of corticosteroid treatment ultimately heal the heart damage. Fortunately, we observed that lesions were stable and maintained for a long time after cessation of using pembrolizumab for eight months.
Case Presentation
A 62-year-old male with past medical history of hypertension and coronary heart disease was diagnosed with EGFR/ALK/ ROS1-negative, stage IV lung adenocarcinoma. He received six cycles of pembrolizumab treatment combined with pemetrexed-cisplatin and eight cycles of pembrolizumab therapy. The patient remained in partial disease remission when undergoing CT (as shown in Figure 1).
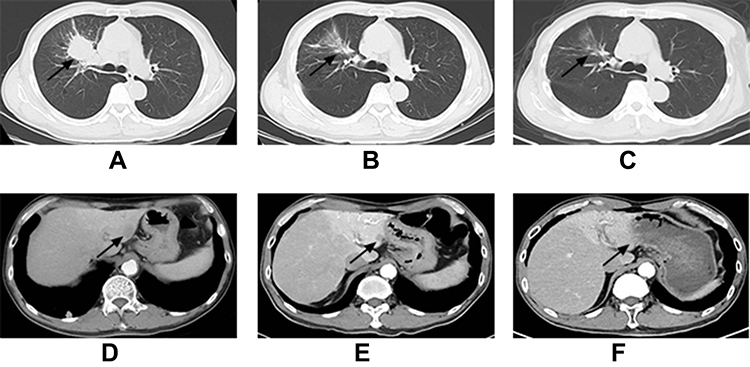 |
Figure 1 (A–C) Right lung lesions showed by CT scan (arrows). (A) Right upper lobe mass (arrow) measures approximately 4.0 cm shows in the first chest CT scan. (B) The lung lesions shrunk after PD-1/PD-L1 inhibitors treatment. (C) The lung lesions remained stable after discontinuation of pembrolizumab for eight month. (D–F) Liver metastatic lesions shown by CT scan. (D) Liver metastatic lesions (arrow) measures approximately 1.7 cm showsin the first abdominal CT scan. (E) Liver metastatic lesions measures approximately 1.1 cm after PD-1/PD-L1 inhibitors treatment. (F) Liver metastatic lesions disappeared after discontinuation of pembrolizumab for eight month. |
One year after being on pembrolizumab immunotherapy, he presented to the emergency department with subacute features including fever (the axillary temperature is 39°C), lethargy, and cognitive dysfunction. Initial laboratory data of the patient, including blood counts, liver functional indexes and procalcitonin were not significantly abnormal. While further laboratory evaluations revealed the level of myoglobin, troponin and creatinine elevated (as shown in Table 1). In addition, ECG characteristics distinctly indicated atrial fibrillation (fast ventricular rate type) as shown in Figure 2. Together, these results illustrated that he had immune-related cardiotoxicity and kidney toxicity. This patient was received methylprednisolone (80mg/day) treatment for consecutive seven days. During the course of corticosteroids administration, the body temperature of this patient returned to normal, and his cognitive function gradually recovered. Meanwhile, the level of myocardial enzyme and creatinine restored to normal, and the rhythm reverted to sinus rhythm. In the following two weeks, he was administrated with a tapering dose of methylprednisolone. Meanwhile, pembrolizumab was discontinued after the patient developed severe irAE.
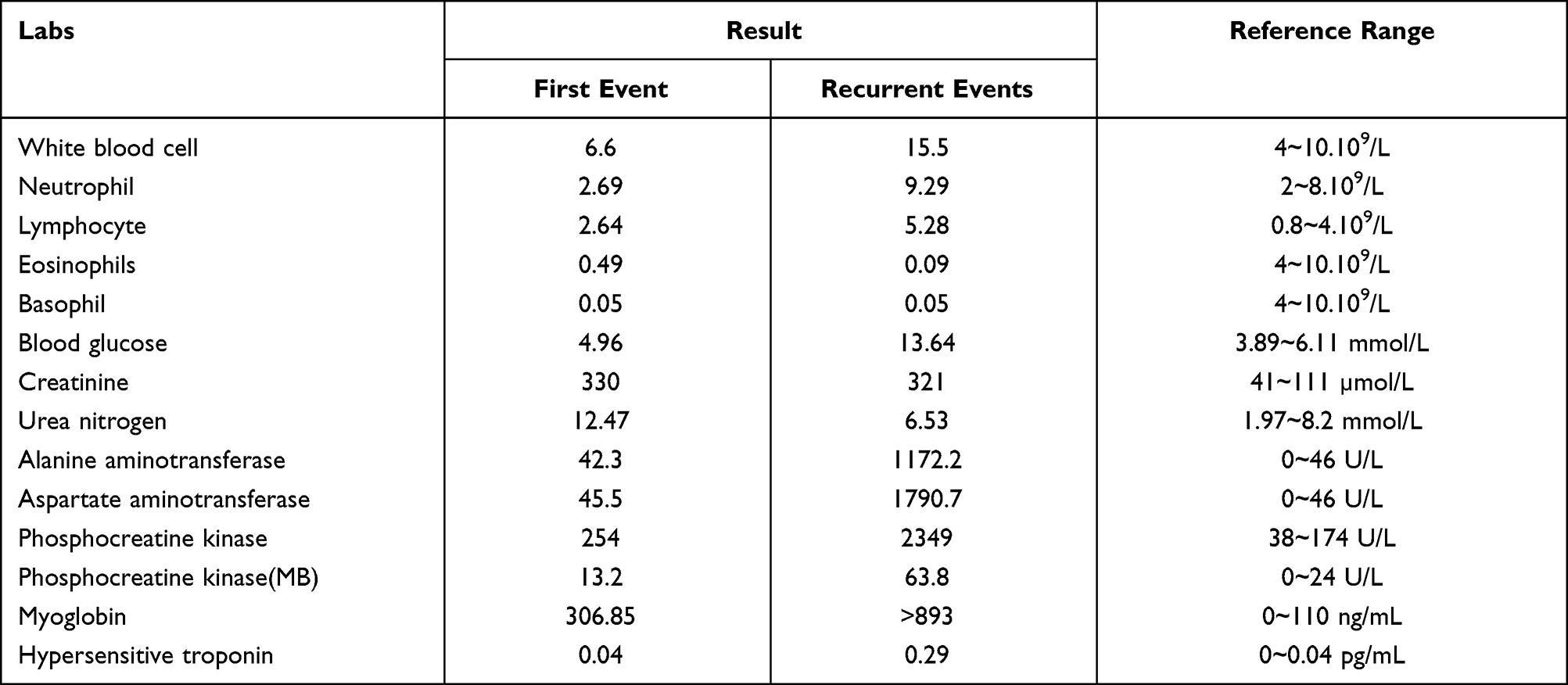 |
Table 1 Initial Workup by Serum Laboratory Testing |
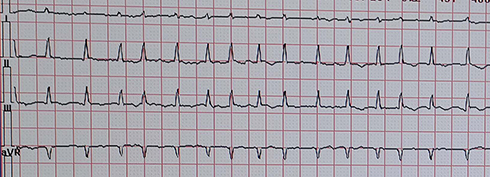 |
Figure 2 Electrocardiography obtained on admission for abnormal manifestations of serum myocardial enzyme spectrum. Rate of 168 beats per minute. Intervals in milliseconds: PR 70, QRS duration 68, QT 186, QTc 274. The electrocardiography indicated atrial fibrillation (fast ventricular rate type). |
Unfortunately, he presented to the emergency department once again with a semi-comatose condition two weeks after cessation of corticoids. He was found to be tachypneic (respiratory rate of 30), hypoxic (peripheral oxygen saturation of 85% on room air), and hypotension (blood pressure 70/30 mmHg), and oliguria (250 mL within past 24 hours). Initial serum laboratory data showed that (as shown in Table 1): white blood count elevated, accompanied with increased serum levels of CK-MB, myoglobin and troponin. Meanwhile, both markers of liver and kidney dysfunction were elevated. With integrative analysis upon the clinical manifestation and laboratory results, he was considered to have immune-related multiple organ injury, including the injury of heart, liver, and kidney. He was admitted to the intensive care unit (ICU) and was performed with hepatoprotective treatment and continuous renal replacement therapy (CRRT). With the treatment of methylprednisolone dose (240 mg/day) for seven days, the symptoms and physical signs were alleviated and the main laboratory indexes were improved. Interestingly, the patient developed fever again when corticoids were discontinued, and the body temperature returned to normal with low dose of corticoids. He was treated with a tapering dose of corticosteroid in the following 10 weeks.
Fortunately, the lung lesions remained stable, while the liver metastatic lesions disappeared after discontinuation of pembrolizumab for eight month (as shown in Figure 1). The patient maintained effective tumor control after cessation of pembrolizumab for eight months up to now.
Discussion
PD-1/PD-L1 inhibitors become the preferable alternative for driver gene-negative NSCLC patients.6 Mono-therapy with pembrolizumab is recommended as the first line treatment in high PD-L1 expression patients. While for those with low expression of PD-L1, they may benefit greater from a combination of immunotherapy with chemotherapy.18 In this case, the EGFR/ALK/ROS1 status of the patient was negative and PD-L1 expression was not tested. Correspondingly, the combination treatment of pembrolizumab with pemetrexed/cisplatin was applied. The patient remained in partial disease remission in the combination treatment phase and in mono-therapy with pembrolizumab phase.
PD-1/PD-L1 inhibitors can be associated with common and uncommon irAEs, which result from misdirected stimulation of the immune system.19 The common irAEs include endocrinopathies, dermatitis, pneumonitis, colitis and hepatitis.20 Meanwhile, uncommon irAEs, such as cardiotoxicity, have also been reported. The incidence of immune-related cardiotoxicity is 1.14%, but the fatality rate is as high as 46%.13,21 It usually occurs 21–75 days after initiative immunotherapy, with a median time of 34 days.13 In this case, the time to onset of cardiotoxicity was one year. As shown in trails, cardiotoxicity may be diagnosed range from 2 to 454 days after the initiation treatment,11 immune-related cardiotoxicity requiring management persist even emerge over time.
Signs and symptoms vary depending on the degree of involvement. Mild symptoms are atypical, mainly including chest pain, shortness of breath, palpitations and arrhythmia.13 Some clinical manifestation may be asymptomatic, while some patients may develop acute heart failure and death.22,23 Troponin elevation (94%) and ECG abnormalities (89%) appeared in nearly all myocarditis cases.13 Troponin is the most sensitive indicator (94–100%), while creatine kinase and myoglobin is valuable indicator generally applied in early diagnosis. Nearly 50% of patients have decreased ejection fraction in cardiac ultrasound evaluation.13 Cardiac MRI is the most sensitive approach for cardiac morphology evaluating, which can reflect cardiac fibrosis and inflammation.24 In some cases, endocardial myocardial biopsy, which is standard but invasive approach, was needed.25,26 In this case, the patient presented with sudden high fever, lethargy, and cognitive dysfunction, which are not consistent with cardiotoxicity. While the features involved elevated myocardial enzymes and ECG abnormalities suggested myocardial injury. Reviewing this case, the early symptoms of immunotherapy cardiotoxicity are not typical, and the patients receiving immunotherapy have elevated myocardial enzymes. Therefore, continuous monitoring of myocardial enzymes and electrocardiogram deserve to be regarded as significant and important for immediate detection of immune-related cardiotoxicity during PD-1/PD-L1 inhibitors treatment. The presence of one or more serum enzymes and ECG abnormalities exist is worthy of attention.
The primary treatment of immune-related cardiotoxicity is immunosuppression, and large dose of corticosteroids is urgent.19 Studies have suggested that initiation of high-dose corticosteroids was beneficial for recovery of ventricular function as well as for reducing the burden of major adverse cardiac events.11,13 Therefore, the corticosteroids should be applied without any further delay for confirmatory testing. Besides, infliximab, intravenous immunoglobulin, anti-thymocyte globulin and plasma exchange are potential alternatives.27–29 In this case, since immune-related cardiotoxicity was diagnosed, methylprednisolone was applied immediately. With enhanced corticosteroid treatment, the symptoms were relieved as well as myocardial enzymes gradually turned to normal levels. Afterwards, the dose of corticosteroids was gradually reduced in the following two weeks. However, two weeks after cessation of corticoids, the patient developed multiple organ injury (heart, liver and kidney). When dealing with the recurrence of irAEs, increased dose with 240 mg methylprednisolone per day was used. And the course of corticosteroid treatment was significantly longer than the previous course. The patient recovered once again with enhanced corticosteroid treatment. Conclusively, for the recurrence of cardiotoxicity, we consider that the inadequate of does and course of corticosteroids may be the major cause of recurrence. However, the recurrence of immune-related cardiotoxicity has been reported rarely, and this needs to be a cause for concern.
Previous reports revealed that the occurrence of irAEs may be related to the outcome. Patients with skin toxic effects showed significantly improved overall survival and progression-free survival.30 The relationship between outcome and the development of irAE (pruritus, rash, and thyroid disease) was examined.31 In this case, although the patient had developed immune-related cardiotoxicity, he had improved outcome. The lung lesions remained stable, while the liver metastatic lesions disappeared after cessation of pembrolizumab for eight months. We reported the relationship between outcome and the development of immune-related cardiotoxicity. We deduced that immune activation maintained for a long time. While previous reports have suggested that irAEs are associated with response rates, this case suggests that they might be also related to PFS.
Conclusion
In this case, the patient experienced immunotherapy-related cardiotoxicity after receiving treatment of pembrolizumab for one year. Since immune-related cardiotoxicity was diagnosed, corticosteroids were used and the immunotherapy-related cardiotoxicity was relieved. However, two weeks after cessation of corticoids, serve irAEs reappeared. Larger doses and longer courses of corticosteroids may be an effective alternative when dealing with the re-emergence of irAEs. To the best of our knowledge, the cases with a recurrence of immune-related cardiotoxicity are rare, and re-emergence of serve irAEs should be more of a cause for concern. In addition, although the patient had developed immune-related cardiotoxicity, the disease control remained excellent after cessation of pembrolizumab for eight months. Despite examining the relationship between outcome and the development of irAE (pruritus, rash, and thyroid disease), the relationship between outcome and immune-related cardiotoxicity has been reported rarely. We understand that more data are needed to verify the relationship between outcome and the development of irAE.
Ethics Approval and Consent for Publication
This research was approved by the Ethical Committee of Huazhong University of Science and Technology, and written informed consent for publication of the clinical details and images was obtained from the patient, and did not require institutional approval to publish the case details.
Disclosure
Yuanxiang Li and Yang Hu are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Seidel JA, Otsuka A, Kabashima K. Anti-PD-1 and anti-CTLA-4 therapies in cancer: mechanisms of action, efficacy, and limitations. Front Oncol. 2018;8:86. doi:10.3389/fonc.2018.00086
2. Swaika A, Hammond WA, Joseph RW. Current state of anti-PD-L1 and anti-PD-1 agents in cancer therapy. Mol Immunol. 2015;67(2 Pt A):4–17. doi:10.1016/j.molimm.2015.02.009
3. Hsieh T-C, Wu JM. Tumor PD-L1 induction by resveratrol/piceatannol may function as a Search, Enhance, and Engage (“SEE”) signal to facilitate the elimination of “cold, non-responsive” low PD-L1-expressing tumors by PD-L1 blockade. Int J Mol Sci. 2019;20(23):5969. doi:10.3390/ijms20235969
4. Wolchok JD. PD-1 blockers. Cell. 2015;162(5):937. doi:10.1016/j.cell.2015.07.045
5. Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018;359(6382):1350–1355. doi:10.1126/science.aar4060
6. Havel JJ, Chowell D, Chan TA. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat Rev Cancer. 2019;19(3):133–150.
7. Johnson DB, Chandra S, Sosman JA. Immune checkpoint inhibitor toxicity in 2018. JAMA. 2018;320(16):1702–1703. doi:10.1001/jama.2018.13995
8. Akturk HK, Michels AW. Adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378(12):1163–1164.
9. Champiat S, Lambotte O, Barreau E, et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol. 2016;27(4):559–574. doi:10.1093/annonc/mdv623
10. Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. 2016;54:139–148. doi:10.1016/j.ejca.2015.11.016
11. Escudier M, Cautela J, Malissen N, et al. Clinical features, management, and outcomes of immune checkpoint inhibitor–related cardiotoxicity. Circulation. 2017;136(21):2085–2087. doi:10.1161/CIRCULATIONAHA.117.030571
12. Varricchi G, Galdiero MR, Marone G, et al. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open. 2017;2(4):e000247.
13. Mahmood SS, Fradley MG, Cohen JV, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. 2018;71(16):1755–1764. doi:10.1016/j.jacc.2018.02.037
14. Lyon AR, Varricchi G, Galdiero MR, et al. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018;19(9):e447–e458. doi:10.1016/S1470-2045(18)30457-1
15. Michel L, Rassaf T, Totzeck M. Biomarkers for the detection of apparent and subclinical cancer therapy-related cardiotoxicity. J Thorac Dis. 2018;10(Suppl 16):S4282–S4295. doi:10.21037/jtd.2018.08.15
16. Spisarova M. [Immunotherapy-associated myocarditis]. Klin Onkol. 2020;33(1):20–22. Czech. doi:10.14735/amko202020
17. Zhou Y-W, Zhu Y-J, Wang M-N, et al. Immune checkpoint inhibitor-associated cardiotoxicity: current understanding on its mechanism, diagnosis and management. Front Pharmacol. 2019;10:1350. doi:10.3389/fphar.2019.01350
18. Saxena P, Singh PK, Malik PS, et al. Immunotherapy alone or in combination with chemotherapy as first-line treatment of non-small cell lung cancer. Curr Treat Options Oncol. 2020;21(8):69. doi:10.1007/s11864-020-00768-2
19. Ganatra S, Neilan TG. Immune checkpoint inhibitor-associated myocarditis. Oncologist. 2018;23(8):879–886. doi:10.1634/theoncologist.2018-0130
20. Kadono T. [Immune-related adverse events by immune checkpoint inhibitors]. Nihon Rinsho Meneki Gakkai Kaishi. 2017;40(2):83–89. Japanese. doi:10.2177/jsci.40.83
21. Moslehi JJ, Salem JE, Sosman JA, Lebrun-Vignes B, Johnson DB. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet. 2018;391(10124):933. doi:10.1016/S0140-6736(18)30533-6
22. Laubli H, Balmelli C, Bossard M, Pfister O, Glatz K, Zippelius A. Acute heart failure due to autoimmune myocarditis under pembrolizumab treatment for metastatic melanoma. J Immunother Cancer. 2015;3:11. doi:10.1186/s40425-015-0057-1
23. Samara Y, Yu CL, Dasanu CA. Acute autoimmune myocarditis and hepatitis due to ipilimumab monotherapy for malignant melanoma. J Oncol Pharm Pract. 2019;25(4):966–968. doi:10.1177/1078155218755868
24. Aquaro GD, Perfetti M, Camastra G, et al. Cardiac MR with late gadolinium enhancement in acute myocarditis with preserved systolic function: ITAMY Study. J Am Coll Cardiol. 2017;70(16):1977–1987. doi:10.1016/j.jacc.2017.08.044
25. Heinzerling L, Ott PA, Hodi FS, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J Immunother Cancer. 2016;4(1):50. doi:10.1186/s40425-016-0152-y
26. Koelzer VH, Rothschild SI, Zihler D, et al. Systemic inflammation in a melanoma patient treated with immune checkpoint inhibitors—an autopsy study. J Immunother Cancer. 2016;4(1):13. doi:10.1186/s40425-016-0117-1
27. Kwon HJ, Cot TR, Cuffe MS, et al. Case reports of heart failure after therapy with a tumor necrosis factor antagonist. Ann Intern Med. 2003;138(10):807–811. doi:10.7326/0003-4819-138-10-200305200-00008
28. Rodriguez ER, Skojec DV, Tan CD, et al. Antibody-mediated rejection in human cardiac allografts: evaluation of immunoglobulins and complement activation products C4d and C3d as markers. Am J Transplant. 2005;5(11):2778–2785. doi:10.1111/j.1600-6143.2005.01074.x
29. Kobashigawa J, Crespo-Leiro MG, Ensminger SM, et al. Report from a consensus conference on antibody-mediated rejection in heart transplantation. J Heart Lung Transplant. 2011;30(3):1977–1987. doi:10.1016/j.healun.2010.11.003
30. Berner F, Bomze D, Diem S, et al. Association of checkpoint inhibitor–induced toxic effects with shared cancer and tissue antigens in non–small cell lung cancer. JAMA Oncol. 2019;5(7):1043–1047. doi:10.1001/jamaoncol.2019.0402
31. Maher VE, Fernandes LL, Weinstock C, et al. Analysis of the association between adverse events and outcome in patients receiving a programmed death protein 1 or programmed death ligand 1 antibody. J Clin Oncol. 2019;37(30):2730–2737. doi:10.1200/JCO.19.00318
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.