Back to Journals » ImmunoTargets and Therapy » Volume 10
Immunotherapy of Multiple Myeloma: Promise and Challenges
Authors Abramson HN
Received 15 July 2021
Accepted for publication 25 August 2021
Published 9 September 2021 Volume 2021:10 Pages 343—371
DOI https://doi.org/10.2147/ITT.S306103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Hanley N Abramson
Wayne State University, Department of Pharmaceutical Sciences, Detroit, MI, 48201, USA
Correspondence: Hanley N Abramson
Wayne State University, Department of Pharmaceutical Sciences, 259 Mack Ave, Detroit, Mi, 48201, USA
Tel +1 248 420 5335
Email [email protected]
Abstract: Whereas the treatment of MM was dependent solely on alkylating agents and corticosteroids during the prior three decades, the landscape of therapeutic measures to treat the disease began to expand enormously early in the current century. The introduction of new classes of small-molecule drugs, such as proteasome blockers (bortezomib and carfilzomib), immunomodulators (lenalidomide and pomalidomide), nuclear export inhibitors (selinexor), and histone deacetylase blockers (panobinostat), as well as the application of autologous stem cell transplantation (ASCT), resulted in a seismic shift in how the disease is treated. The picture changed dramatically once again starting with the 2015 FDA approval of two monoclonal antibodies (mAbs) – the anti-CD38 daratumumab and the anti-SLAMF7 elotuzumab. Daratumumab, in particular, has had a great impact on MM therapy and today is often included in various regimens to treat the disease, both in newly diagnosed cases and in the relapse/refractory setting. Recently, other immunotherapies have been added to the arsenal of drugs available to fight this malignancy. These include isatuximab (also anti-CD38) and, in the past year, the antibody-drug conjugate (ADC) belantamab mafodotin and the chimeric antigen receptor (CAR) T-cell product idecabtagene vicleucel (ide-cel). While the accumulated benefits of these newer agents have resulted in a doubling of the disease’s five-year survival rate to more than 5 years and improved quality of life, the disease remains incurable. Almost without exception patients experience relapse and/or become refractory to the drugs used, making the search for innovative therapies all the more essential. This review covers the current scope of anti-myeloma immunotherapeutic agents, both those in clinical use and on the horizon, including naked mAbs, ADCs, bi- and multi-targeted mAbs, and CAR T-cells. Emphasis is placed on the benefits of each along with the challenges that need to be overcome if MM is to be considered curable in the future.
Keywords: multiple myeloma, monoclonal antibodies, antibody-drug conjugates, bi-specific antibodies, chimeric antigen receptor T-cells, cytokine release syndrome
Introduction
Multiple myeloma (MM) is characterized by clonal proliferation of plasma cells in the bone marrow accompanied by high levels of monoclonal immunoglobulins in the urine and/or blood. In the United States, the disease ranks second behind non-Hodgkin’s lymphoma (NHL) as a hematological cancer and 14th among all cancers in terms of incidence. According to current estimates, in 2021 MM will be diagnosed in a total of 34,920 individuals (55.3% male) and will be responsible for 12,410 deaths in the U.S.1 The median age at diagnosis is 69 years, which has been trending lower in recent years. Significant racial disparities have been noted for all stages of MM with the prevalence of the disease in the US being substantially greater among African Americans than among Caucasians.2 For example, in one analysis of the SEER (Surveillance, Epidemiology, and End Results) data base, maintained by the National Cancer Institute (NCI), it was found that the annual incidence of the disease per 100,000 population among Caucasians is 6.1 for men and 4.0 for women compared to 13.2 and 9.6, respectively, for African Americans.3
The tetrad of symptoms that typically accompanies an active case of MM is known by the acronym CRAB: hypercalcemia, renal insufficiency, anemia, and bone lesions. An active case often is preceded by an asymptomatic state, monoclonal gammopathy of undetermined significance (MGUS), with a risk of progression from MGUS to MM of about 1% per year.4 A second asymptomatic phase, smoldering multiple myeloma (SMM), intermediate between MGUS and MM, also has been described.5,6 Current guidelines for the diagnosis and treatment of MM have been issued by the National Comprehensive Cancer Network (NCCN).7 While the cause of MM remains unknown, cytogenetic anomalies are known to play a role in some MM patients classified as “high risk”. The most frequently encountered of these variances are the chromosomal deletion del(17p) and the transversions t(14;16) and t(4;14).8
Remarkable progress has attended the treatment of MM over the past half century. Starting in the mid-1960’s and continuing for nearly three decades, two alkylating agents, melphalan (Alkeran®)9 and cyclophosphamide (Cytoxan®), often in regimens that included corticosteroids, were the mainstays of MM therapy. The addition of autologous stem cell transplantation (ASCT) to the MM treatment landscape in the 1990s further improved therapeutic outcomes. However, the picture began to change dramatically by the end of the decade with the discovery of thalidomide’s remarkable immunomodulatory effects that conferred anti-myeloma activity on this once ignominiously regarded drug. Two close chemical derivatives of thalidomide, lenalidomide (Revlimid®) (2005) and pomalidomide (Pomalyst®) (2013), soon supplanted thalidomide for MM. Meanwhile, the discovery of the potent anti-myeloma actions of proteasome inhibitors led to the introduction of bortezomib (Velcade®) (2003), later followed by the mechanistically similar carfilzomib (Kyprolis®) and ixazomib (Ninlaro®), as important additions to the anti-myeloma arsenal. The list of US Food and Drug Administration (FDA)-approved small molecules that work by additional mechanisms to treat MM has recently expanded to include the pan-histone deacetylase inhibitor panobinostat (Farydak®) (2015) and the nuclear export blocker selinexor (Xpovio®) (2019). The cumulative benefits of these therapeutic advances can be seen in the 2.26-fold increase of the MM five-year survival rate over the period from 1975–77 (24.6%) to 2011–17 (55.6%),10 as well as in the median survival, which has increased from 2.5 years in the mid-1990s to 5.7 years today.11
Treatment options for MM underwent a paradigm shift beginning with the 2015 approval by the FDA of two monoclonal antibodies (mAbs), daratumumab (Darzalex®) and elotuzumab (Empliciti®), followed by additional immunotherapies, including a third mAb, isatuximab (Sarclisa®), an antibody-drug conjugate (belantamab mafodotin; Blenrep®), and idecabtagene vicleucel (Abecma®), the first chimeric antigen receptor (CAR) T-cell product for the disease. This review is intended to cover the fundamental aspects of these newer agents and the prospects for additional immunotherapeutic agents that now occupy the anti-myeloma pipeline.12 For recent reviews of the background, history, and current status of the applications of immunotherapy to cancer treatment, the reader is directed to the recent publications of Esfahani,13 Waldman,14 and Tan.15
CD38 as a Monoclonal Antibody Target
CD38, which has elicited much interest as a target in MM, is a 45 kDa transmembrane glycoprotein, expressed at high levels in both normal and neoplastic plasma cells, as well as at lower levels by a number of other blood cells.16 This important surface biomarker is known to perform several roles in cells. These functions include, among others, acting as a receptor for CD31 (platelet endothelial cell adhesion molecule; PECAM-1) and as an ectoenzyme with cyclic ADP ribose hydrolase activity, the products of which are important regulators of intracellular calcium levels.17,18
The principal mechanisms by which anti-CD38 antibodies are lethal to myeloma cells are three-fold: antibody-dependent cellular cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), and complement-dependent cytotoxicity (CDC). In addition, crosslinks between CD38 on myeloma cells and effector cell Fcγ receptors may be responsible for initiation of apoptosis of myeloma cells.19 Moreover, anti-CD38 antibodies have demonstrated immunomodulatory actions by blocking myeloid-derived suppressor cells and regulatory T- and B-cells.20
In 2015, daratumumab, a fully human IgG1k mAb directed against CD38, became the first immunotherapeutic agent approved for treatment of MM. Approval was granted based on supporting data from two Phase III trials – CASTOR (NCT02136134) and POLLUX (NCT02076009) – wherein the mAb and dexamethasone were combined with either a proteasome inhibitor (bortezomib)21 or an immunomodulator (lenalidomide).22 Initial approval limited daratumumab-dexamethasone use to monotherapy in patients who had relapsed following a minimum of three prior therapies that included either a proteasome inhibitor or an immunomodulator. However, daratumumab-dexamethasone in combination with proteasome inhibitors and/or immunomodulators has since assumed a key role in even earlier courses of anti-myeloma therapy as data from additional phase III trials demonstrated more sustained responses and good tolerability from such combinations, including use in newly diagnosed patients whether ASCT-eligible23 or -ineligible.24
Current NCCN treatment guidelines for MM, based on most favorable response and safety data, include one triplet protocol (daratumumab- lenalidomide-dexamethasone); and a number of quartet regimens which include, in addition to daratumumab-bortezomib-corticosteroid (dexamethasone or prednisone), either an alkylating agent (cyclophosphamide or melphalan) or an immunomodulator (lenalidomide or thalidomide).7 Moreover, combinations with pomalidomide25 and more recently carfilzomib26,27 also have received FDA approval for use in relapsed and/or refractory MM (RRMM). Several network meta-analytic studies of random controlled trials provide further evidence of daratumumab’s benefits in various myeloma-based settings.28 In addition, recent FDA approval of a subcutaneous (sc) formulation of daratumumab combined with hyaluronidase provides the substantial benefit of enabling markedly shorter administration times – 3–5 minutes vs several hours of intravenous (iv) infusion of the mAb without compromising efficacy or patient safety.29–31
Infusion reactions, which include dyspnea, rash, headache, cough, nausea, vomiting, and nasal congestion represent an adverse, although generally low grade, effect of daratumumab, being noted in up to 50% of patients receiving the drug, especially during the first two infusions. Pre-medication with a glucocorticoid and/or a leukotriene blocker (montelukast) may help mitigate this effect and may be particularly useful in patients with underlying respiratory disease.32 Also, the drug can interfere with blood typing due to its capacity for binding to CD38 on reagent blood cells, resulting in a positive indirect Coombs test. This can be circumvented by conducting patient blood-typing procedures prior to using daratumumab.33 The risk of infection, primarily due to the bone marrow suppression, also has been shown to accompany use of the agent and necessitates use of prophylactic antimicrobials, such as co-trimoxazole to prevent Pneumocystis carinii pneumonia and antivirals. Table 1 contains a partial list of current clinical trials that include daratumumab.
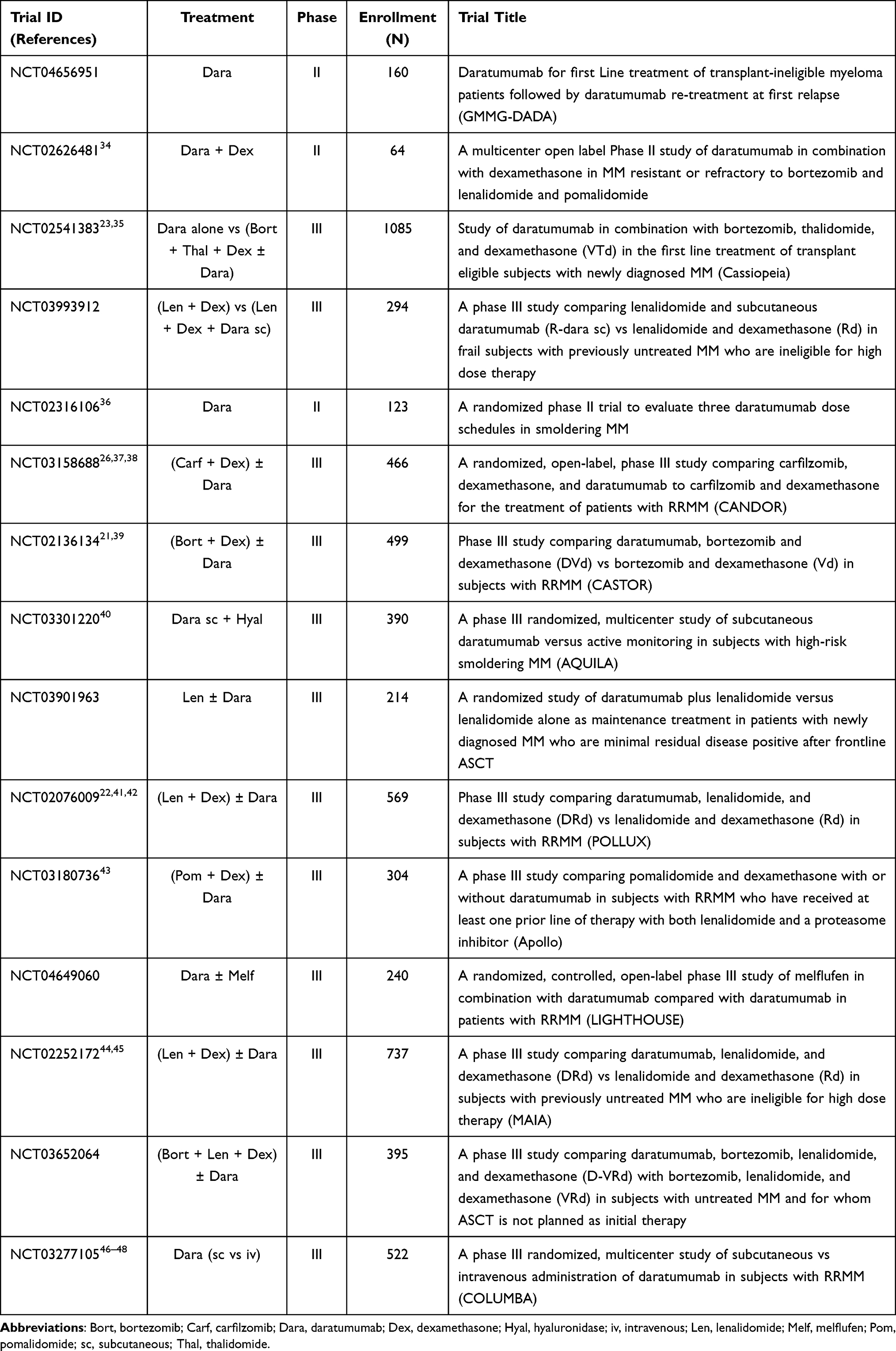 |
Table 1 Selected Clinical Trials of Daratumumab in Multiple Myeloma (MM) |
Isatuximab, a more recent addition to the anti-CD38 mAb arsenal, differs from daratumumab in that it represents a chimeric mouse-human IgG1k construct. Its mechanism of action is similar to that of daratumumab although cross-linking apparently is not a prerequisite for apoptosis induction.49 Initial FDA approval of isatuximab (March 2020) specified its use for the treatment of RRMM in combination with pomalidomide and dexamethasone in patients who have failed at least two prior therapies, including lenalidomide and a proteasome inhibitor.50 This was based on the results of the phase III ICARIA trial in which addition of isatuximab to RRMM patients receiving pomalidomide-dexamethasone exhibited significantly longer PFS (11.5 months vs 6.5 months).51,52 Subsequently (March 2021), the combination of isatuximab-dexamethasone with carfilzomib was approved for treatment of RRMM patients who had received one to three prior therapies. Approval in this case was predicated on efficacy and safety data from the phase III IKEMA study (NCT03275285) in which the cohort receiving the isatuximab-based regimen exhibited a 45% reduction in the risk of disease progression or death compared to that given carfilzomib-dexamethasone alone.53–55 Infusion reactions and upper respiratory infections are the most common adverse reactions noted for isatuximab. An isatuximab formulation intended for subcutaneous use is currently the subject of an ongoing clinical trial (NCT04045795). Several of the current isatuximab-containing clinical trials are shown in Table 2.
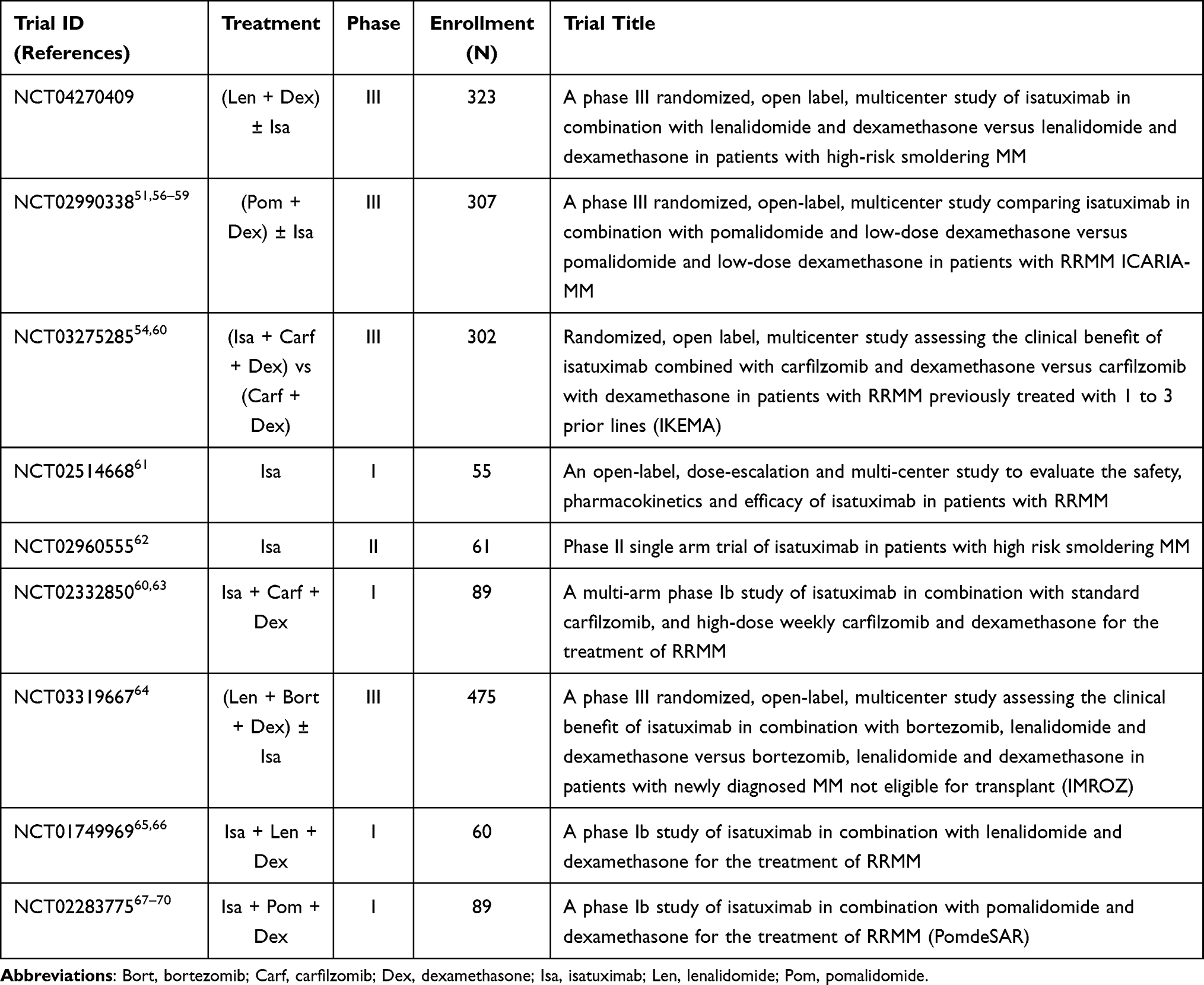 |
Table 2 Selected Clinical Trials of Isatuximab in Multiple Myeloma (MM) |
Other anti-CD38 mAbs that have been investigated for MM include felzartamab (MOR202), TAK-573, and mezagitamab (TAK-079). The first of these has been dropped by its sponsor from further consideration in MM while the other two, developed by Takeda, remain in early phase clinical trials – NCT03215030 (iv) and NCT03984097 (sc), respectively.
SLAMF7 as a Monoclonal Antibody Target
Members of the signaling lymphocytic activation molecule family (SLAMF) of proteins are highly expressed on the surface of plasma cells, both normal and from MM patients, as well as natural killer (NK) cells, but not on other blood cells or other body tissues. While mAbs directed against SLAMF3 and SLAMF6 (SGN-CD48A and azintuxizumab vedotin/ABBV-838, respectively) have proven unsuccessful in early stages of myeloma-directed clinical trials, SLAMF7 (CS1 or CD319) has emerged as a major target in the fight against MM. The anti-myeloma activity of SLAMF7-targeted antibodies results from their ability to initiate ADCC toward myeloma cells following activation and engagement of NK cells.71–74 The foremost anti-SLAMF7 mAb is elotuzumab, a humanized IgG1k antibody.
In 2015, shortly following its action regarding daratumumab, elotuzumab was approved for treatment of MM in the US. Approval was granted for use in combination with lenalidomide and dexamethasone in MM patients who had already received one to three prior therapies.75 Unlike daratumumab, elotuzumab lacks single-agent activity.76 The FDA’s action was prompted by the favorable results of the ELOQUENT-2 trial (NCT01239797) that included 646 RRMM patients, randomly assigned to receive the mAb combined with dexamethasone with or without lenalidomide. A progression-free survival (PFS) of 19.4 months for the elotuzumab group plus an overall response rate (ORR) of 68% after one year and 41% at two years compared very favorably to the 14.9 months and 57% and 27% exhibited by the control cohort.77 A four-year follow-up provided further confirmation of the result of this trial.78 The ELOQUENT-3 trial (NCT02654132), which investigated the use of elotuzumab-dexamethasone plus pomalidomide in RRMM patients refractory to both lenalidomide and a proteasome blocker, resulted in formal approval of this triplet therapy in patients who had received at least two prior therapies that included these two agents.79 Trials with thalidomide, another immunomodulator, have proven inferior in RRMM patients compared to those obtained with lenalidomide or pomalidomide.80 Moreover, additional trials combining elotuzumab with proteasome inhibitors – bortezomib80–82 or carfilzomib83 – have, thus far, failed to generate the level of favorable outcomes of the scale produced by immunomodulator combinations. A list of selected trials that include elotuzumab is presented in Table 3.
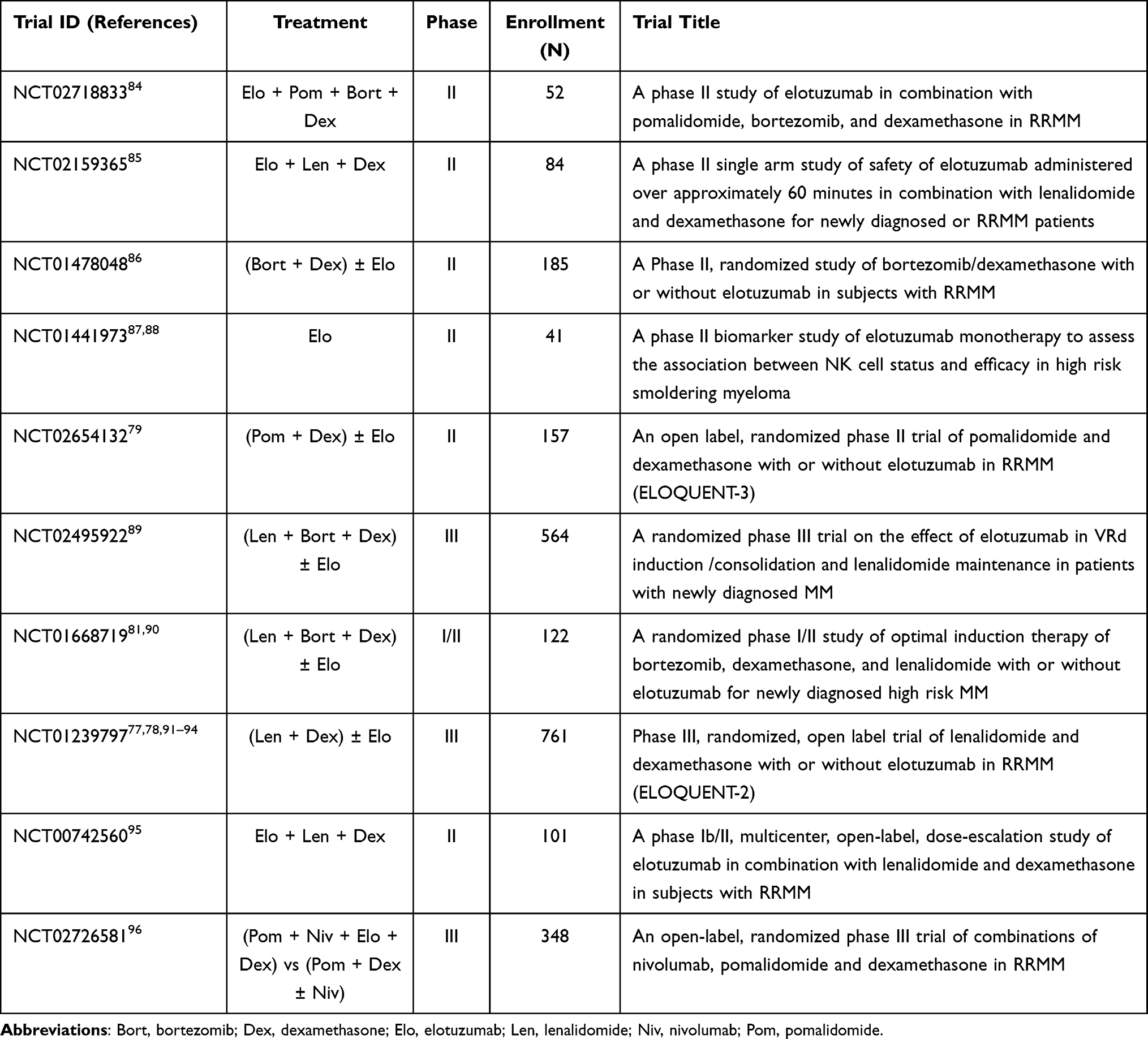 |
Table 3 Selected Trials of Elotuzumab in Multiple Myeloma (MM) |
Antibody-Drug Conjugates
Antibody-drug conjugates (ADCs) are drugs designed to kill tumor cells by chemically linking a cytotoxin (or, in some cases a radionuclide) to an antibody which targets either a tumor-specific antigen (TSA) or tumor-associated antigen (TAA). Over the past several years a number of ADCs have been developed to treat an array of malignancies, including breast cancer, acute leukemias, and Hodgkin’s lymphoma.
ADC construction is based on three components – a mAb with high specificity for a particular TAA or TSA, a small cytotoxic molecule (the payload), and a linker designed to attach the payload to the mAb. Internalization of the ADC by endocytosis followed by lysosomal processing releases the cytotoxin to initiate apoptosis of the tumor cell. Fully human or humanized IgG1 antibodies often are preferred in these constructs due to their potent ability to activate ADCC and ADCP through FcγRIIIa binding to NK cells.97 Removal of fucosyl groups (afucosylation) from the N-linked biantennary complex oligosaccharides in the antibody’s Fc region further improves binding to FcγIIIa receptors on NK cells, resulting in enhanced ADCC.98
B-cell maturation antigen (BCMA, CD269, TNFRSF17) is a tumor necrosis factor (TNF) family member that acts as a ligand for BAFF (B-cell activating factor) and APRIL (a proliferation-inducing ligand), two cytokines that play key roles in myeloma cell viability and proliferation.99 While inhibitors of BAFF and APRIL have fared poorly in MM trials,100,101 BCMA, which was first discovered nearly thirty years ago,102–105 has come to the fore in recent years as an attractive target in the search for new drugs to treat MM.106–109 As its name implies, expression of this 184-amino acid glycoprotein is a key factor in the normal maturation and differentiation of B-cells into fully functional plasmacytes. Both BCMA and its mRNA, whose presence is almost exclusively confined to plasma cells, are known to be consistently overexpressed during malignant transformation to MM, driving tumor cell growth, survival, and drug resistance as determined in both cell lines and patient samples. Furthermore, much evidence suggests that measurements of membrane bound BCMA may serve not only as a biomarker for MM diagnosis and prognosis, but also as a predictor of treatment response.110
Cleavage of the extracellular domain from membrane-bound BCMA by the action of gamma-secretase results in release of soluble BCMA (sBCMA) into the plasma;111 elevation of sBCMA blood levels in MM patients has been correlated with inferior clinical outcomes.112 Moreover, sBCMA not only lowers the density of the target antigen but also provides a soluble decoy having the capacity to reduce the efficacy of new anti-BCMA agents currently under investigation. In an effort to mitigate this potential hurdle, a number of gamma-secretase inhibitors have been developed to enhance effectiveness of BCMA-directed therapies.113,114 Crenigacestat (LY3039478, JSMD-194) and nirogacestat are among the orally active γ-secretase inhibitors that have been included in clinical trials of anti-BCMA immunotherapies.
Belantamab mafodotin (Blenrep®, belamaf, GSK2857916) is an ADC in which the BCMA-targeted humanized afucosylated IgG1 antibody is coupled to the microtubule inhibitor monomethyl auristatin F (mafodotin, MMAF) through a non-cleavable maleimidocaproyl linker.115,116 ADCC is induced by the antibody following its binding to the BCMA receptor on the myeloma cell surface while the cytotoxic component causes cell cycle arrest at the G2/M checkpoint.117 In August 2020, belantamab mafodotin became the first ADC to receive FDA approval for MM. The endorsement was provided on an accelerated basis for use in RRMM patients who had received at least four earlier regimens, including a proteasome inhibitor, an anti-CD38 mAb, and an immunomodulator.118 Approval was predicated on data from the DREAMM-2 trial (NCT03525678), which included a total of 196 RRMM patients, divided into two dosage cohorts: 2.5 mg/kg (N = 97) and 3.4 mg/kg (N = 99). ORR and PFS data recorded for the two groups was 31% and 2.9 months and 34% and 4.9 months, respectively.119 Table 4 lists a number of clinical trials that include belantamab mafodotin, which are currently active or in the initial planning stages. Thrombocytopenia and anemia were among the commonly reported adverse events noted with the drug in the DREAMM-2 trial, as well as in the earlier Phase I study. However, the toxic effect of greatest concern has been the corneal microcyst-like epithelial changes (MECs) that were observed with belantamab mafodotin as a single agent in 72% (68/95) of patients.120 Neither corticosteroid eye drops nor artificial tears appeared to mitigate this toxic reaction, whose mechanism is unknown. MECs also have been a commonly reported issue in studies of patients receiving other ADCs that employ MMAF as the cytotoxic component.121 For this reason, FDA approval was accompanied by a Boxed Warning requirement indicating that changes in the corneal epithelium may result in vision loss, blurred vision, corneal ulcers, and dry eyes. Consequently, the drug is available only under a restricted Risk Evaluation and Mitigation Strategy (REMS) program.
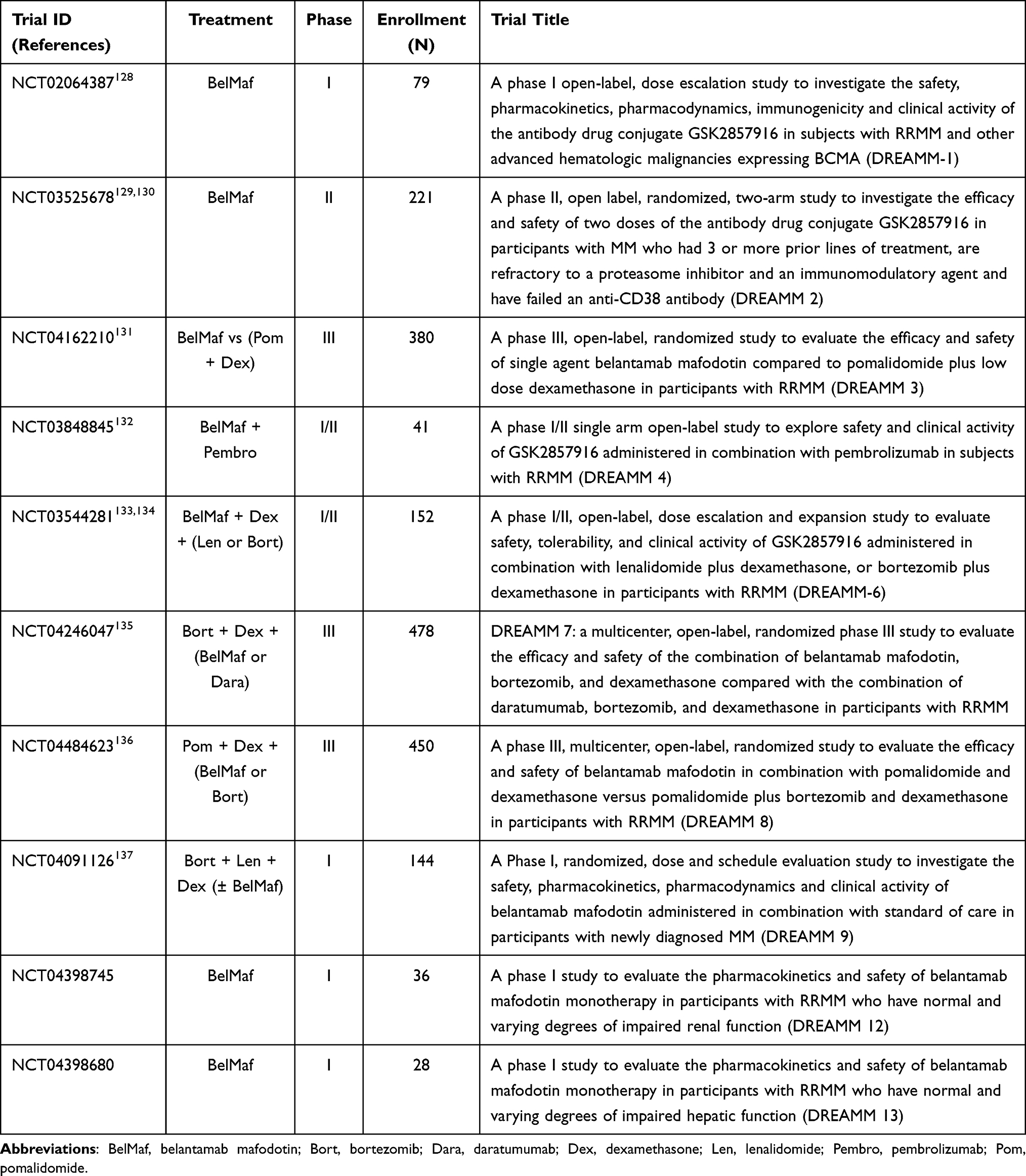 |
Table 4 Selected Trials of Belantamab Mafodotin in Multiple Myeloma (MM) |
Another BCMA-targeted ADC that has been in a phase I trial (NCT03489525) for RRMM is MEDI2228. Although this agent had shown some early promise in terms of efficacy and toxicity, it was recently announced that the drug has been dropped by its sponsor (AstraZeneca) from further consideration for MM. AMG 224, an IgG1 mAb, conjugated to the microtubule inhibitor mertansine via a maleimidocaproyl-derived non-cleavable linker, has shown some encouraging results in a phase I trial (NCT02561962) in which an ORR of 23% was reported in an initial study of 40 heavily pretreated RRMM patients.122
Amanitin, an extremely potent inhibitor of RNA polymerase II that is produced by the deadly Amanita phalloides (“death cap”) mushroom, has come to the fore recently as a cytotoxin exhibiting a novel mode of action among ADCs. One such ADC is HDP-101, comprised of an amanitin analog coupled to a BCMA-targeted antibody via a cathepsin B-cleavable linker.123–125 Based on the highly favorable results of a pre-clinical study,126 HDP-101 recently (May 2021) was advanced to a phase I safety-assessment trial (NCT04879043) in RRMM patients.127
T-Cell-Engaging Bi-Specific Antibodies
T-cell-based immunotherapies have assumed major importance as viable approaches to cancer treatment, especially during the past decade. The field has been dominated particularly by two areas of research: chimeric antigen receptor (CAR) T-cell therapies and T-cell-engaging bi-specific antibodies (T-BsAbs). The latter will be described in this section first while discussion of the former will be reserved for the following segment.
Based on a concept originally proposed sixty years ago by Nisonoff,138 T-BsAbs are predicated on the construction of a dual-targeting antibody whereby one arm first binds to the T-cell CD3 co-receptor while the other arm subsequently is recruited to a TAA or TSA on the targeted cancer cell. Although there are numerous variations on this concept, the basic strategy results in tethering of cytotoxic T-cells to tumor cells in order to cause cytolysis of the latter.139–141 The destructive effects are due to the combined actions of two cytolytic-initiating proteins released by cytotoxic T-cells: perforin, which generates transmembrane pores in the tumor cells and granzyme B, which navigates through the formed pores to initiate apoptotic death of the tumor cell.142,143 The bi-specific antibody approach affords certain advantages by obviating the need for antibody-presenting cells, co-stimulatory molecules, or interaction between an antigen and a major histocompatibility complex (MHC) molecule. In addition, the persistent T-cell activation enables polyclonal expansion of T memory cells. Furthermore, such constructs remove any requirement for ex vivo T-cell manipulation, thus making “off the shelf” products feasible. Modification of each arm’s relative binding affinity for its respective target permits fine-tuning of each construct’s therapeutically relevant properties to optimize activity and biopharmaceutic parameters.144–147
The first, and thus far only, successful application of the bi-specific antibody concept to cancer immunotherapy has been the result of a collaboration between Amgen and Micromet that developed the BiTE® (Bi-specific T-cell Engager) platform in which the crosslink between T-cell CD3 co-receptor and tumor cell lymphocyte antigen CD19, is provided by tandem single-chain variable fragments (scFvs). The resulting product, blinatumomab (Blincyto®), was granted accelerated FDA approval in 2014 for use in B-cell precursor acute lymphocytic leukemia (B-cell ALL).148,149 However, extension of the blinatumomab success to RRMM has not been as favorable in terms of employing CD19 as a bi-specific binding partner. This may be related to the observation that CD19 expression by B-cells is known to progressively decrease throughout their development from the pre-B-cell stage to differentiation into plasma cells and even further during transformation into myeloma cells.150,151 This increasing loss of CD19 has been proposed as a contributing factor in myeloma cell proliferation, which would appear to preclude realization of benefits of anti-CD19 therapy in MM. However, the recent finding of CD19 at very low levels on MM cells by super-resolution microscopy,152 although undetectable by conventional flow cytometry, may yet make CD19 an intriguing target for immunotherapy of MM. A single phase I RRMM-based trial (NCT03173430) of blinatumomab, combined with ASCT, unfortunately had to be terminated at an early stage because of “slow patient accrual”.
Although utilization of CD19 as a suitable binding partner for bi-specific antibodies in MM appears to be stymied at this point, BCMA, as in the ADC arena, has assumed a major role in BiTE® research.153–156 One such agent, AMG 420 (BI-836909) demonstrated favorable results in a phase I dose-escalation trial (NCT02514239), achieving a 31% ORR in 42 RRMM patients, including 70% (7/10) in those who received the maximum tolerated dose (400 mg/day). Infections and polyneuropathy were the most serious adverse events related to treatment. Cytokine release syndrome (CRS) (see below), primarily grade 1, was reported in 38% of patients in the study.157 Pavurutamab (AMG 701), another BiTE® product from Amgen, with an extended serum half-life compared to AMG 420, is the subject of a phase I study (NCT03287908), both as monotherapy and in combination with pomalidomide; inclusion of the latter was suggested by the results of an earlier preclinical study.158 Initial results from 75 heavily pretreated RRMM patients indicated that monotherapy with pavurutamab demonstrated encouraging activity and a manageable safety profile.159 A recent press release revealed that this study has been paused in order to “discuss protocol modifications to optimize safety monitoring and mitigation with the FDA”.160
Additional BCMAxCD3 bi-specific and related constructs that currently are in phase I trials for RRMM include the following:154,161
- REGN5458 (NCT03761108) and REGN5459 (NCT04083534), under development by a Regeneron/Sanofi partnership. Thus far, both preclinical and preliminary patient data have been reported only for the former.162,163
- Teclistamab (JNJ-64007957), which has been shown to be well tolerated in a monkey model164 and has demonstrated other favorable characteristics in vitro,165 has been included in a dose-escalation study (NCT03145181) in which an ORR of 78% (7/9) was reported for patients receiving the highest dose while exhibiting a manageable safety profile.166–168
- Elranatamab (PF-06863135; PF-3135), derived from hinge-mutation engineering of an IgG2a backbone,169 has been the subject of a safety and efficacy investigation (NCT03269136) for which preliminary results have been reported.170–173 The drug’s advancement to a phase II trial recently was announced.174
- CC-93269, a trivalent T-cell engager in which one arm binds to CD3ε while the other two arms attach bivalently to BCMA, exhibited promise in one cohort of heavily pretreated RRMM patients who attained an ORR of 83% (10/12) at the highest dose level (6 mg.) (NCT03486067).175
- TNB-383B, a collaborative effort between AbbVie and Tenebio, is comprised of a single light chain domain and two variable heavy chains in a BCMAxCD3 format. Its strong T-cell activation kinetics and low-affinity anti-CD3ε arm are said to be responsible for the reduced level of cytokine release without diminishing cytotoxicity associated with the product.176–178 An ORR of 52% (12/23) at well-tolerated doses recently was reported in a preliminary study (NCT03933735) of TNB-383B, which received FDA designation as an Orphan Drug in 2019.179,180
- HPN217, developed by Harpoon Therapeutics, is another example of a tri-specific engager. In this case, the molecule consists of three binding domains in a single chain: a BCMA-binding component at the N-terminus, a CD3ε T-cell receptor (TCR) binding domain at the C-terminus, and a central human serum albumin-binding portion. This product’s smaller size and flexibility are thought to account for its prolonged half-life.181 A recent report outlined the design of a phase I/II investigation of HPN217 in RRMM patients.182
Targeting TAA or TSA receptors on NK cells represents an alternative strategy for development of BCMA-targeted bi-specifics. As with cytotoxic T-cells, NK cells release granzyme and perforin while they also express certain apoptosis-inducing ligands.183,184 A tri-specific engager that binds BCMA and CD200 on myeloma cells and CD16A on NK cells is one such example.106,185 Another is RO7297089 (AFM26), a bi-specific designed to engage myeloma cell BCMA and NK CD16A, which exhibited an acceptable safety profile in preclinical work.186 An additional example is Compass Therapeutics’ bi-specific CTX-4419 in which the binding partners are myeloma cell BCMA and NK cell p30, demonstrating that although NK CD16A binding may enhance cytotoxicity, it may not be a requirement for anti-myeloma activity. Some promise has been shown in preclinical work on CTX-4419.187 Similar properties have been noted for CTX-8573, another Compass entry into the anti-myeloma multi-specific antibody arena.188
Myeloma surface antigens other than BCMA also have served as targets for bi-specific antibody development. A major candidate in this area is cevostamab (BFCR4350A; RO7187797), designed to bind T-cell CD3 with FcRH5,189 expressed on virtually all myeloma cells and now the subject of two clinical trials for RRMM (NCT04910568 and NCT03275103).190,191 Among the other non-BCMA directed constructs also under investigation are the CD3xCD38 mAb found in GBR 1342 (NCT03309111),192 a CD3xCD20 bi-specific,193,194 and talquetamab (JNJ-64407564), a bi-specific construct designed to link CD3 to G-protein-coupled receptor class C group 5 member D (GPRC5D), a TAA expressed at high levels in malignant plasma cells but limited to hair follicles and lung tissue in healthy individuals.168,195–197 An initial phase I evaluation (NCT03399799) of talquetamab monotherapy reported ORRs of 78% (14/18) when given iv and 67% (8/12) when used sc.196 Also under study are combinations of subcutaneous daratumumab (with or without pomalidomide) plus either talquetamab or the above-noted teclistamab (NCT04108195).
A list of selected clinical trials that include T-cell engaging bi-specific antibodies is shown in Table 5.
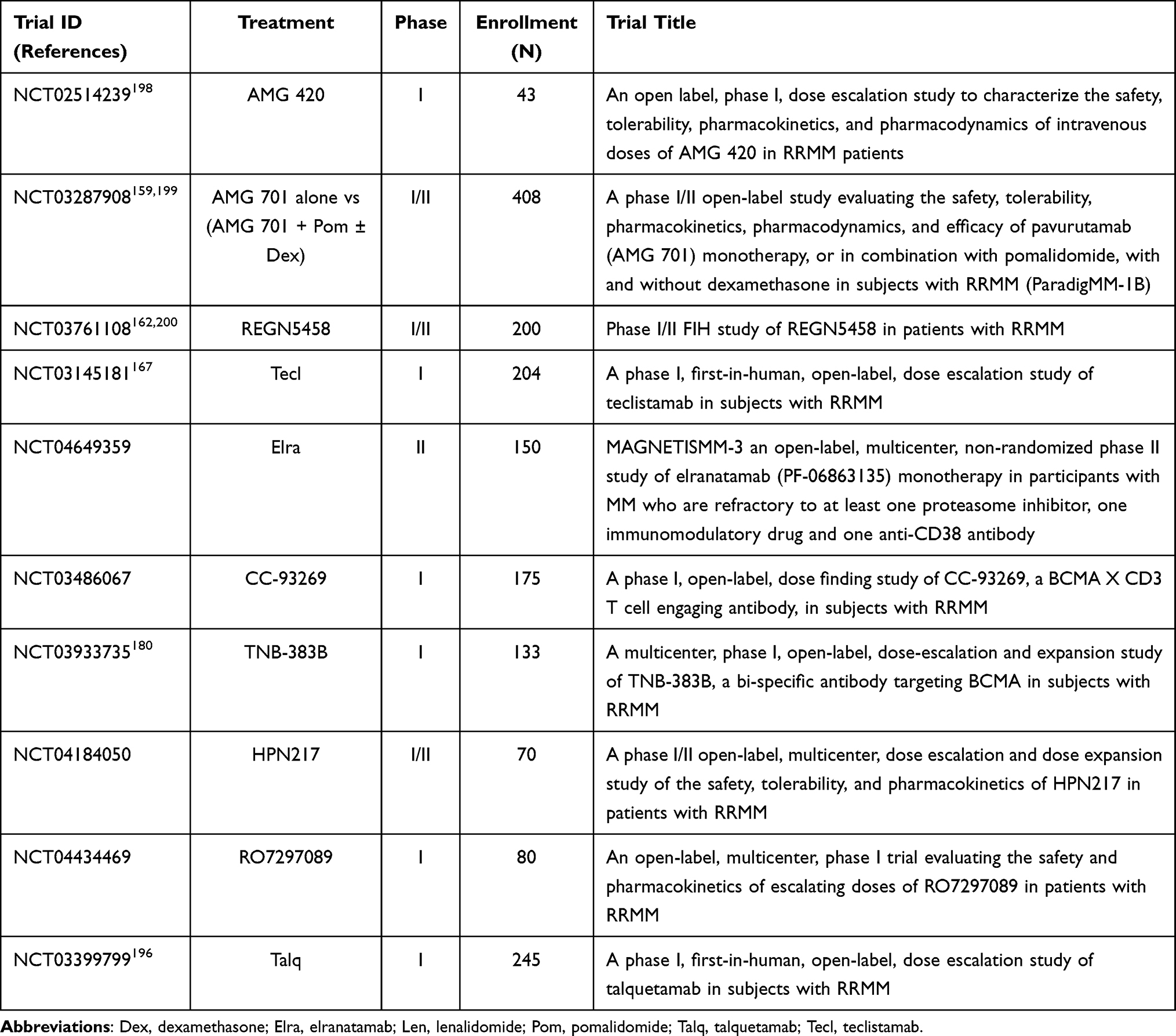 |
Table 5 Selected Trials of T-Cell Engaging Bi-Specific Antibodies in Multiple Myeloma (MM) |
Chimeric Antigen Receptor (CAR) T-Cells
Over the past decade, chimeric antigen receptor (CAR) T-cell therapy has risen to a place of prominence as a viable immunotherapeutic approach to cancer treatment.201,202 As a form of adoptive cell transfer (ACT), this strategy endeavors to genetically modify a patient’s own cytotoxic T-cells to enable them to attack and kill a specific type of malignant cell. By employing recombinant DNA technology a viral vector is constructed so as to enable eventual expression of a chimeric receptor designed to attach to a TAA or TSA found on the targeted cancer cell. Reinfusion of the engineered T-cells back into the patient results in T-cell engagement with the targeted malignant cells leading to their death. The technique has been most successfully applied to the treatment of hematological cancers, particularly B-cell malignancies, targeting CD19 although such has not been the case when applied to MM for reasons described earlier. For example, a trial of the anti-CD19 CAR tisagenlecleucel combined with ASCT only resulted in a poor clinical benefit in a cohort of ten MM subjects (NCT02135406).203
The attainment of durable remissions with anti-CD19 CAR T-cells initially proved difficult even though ORRs in excess of 80% were seen in some early studies.204–207 The solution to this conundrum eventually was revealed when the value of adding lymphodepletion to the pre-ACT regimen became clear. The benefits of lymphodepletion, usually consisting of combined cyclophosphamide and fludarabine, were demonstrated in several CAR T-cell-based trials by reports of enhanced T-cell persistence and expansion, as well as clinical outcomes.208 Although the mechanism underlying the improved efficacy associated with lymphodepletion remains obscure, several possibilities have been proposed, including elimination of homeostatic cytokine sinks for interleukins-2, -7, and -15,209 greater levels of monocyte chemoattract protein-1 (MCP-1),210 and downregulation of tumor cell indoleamine 2,3-dioxygenase (IDO)211 to block formation of tryptophan-derived metabolites known to inhibit T-cell activity and induce tolerance to tumor antigens.212 Parenthetically, it is noteworthy that linrodostat (BMS-986205),213 an oral irreversible inhibitor of IDO1, has been included in a CAR T-cell-based MM trial (NCT04855136) that was started in April 2021.
Just as seen above with bi- and multi-specific antibodies, BCMA has taken its place as the major TSA of interest in anti-myeloma CAR T-cell research.155,214 Several of the anti-BCMA constructs of consequence are described below, and Table 6 lists several of the currently active myeloma-based anti-BCMA CAR T-cell trials.
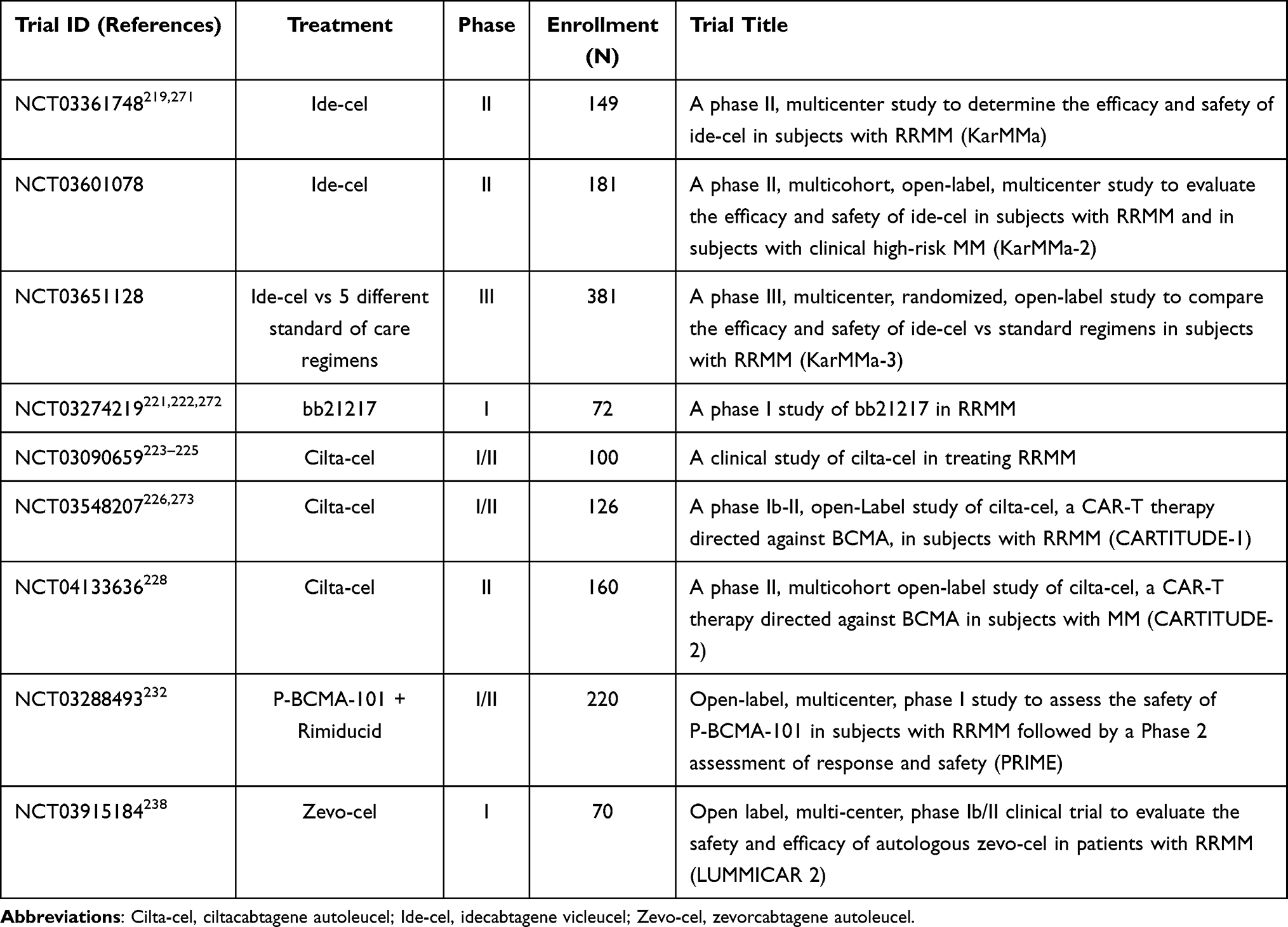 |
Table 6 Selected Trials of CAR T-Cells in Multiple Myeloma (MM) |
The first clinical trial (NCT02215967) of an anti-BCMA CAR T-cell construct utilized a lentivirus engineered paradigm in which the anti-BCMA scFv was linked in series to a CD8 hinge, a transmembrane region, a CD28 co-stimulatory domain, and CD3ζ as the T-cell activator.215 Data reported for 16 RRMM patients in the study (median of 9.5 lines of prior therapy) showed a median PFS of 31 weeks and an ORR of 81% at the highest dose used (9 × 106 T-cells per kg).216 This encouraging result led to a phased series of KarMAa trials of Bluebirdbio’s idecabtagene vicleucel (Abecma®; bb2121; ide-cel), whose structure included an anti-BCMA scFv linked to CD137 (4–1BB) co-stimulatory and CD3ζ signaling domains.217 The product was approved by the FDA in March 2021 for RRMM218 based on the results of a pivotal phase II trial (NCT03361748; KarMAa-1) that incorporated 128 RRMM patients who had failed at least three previous regimens, including a proteasome inhibitor, an immunomodulator, and an anti-CD38 mAb. An ORR of 73% (94/128) was attained and one-third (42/128) experienced complete responses or better. The median PFS was 13.3 months. CRS was the most common non-hematologic adverse effect, being found in 84% of treated subjects with 5% experiencing grade 3 or 4. Neurotoxicity developed in 23 (18%) patients – four in grade 3 and none in grade 4.219 Bluebirdbio’s next generation entry into the field, bb21217, employs the same lentiviral design as its predecessor with the addition during ex vivo culture of an extra phosphoinositide-3-kinase (PI3K) inhibitor domain (bb007). This modification significantly enhances CAR T-cell-based immunotherapy by enriching the product’s population of memory-like T-cells to enhance T-cell durability and potency.220 The drug was the subject of two recent reports of an ongoing dose-escalation study (NCT03274219) of 44 RRMM patients. Confirmed responses were noted in 24 (55%) patients with CRS and neurotoxicity observed in 67% and 10%, respectively. Preliminary data indicated a positive correlation between the presence of memory-associated T-cell markers and peak expansion and duration of response, providing some tentative support for the mechanistic hypothesis underlying the product’s design.221,222
Johnson and Johnson’s contribution to this arena is ciltacabtagene autoleucel (JNJ-68284528; JNJ-4528; LCAR-B38M; cilta-cel), which differs from other BCMA-targeted T-cell therapies by being directed against two BCMA epitopes (VH1 and VH2), a feature which improves affinity for BCMA-expressing cells. The phase I LEGEND-2 study (NCT03090659) of this product was conducted on 57 patients who showed an ORR of 88% and PFS of 15 months. There was evidence of CRS, primarily grades 1 or 2 in 83% of trial subjects.223–225 Reported results from 97 RRMM patients (median of 6 prior lines of therapy) in the CARTITUDE-1 phase Ib/II trial (NCT03548207) were similar (97% ORR, CRS 95%) to those seen in the LEGEND-2 study.226 As a result of data from the LEGEND-2 and CARTITUDE-1 studies, in 2019 this drug was accorded PRIME status by the European Medicines Agency (EMA) and was designated a Breakthrough Therapy and subsequently granted priority review by the FDA.227 Two additional studies of the efficacy of ciltacabtagene autoleucel in RRMM currently are in progress: CARTITUDE-2 (NCT04133636) and CARTITUDE-4 (NCT04181827). Recently reported data from the former trial (phase II) indicated deep and early responses with a single infusion.228 The latter is a phase III comparison with two standard myeloma triplet therapies; no results have been reported as yet from this trial.
P-BCMA-101, a fully humanized anti-BCMA CAR T-cell product from Poseida Therapeutics, contains a CD3ζ/4-1BB signaling domain fused to a non-immunoglobulin Centyrin® scaffold. Such constructs generally are smaller than those patterned after immunoglobulins and offer advantages of higher binding affinities, improved stability, reduced immunogenicity, and lower production costs. Instead of using a viral vector in the manufacturing process, P-BCMA-101 employs proprietary transposon-based technology (piggy-BAC®).229 The process has been shown in preclinical work to yield a preponderance of T stem cell memory cells (Tscm), offering the potential for improved therapeutic longevity.230 The product also is noteworthy for the inclusion in its design of a truncated caspase 9 domain as a safety switch. Rimiducid, a caspase 9 dimerizing agent, can be administered to initiate apoptosis if patient safety is threatened.231 P-BCMA-101 has been the subject of a phase I trial (NCT03288493; PRIME) in heavily pretreated RRMM patients. An ORR of 57% after a single administration recently was reported for a cohort of 34 evaluated subjects in the study. CRS, one in grade 3, was observed in 17% of the patients. A possible case of neurotoxicity also was reported.232 A long-term (15 years) follow-up study (NCT03741127) has been initiated to explore in-depth issues of this product’s efficacy and toxicity.
Orvacabtagene autoleucel (orva-cel; JCARH125) and FCARH143 are two similar fully human svFv bicistronic CARs that incorporate a 4–1BB co-stimulatory domain and use a lentiviral vector although they differ in the method of production.233,234 Initial results of a trial (NCT03430011) of orva-cel in 51 RRMM patients reported an ORR of 91% while exhibiting a manageable safety profile.234,235
Zevorcabtagene autoleucel (zevo-cel; CT053) and CT103A are two BCMA-targeted CAR T-cell products under development by CARSgen Therapeutics. Both are fully human scFv constructs, containing a CD8α hinge, 4–1BB co-stimulatory and CD3ζ activation domains, in addition to a transmembrane component. In 2019, the FDA granted CT053 the Regenerative Medicine Advanced Therapy (RMAT) designation, based on the initial results of two trials (NCT03975907, LUMMICAR-1; and NCT03915184, LUMMICAR-2) in RRMM patients who previously had been treated with a median of four prior regimens.236,237 Updated results on 10 evaluable patients in the LUMMICAR-2 trial were presented recently and showed an ORR of 100% at a dose of 1.5–3.0×108 CAR T-cells.238 Notable early results also have been reported for the related construct CT103A, which recently has been under study in the RRMM setting in China (ChiCTR1800018137): ORR of 100% in the first 18 patients in this phase I trial.239,240 Numerous other strategic approaches to BCMA-based autologous CAR T-cell product development are represented in the array of currently active clinical trials extant in the NCI data base for MM. Included among these products are CART-ddBCMA,241 C-CAR088,242 and FHVH-BCMA-T.243,244
Both CD19- and BCMA-targeted CAR T-cells have been used in combination in some trials in order to enhance efficacy, improve patient safety, and deepen clinical response. Simultaneous targeting of BCMA and SLAMF7 also is being studied.245 The dual-targeting strategy may involve co-infusion of two different pools of T-cells each expressing a different CAR or a single T-cell pool in which each T-cell expresses two different CARs (arranged either bicistronic or in tandem).246–249 For example, dual targeting has been explored in trials in newly diagnosed high-risk MM (NCT03455972) and in RRMM patients (NCT03196414). A recent review detailed the various combinations of dual-targeting strategies.250 However, meaningful patient data from trials of these dual-targeted combinations in MM have thus far been very limited.249,251–253 Future work needs to focus on the relevance of the various combinatorial approaches to the different stages of MM from newly diagnosed patients to those who fail established regimens.
Finally, preclinical data have informed trials of CAR T-cells that are directed against TSAs or TAAs other than BCMA. These targets include SLAMF7 (NCT03958656; NCT03710421),254,255 CD38 (NCT03464916),256 and CD138.257 However, only limited patient data are available on these studies. Alternatives to T-cells also have been explored in efforts to expand available options to treat RRMM. The primary contemporary candidates here are anti-BCMA-engineered NK cells;256,258–260 although SLAMF7 and CD138 also have been considered as NK cell targets in the past.261,262 Nevertheless, only a single trial (NCT03940833), involving a product from Asclepius Technology in China, is now in progress to explore the potential role of BCMA-directed NK-engineered CARs in RRMM.
Although the autologously administered CAR T-cells described above have thus far produced highly promising results, their use is not without drawbacks, such as the short-lived responses they elicit and the high risk of CRS and other dose-limiting adverse events. As a result, some CAR T-cell originators have initiated innovative programs to develop “off-the shelf” allogeneic anti-BCMA products that use T-cells from healthy donors. The pipeline of agents in this category currently is headed by two major players: ALLO-715 from Allogene Therapeutics and Precision Bioscience’s PCAR269A.
ALLO-715 is manufactured using the proprietary Transcription Activator-like Effector Nuclease (TALEN®) system, a site-specific BCMA gene-editing technique that is hypothesized to limit the product’s potential T-cell receptor-mediated immune responses, such as graft versus host disease (GvHD) and rapid rejection.263,264 Recently (April 2021), ALLO-715 received the FDA’s RMAT designation,265 which was based on the initial findings of the dose-escalation phase I UNIVERSAL trial (NCT04093596) of 15 heavily pre-treated RRMM patients in whom were reported an acceptable safety profile and an ORR of 33% at the dose levels tested.266 Significantly, ALLO-715 is the first anti-BCMA CAR T-cell product whose design strategy incorporates a CD20-based mimotope capable of activation by rituximab. Moreover, the UNIVERSAL trial also is noteworthy for its use of an anti-CD52 antibody, ALLO-647, as a selective lymphodepletion agent.267
PBCAR269A was developed using Arcus Bioscience’s patented nuclease gene-editing platform, which is based on the homing endonuclease I-CreI scaffold.268,269 In 2020, this product received Fast-Track status from the FDA270 and was advanced to a phase I trial for RRMM (NCT04171843).
Cytokine Release Syndrome (CRS) and Neurotoxicity
Issues related to toxicity constitute important challenges that effect immunotherapy of hematologic cancers, including the bi- and multi-specific engaging antibodies and CAR T-cell platforms described in this review. These potentially lethal toxicities, whose inability to be easily reversed may require multidisciplinary management and intensive care, often are divided into two different types: 1) a general toxicity caused by T-cell recognition and activation against the targeted malignant cells and subsequent uncontrolled cytokine release at high levels (on-target, on-tumor toxicity) and 2) toxicity caused by cytokine release when CAR T-cells bind to the target antigen located on normal cells (on-target, off-tumor toxicity). BCMA-targeted anti-myeloma products carry a low-risk of on-target, off-tumor type reactions given the virtually exclusive confinement of the antigen to plasma cells. The discussion that follows is devoted to the on-target, on-tumor types of adverse events.
The most important adverse effects that accompany on-target, on-tumor toxicity are the cytokine release syndrome (cytokine storm; CRS) and neurotoxicity. Two terms often are used in the literature to describe the neurotoxic reactions: CAR T-cell-related encephalopathy syndrome (CRES) and immune effector cell–associated neurotoxicity syndrome (ICANS). Almost without exception, CRS and neurotoxicity are seen in varying degrees of severity in a percentage of participants in every trial of the immunotherapeutic agents described in this paper.274,275 For instance, in the CAR T-cell therapy setting meta-analysis of 15 trials (N=977) of anti-CD19 or anti-BCMA constructs, 62.3% (range: 11% to 100%) experienced some degree of CRS with 18.4% (range 0.8% to 46%) in grades 3 or 4.276 Also, attempts to assess relative safety risks between different immunotherapeutic modalities may present complex problems. For example, meta-analysis of 8 clinical trials of anti-CD19 blinatumomab in relapsed/refractory ALL and NHL patients (N=729) found that the pooled occurrence rate of CRS of grades 3 or 4 was 3.5% and that of neurotoxicity was 12%.277 These data compare with the 19% and 18% respective rates of grades 3 or higher found in a recent meta-analysis of 15 trials (N=448) of RR B-cell ALL patients who received C-19-specific CAR T-cell therapy.278 Although tending to indicate that CRS and neurotoxicity may occur with greater frequency and severity in patients receiving CAR T-cell therapy as opposed to bi-specific antibody therapy, at least in terms of treatments targeting CD16, a number of factors, including type of malignancy under study, structure and target of the immunotherapeutic product involved, the grading scales used, and routes and timing of administration, as well as other variables may account for observed differences.
The symptoms of CRS, which generally occur in the first two weeks of therapy and resemble those of a severe inflammatory reaction, are attributed to marked increased expression and release of certain cytokines, including IL-6, IL-2R, IL-10, IFN-γ, and TNF-α.279,280 Furthermore, CRS has been effectively implicated as a major contributor to the deadly effects associated with COVID-19 infections during the current global pandemic.281–284 The IL-6 blocker tocilizumab (Actemra®) is the treatment of choice for cases of CRS associated with CAR T-cell therapy, FDA approval for this indication having been granted in 2017.285 However, optimal timing of tocilizumab intervention in patients at-risk for CRS remains an open question.286,287 In addition, the agent usually is administered with corticosteroid infusions although the efficacy of combining corticosteroids with tocilizumab in the management of CRS has not been tested through randomized controlled studies.
ICANS/CRES symptoms, which typically begin around 4–5 days after initiation of CART-cell therapy and usually follow the peak of CRS severity, are related to impairment of blood–brain barrier (BBB) integrity enabling CSF cytokine and lymphocyte infiltration. Tocilizumab is not effective in the management of neurotoxicity. Rather, glucocorticoids play the major role in its treatment although their efficacy remains undocumented.288–290
In efforts to gain better control over toxicity of CAR T-cell therapy some formats have been designed to incorporate a safety switch to enable activity curtailment through administration of a pharmacologic antagonist.291 Inclusion in the construct of a transduced CD20 receptor that can be switched “off” by administration of the CD20 blocker rituximab is one illustration of this strategy.292 Another is the incorporation of a non-functional truncated epidermal growth factor receptor (tEGFR) that can be antagonized by cetuximab.293,294 Dimerization of caspase-9 to activate apoptosis by use of the dimerizing agent rimiducid represents yet another example.295–297 The strengths and weaknesses of the various molecular safety switches employed in CAR T-cell design have been described in a recent comprehensive review of the subject.298
Checkpoint Inhibitors
Over the course of the past decade, immune checkpoint blockade has become a major strategy for immunotherapeutic drug development in the anticancer field. The approach is predicated on the interaction of specific cell surface biomarkers and their cognate ligands that enable the immune system to overcome the ability of malignant cells to evade immune surveillance and elimination. This tactic has resulted in the introduction of several antitumor mAbs designed to block these biomarker/ligand interactions. In particular, two of these biomarkers cytotoxic T-lymphocyte–associated protein-4 (CTLA-4) and the programmed death (PD) receptor thus far have been successfully applied as targets in this innovative line of attack on a variety of cancers.13 However, their utility as targets in MM has yet to be conclusively demonstrated.299 Two myeloma-based trials (NCT01592370 and NCT02681302) of the anti-CTLA-4 mAb ipilimumab combined with another checkpoint inhibitor, nivolumab, are currently ongoing. An initial report in the latter trial concluded that the combined checkpoint inhibitor therapy is safe and has potential to increase the “depth of response in patients with high-risk disease”.300 Encouraging results were seen in early phase studies of PD-1 blocker pembrolizumab in MM, especially when used together with immunomodulators.301 However, major safety issues arose concerning these pairings in phase III trials, resulting in suspension of these studies although it is noteworthy that additional combinations of pembrolizumab and other PD-1/PD-L1 blockers continue to be studied in MM as shown in Table 7. In addition to those studies shown in the table is a myeloma-based trial (NCT03111992; N=26) in which the PD-1 blocker spartalizumab was combined with an anti-IL17A mAb (CJM112) and a SMAC (second mitochondrial-derived activator of caspases) mimetic (LCL161); no results have yet appeared for this recently completed study.
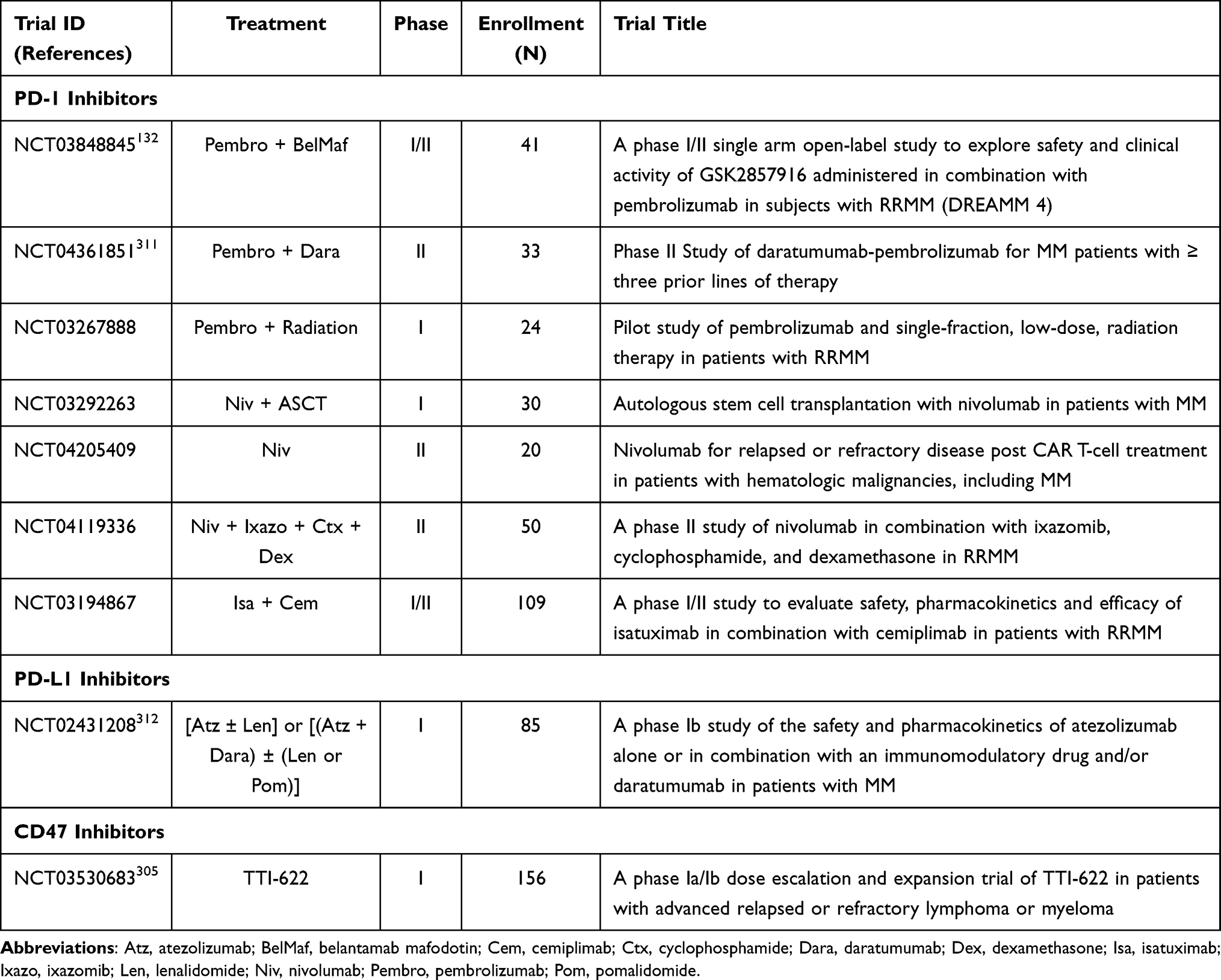 |
Table 7 Selected Trials of Checkpoint Inhibitors in Multiple Myeloma (MM) |
In addition to CTLA-4 and PD-1/PD-L1, other checkpoints have been proposed as potential targets for immunotherapy in general or MM specifically although only limited preclinical or clinical data are available at present.302 These include killer-cell immunoglobulin-like receptors (KIR),259,303 CD47,304,305 LAG3,306 TIGIT,307–309 and TIM-3.310 In this connection, note should be made of an ongoing phase I/II trial (NCT04150965; N=104) in which RRMM patients receiving the anti-LAG3 relatlimab (BMS-986016) or anti-TIGIT BMS-986207 are compared to a control arm receiving a standard care regimen of elotuzumab-pomalidomide-dexamethasone.
Summary and Conclusions
The therapeutic landscape of MM has shifted dramatically in the past two decades as the number of treatment options has expanded enormously and five-year survival rates, progression-free survival data, and quality of life studies continue to evidence major advances.313 The disease itself has become redefined over the years, moving away from the traditional CRAB symptoms to a risk stratification approach that aims to identify factors that can be determinant before signs and symptoms of the disease emerge, such as the progression from asymptomatic MGUS to SMM to MM. These criteria, encompassing bone marrow evaluation, immunoglobulin and free light chain analyses, cytogenetic studies, and imaging technologies, have become pillars of contemporary diagnostic evaluation, prognostication of disease course, and determination of intervention strategies.7 This optimism has been invigorated further in recent years by the advent of immunologic-based approaches to cancer treatment in general and MM in particular. Once considered an idealistic fantasy, cancer immunotherapy has now emerged as a validated fixture in medicine, grounded in decades of work aimed at deciphering the fundamental complex relationships between the immune system and cancer initiation, proliferation, and metastasis. This bright picture is tempered, however, by the knowledge that MM is still considered incurable regardless of the treatment measures used. The vast majority of patients who experience initial therapeutic benefits eventually become refractory to treatment modalities and experience relapse. Thus, although much progress has been made to date, the obstacles that remain must be overcome if MM is ever to be considered curable.
Fundamental to MM immunotherapy is the challenge to identify potential cancer-driving biomarkers that can serve as targets for therapy. At the forefront of this search are CD38, SLAMF7, and BCMA, which serve as the basis for the immunotherapies in use today. CAR T-cell-based therapies targeting BCMA have demonstrated remarkable clinical efficacy in MM with ORRs of at least 80% recorded in several clinical studies; however, response durations are short. It is now recognized that BCMA expression by myeloma cells is not as homogeneous as once thought. For example, one study found that a substantial proportion (33/85) of MM patients was BCMA-negative.215 Moreover, downregulated tumor-cell BCMA expression (antigen escape) has been reported during CAR T-cell therapy, as well as instances in which a significant fraction of initially responding patients experienced relapse despite continuing to express BCMA.216,246,314–317 Furthermore, a genome-wide gene-editing CRISPR study failed to identify BCMA as being among 90 different genes essential for MM.318 Thus, combinatorial strategies using BCMA and other established targets, such as CD19, CD38, and SLAMF7 or emerging viable targets, for instance GPRC5D319 and FcRH5,190 may be of value in overcoming this issue.250 The orphan receptor GPRC5D has special appeal as a target in immunotherapy constructs since its expression is associated with poor prognosis in MM.320 Moreover, as a seven-pass transmembrane protein it, unlike BCMA, does not shed into the serum. In addition, expression of GPRC5D is independent of BCMA, offering the possibility of a suitable alternative target in instances of anti-BCMA therapy relapse. The encouraging results, noted earlier, from myeloma-based studies of the CD3xGPRC5D bi-specific talquetamab should inform future clinical exploration of the potential of GPRC5D-targeted CARs. Indeed, this prospect was bolstered by the finding that anti-GPRC5D CAR T-cells produced long-term survival, accompanied by disease eradication, in a myeloma mouse model resistant to BCMA-targeted therapy.319
As CAR T-cell and T-BsAb-based immunotherapies become more widespread in the future, the role of ASCT in MM patients who are considered transplant-ineligible, generally defined as elderly (over 75 years) and/or exhibiting frailty and possible comorbidities, will need to be more clearly defined. Current treatment protocols tend to favor the combination of daratumumab, lenalidomide, and dexamethasone for newly diagnosed and RRMM patients who are ASCT ineligible.24 However, much more work lies ahead, including the need to conduct head-to-head comparison trials, in order to adequately serve this patient population.321
Going forward, much better insight into the mechanisms that drive resistance to MM therapy needs to be gained. A key to deepening our knowledge in this area is the bone marrow microenvironment and the role it plays in enabling malignant cells to escape immune detection. Better understanding of the mechanisms at play here will contribute to future advances that will translate into further improving immunotherapeutic outcomes for MM, including the ability to reverse bone loss.322 In addition to PFS, OS, ORR, and other measures, the ability to detect minimal residual disease (MRD) is now emerging as a key element in directing anti-myeloma therapy. Achievement of MRD negativity is increasingly viewed as a reliable prognostication marker of PFS and potential relapse.323 As technological advances enable malignant cell detection at extremely low levels, MRD measurements need to be more consistently and uniformly employed in clinical trials in order to drive therapeutic decision-making in the future.
The upsurge in knowledge gained about MM and its treatment over the past twenty years has been most impressive. The deeper understanding of the mechanisms that underlie the disease and the identification of an array of druggable biomarkers have been translated into more efficacious treatments that enable positive outcomes with greater frequency, elevating the disease to its current status as a reasonably manageable chronic condition, at least in the short-term. However, the road to a true cure for MM remains fraught with challenges which, although not insurmountable, will need to be overcome for that dream to become a future reality.
Acknowledgment
The author would like to express his gratitude to Professor George B. Corcoran, III, Chair of the Wayne State University Department of Pharmaceutical Sciences, for his 25 years of steadfast service to the Department. This manuscript is dedicated to him in honor of his unceasing support and encouragement to the author and unparalleled leadership within the University.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Ailawadhi S, Parikh K, Abouzaid S, et al. Racial disparities in treatment patterns and outcomes among patients with multiple myeloma: a SEER-Medicare analysis. Blood Advances. 2019;3(20):2986–2994. doi:10.1182/bloodadvances.2019000308
3. Waxman AJ, Mink PJ, Devesa SS, et al. Racial disparities in incidence and outcome in multiple myeloma: a population-based study. Blood. 2010;116(25):5501–5506. doi:10.1182/blood-2010-07-298760
4. Kyle RA, Therneau TM, Rajkumar SV, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med. 2002;346(8):564–569. doi:10.1056/NEJMoa01133202
5. Yavorkovsky LL. Smoldering multiple myeloma 40 years later: a story of unintended disease. Expert Rev Hematol. 2021;14(2):149–153. doi:10.1080/17474086.2021.1875815
6. Kyle RA, Remstein ED, Therneau TM, et al. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med. 2007;356(25):2582–2590. doi:10.1056/NEJMoa070389
7. Kumar SK, Callander NS, Adekola K, et al. Multiple Myeloma, Version 3.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;18(12):1685–1717. doi:10.6004/jnccn.2020.0057
8. Chan HS, Chen CI, Reece DE. Current review on high-risk multiple myeloma. Curr Hematol Malig Rep. 2017;12:96–108. doi:10.1007/s11899-017-0368-z
9. Poczta A, Rogalska A, Marczak A. Treatment of multiple myeloma and the role of melphalan in the era of modern therapies-current research and clinical approaches. J Clin Med. 2021;10(9):1841. doi:10.3390/jcm10091841
10. Myeloma - Cancer stat facts; 2021. Available from: https://seer.cancer.gov/statfacts/html/mulmy.html.
11. Nandakumar B, Binder M, Dispenzieri A, et al. Continued improvement in survival in multiple myeloma (MM) including high-risk patients. J Clin Oncol. 2019;37(Supplement 15):8039. doi:10.1200/JCO.2019.37.15_suppl.8039
12. Braunstein M, Weltz J, Davies F. A new decade: novel immunotherapies on the horizon for relapsed/refractory multiple myeloma. Expert Rev Hematol. 2021;14(4):377–389. doi:10.1080/17474086.2021.1909469
13. Esfahani K, Roudaia L, Buhlaiga N, et al. A review of cancer immunotherapy: from the past, to the present, to the future. Curr Oncol. 2020;27(Suppl 2):S87–s97. doi:10.3747/co.27.5223
14. Waldman AD, Fritz JM, Lenardo MJ. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat Rev Immunol. 2020;20(11):651–668. doi:10.1038/s41577-020-0306-5
15. Tan S, Li D, Zhu X. Cancer immunotherapy: pros, cons and beyond. Biomed Pharmacother. 2020;124:109821. doi:10.1016/j.biopha.2020.109821
16. Jiao Y, Yi M, Xu L, et al. CD38: targeted therapy in multiple myeloma and therapeutic potential for solid cancers. Expert Opin Investig Drugs. 2020;29(11):1295–1308. doi:10.1080/13543784.2020.181425
17. Deaglio S, Morra M, Mallone R, et al. Human CD38 (ADP-ribosyl cyclase) is a counter-receptor of CD31, an Ig superfamily member. J Immunol. 1998;160(1):395–402.
18. Aarhus R, Graeff RM, Dickey DM, et al. ADP-ribosyl cyclase and CD38 catalyze the synthesis of a calcium-mobilizing metabolite from NADP. J Biol Chem. 1995;270(51):30327–30333. doi:10.1074/jbc.270.51.30327
19. Laubach JP, Richardson PG. CD38-targeted immunochemotherapy in refractory multiple myeloma: a new horizon. Clin Cancer Res. 2015;21(12):2660–2662. doi:10.1158/1078-0432.ccr-14-3190
20. van de Donk N. Immunomodulatory effects of CD38-targeting antibodies. Immunol Lett. 2018;199:16–22. doi:10.1016/j.imlet.2018.04.005
21. Palumbo A, Chanan-Khan A, Weisel K, et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(8):754–766. doi:10.1056/NEJMoa1606038
22. Dimopoulos MA, Oriol A, Nahi H, et al. Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(14):1319–1331. doi:10.1056/NEJMoa1607751
23. Moreau P, Attal M, Hulin C, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, Phase 3 study. Lancet. 2019;394:29–38. doi:10.1016/s0140-6736(19)31240-1
24. Durie BGM, Kumar SK, Usmani SZ, et al. Daratumumab-lenalidomide-dexamethasone vs standard-of-care regimens: efficacy in transplant-ineligible untreated myeloma. Am J Hematol. 2020;95(12):1486–1494. doi:10.1002/ajh.25963
25. Chari A, Suvannasankha A, Fay JW, et al. Daratumumab plus pomalidomide and dexamethasone in relapsed and/or refractory multiple myeloma. Blood. 2017;130(8):974–981. doi:10.1182/blood-2017-05-785246
26. Dimopoulos M, Quach H, Mateos MV, et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): results from a randomised, multicentre, open-label, phase 3 study. Lancet. 2020;396(10245):186–197. doi:10.1016/s0140-6736(20)30734-0
27. Janssen Pharmaceutical Co. U.S. FDA approves new DARZALEX® (daratumumab)-based combination regimen for patients with relapsed/refractory multiple myeloma [press release]. Horsham, PA; 2020. Available from:https://www.prnewswire.com/news-releases/us-fda-approves-new-darzalex-daratumumab-based-combination-regimen-for-patients-with-relapsedrefractory-multiple-myeloma-301116063.html.
28. Musto P, La Rocca F. Monoclonal antibodies in relapsed/refractory myeloma: updated evidence from clinical trials, real life studies and meta-analyses. Expert Rev Hematol. 2020;13(4):331–349. doi:10.1080/17474086.2020.1740084
29. Sanchez L, Richter J, Cho HJ, et al. Subcutaneous daratumumab and hyaluronidase-fihj in newly diagnosed or relapsed/refractory multiple myeloma. Ther Adv Hematol. 2021;12:2040620720987075. doi:10.1177/2040620720987075
30. Usmani SZ, Nahi H, Mateos MV, et al. Subcutaneous delivery of daratumumab in relapsed or refractory multiple myeloma. Blood. 2019;134(8):668–677. doi:10.1182/blood.2019000667
31. U.S. Food and Drug Administration. FDA approves daratumumab and hyaluronidase-fihj for multiple myeloma [press release]. Washington, DC; 2020. Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-daratumumab-and-hyaluronidase-fihj-multiple-myeloma.
32. Nooka AK, Gleason C, Sargeant MO, et al. Managing infusion reactions to new monoclonal antibodies in multiple myeloma: daratumumab and elotuzumab. J Oncol Pract. 2018;14(7):414–422. doi:10.1200/jop.18.00143
33. Chapuy CI, Nicholson RT, Aguad MD, et al. Resolving the daratumumab interference with blood compatibility testing. Transfusion. 2015;55(6 Pt 2):1545–1554. doi:10.1111/trf.13069
34. Boyle EM, Petillon MO, Herbaux C, et al. Daratumumab in combination with dexamethasone in resistant or refractory multiple myeloma: primary results of the IFM2014-04 trial. Blood. 2016;128(22):2138. doi:10.1182/blood.V128.22.2138.2138
35. Roussel M, Moreau P, Hebraud B, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab for transplantation-eligible patients with newly diagnosed multiple myeloma (CASSIOPEIA): health-related quality of life outcomes of a randomised, open-label, phase 3 trial. Lancet Haematol. 2020;7(12):e874–e883. doi:10.1016/s2352-3026(20)30356-2
36. Chari A, Munder M, Weisel K, et al. Evaluation of cardiac repolarization in the randomized phase 2 study of intermediate- or high-risk smoldering multiple myeloma patients treated with daratumumab monotherapy. Adv Ther. 2021;38(2):1328–1341. doi:10.1007/s12325-020-01601-w
37. Leleu X, Beksac M, Chou T, et al. Efficacy and safety of weekly carfilzomib (70 mg/m(2)), dexamethasone, and daratumumab (KdD70) is comparable to twice-weekly KdD56 while being a more convenient dosing option: a cross-study comparison of the CANDOR and EQUULEUS studies. Leuk Lymphoma. 2021;62(2):358–367. doi:10.1080/10428194.2020.1832672
38. Usmani SZ, Quach H, Mateos MV, et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for the treatment of patients with relapsed or refractory multiple myeloma (RRMM): primary analysis results from the randomized, open-label, phase 3 study CANDOR (NCT03158688). Blood. 2019;134:LBA–6. doi:10.1182/blood-2019-132629
39. Weisel K, Spencer A, Lentzsch S, et al. Daratumumab, bortezomib, and dexamethasone in relapsed or refractory multiple myeloma: subgroup analysis of CASTOR based on cytogenetic risk. J Hematol Oncol. 2020;13(1):115. doi:10.1186/s13045-020-00948-5
40. Rajkumar SV, Voorhees PM, Goldschmidt H, et al. Randomized, open-label, phase 3 study of subcutaneous daratumumab (DARA SC) versus active monitoring in patients (pts) with high-risk smoldering multiple myeloma (SMM): AQUILA. J Clin Oncol. 2018;36(15):2. doi:10.1200/JCO.2018.36.15_suppl.TPS8062
41. Dimopoulos MA, San-Miguel J, Belch A, et al. Daratumumab plus lenalidomide and dexamethasone versus lenalidomide and dexamethasone in relapsed or refractory multiple myeloma: updated analysis of POLLUX. Haematologica. 2018. doi:10.3324/haematol.2018.194282
42. Plesner T, Dimopoulos MA, Oriol A, et al. Health-related quality of life in patients with relapsed or refractory multiple myeloma: treatment with daratumumab, lenalidomide, and dexamethasone in the phase 3 POLLUX trial. Br J Haematol. 2021;194:132–139. doi:10.1111/bjh.17435
43. Sonneveld P, Terpos E, Dimopoulos MA, et al. Pomalidomide and dexamethasone (pom-dex) with or without daratumumab (DARA) in patients (pts) with relapsed or refractory multiple myeloma (RRMM): a multicenter, randomized, phase 3 study (APOLLO). J Clin Oncol. 2018;36(15):1. doi:10.1200/JCO.2018.36.15_suppl.TPS8059
44. Perrot A, Facon T, Plesner T, et al. Health-related quality of life in transplant-ineligible patients with newly diagnosed multiple myeloma: findings from the phase III MAIA trial. J Clin Oncol. 2021;39(3):227–237. doi:10.1200/jco.20.01370
45. Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N Engl J Med. 2019;380(22):2104–2115. doi:10.1056/NEJMoa1817249
46. Usmani SZ, Mateos MV, Hungria V, et al. Greater treatment satisfaction in patients receiving daratumumab subcutaneous vs. intravenous for relapsed or refractory multiple myeloma: COLUMBA clinical trial results. J Cancer Res Clin Oncol. 2021;147:619–631. doi:10.1007/s00432-020-03365-w
47. Iida S, Ishikawa T, Min CK, et al. Subcutaneous daratumumab in Asian patients with heavily pretreated multiple myeloma: subgroup analyses of the noninferiority, phase 3 COLUMBA study. Ann Hematol. 2021;100(4):1065–1077. doi:10.1007/s00277-021-04405-2
48. Mateos MV, Usmani SZ. Subcutaneous versus intravenous daratumumab in multiple myeloma - Authors’ reply. Lancet Haematol. 2020;7(8):e559. doi:10.1016/s2352-3026(20)30188-5
49. Moreno L, Perez C, Zabaleta A, et al. The mechanism of action of the anti-CD38 monoclonal antibody isatuximab in multiple myeloma. Clin Cancer Res. 2019;25(10):3176–3187. doi:10.1158/1078-0432.Ccr-18-1597
50. Dhillon S. Isatuximab: first approval. Drugs. 2020;80(9):905–912. doi:10.1007/s40265-020-01311-1
51. Attal M, Richardson PG, Rajkumar SV, et al. Isatuximab plus pomalidomide and low-dose dexamethasone versus pomalidomide and low-dose dexamethasone in patients with relapsed and refractory multiple myeloma (ICARIA-MM): a randomised, multicentre, open-label, phase 3 study. Lancet. 2019;394(10214):2096–2107. doi:10.1016/s0140-6736(19)32556-5
52. Richter J, Sanchez L, Thibaud S. Therapeutic potential of isatuximab in the treatment of multiple myeloma: evidence to date. Semin Oncol. 2020;47(2–3):155–164. doi:10.1053/j.seminoncol.2020.04.004
53. U.S. Food and Drug Administration. FDA approves isatuximab-irfc for multiple myeloma [press release]. Washington, DC; 2021. Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-isatuximab-irfc-multiple-myeloma.
54. Moreau P, Dimopoulos MA, Yong K, et al. Isatuximab plus carfilzomib/dexamethasone versus carfilzomib/dexamethasone in patients with relapsed/refractory multiple myeloma: IKEMA Phase III study design. Future Oncol. 2020;16(2):4347–4358. doi:10.2217/fon-2019-0431
55. Martin T, Mikhael J, Hajek R, et al. Depth of response and response kinetics of isatuximab plus carfilzomib and dexamethasone in relapsed multiple myeloma: ikema interim analysis. Blood. 2020;136(Supplement 1):7–8. doi:10.1182/blood-2020-137681
56. Bringhen S, Pour L, Vorobyev V, et al. Isatuximab plus pomalidomide and dexamethasone in patients with relapsed/refractory multiple myeloma according to prior lines of treatment and refractory status: ICARIA-MM subgroup analysis. Leuk Res. 2021;104:106576. doi:10.1016/j.leukres.2021.106576
57. Richardson PG, Attal M, Campana F, et al. Isatuximab plus pomalidomide/dexamethasone versus pomalidomide/dexamethasone in relapsed/refractory multiple myeloma: ICARIA Phase III study design. Future Oncol. 2018;14(11):1035–1047. doi:10.2217/fon-2017-0616
58. Richardson PG, Attal M, San Miguel J, et al. A phase III, randomized, open-label study of isatuximab (SAR650984) plus pomalidomide (Pom) and dexamethasone (Dex) versus Pom and Dex in relapsed/refractory multiple myeloma. J Clin Oncol. 2017;35 Supplement 15:TPS8057. doi:10.1200/JCO.2017.35.15_suppl.TPS8057
59. Harrison SJ, Perrot A, Alegre A, et al. Subgroup analysis of ICARIA-MM study in relapsed/refractory multiple myeloma patients with high-risk cytogenetics. Br J Haematol. 2021;184:120–131. doi:10.1111/bjh.17499
60. Chari A, Richter JR, Shah N, et al. Phase I-b study of isatuximab + carfilzomib in relapsed and refractory multiple myeloma (RRMM). J Clin Oncol. 2018;36(Supplement 15):8014. doi:10.1200/JCO.2018.36.15_suppl
61. Thai HT, Gaudel-Dedieu N, Cerou M, et al. Model based approach to evaluate isatuximab monthly dosing regimen in relapsed/refractory multiple myeloma patients. Blood. 2020;136(Supplement 1):44. doi:10.1182/blood-2020-139358
62. Manasanch EE, Jagannath S, Lee HC, et al. A multicenter phase II single arm trial of isatuximab in patients with high risk smoldering multiple myeloma (HRSMM). Blood. 2019;134(Supplement 1):3116. doi:10.1182/blood-2019-123205
63. Martin III TG, Mannis GN, Chari A, et al. Phase Ib study of isatuximab and carfilzomib in relapse and refractory multiple myeloma. Blood. 2016;128(22):2111. doi:10.1182/blood.V128.22.2111.2111
64. Orlowski RZ, Goldschmidt H, Cavo M, et al. Phase III (IMROZ) study design: isatuximab plus bortezomib (V), lenalidomide (R), and dexamethasone (d) vs VRd in transplant-ineligible patients (pts) with newly diagnosed multiple myeloma (NDMM). J Clin Oncol. 2018;36 Supplement 15:TPS8055. doi:10.1200/JCO.2018.36.15_suppl.TPS805
65. Martin T, Richter J, Vij R, et al. A dose finding phase II trial of isatuximab (SAR650984, anti-CD38 mAb) as a single agent in relapsed/refractory multiple myeloma. Blood. 2015;126(23):509. doi:10.1182/blood.V126.23.509.509
66. Martin T, Baz R, Benson DM, et al. A Phase 1b study of isatuximab plus lenalidomide and dexamethasone for relapsed/refractory multiple myeloma. Blood. 2017;129(25):3294–3303. doi:10.1182/blood-2016-09-740787
67. Mikhael J, Richardson PG, Usmani SZ, et al. A phase Ib study of isatuximab in combination with pomalidomide (Pom) and dexamethasone (Dex) in relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2017;35(Supplement 15):8038. doi:10.1200/JCO.2018.36.15_suppl.8038
68. Mikhael J, Richardson PG, Usmani SZ, et al. Final results of a phase Ib study of isatuximab (ISA) plus pomalidomide (Pom) and dexamethasone (dex) in relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2018;36:8038. doi:10.1200/JCO.2018.36.15_suppl.8038
69. Mikhael J, Richardson P, Usmani SZ, et al. A phase 1b study of isatuximab plus pomalidomide/dexamethasone in relapsed/refractory multiple myeloma. Blood. 2019;134(2):123–133. doi:10.1182/blood-2019-02-895193
70. Usmani SZ, Karanes C, Bensinger WI, et al. Final results of a phase 1b study of isatuximab short-duration fixed-volume infusion combination therapy for relapsed/refractory multiple myeloma. Leukemia. 2021. doi:10.1038/s41375-021-01262-w
71. Grosicki S, Bednarczyk M, Barchnicka A, et al. Elotuzumab in the treatment of relapsed and refractory multiple myeloma. Future Oncol. 2021;17(13):1581–1591. doi:10.2217/fon-2020-1088
72. Gavriatopoulou M, Terpos E, Kastritis E, et al. Efficacy and safety of elotuzumab for the treatment of multiple myeloma. Expert Opin Drug Saf. 2017;16(2):237–245. doi:10.1080/14740338.2017.1279603
73. Collins SM, Bakan CE, Swartzel GD, et al. Elotuzumab directly enhances NK cell cytotoxicity against myeloma via CS1 ligation: evidence for augmented NK cell function complementing ADCC. Cancer Immunol Immunother. 2013;62(12):1841–1849. doi:10.1007/s00262-013-1493-8
74. Hsi ED, Steinle R, Balasa B, et al. CS1, a potential new therapeutic antibody target for the treatment of multiple myeloma. Clin Cancer Res. 2008;14(9):2775–2784. doi:10.1158/1078-0432.ccr-07-4246
75. Markham A. Elotuzumab: first global approval. Drugs. 2016;76(3):397–403. doi:10.1007/s40265-016-0540-0
76. Zonder JA, Mohrbacher AF, Singhal S, et al. A phase 1, multicenter, open-label, dose escalation study of elotuzumab in patients with advanced multiple myeloma. Blood. 2012;120(3):552–559. doi:10.1182/blood-2011-06-360552
77. Lonial S, Dimopoulos M, Palumbo A, et al. Elotuzumab therapy for relapsed or refractory multiple myeloma. N Engl J Med. 2015;373(7):621–631. doi:10.1056/NEJMoa1505654
78. Dimopoulos MA, Lonial S, Betts KA, et al. Elotuzumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: extended 4-year follow-up and analysis of relative progression-free survival from the randomized ELOQUENT-2 trial. Cancer. 2018;124(20):4032–4043. doi:10.1002/cncr.31680
79. Dimopoulos MA, Dytfeld D, Grosicki S, et al. Elotuzumab plus pomalidomide and dexamethasone for multiple myeloma. N Engl J Med. 2018;379(19):1811–1822. doi:10.1056/NEJMoa1805762
80. Trudel S, Moreau P, Touzeau C. Update on elotuzumab for the treatment of relapsed/refractory multiple myeloma: patients’ selection and perspective. Onco Targets Ther. 2019;12:5813–5822. doi:10.2147/ott.S174640
81. Usmani SZ, Hoering A, Ailawadhi S, et al. Bortezomib, lenalidomide, and dexamethasone with or without elotuzumab in patients with untreated, high-risk multiple myeloma (SWOG-1211): primary analysis of a randomised, phase 2 trial. Lancet Haematol. 2021;8(1):e45–e54. doi:10.1016/s2352-3026(20)30354-9
82. Jakubowiak AJ, Benson DM, Bensinger W, et al. Phase I trial of anti-CS1 monoclonal antibody elotuzumab in combination with bortezomib in the treatment of relapsed/refractory multiple myeloma. J Clin Oncol. 2012;30(16):1960–1965. doi:10.1200/jco.2011.37.7069
83. Silvennoinen RH, Nahi H, Anttila P, et al. Carfilzomib, elotuzumab and dexamethasone for relapsed or refractory myeloma patients. Blood. 2020;136(Supplement 1):20. doi:10.1182/blood-2020-138447
84. Yee AJ, Laubach J, Campagnaro EL, et al. A phase II study of elotuzumab in combination with pomalidomide, bortezomib, and dexamethasone in relapsed and refractory multiple myeloma. J Clin Oncol. 2018;36(Supplement 15):8012. doi:10.1200/JCO.2018.36.15_suppl.8012
85. Berenson J, Manges R, Badarinath S, et al. A phase 2 safety study of accelerated elotuzumab infusion, over less than 1 h, in combination with lenalidomide and dexamethasone, in patients with multiple myeloma. Am J Hematol. 2017;92(5):460–466. doi:10.1002/ajh.24687
86. Jakubowiak A, Offidani M, Pegourie B, et al. Randomized phase 2 study: elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexamethasone for relapsed/refractory MM. Blood. 2016;127(23):2833–2840. doi:10.1182/blood-2016-01-694604
87. Jagannath S, Laubach J, Wong E, et al. Elotuzumab monotherapy in patients with smouldering multiple myeloma: a phase 2 study. Br J Haematol. 2018;182:495–503. doi:10.1111/bjh.15384
88. Passey C, Darbenzio R, Jou YM, et al. Effects of elotuzumab on QT interval and cardiac safety in patients with multiple myeloma. Cancer Chemother Pharmacol. 2016;78(6):1237–1244. doi:10.1007/s00280-016-3182-8
89. Salwender H, Bertsch U, Weisel K, et al. Rationale and design of the German-speaking myeloma multicenter group (GMMG) trial HD6: a randomized phase III trial on the effect of elotuzumab in VRD induction/consolidation and lenalidomide maintenance in patients with newly diagnosed myeloma. BMC Cancer. 2019;19(1):504. doi:10.1186/s12885-019-5600-x
90. Usmani SZ, Ailawadhi S, Sexton R, et al. Primary analysis of the randomized phase II trial of bortezomib, lenalidomide, dexamthasone with/without elotuzumab for newly diagnosed, high-risk multiple myeloma (SWOG-1211). J Clin Oncol. 2020;38 Supplement 15:8507. doi:10.1200/JCO.2020.38.15_suppl.8507
91. Passey C, Mora J, Dodge R, et al. An integrated assessment of the effects of immunogenicity on the pharmacokinetics, safety, and efficacy of elotuzumab. Aaps j. 2017;19(2):557–567. doi:10.1208/s12248-016-0033-9
92. Taniwaki M, Yoshida M, Matsumoto Y, et al. Elotuzumab for the treatment of relapsed or refractory multiple myeloma, with special reference to its modes of action and SLAMF7 signaling. Mediterr J Hematol Infect Dis. 2018;10(1):e2018014. doi:10.4084/mjhid.2018.014
93. Dimopoulos MA, Lonial S, White D, et al. Elotuzumab plus lenalidomide/dexamethasone for relapsed or refractory multiple myeloma: ELOQUENT-2 follow-up and post-hoc analyses on progression-free survival and tumour growth. Br J Haematol. 2017;178(6):896–905. doi:10.1111/bjh.14787
94. Dimopoulos MA, Lonial S, White D, et al. Elotuzumab, lenalidomide, and dexamethasone in RRMM: final overall survival results from the phase 3 randomized ELOQUENT-2 study. Blood Cancer J. 2020;10(9):91. doi:10.1038/s41408-020-00357-4
95. Richardson PG, Jagannath S, Moreau P, et al. Elotuzumab in combination with lenalidomide and dexamethasone in patients with relapsed multiple myeloma: final phase 2 results from the randomised, open-label, phase 1b-2 dose-escalation study. Lancet Haematol. 2015;2(12):e516–527. doi:10.1016/s2352-3026(15)00197-0
96. Lonial S, Richardson PG, Reece DE, et al. CheckMate 602: an open-label, randomized, phase 3 trial of combinations of nivolumab, elotuzumab, pomalidomide and dexamethasone in relapsed/refractory multiple myeloma. J Clin Oncol. 2017;35(15):8052. doi:10.1200/JCO.2017.35.15_suppl.TPS8052
97. Yu J, Song Y, Tian W. How to select IgG subclasses in developing anti-tumor therapeutic antibodies. J Hematol Oncol. 2020;13(1):45. doi:10.1186/s13045-020-00876-4
98. Pereira NA, Chan KF, Lin PC, et al. The “less-is-more” in therapeutic antibodies: afucosylated anti-cancer antibodies with enhanced antibody-dependent cellular cytotoxicity. mAbs. 2018;10(5):693–711. doi:10.1080/19420862.2018.1466767
99. Pan J, Sun Y, Zhang N, et al. Characteristics of BAFF and APRIL factor expression in multiple myeloma and clinical significance. Oncol Lett. 2017;14(3):2657–2662. doi:10.3892/ol.2017.6528
100. Raje NS, Moreau P, Terpos E, et al. Phase 2 study of tabalumab, a human anti-B-cell activating factor antibody, with bortezomib and dexamethasone in patients with previously treated multiple myeloma. Br J Haematol. 2017;176(5):783–795. doi:10.1111/bjh.14483
101. Rossi J-F, Moreaux J, Hose D, et al. Atacicept in relapsed/refractory multiple myeloma or active Waldenström’s macroglobulinemia: a phase I study. Br J Cancer. 2009;101(7):1051–1058. doi:10.1038/sj.bjc.6605241
102. Laabi Y, Gras M-P, Brouet J-C, et al. The BCMA gene, preferentially expressed during B lymphoid maturation, is bidirectionally transcribed. Nucleic Acids Res. 1994;22(7):1147–1154. doi:10.1093/nar/22.7.1147
103. Kozlow EJ, Wilson GL, Fox CH, et al. Subtractive cDNA cloning of a novel member of the Ig gene superfamily expressed at high levels in activated B lymphocytes. Blood. 1993;81(2):454–461. doi:10.1182/blood.V81.2.454.454
104. Zhou LJ, Schwarting R, Smith HM, et al. A novel cell-surface molecule expressed by human interdigitating reticulum cells, Langerhans cells, and activated lymphocytes is a new member of the Ig superfamily. J Immunol. 1992;149(2):735–742.
105. Laabi Y, Gras MP, Carbonnel F, et al. A new gene, BCM, on chromosome 16 is fused to the interleukin 2 gene by a t(4;16)(q26;p13) translocation in a malignant T cell lymphoma. EMBO J. 1992;11(11):3897–3904. doi:10.1002/j.1460-2075.1992.tb05482.x
106. Cho SF, Anderson KC, Tai YT. Targeting B cell maturation antigen (BCMA) in multiple myeloma: potential uses of BCMA-based immunotherapy. Front Immunol. 2018;9:1821. doi:10.3389/fimmu.2018.01821
107. Cho SF, Lin L, Xing L, et al. BCMA-targeting therapy: driving a new era of immunotherapy in multiple myeloma. Cancers. 2020;12(6):1473. doi:10.3390/cancers12061473
108. Fang Y, Hou J. Immunotherapeutic strategies targeting B cell maturation antigen in multiple myeloma. Mil Med Res. 2021;8(1):9. doi:10.1186/s40779-021-00302-x
109. Shah N, Chari A, Scott E, et al. B-cell maturation antigen (BCMA) in multiple myeloma: rationale for targeting and current therapeutic approaches. Leukemia. 2020;34(4):985–1005. doi:10.1038/s41375-020-0734-z
110. Sanchez E, Tanenbaum EJ, Patil S, et al. The clinical significance of B-cell maturation antigen as a therapeutic target and biomarker. Expert Rev Mol Diagn. 2018;18(4):319–329. doi:10.1080/14737159.2018.1448269
111. Laurent SA, Hoffmann FS, Kuhn PH, et al. Gamma-secretase directly sheds the survival receptor BCMA from plasma cells. Nat Commun. 2015;6:7333. doi:10.1038/ncomms8333
112. Sanchez E, Li M, Kitto A, et al. Serum B-cell maturation antigen is elevated in multiple myeloma and correlates with disease status and survival. Br J Haematol. 2012;158(6):727–738. doi:10.1111/j.1365-2141.2012.09241.x
113. Pont MJ, Hill T, Cole GO, et al. Gamma-secretase inhibition increases efficacy of BCMA-specific chimeric antigen receptor T cells in multiple myeloma. Blood. 2019;134(19):1585–1597. doi:10.1182/blood.2019000050
114. Sanchez E, Gillespie A, Tang G, et al. Soluble B-cell maturation antigen mediates tumor-induced immune deficiency in multiple myeloma. Clin Cancer Res. 2016;22(13):3383–3397. doi:10.1158/1078-0432.Ccr-15-2224
115. Lassiter G, Bergeron C, Guedry R, et al. Belantamab mafodotin to treat multiple myeloma: a comprehensive review of disease, drug efficacy and side effects. Curr Oncol. 2021;28(1):640–660. doi:10.3390/curroncol28010063
116. Tai YT, Anderson KC. Targeting B-cell maturation antigen in multiple myeloma. Immunotherapy. 2015;7(11):1187–1199. doi:10.2217/imt.15.77
117. Tai YT, Mayes PA, Acharya C, et al. Novel afucosylated anti-B cell maturation antigen-monomethyl auristatin F antibody-drug conjugate (GSK2857916) induces potent and selective anti-multiple myeloma activity. Blood. 2014;123(20):3128–3138. doi:10.1182/blood-2013-10-535088
118. U.S. Food and Drug Administration. FDA granted accelerated approval to belantamab mafodotin-blmf for multiple myeloma [press release]. Washington, DC; 2020. Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-granted-accelerated-approval-belantamab-mafodotin-blmf-multiple-myeloma.
119. Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2019;21(2):207–221. doi:10.1016/s1470-2045(19)30788-0
120. Farooq AV, Degli Esposti S, Popat R, et al. Corneal epithelial findings in patients with multiple myeloma treated with antibody-drug conjugate belantamab mafodotin in the pivotal, randomized, DREAMM-2 study. Ophthalmol Ther. 2020;9:889–911. doi:10.1007/s40123-020-00280-8
121. Eaton JS, Miller PE, Mannis MJ, et al. Ocular adverse events associated with antibody-drug conjugates in human clinical trials. J Ocul Pharmacol Ther. 2015;31(10):589–604. doi:10.1089/jop.2015.0064
122. Lee HC, Raje NS, Landgren O, et al. Letter: phase 1 study of the anti-BCMA antibody-drug conjugate AMG 224 in patients with relapsed/refractory multiple myeloma. Leukemia. 2020;35:255–258. doi:10.1038/s41375-020-0834-9
123. Joubert N, Beck A, Dumontet C, et al. Antibody-drug conjugates: the last decade. Pharmaceuticals. 2020;13(9):245. doi:10.3390/ph13090245
124. Pahl A, Lutz C, Hechler T. Amanitins and their development as a payload for antibody-drug conjugates. Drug Discov Today Technol. 2018;30:85–89. doi:10.1016/j.ddtec.2018.08.005
125. Spycher PR, Frei JC, Wehrmuller JE, et al. Overcoming limitations of current antibody-drug conjugates (ADCs) by a novel linker technology. Cancer Res. 2019;79(13):LB–106. doi:10.1158/1538-7445.Am2019-lb-106
126. Figueroa-Vazquez V, Ko J, Breunig C, et al. HDP-101, an anti-BCMA antibody-drug conjugate, safely delivers amanitin to induce cell death in proliferating and resting multiple myeloma cells. Mol Cancer Ther. 2021;20(2):367–378. doi:10.1158/1535-7163.Mct-20-0287
127. Heidelberg Pharma AG FDA allows Heidelberg Pharma to start a phase I/IIa clinical trial with ATAC candidate HDP-101 [press release]. Ladenburg, Germany; 2021. Available from:https://pipelinereview.com/index.php/2021020477353/Antibodies/FDA-Allows-Heidelberg-Pharma-to-Start-A-Phase-I/IIa-Clinical-Trial-with-ATAC-Candidate-HDP-101.html.
128. Trudel S, Lendvai N, Popat R, et al. Deep and durable responses in patients (pts) with relapsed/refractory multiple myeloma (MM) treated with monotherapy GSK2857916, an antibody drug conjugate against B-cell maturation antigen (BCMA): preliminary results from part 2 of study BMA117159. Blood. 2017;130:741. doi:10.1182/blood.V130.Suppl_1.741.741
129. Popat R, Suvannasankha A, Kapetanakis V, et al. DREAMM-2: assessing efficacy via indirect comparison of single-agent belantamab mafodotin versus selinexor plus dexamethasone combination in anti-CD38 exposed relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2020;38 Supplement 15:e20527. doi:10.1200/JCO.2020.38.15_suppl.e20527
130. Richardson PG, Lee HC, Abdallah AO, et al. Single-agent belantamab mafodotin for relapsed/refractory multiple myeloma: analysis of the lyophilised presentation cohort from the pivotal DREAMM-2 study. Blood Cancer J. 2020;10(10):106. doi:10.1038/s41408-020-00369-0
131. Weisel K, Hopkins TG, Fecteau D, et al. DREAMM-3: a phase 3, open-label, randomized study to evaluate the efficacy and safety of belantamab mafodotin (GSK2857916) monotherapy compared with pomalidomide plus low-dose dexamethasone (pom/dex) in participants with relapsed/refractory multiple myeloma (RRMM). Blood. 2019;134 Supplement 1:1900. doi:10.1182/blood-2019-129893
132. Trudel S, Nooka A, Fecteau D, et al. DREAMM 4: a phase I/II single-arm open-label study to explore safety and clinical activity of belantamab mafodotin (GSK2857916) administered in combination with pembrolizumab in patients with relapsed/refractory multiple myeloma (RRMM). Ann Oncol. 2019;30 Supplement 5:V447. doi:10.1093/annonc/mdz251.039
133. Nooka AK, Stockerl-Goldstein K, Quach H, et al. DREAMM-6: safety and tolerability of belantamab mafodotin in combination with bortezomib/dexamethasone in relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2020;38 Supplement 15:8502. doi:10.1200/JCO.2020.38.15_suppl.8502
134. Popat R, Nooka A, Stockerl-Goldstein K, et al. DREAMM-6: safety, tolerability and clinical activity of belantamab mafodotin (belamaf) in combination with bortezomib/dexamethasone (bordex) in relapsed/refractory multiple myeloma. Blood. 2020;136(Supplement 1):19–20. doi:10.1182/blood-2020-139332
135. Rifkin RM, Boyd K, Grosicki S, et al. DREAMM-7: a phase III study of the efficacy and safety of belantamab mafodotin (belamaf) with bortezomib, and dexamethasone (B-Vd) in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2020;136(Supplement 1):53–54. doi:10.1182/blood-2020-139181
136. Trudel S, Davis R, Lewis NM, et al. DREAMM-8: a phase III study of the efficacy and safety of belantamab mafodotin with pomalidomide and dexamethasone (B-Pd) vs pomalidomide plus bortezomib and dexamethasone (PVd) in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2020;136(Supplement 1):4. doi:10.1182/blood-2020-139785
137. Usmani SZ, Terpos E, Janowski W, et al. DREAMM-9: phase III study of belantamab mafodotin plus VRd versus VRd alone in transplant-ineligible newly diagnosed multiple myeloma (TI NDMM). J Clinical Oncol. 2020;38(15):TPS8556. doi:10.1200/JCO.2020.38.15_suppl.TPS8556
138. Nisonoff A, Rivers MM. Recombination of a mixture of univalent antibody fragments of different specificity. Arch Biochem Biophys. 1961;93:460–462. doi:10.1016/0003-9861(61)90296-x
139. Huang S, van Duijnhoven SMJ, Sijts A, et al. Bispecific antibodies targeting dual tumor-associated antigens in cancer therapy. J Cancer Res Clin Oncol. 2020;146(12):3111–3122. doi:10.1007/s00432-020-03404-6
140. Rader C. Bispecific antibodies in cancer immunotherapy. Curr Opin Biotechnol. 2020;65:9–16. doi:10.1016/j.copbio.2019.11.020
141. Wang Q, Chen Y, Park J, et al. Design and production of bispecific antibodies. Antibodies. 2019;8(3):43. doi:10.3390/antib8030043
142. Spicer BA, Conroy PJ, Law RHP, et al. Perforin-A key (shaped) weapon in the immunological arsenal. Semin Cell Dev Biol. 2017;72:117–123. doi:10.1016/j.semcdb.2017.07.033
143. Voskoboinik I, Whisstock JC, Trapani JA. Perforin and granzymes: function, dysfunction and human pathology. Nat Rev Immunol. 2015;15(6):388–400. doi:10.1038/nri3839
144. Baeuerle PA, Reinhardt C. Bispecific T-cell engaging antibodies for cancer therapy. Cancer Res. 2009;69(12):4941–4944. doi:10.1158/0008-5472.Can-09-0547
145. Mandikian D, Takahashi N, Lo AA, et al. Relative target affinities of T-cell-dependent bispecific antibodies determine biodistribution in a solid tumor mouse model. Mol Cancer Ther. 2018;17(4):776–785. doi:10.1158/1535-7163.Mct-17-0657
146. Mazor Y, Sachsenmeier KF, Yang C, et al. Enhanced tumor-targeting selectivity by modulating bispecific antibody binding affinity and format valence. Sci Rep. 2017;7:40098. doi:10.1038/srep40098
147. Velders MP, van Rhijn CM, Oskam E, et al. The impact of antigen density and antibody affinity on antibody-dependent cellular cytotoxicity: relevance for immunotherapy of carcinomas. Br J Cancer. 1998;78(4):478–483. doi:10.1038/bjc.1998.518
148. Jen EY, Xu Q, Schetter A, et al. FDA approval: blinatumomab for patients with B-cell precursor acute lymphoblastic leukemia in morphologic remission with minimal residual disease. Clin Cancer Res. 2019;25(2):473–477. doi:10.1158/1078-0432.Ccr-18-2337
149. Sanford M. Blinatumomab: first global approval. Drugs. 2015;75(3):321–327. doi:10.1007/s40265-015-0356-3
150. Haas KM, Tedder TF. Role of the CD19 and CD21/35 receptor complex in innate immunity, host defense and autoimmunity. Adv Exp Med Biol. 2005;560:125–139. doi:10.1007/0-387-24180-9_16
151. Wang K, Wei G, Liu D. CD19: a biomarker for B cell development, lymphoma diagnosis and therapy. Exp Hematol Oncol. 2012;1(1):36. doi:10.1186/2162-3619-1-36
152. Nerreter T, Letschert S, Gotz R, et al. Super-resolution microscopy reveals ultra-low CD19 expression on myeloma cells that triggers elimination by CD19 CAR-T. Nat Commun. 2019;10(1):3137. doi:10.1038/s41467-019-10948-w
153. Abramson HN. B-cell maturation antigen (BCMA) as a target for new drug development in relapsed and/or refractory multiple myeloma. Int J Mol Sci. 2020;21(15):5192. doi:10.3390/ijms21155192
154. Caraccio C, Krishna S, Phillips DJ, et al. Bispecific antibodies for multiple myeloma: a review of targets, drugs, clinical trials, and future directions. Front Immunol. 2020;11:501. doi:10.3389/fimmu.2020.00501
155. Martino M, Paviglianiti A. An update on B-cell maturation antigen-targeted therapies in multiple myeloma. Expert Opin Biol Ther. 2021;1–10. doi:10.1080/14712598.2021.1872540
156. Sanchez L, Dardac A, Madduri D, et al. B-cell maturation antigen (BCMA) in multiple myeloma: the new frontier of targeted therapies. Ther Adv Hematol. 2021;12:2040620721989585. doi:10.1177/2040620721989585
157. Topp MS, Duell J, Zugmaier G, et al. Anti-B-cell maturation antigen BiTE molecule AMG 420 induces responses in multiple myeloma. J Clin Oncol. 2020;38(8):775–783. doi:10.1200/jco.19.02657
158. Cho SF, Lin L, Xing L, et al. The immunomodulatory drugs lenalidomide and pomalidomide enhance the potency of AMG 701 in multiple myeloma preclinical models. Blood Advances. 2020;4(17):4195–4207. doi:10.1182/bloodadvances.2020002524
159. Harrison SJ, Minnema MC, Lee HC, et al. A phase 1 first in human (FIH) study of AMG 701, an anti-B-cell maturation antigen (BCMA) half-life extended (HLE) BiTE (R) (bispecific T-cell engager) molecule, in relapsed/refractory (RR) multiple myeloma (MM). Blood. 2020;136 Supplement 1:28–29. doi:10.1182/blood-2020-134063
160. Amgen Inc. Amgen reports fourth quarter and full year 2020 financial results [press release]. Thousand Oaks, CA; 2021. Available from:https://investors.amgen.com/news-releases/news-release-details/amgen-reports-fourth-quarter-and-full-year-2020-financial/.
161. Lancman G, Richter J, Chari A. Bispecifics, trispecifics, and other novel immune treatments in myeloma. Hematology Am Soc Hematol Educ Program. 2020;2020(1):264–271. doi:10.1182/hematology.2020000110
162. Cooper D, Madduri D, Lentzsch S, et al. Safety and preliminary clinical activity of REGN5458, an anti-BCMA x anti-CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma. Blood. 2019;134:3176. doi:10.1182/blood-2019-126818
163. DiLillo DJ, Olson K, Mohrs K, et al. A BCMAxCD3 bispecific T cell-engaging antibody demonstrates robust antitumor efficacy similar to that of anti-BCMA CAR T cells. Blood Advances. 2021;5(5):1291–1304. doi:10.1182/bloodadvances.2020002736
164. Girgis S, Shetty S, Jiao T, et al. Exploratory pharmacokinetic/pharmacodynamic and tolerability study of BCMAxCD3 in cynomolgus monkeys. Blood. 2016;128:5668. doi:10.1182/blood.V128.22.5668.5668
165. Pillarisetti K, Powers G, Luistro L, et al. Teclistamab is an active T cell-redirecting bispecific antibody against B-cell maturation antigen for multiple myeloma. Blood Advances. 2020;4(18):4538–4549. doi:10.1182/bloodadvances.2020002393
166. Garfall AL, Usmani SZ, Mateos MV, et al. Updated phase 1 results of teclistamab, a B-cell maturation antigen (BCMA) x CD3 bispecific antibody, in relapsed and/or refractory multiple myeloma (RRMM). Blood. 2020;136:4. doi:10.1182/blood-2020-138831
167. Usmani SZ, Mateos MV, Nahi H, et al. Phase I study of teclistamab, a humanized B-cell maturation antigen (BCMA) x CD3 bispecific antibody, in relapsed/refractory multiple myeloma (R/R MM). J Clin Oncol. 2020;38(15Supplement):100. doi:10.1200/JCO.2020.38.15_suppl.100
168. Krishnan AY, Garfall AL, Mateos MV, et al. Updated phase 1 results of teclistamab, a B-cell maturation antigen (BCMA) × CD3 bispecific antibody, in relapsed/refractory multiple myeloma (MM). J Clin Oncol. 2021;39(15Supplement):8007. doi:10.1200/JCO.2021.39.15_suppl.8007
169. Suzuki S, Annaka H, Konno S, et al. Engineering the hinge region of human IgG1 Fc-fused bispecific antibodies to improve fragmentation resistance. Sci Rep. 2018;8(1):17253. doi:10.1038/s41598-018-35489-y
170. Lesokhin AM, Raje N, Gasparetto CJ, et al. A phase I, open-label study to evaluate the safety, pharmacokinetic, pharmacodynamic, and clinical activity of PF-06863135, a B-cell maturation antigen/CD3 bispecific antibody, in patients with relapsed/refractory advanced multiple myeloma. Blood. 2018;132 Supplement 1:3229. doi:10.1182/blood-2018-99-110427
171. Raje NS, Jakubowiak A, Gasparetto C, et al. Safety, clinical activity, pharmacokinetics, and pharmacodynamics from a phase I study of PF-06863135, a B-cell maturation antigen (BCMA)–CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2019;128:1869. doi:10.1182/blood-2019-121805
172. Lesokhin AM, Levy MY, Dalovisio AP, et al. Preliminary safety, efficacy, pharmacokinetics, and pharmacodynamics of subcutaneously (SC) administered PF-06863135, a B-cell maturation antigen (BCMA)-CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2020;136 Supplement 1:8–9. doi:10.1182/blood-2020-133355
173. Bahlis NJ, Raje NS, Costello C, et al. Efficacy and safety of elranatamab (PF-06863135), a B-cell maturation antigen (BCMA)-CD3 bispecific antibody, in patients with relapsed or refractory multiple myeloma (MM). J Clin Oncol. 2021;39 15 suppl:8006. doi:10.1200/JCO.2021.39.15_suppl.8006
174. Pfizer, Inc. Pfizer initiates pivotal phase 2 MAGNETISMM-3 trial of BCMA-CD3 bispecific antibody elranatamab (PF-06863135) in multiple myeloma [press release]. New York, NY; 2021. Available from:https://www.pfizer.com/news/press-release/press-release-detail/pfizer-initiates-pivotal-phase-2-magnetismm-3-trial-bcma.
175. Costa LJ, Wong SW, Bermúdez A, et al. First clinical study of the B-cell maturation antigen (BCMA) 2+1 T cell engager (TCE) CC-93269 in patients (pts) with relapsed/refractory multiple myeloma (RRMM): interim results of a phase 1 multicenter trial. Blood. 2019;134:143. doi:10.1182/blood-2019-122895
176. Trinklein ND, Pham D, Schellenberger U, et al. Efficient tumor killing and minimal cytokine release with novel T-cell agonist bispecific antibodies. mAbs. 2019;11(4):639–652. doi:10.1080/19420862.2019.1574521
177. Foureau DM, Bhutani M, Robinson M, et al. Ex vivo efficacy of BCMA-bispecific antibody TNB-383B in relapsed/refractory multiple myeloma. eJHaem. 2020;1(1):113–121. doi:10.1002/jha2.69
178. Buelow B, Choudry P, Clarke S, et al. Pre-clinical development of TNB-383B, a fully human T-cell engaging bispecific antibody targeting BCMA for the treatment of multiple myeloma. J Clin Oncol. 2018;36(15Supplement):8034. doi:10.1200/JCO.2018.36.15_suppl.8034
179. Buelow B, D’Souza A, Rodriguez C, et al. A multicenter, phase 1, open-label, dose-escalation and expansion study of TNB-383B, a bispecific antibody targeting BCMA in subjects with relapsed or refractory multiple myeloma. Blood. 2019;(134 Supplement 1):1874. doi:10.1182/blood-2019-123220
180. Rodriguez C, D’Souza A, Shah N, et al. Initial results of a phase I study of TNB-383B, a BCMA x CD3 bispecific T-cell redirecting antibody, in relapsed/refractory multiple myeloma. Blood. 2020;136 Supplement 1:43–44. doi:10.1182/blood-2020-139893
181. Law CL, Aaron W, Austin R, et al. Preclinical and nonclinical characterization of HPN217: a tri-specific T cell activating construct (TriTAC) targeting B cell maturation antigen (BCMA) for the treatment of multiple myeloma. Blood. 2018;132:3225. doi:10.1182/blood-2018-99-113921
182. Schade H, Madan S, Medvedova E, et al. HPN217-3001: a phase 1/2 open-label, multicenter, dose escalation and dose expansion study of the safety, tolerability, and pharmacokinetics of HPN217, a Bcma-targeting T-cell engager, in patients with relapsed/refractory multiple myeloma. Blood. 2020;136:10. doi:10.1182/blood-2020-136012
183. Smyth MJ, Cretney E, Kelly JM, et al. Activation of NK cell cytotoxicity. Mol Immunol. 2005;42(4):501–510. doi:10.1016/j.molimm.2004.07.034
184. Duell J, Lammers PE, Djuretic I, et al. Bispecific antibodies in the treatment of hematologic malignancies. Clin Pharmacol Ther. 2019;106(4):781–791. doi:10.1002/cpt.1396
185. Gantke T, Weichel M, Reusch U, et al. Trispecific antibodies for selective CD16A-directed NK-cell engagement in multiple myeloma. Blood. 2016;128:4513. doi:10.1182/blood.V128.22.4513.4513
186. Kakiuchi-Kiyota S, Schutten MM, Adedeji AO, et al. Preclinical pharmacology and safety of RO7297089, a novel anti-BCMA/CD16a bispecific antibody for the treatment of multiple myeloma. Cancer Res. 2020;80(16Supplement):4556. doi:10.1158/1538-7445.Am2020-4556
187. Draghi M, Schafer JL, Nelson A, et al. Preclinical development of a first-in-class NKp30xBCMA NK cell engager for the treatment of multiple myeloma. Cancer Res. 2019;79:4972. doi:10.1158/1538-7445.AM2019-4972
188. Watkins-Yoon J, Guzman W, Oliphant A, et al. CTX-8573, an innate-cell engager targeting BCMA, is a highly potent multispecific antibody for the treatment of multiple myeloma. Blood. 2019;134:3182. doi:10.1182/blood-2019-128749
189. Li J, Stagg NJ, Johnston J, et al. Membrane-proximal epitope facilitates efficient T cell synapse formation by anti-FcRH5/CD3 and is a requirement for myeloma cell killing. Cancer Cell. 2017;31(3):383–395. doi:10.1016/j.ccell.2017.02.001
190. Cohen AD, Harrison SJ, Krishnan A, et al. Initial clinical activity and safety of BFCR4350A, a FcRH5/CD3 T-cell-engaging bispecific antibody, in relapsed/refractory multiple myeloma. Blood. 2020;136 Supplement 1:42–43. doi:10.1182/blood-2020-136985
191. Nakamura R, Lear S, Wilson D, et al. Early pharmacodynamic changes in T-cell activation, proliferation, and cytokine production confirm the mode of action of BFCR4350A, a FcRH5/CD3 T-cell-engaging bispecific antibody, in patients with relapsed/refractory multiple myeloma. Blood. 2020;136 Supplement 1:14–15. doi:10.1182/blood-2020-136980
192. Richter JR, Landgren CO, Kauh JS, et al. Phase 1, multicenter, open-label study of single-agent bispecific antibody T-cell engager GBR 1342 in relapsed/refractory multiple myeloma. J Clin Oncol. 2018;36(15):2. doi:10.1200/JCO.2018.36.15_suppl.TPS3132
193. Lum LG, Thakur A, Al-Kadhimi Z, et al. Induction of anti-myeloma cellular and humoral immunity by pre-targeting clonogenic myeloma cells prior to stem cell transplant with T cells armed with anti-CD3 x anti-CD20 bispecific antibody leads to transfer of cellular and humoral anti-myeloma immunity. Blood. 2013;122(21):139. doi:10.1182/blood.V122.21.139.139
194. Lum LG, Archana T, Muneer A, et al. Targeting myeloma stem cells with T cells armed with anti-CD3 x anti-CD20 bispecific antibody (CD20BI) prior to ASCT leads to development of anti-myeloma immune responses post autologous stem cell transplant that can be boosted with targeted T cells. Biology Blood Marrow Transplantation. 2012;18(2Supplement 2):S259. doi:10.1016/j.bbmt.2011.12.162
195. Verkleij CPM, Broekmans MEC, van Duin M, et al. Preclinical activity and determinants of response of the GPRC5DxCD3 bispecific antibody talquetamab in multiple myeloma. Blood Advances. 2021;5(8):2196–2215. doi:10.1182/bloodadvances.2020003805
196. Chari A, Berdeja JG, Oriol A, et al. A phase 1, first-in-human study of talquetamab, a G protein-coupled receptor family C group 5 member D (GPRC5D) x CD3 bispecific antibody, in patients with relapsed and/or refractory multiple myeloma (RRMM). Blood. 2020;136:40–41. doi:10.1182/blood-2020-133873
197. Kodama T, Kochi Y, Nakai W, et al. Anti-GPRC5D/CD3 bispecific T cell-redirecting antibody for the treatment of multiple myeloma. Mol Cancer Ther. 2019;18(9):1555–1564. doi:10.1158/1535-7163.Mct-18-1216
198. Topp M, Duell J, Zugmaier G, et al. Evaluation of AMG 420, an anti-BCMA bispecific T-cell engager (Bite®) immunotherapy, in R/R multiple myeloma (MM) patients: updated results of a first-In-human (FIH) phase 1 dose escalation study. J Clin Oncol. 2019;37(15Supplement):8007. doi:10.1200/JCO.2019.37.15_suppl.8007
199. Cho S-F, Lin L, Xing L, et al. AMG 701, a half-life extended anti-BCMA BiTE®, potently induces T cell-redirected lysis of human multiple myeloma cells and can be combined with IMiDs to overcome the immunosuppressive bone marrow microenvironment. Clin Lymphoma Myeloma Leuk. 2019;19(10):e54. doi:10.1016/j.clml.2019.09.082
200. Madduri D, Rosko A, Brayer J, et al. REGN5458, a BCMA x CD3 bispecific monoclonal antibody, induces deep and durable responses in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2020;136 Supplement 1:41–42. doi:10.1182/blood-2020-139192
201. Wall DA, Krueger J. Chimeric antigen receptor T cell therapy comes to clinical practice. Curr Oncol. 2020;27(Suppl 2):S115–S123. doi:10.3747/co.27.5283
202. Rosenbaum L. Tragedy, perseverance, and chance - the story of CAR-T therapy. N Engl J Med. 2017;377(14):1313–1315. doi:10.1056/NEJMp1711886
203. Garfall AL, Stadtmauer EA, Hwang WT, et al. Anti-CD19 CAR T cells with high-dose melphalan and autologous stem cell transplantation for refractory multiple myeloma. JCI Insight. 2018;3(8):e120505. doi:10.1172/jci.insight.120505
204. Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N Engl J Med. 2017;377(26):2531–2544. doi:10.1056/NEJMoa1707447
205. Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1–2 trial. Lancet Oncol. 2019;20(1):31–42. doi:10.1016/s1470-2045(18)30864-7
206. Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019;380(1):45–56. doi:10.1056/NEJMoa1804980
207. Abramson JS, Gordon LI, Palomba ML, et al. Updated safety and long term clinical outcomes in TRANSCEND NHL 001, pivotal trial of lisocabtagene maraleucel (JCAR017) in R/R aggressive NHL. J Clin Oncol. 2018;36:7505. doi:10.1200/JCO.2018.36.15_suppl.7505
208. Muranski P, Boni A, Wrzesinski C, et al. Increased intensity lymphodepletion and adoptive immunotherapy–how far can we go? Nat Clin Pract Oncol. 2006;3(12):668–681. doi:10.1038/ncponc0666
209. Gattinoni L, Finkelstein SE, Klebanoff CA, et al. Removal of homeostatic cytokine sinks by lymphodepletion enhances the efficacy of adoptively transferred tumor-specific CD8+ T cells. J Exp Med. 2005;202(7):907–912. doi:10.1084/jem.20050732
210. Hirayama AV, Gauthier J, Hay KA, et al. The response to lymphodepletion impacts PFS in patients with aggressive non-Hodgkin lymphoma treated with CD19 CAR T cells. Blood. 2019;133(17):1876–1887. doi:10.1182/blood-2018-11-887067
211. Shimizu T, Nomiyama S, Hirata F, et al. Indoleamine 2,3-dioxygenase. Purification and some properties. J Biol Chem. 1978;253(13):4700–4706.
212. Ninomiya S, Narala N, Huye L, et al. Tumor indoleamine 2,3-dioxygenase (IDO) inhibits CD19-CAR T cells and is downregulated by lymphodepleting drugs. Blood. 2015;125(25):3905–3916. doi:10.1182/blood-2015-01-621474
213. Balog A, Lin TA, Maley D, et al. Preclinical characterization of linrodostat mesylate, a novel, potent, and selective oral indoleamine 2,3-dioxygenase 1 inhibitor. Mol Cancer Ther. 2021;20(3):467–476. doi:10.1158/1535-7163.Mct-20-0251
214. van de Donk N, Usmani SZ, Yong K. CAR T-cell therapy for multiple myeloma: state of the art and prospects. Lancet Haematol. 2021;8(6):e446–e461. doi:10.1016/s2352-3026(21)00057-0
215. Ali SA, Shi V, Maric I, et al. T cells expressing an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of multiple myeloma. Blood. 2016;128(13):1688–1700. doi:10.1182/blood-2016-04-711903
216. Brudno JN, Maric I, Hartman SD, et al. T cells genetically modified to express an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of poor-prognosis relapsed multiple myeloma. J Clin Oncol. 2018;36(22):2267–2280. doi:10.1200/jco.2018.77.8084
217. Friedman KM, Garrett TE, Evans JW, et al. Effective targeting of multiple B-cell maturation antigen-expressing hematological malignances by anti-B-cell maturation antigen chimeric antigen receptor T Cells. Hum Gene Ther. 2018;29(5):585–601. doi:10.1089/hum.2018.001
218. U.S. Food and Drug Administration. FDA approves idecabtagene vicleucel for multiple myeloma [press release]. Washington, DC; 2021. Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-idecabtagene-vicleucel-multiple-myeloma.
219. Munshi NC, Anderson LD, Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. doi:10.1056/NEJMoa2024850
220. Zheng W, O’Hear CE, Alli R, et al. PI3K orchestration of the in vivo persistence of chimeric antigen receptor-modified T cells. Leukemia. 2018;32(5):1157–1167. doi:10.1038/s41375-017-0008-6
221. Berdeja JG, Alsina M, Shah ND, et al. 1. Blood. 2019;(134 Supplement 1):927. doi:10.1182/blood-2019-126660
222. Alsina M, Shah N, Raje NS, et al. Updated results from the phase I CRB-402 study of anti-Bcma CAR-T cell therapy bb21217 in patients with relapsed and refractory multiple myeloma: correlation of expansion and duration of response with T cell phenotypes. Blood. 2020;136 Supplement 1:25–26. doi:10.1182/blood-2020-140410
223. Xu J, Chen LJ, Yang SS, et al. Exploratory trial of a biepitopic CAR T-targeting B cell maturation antigen in relapsed/refractory multiple myeloma. Proc Natl Acad Sci U S A. 2019;116(19):9543–9551. doi:10.1073/pnas.1819745116
224. Zhao WH, Liu J, Wang BY, et al. A phase 1, open-label study of LCAR-B38M, a chimeric antigen receptor T cell therapy directed against B cell maturation antigen, in patients with relapsed or refractory multiple myeloma. J Hematol Oncol. 2018;11(1):141. doi:10.1186/s13045-018-0681-6
225. Zhao WH, Liu J, Wang BY, et al. Updated analysis of a phase 1, open-label study of LCAR-B38M, a chimeric antigen receptor T cell therapy directed against B-cell maturation antigen, in patients with relapsed/refractory multiple myeloma. Blood. 2018;132 Supplement 1:955. doi:10.1182/blood-2018-99-110548
226. Madduri D, Berdeja JG, Usmani SZ, et al. CARTITUDE-1: phase 1b/2 study of ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T cell therapy, in relapsed/refractory multiple myeloma. Blood. 2020;(136 Supplement 1):22–25. doi:10.1182/blood-2020-136307
227. Legend Biotech Corp. U.S. Food and Drug Administration grants BCMA CAR-T cilta-cel priority review for the treatment for relapsed/refractory multiple myeloma [press release]. Somerset, NJ; 2021. Available from:https://www.businesswire.com/news/home/20210526006114/en/U.S.-Food-and-Drug-Administration-Grants-BCMA-CAR-T-Cilta-cel-Priority-Review-for-the-Treatment-for-RelapsedRefractory-Multiple-Myeloma.
228. Agha ME, Cohen AD, Madduri D, et al. CARTITUDE-2: efficacy and safety of ciltacabtagene autoleucel (cilta-cel), a BCMA-directed CAR T-cell therapy, in patients with progressive multiple myeloma (MM) after one to three prior lines of therapy. J Clin Oncol. 2021;39(15Supplement):8013. doi:10.1200/JCO.2021.39.15_suppl.8013
229. Goldberg SD, Cardoso RM, Lin T, et al. Engineering a targeted delivery platform using Centyrins. Protein Eng Des Sel. 2016;29(12):563–572. doi:10.1093/protein/gzw054
230. Gattinoni L, Speiser DE, Lichterfeld M, et al. T memory stem cells in health and disease. Nat Med. 2017;23(1):18–27. doi:10.1038/nm.4241
231. Amatya C, Pegues MA, Lam N, et al. Development of CAR T cells expressing a suicide gene plus a chimeric antigen receptor targeting signaling lymphocytic-activation molecule. Mol Ther. 2020;29(2):702–717. doi:10.1016/j.ymthe.2020.10.008
232. Costello CL, Cohen AD, Patel KK, et al. Phase 1/2 study of the safety and response of P-BCMA-101 CAR-T cells in patients with relapsed/refractory (R/R) multiple myeloma (MM) (PRIME) with novel therapeutic strategies. Blood. 2020;136 Supplement 1:29–30. doi:10.1182/blood-2020-142695
233. Mailankody S, Htut M, Lee KP, et al. JCARH125, anti-BCMA CAR T-cell therapy for relapsed/refractory multiple myeloma: initial proof of concept results from a phase 1/2 multicenter study (EVOLVE). Blood. 2018;132 Supplement 1:957. doi:10.1182/blood-2018-99-113548
234. Colonna L, Navarro G, Devries T, et al. Orvacabtagene autoleucel (orva-cel; JCARH125): a fully human BCMA-targeted second-generation CAR T cell product characterized by a predominant central memory phenotype with high in vitro and In vivo proliferative potential and sustained In vivo persistence. Blood. 2020;136 Supplement 1:957. doi:10.1182/blood-2020-136748
235. Mailankody S, Jakubowiak AJ, Htut M, et al. Orvacabtagene autoleucel (orva-cel), a B-cell maturation antigen (BCMA)-directed CAR T cell therapy for patients (pts) with relapsed/refractory multiple myeloma (RRMM): update of the phase 1/2 EVOLVE study (NCT03430011). J Clin Oncol. 2020;38(15Spplement):8504. doi:10.1200/JCO.2020.38.15_suppl.8504
236. Jiang S, Jin J, Hao S, et al. Low dose of human scFv-derived BCMA-targeted CAR-T cells achieved fast response and high complete remission in patients with relapsed/refractory multiple myeloma. Blood. 2018;132(Supplement 1):960. doi:10.1182/blood-2018-99-113220
237. CARSgen Therapeutics Co. Ltd. CARsgen announces investigational CAR-T therapy CT053 granted RMAT designation by the U.S. FDA for R/R multiple myeloma [press release]. Shanghai, 2019. Available from:https://www.prnewswire.com/news-releases/carsgen-announces-investigational-car-t-therapy-ct053-granted-rmat-designation-by-the-us-fda-for-rr-multiple-myeloma-300945966.html.
238. Kumar SK, Baz RC, Orlowski RZ, et al. Results from Lummicar-2: a phase 1b/2 study of fully human B-cell maturation antigen-specific CAR T cells (CT053) in patients with relapsed and/or refractory multiple myeloma. Blood. 2020;136 Supplement 1:28–29. doi:10.1182/blood-2020-139802
239. Wang D, Wang J, Hu G, et al. A phase 1 study of a novel fully human BCMA-targeting CAR (CT103A) in patients with relapsed/refractory multiple myeloma. Blood. 2021;137(21):2890–2901. doi:10.1182/blood.2020008936
240. Xu J, Melenhorst J. CT103A, a forward step in multiple myeloma immunotherapies. Blood Science. 2021;3(2):59–61. doi:10.1097/BS9.0000000000000068
241. Frigault MJ, O’Donnell E, Raje NS, et al. Phase 1 study of CART-ddBCMA, a CAR-T therapy utilizing a novel synthetic binding domain, for the treatment of subjects with relapsed and refractory multiple myeloma. J Clin Oncol. 2021;1(15Supplement):8015. doi:10.1200/JCO.2021.39.15_suppl.8015
242. An G, Sui WW, Wang TY, et al. An anti-Bcma CAR T-cell therapy (C-CAR088) shows promising safety and efficacy profile in relapsed or refractory multiple myeloma. Blood. 2020;136 Supplement 1:29–30. doi:10.1182/blood-2020-138734
243. Lam N, Trinklein ND, Buelow B, et al. Anti-BCMA chimeric antigen receptors with fully human heavy-chain-only antigen recognition domains. Nat Commun. 2020;11(1):283. doi:10.1038/s41467-019-14119-9
244. Mikkilineni L, Manasanch EE, Vanasse D, et al. Deep and durable remissions of relapsed multiple myeloma on a first-in-humans clinical trial of T cells expressing an anti-B-cell maturation antigen (BCMA) chimeric antigen receptor (CAR) with a fully-human heavy-chain-only antigen recognition domain. Blood. 2020;136(Supplement 1):50–51. doi:10.1182/blood-2020-138839
245. Zah E, Nam E, Bhuvan V, et al. Systematically optimized BCMA/CS1 bispecific CAR-T cells robustly control heterogeneous multiple myeloma. Nat Commun. 2020;11(1):2283. doi:10.1038/s41467-020-16160-5
246. Timmers M, Roex G, Wang Y, et al. Chimeric antigen receptor-modified T cell therapy in multiple myeloma: beyond B cell maturation antigen. Front Immunol. 2019;10:1613. doi:10.3389/fimmu.2019.01613
247. Jindal V, Khoury J, Gupta R, et al. Current status of chimeric antigen receptor T-cell therapy in multiple myeloma. Am J Clin Oncol. 2020;43(5):371–377. doi:10.1097/coc.0000000000000669
248. Huang H, Wu HW, Hu YX. Current advances in chimeric antigen receptor T-cell therapy for refractory/relapsed multiple myeloma. J Zhejiang Univ Sci B. 2020;21(1):29–41. doi:10.1631/jzus.B1900351
249. Li CG, Mei H, Hu Y, et al. A bispecific CAR-T cell therapy targeting BCMA and CD38 for relapsed/refractory multiple myeloma: updated results from a phase 1 dose-climbing trial. Blood. 2019;134 Supplement 1:930. doi:10.1182/blood-2019-130340
250. van der Schans JJ, van de Donk N, Mutis T. Dual targeting to overcome current challenges in multiple myeloma CAR T-cell treatment. Front Oncol. 2020;10:1362. doi:10.3389/fonc.2020.01362
251. Tang F, Lu Y, Ge Y, et al. Infusion of chimeric antigen receptor T cells against dual targets of CD19 and B-cell maturation antigen for the treatment of refractory multiple myeloma. J Int Med Res. 2020;48(1):300060519893496. doi:10.1177/0300060519893496
252. Yan L, Qu S, Shang J, et al. Sequential CD19 and BCMA-specific CAR T-cell treatment elicits sustained remission of relapsed and/or refractory myeloma. Cancer Med. 2021;10:563–574. doi:10.1002/cam4.3624
253. Jiang H, Dong BX, Gao L, et al. Clinical results of a multicenter study of the first-in-human dual BCMA and CD19 targeted novel platform fast CAR-T cell therapy for patients with relapsed/refractory multiple myeloma. Blood. 2020;136 Supplement 1:25–26. doi:10.1182/blood-2020-138614
254. Prommersberger S, Reiser M, Beckmann J, et al. CARAMBA: a first-in-human clinical trial with SLAMF7 CAR-T cells prepared by virus-free Sleeping Beauty gene transfer to treat multiple myeloma. Gene Ther. 2021. doi:10.1038/s41434-021-00254-w
255. Wang X, Walter M, Urak R, et al. Lenalidomide enhances the function of CS1 chimeric antigen receptor-redirected T cells against multiple myeloma. Clin Cancer Res. 2018;24(1):106–119. doi:10.1158/1078-0432.Ccr-17-0344
256. Shah UA, Mailankody S. CAR T and CAR NK cells in multiple myeloma: expanding the targets. Best Pract Res Clin Haematol. 2020;33(1):101141. doi:10.1016/j.beha.2020.101141
257. Rodríguez-Lobato LG, Ganzetti M, Fernández de Larrea C. CAR T-cells in multiple myeloma: state of the art and future directions. Front Oncol. 2020;10:1243. doi:10.3389/fonc.2020.01243
258. Lamb MG, Rangarajan HG, Tullius BP, et al. Natural killer cell therapy for hematologic malignancies: successes, challenges, and the future. Stem Cell Res Ther. 2021;12:1. doi:10.1186/s13287-021-02277-x
259. Rubio MT, Dhuyser A, Nguyen S. Role and modulation of NK cells in multiple myeloma. hemato. 2021;2(2):167–181. doi:10.3390/hemato2020010
260. Shimasaki N, Jain A, Campana D. NK cells for cancer immunotherapy. Nat Rev Drug Discov. 2020;19(3):200–218. doi:10.1038/s41573-019-0052-1
261. Chu J, Deng Y, Benson DM, et al. CS1-specific chimeric antigen receptor (CAR)-engineered natural killer cells enhance in vitro and in vivo antitumor activity against human multiple myeloma. Leukemia. 2014;28(4):917–927. doi:10.1038/leu.2013.279
262. Jiang H, Zhang W, Shang P, et al. Transfection of chimeric anti-CD138 gene enhances natural killer cell activation and killing of multiple myeloma cells. Mol Oncol. 2014;8(2):297–310. doi:10.1016/j.molonc.2013.12.001
263. Sachdeva M, Busser BW, Temburni S, et al. Repurposing endogenous immune pathways to tailor and control chimeric antigen receptor T cell functionality. Nat Commun. 2019;10(1):5100. doi:10.1038/s41467-019-13088-3
264. Sommer C, Bentley T, Sutton J, et al. Off-the-shelf AlloCAR T (TM) cells targeting BCMA for the treatment of multiple myeloma. Clin Lymphoma Myeloma Leuk. 2019;19(10):E24. doi:10.1016/j.clml.2019.09.035
265. Allogene Therapeutics, Inc. Allogene Therapeutics announces FDA Regenerative Medicine Advanced Therapy (RMAT) designation granted to ALLO-715, an AlloCAR T™ cell therapy in development for relapsed/refractory multiple myeloma [press release]. South San Francisco, CA, 2021. Available from:https://www.globenewswire.com/news-release/2021/04/21/2214140/0/en/Allogene-Therapeutics-Announces-FDA-Regenerative-Medicine-Advanced-Therapy-RMAT-Designation-Granted-to-ALLO-715-an-AlloCAR-T-Cell-Therapy-in-Development-for-Relapsed-Refractory-Mul.html.
266. Mailankody S, Matous JV, Liedtke M, et al. Universal: an allogeneic first-in-human study of the anti-Bcma ALLO-715 and the anti-CD52 ALLO-647 in relapsed/refractory multiple myeloma. Blood. 2020;1:24–25. doi:10.1182/blood-2020-140641
267. Tees MT, Neelapu SS, Hari P, et al. Safety and PK/PD of ALLO-647, an anti-CD52 antibody, with fludarabine (flu)/cyclophosphamide (cy) for lymphodepletion in the setting of allogeneic CAR-T cell therapy. J Clin Oncol. 2021;39(15supplement):2527. doi:10.1200/JCO.2021.39.15_suppl.2527
268. Prieto J, Redondo P, Lopez-Mendez B, et al. Understanding the indirect DNA read-out specificity of I-CreI meganuclease. Sci Rep. 2018;8(1):10286. doi:10.1038/s41598-018-28599-0
269. Jurica MS, Monnat RJ, Stoddard BL. DNA recognition and cleavage by the LAGLIDADG homing endonuclease I-CreI. Mol Cell. 1998;2(4):469–476. doi:10.1016/s1097-2765(00)80146-x
270. Precision Biosciences, Inc. Precision BioSciences receives fast track designation from U.S. Food and Drug Administration for PBCAR269A, an investigational allogeneic CAR T therapy for relapsed/refractory multiple myeloma [press release]. Durham, NC, 2020. Available from:https://investor.precisionbiosciences.com/news-releases/news-release-details/precision-biosciences-receives-fast-track-designation-us-food.
271. Da Vià MC, Dietrich O, Truger M, et al. Homozygous BCMA gene deletion in response to anti-BCMA CAR T cells in a patient with multiple myeloma. Nat Med. 2021;27:616–619. doi:10.1038/s41591-021-01245-5
272. Madduri D, Parekh S, Campbell TB, et al. Anti-BCMA CAR T administration in a relapsed and refractory multiple myeloma patient after COVID-19 infection: a case report. J Med Case Rep. 2021;15(1):90. doi:10.1186/s13256-020-02598-0
273. Costa LJ, Lin Y, Martin TG, et al. Cilta-cel versus conventional treatment in patients with relapse/refractory multiple myeloma. Blood. 2021;39(Supplement 15):8030. DOI:10.1200/JCO.2021.39.15_suppl.8030
274. Strohl WR, Naso M. Bispecific T-cell redirection versus chimeric antigen receptor (CAR)-T cells as approaches to kill cancer cells. Antibodies. 2019;8(3):41. doi:10.3390/antib8030041
275. Kennedy LB, Salama AKS. A review of cancer immunotherapy toxicity. CA Cancer J Clin. 2020;70(2):86–104. doi:10.3322/caac.21596
276. Shimabukuro-Vornhagen A, Godel P, Subklewe M, et al. Cytokine release syndrome. J Immunother Cancer. 2018;6(1):56. doi:10.1186/s40425-018-0343-9
277. Yu J, Wang W, Huang H. Efficacy and safety of bispecific T-cell engager (BiTE) antibody blinatumomab for the treatment of relapsed/refractory acute lymphoblastic leukemia and non-Hodgkin’s lymphoma: a systemic review and meta-analysis. Hematology. 2019;24(1):199–207. doi:10.1080/16078454.2018.1549802
278. Aamir S, Anwar MY, Khalid F, et al. Systematic review and meta-analysis of CD19-specific CAR-T cell therapy in relapsed/refractory acute lymphoblastic leukemia in the pediatric and young adult population: safety and efficacy outcomes. Clin Lymphoma Myeloma Leuk. 2021;21(4):E334–E347. doi:10.1016/j.clml.2020.12.010
279. Wang Z, Han W. Biomarkers of cytokine release syndrome and neurotoxicity related to CAR-T cell therapy. Biomarker Research. 2018;6:4. doi:10.1186/s40364-018-0116-0
280. Billiau AD, Roskams T, Van Damme-lombaerts R, et al. Macrophage activation syndrome: characteristic findings on liver biopsy illustrating the key role of activated, IFN-gamma-producing lymphocytes and IL-6- and TNF-alpha-producing macrophages. Blood. 2005;105(4):1648–1651. doi:10.1182/blood-2004-08-2997
281. Mehta P, McAuley DF, Brown M, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033–1034. doi:10.1016/s0140-6736(20)30628-0
282. Felsenstein S, Herbert JA, McNamara PS, et al. COVID-19: immunology and treatment options. Clin Immunol. 2020;215:108448. doi:10.1016/j.clim.2020.108448
283. Soy M, Keser G, Atagündüz P, et al. Cytokine storm in COVID-19: pathogenesis and overview of anti-inflammatory agents used in treatment. Clin Rheumatol. 2020:1–10. doi:10.1007/s10067-020-05190-5.
284. Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020;130(5):2620–2629. doi:10.1172/jci137244
285. U.S. Food and Drug Administration. FDA approves tisagenlecleucel for B-cell ALL and tocilizumab for cytokine release syndrome [press release]. Washington, DC, 2017. Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-tisagenlecleucel-b-cell-all-and-tocilizumab-cytokine-release-syndrome.
286. Neelapu SS. Managing the toxicities of CAR T-cell therapy. Hematol Oncol. 2019;37(Suppl 1):48–52. doi:10.1002/hon.2595
287. Si S, Teachey DT. Spotlight on tocilizumab in the treatment of CAR-T-cell-induced cytokine release syndrome: clinical evidence to date. Ther Clin Risk Manag. 2020;16:705–714. doi:10.2147/tcrm.S223468
288. Freyer CW, Porter DL. Cytokine release syndrome and neurotoxicity following CAR T-cell therapy for hematologic malignancies. J Allergy Clin Immunol. 2020;146(5):940–948. doi:10.1016/j.jaci.2020.07.025
289. Santomasso BD, Park JH, Salloum D, et al. Clinical and biological correlates of neurotoxicity associated with CAR T-cell therapy in patients with B-cell acute lymphoblastic leukemia. Cancer Discov. 2018;8(8):958–971. doi:10.1158/2159-8290.Cd-17-1319
290. Gust J, Hay KA, Hanafi LA, et al. Endothelial activation and blood-brain barrier disruption in neurotoxicity after adoptive immunotherapy with CD19 CAR-T cells. Cancer Discov. 2017;7(12):1404–1419. doi:10.1158/2159-8290.Cd-17-0698
291. Yu S, Yi M, Qin S, et al. Next generation chimeric antigen receptor T cells: safety strategies to overcome toxicity. Mol Cancer. 2019;18(1):125. doi:10.1186/s12943-019-1057-4
292. Griffioen M, van Egmond EH, Kester MG, et al. Retroviral transfer of human CD20 as a suicide gene for adoptive T-cell therapy. Haematologica. 2009;94(9):1316–1320. doi:10.3324/haematol.2008.001677
293. Liu YR, Chen Z, Fang HL, et al. Durable remission achieved from Bcma-directed CAR-T therapy against relapsed or refractory multiple myeloma. Blood. 2018;132(Supplement 1):956. doi:10.1182/blood-2018-99-112786
294. Fu WJ, Du J, Jiang H, et al. Efficacy and safety of CAR-T therapy with safety switch targeting Bcma for patients with relapsed/refractory multiple myeloma in a phase 1 clinical study. Blood. 2019;134 Supplement 1:3154. doi:10.1182/blood-2019-127608
295. Di Stasi A, Tey SK, Dotti G, et al. Inducible apoptosis as a safety switch for adoptive cell therapy. N Engl J Med. 2011;365(18):1673–1683. doi:10.1056/NEJMoa1106152
296. Diaconu I, Ballard B, Zhang M, et al. Inducible caspase-9 selectively modulates the toxicities of CD19-specific chimeric antigen receptor-modified T cells. Mol Ther. 2017;25(3):580–592. doi:10.1016/j.ymthe.2017.01.011
297. Gargett T, Brown MP. The inducible caspase-9 suicide gene system as a “safety switch” to limit on-target, off-tumor toxicities of chimeric antigen receptor T cells. Front Pharmacol. 2014;5:235. doi:10.3389/fphar.2014.00235
298. Moghanloo E, Mollanoori H, Talebi M, et al. Remote controlling of CAR-T cells and toxicity management: molecular switches and next generation CARs. Transl Oncol. 2021;14(6):101070. doi:10.1016/j.tranon.2021.101070
299. Liao D, Wang M, Liao Y, et al. A review of efficacy and safety of checkpoint inhibitor for the treatment of acute myeloid leukemia. Front Pharmacol. 2019;10:609. doi:10.3389/fphar.2019.00609
300. Skarbnik AP, Donato ML, Feinman R, et al. Safety and efficacy of consolidation therapy with ipilimumab plus nivolumab after autologous stem cell transplantation. Transplant Cell Ther. 2021;27(5):391–403. doi:10.1016/j.jtct.2020.12.026
301. Mateos M-V, Orlowski RZ, Siegel DS, et al. Pembrolizumab in combination with lenalidomide and low-dose dexamethasone for relapsed/refractory multiple myeloma (RRMM): final efficacy and safety analysis. J Clin Oncol. 2016;34((15 Supplement):8010). doi:10.1200/JCO.2016.34.15_suppl.8010
302. Pant A, Medikonda R, Lim M. Alternative checkpoints as targets for immunotherapy. Curr Oncol Rep. 2020;22(12):126. doi:10.1007/s11912-020-00983-y
303. Zhang C, Liu Y. Targeting NK cell checkpoint receptors or molecules for cancer immunotherapy. Front Immunol. 2020;11:1295. doi:10.3389/fimmu.2020.01295
304. Sun J, Muz B, Alhallak K, et al. Targeting CD47 as a novel immunotherapy for multiple myeloma. Cancers. 2020;12(2):305. doi:10.3390/cancers12020305
305. Patel K, Maris MB, Cheson BD, et al. Ongoing, first-in-human, phase I dose escalation study of the investigational CD47-blocker TTI-622 in patients with advanced relapsed or refractory lymphoma. J Clin Oncol. 2020;38:15. doi:10.1200/JCO.2020.38.15_suppl.3030
306. Lucas F, Pennell M, Huang Y, et al. T-cell transcriptional profiling and immunophenotyping uncover LAG3 as a potential significant target of immune modulation in multiple myeloma. Biol Blood Marrow Transplant. 2019;26(1):7–15. doi:10.1016/j.bbmt.2019.08.009
307. Guillerey C, Harjunpää H, Carrié N, et al. TIGIT immune checkpoint blockade restores CD8(+) T-cell immunity against multiple myeloma. Blood. 2018;132(16):1689–1694. doi:10.1182/blood-2018-01-825265
308. Asimakopoulos F. TIGIT checkpoint inhibition for myeloma. Blood. 2018;132(16):1629–1630. doi:10.1182/blood-2018-08-864231
309. Harjunpää H, Guillerey C. TIGIT as an emerging immune checkpoint. Clin Exp Immunol. 2020;200(2):108–119. doi:10.1111/cei.13407
310. Alfarra H, Weir J, Grieve S, et al. Targeting NK cell inhibitory receptors for precision multiple myeloma immunotherapy. Front Immunol. 2020;11:575609. doi:10.3389/fimmu.2020.575609
311. Paul B, Symanowski J, Osipoff P, et al. A phase 2 trial of daratumumab and pembrolizumab in refractory multiple myeloma. Blood. 2020;136 Supplement 1:2. doi:10.1182/blood-2020-141623
312. Cho HJ, Costa LJ, Davies FE, et al. Atezolizumab in combination with daratumumab with or without lenalidomide or pomalidomide: a phase Ib study in patients with multiple myeloma. Blood. 2018;132:3. doi:10.1182/blood-2018-99-114960
313. Branagan A, Lei M, Lou U, et al. Current treatment strategies for multiple myeloma. JCO Oncol Pract. 2020;16(1):5–14. doi:10.1200/jop.19.00244
314. Cohen AD, Garfall AL, Stadtmauer EA, et al. B cell maturation antigen-specific CAR T cells are clinically active in multiple myeloma. J Clin Invest. 2019;129(6):2210–2221. doi:10.1172/jci126397
315. Cohen AD, Garfall AL, Stadtmauer EA, et al. Safety and efficacy of B-cell maturation antigen (BCMA)-specific chimeric antigen receptor T cells (CART-BCMA) with cyclophosphamide conditioning for refractory multiple myeloma (MM). Blood. 2017;130(Supplement 1):505. doi:10.1182/blood.V130.Suppl_1.505.505
316. Green DJ, Pont M, Sather BD, et al. Fully human BCMA targeted chimeric antigen receptor T cells administered in a defined composition demonstrate potency at low doses in advanced stage high risk multiple myeloma. Blood. 2018;132(Supplement 1):1011. doi:10.1182/blood-2018-99-117729
317. Hamieh M, Dobrin A, Cabriolu A, et al. CAR T cell trogocytosis and cooperative killing regulate tumour antigen escape. Nature. 2019;568:112–116. doi:10.1038/s41586-019-1054-1
318. Simoes RD, Shirasaki R, Downey-Kopyscinski SL, et al. Systematic characterization of genes representing preferential molecular vulnerabilities for myeloma cells compared to other neoplasias - implications for the biology and therapeutic targeting of myeloma. Blood. 2019;134(Supplement 1):4407. doi:10.1182/blood-2019-130901
319. Smith EL, Harrington K, Staehr M, et al. GPRC5D is a target for the immunotherapy of multiple myeloma with rationally designed CAR T cells. Sci Transl Med. 2019;11:485. doi:10.1126/scitranslmed.aau7746
320. Atamaniuk J, Gleiss A, Porpaczy E, et al. Overexpression of G protein-coupled receptor 5D in the bone marrow is associated with poor prognosis in patients with multiple myeloma. Eur J Clin Invest. 2012;42(9):953–960. doi:10.1111/j.1365-2362.2012.02679.x
321. Bonello F, Grasso M, D’Agostino M, et al. The role of monoclonal antibodies in the first-line treatment of transplant-ineligible patients with newly diagnosed multiple myeloma. Pharmaceuticals. 2020;14(1):20. doi:10.3390/ph14010020
322. Holthof LC, Mutis T. Challenges for immunotherapy in multiple myeloma: bone marrow microenvironment-mediated immune suppression and immune resistance. Cancers. 2020;12(4):988. doi:10.3390/cancers12040988
323. Kostopoulos IV, Ntanasis-Stathopoulos I, Gavriatopoulou M, et al. Minimal residual disease in multiple myeloma: current landscape and future applications with immunotherapeutic approaches. Front Oncol. 2020;10:860. doi:10.3389/fonc.2020.00860
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.