Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Immunological Response During HAART and Determinants of Current CD4+ T-Cell Count Among HIV/AIDS Patients Attending University of Gondar Referral Hospital, Northwest Ethiopia
Authors Manaye GA ![]() , Abateneh DD
, Abateneh DD ![]() , Kebede KM
, Kebede KM ![]() , Belay AS
, Belay AS ![]()
Received 2 April 2020
Accepted for publication 12 July 2020
Published 31 July 2020 Volume 2020:12 Pages 295—306
DOI https://doi.org/10.2147/HIV.S255751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Gizachew Ayele Manaye,1 Dejene Derseh Abateneh,1,2 Kindie Mitiku Kebede,1 Alemayehu Sayih Belay1
1Mizan Tepi University, College of Health Sciences, Mizan Tefri, Ethiopia; 2Kotebe Metropolitan University, Menelik II College of Medicine and Health Sciences, Addis Ababa, Ethiopia
Correspondence: Dejene Derseh Abateneh
Kotebe Metropolitan University, Menelik II College of Medicine and Health Sciences Department of Medical Laboratory Sciences, P.O. Box: 3268, Addis Ababa, Ethiopia
Tel +251920514158
Email [email protected]
Purpose: After the initiation of highly active antiretroviral therapy (HAART), successful HAART is characterized by an increase in the CD4+ count. Several factors affect the CD4+ T-cell count. This study aimed to assess the immunological response during HAART and determinants of the current CD4+ T-cell count among HIV/AIDS patients on HAART.
Patients and Methods: A hospital-based cross-sectional study was conducted from February 1 to April 1, 2017. A total of 423 HIV/AIDS patients on HAART were enrolled using simple random sampling. Descriptive statistics, and bivariate and multiple regression analyses were conducted. Variables with p-value < 0.2 in the bivariate analysis were entered in the multiple regression models. p-Values < 0.05 and 95% confidence intervals were used to identify determinants of the current CD4+ T-cell count.
Results: The mean CD4+ T-cell count gradually increased until 8 years on HAART but declined thereafter. An increased current CD4+ T-cell count was observed among patients with an initial regimen of pediatric d4T-3TC-NVP [β=185.5, 95% CI (8.8, 362.2)] (p=0.040), with increased baseline CD4+ T-cell count [β=0.468, 95% CI (0.342, 0.594)] (p< 0.0001), and with long duration on HAART [β=18.0, 95% CI (9.9, 26.1)] (p< 0.0001), whereas a decreased level of current CD4+ T-cell count was observed among males [β=− 72.7, 95% CI (− 114.5, – 30.9)]) (p< 0.0001) and those with poor baseline adherence [β=− 108.9, 95% CI (− 210.9, − 7.0)] (p=0.036) and viral load > 1000 copies [β=− 189.2, 95% CI (− 243.5, − 134.9)] (p< 0.0001).
Conclusion: The trend in immunological response was not increased linearly throughout the HAART duration. Sex, type of initial regimen, baseline adherence, baseline CD4+ count, viral load, and duration on HAART were independent determinants of current CD4+ count. These determinants could be addressed by regular monitoring of HIV patients on HAART, and special attention should be paid to male patients.
Keywords: immunological responses, trends, current CD4+ count, HIV/AIDS, HAART
Introduction
Highly active antiretroviral therapy (HAART) helps to reduce the morbidity and mortality rates associated with human immunodeficiency virus (HIV) infection by decreasing the viral ribonucleic acid (RNA) concentration below detection levels and allowing immune restoration.1,2 The CD4+ T-cell count has been used to assess the urgency of HAART initiation and the need for opportunistic infection prophylaxis, and to provide information regarding the magnitude of immune reconstitution.3 Different studies have shown that the immunological response (measured by CD4+ T-cell count) increases as the duration on HAART increases.4–6 After the initiation of HAART, a successful HAART is characterized by a quicker response during the first 3 months, which gradually increases as the duration on HAART increases.7,8
The CD4+ T-cell count and HIV viral load are routinely used prognostic tests for patients on HAART. Studies have shown that these two prognostic tests have an inverse relationship. After the initiation of HAART drugs, the viral load increases.9,10 In addition to viral load, the baseline CD4+ T-cell count also determines the immunological decrease in CD4+ cell response. There are controversial findings related to the correlation between the baseline CD4+ T-cell count and the current CD4+ T-cell count. Some studies show a positive correlation,11,12 whereas other studies indicate a negative correlation.13–15 Furthermore, sex,13,16,17 baseline adherence,18,19 duration on HAART,4,5 advanced WHO clinical stage, and treatment interruption also determine the level of current CD4+ T-cell count.12
Trends in the immunological response and the factors contributing to the current CD4+ T-cell count vart from one setting to another. Studies on the trends in immunological response and determinants of current CD4+ T-cell count are scarce in Ethiopia. Most available studies in Ethiopia are focused on immunological failure, which is defined as the decline in CD4 cells by 50% from their peak value, or persistently <100 cells/mm3, or a fall in CD4 counts below the baseline count.11-13,20-22 To the investigators’ knowledge, no studies have been conducted on the trends in immunological response and determinants of current CD4+ T-cell count using more advanced regression analysis in this study area. Furthermore, most of the previous studies on immunological response in Ethiopia did not control for the confounding effect of viral load, as viral load testing was only introduced in Ethiopia after the end of 2016. Therefore, this study aimed to assess the trends in immunological response and determinants of the current CD4+ T-cell count using a more advanced regression analysis and controlling the confounding effects of viral load. Up-to-date information on immunological response and determinants of the current CD4+ T-cell count is important for understanding the immunological response to treatment outcome, regimen change, and patient management. This may, in turn, provide valuable inputs to achieve the ambitious 90–90-90 plan to end the AIDS epidemic by 2030.23
Patients and Methods
Study Area and Period
The study was conducted at the University of Gondar Referral Hospital (UOGRH) from February 1 to April 1, 2017. The hospital is located 747 km from the capital city of Ethiopia, Addis Ababa. According to the recent administration, the town has 12 sub-cities, which consist of 21 kebeles (the smallest administrative unit in Ethiopia). According to the 2007 central statistical agency report, Gondar town has an estimated population of more than 206,987.24 The town has one teaching referral hospital, eight health centers, and 15 private clinics. At the time of the study, there were a total of 13,753 HIV patients; of these, 5389 patients were on HAART.
We followed the methods of Ayele et al for the identification of eligible study participants, data collection, specimen collection, and analysis.25
Study Design and Study Population
A hospital-based cross-sectional study design supported by a retrospective record review was conducted among adult HIV/AIDS patients on HAART.
Inclusion and Exclusion Criteria
All adult HIV patients on HAART whose age was greater than 18 years old, had a baseline CD4+ T-cell count, and had at least 6 months’ follow-up on HAART were included in the study. Those patients who had been seriously sick and were unable to respond and give blood specimens, or who had incomplete secondary data records, especially for laboratory and clinical data such as baseline CD4+ T-cell count, were excluded from the study.
Operational Definitions
In the current study, “baseline data” refers to the data before the initiation of HAART and “current CD4+ T-cell count” refers to the CD4+ T-cell count during the data collection time. Adherence was calculated using  . We considered good adherence if >95%, fair adherence if 85–95%, and poor adherence if <85% of doses were taken.26,27
. We considered good adherence if >95%, fair adherence if 85–95%, and poor adherence if <85% of doses were taken.26,27
Study Variables
In this study, the level of current CD4+ T-cell count was considered as a dependent variable and treated as a continuous variable. The independent variables included age, marital status, sex, residence, religion, education, occupation, WHO clinical stage, HIV/AIDS co-infection, baseline CD4+ T-cell count, regimen type, duration on HAART, viral load, and adherence.
Sample Size Determination and Sampling Techniques
A single population proportion formula (n=(Zα/2)2 p(1–p)/d2) was used to estimate the sample size. The following assumptions were considered when calculating the sample size: margin of error d=0.05, Zα/2=1.96, P=population proportion (estimated prevalence)=0.5, and 95% confidence interval. After adding a 10% non-response rate, the final sample size was 423 participants. A systematic random sampling technique was used to select study participants. There was an average of 20 HIV/AIDS patients per day under follow-up in the antiretroviral therapy (ART) clinic who gave a blood sample for viral load and CD4+ T-cell count concurrently. During the 3-month data collection period, 1320 HIV/AIDS patients were expected to visit the hospital for viral load and CD4+ T-cell count follow-up. The sampling interval (K) value was calculated by dividing the total number of HIV/AIDS patients during our study period by the sample size (1320/423=3.12=3). To determine the first participant, the lottery method was used among the first three patients and every third interval participant was selected (Figure 1).
 |
Figure 1 Schematic representation of the sampling procedure of HIV-positive adults on HAART at University of Gondar Referral Hospital from February to April 2017. |
Data Collection and Laboratory Methods
Sociodemographic characteristics, including age, gender, occupation, residence, marital status, religion, and educational status, were collected from each study participant using a structured questionnaire developed from the literature.21,28 Relevant clinical characteristics of participants (weight, WHO clinical stage, CD4+ T-cell count, HAART regimen, adherence with and duration on HAART, initial regimen, types of co-infections, adverse effects, and reason for drug switching) were retrieved from medical records by trained nurses using a data extraction checklist (S1 file).
For CD4+ T-cell count and viral load tests, 3–5 mL of whole blood was drawn from each participant using Vacutainer tubes, separately in two tubes containing ethylene diamine tetra-acetic acid (EDTA) following standard blood collection procedures. After centrifugation (3000 rpm for 20 minutes), plasma was separated and aliquots were prepared for viral load testing. Collected specimens were labeled and immediately transported to the Gondar Hospital laboratory. The CD4+ T-cell count specimens were stored at room temperature and processed within 24 hours. For viral load testing, plasma was separated within 5 hours and two aliquots of cryo-vials (with a capacity of 1 mL each) were prepared for transportation. The specimens were transported on dry ice and stored at −80°C until processing. Centrifugation, pipetting, and aliquoting were performed following standard protocol and laboratory biosafety precautions at both the collection and testing sites.
Quantification of absolute CD4+ T-cell count on whole blood specimens was performed using the BD FACSCalibur flow cytometry system (BD, CA, USA) following the standard operational procedures in the laboratory. The CD4+ T-cell count was carried out by adding 50 µL whole blood to a reagent tube containing 20 µL of monoclonal antibodies, followed by vortexing and incubation for 30 minutes under dark conditions. Plasma viral load was measured using a quantitative real-time PCR HIV-1 assay, with the COBAS® AmpliPrep instrument (Roche, Homburg, Germany). Plasma was prepared from 5 mL of blood by centrifugation at 3000 rpm for 20 minutes.
Data Analysis
The data were entered, cleaned, checked for completeness, and analyzed using SPSS version 21. Descriptive statistics, and bivariate and multiple regression analyses were conducted. Before applying the multiple regression models, all the assumptions were assessed. Variables with p-value <0.2 in the bivariate analysis were entered in the multiple regression model. p-Values <0.05 and 95% confidence intervals were used to determine the independent factors associated with the current CD4+ T-cell count.
Results
Sociodemographic Characteristics of Participants
A total of 423 HIV/AIDS participants who received HAART were enrolled in the study. Of these, 272 (64.3%) were female and 151 (35.7%) were male. The mean±SD age of the participants was 39±9.8 years (range 18–78 years). The mean weight of participants at the baseline and at the time of the study (current) was 50 kg and 56 kg, respectively. At the time of the study, almost half of the participants, 209 (49.4%), were married, 343 (81.1%) were urban inhabitants, and 386 (91.6%) were Orthodox Christians (Table 1).
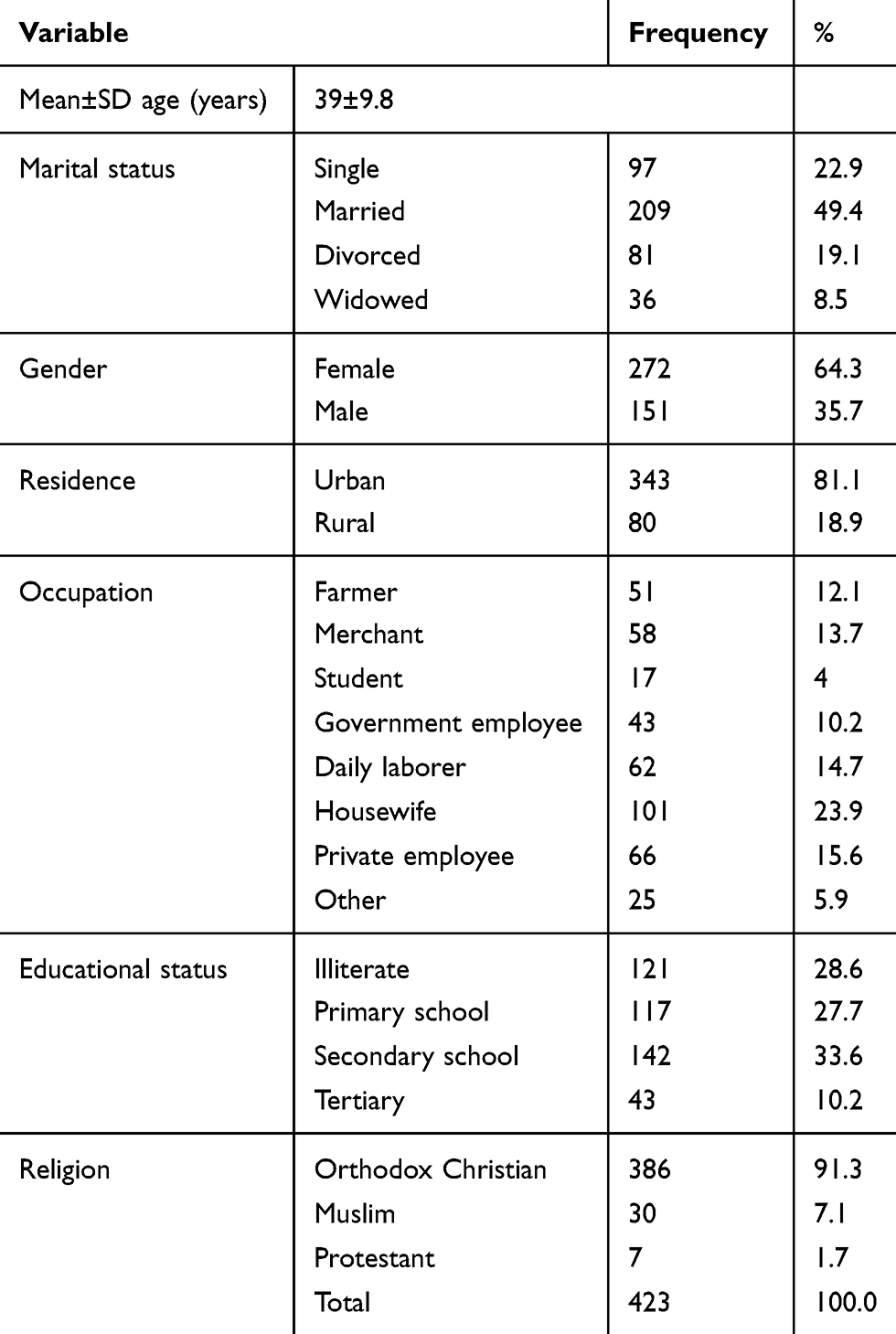 |
Table 1 Sociodemographic Characteristics of HIV/AIDS Patients on HAART in University of Gondar Referral Hospital, 2017 |
Clinical Characteristics of Participants
The study patients were on HAART for a minimum of 6 months up to 12 years, with an average duration of 7(3 years. At baseline, most of the participants, 269 (63.6%), had WHO clinical stage III and IV disease, 267 (63.1%) had a CD4+ T-cell count <200 cells/mm3, 408 (96.5%) had good adherence, 156 (36.9%) were on a regimen of AZT+3TC+NVP, and 87 (20.6%) were on TDF+3TC+EFV. At the time of data collection, 420 (99.1%) had WHO clinical stage I and II disease, 44 (10.4%) had a CD4+ T-cell count <200 cells/mm3, 420 (99.3%) had good adherence, and 162 (38.2%) had switched, to either a first-line regimen, 150 (35.5%), or a second-line regimen, 12 (2.8%) (Table 2).
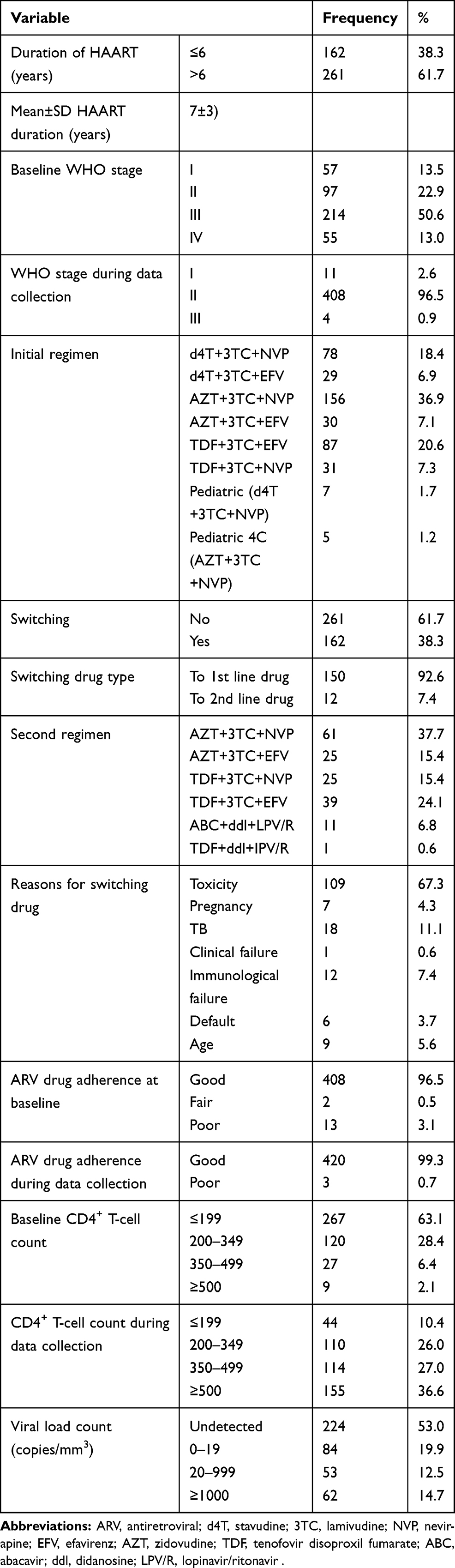 |
Table 2 Clinical Characteristics of HIV/AIDS Patients on HAART in University of Gondar Referral Hospital 2017 |
Trends in Immunological Response
The mean CD4+ T-cell count gradually increased from baseline to 8 years on HAART (from 184 to 493 cells/mm3). However, the mean CD4+ T-cell count slightly declined 8 years after HAART initiation (464 cells/mm3) (Figure 2).
 |
Figure 2 Trend in CD4+ T-cell count at baseline, 6 months, and 1, 4, 8, and 12 years in HIV/AIDS patients on HAART at the University of Gondar Referral Hospital 2017. |
Correlation Between Current Virological and Immunological Status
Using paired sample t-test analysis, baseline CD4+ T-cell count and CD4+ T-cell count at the time of data collection were positively correlated (r=0.285, p<0.0001) (Figure 3). Furthermore, a Pearson’s correlation revealed that there was weak negative correlation between current CD4+ T-cell count and viral load (r=−0.243, p<0.0001) (Figure 4).
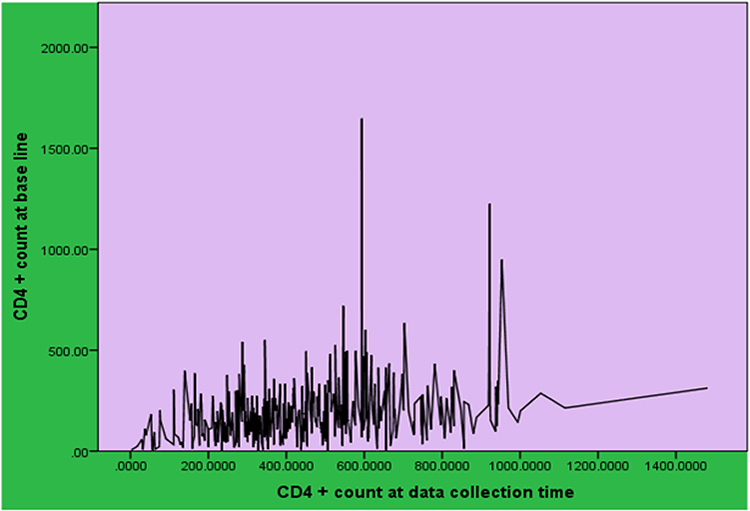 |
Figure 3 Correlation between baseline CD4+ T-cell count and current CD4+ T-cell count in HIV/AIDS patients on HAART at the University of Gondar Referral Hospital 2017. |
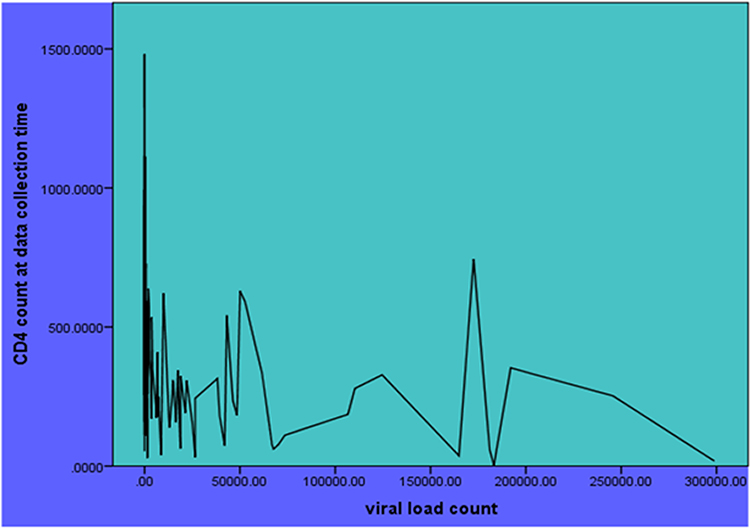 |
Figure 4 Correlation between current CD4+ T-cell count and viral load in HIV/AIDS patients on HAART at the University of Gondar Referral Hospital 2017. |
Bivariate Regression Analysis Results
Without controlling potential confounding, sex, occupation, type of initial HAART regimen, duration on HAART, baseline adherence, baseline CD4+ T-cell count and viral load, and duration on HAART were significantly associated with current CD4+ T-cell count (p<0.05). However, age, marital status, residence, educational status, baseline WHO stage, opportunistic infections, switching of drug regimens, current adherence, baseline weight, current weight, and type of second regimens were not significantly associated with the current CD4+ T-cell count (p>0.05). Variables with p-value <0.2 were included in the multiple regression models.
Multiple Regression Analysis Results
The multiple regression analysis showed that 32.8% of the variation in CD4+ T-cell count was explained by our model (R2=0.328, p<0.0001). The assumption of a linear relationship between the continuous independent variables and current CD4+ T-cell count was met. Analysis of collinearity statistics showed that there were no variables with a variance inflation factor of greater than 10 and tolerance scores above 0.2. The Durbin–Watson statistic showed that the values of the residuals were independent (Durbin–Watson=1.81). The plot of standardized residuals versus standardized predicted values showed no obvious signs of funneling, suggesting that the assumption of homoscedasticity had been met. In addition, the normal P-P plot suggested that the assumption of values of the residuals being normally distributed may have been violated. However, the deviations from normality were not extreme and are not likely to have a significant impact on our findings. Therefore, the results are still valid. Finally, Cook’s distance values were all under 1, suggesting that individual cases were not improperly influencing the model. After applying the multiple regression models, occupation and type of second-line HAART regimens were not significantly associated with the current CD4+ T-cell count. The other variables (sex, type of initial HAART regimen, duration on HAART, baseline adherence, baseline CD4+ T-cell count, and viral load) remained significantly associated with current CD4+ T-cell count.
Keeping other independent variables constant, for each cell/mm3 of blood increment in the baseline CD4+ T-cell count, the current CD4+ T-cell count increased by 0.468 cells/mm3 of blood (p<0.0001). For every additional one-year stay on HAART, the current CD4+ T-cell count increased by 18.02 cells/mm3 of blood (p<0.0001). Males’ current CD4+ T-cell count was lower than females’, by 72.73 cells/mm3 of blood (p<0.0001). Similarly, the current CD4+ T-cell count of HIV patients who took the initial HAART regimen type pediatric d4T-3TC-NVP was higher by 185.5 cells/mm3 of blood compared to others (p=0.040). Furthermore, the current CD4+ T-cell count of HIV patients with poor adherence was less than those with good adherence by 108.93 cells/mm3 of blood (p=0.036). Lastly, current CD4+ T-cell count among HIV patients with ≥1000 copies/mm3 of viral load was lower than in those with an undetectable viral load by 189.17 copies/mm3 (p<0.0001) (Table 3).
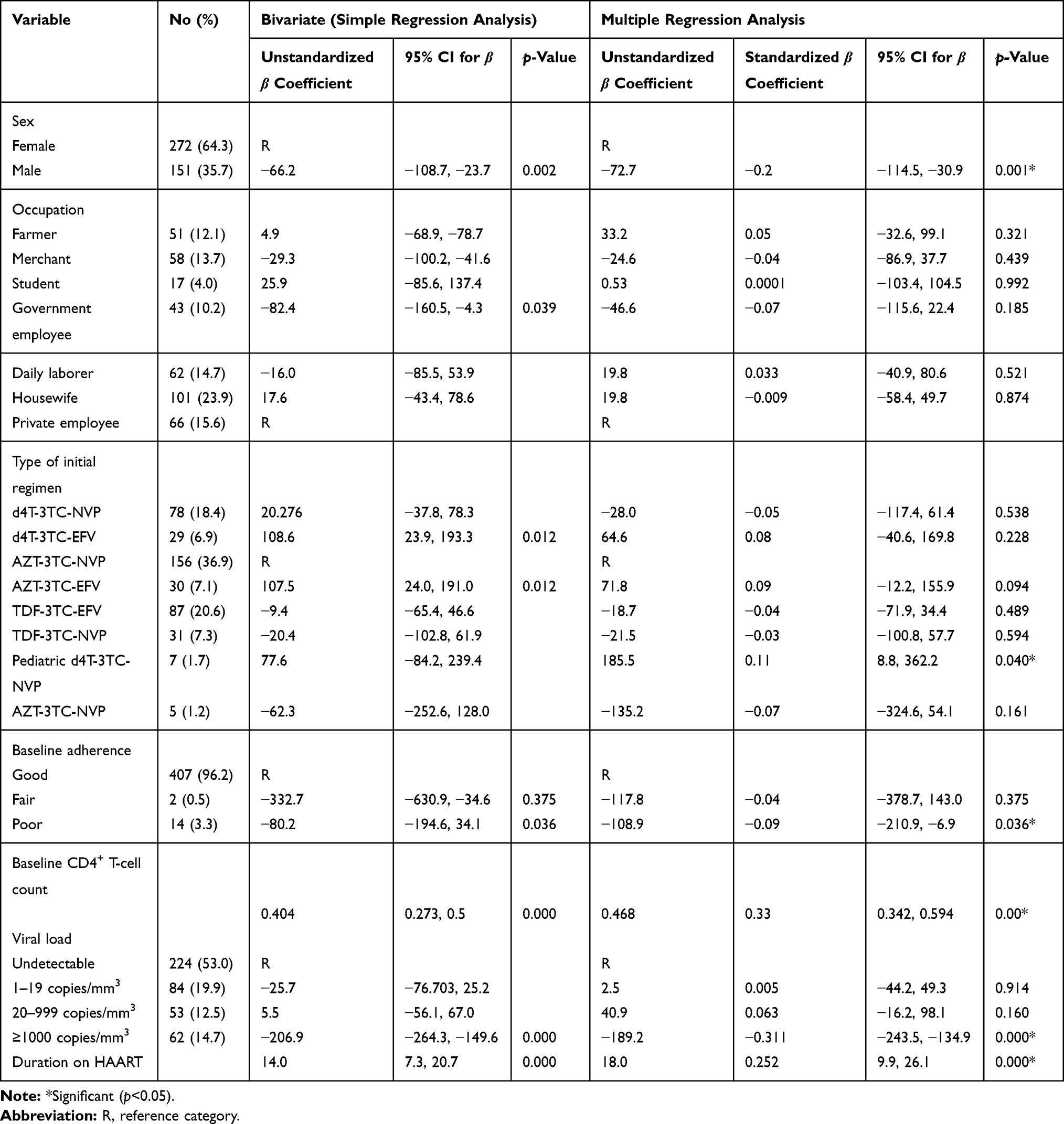 |
Table 3 Bivariate and Multiple Regression Analysis Results of HIV/AIDS Patients on HAART Attending University of Gondar Referral Hospital, Northwest Ethiopia, 2017 |
Discussion
In this study, the trend in the immunological response comprised an increase until 8 years on HAART and then a aslight decrease after 8 years. The trends in the immunological response observed in this study were similar to other study findings in Ethiopia22,29 and Ghana.30 The large increases in the CD4+ T-cell count until 8 years on HAART may be due to immune reconstitution and redistribution of CD4 T-cells that are sequestered from the lymphoid tissues into the circulating blood. The reduction in CD4+ T-cell count after 8 years on HAART in our study may be due to two factors: 1) natural aging leads to a long-term decline in the immune system (CD4+ T-cell count through low-grade chronic immune activation); and 2) long-term HIV infection despite viral suppression from combined antiretroviral therapy (cART) may accelerate the body’s natural aging trajectory, primarily as a result of persistent immune activation and cART-induced pro-inflammatory effects leading to premature immunosenescence.31
In this study, there was a positive correlation between baseline and current CD4+ T-cell count. This result was in line with research conducted in southern India.32–34 The lower the CD4+ T-cell count at baseline, the less probable it is that the patient will normalize and convalesce completely,35,37 and the greater the CD4+ T-cell count at baseline, the more possible it is for them to normalize and convalesce completely. For instance, many individuals who initiate treatment with a CD4+ T-cell count <350 cells/mm3 never attain a CD4+ T-cell count of >500 cells/mm3, even with up to 10 years on HAART.38,39 Some studies showed that HIV patients who started HAART with a lower CD4+ T-cell count have a shorter life expectancy than those starting at higher CD4+ T-cell counts.38–40 As expected, a negative correlation between the current CD4+ T-cell count and viral load was observed. This agrees with studies conducted in Rwanda and the USA.41–43
The reconstitution of the immune system through viral suppression and increased CD4+ T-cell count is the goal of HAART. However, attaining the target immune response to HAART is affected by several factors. In the current study, sex was an independent predictor of the current CD4+ T-cell count. Compared with female HIV patients, male HIV patients on HAART showed a decreased current CD4+ count. This result is in line with study findings in Nigeria,17 Northern Ethiopia,13 and China,16 and in a multicenter study conducted in low-income countries.44 The increased CD4+ T-cell count among females could be explained by the fact that females may have more access to expanded routine HIV testing in antenatal care during pregnancy and thus they may be linked to ART facilities early on. Females are more likely to be diagnosed with HIV infection earlier than males.45,46 Early diagnoses may lead to early initiation of HAART. This may, in turn, improve the immunological response.47 On the other hand, health-seeking behavior of males is poor, which may result in lower rates of screening for HIV, lower acceptance of screening results, and less linkage to ART facilities after a HIV-positive diagnosis.48,49 A delay in the diagnosis of HIV and failure to initiate HAART early favor a poor response to HAART.50
In the current study, poor baseline adherence to HAART was significantly associated with a decreased current CD4+ T-cell count. Study findings in resource-limited settings18 and a study conducted in Uganda and Zimbabwe19 showed that poor first-year adherence to HAART exposes the patient to a higher risk of immunological failure.
In addition to poor baseline adherence, baseline CD4+ T-cell count was found to be a significant predictor of current CD4+ T-cell count. This finding is in line with previous studies conducted in Ethiopia, where HAART initiated at higher CD4+ T-cell count had positive effects on the immunological response.11,12,20 Furthermore, in this study, the current CD4+ T-cell count was increased as the duration of HAART increased. Similar results were reported from studies in Cameroon and China, in which the CD4+ T-cell count continually increased along with HAART duration, even a long time after HAART initiation.4,5
Finally, the current study indicates that patients with an initial regimen of first-line drugs, specifically d4T-3TC-NVP, showed a significantly increased current CD4+ T-cell count compared to those patients who started with an initial regimen of TDF-3TC-EFV. d4T-3TC-NVP used to be given to children before this combination was banned. In the current study, the age of study participants who were started with the initial regimen d4T-3TC-NVP was <18 years. It is known that children have a high baseline CD4+ T-cell count physiologically. Therefore, an increased current CD4+ T-cell count among patients with initial regimen of d4T-3TC-NVP may be due to those participants having been children at the baseline. However, a further study is needed to ascertain this claim.
This study has some limitations. First, baseline values for viral load were not tested because of the unavailability of viral load testing facilities in Ethiopia before 2017. Second, we could not control the confounding effect of drug resistance on HIV strains because of the unavailability of drug resistance testing facilities. In addition, the impact of survival bias was not assessed. As this study was conducted in only one referral hospital, it may not reflect the trends in immunological response and determinants of current CD4+ T-cell count in the wider community. Despite these limitations, the findings of this study may provide insights into the trends in the immunological response after initiation of HAART and determinants of the current CD4+ T-cell count.
Conclusions
The trend in immunological response did not increase linearly throughout the HAART duration. Sex, type of initial regimen, baseline adherence, baseline CD4+ T-cell count, viral load, and duration on HAART were independent determinants of current CD4+ T-cell count. These determinants could be addressed by regular monitoring of HIV patients on HAART using both virological and immunological tests. During monitoring, special attention needs to be paid to males. Further studies need to be conducted in a wider community and at multiple ART centers to determine whether there are differences in immunological response and associated factors of current CD4+ T-cell count in different set-ups.
Abbreviations
ABC, abacavir; AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; ARV, antiretroviral; AZT, zidovudine; CD4, cluster of differentiation; d4T, stavudine; ddl, didanosine; EFV, efavirenz; HAART, highly active antiretroviral therapy; HIV, human immunodeficiency virus; LPV/R, lopinavir/ritonavir; NVP, nevirapine; RNA, ribonucleic acid; 3TC, lamivudine; TDF, tenofovir disoproxil fumarate; UOGRH, University of Gondar Referral Hospital.
Data Sharing Statement
All the data (SPSS) sets generated and/or analyzed in this study are available from the corresponding author on reasonable request ([email protected]).
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki after ethical clearance was obtained from the University of Gondar, School of Biomedical and Laboratory Sciences Ethical Review Committee, and an official letter was submitted to University of Gondar Referral Hospital administration prior to data collection with Ref. No. SBMLS/678/09. Written informed consent was obtained from each study participant after explaining the purpose and objective of the study. Patients who were not willing to participate in the study were not forced to participate. All the data and samples obtained from them were kept confidential by using codes instead of any personal identifiers and meant only for the purpose of the study. The laboratory results from the study participants were communicated to their physicians for appropriate management.
Acknowledgments
We would like to thank the Department of Medical Microbiology School of Biomedical and Laboratory Science, College of Medicine and Health Science, and University of Gondar for giving us the chance to conduct this research.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they do not have any conflicts of interest.
References
1. Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science. 1997;277(5322):112–116. doi:10.1126/science.277.5322.112
2. Volberding PA, Deeks SG. Antiretroviral therapy and management of HIV infection. Lancet. 2010;376(9734):49–62. doi:10.1016/S0140-6736(10)60676-9
3. Masur H, Brooks JT, Benson CA, Holmes KK, Pau AK, Kaplan JE. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: updated guidelines from the centers for disease control and prevention, National Institutes of Health, and HIV medicine association of the infectious diseases society of America. Clin Infect Dis. 2014;58(9):1308–1311. doi:10.1093/cid/ciu094
4. Fokam J, Billong SC, Jogue F, et al. Immuno-virological response and associated factors amongst HIV-1 vertically infected adolescents in Yaounde-Cameroon. PLoS One. 2017;12(11):e0187566. doi:10.1371/journal.pone.0187566
5. He L, Pan X, Dou Z, et al. The factors related to CD4+ T-cell recovery and viral suppression in patients who have low CD4+ T cell counts at the initiation of HAART: a retrospective study of the national HIV treatment sub-database of Zhejiang Province, China, 2014. PLoS One. 2016;11(2):e0148915. doi:10.1371/journal.pone.0148915
6. Casotti JA, Passos LN, Oliveira FJ, Cerutti C. Factors associated with paradoxical immune response to antiretroviral therapy in HIV infected patients: a case-control study. BMC Infect Dis. 2011;11(1):306. doi:10.1186/1471-2334-11-306
7. French experts group’s recommendations for medical management of hiv infection: highlights and recommendations; 2008. Available from: https://solidarites-sante.gouv.fr/IMG/pdf/synthese_rapport_yeni_version_anglaise.pdf. Accessed July 14, 2020.
8. Bartlett J. Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department Health Human Services Panel on Antiretroviral Guidelines Adult Adolescents. 2008;42–43.
9. Mendoza Y, Mewa JC, Martínez AA, et al. HIV-1 antiretroviral drug resistance mutations in treatment-naive and experienced Panamanian subjects: impact on the national use of EFV-based schemes. PLoS One. 2016;11(4):e0154317. doi:10.1371/journal.pone.0154317
10. Meintjes G, Maartens G. Guidelines for antiretroviral therapy in adults. South Afr J HIV Med. 2012;13(3):114–133. doi:10.4102/sajhivmed.v13i3.125
11. Gezie LD. Predictors of CD4 count over time among HIV patients initiated ART in Felege Hiwot Referral Hospital, northwest Ethiopia: multilevel analysis. BMC Res Notes. 2016;9(1):377. doi:10.1186/s13104-016-2182-4
12. Kokeb M, Degu G. Immunological response of HIV-infected children to highly active antiretroviral therapy at Gondar university hospital, north-western Ethiopia. Ethiop J Health Sci. 2016;26(1):25–30. doi:10.4314/ejhs.v26i1.6
13. Asfaw A, Ali D, Eticha T, Alemayehu A, Alemayehu M, Kindeya F. CD4 cell count trends after commencement of antiretroviral therapy among HIV-infected patients in Tigray, Northern Ethiopia: a retrospective cross-sectional study. PLoS One. 2015;10(3):e0122583. doi:10.1371/journal.pone.0122583
14. Lawn SD, Myer L, Bekker L-G, Wood R. CD4 cell count recovery among HIV-infected patients with very advanced immunodeficiency commencing antiretroviral treatment in sub-Saharan Africa. BMC Infect Dis. 2006;6(1):59. doi:10.1186/1471-2334-6-59
15. Smith CJ, Sabin CA, Youle MS, et al. Factors influencing increases in CD4 cell counts of HIV-positive persons receiving long-term highly active antiretroviral therapy. J Infect Dis. 2004;190(10):1860–1868. doi:10.1086/425075
16. Dou Z, Xu J, Jiao JH, et al. Gender difference in 2-year mortality and immunological response to ART in an HIV-infected Chinese population, 2006–2008. PLoS One. 2011;6(8):e22707. doi:10.1371/journal.pone.0022707
17. Anude CJ, Eze E, Onyegbutulem HC, et al. Abimiku Al: immuno-virologic outcomes and immuno-virologic discordance among adults alive and on antiretroviral therapy at 12 months in Nigeria. BMC Infect Dis. 2013;13(1):113. doi:10.1186/1471-2334-13-113
18. Abrogoua DP, Kablan BJ, Kamenan BAT, Aulagner G, N’Guessan K, Zohoré C. Assessment of the impact of adherence and other predictors during HAART on various CD4 cell responses in resource-limited settings. Patient Prefer Adherence. 2012;6:227. doi:10.2147/PPA.S26507
19. Kiwuwa MS, Walker AS, Oja H, et al., DART Trial Team. The impact of first-year adherence to antiretroviral therapy on long‐term clinical and immunological outcomes in the DART trial in Uganda and Zimbabwe. Tropical Med Int Health. 2012;17(5):584–594. doi:10.1111/j.1365-3156.2012.02974.x
20. Teshome W, Assefa A. Predictors of immunological failure of antiretroviral therapy among HIV infected patients in Ethiopia: a matched case-control study. PLoS One. 2014;9(12):e115125. doi:10.1371/journal.pone.0115125
21. Ayalew MB, Kumilachew D, Belay A, et al. First-line antiretroviral treatment failure and associated factors in HIV patients at the University of Gondar Teaching Hospital, Gondar, Northwest Ethiopia. HIV/AIDS. 2016;8:141.
22. Yirdaw KD, Hattingh S. Prevalence and predictors of immunological failure among HIV patients on HAART in southern Ethiopia. PLoS One. 2015;10(5):e0125826. doi:10.1371/journal.pone.0125826
23. 90-90-90 An ambitious treatment target to help end the AIDS epidemic. Geneva Switzerland. Available from: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf.
24. Population and housing census 2007 report, Amhara, Part I: population size and characteristics. Available from: http://microdata.worldbank.org/index.php/catalog/2747/download/39220.
25. Ayele G, Tessema B, Amsalu A, Ferede G, Yismaw G. Prevalence and associated factors of treatment failure among HIV/AIDS patients on HAART attending University of Gondar Referral Hospital Northwest Ethiopia. BMC Immunol. 2018;19(1):37. doi:10.1186/s12865-018-0278-4
26. National guidelines on second-line ART for adults and adolescents India: department of AIDS control national AIDS control organization ministry of health & family welfare Government of India. Available from: http://naco.gov.in/sites/default/files/National%20Guidelines%20on%20Second-line%20and%20Alternative%20First-line%20ART%20For%20Adults%20and%20Adolescents%20May%202013_0.pdf.
27. World Health Organization. March 2014 Supplement to the 2013 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach; 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/104264/9789241506830_eng.pdf. Accessed July 15,2020.
28. Bokretsion GB, Endalkachew N, Getachew KA. HIV/AIDS treatment failure and its determinant factors among first-line HAART patients at Felege-Hiwot Referral Hospital, Bahir Dar, Northwest Ethiopia. J AIDS Clin Res. 2017;8:11.
29. Mulu A, Liebert UG, Maier M. Virological efficacy and immunological recovery among Ethiopian HIV-1 infected adults and children. BMC Infect Dis. 2014;14(1):28. doi:10.1186/1471-2334-14-28
30. Annison L, Dompreh A, Adu-Sarkodie Y. The immunological response of HIV-positive patients initiating HAART at the Komfo Anokye Teaching Hospital, Kumasi, Ghana. Ghana Med J. 2013;47(4):164.
31. Appay V, Sauce D. Immune activation and inflammation in HIV‐1 infection: causes and consequences. J Pathol. 2008;214(2):231–241. doi:10.1002/path.2276
32. Kannan VP, Babu Anand C, Nehru D. A study of antiretroviral therapy outcomes in a tertiary care center in thanjavur medical college hospital, Southern India. J. Evid. Based Med. Healthc. 2017; 4(38), 2273-2279. doi: 10.18410/jebmh/2017/446. Available from: https://jebmh.com/latest_articles/96125. Accessed Juy 15, 2020.
33. Florence E, Lundgren J, Dreezen C, et al. EuroSIDA Study Group. Factors associated with a reduced CD4 lymphocyte count response to haart despite full viral suppression in the eurosida study. HIV Med. 2003;4(3):255–262.
34. García F, de Lazzari E, Plana M, et al. Long-term CD4+ T-cell response to highly active antiretroviral therapy according to baseline CD4+ T-cell count. JAIDS. 2004;36(2):702–713. doi:10.1097/00126334-200406010-00007
35. Kaufmann GR, Furrer H, Ledergerber B, et al. Characteristics, determinants, and clinical relevance of CD4 T cell recovery to< 500 cells/µL in HIV Type 1 infected individuals receiving potent antiretroviral therapy. Clin Infect Dis. 2005;41(3):361–372. doi:10.1086/431484
36. Robbins GK, Spritzler JG, Chan ES, et al. Incomplete reconstitution of T cell subsets on combination antiretroviral therapy in the AIDS clinical trials group protocol 384. Clin Infect Dis. 2009;48(3):350–361. doi:10.1086/595888
37. Kanters S, Nachega J, Funk A, et al. CD4 (+) T-cell recovery after initiation of antiretroviral therapy in a resource-limited setting: a prospective cohort analysis. Antivir Ther. 2014;19(1):31–39. doi:10.3851/IMP2670
38. Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis. 2007;44(3):441–446. doi:10.1086/510746
39. Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One. 2013;8(12):e81355. doi:10.1371/journal.pone.0081355
40. Palella F
41. Liang H, Wu H, Carroll RJ. The relationship between virologic and immunologic responses in AIDS clinical research using mixed‐effects varying‐coefficient models with measurement error. Biostatistics. 2003;4(2):297–312. doi:10.1093/biostatistics/4.2.297
42. Pakker NG, Notermans DW, De Boer RJ, et al. Biphasic kinetics of peripheral blood T cells after triple combination therapy in HIV-1 infection: a composite of redistribution and proliferation. Nat Med. 1998;4(2):208–214. doi:10.1038/nm0298-208
43. Twizerimana AP, Mwatha J, Musabyimana JP, Kayigi E, Harelimana JD, Karanja SM, Mutesa L. Immunological profiles in HIV positive patients following highly active antiretroviral treatment initiation in Kigali,Rwanda. East African Medical Journal. 2014 Dec 3;91 (8):261-6.
44. Nash D, Katyal M, Brinkhof MW, et al. Long-term immunologic response to antiretroviral therapy in low-income countries: collaborative analysis of prospective studies: the antiretroviral therapy in lower-income countries (ART-LINC) collaboration of the international epidemiological databases to evaluate AIDS. AIDS. 2008;22(17):2291.
45. Kwobah CM, Braitstein P, Koech JK, et al. Factors associated with late engagement to HIV care in Western Kenya: a cross-sectional study. J Int Association Providers AIDS Care. 2016;15(6):505–511. doi:10.1177/2325957414567682
46. Mojumdar K, Vajpayee M, Chauhan NK, Mendiratta S. Late presenters to HIV care and treatment, identification of associated risk factors in HIV-1 infected Indian population. BMC Public Health. 2010;10(1):416. doi:10.1186/1471-2458-10-416
47. World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy; 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/255884/9789241550062-eng.pdf. Accessed July 15,2020.
48. Galdas PM, Cheater F, Marshall P. Men and health help‐seeking behavior: a literature review. J Adv Nurs. 2005;49(6):616–623. doi:10.1111/j.1365-2648.2004.03331.x
49. Braitstein P, Boulle A, Nash D, et al. Gender and the use of antiretroviral treatment in resource-constrained settings: findings from a multicenter collaboration. J Women’s Health. 2008;17(1):47–55. doi:10.1089/jwh.2007.0353
50. Gea-Banacloche JC, Clifford HL. Immune reconstitution in HIV infection. AIDS. 1999;13:S2538.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.