Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Immunological Features of Children with Gastrointestinal Bleeding Due to Henoch-Schönlein Purpura
Authors Yang L, Guo J, Xiong F
Received 11 July 2023
Accepted for publication 9 January 2024
Published 23 January 2024 Volume 2024:15 Pages 59—66
DOI https://doi.org/10.2147/PHMT.S429961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Lingrong Yang, Jing Guo, Fu Xiong
Sichuan Provincial Maternity and Child Health Care Hospital, Women and Children’s Hospital of Chengdu Medical College, Sichuan, Chengdu, 610045, People’s Republic of China
Correspondence: Fu Xiong, Email [email protected]
Background: This study aims to evaluate the immunological features of gastrointestinal (GI) bleeding in children with Henoch-Schönlein purpura (HSP).
Study Design: This retrospective study was conducted on children with HSP. Demographic and clinical data were collected, including serum immunoglobulin (Ig) levels, complement C3 and C4 levels, and lymphocyte subtype percentage.
Results: A total of 446 hospitalized children had HSP. Eighty-six children with HSP had GI bleeding, 114 had proteinuria, and 107 had hematuria. Lower arthralgia, prolonged glucocorticoid use, increased white blood cell counts, elevated neutrophils and neutrophil-to-lymphocyte ratio, reduced IgG and C3 levels, elevated CD19+ cell percentage, and reduced CD3+ cell and natural killer cell percentages were associated with GI bleeding risk in patients with HSP. Multivariate regression analysis revealed that arthralgia, glucocorticoid use, increased neutrophil percentage, reduced IgG and C3 levels, and increased CD19+ cell percentage were independent predictors of GI bleeding. Further analysis indicated that the combination of C3 and CD19+ cell percentages had a high predictive ability for GI bleeding in children with HSP.
Conclusion: This study indicated that reduced C3 and increased CD19+ cell percentages contributed to the development of GI bleeding in children with HSP. Specific immunologic profiles may be strongly correlated with GI bleeding risk in children with HSP.
Keywords: children, complement, gastrointestinal bleeding, Henoch-Schönlein purpura, lymphocyte subtype
Introduction
Henoch-Schönlein purpura (HSP), also called IgA vasculitis (IgAV), is the most common form of systemic vasculitis in childhood. HSP is characterized by widespread leukocytoclastic vasculitis of small vessels resulting from vascular entrapment of circulating immunoglobulin A (IgA) immune complexes with complement activation.1,2 The reported incidence varied from 3 to 27 per 100,000 children, and the incidence could reach 56 per 100,000 Asian children with a peak incidence of five years.3,4 The clinical features of HSP include non-thrombocytopenic purpura, arthritis, arthralgia, gastrointestinal (GI) disorders, and renal involvement.1 About two-thirds of children with HSP have abdominal pain with or without abdominal distension, nausea, vomiting, and GI bleeding.4,5 Although GI bleeding accounts for about 18–52% of HSP abdominal symptoms, it threatens children’s lives.2,6,7 Furthermore, massive intestinal bleeding is associated with a significantly increased mortality.7,8 Some children with severe or refractory GI bleeding require long-term nutritional support and treatment.2 This leads to substantially increased medical costs and longer hospital stays. Consequently, early detection of GI bleeding is crucial for HSP treatment and prognosis.
Clinical studies have shown that the platelet (PLT) counts, mean platelet volume (MPV), platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio (NLR), C3 level, D-dimer level, and low-density lipoprotein level are associated with gastrointestinal hemorrhage in HSP.9–11 This is an important basis for doctors to diagnose the gastrointestinal bleeding status of HSP patients, which greatly aids clinical judgment. However, the etiology and pathogenesis of gastrointestinal bleeding in patients with HSP remain unclear. Many studies have indicated that fluid and cellular immune dysfunctions contribute to HSP pathogenesis.12–14 Some studies have indicated that elevated blood NLR and decreased MPV can be good predictors of HSP in patients with symptoms of gastrointestinal involvement.15,16 Skin rash and elevated D-dimer levels may also cause GI bleeding. Considering the importance of the immune response in HSP, we hypothesized that immune function abnormalities may cause gastrointestinal bleeding in children with HSP.
Methods
Patients
This retrospective study was conducted on a primary cohort of patients with HSP between January 2017 and December 2022 at the Sichuan Maternal and Child Health Hospital (Sichuan, China). The patients were mostly aged 5–15 years. HSP diagnosis was based on the EULAR/PRINTO/PRES criteria, including purpura or petechiae with lower limb predominance and at least one of the following four criteria: abdominal pain, histopathology, arthritis or arthralgia, and renal involvement.17 Proteinuria was determined as > 0.3 g/24 h or > 30 mmol/mg of urine albumin/creatinine ratio on a spot morning sample, and hematuria was determined as >5 red blood cells/high power field or red blood cells casts in the urinary sediment or ≥2+ on the dipstick.17 GI bleeding included hematemesis, melena, and hematochezia. The HSP in children without GI bleeding were labeled as the control group. Patients with missing data were excluded from this study.
Detection of Lymphocyte Subtypes and Data Collections
Venous blood samples were collected within 24 h of admission. Lymphocyte subtype percentages were estimated using BD Multitest 6-color T, B, and NK (TBNK) lymphocytes Reagent via Cantoll (Becton Dickinson, San Jose, CA, USA) and analyzed using DIVA software (Becton Dickinson, San Jose, CA) according to the manufacturer’s recommendations. Briefly, the CD3 FITC was used to identify T lymphocytes, CD4 PE-Cy™7 to detect T helper/inducer lymphocytes, CD8 APC-Cy7 to identify suppressor/cytotoxic T lymphocytes, and CD19 APC to identify B lymphocytes. The TBNK reagent defines NK cells by simultaneously analyzing the expression of CD16 and CD56 using the same conjugation.
Demographic and clinical data were collected, including age, sex, disease duration, complications, white blood cell (WBC) counts, neutrophil percentage, lymphocyte classification and counts, hemoglobin (Hgb) concentration, PLT counts, C-reactive protein (CRP) levels, erythrocyte sedimentation rate (ESR), procalcitonin level (PCT), immunoglobulin (Ig)G, IgE, IgA, complement C3 and C4, CD19+, CD3+, CD4+, CD8+, and NK cell percentages. All laboratory tests were performed on admission.
Statistical Analysis
Continuous variables were expressed as mean and standard differences (SD) and compared using an unpaired, two-tailed t-test or Mann–Whitney test. Categorical variables were compared using the x2 test or Fisher’s exact test. The logistic regression analysis was used to assess potential risk factors for developing GI due to HSP. The area under the receiver operating characteristic (ROC) curve was used to evaluate the predictive power of the logistic regression model. The PASW statistical software package was used to perform all statistical analyses and graphics. Moreover, P < 0.05 was considered statistically significant.
Ethical Considerations
This study was approved by the Ethics Review Board of Sichuan Maternal and Child Health Hospital 20230331-030), which followed the ethical procedures established by the Declaration of Helsinki. Since the hospital ethics committee approved this retrospective study, all patients were anonymous, and independent informed consent was not required.
Results
Clinical Characteristics of HSP with GI Bleeding
Four hundred forty-six hospitalized children had HSP. In total, 86 children with HSP had GI bleeding, 114 had proteinuria, and 107 had hematuria (Table 1). The clinical characteristics of the HSP with GI bleeding and control groups are shown in Table 1. The HSP in children with GI bleeding had lower arthralgia frequency (26.7% vs 47.5%, P < 0.001), higher WBC counts (13.86 vs 11.73, P = 0.001), higher neutrophil percentage (71.35% vs 65.31%, P = 0.001), higher NLR (3.66 vs 2.67, P = 0.009), higher PLT counts (405.19 vs 363.98. P = 0.025), and higher serum creatine levels (45.2 vs 36.77, P < 0.001) compared to control group. There were no significant differences in gender ratio, proteinuria and hematuria quantities, Hgb concentrations, CRP levels, and liver function between the two groups.
 |
Table 1 Clinical Characteristics and Laboratory Findings Between Children with or Without GI Bleeding Due to IgAV |
Immunologic Features of GI Bleeding in Children with HSP
The HSP in children with GI bleeding showed higher CD19+ lymphocyte percentage (26.51% vs 19.31%, P < 0.001), lower CD3+ T cell (61.53% vs 67.73%, P < 0.001), lower NK cell percentage (7.09% vs 9.66%, P = 0.009), lower IgG levels (9.40% vs 10.80%, P = 0.003), and lower C3 levels (1.17 vs 1.26, P = 0.01) compared to those without GI bleeding (Table 1). However, patients with HSP who experienced GI bleeding had lower IgA and C4 levels and lower CD4+ and CD8+ cell percentages than those without GI bleeding. There was no statistically significant difference between the two groups.
Risk Factors for Developing GI Bleeding in HSP
Univariate logistic regression models used to predict GI bleeding in children with HSP depicted significant differences in most of the risk factors (Table 2). The clinical features most strongly associated with gastrointestinal bleeding were less arthralgia (OR 0.404, P = 0.001), longer glucocorticoid use (OR 1.030, P < 0.001), increased leukocyte count (OR 1.065, P = 0.002), elevated neutrophils (OR 1.029, P = 0.001), and neutrophil/ lymphocyte percentages (OR 1.142, P = 0.002), PLTs (OR 1.002, P = 0.007), decreased ESR (OR 0.923, P < 0.001), low serum IgG levels (OR 0.864, P = 0.003), and elevated percentage of CD19+ cells (OR 1.122, P < 0.001), and compared to the CD3+ (OR 0.957, P = 0.001), lower percentage of NK cells (OR 0.909, P = 0.008), and lower C3 levels (OR 0.230, P < 0.05) compared to the control group. The multivariate logistic regression model revealed that only a decrease in arthralgia level, prolonged glucocorticoid use, an increase in neutrophil percentage, and a decrease in IgG, C3, and CD19+ cell percentages were associated with a higher risk of gastrointestinal bleeding, which was an independent predictor of the risk of gastrointestinal bleeding (Table 3). The area under the curve (AUC) for this model was 0.861 (Figure 1).
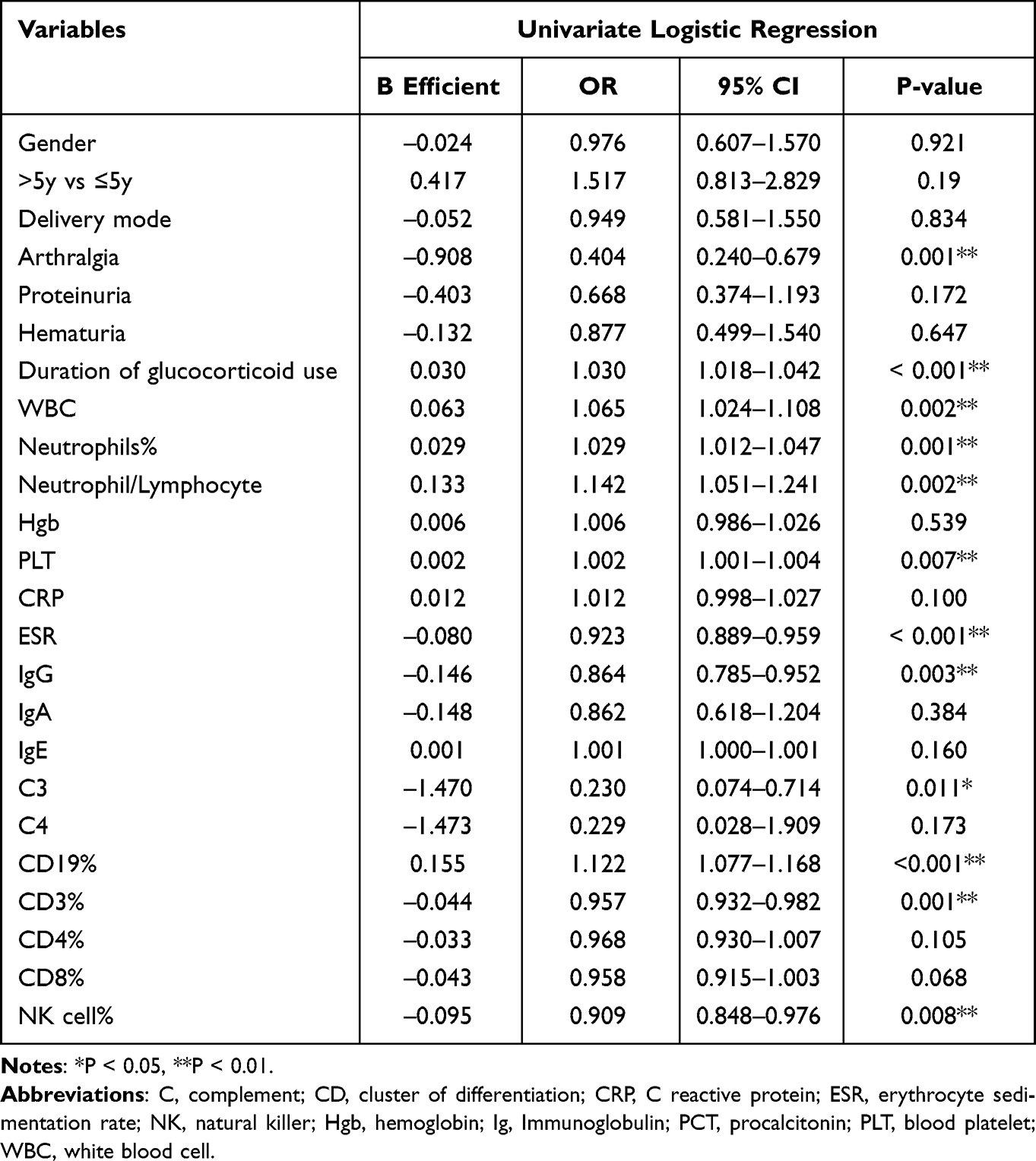 |
Table 2 Risk Factors Associated with the Development of GI Bleeding Due to HSP on Univariate Analysis |
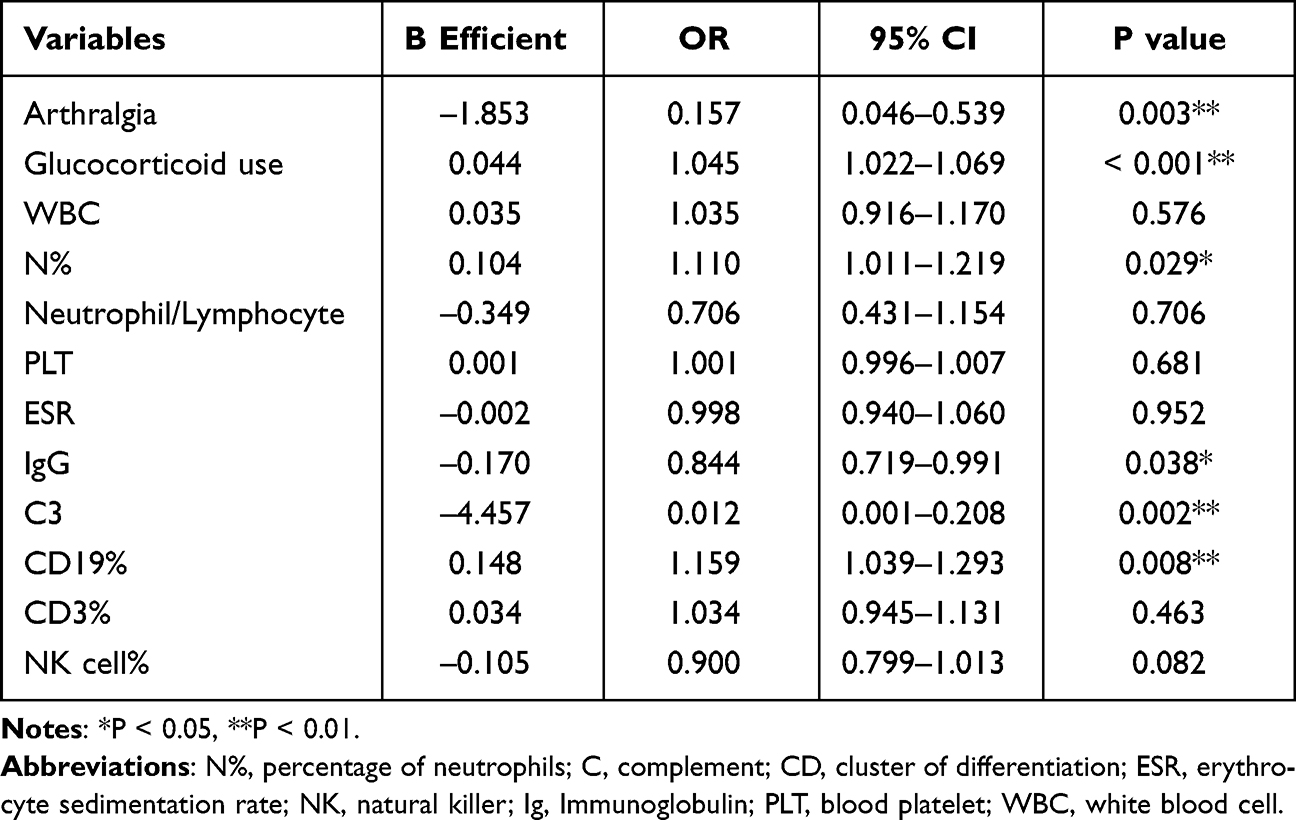 |
Table 3 Risk Factors Associated with the Development of GI Bleeding Due to HSP on Multivariate Analysis |
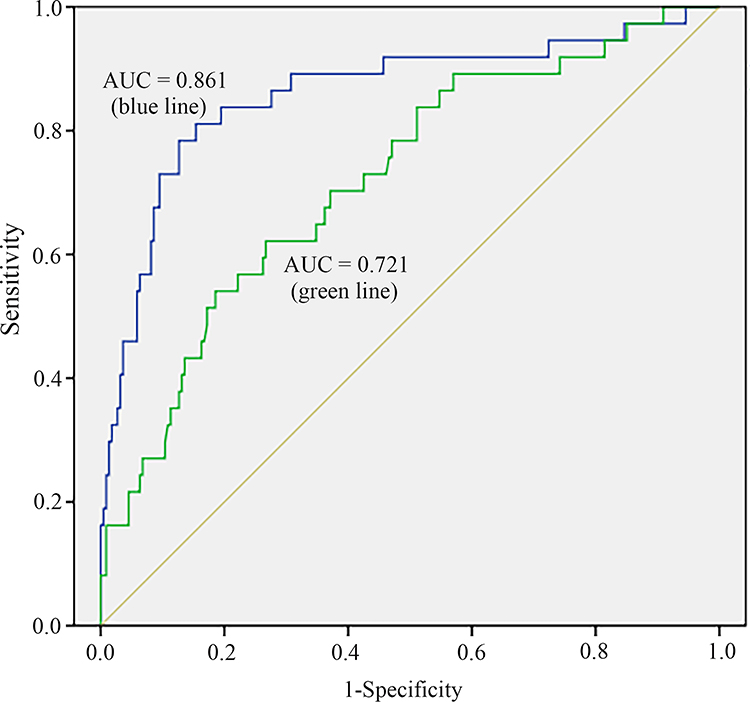 |
Figure 1 Predictive ability of the multivariate logistic regression model for developing GI bleeding. The AUC for the blue line (arthralgia, glucocorticoid use, N%, IgG, C3, and CD19%) is 0.861 (95% CI: 0.784–0.938, P < 0.001). The AUC for the green line (C3 and CD19%) is 0.721 (95% CI: 0.632–0.811, P < 0.001). |
Role of Immunologic Response in HSP with GI Bleeding
The final multivariate logistic regression model included only serum C3 levels and CD19+ cell percentage to better elucidate the immunologic role in GI bleeding. ROC curve analysis revealed that this model could predict the development of GI bleeding in children with HSP, with an AUC of 0.721 (Figure 1, 95% CI: 0.632–0.811, P < 0.001). This suggests that immunologic mechanisms may be crucial for GI involvement in HSP patients.
Discussion
In this study, univariate logistic regression showed that decreased arthralgia, prolonged glucocorticoid use, increased white blood cell counts, elevated neutrophils and NLR, elevated PLTs, decreased ESR levels, decreased C3 levels, decreased serum IgG levels, increased CD19+ cell percentage, and decreased CD3+ and NK cell percentages were significantly associated with gastrointestinal bleeding risk in patients with HSP. However, multivariate regression analyses depicted that only a decrease in arthralgia level, an increase in glucocorticoid use, an increase in neutrophil percentage, a decrease in IgG and C3, and an increase in CD19+ cell percentage were independent predictors of gastrointestinal bleeding. Further analysis showed that the combination of C3 and CD19+ cell percentages predicted gastrointestinal bleeding in children with HSP.
A predictive model7 for GI bleeding risk in children with HSP revealed that eosinophils, high-sensitivity C-reactive protein, activated partial thromboplastin time, potassium, albumin, and IgE were independent predictors. Age at onset below six years, not receiving glucocorticoid therapy within 72 h of the onset of GI symptoms, hematochezia, and high D-dimer levels were associated with intussusception in pediatric HSP with GI involvement.18 A study found that the platelet‑to‑lymphocyte ratio and NLR can be reliable predictors of GI tract involvement in HSP patients but are not significantly associated with renal involvement.19 Additionally, an abdominal pain duration of more than seven days and a methylprednisolone dose of over 2 mg/kg increased gastrointestinal perforation in children with HSP.20 The HSP in children with intermittent abdominal pain had a high risk of nephritis and severe GI bleeding. These patients should be followed up strictly with clinical and laboratory assessments, mainly during the first month of the disease course.21
There are inconsistent results in the literature regarding serum IgA, IgG, and IgM levels in children with HSP. Patients with HSP could have immune disorders outside the IgA compartment, and there could be interactions between IgA and other Igs, likely contributing to the higher likelihood of complications.22 Furthermore, HSP in children with GI symptoms who had elevated neutrophil counts, B lymphocyte percentage, and reduced IgG levels were associated with refractory GI involvement.6 Our study also demonstrated reduced IgG levels in HSP patients with GI bleeding than those without GI bleeding, indicating that humoral immune imbalance may contribute to HSP pathogenesis. However, the underlying mechanism remains unclear.
The reduced C3 levels were observed in the present HSP cases with GI bleeding. The complement system is involved in the pathogenesis of several autoimmune diseases, including HSP.23 Lower C3 levels were associated with renal involvement and severity.9 Lin et al demonstrated that patients with HSP had a profound C4 reduction and moderate C3 reduction, indicating classical or lectin pathway activation.24 However, the decrease in complement levels in HSP did not affect the prognosis of HSP and did not develop into systemic lupus erythematosus (SLE).25 Glomerular deposition of complement factors, including C3 and C4, has been observed in most patients with HSP nephritis without C1q deposits, supporting the hypothesis of prevalent activation of the lectin pathway.23 Urinary complement C3 and C4 levels were significantly higher in all children with HSP than in SLE patients,26 indicating that reduced complement could be associated with urine loss. Although some patients with HSP have no detectable proteinuria, they still have hypoalbuminemia, probably due to intestinal protein loss.27 These findings further suggest that, besides immune activation, gastrointestinal loss could contribute to hypocomplementemia.
Increasing evidence suggests that immune dysfunction is involved in HSP pathogenesis.9,14,24,28,29 This study showed that HSP in children with GI bleeding had a significantly increased serum CD19+ cell percentage than those without GI bleeding, consistent with prior studies. The HSP patients had a lower CD3+ lymphocyte percentage and higher CD19+ percentage than patients with infectious mononucleosis or Mycoplasma pneumoniae infection.29 Additionally, circulating cytotoxic T lymphocytes and NK cells were activated, and their number in the glomeruli increased in HSP nephritis patients with severe proteinuria.28 These results further revealed that different immune cell predominance may be disease-specific. Increased CD19+ cells in children with HSP were likely associated with GI bleeding.
Furthermore, it was intriguing to find a strong association between lower arthritis in HSP patients and GI hemorrhage. HSP can be categorized into simple cutaneous, arthritic, abdominal, renal, and mixed phenotypes, depending on the site of involvement and clinical presentation. Symptoms in patients with the articular form consist mainly of joint swelling and pain, commonly in the elbow, knee, and ankle,30 which may be associated with exudates and hematomas. The most common complications in patients with the abdominal form include gastrointestinal bleeding, which may be related to the inflammatory response that occurs during the acute phase of HSP, and alterations in the PLT-activating factor and its acetyl hydrolase.31–33 In this study, using unifactorial and multifactorial logistic regression analyses, we found that children with arthralgia may be less likely to have concomitant gastrointestinal hemorrhage; however, the exact mechanism remains unclear. Current studies and clinical practice cannot prove that arthralgia is not associated with gastrointestinal bleeding; however, we can determine that the direction of involvement may significantly differ.
Our study has some limitations. First, this retrospective study is based on a single-center hospital, and there may be selection bias. Future multicenter and prospective studies and recurrence follow-ups will help us better understand the HSP pathogenesis. Second, all laboratory tests were performed within 24 h of admission without dynamic monitoring. Finally, our GI bleeding classification relied mainly on the description of the medical history, perhaps missing some patients.
In conclusion, our study suggests that patients with IgAV who have reduced C3 levels or an increased CD19 lymphocyte proportion may have a higher risk of gastrointestinal bleeding. Specific immunologic features may be strongly associated with gastrointestinal bleeding in patients with HSP. Prospective multicenter studies on immune responses will help explain the pathogenesis of HSP.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
2022 In-hospital Science and Technology Innovation Fund of Sichuan Provincial Maternity and Child Health Care Hospital (CXPJ2022-01).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised international Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11. doi:10.1002/art.37715
2. Yang Y, Shu J, Mu J, et al. Clinical analysis of 99 children with Henoch-Schonlein purpura complicated with overt gastrointestinal bleeding. Clin Rheumatol. 2022;41(12):3783–3790. doi:10.1007/s10067-022-06323-8
3. Shim JO, Han K, Park S, Kim GH, Ko JS, Chung JY. Ten-year Nationwide Population-based Survey on the characteristics of children with Henoch-Schӧnlein Purpura in Korea. J Korean Med Sci. 2018;33(25):e174. doi:10.3346/jkms.2018.33.e174
4. Trapani S, Rubino C, Indolfi G. Gastrointestinal involvement in childhood vasculitides. Acta Paediatr. 2020;109(11):2226–2236. doi:10.1111/apa.15381
5. Choong CK, Beasley SW. Intra-abdominal manifestations of Henoch-Schonlein purpura. J Paediatr Child Health. 1998;34(5):405–409. doi:10.1046/j.1440-1754.1998.00263.x
6. Zhang X, Che R, Xu H, et al. Hemoperfusion and intravenous immunoglobulins for refractory gastrointestinal involvement in pediatric Henoch-Schonlein purpura: a single-center retrospective cohort study. BMC Pediatr. 2022;22(1):692. doi:10.1186/s12887-022-03709-0
7. Sun L, Liu W, Li C, Zhang Y, Shi Y. Construction and internal validation of a predictive model for risk of gastrointestinal bleeding in children with abdominal Henoch-Schonlein purpura: a single-center retrospective case-control study. Front Immunol. 2022;13:1025335. doi:10.3389/fimmu.2022.1025335
8. Chang WL, Yang YH, Lin YT, Chiang BL. Gastrointestinal manifestations in Henoch-Schonlein purpura: a review of 261 patients. Acta Paediatr. 2004;93(11):1427–1431. doi:10.1080/08035250410020181
9. Song Z, Nie Y, Yang L, Tao J. Predicting severe renal and gastrointestinal involvement in childhood immunoglobulin A vasculitis with routine laboratory parameters. Dermatology. 2022;238(4):745–752. doi:10.1159/000519665
10. Shao X, Li H, Chen T, et al. Association of the monocyte-to-high-density lipoprotein cholesterol ratio with gastrointestinal involvement of immunoglobulin a vasculitis. Clin Cosmet Invest Dermatol. 2023;16:359–367. doi:10.2147/CCID.S398134
11. Hocevar A, Tomsic M, Jurcic V, Perdan Pirkmajer K, Rotar Ž. Predicting gastrointestinal and renal involvement in adult IgA vasculitis. Arthritis Res Ther. 2019;21(1):302. doi:10.1186/s13075-019-2089-2
12. Wang Y. The role of T cells in the development of Henoch-Schonlein purpura. Front Biosci. 2018;23(3):837–851. doi:10.2741/4619
13. Besbas N, Saatci U, Ruacan S, et al. The role of cytokines in Henoch Schonlein purpura. Scand J Rheumatol. 1997;26(6):456–460. doi:10.3109/03009749709065719
14. Ding Y, Zhou Y, Li HR, Xiong YH, Yin W, Zhao L. Characteristics of immune function in the acute phase of Henoch-Schonlein purpura. Clin Rheumatol. 2021;40(9):3711–3716. doi:10.1007/s10067-021-05707-6
15. Makay B, Gücenmez ÖA, Duman M, Ünsal E. The relationship of neutrophil-to-lymphocyte ratio with gastrointestinal bleeding in Henoch-Schonlein purpura. Rheumatol Int. 2014;34(9):1323–1327. doi:10.1007/s00296-014-2986-2
16. Li B, Ren Q, Ling J, Tao Z, Yang X, Li Y. Clinical relevance of neutrophil-to-lymphocyte ratio and mean platelet volume in pediatric Henoch-Schonlein Purpura: a meta-analysis. Bioengineered. 2021;12(1):286–295. doi:10.1080/21655979.2020.1865607
17. Ozen S, Pistorio A, Iusan SM, et al. EULAR/PRINTO/PRES criteria for Henoch-Schonlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: ankara 2008. Part II: final classification criteria. Ann Rheum Dis. 2010;69(5):798–806. doi:10.1136/ard.2009.116657
18. Zhao Q, Yang Y, He SW, Wang XT, Liu C. Risk factors for intussusception in children with Henoch-Schonlein purpura: a case-control study. World J Clin Cases. 2021;9(22):6244–6253. doi:10.12998/wjcc.v9.i22.6244
19. Inamadar A, George R, Janagond A. Neutrophil-to-lymphocyte ratio: a biomarker for predicting systemic involvement in iga vasculitis. Indian J Rheumatol. 2020;31(6):1033–1037.
20. Guo Q, Hu X, Song C, et al. Clinical characteristics and associating risk factors of gastrointestinal perforation in children with IgA vasculitis. Ann Med. 2021;53(1):2315–2320. doi:10.1080/07853890.2021.2009554
21. Buscatti IM, Simon JR, Viana VSL, et al. Intermittent abdominal pain in IgA vasculitis. Rev Paul Pediatr. 2021;40:e2020202. doi:10.1590/1984-0462/2022/40/2020202
22. Sestan M, Kifer N, Frkovic M, et al. Gastrointestinal involvement and its association with the risk for nephritis in IgA vasculitis. Ther Adv Musculoskelet Dis. 2021;13:1759720X211024828. doi:10.1177/1759720X211024828
23. Chimenti MS, Ballanti E, Triggianese P, Perricone R. Vasculitides and the Complement System: a Comprehensive Review. Clin Rev Allergy Immunol. 2015;49(3):333–346. doi:10.1007/s12016-014-8453-8
24. Lin Q, Min Y, Li Y, et al. Henoch-Schonlein purpura with hypocomplementemia. Pediatr Nephrol. 2012;27(5):801–806. doi:10.1007/s00467-011-2070-z
25. Lin Q, Li X. Children with Henoch-Schonlein purpura with low complement levels: follow-up for >6 years. Pediatr Nephrol. 2017;32(7):1279. doi:10.1007/s00467-017-3630-7
26. Wright RD, Marro J, Northey SJ, Corkhill R, Beresford MW, Oni L. Urinary complement proteins are increased in children with IgA vasculitis (Henoch-Schonlein purpura) nephritis. Pediatr Nephrol. 2022. doi:10.1007/s00467-022-05747-3
27. Jauhola O, Ronkainen J, Koskimies O, et al. Clinical course of extrarenal symptoms in Henoch-Schonlein purpura: a 6-month prospective study. Arch Dis Child. 2010;95(11):871–876. doi:10.1136/adc.2009.167874
28. Imai T, Nishiyama K, Ueki K, et al. Involvement of activated cytotoxic T lymphocytes and natural killer cells in Henoch-Schonlein purpura nephritis. Clin Transl Immunol. 2020;9(11):e1212. doi:10.1002/cti2.1212
29. Zhao L, Wang H, Wei HX, Lv Y. The pathophysiologic significance of lymphocyte subset determination in children with infectious mononucleosis, mycoplasma pneumonia and Henoch-Schonlein purpura. BMC Pediatr. 2022;22(1):698. doi:10.1186/s12887-022-03770-9
30. Du L, Wang P, Liu C, Li S, Yue S, Yang Y. Multisystemic manifestations of IgA vasculitis. Clin Rheumatol. 2021;40(1):43–52. doi:10.1007/s10067-020-05166-5
31. Hong SH, Kim CJ, Yang EM. Neutrophil-to-lymphocyte ratio to predict gastrointestinal bleeding in Henoch: schonlein purpura. Pediatr Int. 2018;60(9):791–795. doi:10.1111/ped.13652
32. Gayret OB, Erol M, Tekin Nacaroglu H. The relationship of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio with gastrointestinal bleeding in Henoch-Schonlein Purpura. Iran J Pediatr. 2016;26(5):e8191. doi:10.5812/ijp.8191
33. Wang B-X, Mei H, Peng H-M, Gao Y, Ding Y. 血小板活化因子乙酰水解酶基因多态性与过敏性紫癜消化道出血的相关性研究 [Association between platelet-activating factor acetylhydrolase gene polymorphisms and gastrointestinal bleeding in children with Henoch-Schönlein purpura]. Zhongguo Dang Dai Er Ke Za Zhi. 2017;19(4):385–388. Chinese.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.