Back to Journals » International Journal of General Medicine » Volume 16
Immunohistochemical Expression of IDH1, ATRX, Ki67, GFAP, and Prognosis in Indonesian Glioma Patients
Authors Priambada D, Thohar Arifin M, Saputro A, Muzakka A, Karlowee V, Sadhana U, Bakhtiar Y, Prihastomo KT ![]() , Risdianto A, Brotoarianto HK, Andar E, Muttaqin Z
, Risdianto A, Brotoarianto HK, Andar E, Muttaqin Z ![]()
Received 1 December 2022
Accepted for publication 7 January 2023
Published 1 February 2023 Volume 2023:16 Pages 393—403
DOI https://doi.org/10.2147/IJGM.S397550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dody Priambada,1 Muhamad Thohar Arifin,1 Abdi Saputro,1 Azka Muzakka,1 Vega Karlowee,2 Udadi Sadhana,2 Yuriz Bakhtiar,1 Krisna Tsaniadi Prihastomo,1 Ajid Risdianto,1 Happy Kurnia Brotoarianto,1 Erie Andar,1 Zainal Muttaqin1
1Department of Neurosurgery, Faculty of Medicine, Diponegoro University/Dr. Kariadi Hospital, Semarang, Indonesia; 2Department of Clinical Pathology, Faculty of Medicine, Diponegoro University, Dr. Kariadi Hospital, Semarang, Indonesia
Correspondence: Muhamad Thohar Arifin, Department of Neurosurgery, Faculty of Medicine, Diponegoro University/Dr. Kariadi Hospital, Dr. Soetomo Street Number 16-18, Semarang, Indonesia, Tel +62 813 2586 1628, Email [email protected]
Background: The current World Health Organization (WHO) 2021 classification of human glioma is based on key molecular biomarkers to define neoplastic entities. This review further delineates mutant IDH (isocitrate dehydrogenase) from wild-type IDH disease, a necessity given the large survival gap between mutant IDH and wild-type IDH tumors. In Indonesia, there are currently few reports on the distribution and significance of these mutations. Therefore, this research aims to determine the relationship between IDH mutations, as well as clinicopathological and prognostic factors in patients with gliomas. Other immunohistochemical markers including ATRX (alpha-thalassemia/mental retardation, X-linked), Ki67 and GFAP (glial fibrillary acidic protein) expression were also evaluated.
Methods: Forty-two glioma samples were collected from patients who underwent surgery at Dr. Kariadi General Hospital in Semarang, Central Java, Indonesia. Fresh and paraffin-embedded, formalin-fixed tissue samples were removed and sectioned for hematoxylin and eosin staining, immunohistochemistry, and IDH analysis of mutation. Medical records were used to collect clinicopathological and survival data.
Results: IDH1 mutations were discovered in 32 (76,1%) patients, and those with IDH1 mutation had longer overall survival when corresponded to patients with IDH1-wild-type. Lower expression of Ki67 was discovered to be very associated with a better prognosis.
Conclusion: IDH1 mutations status showed a significant relationship with prognosis in patients with glioma. Meanwhile, other markers (ATRX, Ki67, and GFAP) did not correlate with the prognosis.
Keywords: IDH1, immunohistochemical expression, prognosis, glioma, Indonesia
Introduction
Glioma is the most common primary brain tumor, accounting for 80% of all central nervous system tumors. The worldwide prevalence reaches 3.5 million per year, however, in Indonesia, there is a lack of report of the exact prevalence of gliomas. Since 2016, the WHO classification has included immunohistochemical components as a determining factor for diagnosis, which has a major impact on the prognosis of glioma patients. Isocitrate dehydrogenase (IDH) enzymes are crucial enzymes that are involved in a number of important metabolic processes, including the Krebs cycle, redox regulation, and glutamine metabolism. There are three distinct isoforms of IDH; the mitochondrial matrix is rich in IDH2 and IDH3, while the cytoplasm and peroxisomes contain IDH1. IDH mutations, which are common in human malignancies, have been discovered in more than 80% of grade II/III glioma cases reported to the World Health Organization (WHO). Around 73% of WHO grade IV glioblastoma (GBM) contain the mutations, however only 3.7% of wild-type IDH GBM cases do.1 Patients with IDH mutations had more promising prognoses than those with wild-type IDH, with a median survival time of 31 months for GBM and 15 months for anaplastic astrocytoma (IDH wild type: 20 months; IDH mutant: 65 months). The considerable incidence of IDH mutations in secondary GBM reveals that lower-grade glioma with IDH mutations frequently arises following malignant transition to a higher grade, even though IDH mutant glioma has a better overall prognosis. A hypermutation phenotype, which is linked to a poor prognosis, is also more common in IDH mutant gliomas.2. IDH1 is the main NADPH producer in the brain, which is a key cellular reducing agent required for detoxification processes through reduction of glutathione and thioredoxins and activation of catalase, which are all involved in the protection against the toxicity of reactive oxygen species and oxidative DNA damage.3
In addition to IDH mutation status, gliomas possess mutations in ATRX, which are known as guardians of the genome. Several studies have shown that mutations in ATRX also determine changes in the genome and DNA damage that affects epigenetics, which ultimately play a role in glioma patients’ outcomes.4 The ATRX glioma mutation was first discovered in teenagers and young adults. ATRX is mutated less frequently in adults (age >30) with primary GBM, but it is common in lower grade gliomas and secondary GBM. ATRX mutations have been found in 15 types of human cancers. The contribution of ATRX to oncogenesis, on the other hand, is unknown.5 The WHO 2016 glioma diagnosis protocol also states that ATRX loss is a characteristic feature of an IDH-mutant diffuse astrocytoma, although this is not required for diagnosis.
Glial fibrillary acidic protein (GFAP) is an intermediate filament in the cytoskeleton that is nearly exclusively expressed in astrocytes.6 Stroke and traumatic brain damage are associated with elevated serum GFAP levels. There is evidence that serum GFAP levels are a diagnostically useful biomarker since they are higher in primary high-grade gliomas before surgical resection. In spite of this, neither its prognostic value nor its association with established prognostic indicators like IDH1 mutations have been investigated. Researchers have hitherto focused solely on primary high-grade gliomas, ignoring the correlation between blood GFAP levels and tumor load in recurrent high-grade gliomas.7
Extreme brain damage, such as that induced by a traumatic brain injury or intracerebral hemorrhage, is typically accompanied by elevated levels of GFAP. However, it seems plausible that elevated GFAP levels are detectable in the blood of patients with GBM but not in patients with other intracerebral space-occupying lesions, such as metastases, because GFAP expression and blood-brain barrier disruption are two typical histopathological features of malignant glioma.8 Serum GFAP levels in patients with glioblastoma are much greater than in individuals with other intracranial neoplasms, according to the few prospective case series that have been published so far (including low-grade astrocytomas and metastases). Studies have shown a sensitivity gap,9 but the specificity and positive predictive value of the GFAP test are both adequate (high levels are linked with GBM in about 100% of cases). Even though several studies have shown that people with glioblastoma have much higher serum GFAP levels than people with other intracranial neoplasms,10 no research has been done in Indonesia on GFAP as an immunohistochemical test for glioma prognosis.
As a potent biomarker, the proliferation index evaluates neoplasm growth and contributes to patient prognosis. The proliferation index of central nervous system malignancies has been estimated using a variety of approaches. One of the most effective approaches is the Ki67 labeling index (Ki67 LI), which has been widely used to quantify cell proliferation activity in a range of human malignancies, including brain neoplasms.11 To predict biological behavior, we may apply the Ki67 LI (labeling index) to the WHO histological grades of astrocytomas. This gives us guidance for utilizing Ki67 LI as an adjunct to routine histology in grading astrocytomas quickly.2
In various centers in Indonesia, immunohistochemical-based diagnosis has not been widely applied. Furthermore, due to limited resources, the management of glioma patients are still based on histopathology rather than immunohistochemical profilings. Little is known about the prevalence and outcome of IDH1 mutations in the Indonesian glioma cohort at the present time. This research intends to examine the relationship between IDH1 mutations, as well as clinicopathological and prognostic variables in patients with gliomas. Furthermore, we also examined the expression level of other markers that may be associated with gliomas in Indonesian patients, including ATRX, GFAP, and Ki67 labeling index.
Materials and Methods
Patients and Samples
We performed a retrospective analysis glioma patients treated with radiation and surgery at Dr. Kariadi General Hospital, Semarang, Indonesia, from January 2019 to November 2021 (continuous samples). The total number of patients undergoing surgery between January 2019 and June 2021 was 42. The mean age of patients at the time of primary surgery was 45.45 ± 11.07 (range 23–68 years). Subsequently, tumor samples were obtained from the initial operation and recurrent cases. Patients who were diagnosed with a grade III–IV glioma and who had 60 Gy of radiation therapy followed by temozolomide-based chemotherapy had their progress tracked using data gathered from hospital records. Patients with grade II glioma were given surgery and then followed by observation unless the cancer returned. An expert neuropathologist reviewed hematoxylin-eosin-stained tissue sections and assigned them a classification based on the 2016 WHO categorization of neoplasms of the central nervous system. Medical records were mined for demographic and clinical information.
Tissue Specimens and Immunohistochemical Staining
Tumor specimens are placed in 10% formalin and embedded in paraffin. For standard histological diagnosis, representative sections were stained with hematoxylin and eosin. Subsequently, histological subtypes were defined according to WHO criteria by an examiner who was blinded from clinical information. All immunohistochemistry staining was performed manually with 45 minutes of heat-induced epitope retrieval (HIER) treatment in pH 6; and 4°C overnight incubation using-Anti-human IDH1 R132H (1:50, Dianova, Hamburg, Germany), anti-ATRX (1:200, Sigma-Aldrich, Missouri, USA), anti-human Ki67 antigen clone MIB-1 (1:100, Sigma-Aldrich, California, USA), and anti-human GFAP protein (1:100, Cell Marque, California, USA).
The proportions of positively stained tumor cells were used to semi-quantitatively determine the expression of IDH mutations. Positive cases were defined as specimens showing ≥10% of stained cells. Then, using an antibody for Ki67, immunohistochemical staining was used to identify Ki67 expression. Counting at least 1000 tumor cells in an area that has been uniformly stained allows for the determination of nuclear positive for Ki67. The internal positive control of pre-existing glial cells was defined as ATRX protein in all cell nuclei, and cases with ≥10 and ≤10% stained cells were designated as positive and negative. Mutations in its genes cause the core protein to no longer be expressed in tumor cells, although it is still present in non-tumor cells (eg, endothelial cells). ATRX loss (negative) cases had cases with <10% stained cells, and ATRX retained cases had cases with more than <10% stained cells (positive). The control cortex’s white matter and pial surface then exhibited the majority of the GFAP immunoreactivity, but the injured cortex’s astrocytic cell bodies, processes, and staining intensity were significantly elevated. Cases with <10%, >10%, and >50% stained cells were categorized as 0, 1, and 2, respectively.
Surveillance and Follow-Up
The outpatient clinic, the hospital ward, and telephone calls were all used to gather survival information from patients. Overall survival was estimated as the interval from the first surgical operation to death or the last follow-up (for censored cases).
Ethical Statement
The joint Ethics Committee of the Kariadi General Hospital (No.606–1/EC/KEPK-RSDK/2020) approved this research. Informed consent was obtained from the subject’s parents or guardians, and if they are 18 years of age or older, they can give consent without parental consent.
Statistical Analysis
Clinicopathological characteristics and mutations in the IDH gene are studied. Statistical information is typically displayed as means, with the T-test or Mann–Whitney U-test used for analysis. Categorical variables, on the other hand, are shown in proportions after being analyzed with Chi-square. The survival distributions for each group were plotted using the Kaplan-Meier method, and statistical comparisons were made using Log rank testing. Two-tailed p values are given, and a value of p ≤ 0.05 is regarded to be statistically significant.
Results
Table 1 indicates the patients’ demographic and clinical characteristics, with 32 in the IDH1 mutant group (mean age 45 ±11.07 years) vs 10 patients in the IDH wild-type group (mean age 44.4 ± 8.9 years) (Table 1). Out of 42 patients, 57.1% were morphologically diagnosed as glioblastoma (grade IV), 28.5% with anaplastic features (grade III), and 14.2% with grade II histology. Subsequently, 32 (76,1%) patients carried IDH1 mutations.
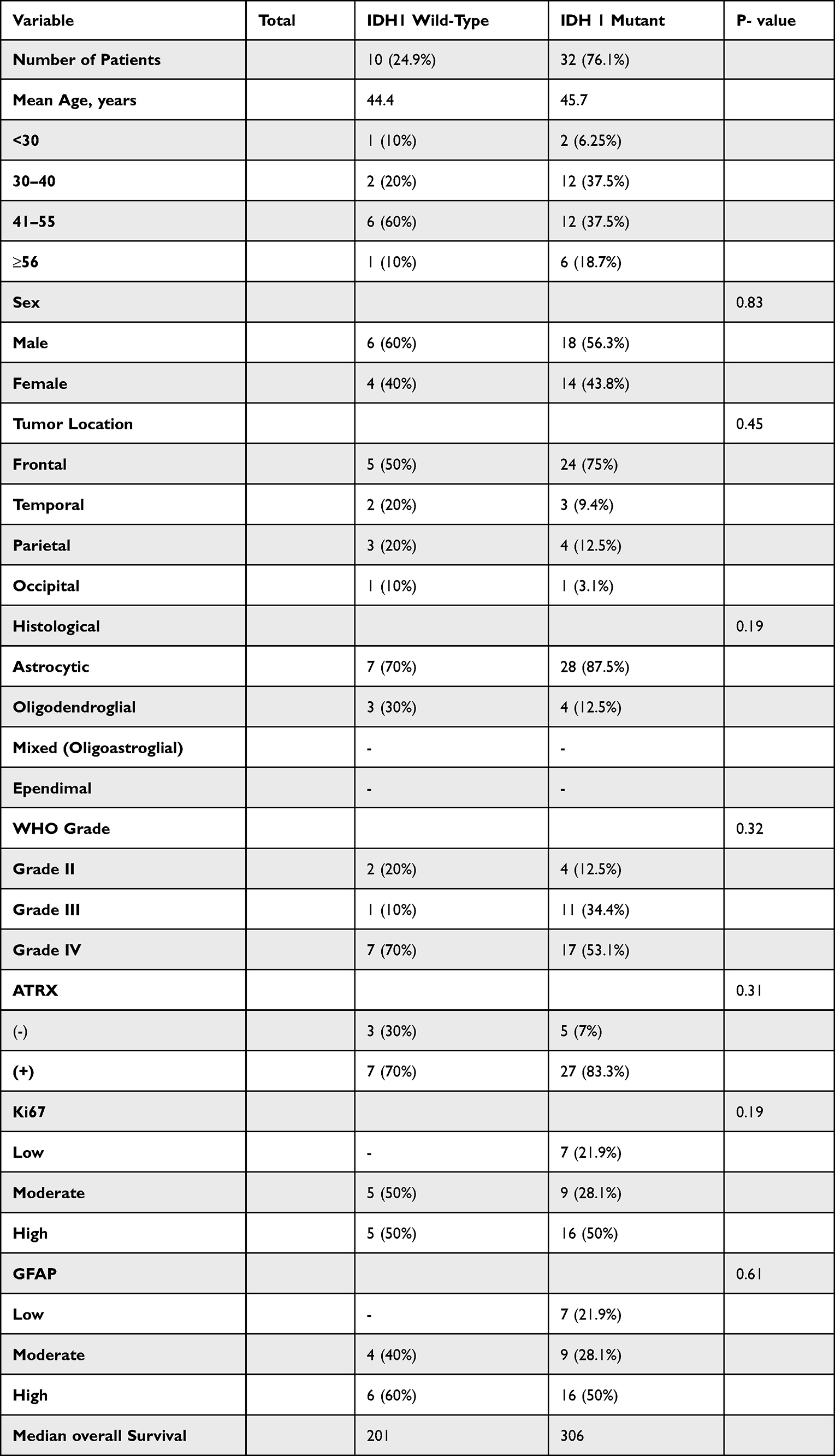 |
Table 1 Subjects’ Characteristics (n=42) |
In the wild-type IDH group, there were 6 male and 4 female patients with the frontal lobe as the dominant location (50%). WHO grade IV dominated the wild-type IDH group and comprises 70% of patients. There were 18 (56.3%) male and 14 (43.8%) female in the IDH mutant group. In 24 (75%) of patients, the tumor was primarily located in the frontal lobe. Histological findings included 28 astrocytic cells (87.5%) and 4 oligodendroglial cells (12.5%) (Figures 1–6).
 |
Figure 1 Immunohistochemistry staining for IDH1 (patient with diffuse astrocytoma). IHC staining of one tumor sample with IDH1 mutated. |
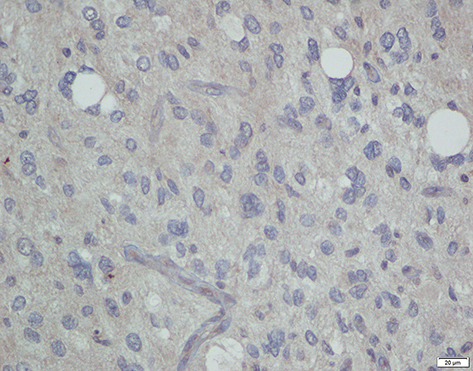 |
Figure 2 Another tumor sample with IDH wild-type (patient with glioblastoma). |
 |
Figure 3 Immunohistochemistry staining for ATRX+ (patient with glioblastoma). |
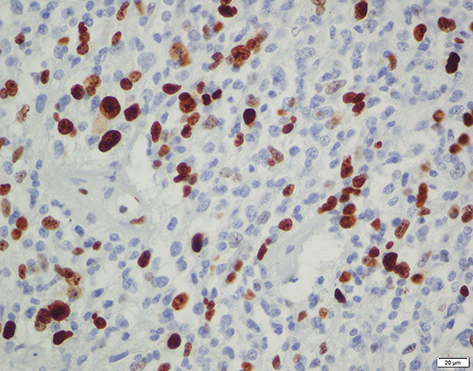 |
Figure 4 Immunohistochemistry staining for Ki67 (glioblastomareccurent) showed high expression. |
 |
Figure 5 Immunohistochemistry staining for Ki67 (glioblastoma) showed medium expression. |
 |
Figure 6 Immunohistochemistry staining for Ki67 (diffuse astrocytoma) showed low expression. |
The Kaplan-Meier survival analysis demonstrated that patients with IDH1 mutations had longer overall survival (OS) than those in the wild-type group (median OS 306.5 ±315.01 vs 201± 208 days)(Figure 7). A significant p-value of 0.044 for the difference in OS was obtained through Log rank tests. The IDH mutant was divided into two groups, ATRX loss/mutation and ATRX retained. Based on the Kaplan Meier curve, the group with IDH mutant + ATRX loss had a higher survival rate than the IDH mutant with ATRX retained (Figure 8–10).
 |
Figure 7 Immunohistochemistry staining for GFAP+ (diffuse astrocytoma). |
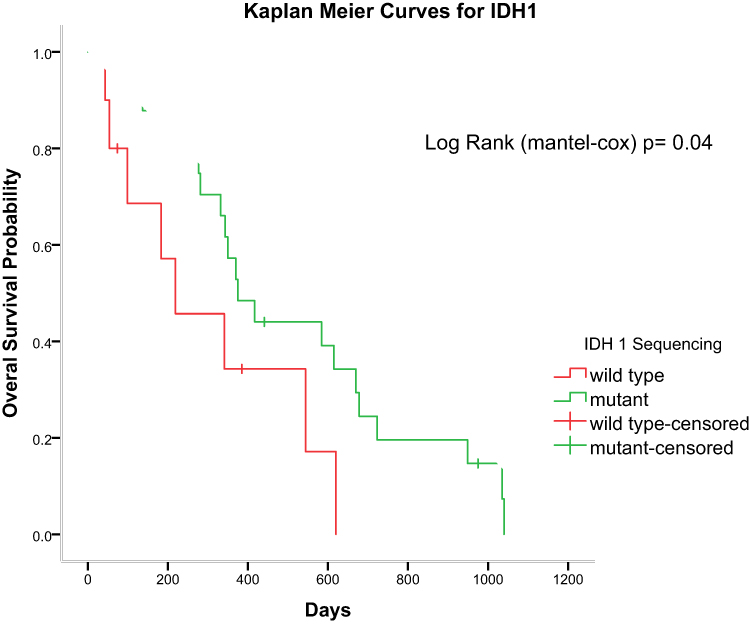 |
Figure 8 Kaplan-Meier survival analysis demonstrating IDH1 mutant glioma patients (green Line) had a significantly longer overall survival (p = 0.04; Log rank test). |
Patients are divided into 3 groups, those with a labeling index <5% Ki67, <5–15%, and those with >15%, and a comparison between the three groups’ survival curves was performed. Patients with Ki67-expressing glioma had longer OS, but not significantly (p=0.05; Log rank test) (Figure 9).
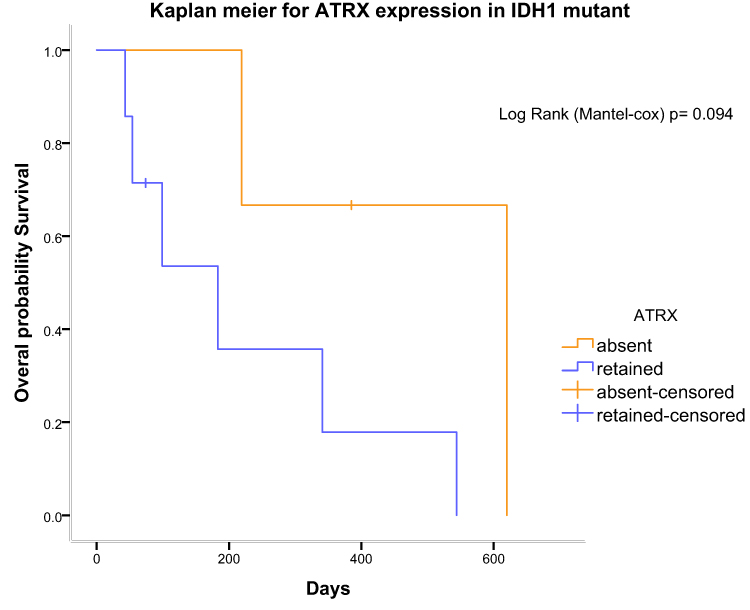 |
Figure 9 Kaplan-Meier survival analysis demonstrating that ATRX absent in IDH1 mutant. Glioma patients (yellow Line) had a longer overall survival but not significant (p = 0.094; Log rank test). |
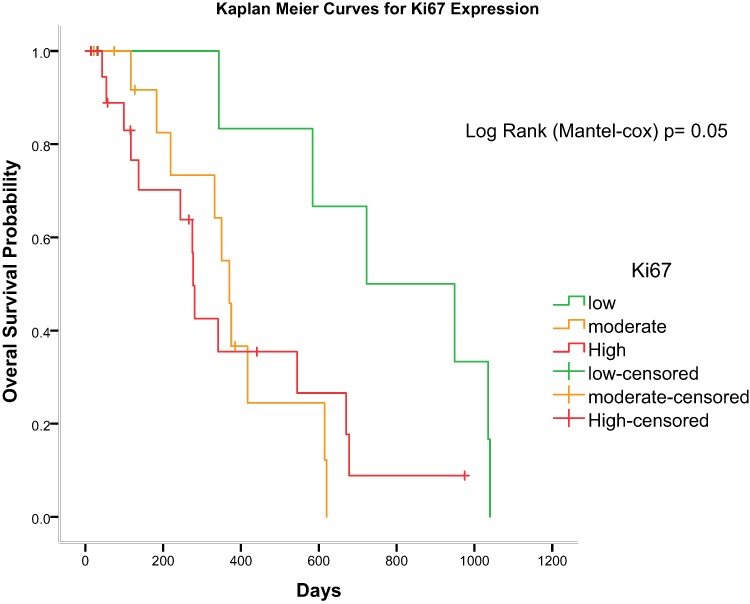 |
Figure 10 Kaplan-Meier survival analysis demonstrating low Ki67 expression glioma. Patients (green Line) had a longer overall survival but not significantly (p = 0.05; Log rank test). |
Several studies evaluated the correlation between serum GFAP and survival. The prognostic significance of GFAP was evaluated by analysis of the relationship between the baseline levels of the marker and the overall survival of patients with glioblastoma. In this research, GFAP was assessed using immunohistochemistry. The data used showed that there is no statistically significant difference between the two groups (p= 0.58) (Figure 11).
 |
Figure 11 Kaplan-Meier survival analysis demonstrating GFAP expression in glioma patients had an insignifcant difference of overall survival between two groups (p = 0.58; Log rank test). |
Discussion
IDH1 mutation frequencies in Asian populations have previously been observed to range from 16.1% in Japan to 74% in China. Populations throughout East and South Asia were the subject of the investigation. The prevalence of IDH1 mutations was reported to be 35% in a study from Southeast Asia.12 Moreover, their investigation covered all varieties of brain tumors, including meningiomas and medulloblastomas. Prior investigation on glioma patients in Indonesia found that IDH1 mutations were present in 21.7% of cases but not IDH2 mutations. Lower Ki67 expression correlates with a longer lifespan.13 According to this research, IDH1 mutations were reported in 76.1% of glioma patients. Subsequently, this examines and reports the inclusion of ATRX and GFAP markers in a Southeast Asian glioma population.
This research indicated that patients with IDH1 mutant glioma had very longer OS (p = 0.04; Log rank test). This is in line with a previous report Shen et al, 2020.14 IDH 1, 2, and 3 are the three distinct IDH enzyme subtypes that are encoded by the IDH gene. Isocitrate is changed by these enzymes into alpha-ketoglutarate (-KG) and NADPH, which shield cells from oxidative stress. Following loss of gene function brought on by IDH mutations, production of -KG is decreased and production of D-2-hydroxyglutarate (D-2HG) is increased. D-2HG competitively inhibits the activity of many dioxygenase enzymes and shares a structure with -KG.11 This promotes the growth of gliomas. The expression of vascular endothelial growth factor is understood to be stimulated by D-2HG, and this in turn encourages angiogenesis and tumor growth.15
ATRX loss in IDH1 mutant glioma patients had a longer OS but was not significant (p = 0.094; Log rank test). Several studies reported that loss of ATRX in grade II and III IDH mutation-noncodeletion tumors are prognostically beneficial. Subsequently, ATRX regulates chromatin remodeling and is closely related to IDH mutations associated with a distinct epigenetic signature, the glioma Cpg island methylator phenotype (g-CIMP). Accordingly, epigenetic differences between ATRX expressers and non-expressers can explain the different clinical courses of astrocytic tumors.16 ATRX proteins play an important epigenetic role in the formation of histones at the level of heterochromatin and telomeric DNA. Patients with low-grade gliomas, ATRX retention, and IDH mutations have worse prognoses in terms of progression-free survival and overall survival (OS) than those whose tumors have 1p/19q codeletions and IDH mutations, and their treatment failure times are longer than those who have IDH mutations and wild-type ATRX (55.6 vs 31.8 months, respectively).5 ATRX deletion encourages tumor growth, demonstrating how it affects the growth of glioma tumors.17
Low Ki67 expression in glioma patients had a longer OS but was not significant (p = 0.05; Log rank test). This research showed that lower expression of Ki67 in glioma patients correlated with a better prognosis. This concurs with a prior study conducted in Indonesia.13 The mechanism underlying how Ki67 expression affects the development and prognosis of tumors is mainly unclear. It should be emphasized, nevertheless, that the presence of the Ki67 antigen might be a sign of a cell’s capacity for growth following tumor removal. During the active stages of the cell cycle, this non-histone nuclear protein is expressed (G1, S, G2, and mitosis).18
In this research, GFAP expression in glioma patients indicated a non-significant difference in OS between the two groups (p = 0.58; Log rank test). A previous study showed that higher WHO grade cases, oligodendroglial differentiation, and IDH wild-type diffuse astrocytomas all showed decreased GFAP expression. In univariate analysis, GFAP expression was substantially associated with better outcomes (greater than IRS=immunoreactive scores 7.8), but it was not significant in multivariate analysis.10 Because there are more low-grade IDH mutant tumors in their community, which is a separate prognostic indicator for a better outcome, the higher scores can be partially attributed.
Several factors that influence the prognosis were not identified in this study, including the tumor size before surgery, which has implications for the condition at admission. The target of surgery in gliomas is safe maximal surgical resection, which preserves the eloquent area of the brain. Data related to it have not been well identified in this study. Radiotherapy and chemotherapy were carried out according to the protocol in the management of glioma patients. Those who had a low tumor grade or died before the protocol was implemented did not receive radiotherapy or chemotherapy in this study. Data on comorbid or complicated patients were not well identified in this study. Given that the cohort was obtained from a single center, this study may have some limitations, including limited sample size and retrospective study design. We also acknowledge the selection bias due to the majority of patients were admitted with advanced conditions of diseases rather than early stages. However, it should be understood that IDH1 examinations have not become a routine procedure in the majority of Indonesian hospitals due to limited facilities and financing policies. This research demonstrated the role of IDH1 mutations in glioma prognosis in the Indonesian population, which is the largest nation in Southeast Asia and the fourth most populous in the world.
Conclusion
IDH1 mutations status showed a significant relationship with prognosis in patients with glioma. Meanwhile, ATRX status, Ki67, and GFAP expression were not correlated with prognosis. These findings suggested that identifying IDH1 mutations is an essential step in the management of patients with glioma. Subsequently, it was observed that the detection of IDH mutations in adult glioma is critical for patient management and education. Further study is needed to learn more about the role of IDH mutations, and Ki67 status, including its impact on patient response to treatments, particularly in developing countries.
Funding
The authors thank to Kementerian Riset dan Badan Teknologi/Riset dan Inovasi Nasional with number (225-57/UN7.6.1/PP/2021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nobusawa S, Watanabe T, Kleihues P, Ohgaki H. IDH1 mutations as molecular signature and predictive factor of secondary glioblastomas. Clin Cancer Res. 2009;15:19. doi:10.1158/1078-0432.CCR-09-0715
2. Yan H, Parsons DW, Jin G, et al. IDH1 and IDH2 mutations in gliomas. N Engl J Med. 2009;360(8):765–773. doi:10.1056/NEJMoa0808710
3. Mondesir J, Willekens C, Touat M, de Botton S. IDH1 and IDH2 mutations as novel therapeutic targets: current perspectives. J Blood Med. 2016;7:171–180. doi:10.2147/JBM.S70716
4. Whitfield BT, Huse JT. Classification of adult-type diffuse gliomas: impact of the World Health Organization 2021 update. Brain Pathol. 2022;32(4). doi:10.1111/bpa.13062
5. Leeper HE, Caron AA, Decker PA, Jenkins RB, Lachance DH, Giannini C. IDH mutation, 1p19q codeletion and ATRX loss in WHO grade II gliomas. Oncotarget. 2015;6(30):30295–30305. doi:10.18632/oncotarget.4497
6. Ellor SV, Pagano-Young TA, Avgeropoulos NG. Glioblastoma: background, standard treatment paradigms, and supportive care considerations. J Law Med Ethics. 2014;42(2):171–182. doi:10.1111/jlme.12133
7. Ostrom QT, Gittleman H, Xu J, et al. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2009–2013. Neuro Oncol. 2016;18:v1–v75. doi:10.1093/neuonc/now207
8. Raposo G, Stoorvogel W. Extracellular vesicles: exosomes, microvesicles, and friends. J Cell Biol. 2013;200(4):373–383. doi:10.1083/jcb.201211138
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
10. Schwab DE, Lepski G, Borchers C, Trautmann K, Paulsen F, Schittenhelm J. Immunohistochemical comparative analysis of GFAP, MAP – 2, NOGO – a, OLIG – 2 and WT – 1 expression in WHO 2016 classified neuroepithelial tumours and their prognostic value. Pathol Res Pract. 2018;214(1):15–24. doi:10.1016/j.prp.2017.12.009
11. Kloosterhof NK, Bralten LBC, Dubbink HJ, French PJ, van den Bent MJ. Isocitrate dehydrogenase-1 mutations: a fundamentally new understanding of diffuse glioma? Lancet Oncol. 2011;12(1):83–91. doi:10.1016/S1470-2045(10)70053-X
12. Yusoff AAM, Zulfakhar FN, Sul’Ain MD, Idris Z, Abdullah JM. Association of the IDH1 C.395G>A (R132H) mutation with histological type in Malay brain tumors. Asian Pacific J Cancer Prevent. 2016;17(12):5195–5201. doi:10.22034/APJCP.2016.17.12.5195
13. Malueka RG, Dwianingsih EK, Bayuangga HF, et al. Clinicopathological features and prognosis of Indonesian patients with gliomas with IDH mutation: insights into its significance in a Southeast Asian population. Asian Pacific J Cancer Prevent. 2020;21(8):2287–2295. doi:10.31557/APJCP.2020.21.8.2287
14. Shen G, Wang R, Gao B, Zhang Z, Wu G, Pope W. The MRI features and prognosis of gliomas associated with idh1 mutation: a single center study in Southwest China. Front Oncol. 2020;10. doi:10.3389/fonc.2020.00852
15. Ichimura K. Molecular pathogenesis of IDH mutations in gliomas. Brain Tumor Pathol. 2012;29(3):131–139. doi:10.1007/s10014-012-0090-4
16. Wiestler B, Capper D, Holland-Letz T, et al. ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol. 2013;126(3):443–451. doi:10.1007/s00401-013-1156-z
17. Nandakumar P, Mansouri A, Das S. The role of ATRX in glioma biology. Front Oncol. 2017;7. doi:10.3389/fonc.2017.00236
18. Chen WJ, He DS, Tang RX, Ren FH, Chen G. Ki-67 is a valuable prognostic factor in gliomas: evidence from a systematic review and meta-analysis. Asian Pacific J Cancer Prevent. 2015;16(2):411–420. doi:10.7314/APJCP.2015.16.2.411
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.