Back to Journals » Cancer Management and Research » Volume 13
Imaging Features and Prognostic Value of FDG PET/CT in Patients with Intravascular Large B-Cell Lymphoma
Authors Lim CH, Yoon SE, Kim WS, Lee KH, Kim SJ ![]()
Received 20 July 2021
Accepted for publication 9 September 2021
Published 21 September 2021 Volume 2021:13 Pages 7289—7297
DOI https://doi.org/10.2147/CMAR.S330308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Chae Hong Lim,1 Sang Eun Yoon,2 Won Seog Kim,2 Kyung-Han Lee,3,4 Seok Jin Kim2,4
1Department of Nuclear Medicine, Soonchunhyang University College of Medicine, Seoul, Korea; 2Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 3Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 4Department of Health Sciences and Technology, Samsung Advanced Institute for Health Sciences and Technology, Sungkyunkwan University, Seoul, Korea
Correspondence: Seok Jin Kim
Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, Korea
Tel +82-2-3410-1766
Fax +82-2-3410-1754
Email [email protected]
Kyung-Han Lee
Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, Korea
Tel +82-2-3410-2630
Fax + 82-2-3410-2638
Email [email protected]
Purpose: The clinical value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) in intravascular large B-cell lymphoma (IVLBCL) is unknown. This study investigated the association between PET/CT features and prognosis in IVLBCL patients.
Patients and Methods: Subjects were 30 newly diagnosed Asian variant IVLBCL patients at a single institution. Baseline PET/CT was analyzed for the distribution and intensity of FDG lesions, and PET/CT pattern groups were compared for the outcome.
Results: Eight patients had hypermetabolic lymph node (LN) lesions (Nodal group). The remaining 22 patients with extranodal (EN) involvement were categorized into Deauville score 3– 4 (EN/DS3-4; n = 14) and DS5 groups (EN/DS5; n = 8). First-line therapy resulted in a complete or partial response in 75.0%, 64.3%, and 100% of the respective groups. Treatment-related deaths occurred in one nodal group and three EN/DS3-4 group cases, but none among the EN/DS5 group. During 56 months of follow-up, disease progression or relapse occurred in five, four, and one case of respective groups. Cancer-related death occurred more frequently in the Nodal (n = 6) and EN/DS3-4 groups (n = 7) than the EN/DS5 group (n = 1; P = 0.041). Nodal and EN/DS3-4 groups had worse 5-year event-free survival (EFS; 25.0% and 49.0%, respectively, P = 0.010 and 0.076) and overall survival (OS; 33.3% and 48.2%, P = 0.010 and 0.068) compared to the EN/DS5 group (87.5% EFS and 87.5% OS).
Conclusion: In patients with Asian variant IVLBCL, the distribution and intensity of FDG uptake lesions on PET/CT can be useful for predicting treatment outcomes and survival.
Keywords: intravascular lymphoma, 18F-fluorodeoxyglucose, PET/CT, prognosis
Introduction
Intravascular large B-cell lymphoma (IVLBCL) is a rare type of extranodal lymphoma that is recognized to be distinct from diffuse large B-cell lymphoma (DLBCL).1 The disease is characterized by malignant lymphoma cells proliferating inside small vessels.2 Patients with the Western variant generally experience skin rash and neurological deficits, whereas those with the Asian variant often demonstrate fever and hemophagocytic lymphohistiocytosis, which can mimic an autoimmune or infectious disease.3 These highly variable clinical manifestations and nonspecific laboratory findings complicate timely diagnosis of IVLBCL.2 Furthermore, patients with the Asian variant often present with stage IV disease from bone marrow and/or liver involvement and have elevated serum lactate dehydrogenase, which results in greater International Prognostic Index (IPI) score.4 This makes it important to promptly diagnose and stratify prognosis in patients with this rare but aggressive disease.
18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) is an essential tool for lymphoma staging and response assessment. Studies have previously reported increased FDG uptake in organs with Asian variant IVLBCL involvement.5 Elevated FDG uptake can reveal bone marrow involvement undetected by CT.6 Other reports have described additional atypical patterns of FDG lesions.7,8 However, systemic analysis of FDG PET/CT features in IVLBCL has been limited by the rarity of the disease. Importantly, it remains unknown whether PET/CT findings could be helpful for predicting patient outcomes.
Herein, we analyzed FDG PET/CT features of 30 patients newly diagnosed with the Asian variant IVLBCL and investigated the prognostic value of the PET/CT patterns.
Patients and Methods
Study Subjects
In this single-center study, we retrospectively reviewed the PET/CT findings of IVLBCL patients and investigated the association between patterns of lesion FDG uptake and outcomes after first-line treatment. Study candidates were 46 patients newly diagnosed with IVLBCL at our institution between January 2001 and December 2018, who had been the subjects of a previous study.9 Of these candidates, 30 who had a complete set of FDG PET/CT image data for analysis were included. IVLBCL was confirmed by histopathological criteria in all cases, including CD20-positive neoplastic B cells with large cell morphology and intravascular or sinusoidal proliferation. This study was approved by the Samsung Medical Center Institutional Review Board (IRB: 2021-01-106), and the requirement for informed consent was waived.
Study Design
Electronic medical records were reviewed for clinical characteristics at diagnosis and archived work-up data included Ann Arbor stage, IPI score, serum biochemistry, chest and abdominal pelvis CT findings, and bone marrow aspiration/biopsy results. CT and PET/CT provided evidence of involved organs at diagnosis and of relapse or progression. Central nervous system (CNS) involvement was determined by cerebrospinal fluid analysis and brain/spine magnetic resonance imaging (MRI).
After first-line treatment with R-CHOP (rituximab, cyclophosphamide, vincristine, and prednisone), the treatment response was assessed by CT and PET/CT. Intrathecal or intravenous methotrexate was added for CNS involvement.9 Patients who responded to first-line treatment were monitored every three to six months for the first two years and every six to 12 months thereafter. Disease progression on imaging studies was noted regardless of immediate treatment for progression. The last survival and disease status update was collected in August 2020.
FDG PET/CT and Image Analysis
All patients fasted for at least six hours, and blood glucose was <150 mg at the time of imaging with a Discovery LS or a Discovery STE PET/CT scanner (GE Healthcare) at 60 min after injecting 5.0 MBq/kg of FDG. Continuous spiral CT was performed without intravenous or oral contrast on an 8-slice (140 keV; 40–120 mA; Discovery LS) or 16-slice helical CT (140 keV; 30–170 mA; Discovery STE). Emission scans were obtained from the skull base to the thigh for 4 min per frame in 2-D mode (Discovery LS) or 2.5 min per frame in 3-D mode (Discovery STE). PET images were reconstructed with CT attenuation correction by an ordered-subsets expectation maximization (OSEM) algorithm with 28 subsets and 2 iterations (matrix 128 × 128, voxel size 4.3×4.3 × 3.9 mm, Discovery LS) or an OSEM algorithm with 20 subsets and 2 iterations (matrix 128 × 128, voxel size 3.9×3.9 × 3.3 mm).
PET/CT images were analyzed on an Advantage Workstation 4.4 (GE Healthcare, Chicago, IL) by a board-certified nuclear medicine physician blinded to all clinical information except biopsy results. PET/CT images were evaluated for FDG-avid lymph node (LN) and extra-nodal (EN) lesions, and any FDG uptake greater than the surrounding tissue and that was unrelated to physiologic/benign uptake was considered positive. Brain lesions were not covered in our protocol. The intensity of lesion FDG uptake in each patient was graded by Deauville score (DS), and the maximum standardized uptake value (SUVmax) of FDG-avid lesions and biopsy-proven organs was calculated from 3D volumes-of-interest. This was done as follows: SUVmax = C (kBq/mL)/ID (kBq)/body weight (kg), where C is the tissue activity concentration measured by PET and ID is the injected dose.
Statistical Analyses
Patients with different PET/CT patterns were compared for FDG parameters and clinical factors using Pearson’s chi-square tests, Fisher’s exact tests, and Mann–Whitney U-tests. Event-free survival (EFS) was calculated from the date of diagnosis to the day of disease progression, relapse, any death, or last follow-up. Overall survival (OS) was calculated from the date of diagnosis to any death, or last follow-up. Survival curves were generated using the Kaplan–Meier method, and survival rates were compared using the Log rank test. Median follow-up was calculated using a reverse Kaplan–Meier survival curve, which was constructed by reversing “censor” and “event”.10 All statistical tests were two-sided with significance level set at 0.05 and were performed with SPSS 23.0 (SPSS Inc., Chicago, IL, USA) and MedCalc 15.5 (MedCalc, Mariakerke, Belgium).
Results
Clinical Characteristics
The cohort of 30 patients had a median age at diagnosis of 62 years (range: 52–82 y) and 56.7% were males. Fever was the most common presenting symptom, and 20 patients had B symptoms (66.7%). Eighteen had bone marrow involvement, eight had CNS involvement, and 12 had hemophagocytic lymphohistiocytosis. Twenty-three (76.7%) and 18 (60.0%) were high risk based on IPI and NCCN-IPI scores, respectively (Table 1).
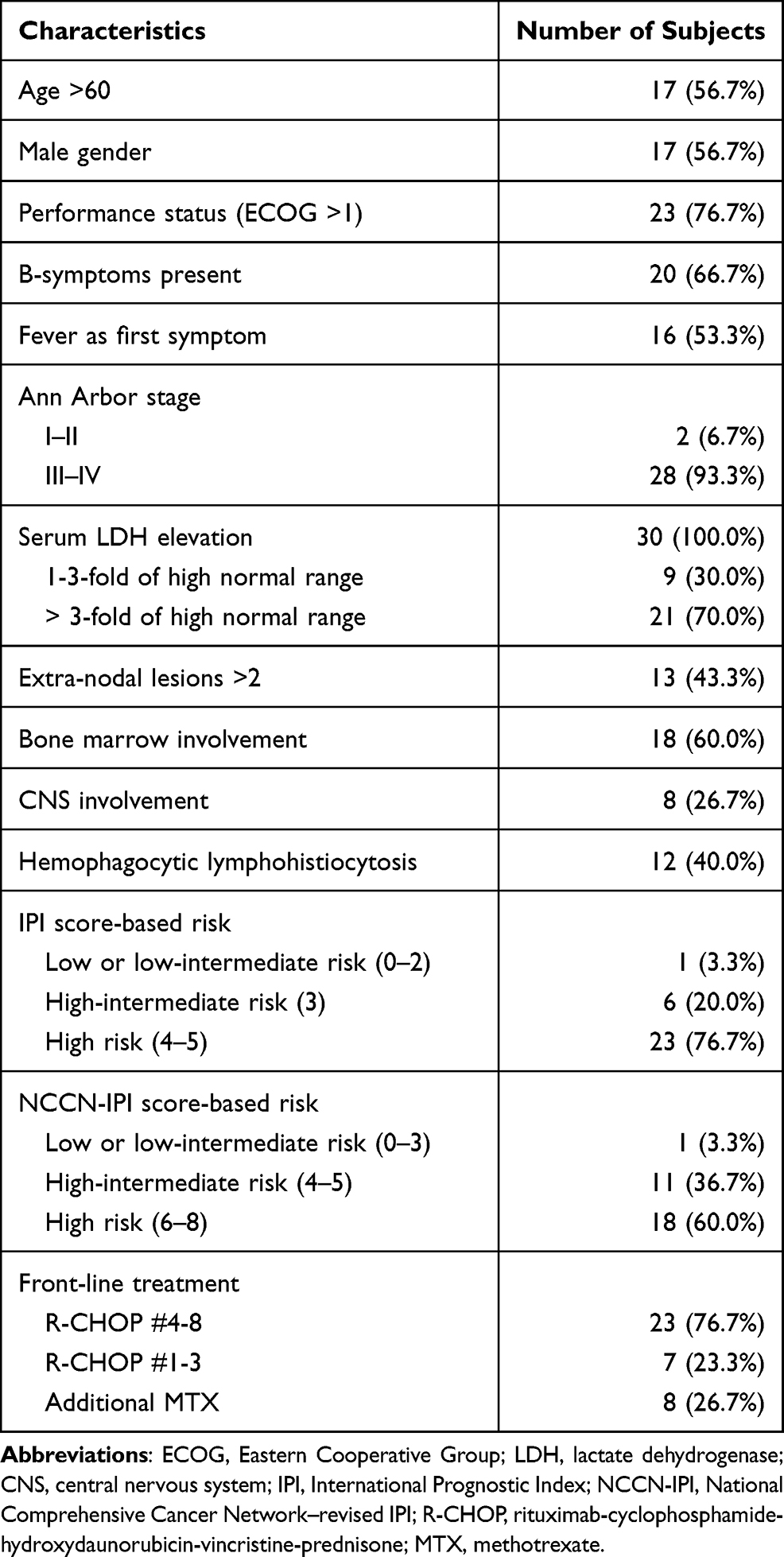 |
Table 1 Clinical Characteristics of 30 Study Subjects at Presentation |
FDG PET/CT Patterns
A major finding of this study was that 26.7% of the cohort (n = 8) had multiple LN lesions with high FDG uptake (DS 5; Figure 1A). The hypermetabolic lymphadenopathy was extensive (>10 LNs) in four and moderate (5–10 LNs) in four of the cases. IVLBCL involvement in the LNs was confirmed by biopsy in one of the former and two of the latter cases. This finding is significant since LN involvement represents IVLBCL extravasation. We categorized subjects with hypermetabolic LN lesions as a separate Nodal group.
 |
Figure 1 Maximum intensity projection (MIP) FDG PET/CT images of representative IVLBCL patients of the Nodal and EN/DS5 groups. (A) A 59-year-old patient (left) and a 52-year-old patient (right) with hypermetabolic LN involvement. (B) A 69-year-old patient with high-uptake involvement of the bone marrow and spleen (left) and a 70-year-old patient with high-uptake involvement of the liver and spleen (right). |
The remaining 22 subjects had EN involvement only. An obvious PET/CT pattern in these subjects was magnitude of lesion FDG uptake. Based on DS, eight subjects were categorized as the EN/DS5 group (Figure 1B) and 14 as the EN/DS3-4 group (Figure 2).
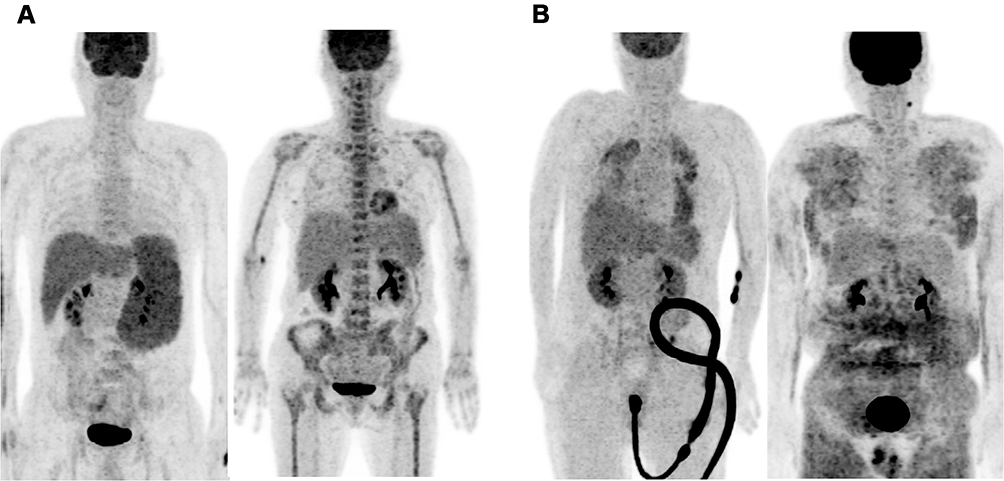 |
Figure 2 MIP FDG PET/CT images of representative IVLBCL patients of the EN/DS3-4 group. (A) A 56-year-old patient with spleen involvement (left) and a 64-year-old patient with bone marrow involvement (right). (B) A 57-year-old patient with lung bone marrow and spleen involvement (left) and a 61-year-old patient with skin and subcutaneous involvement (right). |
Clinical Characteristics According to PET/CT Pattern
The clinical characteristics of the three PET/CT groups are summarized in Table 2. The Nodal group (n = 8) had hypermetabolic lesions in LNs, lung, liver, spleen, and bone marrow. Uptake was highest in most frequent LN lesions (75.0%). The EN/DS5 group (n = 8) had strong hypermetabolic lesions in the bone marrow, liver, spleen, adrenal gland, heart, kidney, and uterus. The patient SUVmax ranged from 8.0 to 23.5, and FDG uptake was highest most frequently in bone marrow lesions (50.0%).
 |
Table 2 Comparison of Clinical Characteristics and FDG Uptake Between PET/CT Groups |
The EN/DS3-4 group (n = 14) displayed diffuse (n = 11) or diffuse/focal lesions (n = 3) with mild (DS3; n = 3) or moderately increased FDG uptake (DS4; n = 11). Diffuse lesions were identified in bone marrow or major organs, and diffuse/focal lesions were found in the liver (n = 1) or lungs (n = 2). The patient's SUVmax was lower than that of the Nodal and EN/DS5 groups (range, 3.0 to 6.1; P < 0.001), and uptake was highest most frequently in liver or bone marrow lesions (50.0%). The three groups did not show significant differences in clinical characteristics including age, symptoms, LDH, hemophagocytic lymphohistiocytosis, CNS involvement, or NCCN-IPI score (Table 2).
FDG Uptake in Organs with Biopsy-Proven Involvement
FDG PET/CT findings for major organs with biopsy-confirmed involvement are summarized in Supplementary Table 1. This occurred in 17 cases with bone marrow involvement that included four cases of the Nodal group, five of the EN/D5 group, and eight of the EN/DS3-4 group. Liver involvement was confirmed with biopsy in 5 cases (1, 3, and 1 case of the respective groups), and lung involvement was biopsy-confirmed in 5 cases (1, 0, and 4 cases). Among these, SUVmax was highest for liver involvement (8.2 ± 4.5), followed by bone marrow (5.7 ± 4.2) and lung (4.5 ± 3.6). FDG uptake was focal in 5/17 bone marrow involvements, 2/5 liver, and 3/5 lung involvements (Supplementary table 1). SUVmax was higher in focal compared to diffuse lesions (Figure 3A and B), but the FDG level was variable overall, with some bone marrow and liver involvements failing to display obvious increased uptake (Figure 3B). Biopsy-confirmed lung involvements appeared as bilateral consolidations with moderate uptake (Figure 3A) or diffuse ground glass opacities (GGOs) with mild uptake (Figure 3B).
 |
Figure 3 Examples of fusion PET/CT of organs with biopsy-proven IVLBCL involvement. (A) Axial fusion PET/CT and PET images of a Nodal group patient with bilateral focal consolidative lung involvement (left) and an EN/DS5 group patient with focal liver and bone marrow involvement (right) showing intense FDG uptake (DS 5). (B) Axial fusion PET/CT and PET images of an EN/DS3-4 group patient with lung involvement showing bilateral diffuse GGOs with mild FDG uptake (left; DS 3) and another patient with liver involvement showing diffuse moderate FDG uptake (right; DS 4). |
Other biopsy-confirmed cases comprised one with hypermetabolic skin involvement (EN/DS3-4 group; Figure 2), two with kidney involvement (one each of EN/DS3-4 and EN/DS5 groups), two with spleen involvement (one each of EN/DS3-4 and EN/DS5 groups), and one with uterus involvement (EN/DS5 group). All spleen and kidney involvements showed diffuse uptake and were accompanied by organ enlargement.
Treatment Outcome According to PET/CT Pattern
All patients received R-CHOP as a first-line treatment with curative intent. Six to eight cycles were completed in 23 patients (76.7%), and 22 achieved complete response. The remaining case was in the EN/DS5 group, and the patient initially showed a partial response but reached complete remission after additional radiotherapy. The overall rate of complete remission was 75.0% for the Nodal group, 64.3% for the EN/DS3-4 group, and 100% for the EN/DS5 group (Table 3).
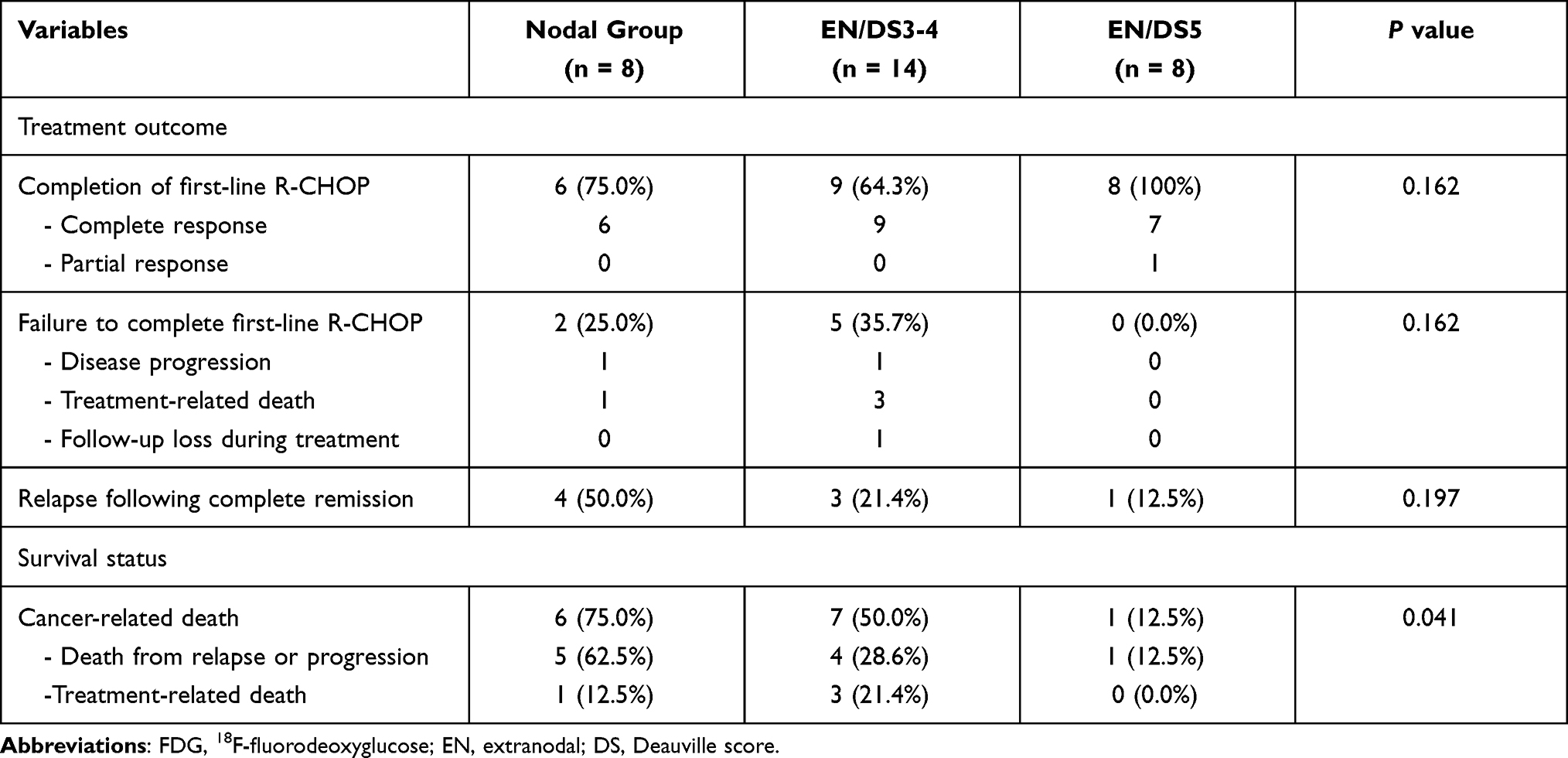 |
Table 3 Treatment Outcome and Survival Status According to FDG PET/CT Pattern |
Seven patients (23.3%) failed to complete chemotherapy due to CNS progression (one case each for the Nodal and EN/DS3-4 groups), fatal sepsis from pneumonia or pulmonary hemorrhage within two cycles (one Nodal and three EN/DS3-4 group cases; Supplementary Figure 1), or follow-up loss after the first cycle (one EN/DS3-4 group).
Following first-line treatment, recurrence occurred in four patients of the Nodal group, one of the EN/DS5 group, and three of the EN/DS3-4 group.
Survival According to PET/CT Pattern
During a median follow-up of 56 months (interquartile range: 41–75 months), there were 14 cancer-related deaths (46.7%). Ten of these cases had disease progression or relapse during or following treatment. Four deaths were treatment-related, including three in the EN/DS3-4 group (21.4% rate) and one in the Nodal group (12.5% rate). Cancer-related deaths occurred significantly more frequently in the Nodal (75.0%) and EN/DS3-4 groups (50.0%) compared to the EN/DS5 group (12.5%; P = 0.041; Table 3).
Survival analyses revealed that 5-year EFS was worse for Nodal (25.0%, P = 0.010) and EN/DS3-4 groups (49.0%, P = 0.076) compared to the EN/DS5 group (87.5%; Figure 4A). The 5-year OS also was worse for the Nodal (33.3%, P = 0.010) and EN/DS3-4 groups (48.2%, P = 0.068) compared to the EN/DS5 group (87.5%; Figure 4B). In additional analysis using NCCN-IPI, a known prognostic factor of lymphoma, neither 5-year EFS (48.1% versus 58.3%, P = 0.678; Figure 4C) nor 5-year OS (54.2% versus 55.6%, P = 0.618; Figure 4D) showed significant differences between patients with high and low to intermediate risk scores.
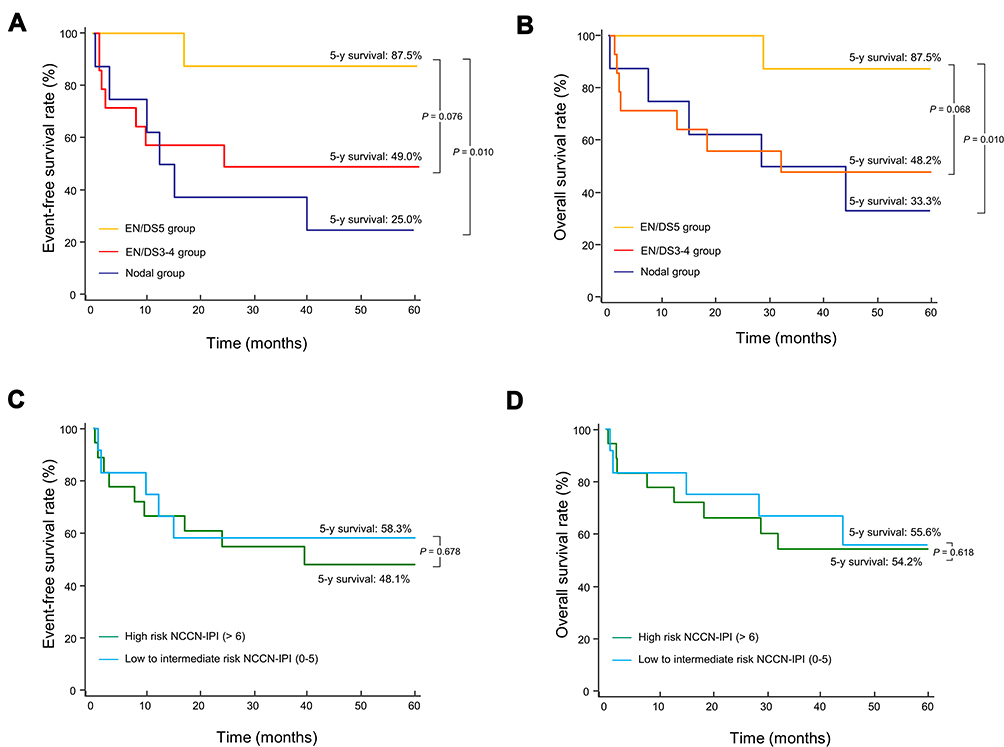 |
Figure 4 Kaplan–Meier curves for survival. Event-free survival rate (A) and overall survival rate (B) for the Nodal group, EN/DS3-4 group, and EN/DS5 group. Event-free survival rate (C) and overall survival rate (D) according to NCCN-IPI scores (high and low to intermediate risk). |
Discussion
The World Health Organization classifies IVLBCL as a distinct DLBCL subtype.1 FDG PET/CT is a well-established measure for staging and monitoring treatment response in DLBCL.11 Due to the limited number of cases, clinical knowledge of PET/CT findings of IVLBCL is limited to anecdotal case reports. In this study, we describe detailed FDG PET/CT features of 30 newly diagnosed Asian variant IVLBCL patients from a single institute.
The results revealed that 26.7% of the study cohort displayed prominent hypermetabolic lymphadenopathy, and the LN biopsy in three of these cases verified IVLBCL involvement. This finding is significant because, in contrast to the nodal predilection of DLBCL, IVLBCL characteristically disseminates to EN sites,12 while LN involvement represents extravasation by more aggressive disease.13 We therefore categorized patients with hypermetabolic lymphadenopathy as a separate Nodal group.
A second feature that can be used for subject grouping is lesion FDG intensity, which is linked to patient outcomes in many types of B cell lymphomas.14 Unlike DLBCL, which consistently has high FDG uptake,15 IVLBCL lesions in our patients displayed variable levels of FDG uptake. Biopsy was used to verify IVLBCL involvement in many of the suspected EN organs. Given these findings, we divided patients with EN involvement, but without LN lesions into DS3-4 and DS5 groups.
Compared to the EN/DS5 group that showed highly hypermetabolic focal lesions, PET/CT features of the EN/DS3-4 group were remarkable in that many involved organs displayed a diffuse pattern of mild-to-moderate uptake, similar to that seen in inflammatory or infectious disease.16 This was most frequent in the bone marrow and liver. Lung involvement in the EN/DS3-4 group appeared as bilateral diffuse GGOs with mild uptake or diffuse consolidations with moderate uptake. Given the non-specific symptoms and laboratory findings of IVLBCL,17 the presence of such PET/CT findings could be useful for selecting diagnostic biopsy sites.
Importantly, survival analysis revealed that patients with hypermetabolic LN lesions had worse treatment outcomes and survival compared to patients with high FDG-uptake EN lesions. This result is consistent with the recognition that LN involvement represents extravasated IVLBCL with more aggressive behavior.13
However, patients in the EN/DS3-4 group who had EN disease with mild-to-moderate uptake had worse survival outcomes compared to those with high FDG uptake in EN lesions. Indeed, the EN/DS5 group demonstrated excellent 5-year EFS and OS. While the survival advantage of this group is not explained readily, complete response to first-line chemotherapy was achieved in all subjects of this group, except for one case with partial response. This contrasts to the Nodal and EN/DS3-4 groups that showed only 75.0% and 64.3% partial or complete response, respectively. The remaining subjects in the latter groups either progressed or died during treatment. A similar good treatment response associated with high tumor FDG uptake was reported previously for non-Hodgkin’s lymphoma.18 Together, our findings suggest that Asian variant IVLBCLs with high glycolytic metabolism respond better to R-CHOP chemotherapy, and this could contribute to more favorable treatment outcomes and patient survival.
In our study, patients of the EN/DS3-4 group had worse survival than those of the EN/DS5 group and were prone to treatment-related death (21.4%). As an example, an EN/DS3-4 group patient with lung involvement died of pulmonary hemorrhage following rituximab infusion at the first cycle (Supplementary Figure 1). Thus, while the overall 13.3% rate of treatment-related deaths in our cohort is comparable to the 7.5% previously reported by Shimada et al,4 the rate was greater in the EN/DS3-4 group in our study. In this group, organs with diffuse moderate uptake might represent dilution of FDG intensity by IVLBCL cells that are spread across the tissue via small vessels.2 Such tissue spreading is likely to disturb vital organ function during and after treatment,19,20 causing treatment-related adverse events. A similar explanation was suggested for an inverse relationship between FDG intensity and prognosis in bile duct cancer with papillary or periductal infiltrating growth patterns.21
Together, our findings indicate that hypermetabolic LN lesions and diffuse mild-to-moderate organ uptake are associated with poor prognosis in IVLBCL patients. However, this study is limited by its retrospective design and relatively small number of study subjects due to the rarity of the disease. Prospective studies with larger numbers of subjects are required to confirm our findings.
Conclusions
FDG PET/CT features in IVLBCL patients include hypermetabolic LNs indicating extravasated disease, hypermetabolic lesions limited to EN sites, and diffuse bone marrow, liver, or lung involvement with mild-to-moderate uptakes. Patients with hypermetabolic LNs and those with diffuse mild-to-moderate organ uptake have significantly worse prognoses. Recognition of these PET/CT patterns can be useful for identifying IVLBCL patients at greater risk.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not include any studies with animals performed by any of the authors.
Informed Consent
Informed consent was waived by the institutional review board for this retrospective study.
Acknowledgments
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (NRF-2021R1A2C1007531), and the Soonchunhyang University Research Fund.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval for the version to be published, agreed to the submitted journal, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sabattini E, Bacci F, Sagramoso C, Pileri SA. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica. 2010;102(3):83–87.
2. Shimada K, Kinoshita T, Naoe T, Nakamura S. Presentation and management of intravascular large B-cell lymphoma. Lancet Oncol. 2009;10(9):895–902. doi:10.1016/s1470-2045(09)70140-8
3. Ponzoni M, Ferreri AJ, Campo E, et al. Definition, diagnosis, and management of intravascular large B-cell lymphoma: proposals and perspectives from an international consensus meeting. J Clin Oncol. 2007;25(21):3168–3173. doi:10.1200/JCO.2006.08.2313
4. Shimada K, Matsue K, Yamamoto K, et al. Retrospective analysis of intravascular large B-cell lymphoma treated with rituximab-containing chemotherapy as reported by the IVL study group in Japan. J Clin Oncol. 2008;26(19):3189–3195. doi:10.1200/jco.2007.15.4278
5. Hong JY, Kim HJ, Ko YH, et al. Clinical features and treatment outcomes of intravascular large B-cell lymphoma: a single-center experience in Korea. Acta Haematol. 2014;131(1):18–27. doi:10.1159/000351060
6. Ha JM, Kim E, Lee WJ, et al. Unusual manifestation of intravascular large B-cell lymphoma: severe hypercalcemia with parathyroid hormone-related protein. Cancer Res Treat. 2014;46(3):307–311. doi:10.4143/crt.2014.46.3.307
7. Hoshino A, Kawada E, Ukita T, et al. Usefulness of FDG-PET to diagnose intravascular lymphomatosis presenting as fever of unknown origin. Am J Hematol. 2004;76(3):236–239. doi:10.1002/ajh.20099
8. Yamashita H, Suzuki A, Takahashi Y, Kubota K, Kano T, Mimori A. Intravascular large B-cell lymphoma with diffuse FDG uptake in the lung by 18FDG-PET/CT without chest CT findings. Ann Nucl Med. 2012;26(6):515–521. doi:10.1007/s12149-012-0600-9
9. Yoon SE, Kim WS, Kim SJ. Asian variant of intravascular large B-cell lymphoma: a comparison of clinical features based on involvement of the central nervous system. Korean J Intern Med. 2020;35(4):946–956. doi:10.3904/kjim.2018.396
10. Shuster JJ. Median follow-up in clinical trials. J Clin Oncol. 1991;9(1):191–192. doi:10.1200/JCO.1991.9.1.191
11. Barrington SF, Mikhaeel NG. PET scans for staging and restaging in diffuse large B-cell and follicular lymphomas. Curr Hematol Malig Rep. 2016;11(3):185–195. doi:10.1007/s11899-016-0318-1
12. McDonough SP, Van Winkle TJ, Valentine BA, vanGessel YA, Summers BA. Clinicopathological and immunophenotypical features of canine intravascular lymphoma (malignant angioendotheliomatosis). J Comp Pathol. 2002;126(4):277–288. doi:10.1053/jcpa.2002.0553
13. Thomas CA, Guileyardo JM, Krause JR. An intravascular lymphoma with extravascular tendencies. Proc Bayl Univ Med Cent. 2014;27(4):341–343. doi:10.1080/08998280.2014.11929153
14. Ngeow JYY, Quek RHH, Ng DCE, et al. High SUV uptake on FDG-PET/CT predicts for an aggressive B-cell lymphoma in a prospective study of primary FDG-PET/CT staging in lymphoma. Ann Oncol. 2009;20(9):1543–1547. doi:10.1093/annonc/mdp030
15. Schoder H, Noy A, Gonen M, et al. Intensity of 18 fluorodeoxyglucose uptake in positron emission tomography distinguishes between indolent and aggressive non-Hodgkin’s lymphoma. J Clin Oncol. 2005;23(21):4643–4651. doi:10.1200/jco.2005.12.072
16. Long NM, Smith CS. Causes and imaging features of false positives and false negatives on F-PET/CT in oncologic imaging. Insights Imaging. 2011;2(6):679–698. doi:10.1007/s13244-010-0062-3
17. Liew CL, Shyu WC, Tsao WL, Li H. Intravascular lymphomatosis mimics a cerebral demyelinating disorder. Acta Neurol Taiwan. 2006;15(4):264–268.
18. Spaepen K, Stroobants S, Dupont P, et al. Prognostic value of positron emission tomography (PET) with fluorine-18 fluorodeoxyglucose ([18F]FDG) after first-line chemotherapy in non-Hodgkin’s lymphoma: is [18F]FDG-PET a valid alternative to conventional diagnostic methods? J Clin Oncol. 2001;19(2):414–419. doi:10.1200/jco.2001.19.2.414
19. Liu B, Ezeogu L, Zellmer L, Yu B, Xu N, Joshua Liao D. Protecting the normal in order to better kill the cancer. Cancer Med. 2015;4(9):1394–1403. doi:10.1002/cam4.488
20. Cheok CF. Protecting normal cells from the cytotoxicity of chemotherapy. Cell Cycle. 2012;11(12):2227–2228. doi:10.4161/cc.20961
21. Yi HK, Park YJ, Bae JH, et al. Inverse prognostic relationships of (18) F-FDGPET/CT metabolic parameters in patients with distal bile duct cancer undergoing curative surgery. Nucl Med Mol Imaging. 2018;52(5):334–341. doi:10.1007/s13139-018-0542-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.