")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Identification of Significant Predictors for the Need of Insulin Therapy and Onset of Postpartum Impaired Glucose Tolerance in Gestational Diabetes Mellitus Patients
Authors Wang T, Yin W, Huang Y, Zhang Q
Received 4 March 2021
Accepted for publication 21 April 2021
Published 10 June 2021 Volume 2021:14 Pages 2609—2617
DOI https://doi.org/10.2147/DMSO.S309618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Ting Wang,1,2 Wei Yin,3 Yonghan Huang,2 Qingxue Zhang1
1Department of Reproductive Medicine Center, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Reproductive Medicine Center, The First People’s Hospital of Foshan(Affiliated FoShan Hospital of Sun Yat-sen University), Foshan, People’s Republic of China; 3Department of Obstetrics, Guangzhou Women and Children’s Center, Guangzhou, People’s Republic of China
Correspondence: Qingxue Zhang Email [email protected]
Background: Gestational diabetes mellitus (GDM) during pregnancy can greatly increase the risk for a number of adverse prenatal and postpartum consequences, including postpartum impaired glucose tolerance (IGT). Determining the need for insulin therapy is critical for controlling the glycemic level in GDM patients. The study contains two major purposes: 1) to identify the potential predictors for the need of insulin therapy in GDM patients; 2) to identify the factors that are related to the onset of postpartum IGT.
Materials and Methods: Here, we performed a retrospective study on 112 GDM patients in China to identify the significant predictors for the need of insulin therapy and onset of postpartum IGT in patients with GDM.
Results: Age and gestational weeks at GDM diagnosis, pregestational BMI, family history of diabetes mellitus (DM), plasma glucose levels assessed by 75-g OGTT at both the 1-hour and 2-hour time points (PG-1h and PG-2h) and HbA1c level were all significantly different between the patients that received insulin therapy and those did not. During postpartum, family history of DM, PG-1h PG-2h and HbA1c level were found to be significantly different between the patients with normal glucose tolerance and those with IGT.
Conclusion: Our results reveal a number of factors that are closely associated with the need of insulin therapy and onset of postpartum IGT, especially the PG-1h and PG-2h levels. These findings will provide valuable indications on selection of treatment strategy for GDM and GDM-induced postpartum IGT.
Keywords: insulin, glucose, diabetes, pregnancy, postpartum
Background
Gestational diabetes mellitus (GDM) is a condition, in which a woman experiences high blood sugar levels without prior diabetes history. It is a common medical complication associated with pregnancy, especially in elderly women (age above 65) with maternal obesity and physical inactivity.1 Presence of GDM during pregnancy has been reported to greatly increase the risk of pre-eclampsia and the need for labor induction, as well as cesarean section.2 GDM also increases the risk of diabetes mellitus (DM) onset in the mother. Over 10% of women with GDM acquired impaired glucose tolerance (IGT) shortly after delivery, where 20 to 60% of them developed into DM within 5 to 10 years after pregnancy.3 Babies born to mothers with poorly managed GDM have a higher tendency of being overweight, experiencing low blood sugar and acquiring jaundice and type 2 diabetes.2 Therefore, it is critical to strictly control the maternal blood sugar level during pregnancy.
Medical diet therapy and exercise are the primary treatments for GDM. If these treatments fail to restore the normal glycemic level, insulin therapy should be initiated. However, exogenous insulin has been reported to produce significant effects on the placental and fetal development, including placental weight, cord width and baby weight.4 Therefore, it is important to define the criteria for the initiation of insulin therapy.
In the present study, we performed a retrospective study on GDM patients admitted at our institution to identify the patient characteristics and diagnostic factors that are necessary for the initiation of insulin therapy and the onset of postpartum IGT.
Methods
Ethics Approval and Consent to Participate
The study was approved by the ethical committee of Sun Yat-Sen Memorial Hospital of Sun Yat-Sen University and Guangzhou Women and Children's Center (2013–093546) and was conducted in accordance with the Declaration of Helsinki. Verbal consent for participating the study was obtained from each patient at the time of diagnosis. The purpose and design of the study was carefully explained to all individual participants accompanied by their close relatives before verbal consent was obtained according to the guidance provided by the ethical committee. Verbal consent was selected due to the limited writing ability of some participants. This procedure has been approved by the ethical committee.
Patients
112 female patients with GDM administered at Sun Yat-Sen Memorial Hospital and Guangzhou Women and Children's Center from 2014 to 2019 were enrolled in the present study. GDM was diagnosed based on the criteria set by the International Association of Diabetes and Pregnancy Study Groups via a two-step screening.5 Pregnant women with geriatric pregnancy (pregnancy over age of 35), pre-gestational obesity, history of GDM and macrosomia, large for gestational age, glycosuria or a casual plasma glucose level greater than 5.6 mmol/L were subjected to a 75-g oral glucose tolerance test (OGTT) at their first visit to the hospital. Pregnant women without the above-mentioned risk factors or with a normal 75-g OGTT were subjected to a 1-hour (1h) 50-g oral glucose challenge test between 24 and 28 weeks-of-gestation. If the test result exceeded 7.8 mmol/L, a diagnostic 75-g OGTT was followed to confirm the onset of GDM. GDM was diagnosed if at least one tested value was greater than a fasting glucose level of 5.1 mmol/L, a 1-h glucose level of 10 mmol/L or a 2-h glucose level of 8.5 mmol/L in the 75-g OGTT.
Patients with overt diabetes during pregnancy or a history of type 1 or type 2 DM before pregnancy were excluded from the study. Dietary therapy was conducted at 30 kcal/kg body weight based on the body mass index (BMI) of 22 kg/m2 supplemented with 200 kcal. The 112 patients were separated into two groups: the insulin therapy group (n=59) and the diet therapy only group (n=53).
Guidelines for insulin treatment in clinical practice were followed as previously described.6 Specifically, insulin therapy was initiated when systematic fasting glucose concentrations were greater than 5.3 mmol/L and/or 1h post-prandial glucose concentrations were greater than 7.8 mmol/L. In case of established GDM, insulin therapy was initiated when asymmetric fetal macrosomia and/or increased amniotic fluid were observed. Insulin pumps were not used for GDM treatment. Initiation of insulin therapy was not dependent on gestational age.
Measurements
Assessed patient data include age and gestational weeks at GDM diagnosis, history of gestation and pregnancy, pre-gestational and maximum BMI, family history of DM, prior GDM history, plasma glucose levels, and the number of abnormal 75-g OGTT values at GDM diagnosis. A urine test was performed for each patient during their first visit to the hospital. Level of fasting plasma glucose, glycated hemoglobin (HbA1c), fasting immunoreactive insulin (IRI) and ketone bodies were recorded. Plasma glucose was measured by an electronic blood glucose meter. HbA1c and insulin were measured by enzyme-linked immunosorbent assay (ELISA). The level of ketone bodies of negative, ±, 1+, 2+, 3+ and 4+ were scored as 0, 0.5, 1, 2, 3 and 4, respectively. Levels of plasma glucose and IRI were assessed by a postpartum 75-g OGTT at 0, 30, 60, 90 and 120 min. Homeostatic model assessment for insulin resistance (HOMA-IR), β-cell function and the insulinogenic index were calculated as previously described.7 Specifically, formula for HOMA-IR was fasting glucose (mg/dL) × fasting IRI (μU/mL)/405; formula for β-cell function was fasting IRI (μU/mL) × 360/fasting glucose (mg/dL) − 63; formula for insulinogenic index was fasting IRI (μU/mL)/30-min glucose (mg/dL) − fasting glucose (mg/dL).
Statistical Analysis
All statistical analysis was performed with the SPSS16.0 software. A P-value <0.05 was considered as statistical significance. Data were presented as mean ± standard error. Unpaired t-test, Mann–Whitney U-test and χ2-test were used to analyze between-group differences for continuous variables, ordinal variables and categorical variables, respectively. Multivariate logistic regression analysis was performed with selected independent variables that were identified to be significantly different in the univariate analysis. Logistic regression model was applied to predict the need for insulin therapy and progression of IGT, considering of all the variables that exhibit statistical significance. Bootstrapping was applied to validate the prediction models as previously described.8,9 Receiver operating characteristic (ROC) curve analysis was performed to identify clinical factors that can predict the need for insulin therapy.
Results
Patient Characteristics
The 112 patients were divided into the diet and insulin group depending on whether insulin therapy was initiated. Collected patient characteristics of the two groups are summarized in Table 1. Gestational age for all included patients was 22.78±0.72 weeks. A significant difference was observed in both the age and the gestation length at the time of GDM diagnosis between the two groups. Values for history of pregnancy and gestation were similar between the two groups. In term of BMI, only the BMI value measured at the pre-gestational stage, but not the BMI at 20-years-of-age or the maximal BMI, was significantly different between the two groups. In addition, weight gain during pregnancy was also significantly lower for patients in the insulin group. Moreover, significantly more patients in the insulin group were found to have a family history of DM compared to the diet group; while the number of patients with GDM history was similar between the two groups. 75-g OGTT at GDM diagnosis revealed a significant difference in the plasma glucose level at the 1-hour and 2-hour time points between the two groups (PG-1h and PG-2h). Furthermore, patients in the insulin group had significantly more abnormal 75-g OGTT values than the patients in the diet group. Levels of fasting plasma glucose and HbA1c were both significantly increased in the patients from the insulin group. On the other hand, fasting IRI, urinal ketone bodies, insulin resistance and β-cell function were all similar between the two groups. The coefficients of variation of fasting IRI and insulin resistance were 0.068 versus 0.148 and 0.070 versus 0.083, respectively.
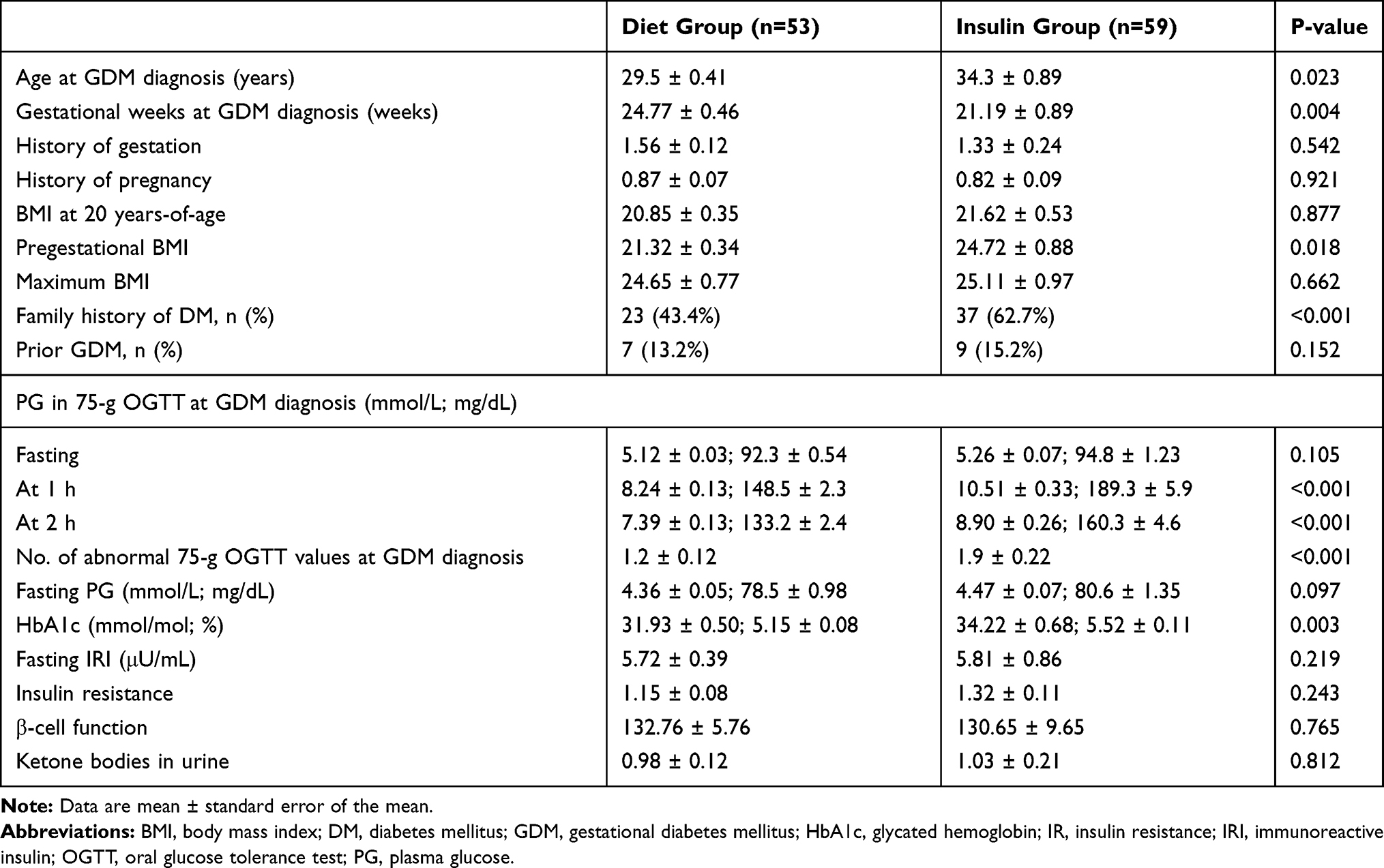 |
Table 1 Characteristics of the GDM Patients in the Diet and Insulin Groups |
Risk Factors Predicting the Need for Insulin Therapy
To identify the clinical factors that correlate with the need for insulin therapy, we performed logistic regression analysis on the variables that were found to be significantly different between the insulin and diet groups (Table 2). PG-1h and PG-2h were found to be the significant predictor for the need of insulin therapy with an odds ratio of 1.035 and 1.006, respectively. We further applied logistic regression model using all the variables found to be significantly different between the two groups to predict the need for insulin therapy and revealed the same outcome (Table 3). Removal of PG-1h and PG-2h from the model did not add any predictive values to other variables (Table 3). Then, we performed ROC curve analysis on the two plasma glucose levels to determine the cut-off values and revealed a value of 9.8 mmol/L (177.4 mg/dL) and 8.6 mmol/L (154.5 mg/dL), respectively (Table 4).
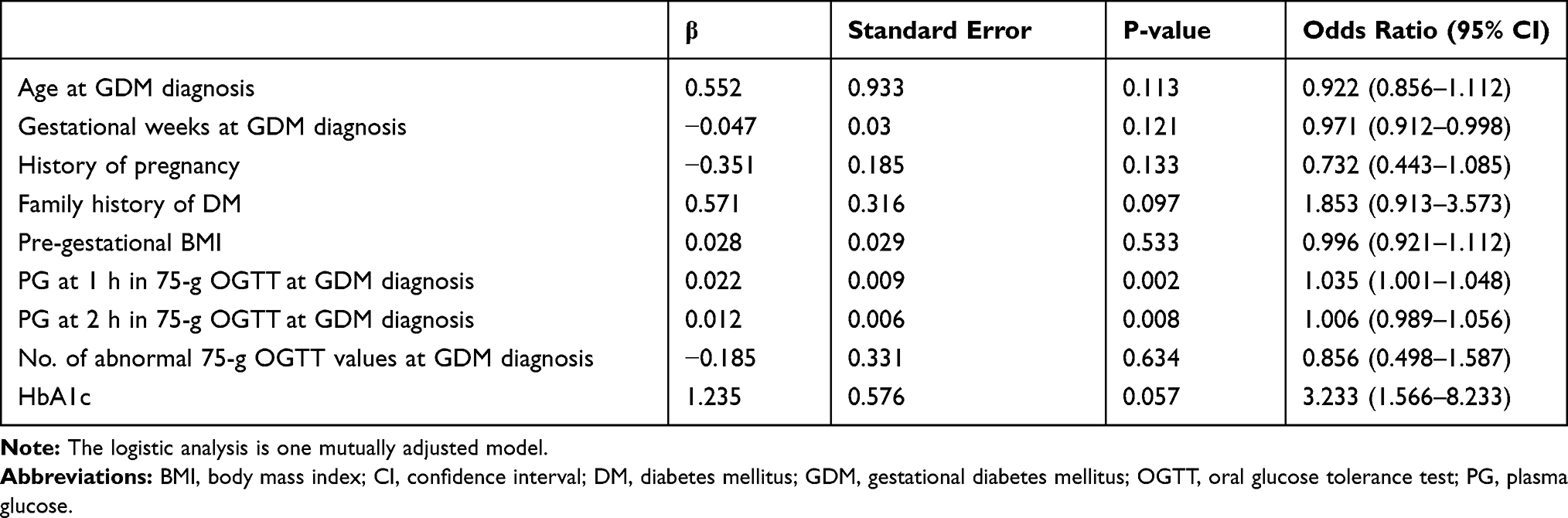 |
Table 2 Logistic Regression Analysis of the Variables That Were Significantly Different Between the Diet and Insulin Groups |
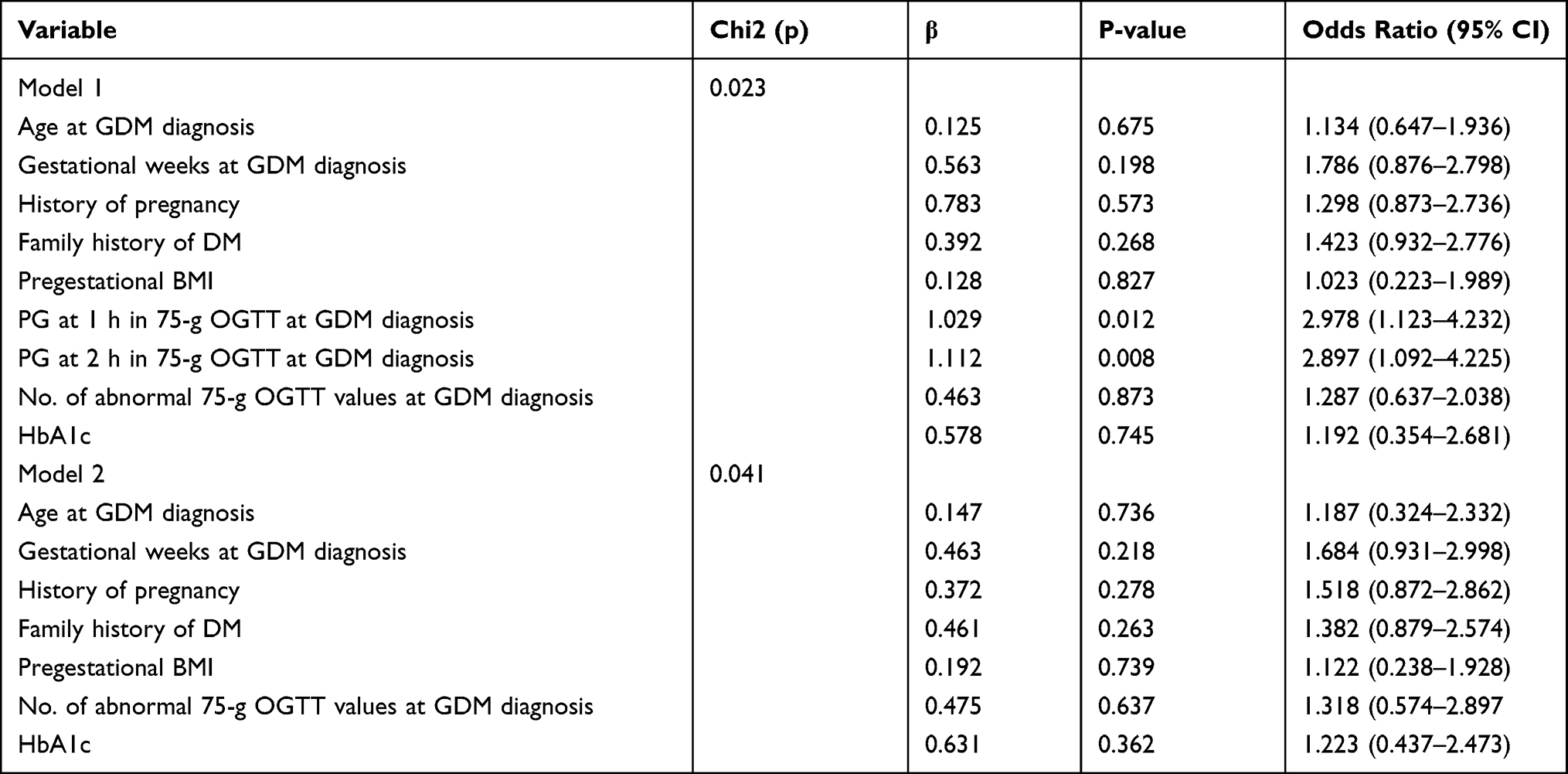 |
Table 3 Logistic Regression Models of Insulin Treatment, Considering All the Variables Found to Be Significantly Different Between the Diet and Insulin Groups |
 |
Table 4 ROC Curve Analysis of PG-1h and PG-2h Between the Diet and Insulin Groups |
Postpartum 75-g OGTT Analysis
A postpartum 75-g OGTT was performed on the same 112 patients at the 6 to 10-week of the postpartum period. Based on the standard glucose level set for DM diagnosis,10 the patients were re-divided into two groups: the normal glucose tolerance (NGT) group (n=93) and the IGT group (n=19) (Table 5). Age and gestational length at the time of GDM diagnosis, history of gestation and pregnancy and all assessed BMI values were all similar between the two groups. 18 out of 19 patients in the IGT group had a family history of DM, whereas only half of the patients in the NGT group had such a history. Percentage of patients with prior GDM was similar between the two groups. PG-1h and PG-2h, but not fasting PG at the time of GDM diagnosis were significantly higher in the IGT group compared to the NGT group. Based on the values of fasting glucose, none of the patients suffered from impaired fasting glucose. Logically, the number of abnormal 75-g OGTT values was also significantly higher in the IGT group. In addition, level of HbAc1 was significantly higher in the patients from the IGT group.
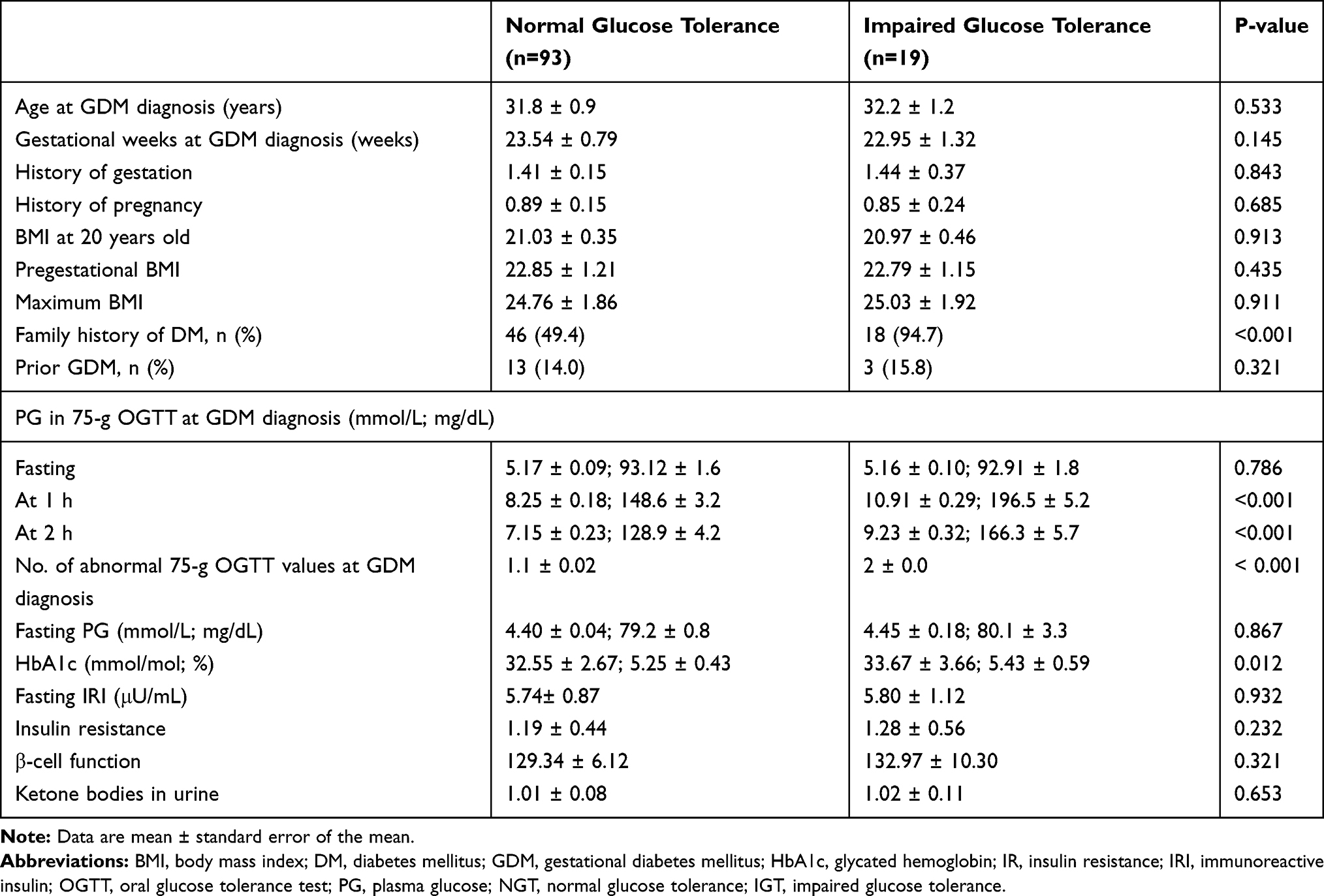 |
Table 5 Characteristics of the GDM Patients in the NGT and IGT Groups |
Risk Factors Predicting the Onset of IGT
To identify the clinical factors that indicate the development of IGT, we performed logistic regression analysis on the variables that were found to be significantly different between the NGT and the IGT groups (Table 6). Same as the predicting factors for the need of insulin therapy, prenatal PG-1h and PG-2h were also identified as significant predictors for the onset of IGT, with an odd ratio value of 1.043 and 1.001, respectively. We further applied logistic regression model using all the variables found to be significantly different between the two groups to predict the development of IGT and revealed the same outcome (Table 7). Removal of PG-1h and PG-2h from the model did not add any predictive values to other variables (Table 7). ROC curve analysis revealed a cut-off value of 10.0 mmol/L (180.5 mg/dL) and 7.9 mmol/L (142.3 mg/dL) for the two factors, respectively (Table 8).
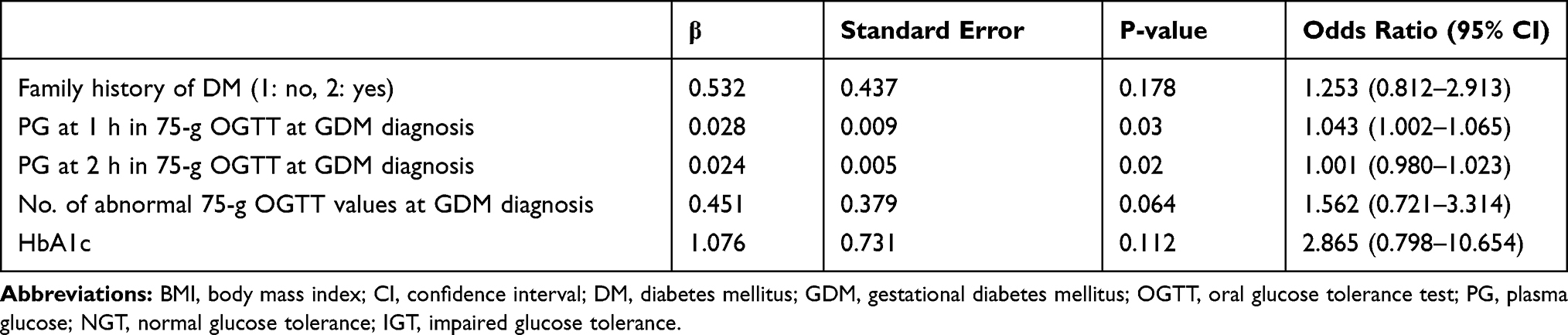 |
Table 6 Logistic Regression Analysis of the Variables That Were Significantly Different Between the NGT and IGT Groups |
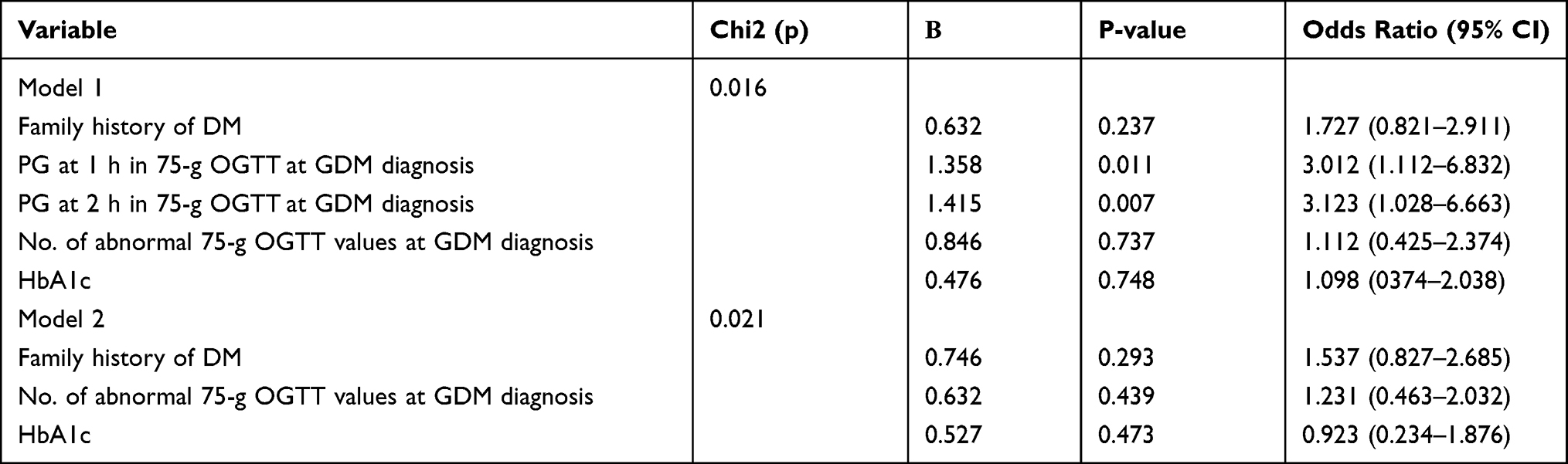 |
Table 7 Logistic Regression Models of Progression to IGT, Considering All the Variables Found to Be Significantly Different Between the NGT and IGT Groups |
 |
Table 8 ROC Curve Analysis of PG-1h and PG-2h Between the NGT and IGT Groups |
Discussion
Poor management of GDM during pregnancy can lead to severely adverse perinatal outcomes for both the mother and the baby, including higher risk of developing type 2 diabetes in later life. Therefore, careful treatment of GDM during pregnancy to keep the glycemic level under control is crucial for the pregnant women. Dietary therapy is the first line of treatment for GDM. If failed, insulin therapy will be needed. In the present study, we performed a retrospective study on 112 pregnant women with GDM to identify the risk factors that can be used to predict the need for insulin therapy and the onset of postpartum IGT. We show that PG-1h and PG-2h are significant predictors for both situations.
Previous studies have suggested that only PG-1h, but not PG-2h was an independent predictor for the need of insulin therapy.11–13 In addition, gestational weeks at the time of GDM diagnosis and the HbA1c level were also shown to be the prediction factor for insulin therapy.12 Both risk factors also appear to be significantly different between the insulin and diet groups, although the significance lost was lost in the logistic regression. This could be due to the limited patient number or the differently analyzed patient population, where all those previous studies were performed on pregnant women from Japan while our study is the first one performed on pregnant women from China. Indeed, ethnicity has been suggested to be a key factor that affects the prediction for the need of insulin therapy.14 Previous study performed on Japanese women with GDM to identify the risk factors associated with early postpartum abnormal glucose tolerance has shown that a lower insulinogenic index and use of insulin therapy are closely associated under such situation.15 In contrast, studies carried out on Swedish women have identified HbA1c and fasting glucose values in the upper normal range during pregnancy, as well as a family history of diabetes and previous pregnancies as risk factors for GDM.16,17 Recently, a study performed on an Italian population suggested a role of ethnicity in both attendance for postpartum follow-up and its outcome.18 Taken together, these results suggest that GDM diagnosis criteria may better be used in an ethnicity-specific manner.
In addition, multiple studies performed on Indian population suggest that urgent needs are required to focus on GDM care to improve the maternal and fetal outcomes,19–21 which can also serve as an indication for other developing countries. Specifically, glucose tolerance status of urban and rural GDM patients at 6 weeks to 1 year postpartum from Tamil Nadu in southern India (WINGS 6) showed that a BMI value above 25 kg/m2 was significantly associated with postpartum dysglycemia.19
Other possible predicting factors, such as pregestational BMI, maternal age and family history of diabetes have also been implicated as potential predicting factors.22–24 Although these factors were not identified in the present study as significant predicting factors for insulin therapy, they were all found to be significantly different between the diet and insulin groups. In addition, gestational weeks at GDM diagnosis and HbA1c level were also significantly different between the two groups. PG-1h and PG-2h were also identified as the only significant predictors for postpartum IGT, indicating that these two factors are indeed critical for GDM-induced glucose levels.
The underlying mechanism for GDM involves impaired pancreatic β‐cell function, resulting in increased insulin resistance during pregnancy. Surprisingly, homeostatic model assessment for insulin resistance, β-cell function and the insulinogenic index did not reveal any significant predictors for either insulin therapy or postpartum IGT, since the fasting glucose and IRI levels did not differ. The reason behind this unexpected phenomenon is unclear. However, our results are in line with a previous study conducted on a Japanese population, where none of the three parameters were identified as predictors either.12 It is likely that severe insulin resistance might not be a necessary factor for the onset of GDM in Asian women. One possible underlying reason is that increased fasting glucose levels are characteristics of overweight/obese subjects; however, the population of women in the present study are close to normal body weight.
In China, the GDM economic burden is significant from a short-term point of view and requires further consideration and awareness. Previous study has indicated the necessity for the incorporation of GDM prevention and care policies at the national level to relieve such burdens.25 In line with this, the present study is the first one performed on GDM patients from a Chinese population. Generally, the findings are in line with the previous studies performed on Japanese population.11–13,15 It is worth noting that high postprandial glucose levels rather than high fasting glucose levels were shown to contribute to excess hyperglycemia in Asian type 2 diabetic patients.26 Besides heath values, socio-demographic factors have also been proposed to be correlated with postpartum glucose screening, including whether they were a first-time mother, the perceived susceptibility score, the perceived seriousness score and the perceived benefit score.27 Therefore, family history of GDM could also be a significant factor that affects glucose screening in GDM patients.
There are several potential limitations need to be considered for the present study. First, the retrospective nature of the present study on patients treated at a single cohort might generate possible selection bias. The included patient number is also limited. Further studies with bigger sample size on patients of different ethnicity and treated at different institutions are required. Second, despite of the simple and minimal invasive nature to predict fasting steady-state glucose and insulin levels, the HOMA indices are only rough measures of insulin resistance and insulin secretion that require further validation with other methods, such as quantitative insulin sensitivity check index (QUICKI); although it has been validated during pregnancy.28 Third, although we have encouraged the patients to monitor their glucose level using the self-monitoring of blood glucose (SMBG) method, this information was not well documented for the purpose of this study. Fourth, a few other factors, such as weight gain during pregnancy and level of physical activity were not assessed.
Conclusions
In summary, PG-1h and PG-2h are significant predictors for both the need of insulin therapy and onset of postpartum IGT in GDM patients. Therefore, extreme care should be taken for these parameters in pregnant women diagnosed with GDM.
Abbreviations
GDM, gestational diabetes mellitus; IGT, impaired glucose tolerance; DM, diabetes mellitus; PG-1h and PG-2h, plasma glucose levels assessed by 75-g OGTT at both the 1-hour and 2-hour time points; OGTT, oral glucose tolerance test; HbA1c, glycated hemoglobin; IRI, fasting immunoreactive insulin; ROC, receiver operating characteristic; BMI, body mass index; NGT, normal glucose tolerance.
Funding
This study was funded by Medical Science and Technology Research Fund of Guangdong Province of China (B2019133).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farrar D. Hyperglycemia in pregnancy: prevalence, impact, and management challenges. Int J Womens Health. 2016;8:519–527. doi:10.2147/IJWH.S102117
2. Hartling L, Dryden DM, Guthrie A, Muise M, Vandermeer B, Donovan L. Benefits and harms of treating gestational diabetes mellitus: a systematic review and meta-analysis for the U.S. Preventive services task force and the national institutes of health office of medical applications of Research. Ann Intern Med. 2013;159(2):123–129. doi:10.7326/0003-4819-159-2-201307160-00661
3. Buchanan TA, Xiang AH, Page KA. Gestational diabetes mellitus: risks and management during and after pregnancy. Nat Rev Endocrinol. 2012;8(11):639–649. doi:10.1038/nrendo.2012.96
4. Arshad R, Karim N, Ara Hasan J. Effects of insulin on placental, fetal and maternal outcomes in gestational diabetes mellitus. Pak J Med Sci. 2014;30(2):240–244. doi:10.12669/pjms.302.4396
5. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(7):676–682. doi:10.2337/dc10-0719
6. Anastasiou E, Farmakidis G, Gerede A, et al. Clinical practice guidelines on diabetes mellitus and pregnancy: iotaI. Gestational diabetes mellitus. Hormones (Athens). 2020.
7. Matthews DR, Hosker JP, Rudenski,AS, et al. Homeostasis model assessment: insulin resistance and beta‐cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi:10.1007/BF00280883
8. Francis EC, Li M, Hinkle SN, et al. Adipokines in early and mid-pregnancy and subsequent risk of gestational diabetes: a longitudinal study in a multiracial cohort. BMJ Open Diabetes Res Care. 2020;8(1):e001333. doi:10.1136/bmjdrc-2020-001333
9. Zhu Y, Tsai MY, Sun Q, et al. A prospective and longitudinal study of plasma phospholipid saturated fatty acid profile in relation to cardiometabolic biomarkers and the risk of gestational diabetes. Am J Clin Nutr. 2018;107(6):1017–1026. doi:10.1093/ajcn/nqy051
10. Association. AD. Classification and diagnosis of diabetes. Diabetes Care. 2017;40(Supplement 1):S11–S24. doi:10.2337/dc17-S005
11. Ito Y, Shibuya M, Hosokawa S, et al. Indicators of the need for insulin treatment and the effect of treatment for gestational diabetes on pregnancy outcomes in Japan. Endocr J. 2016;63(3):231–237. doi:10.1507/endocrj.EJ15-0427
12. Nishikawa T, Hashimoto S, Kinoshita H, et al. One‐hour oral glucose tolerance test plasma glucose at gestational diabetes diagnosis is a common predictor of the need for insulin therapy in pregnancy and postpartum impaired glucose tolerance. J Diabetes Investig. 2018;9(6):1370–1377. doi:10.1111/jdi.12848
13. Watanabe M, Katayama A, Kagawa H, Ogawa D, Wada J. Risk factors for the requirement of antenatal insulin treatment in gestational diabetes mellitus. J Diabetes Res. 2016;2016:9648798. doi:10.1155/2016/9648798
14. Pertot T, Molyneaux K, Tan K, et al. Can common clinical parameters be used to identify patients who will need insulin treatment in gestational diabetes mellitus? Diabetes Care. 2011;34(10):2214–2216. doi:10.2337/dc11-0499
15. Kugishima Y, Yasuhi I, Yamashita H, et al. Risk factors associated with abnormal glucose tolerance in the early postpartum period among Japanese women with gestational diabetes. Int J Gynaecol Obstet. 2015;129(1):42–45. doi:10.1016/j.ijgo.2014.09.030
16. Claesson R, Ignell C, Shaat N, Berntorp K. HbA1c as a predictor of diabetes after gestational diabetes mellitus. Prim Care Diabetes. 2017;11(1):46–51. doi:10.1016/j.pcd.2016.09.002
17. Ekelund M, Shaat N, Almgren P, Groop L, Berntorp K. Prediction of postpartum diabetes in women with gestational diabetes mellitus. Diabetologia. 2010;53(3):452–457. doi:10.1007/s00125-009-1621-3
18. Dalfra MG, Burlina S, Del Vescovo GG, Anti F, Lapolla A. Adherence to a follow-up program after gestational diabetes. Acta Diabetol. 2020;57(12):1473–1480. doi:10.1007/s00592-020-01564-y
19. Bhavadharini B, Mahalakshmi MM, Anjana RM, et al. Prevalence of gestational diabetes mellitus in urban and rural Tamil Nadu using IADPSG and WHO 1999 criteria (WINGS 6). Clin Diabetes Endocrinol. 2016;2(1):8. doi:10.1186/s40842-016-0028-6
20. Kale SD, Yajnik CS, Kulkarni SR, et al. High risk of diabetes and metabolic syndrome in Indian women with gestational diabetes mellitus. Diabet Med. 2004;21(11):1257–1258. doi:10.1111/j.1464-5491.2004.01337.x
21. Mahalakshmi MM, Bhavadharini B, Kumar M, et al. Clinical profile, outcomes, and progression to type 2 diabetes among Indian women with gestational diabetes mellitus seen at a diabetes center in south India. Indian J Endocrinol Metab. 2014;18(3):400–406. doi:10.4103/2230-8210.131205
22. Aktun LH, Yorgunlar B, Karaca N, et al. Predictive risk factors in the treatment of Gestational diabetes mellitus. Clin Med Insights Womens Health. 2015;8:25–28. doi:10.4137/CMWH.S31564
23. Meshel S, Schejter E, Harel T, et al. Can we predict the need for pharmacological treatment according to demographic and clinical characteristics in gestational diabetes? J Matern Fetal Neonatal Med. 2016;20(13):2062–2066. doi:10.3109/14767058.2015.1077225
24. Sapienza AD, Francisco RPV, Trindade,TC, et al. Factors predicting the need for insulin therapy in patients with gestational diabetes mellitus. Diabetes Res Clin Pract. 2010;88:81–86. doi:10.1016/j.diabres.2009.12.023
25. Xu T, Dainelli L, Yu K, et al. The short-term health and economic burden of gestational diabetes mellitus in China: a modelling study. BMJ Open. 2017;7(12):e018893. doi:10.1136/bmjopen-2017-018893
26. Wang JS, Tu ST, Lee IT, et al. Contribution of postprandial glucose to excess hyperglycaemia in Asian type 2 diabetic patients using continuous glucose monitoring. Diabetes Metab Res Rev. 2011;27(1):79–84. doi:10.1002/dmrr.1149
27. Liu ZY, Zhao JJ, Gao LL, Wang AY. Glucose screening within six months postpartum among Chinese mothers with a history of gestational diabetes mellitus: a prospective cohort study. BMC Pregnancy Childb. 2019;19.
28. Lapolla A, Dalfra MG, Mello G, et al. Early detection of insulin sensitivity and beta-cell function with simple tests indicates future derangements in late pregnancy. J Clin Endocrinol Metab. 2008;93(3):876–880. doi:10.1210/jc.2007-1363
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.