Back to Journals » Infection and Drug Resistance » Volume 15
Identification of NS5B Resistance-Associated Mutations in Hepatitis C Virus Circulating in Treatment Naïve Vietnamese Patients
Received 11 December 2021
Accepted for publication 23 March 2022
Published 5 April 2022 Volume 2022:15 Pages 1547—1554
DOI https://doi.org/10.2147/IDR.S353605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Thu Kim Nguyen,1,2 Duyet Van Le1
1Clinical Laboratories, National Hospital for Tropical Diseases, Hanoi, Vietnam; 2Infectious Department, Hanoi Medical University, Hanoi, Vietnam
Correspondence: Duyet Van Le, Tel +84936647979, Email [email protected]
Introduction: Treatment of HCV infection with peginterferon and ribavirin results in a low sustained virologic response rate, but has a number of undesirable adverse effects. Direct-acting antivirals (DAAs) offer a high efficacy, low risk, and a short treatment time. However, the existence of resistance-associated mutations, particularly in the NS5B polymerase, can attenuate the efficacy of DAAs. The objective of this study was to identify amino acid changes in the NS5B gene linked to DAA resistance in treatment-naive Vietnamese chronic hepatitis C patients.
Methods: Blood samples and treatment data were collected from 100 HCV-infected patients hospitalized at the National Hospital for Tropical Diseases between January and December 2020; the plasma was then isolated and stored at – 80°C for molecular analysis. The NS5B gene fragments of 100 samples were amplified with specified primers and the nucleotide sequences were obtained using the Sanger sequencing system. The nucleotide sequences were then analyzed and compared to identify substitutions in the NS5B region.
Results: A total of 100 HCV isolates from patients were classified into three genotypes, including genotypes 1, 3, and 6. The NS5B sequence analysis revealed many amino acid mutations in all genotypes, although these mutations were not strongly associated with resistance to DAAs like S282T. Analytical data on ribavirin–resistance mutations revealed that Q309R was predominantly found in genotype 1a, D310N was mostly found in genotype 1b, and N244I, T329I, A333E were not observed. The following mutations were shown to be related with DAAs resistance: E237G, S282R, L320F, V321A, and V321I. Furthermore, NS5B-resistance mutations were not associated with clinical characteristics, long-term virological response, or improvements in clinical parameters (liver enzymes or liver fibrosis index).
Conclusion: Although NS5B mutations were found in treatment-naive Vietnamese patients, changes in the NS5B gene did not appear to be highly correlated with HCV ribavirin and DAA antiviral resistance.
Keywords: HCV, resistance mutations, ribavirin, DAAs, sustained viral response
Introduction
In Vietnam, the prevalence of HCV was estimated to be around 2%.1 Among those at high risk, drug users (87%) and blood transfusions (54%) were notably high, as were hemodialysis patients (54%) and patients with hemophilia (29%).2 According to previous data, one–third of HCV–infected patients would develop liver cirrhosis and hepatocellular carcinoma.3,4 Previously, the HCV treatment regimen was based on a combination of peg-interferon (peg-IFN) and ribavirin (RBN). However, variable response rates with the combination regimen of peg-IFN and RBV were observed due to the diverse genotypes and subtypes of HCV.5 Recently, our understanding of the HCV life cycle has advanced to the point that various molecules that inhibit multiple HCV targets, such as an NS3 protease inhibitor, NS5A inhibitors, and NS5B polymerase inhibitors, have been licensed for HCV treatment.6 Direct-acting antiviral agents were given to these compounds (DAAs). Several DAAs are being developed to target the NS5B polymerase enzyme (viral RNA-dependent RNA polymerase – RdRp), which is a key component in the HCV infection and life cycle. Nucleoside inhibitors (NIs) and non-nucleoside inhibitors (NNIs) are two types of NS5B inhibitors.7 These inhibitors function at different stages of the HCV life cycle. Previously, sofosbuvir (an NI inhibitor) was developed and licensed as a part of a combination antiviral therapy for the treatment of HCV infection.8
Despite the effectiveness of DAAs, treatment for HCV infection has become exceedingly successful, with over a 90% sustained virological response (SVR) rate and low adverse effects, especially in the cases where peg-IFN/RBV treatment had failed.9 However, due to the fast propagation rate of the HCV life cycle, low polymerase fidelity, immune system pressure, and selective drug therapy, roughly 5–10% of HCV-infected individuals fail the DAAs regimen, resulting in drug resistance-associated variants (RAVs) in the HCV population.10 The DAAs were created to target proteins like NS3, NS5A, and NS5B that that control HCV RNA replication. Many studies have found that HCV is susceptible to develop DAA resistance when RAVs are present.11–13 Recently, a substantial number of mutations with varied degrees of resistance to DAAs have been discovered.6 The variants cause the development of quasispecies,14 leading in decreased DAA efficacy. This is a factor that has been linked to HCV treatment failure.
HCV antiviral drug resistance has become a public health problem in the diagnosis and treatment of people with chronic hepatitis C, based on experience with other chronic viral infections. The characteristics of distinct resistance mutations are extensively established, according to previous laboratory and clinical evidence.6 It is becoming increasingly crucial to improve treatment efficacy in individuals treated with diverse regimens for each genotype infection, especially with the presence of natural RAVs of HCV in DAA-naive patients. This is the premise for the diagnosis and treatment of chronic hepatitis C patients effectively. Therefore, the aim of this study was to explore the presence of ribavirin and DAA resistance-associated variants to NS5B inhibitors in the Hepatitis C virus circulated in treatment-naive Vietnamese patients.
Materials and Methods
Patients and Samples
A total of 100 participants with HCV infection for more than 6 months, with or without clinical manifestations, anti-HCV positivity and HCV RNA quantification, without or with cirrhosis of the liver were recruited from different population groups. These participants were visited and hospitalized at the National Hospital for Tropical Diseases in Hanoi from Jan to Dec 2020. Blood samples from the participants were taken (4–5 mL), thereafter the plasma was separated and stored at −80 °C for further experiments. All participants who agreed to participate in the study were given detailed information and signed written informed consent forms. The study was approved by the Ethics Committee of the National Hospital for Tropical Diseases (approval number 61/HDDD-NDTW) and performed in accordance with the Declaration of Helsinki.
Determination of HCV Viral Load
A total of 100 clinical samples from anti-HCV positive participants were tested for viral load using the commercial kit COBAS/TaqMan HCV Test v2.0. All operating procedures were completed in accordance with the manufacturer's instructions.
RNA Isolation and PCR Amplification of the NS5B Fragment
The plasma of participants that was collected previously was used for viral RNA isolation using Qiagen kits (QIAamp Viral RNA Mini Kit; Qiagen Sciences Germantown, MD, USA) according to the manufacturer’s instructions. Briefly, 140 µL of patient plasma was suspended in 560 µL of the given lysis buffer (Buffer AVL) containing an ARN carrier and incubated at room temperature for 10 minutes. Thereafter, 560 µL of ethanol was added and the sample was treated in accordance with the manufacturer’s protocol.
The application of the NS5B region was done by using one-step RT-PCR. The one-step RT-PCR was performed in a 50-µL reaction volume using SuperScript™ III One-Step RT-PCR System with Platinum™ Taq DNA polymerase (Invitrogen, Carlsbad, CA) with specific primers for the NS5B region: HCV-NS5B-F (5’-CNTAYGGITTCCARTACTCICC-3’), HCV-NS5B-R (5’-GAG GARCAIGATGTTATIARCTC-3’). The PCR reaction contained 25 µL Master mix, 0.4 µL MgSO4 (50 nmol), 2 µL Enzyme, 2 µL HCV-NS5B-F, 2 µL HCV-NS5B-R, 10 µL template RNA, and the final volume was made up to 50 µL with distilled water. The PCR reaction was performed in a ProFlex Thermal Cycler (Applied Biosystem) with a 105 °C heated lid. The cycling parameters were 1 cycle of 50 °C for 30 min (cDNA synthesis); 1 cycle of 95 °C for 3 min; followed by 40 cycles of 95°C for 30s, 58°C for 30 and 72°C for 1 min. PCR products were visualized and detected in a 1.5% agarose gel.
Sanger Sequencing
Dideoxy sequencing of PCR products of the NS5B gene fragment was performed using BigDye™ Terminator Chemistry v. 3.1 (Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s protocol. The sequencing reactions were performed using the HCV-NS5B-F and HCV-NS5B-R primers to replicate DNA fragments. Thereafter, the DNA fragments were purified and the sequences were read on the ABI 3130 Bio-analyzer (Applied Biosystems).
Sequence Analysis of the NS5B Region
The amino acid sequences of the NS5B region were obtained and analyzed using ATGC 7.2 software. Reference sequences of genotype 1 a, 1b, 3b, 6a, 6e, and 6h were collected from the GenBank nucleotide sequence database with accession numbers NC004102, EU181827, D49374, Y12083, KY608690, and KY608700, respectively. Target regions of the NS5B gene were analyzed for all isolates of HCV using MEGA (version 10.1.9) and ClustalX (version 2.2). The amino acid sequences were then compared with the original amino acid sequences of genotype 1a, 1b, 3b, 6a, 6e, and 6h for HCV isolates.
Rerults
The Genotype Distribution of HCV
The sequence analysis of the NS5B region in 100 blood samples from HCV-infected patients with viral load > 4×102 UI/mL, revealed three genotypes: 54 isolates for genotype 1 (42 isolates for 1a and 12 isolates for genotype 1b), two isolates for genotype 3b, and 46 isolates for genotype 6 (32 isolates for genotype 6a, 6 isolates for genotype 6e, and 6 isolates for genotype 6h) (Table 1). Furthermore, roughly 80% of the individuals with HCV infections were male.
 |
Table 1 The HCV Genotype and Gender Distribution of HCV Infected Patients |
Prevalence of Natural NS5B Resistance-Association Mutations
RASs (Resistance-Associated Substitutions) on NS5B polymerase were found in 11/13 amino acid mutations in all HCV isolates, as reported in previous studies.6,11,13 The natural NS5B RASs were most commonly presented in genotypes 1a, 1b, and 6a (Table 2), with a significant incidence of Q309R/W/K (25/42, 59.5%), C326S/L/P (66.6%), L329P/A (30.9%) in genotype 1a. The alterations at positions 273 and 282 were never found in genotype 1a. Furthermore, natural RASs were detected with a frequency of E237G (41.6%), D244R/L (33.3%), S282R (41.6%), and C316A (41.6%) in HCV genotype 1b. Of the 2 HCV isolates with genotype 3b, only two mutations were detected at positions E237S and D33D. At least 10/13 NS5B-RAS were detected in 20/32 HCV genotype 6a isolates, with a greater prevalence at positions N273R/S/K (62.5%), S329F/V/P (28.1%), and S333R (15.6%). The prevalence of NS5B RASs represented in genotypes 6e and 6h did not differ substantially from genotype 3b, with a frequency of S237N and V326A (genotype 6e), V244A, and T333A (genotype 6h).
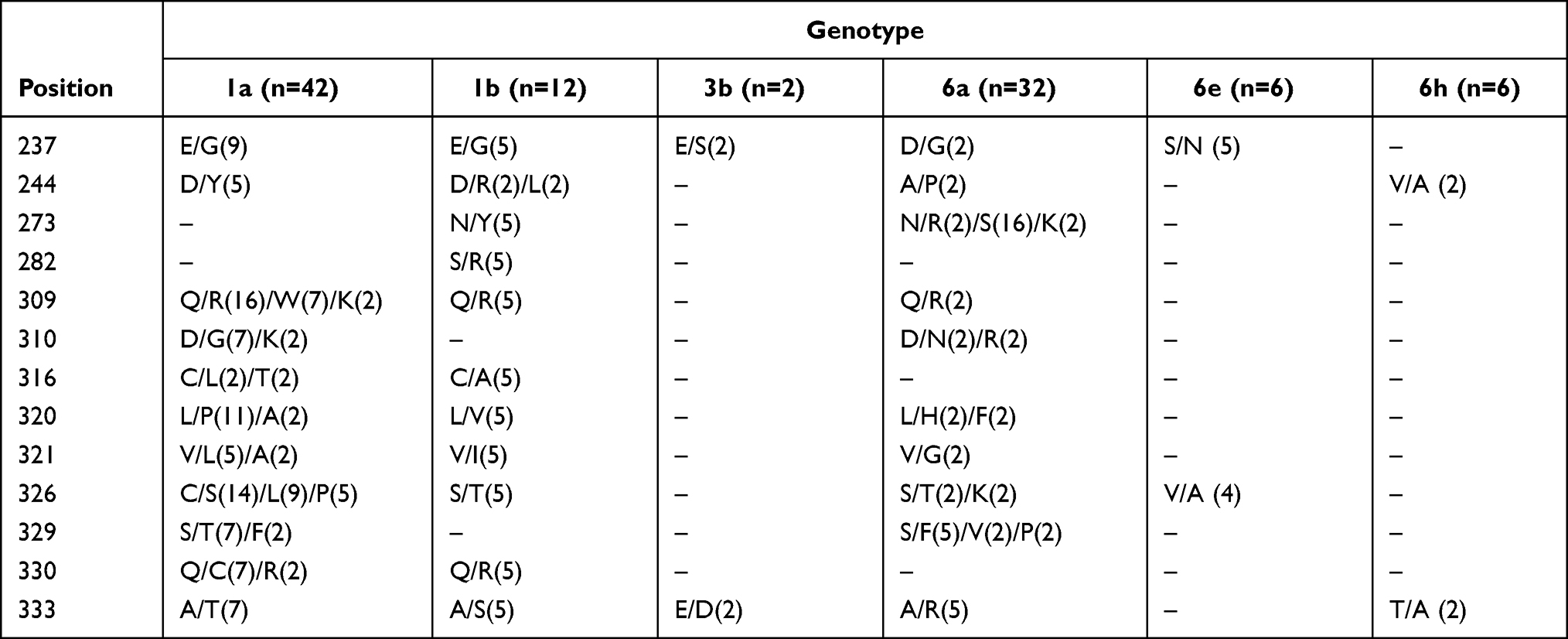 |
Table 2 Amino Acid Alterations in the NS5B Region of HCV Circulated in Treatment-Naive Vietnamese Patients |
Natural NS5B RASs were discovered as single mutations resistant to NS5B protein inhibitors (DAAs) in the 100 patients, including E237G (5%), L320F (2%), and V321A (2%) (Table 3). Among 16 strains with single mutation-associated resistance to ribavirin, the mutations of Q309R and D310N were present in 14/100 and 2/100 of the HCV isolates, respectively. In addition, five HCV isolates revealed multiple mutations in the NS5B region, with a prevalence of S282R + V321A (which confers resistance to DAAs) and E237G + S282R + Q309R + V321I being the most common (confers resistance to both sofosbuvir and ribavirin). In our patient cohort, no codon changes occurred at position S282T (strong resistance to sofosbuvir) and positions N244I, T329I, and A333E (reducing the susceptibility of the HCV to ribavirin). All common NS5B RASs to DAAs have been linked to ribavirin resistance in genotypes 1a and 6a, with mutations found in 16 HCV-infected patients. The detection of NS5B RASs at the same time was more common in genotype 1a patients (14/16, 87.5%), but just a few in genotype 6a patients (1/16, 12.5%). In genotype 1b and 6a, multiple NS5B RASs were discovered, with S282R + V321I in genotype 6a and E237G + S282R + Q309R + V321I in genotype 1b.
 |
Table 3 The Natural NS5B Resistance-Associated Substitutions Found in Naive Patients Exposed to NS5B Inhibitors and Their Treatment Regimen |
Treatment Regimens for HCV-Infected Patients
Nucleotide Inhibitors (NIs) or Nonnucleoside Inhibitors (NNIs) are RNA-dependent RNA polymerase (RdRp–NS5B) inhibitors that resemble natural NS5B-substrates, causing direct chain termination by tackling the NS5B active site. In this study, the treatment regimens were predominantly consisted of sofosbuvir combined with other inhibitors, with 14 patients receiving sofosbuvir/velpatasvir and two patients receiving sofosbuvir/ledipasvir (Table 4). Among the 32 patients with ribavirin-resistant mutations, 12 patients were treated with a regimen of sofosbuvir/velpatasvir/ribavirin and sofosbuvir/ledipasvir/ribavirin (dose of ribavirin: empiric weight-adjusted doses - 1000 mg/d for patients who weighed < or =75 kg and 1200 mg/d for patients who weighed >75 kg). The remaining patients were given a regimen of sofosbuvir/velpatasvir. A sofosbuvir/velpatasvir regimen was used to treat patient with multiple ND5B RASs.
 |
Table 4 Treatment Regimens for Patients with NS5B Resistance-Associated Substitutions |
SOF/VEL was the most common treatment regimen for patients. All of the patients were given 12 weeks of treatment. All nine patients with HCV strains resistant to DAAs were treated with SOF-containing medications; seven patients received the SOF/VEL regimen and two patients received the SOF/LED regimen. Six of the 16 HCV patients with ribavirin-resistant mutations were treated with the SOF/VEL/RIB and SOF/LED/RIB RIB regimens, while the remaining ten patients were treated with the SOF/VEL regimen. The SOF/VEL combo was used to treat five patients with HCV strains that contained various resistance mutations.
Before therapy, all of the 100 patients with HCV-infection who were chosen for the inhibitor regimen as indicated above had viral load of >400 IU/mL. After starting the antiviral regimen, 94/100 (94%) of the patients had a viral load below the quantitative threshold (<1.5 IU/mL), achieving a virological response quickly at the 4th week, and 100% of patients had a viral load below the quantitative threshold (<1.5 IU/mL) after 12 weeks of treatment, achieving a sustained virological response. After 24 weeks of treatment, all HCV-RNA patients had obtained a relapse-free, sustained response (Table 5).
 |
Table 5 Evolution of Clinical Indicators Before and After Antiviral Therapy |
All patients in our study cohort had elevated liver enzymes prior treatment, but 77 cases had ALT and AST return to normal baseline by the fourth week of treatment, and 33 cases had elevated liver enzymes after treatment, the majority of whom were HCV-infected patients with mutations resistant to DAAs (Table 5). Only two After patients had liver enzymes that were greater than the usual baseline after 12 weeks of treatment, and after 24 weeks of treatment, all 100 patients had normal liver enzymes.
Before treatment, only 2 patients had APRI values of < 0.5 (liver fibrosis level F0-F1), 48 patients had APRI scores of 0.5-<1.0 (liver fibrosis level F2), 41 cases had APRI scores of 1.0 - <2.0 (liver fibrosis level F3), and 9 cases had APRI score of > 2.0 (liver fibrosis level F4). The number of patients with ARPI scores of < 0.5 increased from 2 to 18 cases after 4 weeks of treatment, 55 patients after 12 weeks, and 94 patients after 24 weeks (Table 5). Only six patients had scored from 0.5 - <1.0 and no cases showed a score > 1.0. Patients with NS5B resistance-associated substitution and HCV-infected patients with no mutation had similar APRI scores.
Discussion
Resistant Mutations in NS5B to Ribavirin
New inhibitor regimens for the treatment of HCV infection have recently achieved significant progress in terms of efficacy and safety, particularly with DAAs. DAA based regimens fail to eradicate HCV in 1–10% of patients, despite being more successful and safer than PEG-IF/Ribavirin therapy. The establishment of resistance mutations, according to recent studies, is one of the primary factors contributing to treatment failure in these patients. There have never been any studies in Vietnam to look for medication resistance-associated mutations in HCV-infected patients who have failed to respond to treatment. The prevalence of NS5B RASs in HCV genotype 1, 3, and 6 infected DAA-naive patients in Vietnam is reported in this study.
In our study cohort of treatment-naive patients, the Q309R mutation was discovered in 16% of the patients across all HCV genotypes, with genotype 1a and 1b being the most common. Furthermore, the D310N mutation was detected, primarily in genotypes 1a and 6a. In HCV-infected patients, however, the N244I, T329I, and A33E mutations were not detected, even as a modest alteration. The Q309R mutation appeared with a significant frequency in genotype 1a (54.1%) and was less prevalent in genotype 1b, according to the Brazilian study (9%).15 A D310N mutation was also found in 7.2% of HCV isolates. The Q309R mutation was observed in 28.57% of HCV isolates in the South African cohort, but the N244I, D310N, and T329E variants were not detected in any isolates. As a result, the presence of Q309R alteration imparts ribavirin resistance, particularly in HCV genotype 1a infected patients. The analysis results showed that RASs detected at positions 244, 309, and 310 are stable selective pressure (dN/dS < 1), position 329 is directional selectivity pressure (dN/dS = 3), and position 333 is more neutral selective pressure (dN/dS = 0.6) from the perspective of mutation occurrence due to selective pressure through the dN/dS index (non-synonymous/synonymous mutation). As a result of selection pressure during antiviral therapy with ribavirin, the development of the Q309R mutation is thought to be resistant to ribavirin. Despite the fact that the Q309R mutation was found in HCV genotype 1a, patients who received a DAA inhibitor treatment had highly efficient virus eradication and no recurrence after 12 weeks. Liver enzymes and the APRI index restored to normal levels after 12 weeks of treatment. As a result, there is a possibility to enhance the anti-ribavirin activity. Other mutations such as N244I, D310N, and T329E must be paired with the Q309R mutation.
NS5B Variants with Resistance to DAAs Were Found Among Treatment-Naive Vietnamese Patients
The presence of DAAs RASs in the HCV NS5B region was investigated in this study. Several mutations were discovered as natural polymorphisms, including E237G, S282R, L320F, and V321A/I. S282T and C316N were not discovered in any of the HCV isolates, while additional variants at position 282 (S282R) were found in both the 1b and 6a subtypes. C316N substitution was also discovered in HCV genotype 1b in recent studies in Brazil, Asia, Europe, North America, and South Africa, but no mutations of S282T/R, L320F, V321A, or C316Y were found. Another study in Italy found the C316N mutation in 8.1% of HCV genotype 1b,12 while the C316N mutation was found in 67.4% of HCV genotype 1b in China.11 However, the S282T/R mutation was not discovered in these studies. As a result, the C316N mutation was found in many parts of the world, primarily in HCV genotype 1b, suggesting that the C316N mutation is prevalent in Asia and China. However, the C316N mutation was not found in the current investigation. According to Bertoli et al (Italy), the C316N mutation is more common in patients who have been treated with INF.12 Therefore, the HCV isolates circulating in Vietnam may be less vulnerable to INF pressure, resulting in the absence of the C316N mutation. The E237G, L320F, and V321A/I/L mutations, on the other hand, were found at low frequency in the Asian and Europe continents but not Africa or America. Because it inhibits the gene encoding the NS5B RNA-dependent RNA polymerase enzyme, the S282T alteration displays a very high resistance to NI inhibitors, but it is also present at a very low rate and is rarely observed in previous investigation. However, the S282R mutation was detected in our study, which has different effects than NI inhibitors but is worse than S282T. Despite the fact that five HCV isolates possessed the S282R mutation, all five HCV-infected patients responded favorably to sofosbuvir/velpatasvir treatment after 4–12 weeks. As a result, the S282R mutation’s resistance capacity may need to be coupled with other types of mutations to boost the resistance impact and, therefore, needs further studies to elucidate this hypothesis.
Impact of Mutations on Antiviral Drug Efficacy
Despite the fact that HCV genotypes 1, 3, and 6 have numerous mutations in the NS5B gene, all patients in our study were treated for 12 weeks with the new DAA regimens (sofosbuvir/ledipasvir and sofosbuvir/velpatasvir), with 5 patients receiving extra ribavirin due to liver fibrosis. In the fourth week of treatment, 94% of patients had HCV-RNA levels below the quantification threshold (1.5 IU/mL), showing that they had a sustained virological response. 100% of patients exhibited a durable virological response after 12 weeks of treatment, and no patient had relapsed to DAA inhibitors after 24 weeks. Miller et al reported that the sofosbuvir/velpatasvir regimen has been shown to have very good antiviral activity against all 6 HCV genotypes, with a sustained virological response rate ranging from 95% to 100% in HCV-infected populations, including patients with compensated cirrhosis and previous treatment failure, at 12 weeks after completion of treatment. However, because the sample size of genotype 3 is too small (n=2), more research with larger sample size are needed to investigate the effects of mutations on the therapeutic medication effectiveness.
In our study, we discovered that a number of HCV isolates have resistance mutations that impact the virus’s susceptibility to ribavirin and sofosbuvir. HCV isolates with the Q309R mutation, which makes resistant to ribavirin, were given a ribavirin-containing regimen, while HCV isolates with sofosbuvir-resistant mutation were given a sofosbuvir-containing regimen. However, after 12 weeks of treatment, all patients had rapid and sustained viral responses, and liver enzymes as well as liver fibrosis index improved and recovered swiftly. The study by Sarazzin et al evaluated the NS5B segment sequences of 2144 patients treated with the sofosbuvir/ledipasvir regimen and found that 2.5% of the patients revealed mutations impacting the NS5B inhibition before treatment and all of them had persistent viral response after 12 weeks. These data imply that include sofosbuvir in most HCV regimens is still an effective way to treat HCV with sofosbuvir resistant mutations. In HCV isolates from Vietnam, we detected many mutations related to sofosbuvir susceptibility, including S282R, V321A/I, and L320F. Although the S282R mutation was observed in a number of HCV isolates, the S282T mutation (which is highly resistant to NI inhibitors) was not found, indicating that a sofosbuvir-based combination therapy is still very efficient.
Conclusion
All 13 amino acid positions in the study were found to be mutated in HCV isolates circulating in Vietnam. Significant mutations, on the other hand, arose at a low incidence, and their influence on HCV inhibitors was minimal. There were no mutations that conferred high resistance to therapeutic drugs, such as S282T. In terms of treatment response and liver function improvement, there was no significant difference between HCV isolates with and without mutations. All of the patients experienced a sustained viral response, as well as improvements in liver enzymes and fibrosis index.
Disclosure
The authors declare no conflicts of interest.
References
1. Huy Do S. Epidemiology of hepatitis B and C virus infections and liver cancer in Vietnam. Euroas J Hepatogastroenterol. 2015;5(1):49–51. doi:10.5005/jp-journals-10018-1130
2. Nakata S, Song P, Duc DD, et al. Hepatitis C and B virus infections in populations at low or high risk in Ho Chi Minh and Hanoi, Vietnam. J Gastroenterol Hepatol. 1994;9(4):416–419. doi:10.1111/j.1440-1746.1994.tb01265.x
3. Leone N, Rizzetto M. Natural history of hepatitis C virus infection: from chronic hepatitis to cirrhosis, to hepatocellular carcinoma. Minerva Gastroenterol Dietol. 2005;51(1):31–46.
4. Wirth TC, Manns MP. The impact of the revolution in hepatitis C treatment on hepatocellular carcinoma. Ann Oncol. 2016;27(8):1467–1474. doi:10.1093/annonc/mdw219
5. El-Shamy A, Hotta H. Impact of hepatitis C virus heterogeneity on interferon sensitivity: an overview. World J Gastroenterol. 2014;20(24):7555–7569. doi:10.3748/wjg.v20.i24.7555
6. Sorbo MC, Cento V, Di Maio VC, et al. Hepatitis C virus drug resistance associated substitutions and their clinical relevance: update 2018. Drug Resist Updat. 2018;37:17–39. doi:10.1016/j.drup.2018.01.004
7. Powdrill MH, Bernatchez JA, Gotte M. Inhibitors of the hepatitis C virus RNA-dependent RNA polymerase NS5B. Viruses. 2010;2(10):2169–2195. doi:10.3390/v2102169
8. Rolland S, Vachon ML. Sofosbuvir for the treatment of hepatitis C virus infection. CMAJ. 2015;187(3):203–204. doi:10.1503/cmaj.140151
9. Khaliq S, Raza SM. Current status of direct acting antiviral agents against hepatitis C virus infection in Pakistan. Medicina. 2018;54(5). doi:10.3390/medicina54050080
10. Halfon P, Locarnini S. Hepatitis C virus resistance to protease inhibitors. J Hepatol. 2011;55(1):192–206. doi:10.1016/j.jhep.2011.01.011
11. Yang S, Xing H, Feng S, et al. Prevalence of NS5B resistance-associated variants in treatment-naive Asian patients with chronic hepatitis C. Arch Virol. 2018;163(2):467–473. doi:10.1007/s00705-017-3640-6
12. Bertoli A, Sorbo MC, Aragri M, et al. Prevalence of single and multiple natural NS3, NS5A and NS5B resistance-associated substitutions in hepatitis C virus genotypes 1–4 in Italy. Sci Rep. 2018;8(1):8988. doi:10.1038/s41598-018-26862-y
13. Raj VS, Hundie GB, Schurch AC, et al. Identification of HCV resistant variants against direct acting antivirals in plasma and liver of treatment naive patients. Sci Rep. 2017;7(1):4688. doi:10.1038/s41598-017-04931-y
14. Ruiz-Jarabo CM, Arias A, Baranowski E, Escarmis C, Domingo E. Memory in viral quasispecies. J Virol. 2000;74(8):3543–3547. doi:10.1128/JVI.74.8.3543-3547.2000
15. Castilho MC, Martins AN, Horbach IS, et al. Association of hepatitis C virus NS5B variants with resistance to new antiviral drugs among untreated patients. Mem Inst Oswaldo Cruz. 2011;106(8):968–975. doi:10.1590/S0074-02762011000800011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.