Back to Journals » Drug Design, Development and Therapy » Volume 17
Ibrexafungerp for the Treatment of Vulvovaginal Candidiasis: Design, Development and Place in Therapy
Authors Phillips NA, Rocktashel M, Merjanian L
Received 7 September 2022
Accepted for publication 31 December 2022
Published 7 February 2023 Volume 2023:17 Pages 363—367
DOI https://doi.org/10.2147/DDDT.S339349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Nancy A Phillips, Maria Rocktashel, Lena Merjanian
Department Obstetrics, Gynecology & Reproductive Sciences, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA
Correspondence: Nancy A Phillips, Department Obstetrics, Gynecology & Reproductive Sciences, Rutgers Robert Wood Johnson Medical School, 125 Paterson Street CAB 2102, New Brunswick, NJ, 08901, USA, Tel +1 732-235-7755, Fax +1 732-235-6600, Email [email protected]
Abstract: Vulvovaginal candidiasis (VVC) is experienced by an estimated 75% of women at least once in their lifetime and is recurrent, defined as three or more infections per year (RVVC) in 5– 9%. Candida albicans is the most common causative agent, but up to 19% of infections may be related to non-albicans species. Available treatment options for VVC have consisted of oral and topical azoles (except for topical nystatin, a polyene). Oral polyenes are not absorbed and therefore not effective for VVC. Fluconazole is the only oral medication FDA approved for VVC. None of these treatments are FDA approved for RVVC. Ibrexafungerp, a triterpenoid fungicidal agent, was FDA approved in 2021, becoming the first oral non-azole agent for VVC. Ibrexafungerp reaches concentrations up to 9-fold higher in vaginal tissues versus plasma. In Phase 2 clinical trials, ibrexafungerp had a clinical cure rate comparable to fluconazole at day 10, but significantly better at day 25. In Phase 3 clinical trials, ibrexafungerp had both a higher clinical and mycologic cure rate versus placebo at both days 10 and 25. In December 2022, Ibrexafungerp received FDA approval for once monthly dosing to decrease the incidence of RVVC. This approval was based on data from the CANDLE STUDY, which showed 65.4% resolution of symptoms and culture negative success through week 24, compared to 53.1% of placebo. Ibrexafungerp provides an alternative oral option for treatment of acute, severe VVC. It is the only FDA approved antifungal for RVVC. Currently, the population likely to benefit from this drug are those with azole allergy, non-albicans or azole resistant albicans species, or other azole contraindications such as drug interactions (like statins or tricyclics). Side effects are mostly gastrointestinal and mild in nature. Ibrexafungerp, like fluconazole, should be used with caution in women who are or may become pregnant.
Keywords: fungicidal, yeast infection, ibrexafungerp, vulvovaginal candidiasis, recurrent vulvovaginal candidiasis
Introduction
Vulvovaginal candidiasis (VVC) is a global problem and is the second most common cause of vaginitis in women (after bacterial vaginosis). Treatment options for VVC have consisted of fungistatic oral and topical azoles (except for topical nystatin, a polyene). Ibrexafungerp, a triterpenoid fungicidal agent, was developed as an alternative oral treatment for VVC. Ibrexafungerp received FDA for the treatment of VVC in June 2021, and was subsequently approved for recurrent VVC (RVCC) in December 2022.
The purpose of this review is to compare the existing treatment options for VVC to the novel non-azole, non-polyene, ibrexafungerp. The drug’s development, clinical trials and place in clinical practice will be discussed.
Materials and Methods
A literature search was performed through Ovid, Medscape, Google Scholar with keywords vulvovaginal candidiasis, yeast infection, azoles, ibrexafungerp.
Epidemiology
An estimated 75% of women will experience one episode of VVC in their lifetime, 40–45% will experience two or more and an estimated 5 −9% (138 million women annually) will experience recurrent vulvovaginitis (RVCC), defined as three or more infections per year.1,2 VVC is most common in women of reproductive years, with a lower incidence in prepubertal girls and is uncommon in postmenopausal women not on hormone therapy or without underlying conditions like diabetes.3 In the United States, Candida albicans is responsible up to 92% of VVC, with Candida glabrata responsible for most others.4,5
Many women with VVC appear to have no underlying risk factors. Predisposing factors include antibiotics, menopausal hormone therapy, genetic predisposition (polymorphisms in the SIGLEC-15 gene or polymorphisms in the TLR2 and mannose-binding lectin genes) diabetes (increased with sodium glucose cotransporter 2 inhibitors), and immune compromise.6,7
VVC Symptoms and Diagnosis
Symptoms of VVC include vulvovaginal burning, pruritus, irritation and discharge. Clinical signs include edema, erythema, and excoriation, a thick, white “cottage cheese” discharge generally adherent to the vaginal side walls. Vaginal pH is most often acidic (normal 3.5–4.5), but as yeast can coexist with atrophy, bacterial vaginosis or trichomoniasis it can also be present in an elevated vaginal pH (>4.5). The presence of yeast (hyphae or buds) visualized microscopically after adding 10% potassium hydroxide (KOH) can confirm the diagnosis (Figures 1 and 2). As microscopic visualization has a high false-negative rate, the absence of yeast might prompt obtaining cultures, or commercial testing with molecular DNA, or polymerase chain reaction (PCR) laboratory evaluation if clinically suspected. Clinical diagnosis by visual inspection of discharge is unreliable, as is self-report of symptoms or telephone triage diagnosis.
 |
Figure 1 Yeast hyphae (40X) – identified by arrow. |
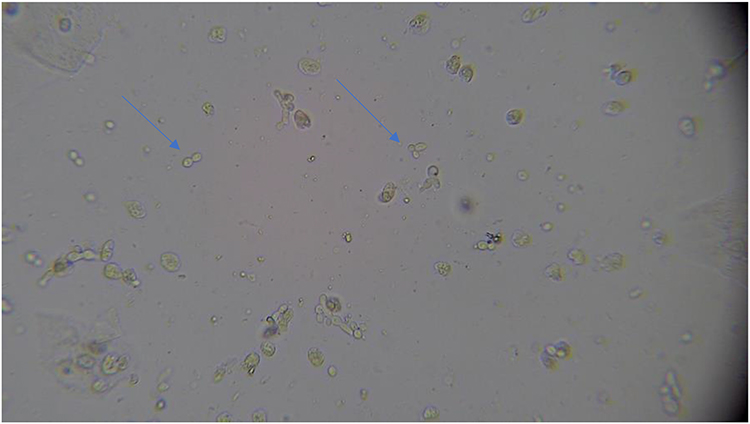 |
Figure 2 Yeast buds (40X) – identified by arrow. |
Treatment of VVC
The azole class of antifungals (both oral and topical) act by inhibition of lanosterol 14-alpha-demethylase, which blocks the synthesis of ergosterol, required for the synthesis of the fungal cell wall. Azoles are fungistatic. The polyene antifungals increase the permeability of fungal cell membrane, causing cellular contents to leak, resulting in both fungicidal and fungistatic activity.8 The oral polyene, nystatin, is not absorbed, and therefore will not treat VVC. Fluconazole had been the only oral azole Food and Drug Administration (FDA) approved for VVC, while oral polyene and echinocandin antifungals are not approved for this condition.9,10
Ibrexafungerp Drug Development
Mechanism of Action
Ibrexafungerp, a triterpenoid antifungal agent, was developed as an alternative oral treatment for VVA and received FDA approval June 2021.11 Prior to its development, there were no (FDA) approved oral non-azole agents for this condition.
Like the echinocandin antifungals, Ibrexafungerp works by inhibition of the enzyme glucan synthase, disrupting the formation of 1.3-β-D-glucan, an essential component of the fungal cell wall, leading to cell lysis. Therefore, Ibrexafungerp is fungicidal.12
Preclinical animal studies showed Ibrexafungerp targeted vaginal tissue, with levels 2–9-fold higher in vaginal tissue over those found in plasma.13 Additionally, in-vitro studies confirmed no change in activity at low pH (4.5), which is more physiologically accurate in the premenopausal female vagina, contrary to the decreased activity of the azoles demonstrated with significantly increased mean inhibitory concentration values for all antifungals when tested at pH 4 versus pH 7(p < 0.001 for all comparisons), including oral fluconazole.14 Also in vitro, ibrexafungerp has shown to disrupt biofilms produced by Candida species, with significantly higher activity than that of fluconazole (P < 0.001).15
Ibrexafungerp has broad-spectrum anti-Candida fungicidal activity with a half-life of 20 hours. As a non-azole, it exerts coverage against azole-resistant species, such as those with fks1 and fks2 point mutations like Candida glabrata and Candida Auris.16 Ibrexafungerp has demonstrated in vitro activity against Candida species (auris, dubliniensis, glabrata, guilliermondii, keyfr, krusei, lusitaniae, parapsilosis, and tropicalis).17
Clinical Trials
There has been one Phase 2 clinical trial of Ibrexafungerp18 versus fluconazole and two Phase 3 clinical trials versus placebo.19,20
The 186 participant Phase 2 trial (DOVE) randomized subjects into a single 150 mg Fluconazole versus 5 study doses of oral Ibrexafungerp with the primary objective to identify an optimal dose of the study drug based on clinical cure rates and tolerability.18 Ibrexafungerp 300mg BID for 1 day was found to have a clinical cure rate of 51.9% versus 58.3% for fluconazole at day 10. At day 25, however, subjects with no VVC signs or symptoms were 70.4% in the Ibrexafungerp group versus 50.0% in the fluconazole group. Ibrexafungerp 300mg BID was chosen for the Phase 3 trials. The most commonly reported side effects were mild gastrointestinal events.
In the first of 2 Phase 3 trials (VANISH 303), 376 subjects were randomized to ibrexafungerp (n = 249) or placebo (n = 127). The treatment group had significantly higher rates of clinical cure (50.5% vs 28.6%; P = 0.001), mycological eradication (49.5% vs 19.4%; P < 0.001 compared with placebo at day 11±3). At day 25±4, the treatment group had significantly more clinical cure versus the placebo group (59.6% vs 44.9%; p=0.009). Post hoc analysis showed similar rates of clinical cure and clinical improvement at test-of-cure for Black patients (54.8% [40/73] and 63.4% [47/73], respectively) and patients with a body mass index >35 (54.5% [24/44] and 68.2% [30/44], respectively) compared with overall rates. Ibrexafungerp was well tolerated. Adverse events were primarily gastrointestinal and mild in severity, including diarrhea (17%), nausea (12%), abdominal pain (11%), dizziness (3%), and vomiting (2%).21
In the second Phase 3 trial (VANISH 306), Sobel et al again showed a significantly higher clinical cure rate (63.3% vs 44%) and negative culture result indicating mycological cure (58.5% vs 29.8%) in those receiving Ibrexafungerp (n = 188) versus placebo (n = 88) when evaluated at day 11±3. Similarly, at follow up (day 25± 4), symptom resolution persisted for 72.3% of treated versus 52.4% of placebo subjects (p = 0.001).20
All studies were double blinded. Within these study groups, females ≥12 years were included. Three pregnancies occurred in the Phase 3 trials: two resulted in live births with no fetal anomalies or complications reported; the other was electively terminated at 12 weeks of gestation. However, due to preclinical animal studies in which teratogenicity was reported, Ibrexafungerp is contraindicated in pregnancy. Contraception should be used while on treatment and for at least 4 days after completion of the last dose in women with pregnancy potential.
For VVC, Ibrexafungerp is FDA approved for the treatment of adult and post-menarche pediatric females. Dosage is 300mg BID for 1 day (total 4 pills = 1200mg). For patients on strong inducers of CYP3A4 (phenobarbital, phenytoin, rifampicin, St. John’s Wort and glucocorticoids), dose should be reduced to 150 mg BID.11
Recurrent Vulvovaginal Candidiasis
RVCC, defined as 3 or more infections per year is typically treated with an induction period followed by prophylactic dosing on a weekly to biweekly schedule. The most common protocol is a 7–14-day course of a topical agent or a single or multi-dose course of fluconazole for acute treatment, followed by dosing of twice a week for the topicals and once a week for fluconazole.22
These regimens are not FDA approved, but rather based on expert opinion.
In December 2022, a monthly dose of Ibrexafungerp was approved for the treatment of RVCC, making it the only therapy approved for this indication.21,22,24 Approval was based on Synexis’ CANDLE study reported that monthly single-day ibrexafungerp showed 65.4% resolution of symptoms and culture negative success through week 24, compared to 53.1% of placebo-treated patients (p = 0.02).24 This advantage over placebo was sustained over a 3 month follow up.24 Additionally, in a nested sub-study ibrexafungerp showed a substantial elimination or resolution of symptoms in 71% of RVVC patients who failed to respond to a 3-dose regimen of fluconazole.23 Effective birth control should be instituted and documented during long-term use of Ibrexafungerp.24 Product labeling for this indication, once available, should provide contraceptive guidelines. There are no current clinical trial data exploring ibrexafungerp for RVCC versus the newly approved long acting azole oteseconazole.
Results – Place in Clinical Use
Ibrexafungerp provides an important additional option for health-care providers in women with acute, severe VVC or RCVV. The population most likely to benefit are those with azole allergy, or other azole contraindications, including drug interactions (statins, tricyclics), non-albicans Candida species, including C. glabrata, for which no consistently effective oral treatments are otherwise available. Ibrexafungerp also offers an oral option of treatment for women with fluconazole resistant C. albicans.23 Monthly dosing of ibrexafungerp offers an FDA approved, evidence-based treatment for RVCC.
Conclusion
Ibrexafungerp is the first oral non-azole approved for both VVC and RCVV, with broad spectrum coverage of both C.albicans and non-albicans species. Ibrexafungerp is fungicidal, acting via inhibition of the enzyme glucan synthase, disrupting the formation of 1.3-β-D-glucan, causing cell lysis. For health-care providers, this is an exciting development representing another means in the ability to treat and potentially eradicate VVC and RVCC. For the millions of women who suffer from these conditions and the associated disruption of work, social and sexual function, ibrexafungerp represents relief.
Disclosure
Nancy A Phillips has served on an advisory board for Synexis concerning ibrexafungerp. The authors report no other conflicts of interest in this work.
References
1. Workowski KA, Bachmann LH, Chan PA, et al. Center for disease control and prevention, sexually transmitted infections treatment guidelines. MMWR Recomm Rep. 2021;70:91–97.
2. Denning DW, Kneale M, Sobel JD, Rautemaa-Richardson R. Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect Dis. 2018;18(11):e339–47. doi:10.1016/S1473-3099(18)30103-8
3. Foxman B, Muraglia R, Dietz JP, Sobel JD, Wagner J. Prevalence of recurrent vulvovaginal candidiasis in 5 European countries and the United States: results from an internet panel survey. J Low Genit Tract Dis. 2013;17(3):340. doi:10.1097/LGT.0b013e318273e8cf
4. Martin Lopez JE. Candidiasis (vulvovaginal). BMJ Clin Evi. 2015;16:815.
5. Vermitsky JP, Self MJ, Chadwick SG, et al. Survey of vaginal-flora Candida species isolates from women of different age groups by use of species-specific PCR detection. J Clin Microbiol. 2008;46(4):1501–1503. doi:10.1128/JCM.02485-07
6. Jaeger M, Pinelli M, Borghi M, et al. A systems genomics approach identifies SIGLEC15 as a susceptibility factor in recurrent vulvovaginal candidiasis. Sci Transl Med. 2019;11:496. doi:10.1126/scitranslmed.aar3558
7. Rosentul DC, Delsing CE, Jaeger M, et al. Gene polymorphisms in pattern recognition receptors and susceptibility to idiopathic recurrent vulvovaginal candidiasis. Front Microbiol. 2014;5:483. doi:10.3389/fmicb.2014.00483
8. Hildago J. Candidiasis Medication. [updated January 17, 2020] https://emedicine.medscape.com/article/213853-medication#4.
9. Grover ND. Echinocandins: a ray of hope in antifungal drug therapy. Indian J Pharmacol. 2010;42(1):9–11. PMID: 20606829; PMCID: PMC2885632. doi:10.4103/0253-7613.62396
10. Carolus H, Pierson S, Lagrou K, Van Dijck P. Amphotericin B and other polyenes-discovery, clinical use, mode of action and drug resistance. J Fungi. 2020;6(4):321. PMID: 33261213; PMCID: PMC7724567. doi:10.3390/jof6040321
11. BREXAFEMME® (ibrexafungerp tablets), for oral use. Product Insert. Available from: https://www.brexafemme.com/prescribinginformation.
12. Jallow S, Govender NP. Ibrexafungerp: a first-in-class oral triterpenoid glucan synthase inhibitor. J Fungi. 2021;7(3):163. PMID: 33668824; PMCID: PMC7996284. doi:10.3390/jof7030163
13. Wring S, Borroto-Esoda K, Solon E, Angulo D. SCY-078, a novel fungicidal agent, demonstrates distribution to tissues associated with fungal infections during mass balance studies with intravenous and oral [14C]SCY-078 in albino and pigmented rats. Antimicrob Agents Chemother. 2019;63(2):e02119–18. PMID: 30478166; PMCID: PMC6355592. doi:10.1128/AAC.02119-18
14. Spitzer M, Wiederhold NP. Reduced antifungal susceptibility of vulvovaginal candida species at normal vaginal pH Levels: clinical Implications. J Low Genit Tract Dis. 2018;22(2):152–158. doi:10.1097/LGT.0000000000000383
15. Gamal A, Chu S, McCormick TS, Borroto-Esoda K, Angulo D, Ghannoum MA Ibrexafungerp, a Novel Oral Triterpenoid Antifungal in Development: Overview of Antifungal Activity Against Candida glabrata. Front Cell Infect Microbiol.2021; 11:642358. doi: 10.3389/fcimb.2021.642358
16. Azie N, Angulo D, Dehn B, Sobel JD. Oral Ibrexafungerp: an investigational agent for the treatment of vulvovaginal candidiasis. Expert Opin Investig Drugs. 2020;29(9):893–900. PMID: 32746636. doi:10.1080/13543784.2020.1791820
17. Quindós G, Miranda-Cadena K, San-Millán R, et al. Vitro antifungal activity of ibrexafungerp (SCY-078) against contemporary blood isolates from medically relevant species of candida: a European study. Front Cell Infect Microbiol. 2022;12(12). doi:10.3389/fcimb.2022.906563
18. Nyirjesy P, Schwebke JR, Angulo DA, Harriott IA, Azie NE, Sobel JD. Phase 2 randomized study of oral ibrexafungerp versus fluconazole in vulvovaginal candidiasis. Clin Infect Dis. 2022;74(12):2129–2135. PMID: 34555149; PMCID: PMC9258939. doi:10.1093/cid/ciab841
19. Schwebke JR, Sobel R, Gersten JK, et al. Ibrexafungerp versus placebo for vulvovaginal candidiasis treatment: a phase 3, randomized, controlled superiority trial (VANISH 303). Clin Infect Dis. 2022;74(11):1979–1985. PMID: 34467969; PMCID: PMC9187327. doi:10.1093/cid/ciab750
20. Sobel R, Nyirjesy P, Ghannoum MA, et al. Efficacy and safety of oral ibrexafungerp for the treatment of acute vulvovaginal candidiasis: a global phase 3, randomized, placebo-controlled superiority study (VANISH 306). BJOG. 2022;129(3):412–420. PMID: 34676663; PMCID: PMC9299454. doi:10.1111/1471-0528.16972
21. Comtemporary OB/GYN . FDA approves ibrexafungerp for reduction in the incidence of RVVC. Available from: https://www.contemporaryobgyn.net/view/fda-approves-ibrexafungerp-for-reduction-in-the-incidence-of-rvvc.
22. Phillips NA, Bachmann G, Haefner H, Martens M, Stockdale C. Topical treatment of recurrent vulvovaginal candidiasis: an expert consensus. Women’s Health Rep. 2022;3(1):38–42. doi:10.1089/whr.2021.0065
23. Marchaim D, Lemanek L, Bheemreddy S, Kaye KS, Sobel JD. Fluconazole-resistant Candida albicans vulvovaginitis. Obstet Gynecol. 2012;120(6):1407–1414. doi:10.1097/AOG.0b013e31827307b2
24. SCYNEXIS. SCYNEXIS Presents Positive Data from Its Pivotal Phase 3 CANDLE Study of Oral Ibrexafungerp for Prevention of Recurrent Vaginal Yeast Infections During the 2022 IDSOG Annual Meeting. Available from: https://d1io3yog0oux5.cloudfront.net/_b74ab29ee08f7c716ae5e6710e5dba4b/scynexis/news/2022-08-04_SCYNEXIS_Presents_Positive_Data_from_Its_Pivotal_298.pdf.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.