Back to Journals » Nature and Science of Sleep » Volume 14
“I Want to Be Safe and Not Still Half Asleep”: Exploring Practical Countermeasures to Manage the Risk of Sleep Inertia for Emergency Service Personnel Using a Mixed Methods Approach
Authors Kovac K, Vincent GE, Paterson JL, Ferguson SA ![]()
Received 26 April 2022
Accepted for publication 8 July 2022
Published 26 August 2022 Volume 2022:14 Pages 1493—1510
DOI https://doi.org/10.2147/NSS.S370488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Katya Kovac,1 Grace E Vincent,1 Jessica L Paterson,2 Sally A Ferguson1
1School of Health, Medical and Applied Sciences, Appleton Institute, Central Queensland University, Wayville, SA, Australia; 2Flinders Institute of Mental Health and Wellbeing, College of Education, Psychology and Social Work, Flinders University, Bedford Park, SA, Australia
Correspondence: Katya Kovac, School of Health, Medical and Applied Sciences, Appleton Institute, Central Queensland University, 44 Greenhill Road, Wayville, SA, 5034, Australia, Tel +61 420 718 242, Email [email protected]
Purpose: The aim of this exploratory cross-sectional mixed methods study was to determine 1) whether sleep inertia, the temporary state of impaired vigilance performance upon waking, is perceived to be a concern by emergency service personnel, 2) what strategies are currently used by emergency service workplaces to manage sleep inertia, 3) the barriers to implementing reactive sleep inertia countermeasures, and 4) what strategies personnel suggest to manage sleep inertia.
Participants and Methods: A sample (n = 92) of employed and volunteer Australian emergency service personnel (fire and rescue, ambulance, police, state-based rescue and recovery personnel) completed an online survey. Data collected included demographic variables and work context, experiences of sleep inertia in the emergency role, barriers to sleep inertia countermeasures, and existing workplace sleep inertia countermeasures and recommendations. Quantitative data were analysed using descriptive statistics, and qualitative data were thematically analysed.
Results: Approximately 67% of participants expressed concern about sleep inertia when responding in their emergency role. Despite this, there were few strategies to manage sleep inertia in the workplace. One major barrier identified was a lack of time in being able to implement sleep inertia countermeasures. Fatigue management strategies, such as reducing on-call periods, and operational changes, such as screening calls to reduce false alarms, were suggested by participants as potential strategies to manage sleep inertia.
Conclusion: Sleep inertia is a concern for emergency service personnel and thus more research is required to determine effective sleep inertia management strategies to reduce the risks associated with sleep inertia and improve personnel safety and those in their care. In addition, future studies could investigate strategies to integrate reactive sleep inertia countermeasures into the emergency response procedure.
Keywords: fatigue management, on-call, shiftwork, intervention effectiveness, barriers
Introduction
The emergency services sector encompasses highly skilled industries such as fire and rescue, ambulance, police, and state-based rescue and recovery services. In Australia, there are 120,000 salaried and retained employees and 240,000 volunteers charged to protect the safety and wellbeing of communities.1 Due to the unpredictable nature of emergencies, the emergency sector uses shift work and on call arrangements to provide round-the-clock coverage1–5. Shift work allows for 24/7 staffing with shifts covering the morning, afternoon, and night,6 and on-call shifts are used during non-peak hours where full, round-the-clock staffing is not necessary or where resources do not allow.7 There are times when emergency service personnel are allowed to sleep when on shift or on-call. For example, personnel working night shifts are sometimes permitted to nap during breaks to help manage fatigue,8,9 and on-call personnel sleep prior to receiving a call either at home, or on site.10 In such settings, if a call occurs, the sleep of personnel will be interrupted and they may be required to drive to an emergency event, make decisions, or perform their emergency role shortly after waking while experiencing sleep inertia.10
Sleep inertia is a transition state that occurs upon waking in which alertness and cognitive performance are temporarily degraded.11 Typically, sleep inertia lasts between 15 and 30 min post waking, however studies have found that performance may not stabilize until 2–3 h post-waking.12 Importantly, sleep inertia can impair vital cognitive abilities such as vigilance13 and decision-making.14 While sleep inertia occurs when waking from most sleep periods, it can be more severe, causing greater performance deficits when waking during the biological night.13,15 Furthermore, both waking from deep sleep slow wave sleep13,16 and prior sleep restriction13,17 have been associated with a greater magnitude of sleep inertia. Since emergency service personnel can experience abrupt night-time awakenings while on-call or during night shifts, they are more likely to experience severe sleep inertia that could impair their ability to perform their jobs safely and effectively. In addition, given that on-call work is associated with a reduction in sleep quantity even when no calls are received, on-call personnel potentially experience chronic sleep loss which can also increase sleep inertia severity.17–20 Furthermore, the period in which sleep inertia is likely to be a risk can overlap with travel to incidents in emergency response, thus impacting the safety of personnel and other road users. In emergency work, it is important that personnel perform optimally and operate safely as small mistakes or lapses in performance and efficiency can have dire consequences for the safety and wellbeing of those involved.21
Research has begun to investigate countermeasures to reduce the impact of sleep inertia and improve the safety and performance of workers.3,22 Sleep inertia countermeasures are typically broken into two categories: proactive countermeasures and reactive countermeasures.22 Proactive countermeasures are strategies that are implemented prior to waking from a sleep period to reduce sleep inertia. While proactive countermeasures, such as caffeine ingestion prior to naps are effective in minimizing sleep inertia under experimental conditions,23,24 these types of countermeasures are not feasible when call outs and wake times are unpredictable and are therefore unsuitable for those with on-call arrangements. Reactive countermeasures, which are implemented upon waking, are more suited to those with unpredictable sleep periods, such as emergency service personnel. Reactive strategies include caffeine ingestion upon waking,25 light exposure,26–28 sound manipulation,29–31 body temperature manipulation,32,33 face washing,27 and exercise.34 It should be noted that no reactive countermeasures have successfully and significantly reduced sleep inertia within the first 10-min post-waking under controlled experimental conditions, but research into faster acting countermeasures is ongoing.
Sleep inertia is commonly cited in the literature as a significant risk for emergency service personnel.3,10,35 Of note, firefighters reported that sleep inertia is a safety concern during alarm response.36 However, few studies have investigated whether sleep inertia is perceived to be prevalent and a cause for concern in other sectors of the emergency workforce (eg, paramedics, state-based rescue and recovery personnel and police). In addition, while several experimental studies investigated both proactive and reactive sleep inertia countermeasures, there are few field-based studies exploring how sleep inertia might be best managed under real-world conditions. Reactive countermeasures are typically targeted to on-call personnel; however, it is unknown whether such countermeasures are practical for personnel in operational conditions. Occupational health and safety intervention effectiveness research serves to evaluate the development and implementation of interventions, as well as the success of the intervention.37 The National Institute for Occupational Safety and Health put forward a conceptual framework for investigating the effectiveness of occupational safety and health interventions, which involved three broad research phases: development, implementation, and evaluation.37 Intervention development is the first phase which seeks to answer questions related to what change is needed, the best practice in addressing these changes, potential barriers in implementing interventions, and whether the intended audience or target population are likely to understand and “buy into” change.37 To answer these questions, data need to be collected to understand the behaviors, attitudes, and knowledge of the target population(s). Strategies can then be developed that are consistent with the needs of that target population, and data can be collected about the context for the intervention.37 With this knowledge, appropriate interventions may be developed, or previously developed interventions may be adapted.37
To the authors’ knowledge, there has been no systematic investigation into the effectiveness of interventions to manage sleep inertia (ie, sleep inertia countermeasures) at the development phase. As a result, the current exploratory research seeks to begin the development phase of intervention effectiveness research into sleep inertia countermeasures with the target population of emergency service workers. Specifically, this research aims to determine: a) whether sleep inertia is a concern for emergency service personnel, and if yes, to what degree it is a concern, b) what sleep inertia countermeasures are already being used by emergency service organizations—if any, c) the barriers to implementing reactive countermeasures for emergency service personnel, and d) what changes could be made in the workplace to reduce the impact of sleep inertia. Such information could help guide or refine experimental research towards strategies to manage sleep inertia that would be both effective and practical to use in the field by the target population and thus improve worker health and safety when waking and responding to calls.
Material and Methods
Participants
The sample comprised retained, salaried, and volunteer Australian emergency service personnel. Participants included fire and rescue personnel, ambulance personnel, police, and state-based rescue and recovery personnel who worked on-call or shift work arrangements. Those with regular shifts (ie, regular day-time shifts, regular rotating shifts, regular night shifts) were included if they had the opportunity to sleep while on shift. The initial sample included 144 participants. Forty-four participants were excluded from the final sample because they did not provide any data beyond the demographic questions. Five participants were excluded from the final sample because their work industry did not meet the definition of emergency services for this study. Three participants were excluded because they did not have an opportunity to sleep, rest or nap while at work. The final sample size was 92 participants (Table 1).
 |
Table 1 Participant Demographic Variables and Work Characteristics |
Design and Procedure
A cross-sectional concurrent mixed methods study design was used. Data were collected through an online questionnaire using Qualtrics (Qualtrics, Provo, UT; for the full survey see Supplementary Material). Recruitment ran from August to October 2020 and the survey was disseminated through industry and personal contacts, as well as posts on social media (Twitter and Facebook). The first page of the survey provided information about the project, including the benefits and risks of participating, consent, data publication, and contact details for any questions and concerns. Participants were notified that their participation was anonymous and voluntary, and they could withdraw at any point by closing the browser. Prior to beginning the survey, participants were required to provide informed consent on the first page of the survey. The survey took approximately 15–20 minutes to complete, and participants were provided with contact details of the study coordinator if they had questions or wanted to request a plain English summary of results. Ethics approval was obtained from the Central Queensland University Human Research Ethics Committee (project number: 0000022402). The study was conducted in compliance with the ethical principles set out in the Declaration of Helsinki.
Survey Items
The study authors created and pre-tested the survey with a small sample (n = 15) comprising the target population (n = 6), lay people (n = 5) and academic experts in the field (n = 4) to establish face and content validity. Based on the feedback, no content-related amendments were needed. The survey comprised four sections including 1) demographic and work context, 2) experiences of sleep inertia in the emergency service role, 3) barriers to sleep inertia countermeasures, and 4) workplace sleep inertia countermeasures and recommendations.
Demographic and Work Context
Participants were asked basic demographic questions followed by specific questions about their work context. The demographic questions included: age, gender (male, female, other), and postcode. Work context questions included: “What area of emergency services are you primarily in?” (fire and rescue, ambulance, police, state-based rescue and recovery, or other; with the employment options of salaried, retained, or volunteer); “How long have you been involved in the emergency service field?” (less than 12 months, 1–2 years, 2–5 years, 5–10 years, and more than 10 years); “What types of schedule do you work/volunteer in your primary emergency service role?” (regular day-time schedule, rotating shift work, combination of days/nights and/or evenings, regular day shifts and on-call at other times, regular night shifts and on-call at other times, regular rotating shifts and on-call at other times, only on-call, and other).
Those who indicated that they work rotating shifts were asked the following questions: “Please briefly describe your rest, nap or sleep environment at work” (open response); “If you are allowed the opportunity to recline or nap on-shift, which one of the following do you do most of the time?” (I will try not to rest or sleep, I will rest but not close eyes, I will recline and close my eyes but try not to fall asleep, I will recline and may fall asleep, I will recline and actively try to sleep); If participants chose any response that indicated that they do not try to sleep (“I will not try to rest or sleep”; “I will rest but not close eyes; “I will recline and close my eyes but try not to fall asleep), they were then asked the two following questions: “Why do you choose not to sleep while on-shift?” (open response); “Do you ever avoid sleeping/napping while on evening or night shift to avoid feeling groggy if you need to attend an emergency event?” (yes/no).
Those who indicated that they do on-call work were asked the following questions regarding sleeping while on-call: “If you work or volunteer on call, are you:” (on-call from home, on-call on-site, mix of on-call from home and on-site); “Typically if you are on-call, do you sleep at any time during the on-call period?”(yes/no); “Why do you choose not to sleep during your on-call period?” (open response); “Do you ever avoid sleeping/napping while on-call to avoid feeling groggy or half-asleep if you receive a call?” (yes/no).
Experiences of Sleep Inertia in the Emergency Service Role
This section sought to determine how often participants experience sleep inertia, whether sleep inertia is a concern for them, and if they used any strategies to reduce sleep inertia. Given that sleep inertia is not a commonly used term in the general public, participants were first provided with the following definition of sleep inertia and sleep inertia countermeasures:
Sleep inertia is the groggy, sleepy state that you may feel immediately after waking. During sleep inertia you also tend to perform tasks worse than compared to when you’re wide awake. Sleep inertia is worse immediately after waking and gets better over time. It can take 20–30 minutes for sleep inertia to wear off, but full recovery can take up to 2 hours or more. Sleep inertia countermeasures are strategies that can be used to reduce sleep inertia, thus helping you to wake up quicker.
Using a 5-point Likert scale, participants were asked “how often do you experience sleep inertia when you wake to immediately respond to your emergency service role?” (1 = always, 5 = never). Participants were then asked, “is sleep inertia a concern for you personally?” (yes/no) and “is sleep inertia a concern for you broadly? (eg, in regard to the safety of others)” (yes/no). Participants were then asked to describe why sleep inertia is or is not a concern for them (open response). Finally, participants were asked “do you do anything in particular to help wake yourself up (ie, reduce sleep inertia) when woken to immediately respond for your emergency services role?” (yes/no). If participants selected ‘yes’ they were then asked, “what do you typically do to help wake yourself up (ie, reduce sleep inertia) when woken to respond for your emergency services role?” (open response). Using a 5-point Likert scale, participants were then asked, “How much does your waking procedure described above actually help to wake you up?” (1 = Does not wake me up, 5 = Completely wakes me up.
Barriers to Sleep Inertia Countermeasures
This section introduced participants to seven different reactive sleep inertia countermeasures that have previously been investigated, or their potential discussed in the literature. These included: 1) a short burst of exercise on equipment (eg, a stationary bike);34,38–40 2) a short burst of exercise without equipment (eg, star jumps);41 3) chewing caffeinated gum upon waking;25 4) face washing upon waking;27 5) drinking a cup of coffee upon waking;27 6) exposure to bright light upon waking;27 and 7) listening to up-beat music upon waking.29,30
For each of the seven countermeasures, participants were asked “Please select from the following list, what would be the main barriers, if any, to introducing this strategy into your workplace?” Options included: accessibility of equipment (workplace does not have the equipment); space; cost; comfort; time (it would take too long); workplace would not support or allow it; this strategy is already formally used in my workplace; no barriers. Participants were also given the option to select “Other barriers” and were provided with a text box to describe the other potential barriers. If participants chose “This strategy is already formally used in my workplace” they were provided with a text box to describe how this strategy was being used in their workplace. To identify which strategies participants were willing to use, participants were provided with the list of seven countermeasures and asked “Which of these strategies would you actually want to use? Please select ‘yes’ if you would use this strategy or ‘no’ if you would not use this strategy. If you select ‘no’ please briefly explain why you would not use this strategy.” Using the same method, participants were then asked “Which of these strategies do you believe would actually reduce sleep inertia? Please select “yes” if you believe this strategy would reduce sleep inertia or “no” if you believe this strategy would not reduce sleep inertia. If you select “no” please briefly explain why you believe this strategy would not reduce sleep inertia.
Existing Workplace Sleep Inertia Countermeasures and Recommendations
The final section allowed participants to describe any other strategies that they thought might reduce sleep inertia in their workplace. Participants were asked “Does your emergency service workplace or volunteer organization have any management strategies for sleep inertia that have not yet been covered in this survey?” (yes/no). If participants indicated “yes”, they were then provided with a text box to describe the strategy(ies), a text box to describe whether the strategy(ies) are successful in reducing sleep inertia, and whether people use these strategies in their organization (yes/no). Participants were then provided with a text box and asked “What changes could be made in your workplace to reduce sleep inertia? (E.g., this may include things such as changing shift schedules). Please be as specific as possible.” Finally, participants were provided with a text box and asked “Are there any other strategies that have not yet been covered in this survey that you think would work in reducing sleep inertia?” A final text box was provided for participants to offer any additional information about sleep inertia and their workplace.
Data Analysis
Quantitative data were analysed descriptively using SPSS Version 26.0 (IBM, Armonk, New York). All string values were recoded into numerical values so that frequency of responses and/or descriptive statistics could be calculated. Qualitative data were thematically analysed using NVivo 12 (QSR International, Victoria, Australia) whereby key themes were extracted from the responses. For qualitative responses, in cases where few responses were provided (for example, where the question only applied to a small number of responders), all responses were reported. The statistical approach for each research question is detailed below.
RQ1: Is Sleep Inertia a Concern for Emergency Service Personnel?
Frequency of responses in categories were generated for the questions: “How often do you experience sleep inertia?”, “Is sleep inertia a personal concern to you?”, “Is sleep inertia a broad concern to you?”, “Do you do anything in particular to help wake yourself up (ie, reduce sleep inertia) when woken to immediately respond for your emergency services role?”, and “how effective is your wake-up procedure in waking you up?” Qualitative responses for the questions “Why is sleep inertia a personal concern for you?”, “Why is sleep inertia a broad concern for you?”, and “What do you typically do to help wake yourself up (ie, reduce sleep inertia) when woken to respond for your emergency services role?” were thematically analysed and key themes were reported.
RQ2: What Sleep Inertia Countermeasures are Already Being Used by Emergency Service Organizations?
The frequency of participants who selected the response “This strategy is already formally used in my workplace” was calculated for each sleep inertia countermeasure. Following this, the average rating for perceived effectiveness of each countermeasure was determined. Due to the low frequency in responses for each countermeasure, qualitative descriptions of how the countermeasure is used in the workplace were not thematically analysed and instead all responses provided were reported. Frequency of “yes” responses were calculated for the question “does your emergency service workplace/organization have any management strategies for sleep inertia that have not yet been covered in this survey?” Qualitative descriptions of existing sleep inertia management strategies were categorized into either “formal” or “informal” strategies.
RQ3: What are the Barriers to Implementing Sleep Inertia Countermeasures for Emergency Service Personnel?
For each sleep inertia countermeasure, frequency of responses was calculated for each type of perceived barrier (accessibility of equipment, space, cost, comfort, takes too long, workplace would not support or allow it, other barriers, no barrier). Qualitative responses related to the “other barriers” option were reported. For each countermeasure, frequency of responses was also calculated for the questions “would you use this strategy (yes/no)” and “do you believe this strategy would reduce sleep inertia (yes/no)” Qualitative responses for why participants would not use this strategy or did not believe the strategy would reduce sleep inertia were thematically analysed and key themes reported.
RQ4: What Changes Could Be Made in Emergency Service Workplaces to Reduce the Impact of Sleep Inertia?
Qualitative responses to the question “what changes could be made in your workplace to reduce sleep inertia” were thematically analysed and key themes reported.
Results
The sample demographic variables including sex, age, emergency service industry, length of service, and type of schedule are reported in Table 1.
Sleeping on Shift and When On-Call
A quarter (25%) of shift workers indicated that, while they had the opportunity to nap or rest while on shift, they chose not to sleep to avoid sleep inertia. Sleep environments for shift workers on-site included dedicated bedrooms with beds and shared rooms with recliners. The majority (95%) of on-call personnel slept while on-call. Of the participants who indicated that they did not sleep while on-call, none specified that they avoided sleeping specifically to avoid sleep inertia.
RQ1: Is Sleep Inertia a Concern for Emergency Service Personnel?
Prevalence of Sleep Inertia Experiences While Responding to Their Emergency Role
When asked about how often participants experienced sleep inertia, 96% of participants indicated that they experienced sleep inertia at some time (ie, all categories except never) when responding to their emergency role. When responding to their emergency service role, participants indicated that they experience sleep inertia: always, 7%; often, 25%; sometimes, 42%, rarely 22%; and never, 4%.
Is Sleep Inertia a Concern for Emergency Service Personnel?
Participants were asked to indicate whether sleep inertia is a concern to them personally, or broadly (ie, regarding the safety others). As illustrated in Figure 1, approximately 45% of participants indicated that sleep inertia is a concern for them personally, and 65% indicated that sleep inertia is a concern for them broadly (in regard to the safety of others). Overall, a majority of participants (67%) indicated some level of concern about sleep inertia (either personally, broadly, or both). Qualitative analyses revealed that when asked to describe why sleep inertia was a personal concern, two main themes emerged: 1) concerns regarding cognitive errors and 2) concerns with driving immediately after waking. With regard to cognitive errors, participants were most concerned about errors related to their job performance with many reporting concerns about their ability to undertake complex tasks and perform at their best while experiencing sleep inertia (see Table 2 for illustrative quotes). One respondent described in detail a serious incident that occurred that they attributed to sleep inertia (see Table 2, Cognitive errors, quote #1). In addition, many participants expressed concern that sleep inertia may impact their judgement, decision-making, and ability to mentally focus. With regard to driving, participants were most concerned about their ability to operate their vehicle and navigate safely while experiencing sleep inertia (see Table 2).
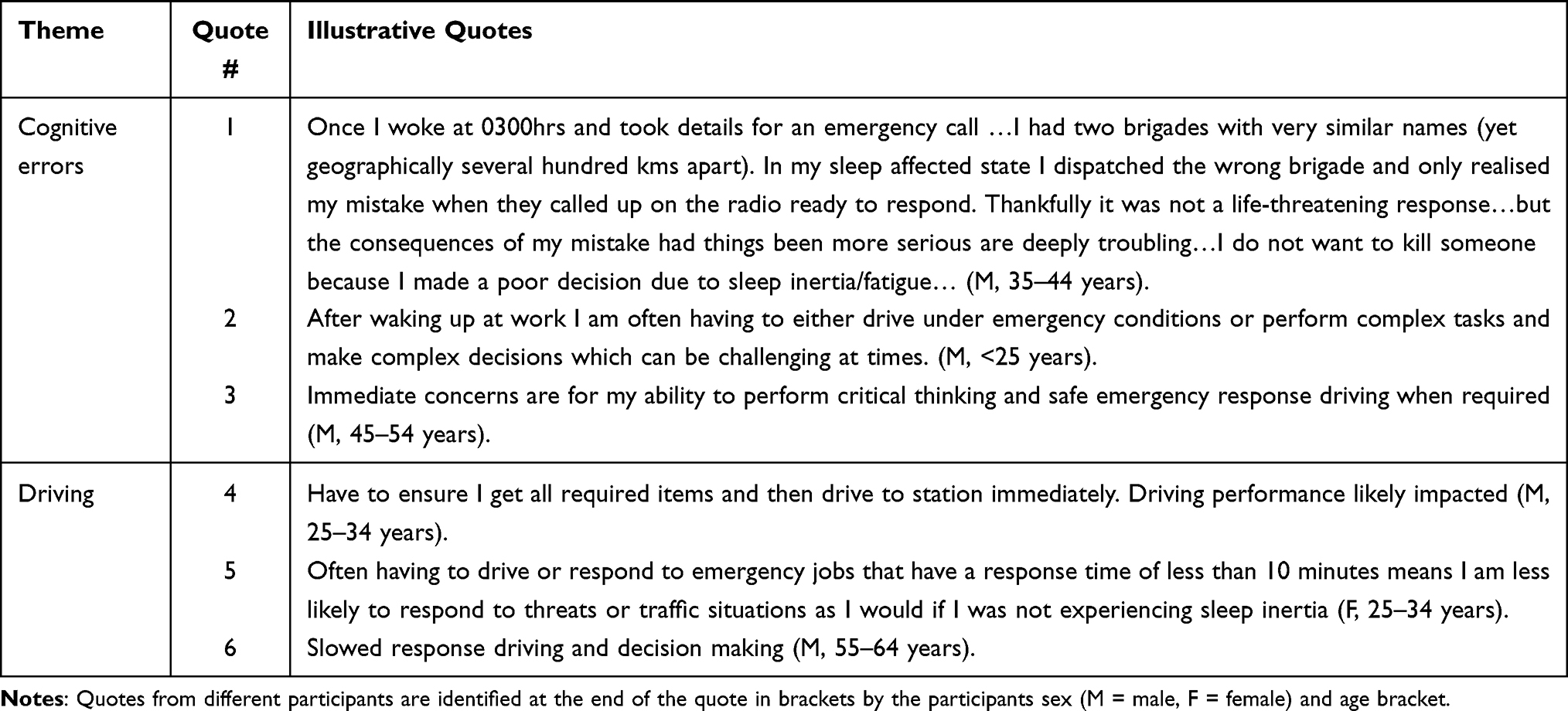 |
Table 2 Themes and Illustrative Quotes for the Question “Why is Sleep Inertia a Concern for You Personally?” |
 |
Figure 1 Percentage of respondents who indicated that sleep inertia is a concern for them personally, broadly and combined percentage of concern (percentage of respondents who indicated either personal or broad concern regarding sleep inertia). |
When asked to describe why sleep inertia was a broad concern, the main themes that emerged were concern for 1) driving with regard to the safety of colleagues and other road users, 2) impaired performance, and 3) not knowing if colleagues are performing at their best. For illustrative quotes see Table 3.
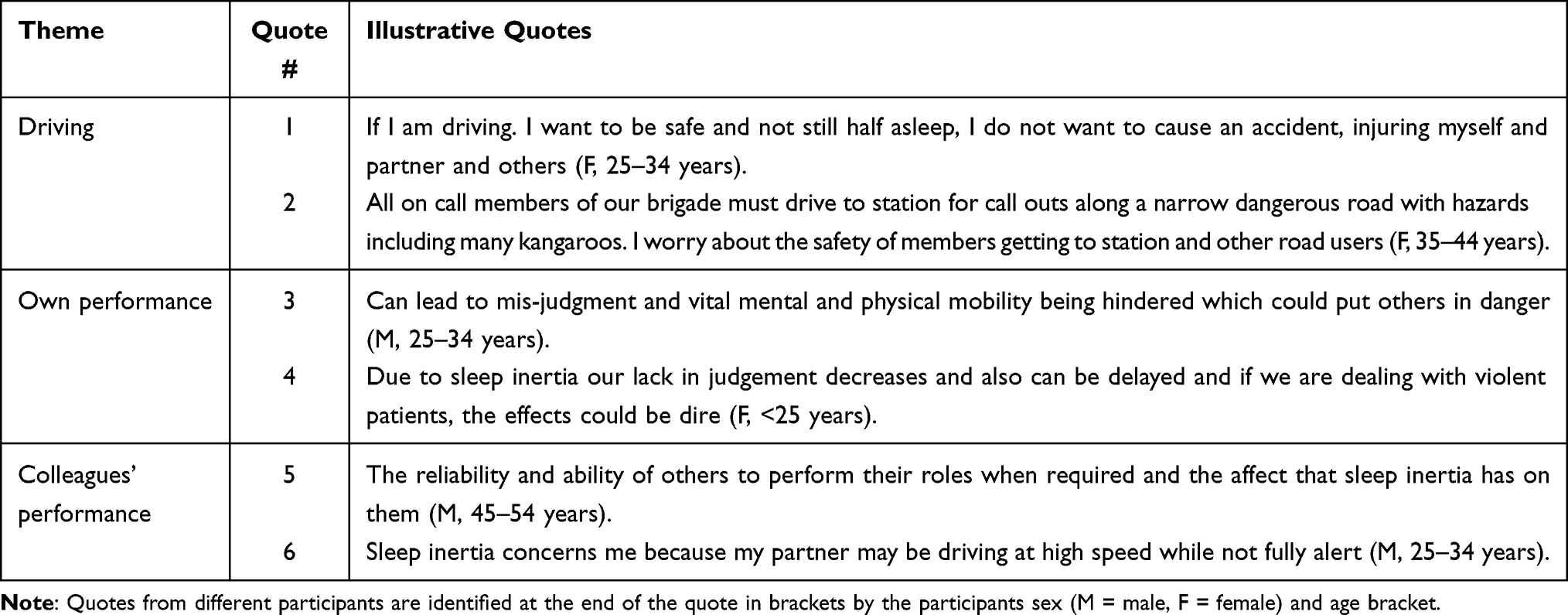 |
Table 3 Themes and Illustrative Quotes for the Question “Why is Sleep Inertia a Concern for You Broadly?” |
When asked “Do you do anything in particular to help wake yourself up when woken to immediately respond for your emergency role?” 33% of participants selected “yes”. Table 4 summarises the strategies reported, the percentage of participants who indicated they used each strategy and the average perceived effectiveness of each strategy. Overall, on average, participants felt that their personal strategies were effective to some extent in helping them wake up (M = 3.5, SD = 0.36; where 1 = the strategy “does not wake me up” and 5 = the strategy “completely wakes me up”).
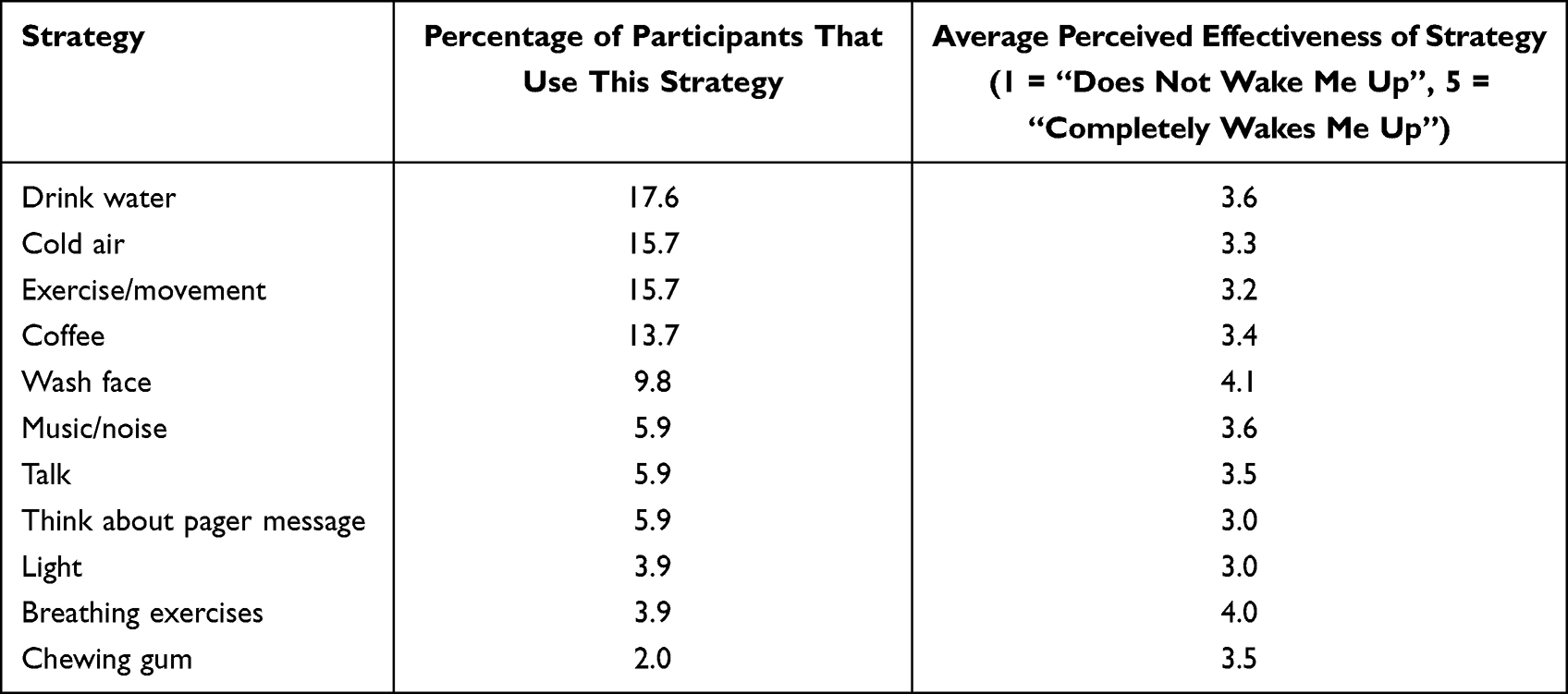 |
Table 4 Personal Strategies Used by Participants to Help Wake Up |
RQ2: What Sleep Inertia Countermeasures are Already Being Used by Emergency Organizations?
To address this research question, we looked at the frequency of responses of “This strategy is already formally used in my workplace” for each reactive sleep inertia countermeasure in the survey. Three out of the seven sleep inertia countermeasures included in this survey were already being used in the workplace: Exposure to bright light (12% of participants), drinking coffee (4% of participants) and listening to music (2% of participants). When asked how exposure to bright light is used to manage sleep inertia in the workplace, those who indicated that they are on-call from home described turning on lights around the house upon waking. Those who indicated that they are on-call and located at work described bright light being used at the station, operations, and communication rooms. Drinking coffee upon waking was primarily used by on-call participants to manage sleep inertia in the workplace as part of fatigue management policy and was often provided by the workplace. Finally, descriptions of how listening to music is used to manage sleep inertia in the workplace indicated that this strategy was used informally by individuals rather than strategically to manage sleep inertia, for example, workers may play music on the way to a job. For all three countermeasures that were already being used in the workplace, participants rated these strategies, on average, as “somewhat effective” at reducing sleep inertia.
This research question was further addressed with the survey question “Does your emergency service workplace or volunteer organization have any management strategies for sleep inertia that have not yet been covered in this survey?” Eight percent of participants indicated that their workplace had strategies to manage sleep inertia outside of those strategies already described in this survey. The strategies reported by participants fell into two categories “formal strategies” and “informal strategies”. Formal strategies included stand down periods if fatigued, extra oversight or supervision, and formal operational fatigue management including limits on shift durations and number of days rostered on and off. Informal strategies included avoiding sleeping, waking to the loud alarm of the pager (the alarm itself was alerting), changing outfits before going to the station, and choosing to sleep on site.
RQ3: What are the Barriers to Implementing Sleep Inertia Countermeasures for Emergency Service Personnel?
Figure 2 depicts the percentage of participants who indicated that they believed each countermeasure would work and the percentage of participants who indicated that they would use each countermeasure.
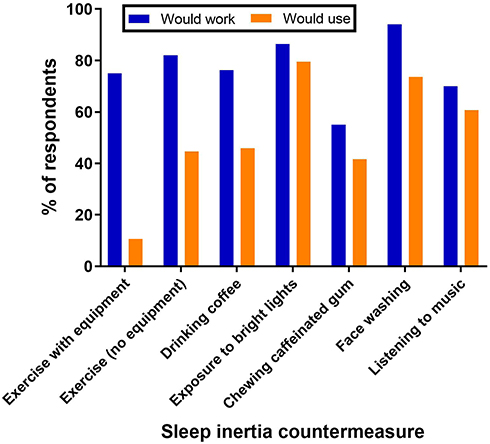 |
Figure 2 A comparison of the percentage of respondents who indicated that they believed each countermeasure would work in reducing sleep inertia with the percentage of respondents who indicate that they would use each countermeasure. |
Figure 3 depicts the prevalence of perceived barriers (accessibility of equipment, space, cost, comfort, time, workplace would not allow) for each sleep inertia countermeasure as indicated by participants.
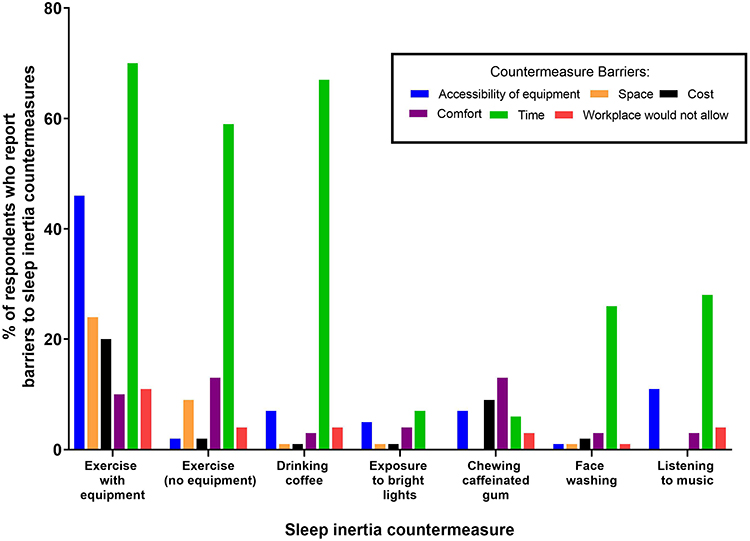 |
Figure 3 Prevalence of perceived barriers reported for each sleep inertia countermeasure. Note: The percentage of participants who reported “no barrier” for each sleep inertia countermeasure is reported in text. |
Exercise with Equipment
Exercise with equipment had the most perceived barriers of all sleep inertia countermeasures (Figure 3). The top 3 barriers for exercise with equipment were time (70%), accessibility of equipment (46%), and space (24%). In addition to the barriers provided in the survey, other barriers to exercise with equipment included “waking the household”. Thirty-three percent of participants believed that there were no barriers for exercise with equipment as a sleep inertia countermeasure. Ten percent of participants reported that they would use exercise with equipment as a sleep inertia countermeasure. Of those who said they would not use exercise with equipment, reasons reported included “no motivation” and “it will impede my performance”. Seventy percent of participants believed that exercise with equipment would work in reducing sleep inertia. Of those who said they do not think that exercise would work, reasons reported included “it would make me more tired” and “no time”.
Exercise with No Equipment
The top 3 barriers for exercise with no equipment included time (59%), comfort (13%), and space (9%). In addition to the barriers provided in the survey, other barriers to exercise with no equipment included “waking the household” and “potential for injury”. Thirty percent of participants believed that there were no barriers to using exercise with no equipment as a sleep inertia countermeasure. Forty-four percent of participants reported that they would use exercise with no equipment as a sleep inertia countermeasure. Of those who indicated that they would not use exercise with no equipment, the main reason reported was “it would impede performance”. Eighty-one percent of participants believed that exercise with no equipment would work in reducing sleep inertia. Of those who said they do not think that exercise with no equipment would work, the main reason reported was “it would increase tiredness”.
Drinking a Cup of Coffee
The top 3 barriers for drinking a cup of coffee included time (67%), accessibility of equipment (7%) and workplace would not allow it (4%). In addition to the barriers provided in the survey, other barriers to drinking a cup of coffee included “dislike coffee” and “trouble returning to sleep after”. Twenty percent of participants believed that there were no barriers for drinking a cup of coffee as a sleep inertia countermeasure. Forty-six percent of participants reported that they would drink a cup of coffee as a sleep inertia countermeasure. Of those who reported that they would not use this strategy, reasons reported included “I dislike coffee” and “trouble returning to sleep”. Seventy-six percent of participants believed that drinking a cup of coffee would work in reducing sleep inertia. Those who indicated that they do not think that drinking a cup of coffee would work reported “it would take too long” and “caffeine affects people differently”.
Listening to Music
The top 3 barriers for listening to music included time (28%), accessibility of equipment (11%) and workplace would not allow it (4%). In addition to the barriers provided in the survey, other barriers to this strategy reported by participants included “it would interfere with work performance/concentration”. Fifty percent of participants believed that there were no barriers for listening to music. Sixty percent of participants reported that they would listen to music as a sleep inertia countermeasure. Of those who reported that they would not use this strategy, reasons included “it would interfere with work performance/concentration”, “would wake household” and “not appropriate”. Seventy percent of participants believed that listening to music would work in reducing sleep inertia. Of those who indicated that they do not think that listening to music would work, reasons included “it could make you sleepy” and “it would depend on the person”.
Chewing Caffeinated Gum
The top 3 barriers for chewing caffeinated gum included comfort (13%), cost (9%) and accessibility of equipment (7%). In addition to the barriers provided in the survey, other barriers to this strategy reported by participants included “dislike gum” and “trouble returning to sleep”. Fifty-two percent of participants believed that there were no barriers for chewing caffeinated gum. Forty-two percent of participants reported that they would use chewing caffeinated gum as a sleep inertia countermeasure. Of those who reported that they would not use this strategy, reasons included: “dislike gum”, “don’t tolerate caffeine”, “trouble falling back asleep”, “not healthy”, and “dislike chemical stimulation”. Fifty-five percent of participants believed that chewing caffeinated gum would work in reducing sleep inertia. Of those who indicated that they do not think that chewing caffeinated gum would work, reasons included “it would take too long to absorb”, “it would not be used” and “caffeine affects people differently”.
Face Washing
The top 3 barriers for face washing included time (26%), comfort (3%) and cost (2%). In addition to the barriers provided in the survey, other barriers to this strategy reported by participants included “it would wake the household”. Sixty-eight percent of participants believed that there were no barriers for face washing. Seventy-three percent of participants reported that they would use face washing as a sleep inertia countermeasure. Of those who reported that they would not use this strategy, reasons included “it would take too long”. Ninety-four percent of participants believed that face washing would work in reducing sleep inertia. Of those who indicated that they do not think that face washing would work, reasons included “it does not work based on personal experience”.
Exposure to Bright Light
The top 3 barriers for exposure to bright light included time (7%), accessibility of equipment (5%) and comfort (4%). In addition to the barriers provided in the survey, other barriers to this strategy reported by participants included “waking others” and “not practical while moving”. Approximately 62% of participants believed that were no barriers for exposure to bright light as a sleep inertia countermeasure. Eighty percent of participants reported that they would use exposure to bright light as a sleep inertia countermeasure. Of those who reported that they would not use this strategy, reasons reported included “it would wake the household” and “causes headaches”. Eighty-six percent of participants believed that exposure to bright light would work in reducing sleep inertia. Of those who indicated they do not think that exposure to bright light would work, reasons reported included “it would be annoying”.
RQ4: What Changes Could Be Made in Emergency Service Workplaces to Reduce the Impact of Sleep Inertia?
When asked what changes could be made in your workplace to reduce sleep inertia, recommendations fell into three key themes: no possible changes, shift changes, and operational changes. Illustrative quotes for each theme are provided in Table 5.
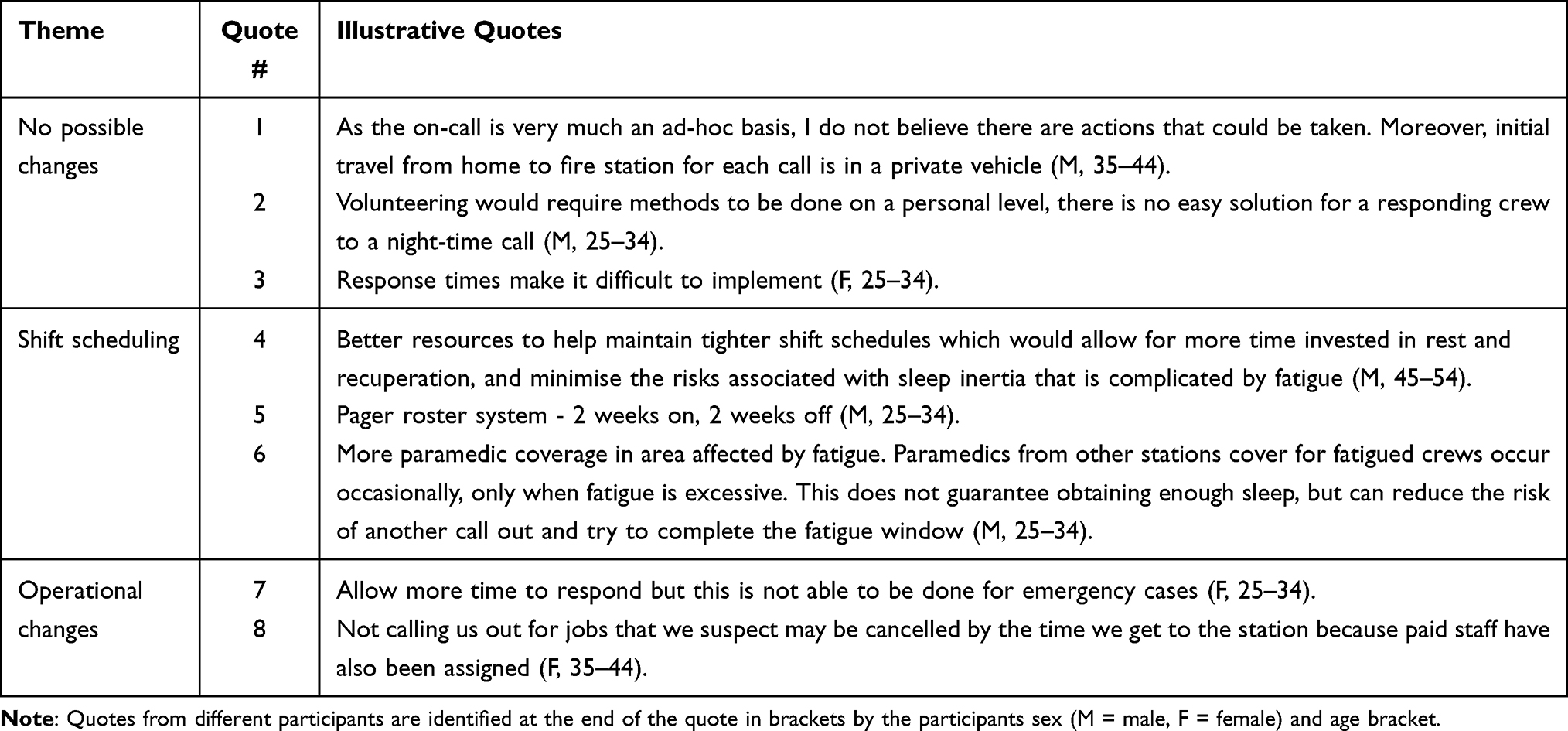 |
Table 5 Themes and Illustrative Quotes for the Question: What Changes Could Be Made in Emergency Service Workplaces to Reduce the Impact of Sleep Inertia? |
No Possible Changes
Approximately 38% of participants believed that there was nothing that could be done to reduce sleep inertia as part of their emergency service role. This was primarily due to the unpredictable 24/7 nature of the role (eg, see quote #1, Table 5). It was also noted that many volunteers are on-call from home, so it is impossible for workplaces to implement any formal management of sleep inertia with the responsibility for sleep inertia management lying with the individual (eg, see quote #2, Table 5). Time was also cited as a major barrier to implementing any sort of sleep inertia management strategy due to the short response times required for emergency situations (eg, see quote #3, Table 5).
Shift Scheduling
Various participants recommended changes in shift scheduling. These strategies were suggested to reduce fatigue and thus reduce the severity of sleep inertia. Such recommendations included changes in shift length to enable greater recovery time between shifts and reduce fatigue while on shift (eg, see quote #4, Table 5). Other participants recommended a rostering system for on-call volunteers, so that those with on-call arrangements have protected recovery time (eg, see quote #5, Table 5). Various participants reported the need to increase staffing levels to enable more recovery time for on-call staff (eg, see quote #6, Table 5).
Operational Changes
Participants recommended several on-shift operational changes to reduce the impact of sleep inertia prior to responding. These changes included delaying response times for non-urgent cases to allow sleep inertia to pass (eg, see quote #7, Table 5). In addition, screening of calls was suggested to reduce sleep being unnecessarily interrupted for false alarms or non-urgent calls (eg, see quote #8, Table 5). Other operational changes that were suggested included introducing reactive sleep inertia countermeasures, such as introducing bright light into stations and providing exercise equipment and coffee and providing education and improving awareness of sleep inertia for personnel.
Discussion
The primary aim of this exploratory study was to determine how sleep inertia is perceived by emergency service personnel and managed by their workplaces, as well as the barriers to implementing reactive sleep inertia countermeasures. Our findings suggest that sleep inertia is a concern for emergency service personnel; however, there are currently few formal strategies to manage sleep inertia implemented in the workplace. This gap in sleep inertia management may be attributed to the practical barriers to undertaking reactive sleep inertia countermeasures for emergency service personnel, with time being a major and unavoidable constraint for this cohort. These results suggest that strategies aimed at eliminating sleep inertia prior to starting work are unlikely to be feasible. Rather, a focus on reducing the magnitude of sleep inertia (eg, fatigue reduction strategies), and/or reducing the potential for errors while experiencing sleep inertia, should be explored for emergency service industries.
Our study found that sleep inertia is experienced by the majority of emergency service personnel, with 77% of participants reporting that they had experienced sleep inertia at some time while undertaking their emergency role. In addition, a third of participants either reported that they experienced sleep inertia “often” or “always” when responding in their emergency role, indicating that sleep inertia is a common experience for many personnel. Approximately two-thirds of participants reported that sleep inertia is a concern for them personally or broadly (ie, in relation to others). Participants’ personal concerns were mainly focused on their ability to perform their role adequately and to drive safely either to the station from their home or to incident sites from the station. Similarly, in other research, firefighters have reported major concerns with driving shortly after waking, particularly in relation to staying alert.36 Participants’ broad concerns also related to their colleagues’ abilities to adequately perform their role and to drive safely. Such concerns regarding performance or driving ability while experiencing sleep inertia are not unfounded since sleep inertia is associated with impairments to various aspects of cognition.42 With regard to driving, a recent study found impairments to lane and speed-keeping abilities soon after waking from sleep.43 One participant in the current study attributed sleep inertia to an incident in which they dispatched an incorrect brigade and expressed concerns about the welfare of those being attended to, had they had not realized their mistake. Such a report clearly illustrates that sleep inertia can have potentially dire consequences in this field of work. Overall, emergency service personnel believe that sleep inertia has the potential to place themselves, their colleagues, other road users, and people that they may be attending to (eg, patients) at risk.
Despite the majority (67%) of participants reporting concerns with sleep inertia, less than 30% of participants reported that their workplace had strategies in place to manage sleep inertia. Approximately 20% of participants reported reactive sleep inertia countermeasures being implemented in their workplace and 8% of participants reported other strategies. Of the reactive sleep inertia countermeasures, bright lights, caffeine, and listening to music were used in some capacity in workplaces. Qualitative findings revealed that bright lights and caffeine were used at an organizational level as part of fatigue management strategies (eg, bright lights in the workplace and coffee available), whereas listening to music appeared to be an informal individual-level strategy (eg, individuals sometimes used the radio in vehicles). It is unknown, however, whether the implementation of these strategies in the workplace is resulting in measurable reductions in sleep inertia in personnel. As such, intervention effectiveness research is needed to determine the actual efficacy of sleep inertia interventions utilised in workplaces under real-world conditions.37
It is possible that the limited use of reactive sleep inertia countermeasures in emergency workplaces could be due to barriers for implementation. Indeed, our findings suggest that emergency service personnel believe there are motivational and practical barriers to implementing reactive sleep inertia countermeasures. With regard to motivational barriers, our results found that for all reactive sleep inertia countermeasure, over half of participants believed that they would be effective in reducing sleep inertia; however, only three countermeasures (exposure to bright light, face washing and listening to music) would be used by more than half of participants. This information is critical as attitudes towards sleep inertia countermeasures could determine whether the countermeasure is implemented. The theory of planned behavior suggests that people will engage in behavior if they believe that the behavior (eg, exposure to bright light) will lead to a valued outcome (eg, will reduce sleep inertia) and/or experience (eg, is convenient/comfortable).44 Reasons cited for not wanting to use reactive sleep inertia countermeasures were primarily based on motivation, comfort, and concerns it would impact negatively on others. Our findings suggest that while many participants believed that sleep inertia countermeasures would lead to a valued outcome (ie, reduce sleep inertia), many countermeasures would not necessarily lead to a valued experience (ie, the countermeasure would be uncomfortable or difficult to perform). As such, future research could focus efforts on sleep inertia countermeasures that participants a) believe will work, b) are willing to perform, and c) have some evidence base for reducing sleep inertia (for example, there is no evidence yet that face washing can significantly reduce sleep inertia).
Participants also perceived several practical barriers to sleep inertia countermeasures. Accessibility of equipment, space, cost, comfort, and workplace support were all considered barriers for all countermeasures to varying extents. However, time was perceived to be the greatest barrier for the majority (six out of seven) of the reactive countermeasures investigated in this study. Given that emergency service work is often time critical, having a limited amount of time to enact reactive sleep inertia countermeasures is an inherent and unavoidable characteristic of the emergency service role. Qualitative responses revealed that time-based concerns were related to how long it might take to undertake a countermeasure, for example, time needed to exercise, and how long it might take for the countermeasure to take effect, for example the onset of an effect of caffeine when chewing caffeinated gum. While reactive sleep inertia countermeasures may take time to complete, it is possible for some countermeasures (exercise, chewing gum, bright light exposure) to be implemented concurrently with other tasks to avoid any loss of time in responding to emergencies. For example, in research conducted by the present authors (currently under review), volunteer firefighters reported that they would incorporate short bursts of exercise to help wake up as part of their response to night-time calls. Specifically, some volunteers reported that they would intentionally run from their houses to their cars to drive to the station, and then they would run from their car to the station to help wake up. Given that our findings suggest that sleep inertia is a concern for emergency service personnel, it would be worthwhile further investigating ways that reactive sleep inertia countermeasures could be tailored and incorporated into the emergency response procedure for different emergency sectors and workplaces so that time is no longer a barrier. In some cases, this may not be possible and so interventions to minimize the severity or associated risks of sleep inertia should be explored, for example, by reducing the factors that lead to severe sleep inertia.39,40
Fatigue reduction strategies, for example, by reducing chronic sleep loss, may help to reduce the likelihood of personnel experiencing severe sleep inertia.17 According to only 8% of participants, fatigue management strategies were already used as strategies to manage sleep inertia in their workplace. Such strategies included stand down periods, limits on shift duration and numbers of days rostered on and off. In addition, fatigue management strategies were often suggested by participants when asked “what could be done in the workplace to manage sleep inertia”. Suggestions included reducing shift lengths, reducing on-call periods, and number of days on-call and screening calls to ensure that sleep is not interrupted by false alarms. While fatigue management strategies could play a role in reducing sleep inertia severity, there are potential financial constraints in doing so, for example, needing to employ more staff to reduce shift lengths or to screen calls for urgency. Such strategies may not be desirable or financially possible for all workplaces.
For workplaces where changes in shift arrangements (eg, reducing shift lengths, reducing on-call periods) are not feasible, another alternative to consider in managing sleep inertia risk may be operational changes. One example of an operational change suggested by participants was delaying response times for non-urgent calls so that personnel are not responding while experiencing sleep inertia. Given that driving performance (speed and lane-keeping) is improved 10 min post-wake, compared to initially upon waking,43 strategically delaying response times for a short period for non-urgent calls may be a practical and evidence-based strategy to manage sleep inertia for these situations. Another operational strategy reported by participants was extra oversight and supervision. Informal double-checking procedures have been reported by personnel in various fatigue-impacted industries and are advocated as a strategy to reduce fatigue-related accidents or errors.3,4,45–47 Delaying response times and extra oversight/double checking procedures could be implemented by workplaces without a substantial financial burden or extra staffing needs. Given that some of these strategies were reported as already being used in some workplaces, these strategies are potentially feasible to implement in emergency industries. Intervention effectiveness research could be conducted in workplaces already implementing strategies to manage sleep inertia (eg, drinking coffee, bright light, listening to music, extra oversight and double checking procedures) to determine to what extent such strategies are effectively implemented (ie, are they being used by personnel?) and the efficacy of the strategies in improving personnel safety (ie, are they reducing sleep inertia for personnel and improving safety?).37 Knowing the effectiveness of interventions could encourage the implementation of such interventions in workplaces where sleep inertia management is lacking.37
Limitations and Future Directions
Some limitations of this study should be considered. First, our sample was primarily made up of fire and rescue (69%) and ambulance personnel (21%), with a small percentage of state emergency service personnel (9%) and police officers (1%). It is possible that state emergency sectors and the police force have differing workplace conditions that may mean that our findings are not generalizable to personnel in these industries. Future field-based research on sleep inertia with emergency service personnel should aim for a larger sample with appropriate representation from all emergency industries. A larger sample would also allow for adequate statistical power to further investigate differences in sleep inertia concerns and perceived barriers for sleep inertia countermeasures between demographic variables such as age, schedule, length of service and emergency industry. Second, only Australian emergency service personnel were included in the sample and thus our findings may not generalize to emergency service personnel in other countries. An international sample may provide new insights on how sleep inertia is experienced and managed around the world. Third, while a definition of sleep inertia was provided in the survey to ensure that participants understood the term, this definition, particularly the statement regarding how sleep inertia can result in worse performance may have unintentionally primed participant responses. This could have resulted in an overestimation of participants’ negative experiences and concern about sleep inertia. While some priming may be unavoidable when providing the definition of sleep inertia, future studies could consider moderating the definition of sleep inertia provided to participants to limit any potential influence on responses. This may include adding that in some cases sleep inertia can resolve quickly and that there may be differences in how people experience sleep inertia. Acknowledging that individuals may experience sleep inertia differently may prompt participants to consider their own experiences of sleep inertia more deeply and could improve the validity of their responses. Fourth, this survey was effective in capturing a broad insight into the ways that workplaces manage sleep inertia; however, individuals and workplaces may have strategies to manage sleep inertia that are not recognized as such by personnel. In addition, there are other barriers to interventions that were not explored in depth in this study, such as organizational culture and values towards safety, which could impact the implementation and success of interventions. Future research could use qualitative interviews or focus groups to gain a deeper insight into how emergency workplaces manage sleep inertia, and organizational culture and values towards safety.
Conclusion
Our findings suggest that sleep inertia is a common and concerning experience for emergency service personnel which can affect themselves, their colleagues, bystanders, and individuals that they may be attending to as part of their role. While inherent to the on-call role, sleep inertia is a complicated problem to address in the emergency services sector with time perceived to be the main barrier in implementing reactive sleep inertia countermeasures. Investigations into how reactive sleep inertia countermeasures could be implemented concurrently into the emergency response procedure could help overcome this barrier. Further research into the efficacy of strategies to manage sleep inertia severity (ie, fatigue management strategies) and risk (ie, operational changes such as delaying response time or double-checking procedures) could be conducted and implemented in addition to reactive sleep inertia countermeasures where possible. Given that sleep inertia is a concern for emergency service personnel, it is important to determine effective and feasible strategies to manage or reduce the risk of sleep inertia in emergency sectors to protect the safety of personnel but also the community and individuals they serve.
Acknowledgments
The authors would like to sincerely thank the emergency service personnel who took the time to complete the survey and acknowledge the important work they do in protecting their communities.
Funding
Katya Kovac is supported by a Research Training Program scholarship through Central Queensland University and a South Australian Commonwealth scholarship.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lawrence D, Kyron M, Rikkers W, et al. Answering the Call: National Survey of the Mental Health and Wellbeing of Police and Emergency Services. Detailed Report. Perth Graduate School of Education: The University of Western Australia; 2018.
2. Courtney JA, Francis AJ, Paxton SJ. Caring for the country: fatigue, sleep and mental health in Australian rural paramedic shiftworkers. J Community Health. 2013;38(1):178–186. doi:10.1007/s10900-012-9599-z
3. Dawson D, Ferguson SA, Vincent GE. Safety implications of fatigue and sleep inertia for emergency services personnel. Sleep Med Rev. 2021;55:101386. doi:10.1016/j.smrv.2020.101386
4. Dawson D, Mayger K, Thomas MJ, Thompson K. Fatigue risk management by volunteer fire-fighters: use of informal strategies to augment formal policy. Accid Anal Prev. 2015;84:92–98. doi:10.1016/j.aap.2015.06.008
5. Paley MJ, Tepas DI. Fatigue and the shiftworker: firefighters working on a rotating shift schedule. Hum Factors. 1994;36(2):269–284. doi:10.1177/001872089403600208
6. Åkerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med. 2003;53(2):89–94. doi:10.1093/occmed/kqg046
7. Nicol A, Botterill J. On-call work and health: a review. Environ Health. 2004;3(1):15. doi:10.1186/1476-069X-3-15
8. Martin-Gill C, Barger LK, Moore CG, et al. Effects of napping during shift work on sleepiness and performance in emergency medical services personnel and similar shift workers: a systematic review and meta-analysis. Prehosp Emerg Care. 2018;22(sup1):47–57. doi:10.1080/10903127.2017.1376136
9. Patterson PD, Weaver MD, Guyette FX, Martin‐Gill C. Should public safety shift workers be allowed to nap while on duty? Am J Ind Med. 2020;63(10):843–850. doi:10.1002/ajim.23164
10. Ferguson SA, Paterson JL, Hall SJ, Jay SM, Aisbett B. On-call work: to sleep or not to sleep? It depends. Chronobiol Int. 2016;33(6):678–684. doi:10.3109/07420528.2016.1167714
11. Tassi P, Muzet A. Sleep inertia. Sleep Med Rev. 2000;4(4):341–353. doi:10.1053/smrv.2000.0098
12. Jewett ME, Wyatt JK, Ritz-De Cecco A, Khalsa S, Dijk D, Czeisler CA. Time course of sleep inertia dissipation in human performance and alertness. J Sleep Res. 1999;8(1):1–8. doi:10.1111/j.1365-2869.1999.00128.x
13. Dinges DF, Orne MT, Orne EC. Assessing performance upon abrupt awakening from naps during quasi-continuous operations. Behav Res Methods Instrum Comput. 1985;17(1):37–45. doi:10.3758/BF03200895
14. Bruck D, Pisani DL. The effects of sleep inertia on decision‐making performance. J Sleep Res. 1999;8(2):95–103. doi:10.1046/j.1365-2869.1999.00150.x
15. Scheer FA, Shea TJ, Hilton MF, Shea SA. An endogenous circadian rhythm in sleep inertia results in greatest cognitive impairment upon awakening during the biological night. J Biol Rhythms. 2008;23(4):353–361. doi:10.1177/0748730408318081
16. Feltin M, Broughton R. Differential effects of arousal from slow wave versus REM sleep. Psychophysiology. 1968;5(2):231.
17. McHill AW, Hull JT, Cohen DA, Wang W, Czeisler CA, Klerman EB. Chronic sleep restriction greatly magnifies performance decrements immediately after awakening. Sleep. 2019;42. doi:10.1093/sleep/zsz032
18. Sprajcer M, Jay SM, Vincent GE, Vakulin A, Lack L, Ferguson SA. The effects of anticipating a high‐stress task on sleep and performance during simulated on‐call work. J Sleep Res. 2018;27(6):e12691. doi:10.1111/jsr.12691
19. Sprajcer M, Jay SM, Vincent GE, Vakulin A, Lack L, Ferguson SA. Uncertain call likelihood negatively affects sleep and next-day cognitive performance while on-call in a laboratory environment. Chronobiol Int. 2018;35(6):838–848. doi:10.1080/07420528.2018.1466788
20. Vincent GE, Kovac K, Signal L, et al. What factors influence the sleep of on-call workers? Behav Sleep Med. 2021;19(2):255–272. doi:10.1080/15402002.2020.1733575
21. Wolkow A, Ferguson S, Aisbett B, Main L. Effects of work-related sleep restriction on acute physiological and psychological stress responses and their interactions: a review among emergency service personnel. Int J Occup Med Environ Health. 2015;28(2):183–208. doi:10.13075/ijomeh.1896.00227
22. Hilditch CJ, Dorrian J, Banks S. Time to wake up: reactive countermeasures to sleep inertia. Ind Health. 2016;54(6):528–541. doi:10.2486/indhealth.2015-0236
23. Dornbierer DA, Yerlikaya F, Wespi R, et al. A novel bedtime pulsatile-release caffeine formula ameliorates sleep inertia symptoms immediately upon awakening. Nature. 2021;11(1):1–12.
24. Van Dongen HP, Price NJ, Mullington JM, Szuba MP, Kapoor SC, Dinges DF. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep. 2001;24(7):813–819. doi:10.1093/sleep/24.7.813
25. Newman RA, Kamimori GH, Wesensten NJ, Picchioni D, Balkin TJ. Caffeine gum minimizes sleep inertia. Percept Mot Skills. 2013;116(1):280–293. doi:10.2466/29.22.25.PMS.116.1.280-293
26. Figueiro MG, Sahin L, Roohan C, Kalsher M, Plitnick B, Rea MS. Effects of red light on sleep inertia. Nat Sci Sleep. 2019;11:45. doi:10.2147/NSS.S195563
27. Hayashi M, Masuda A, Hori T. The alerting effects of caffeine, bright light and face washing after a short daytime nap. J Clin Neurophysiol. 2003;114(12):2268–2278. doi:10.1016/S1388-2457(03)00255-4
28. Hilditch C, Wong L, Bathurst N, et al. Rise and shine: the use of polychromatic short-wavelength-enriched light to mitigate sleep inertia at night following awakening from slow-wave sleep. J Sleep Res. 2022. doi:10.1111/jsr.13558
29. Hayashi M, Uchida C, Shoji T, Hori T. The effects of the preference for music on sleep inertia after a short daytime nap. Sleep Biol Rhythms. 2004;2(3):184–191. doi:10.1111/j.1479-8425.2004.00142.x
30. McFarlane SJ, Garcia JE, Verhagen DS, Dyer AG. Auditory countermeasures for sleep inertia: exploring the effect of melody and rhythm in an ecological context. Clocks Sleep. 2020;2(2):208–224. doi:10.3390/clockssleep2020017
31. Tassi P, Nicolas A, Dewasmes G, et al. Effects of noise on sleep inertia as a function of circadian placement of a one-hour nap. Percept Mot Skills. 1992;75(1):291–302. doi:10.2466/pms.1992.75.1.291
32. Kräuchi K, Cajochen C, Wirz‐Justice A. Waking up properly: is there a role of thermoregulation in sleep inertia? J Sleep Res. 2004;13(2):121–127. doi:10.1111/j.1365-2869.2004.00398.x
33. Krauchi K, Knoblauch V, Wirz-Justice A, Cajochen C. Challenging the sleep homeostat does not influence the thermoregulatory system in men: evidence from a nap vs. sleep-deprivation study. Am J Physiol Regul Integr Comp Physiol. 2006;290(4):R1052–R1061. doi:10.1152/ajpregu.00381.2005
34. Kovac K, Vincent GE, Paterson JL, et al. The impact of a short burst of exercise on sleep inertia. Physiol Behav. 2021;242:113617. doi:10.1016/j.physbeh.2021.113617
35. Ferrara M, Casagrande M, Porcu S, De Gennaro L, Bertini M. Sleep Inertia and on-Call Readiness. Defense Technical Information Centre; 2000.
36. Paterson JL, Aisbett B, Ferguson SA. Sound the alarm: health and safety risks associated with alarm response for salaried and retained metropolitan firefighters. Saf Sci. 2016;82:174–181. doi:10.1016/j.ssci.2015.09.024
37. Goldenhar LM, LaMontagne AD, Katz T, Heaney C, Landsbergis P. The intervention research process in occupational safety and health: an overview from the national occupational research agenda intervention effectiveness research team. J Occup Environ Med. 2001;43(7):616–622. doi:10.1097/00043764-200107000-00008
38. Kovac K, Vincent GE, Paterson JL, Aisbett B, Reynolds AC, Ferguson SA. Can an increase in noradrenaline induced by brief exercise counteract sleep inertia? Chronobiol Int. 2020;37(9–10):1474–1478. doi:10.1080/07420528.2020.1803900
39. McHill A, Hull J, Czeisler C, Klerman E. The effect of chronic sleep restriction and prior sleep duration on sleep inertia measured using cognitive performance. Sleep Med. 2017;40:e163. doi:10.1016/j.sleep.2017.11.480
40. Nielsen K, Taris TW, Cox T. The future of organizational interventions: addressing the challenges of today’s organizations. Work Stress. 2010;24(3):219–233. doi:10.1080/02678373.2010.519176
41. Kovac K, Ferguson SA, Paterson JL, et al. Exercising caution upon waking – can exercise reduce sleep inertia? Front Physiol. 2020;11:254. doi:10.3389/fphys.2020.00254
42. Trotti LM. Waking up is the hardest thing I do all day: sleep inertia and sleep drunkenness. Sleep Med Rev. 2016;35:76–84. doi:10.1016/j.smrv.2016.08.005
43. Wörle J, Metz B, Steinborn MB, Huestegge L, Baumann M. Differential effects of driver sleepiness and sleep inertia on driving behavior. Transp Res Part F. 2021;82:111–120. doi:10.1016/j.trf.2021.08.001
44. Ajzen I. The theory of planned behaviour. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
45. Ferrara, M. Casagrande, S. Porcu, L. De Gennaro, M. Bertini. Sleep Inertia and On-Call Readiness. In: Individual Differences in the Adaptability to Irregular Rest-Work Rhythms/Status of the Use of Drugs in Sleep-Wakefulness Management. Retrieved from Defense Technical Information Centre: https://discover.dtic.mil/; 2000.http://Ferrara(2000)Sleep inertia and on-call readiness.pdf
46. Dawson D, Chapman J, Thomas MJ. Fatigue-proofing: a new approach to reducing fatigue-related risk using the principles of error management. Sleep Med Rev. 2012;16(2):167–175. doi:10.1016/j.smrv.2011.05.004
47. Paterson JL, Aisbett B, Kovac K, Ferguson SA. Informal management of health and safety risks associated with alarm response by Australian firefighters. Ergonomics. 2021;65:1–20.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.