Back to Journals » Journal of Pain Research » Volume 19
“I See What Others Don’t See When They Look at Me”: A Qualitative Study of Body Perception Disturbances in Chronic Non-Cancer Pain
Authors Dagenais M ![]() , Roy JS, Pinard AM, Mercier C
, Roy JS, Pinard AM, Mercier C ![]()
Received 10 January 2026
Accepted for publication 11 April 2026
Published 12 June 2026 Volume 2026:19 594189
DOI https://doi.org/10.2147/JPR.S594189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Marion Dagenais,1,2 Jean-Sébastien Roy,1,2 Anne Marie Pinard,1– 3 Catherine Mercier1,2
1Faculty of Medicine, Laval University, Quebec City, QC, Canada; 2Center for Interdisciplinary Research in Rehabilitation and Social Integration (Cirris), CIUSSS de la Capitale-Nationale (Integrated University Health and Social Services Center for Capitale-Nationale), Quebec City, QC, Canada; 3CHU de Québec-Université Laval (Quebec City – Laval University Hospital Center), Quebec City, QC, Canada
Correspondence: Catherine Mercier, Email [email protected]
Purpose: Body perception disturbances, such as distorted perception of limb size, are well documented in specific pain conditions like complex regional pain syndrome but remain underexplored in chronic pain more broadly. This qualitative study aimed to explore how body perception disturbances manifest in individuals with chronic non-cancer pain.
Materials and Methods: Semi-structured interviews were conducted on a purposive sample of 15 adults (4 men; age range: 26– 76 years) with various chronic pain conditions (eg, fibromyalgia, musculoskeletal pain, migraine, endometriosis), pain severity (average pain intensity: 3 to 7.5 on a 0– 10 scale) and duration (range: 0.5– 53 years), and work status (eg, full-time worker, permanent disability). Interview transcripts were analyzed based on inductive/deductive hybrid thematic analysis principles.
Results: All participants reported body perception disturbances. Six main themes emerged, encompassing 21 sub-themes in total. The six main themes were as follows: (1) distortions of perceived body characteristics; (2) altered proprioceptive and postural awareness; (3) a shifted focus toward or away from the pain; (4) perturbed emotions and beliefs about the body; (5) neglect-like symptoms; and (6) a disturbed sense of agency.
Conclusion: Our results suggest that body perception disturbances are a common phenomenon across several chronic non-cancer pain conditions. Future research should examine body perception disturbances in large, heterogeneous samples to further describe its key features and underlying mechanisms.
Keywords: chronic pain, qualitative, body schema, body image, body ownership, distortion
Introduction
Body perception can be defined as how an individual perceives their own body.1 While not entirely agreed upon, the generally accepted view is that body perception consists of two types of body representations: the body schema and the body image.2,3 The body schema is a dynamic representation of the body which relies on sensorimotor integration to support action,4 whereas the body image encompasses perceptual, cognitive and emotional representations of the body.2,5 Both the body schema and the body image contribute to form a coherent perception of the body and are thought to interact dynamically.6 The present paper will focus on explicit body perception disturbances (ie, disturbances that one is aware of), which can affect both the body image and the body schema. This includes perceptual (eg, perceiving a body segment as larger), cognitive (eg, focusing attention on certain body parts) and emotional manifestations (eg, feeling distrustful toward the body), as well as sensorimotor disturbances (eg, struggling to produce smooth and precise movements).
Recent work has shown that chronic pain is often associated with body perception disturbances,7–10 which are thought to arise from maladaptive plastic changes in sensorimotor cortical representations.11–14 These disturbances can manifest explicitly, ie, the individual is aware of the distortions. For example, distortions of the perceived shape or size of painful body parts have been reported by individuals with chronic low-back pain (CLBP),15,16 complex regional pain syndrome (CRPS),17,18 and fibromyalgia.19 Feelings of foreignness or disownership toward the affected limb were also documented in the CRPS population.20,21 Body perception disturbances can also manifest implicitly, ie, the individual may not be aware of them. For example, a recent study showed that individuals with fibromyalgia had a significantly poorer performance in a laterality judgement task – a task thought to involve implicit motor imagery, thus relying on the body schema22 – compared to pain-free control participants.23 Another study showed that individuals with CRPS displayed an attentional bias affecting the personal space of the painful side of the body, with a tendency to deprioritize the painful side during temporal order judgement tasks.24
While body perception disturbances have been documented in chronic pain conditions such as CLBP, CRPS, and fibromyalgia, few studies have investigated these disturbances across heterogeneous chronic pain samples. With chronic pain being recognized as a disease in its own right,25 we sought to investigate body perception disturbances in chronic pain as a construct independent from a specific diagnosis or body region. Our team recently conducted a scoping review to identify self-reported questionnaires used to assess body perception disturbances in chronic non-cancer pain. This review allowed us to identify five key facets of this construct, which were distorted perceptions of the (1) size and (2) shape of the painful body part, (3) the presence of cognitive neglect-like symptoms, (4) impaired proprioceptive awareness (4), and (5) a disturbed sense of agency.26 Some questionnaires included additional facets of the construct (eg, the presence of motor neglect-like symptoms or distorted perceptions of the weight or temperature of the painful body part) that were not included in other questionnaires. However, the majority of questionnaires were developed for patients with either CRPS or CLBP. This raises the question of whether the five key facets apply to various chronic pain conditions or are specific to certain pain conditions, which would ultimately have clinical implications for assessing body perception disturbances in chronic pain populations. Drawing from these findings, we sought to explore how these facets would manifest, and whether new themes would arise from patients’ perspectives when conducting inductive/deductive interviews with individuals with heterogeneous profiles. The aim of this study was therefore to gain an in-depth understanding of how body perception disturbances manifest in persons living with various conditions of chronic non-cancer pain.
Methodology
Participants and Ethics Statement
Participants with chronic non-cancer pain were recruited and interviewed between June 2023 and November 2024. They were approached face-to-face, by telephone, or by email. The study was advertised by collaborating physicians at the Center of Expertise in Chronic Pain (CEGDC) in Quebec City and at the Institute of Rehabilitation in Physical Deficiency of Quebec City (IRDPQ), as well as through the research team’s personal and professional networks. Inclusion criteria were: adults (≥18 years old) with non-cancer pain persisting or recurring for ≥3 months. Cancer-related pain was excluded because of the emotional and psychological dimensions of cancer, which can influence body perception in a way that is uniquely different from other types of chronic pain.27–29 Purposive sampling was used to ensure the diversity of participants’ characteristics in terms of age, gender, pain condition(s) (diagnoses, pain intensity and duration), and work status.
All participants provided written informed consent prior to their enrollment, which included consent for the publication of anonymized quotes. The study adhered to the principles outlined in the Declaration of Helsinki, and the research protocol received approval from the local ethical review board (CIUSSS de la Capitale Nationale, Quebec City, QC, Canada, no MP-13-2024-2866). Participants were provided with a list of resources (both educational and supportive) to help them cope with any distressing feelings that may arise after participating in this study.
Research Team and Reflexivity
Research Team
The interviews were conducted by MD (she/her), an occupational therapist pursuing a PhD in rehabilitation sciences with over a decade of clinical and research experience working with individuals living with chronic pain. As this was MD’s first experience in qualitative research, she received support from a qualitative research consultant for the study design, data collection and data analysis. Three practice interviews were conducted before recruiting chronic pain participants, in person and via Zoom. Colleagues from our laboratory with relevant clinical and/or research experience with different pain conditions (CLBP, fibromyalgia, phantom limb pain) emulated participants with these conditions.
Relationship with Participants
Prior to enrollment, the interviewer personally contacted each potential participant (by Email or telephone) to verify eligibility, to explain the study, and to answer questions. Participants were informed of the interviewer’s credentials and the broader research aim of the research team, which is to document body perception disturbances associated with chronic pain.
Study Design
This study used a qualitative research design based on the principles of inductive/deductive hybrid thematic analysis.30 This approach was chosen because it allowed to explore a phenomenon – body perception disturbances – based on known themes derived from existing questionnaires26 – which include Galer and Jensen’s framework for neglect-like symptoms31 (ie, deductive), while also allowing new themes to emerge from the data (ie, inductive). Data collection consisted of a single semi-structured interview, taking place either in person at the Center for Interdisciplinary Research in Rehabilitation and Social Integration (Cirris) or on Zoom, which allowed individuals with different levels of disability and digital literacy to participate in the study. Apart from the first three interviews where a research intern (CB) was present, no one else besides the interviewer and participants were present during the interviews. The interviews were conducted in French. An audio recording was made using a recording device (in person) or via Zoom’s recording settings, and field notes were taken during the interviews (eg, non-verbal cues).
Procedure
During the week preceding the interview, each participant was provided with an image depicting the body outline of a woman or man figure, based on their self-reported gender. Participants were instructed to indicate any peculiarity that they might perceive about their body or a part of their body. This could be done by modifying the image on an electronic device, or by printing out the image. Peculiarities were defined as perceptions that could not be acknowledged by looking at or by touching the body. These body drawings were collected at the beginning of the meeting and were used to help orient some of the probing questions. No analyses were performed on the body drawings.
Participants’ Characteristics
Participants’ demographic (eg, age, self-reported gender, work status) and clinical characteristics (pain condition(s): diagnosis, duration; other pain condition(s); other health conditions; pain intensity (0–10): current pain, average pain over the last 7 days; work status) were gathered at the beginning of the interview.
Interviews
The interview procedure was standardized and consisted of open-ended questions about body perception disturbances, discussion about the body drawing, and a visualization and motor imagery exercise. Each interview started with a single open-ended question aiming to explore body perception disturbances (“I would like you to tell me about the peculiarities of how you perceive your body”). If participants were unsure about the question, a clarifying statement was made regarding what could be considered as a peculiarity (“Peculiarities could be perceptions that you have of the body/of a body part, but that are not visible or cannot be felt by touching the body/body part.”). Participants were also invited to discuss the elements they had drawn or written on the body drawing. Probing questions were then used to explore in more detail the elements and experiences described by participants (eg, “You mentioned […] Can you talk more about this?”; “In what context do you experience these perceptions?”; “You mentioned […]. How are these perceptions when your pain is high/low?”; “Can you tell me about the differences, if any, about the way you perceive the different parts of your body?”). Participants were also invited to do a visualization exercise to further explore body perception (“With your eyes closed, I would like you to visualize your body.”). Probing questions were used to elicit more details about their visualization (eg, “What do you see?”; “How clearly do you see it?”; “Please tell me about the differences, if any, in the way you visualize the different parts of your body.”). Participants were then invited to do a visualization and motor imagery exercise to explore the ability to perform imagined movements with painful and non-painful parts of the body (“Still with your eyes closed, and without moving your [body part], I would like you to visualize [this movement].”). Again, probing questions were used to elicit additional details about participants’ experience (eg, “Tell me about the differences, if any, between your ability to do [this movement] in real life, and your ability to do it mentally.”; “What makes this exercise difficult?”). Finally, additional questions aiming to explore themes drawn from questionnaires assessing body perception disturbances in individuals with chronic pain26 were asked to gather relevant experience related to these themes, if applicable. The interview duration varied depending on the participants’ answers. See Appendix S1 for the complete interview guide.
Data Analysis
The audio recordings of the interviews were transcribed using a transcription service (transcribeme.com). Neither the interview transcripts nor the findings were provided to participants for feedback. However, participants could be solicited for transcript corrections if the transcription process had failed to transcribe some parts of the interview (eg, poor audio quality). Verbatims were then coded iteratively and inductively with the NVivo software (NVivo 14, Lumivero, 2023), and new emerging themes were gathered in a saturation matrix to assess data saturation. Data saturation was defined as two interviews without any new emerging theme. The first three interviews, which served as a calibration phase for coding, were independently coded by two evaluators (MD, and CB, a research intern with a bachelor’s degree in occupational therapy) and reviewed by a third evaluator (CM, occupational therapist and senior researcher that has performed research in various chronic pain populations for over two decades). During the calibration phase, MD and CB reviewed all three interviews in full. Any disagreements were identified and discussed, and the two evaluators reached a consensus. If a consensus could not be reached, the disagreements were discussed with CM, who made the final decision. The remaining interviews were coded by one evaluator (MD) and reviewed by a second evaluator (CM). Any disagreements identified by CM were discussed with MD to reach a consensus. If a consensus could not be reached, the final decision was made by CM. While coding was performed inductively (ie, iterative coding was used to build a codebook/framework), concept classification was also informed by known facets of the construct which were drawn from self-reported questionnaires assessing body perception disturbances in chronic non-cancer pain (ie, deductive thematic analysis).26 Once data saturation was reached, the themes were thoroughly reviewed, and a final classification arose. Ultimately, the verbatim extracts chosen for this article were translated from French to English using an online translator (DeepL Translate) and were carefully reviewed by a bilingual researcher (MD). Original and translated verbatim extracts are provided in Appendix S2.
Results
Fifteen participants took part in this study. Data saturation (ie, two interviews without any new emerging theme) was reached after 10 interviews (see Appendix S3 for the saturation matrix), however recruitment continued to ensure greater diversity in the sample. There were no refusals to participate nor drop-outs. Interview duration ranged from 50 minutes to 2 hours and 50 minutes. There were no repeat interviews. In one case, the interview transcript was sent to the participant (Participant 13) for corrections. This was done because some parts of the audio recording were unclear due to internet connection issues during the Zoom interview. Our sample consisted of four men and eleven women aged between 26 and 76 years old, with various pain conditions, pain intensity (average pain intensity ranging from 3 to 7.5 on a scale of 0 to 10), pain chronicity (pain duration ranging from 6 months to 53 years), and work status (ranging from full-time work to permanent disability). Individual participants’ characteristics are reported in Table 1. All 15 participants reported some elements of body perception disturbances during the interviews. Body drawings made by participants were also used to explore in details participants’ perceptions. Figure 1 shows body drawings from two participants with different pain conditions (Participant 01: Figure 1A; Participant 08: Figure 1B). These participants’ drawings were selected because they are representative of different manifestations of body perception disturbances.
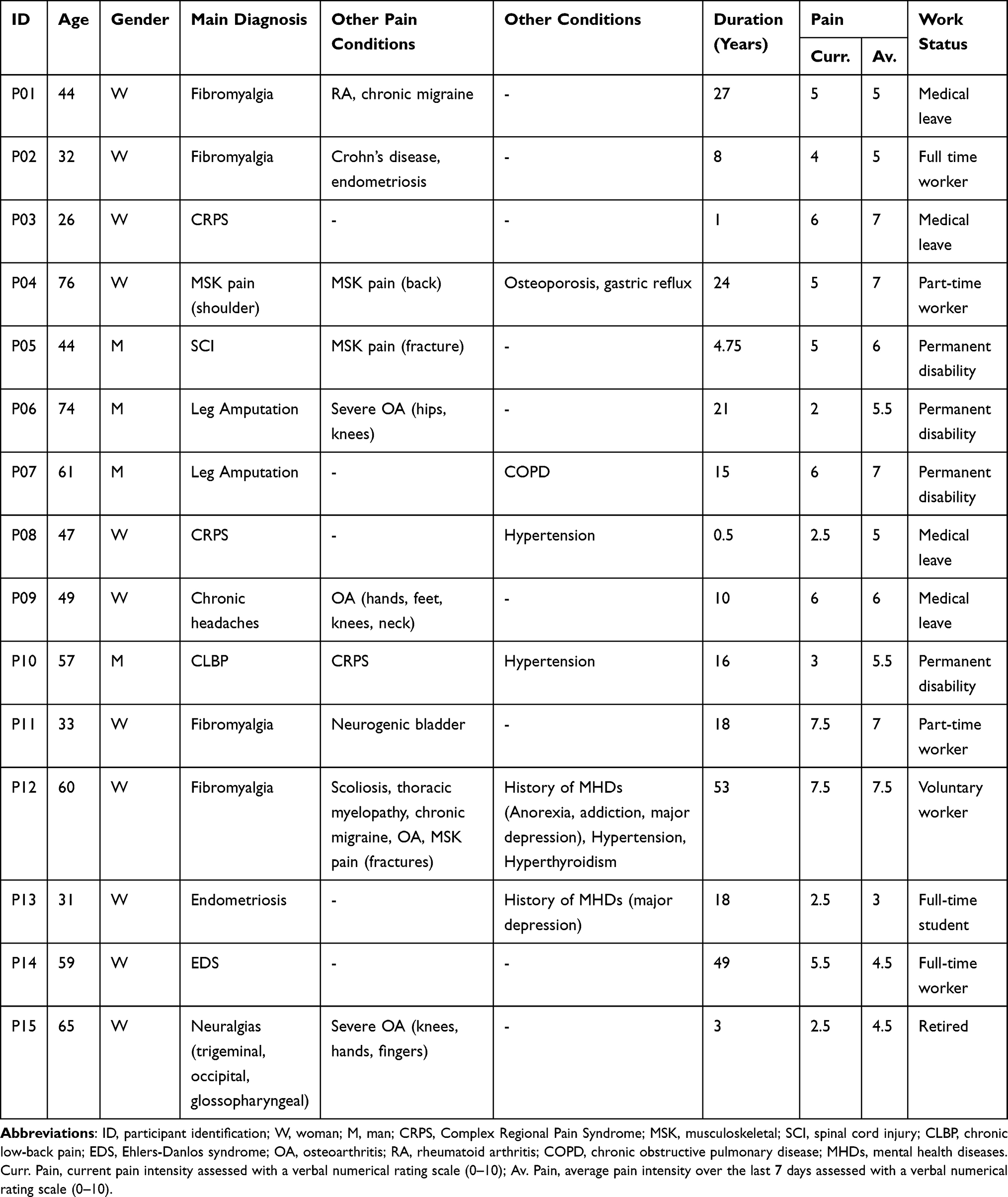 |
Table 1 Participants’ Characteristics |
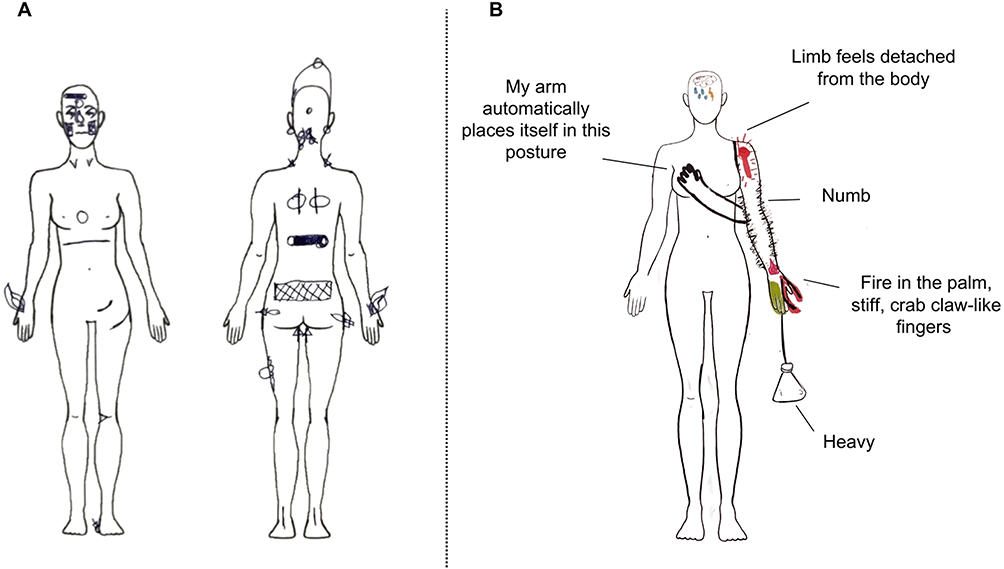 |
Figure 1 Body drawings of Participant 01 (A) and Participant 08 (B). Participants were asked to draw any peculiarity they perceived about their body. Participant 08 gave written details about some of her perceptions. These details were translated in English for the purpose if this article. |
Emerging Themes
Six main themes pertaining to body perception disturbances emerged from the interviews, each encompassing relevant sub-themes (see Figure 2 for details). The six main themes were: (1) distortions of perceived body characteristics (n=15 participants); (2) altered proprioceptive and postural awareness (n=15 participants); (3) a shifted focus toward or away from the pain (n=14 participants); (4) perturbed emotions and beliefs about the body (n=14 participants); (5) neglect-like symptoms (n=10 participants); and (6) a disturbed sense of agency (n=8 participants).
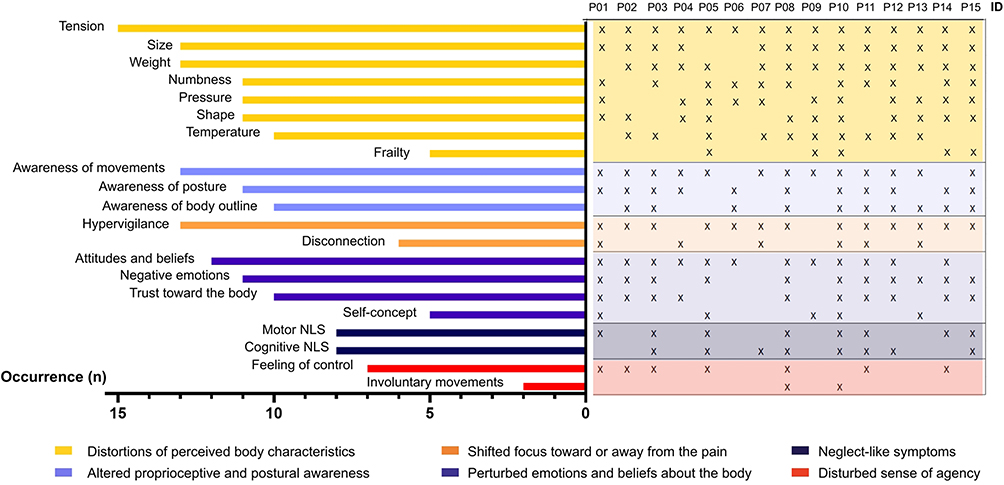 |
Figure 2 Themes and sub-themes of body perception disturbances and their occurrence among study participants (identified with an “X” mark). All 15 participants reported elements of disturbances in at least three of the six main themes (three themes: n=1; four themes: n=4; five themes: n=3; six themes: n=7). Abbreviations: ID, Participant identification; NLS, Neglect-like symptoms. |
Theme 1 - Distortions of Perceived Body Characteristics
All 15 participants reported relevant elements relating to distortions of perceived body characteristics. This theme encompassed eight sub-themes, all of which pertained to discrepancies between how the body or body part is perceived and its actual state. These sub-themes were as follows: tension, size, weight, numbness, pressure, shape, temperature, and frailty.
Tension
This sub-theme related to the perception of tension, tightness, rigidity and twisting in different parts of the body. All 15 participants evoked some elements related to this sub-theme. For example, one participant said:
Um. Well, in the joints, the feeling is really, um. Like, it’s. Everything is tight inside, it can’t move much. (P02).
Another participant mentioned:As if I were frozen in concrete, then I go, ‘Oh no, okay, it’s fine, it’s in my head.’ You know. It’s still soft. (P05).
Size
Thirteen participants described distortions regarding the perceived size of painful body parts. In all but one case, participants described their painful body parts as feeling bigger than they were. For example, one participant said:
I feel like my hand is… big, thick, as if it were full, full of water. Like, say, around Halloween time, the rubber masks at [the dollar store] are really thick. It’s like my hand is like that. (P03).
Another participant mentioned that when pain was greater following joint subluxation for example (which she experienced repeatedly because of Ehlers–Danlos syndrome), she perceived her body part as being oversized:
When my shoulder hurts, when I subluxate my shoulder, it feels like it’s oversized. (P14).
In one case, a participant (P09) recalled an instance in which she had experienced a headache and felt as though her eyes were smaller:It was as if [my eyes] were small and had difficulty opening.
Weight
Distortions in the perceived weight of the body were reported by 13 participants. These distortions mainly affected painful body parts:
My eyelids, it’s a bit as if they were heavy, as if they were going to—it’s hard to explain, I can’t really describe it, but it’s like a heavy weight. (P09).
However, some participants also mentioned having a global feeling of heaviness:My God, yes, my body feels heavy. When I have to stand up, I feel like—it’s as if there’s a weight crushing me all the time, but it’s more like it starts at my shoulders. It’s as if I’m always too heavy or too—and when I walk, I don’t walk the same way anymore. (p12).
In all but one case, participants who reported distortions in perceived weight said that their body or body parts felt heavier. The only account of a body part feeling lighter was that of a phantom limb, which felt heavier when pain was more intense and lighter when pain was less intense:
I would say that… it’s lighter [the phantom leg]. (…) Yes, it varies. It varies. Some days it’s heavier. It varies depending on the pain. (P07).
Numbness
Eleven participants described certain parts of their body as numb, fuzzy, diffuse, or tingling; these accounts were grouped under the Numbness sub-theme. Specifically, these perceptions were related to painful body parts, or phantom limbs. For instance, one participant said:
I feel it all the time [the phantom leg]. Like now, I can feel it. I can feel my foot, it’s numb. (…) Then, when I go to bed, I tell you, my foot immediately goes numb. When I take off my prosthesis, my foot goes numb. (P07)
Pressure
Eleven participants described feelings of pressure affecting a body part. Some accounts referred to the perception of pressure coming from the outside, like something that is pressing on or tightening around a body part:
It’s as if someone were pushing on my eyes. (P01);
Here, the line that surrounds my body [on the body drawing], I can describe it as barbed wire. You know, the wire on the edges of prisons? (…) I have this wire that tightens around my body, and my body feels like it’s going to explode. (P13).
Other accounts related to the perception of pressure coming from inside the body:Especially in the morning, sometimes I say to [my husband], ‘It feels like my knees are going to burst.’ (P12).
Shape
This sub-theme pertained to peculiarities or oddities in the perceived shape, appearance, position, or anatomical structures of the body, or body parts. For example, one participant mentioned that during a migraine episode, her head felt elongated and bald. She said:
I felt like I was a Conehead. Seriously. And you know what, it wasn’t hair, it was scalp, it was scalp without hair. (P01).
This perception was illustrated by Participant 01 in her body drawing (see Figure 1A). Another participant explained that she felt as if there were an extra layer of skin under her arm, like a bat wing:I don’t know, (pause) as if the arm had a. An extension. (…) You know, bats, when they fly, they have [wings]. It’s a little bit like I have that, you know. (P04)
This sub-theme was evoked by 11 participants.
Temperature
Ten participants recounted instances in which they perceived their painful body parts as colder or hotter than they were. Participants emphasized that they sometimes asked others to acknowledge differences in temperature across different parts of their bodies. They said this helped them realize that their perception of temperature was different from the actual temperature. For example, one participant said:
Um… the cold. It’s like swelling. Sometimes it’s really there. Sometimes I can feel it. You know. Same thing, when I consulted lots of people, I felt that one hand was colder than the other. [People said] ‘Your hands are the same temperature.’ Come on, it’s cold!. (P03)
Another participant described a sunburn-like sensation that really felt like his skin was warmer, even though it was not:
Sometimes there’s a burning sensation, not so bad that you think you have blisters, but you know, there’s a feeling of heat, like, um. Like a sunburn. (…) Nothing. (laughs) There’s no heat. I even asked my girlfriend, it’s like ‘Touch!’ (P05).
Frailty
This sub-theme related to perceptions of instability, frailty, and weakness of the body or painful body parts. It was identified in the verbatim transcripts of five participants. For example, one participant emphasized the feeling of instability in his spine and legs:
My legs, definitely my legs and my back, I don’t feel stable. Like I said, I feel a bit like I have a—you know when you stand on a ball, how it feels? That’s kind of what my spine feels like. That’s what I feel. (P10)
Another participant mentioned how her fingers felt fragile, almost brittle:
Fragile. As if my fingers were fragile, as if they were going to break. Yes, sometimes that’s how I feel, as if they were going to snap, my fingers. (P09).
Theme 2 - Altered Proprioceptive and Postural Awareness
All 15 interviews raised content related to altered proprioceptive and postural awareness. This theme was operationalized around three sub-themes, namely: perceiving the body’s movements, perceiving the body’s posture, and perceiving the body’s outline.
Perceiving the Body’s Movements
Thirteen participants mentioned having some issues with perceiving how their body moves. These issues sometimes manifested as clumsiness, especially when one is not entirely focused on the task at hand:
In everyday activities where I’m a little more distracted, where I’m thinking about other things and all sorts of things, I bump into things, I trip, I knock things over. I try to pick them up once, I knock them over. I try to pick them up a second time, I knock them over again. (P02).
Some participants mentioned that they could not rely on proprioceptive information when moving and needed visual information to navigate stairs, for example:
I have proprioception issues. For me, going down stairs is crazy. I hold onto the railing, and I have to look at the steps. (…) It’s like, I don’t know. The distance to the [next] step, even though I just did it, my brain can’t process the distance. I need to see it. (P01).
Perceiving the Body’s Posture
Eleven participants mentioned having issues to accurately perceive their posture. For example, some participants said that they sometimes felt as if they were standing or sitting straight. However, when they saw their reflection, they realized that their posture was not straight:
I feel straight, then I see my reflection in the television, then I lean forward. Then I straighten up, I straighten up, but I’m crooked. I’m crooked, but I don’t feel it when I’m sitting down, but I can see it, I can see that I’m crooked. (P15).
Other participants noticed difficulty perceiving their posture or the precise location of their limbs during the visualization exercise (ie, with eyes closed). For instance, one participant with CRPS said:
Well, I perceived [my hand] further away. Like a little further away. Let’s say, maybe, 15 to 20 centimeters further away from my body. (P08).
Perceiving the Body’s Outline
Ten participants reported issues perceiving the outline of their bodies in space. For some participants, the painful body parts were more blurred than the rest of the body:
If I don’t touch [my face] and I don’t look at it, it’s hard to know where it ends. Do you have a wide face or a narrow one? If I don’t touch it, I can’t tell you where it ends, let’s say. (P15).
In contrast, other participants said that pain helped delineate the body:
It is pain that delimits my body. (…) I think [the perception] is clearer in the places where I have acute pain, let’s say. (P11).
One participant with widespread pain perceived the outline of some body parts clearly, while the outline of others was more blurred:I see my ankle as very clear, the contours. The toes are more blurred. (P14).
Theme 3 - Shifted Focus Toward or Away from the Pain
This theme was operationalized around the idea of paying different amounts of attention to different parts of the body. It manifested as either focusing on painful body parts (ie, hypervigilance) or shifting attention away from them (ie, disconnection). This theme was identified in 14 of the 15 interviews.
Hypervigilance
Thirteen participants mentioned instances in which they focused all their attention on their painful body parts or had a heightened awareness of them. This seemed to be particularly the case when pain intensity was greater and sometimes resulted in avoidance behaviors and a heightened awareness of one’s surroundings:
I just make sure to position myself carefully when there are people around me, as a reflex, so that no one invades my personal space. I’m very conscious of that. (P11).
One participant described her painful body parts as very salient, comparing them to bustling metro stations. In contrast, she said she did not pay much attention to her pain-free body parts, comparing them to the dark tunnels between stations:
If we make a connection with, let’s say, the Montreal metro, it’s as if the pain were stations, lots of things are happening, and the limbs that don’t hurt… that’s… that’s the black tunnel. (P01).
Disconnection
This sub-theme emerged from six interviews. Disconnection, as opposed to hypervigilance, was described by participants as an intentional strategy aimed at diverting attention away from painful body parts. Participants explained that this strategy made the pain more bearable. For example, Participant 10 said:
For a while, I ignored it [my hand]. I ignored it, but I had no choice. For a while, the pain was so intense, and everything else, that I pushed it away from my body and isolated it a little in my mind. I learned to do that with my hernias, because it’s kind of like that, I isolated the lower part of my body [laughs]. It’s as if I separate it from the rest, then I look at what’s going well, and I try to stay with what’s going well. Then I put what hurts in a corner and endure it.
One participant explained that for her, shifting the focus away from the pain also meant that she was ignoring her body:
If I focus on my body, I’ll feel the pain. You understand? Blocking out the pain is also part of it. Blocking out the pain means ignoring it. Ignoring the pain means ignoring the body. For me, that’s what it is. (P04)
In all but one case, participants with content related to the disconnection sub-theme also had content related to the hypervigilance sub-theme.
Theme 4 - Perturbed Emotions and Beliefs About the Body
This theme encompassed elements related to the emotional, spiritual, and cognitive aspects of body perception disturbances. It comprised four sub-themes: attitudes and beliefs, negative emotions toward the body, trust toward the body, and self-concept. This theme emerged from 14 interviews.
Attitudes and Beliefs
This sub-theme was identified in 12 interviews. It pertained to participants’ attitudes and beliefs about how their pain affects their body perception, thereby shedding light on the cognitive and spiritual aspects of their body perception. For example, one participant explained that living with pain made him feel like his body was worn out:
My body is sore, you know, my body is worn out. (P06).
Some participants attributed cause and effects to try and make sense of their condition. For instance, one participant said that she felt like her pain was a consequence of having witnessed abuse:My eyes. Um… my eyes, it’s like… emotionally, they’ve seen the worst. (pause) And… the defense mechanism is not to see abuse for years. Well, now, I feel like my eyes hurt because they’ve seen too much. I know it’s esoteric, but that’s how I feel. (P01).
Negative Emotions Toward the Body
For 11 participants, living with chronic pain has led them to develop negative, sometimes hostile feelings toward their body. For some participants, these feelings manifested as a desire to remove a body part or a sense of being imprisoned in their own body. One participant said:
I’m imprisoned by my pain in my body, by what’s inside it, and every time, I just want to rip off what is hurting me, rip off my belt, actually, and it’s like, I scream, ‘I want to rip everything off,’ because I feel like my intestines are being torn apart. (P13).
For others, these feelings manifested as hatred or disgust toward their own body:
That’s right, when I feel crushed, and fat, I feel disgusted. Yeah. (P15).
Trust Toward the Body
Eleven participants reported experiencing trust issues with their bodies. Some participants reported feeling betrayed by their bodies:
Well, frankly, um… I feel betrayed by my body every day. That’s, um… That’s a difficult realization, honestly. (P02).
Others verbalized feeling that they could not rely on their bodies, leading to frustration:That’s right, yes, it’s unreliable. It’s, um. It’s really, maybe it’s a lack of vocabulary to say it’s ‘crap’, but. It’s deficient, it’s non-functional. (P01).
Finally, some participants verbalized insecurity about their bodies:
Actually, it might sound strange when I say it, but it’s like a form of insecurity, because I never know what’s going well, what’s going not too bad. I’m just insecure about my body. Yes. (P14).
Self-Concept
For five participants, living with chronic pain has unpleasantly altered their self-concept. The operating definition of self-concept was that it reflects the concept one has of oneself as a physical, social, and spiritual or moral being.32 For some participants, this manifested as the feeling that they had changed as a person:
I don’t dare look at myself too much, it seems, because I’m not the same person anymore. (P09).
Others mentioned feeling diminished, “less than”. For instance, when asked about how he perceived his body, Participant 10 responded:I feel diminished. I feel diminished as a person, as a man.
Another participant mentioned that he felt disabled:You know, my body, for me, it makes me feel very disabled. That’s really how it feels. (P05).
For Participant 13, when she experiences intense pain due to endometriosis, her self-concept is disrupted in an in-the-moment kind of way, causing her to lose touch with time and space, and feeling as though she is no longer herself:When that happens to me, as I told you, I lose all sense of time and space, and it’s just me and my pain – we’re together. I’m not – I don’t even realize what I’m saying or doing. I’m not myself.
Theme 5 - Neglect-Like Symptoms
This theme was operationalized based on the definition used by Galer and Jensen to describe symptoms exhibited by individuals with CRPS that resembled the neglect-like behaviors observed in patients with neurological disorders.31 We also used Galer and Jensen’s categorization to group relevant verbatim content into the appropriate sub-themes (ie, motor neglect-like symptoms; cognitive neglect-like symptoms). Two-thirds of participants from the present study reported neglect-like symptoms.
Motor Neglect-Like Symptoms
Eight participants reported experiencing motor neglect-like symptoms. These symptoms included reports of motor delay at movement initiation, consistent with Galer and Jensen’s definition.31 For Participant 03, these delays sometimes occurred when trying to initiate movements with her CRPS-affected hand, which made her feel distraught at times:
I’m trying to get [my hand] to move, but it seems to take a while before it. You know, I’m like, ‘Come on, move, move, move.’ And then, at some point, oh, okay, that’s fine, it’s moving, it’s there.
Other participants struggled with the motor imagery exercise, failing to visualize certain movements that they were unable to perform in real life. For example, when asked to visualize herself crouching down, Participant 14, who has hip pain because of Ehlers-Danlos syndrome, said:
For me, that movement is impossible. I can’t even visualize it. I can bend over, for example, I can imagine that. Crouching down, listen, it’s been maybe 20 years since I last crouched down. So I can’t see it.
Cognitive Neglect-Like Symptoms
Eight participants reported experiencing a sense of foreignness, disownership, or detachment from a painful body part. One participant talked about a recent flare-up of her fibromyalgia symptoms. She said:
It was as if my hands were detached from my body. (…) At that moment, I almost said to myself, ‘Those aren’t my hands. Take that thing away from me, because it’s not mine.’ I don’t know. (P11)
Another participant, talking about her CRPS-affected hand:
Often, I feel as if my hand were dead. (P03).
These accounts are consistent with Galer and Jensen’s definition of cognitive neglect-like symptoms.Theme 6 - Disturbed Sense of Agency
The operating definition for this theme was that the sense of agency reflects one’s feeling of being in control of one’s own actions.33,34 Therefore, when the sense of agency is disrupted, one might feel like they do not have control over their movements (first sub-theme), and one’s body may sometimes move involuntarily (second sub-theme). Eight participants reported having experienced a disrupted sense of agency at times.
Feeling of Control Over One’s Own Movements
Seven participants reported experiencing moments when they did not feel fully in control of their movements. For example, one participant with CRPS said her affected arm “doesn’t listen to [her]” (P08). Another participant, also with CRPS, said:
It seems like. Someone else is controlling the joystick. You know, it’s not me who’s in control. It’s as if there’s a little man in my head right now who… with a little joystick is remotely controlling my hand. (P03)
Other examples include Participant 01, who has struggled with fibromyalgia for 27 years, who said:
For me it’s… I don’t feel like I have much control over my body.
Involuntary Movements
Two participants with CRPS reported involuntary movements of their affected arm. Participant 08:
As soon as I stop thinking about my arm, it moves into this position [close to the heart], because it doesn’t feel comfortable when stretched out. (…) There are several moments when I am completely unaware. It goes in this position all by itself.
This perception was illustrated by Participant 08 in her body drawing (see Figure 1B).
Discussion
This study used an inductive/deductive hybrid thematic analysis approach to qualitatively explore body perception disturbances in individuals living with chronic non-cancer pain. Fifteen interviews were conducted with adults with diverse profiles in terms of age, gender, work status, and pain conditions. Data analysis revealed that all 15 participants reported some elements of body perception disturbances. Six main themes were identified: distortions of perceived body characteristics (theme 1); altered proprioceptive and postural awareness (theme 2); a shifted focus toward or away from the pain (theme 3); perturbed emotions and beliefs about the body (theme 4); neglect-like symptoms (theme 5); and a disturbed sense of agency (theme 6). These themes are consistent with the “key facets” of body perception disturbances previously identified.26
Body Perception Disturbances in Chronic Non-Cancer Pain
All 15 participants reported some elements of body perception disturbances in at least three themes, with nearly half of them (n = 7) reporting disturbances in all six themes. This suggests that body perception disturbances could be quite common among individuals with chronic non-cancer pain. Although it was beyond the scope of the present work to identify specific patterns or co-occurrences of themes and sub-themes, some observations can be made in this regard. For instance, it is interesting to note that most themes and sub-themes seem to be shared by most participants (eg, all participants reported distortions of perceived body characteristics, the most frequently reported sub-theme being a perception of tension in the body). As such, it can be hypothesized that these themes and sub-themes represent frequent manifestations of body perception disturbances across different pain conditions. On the other hand, some hypotheses can be made regarding the less commonly reported themes and sub-themes across our sample. For example, the sub-theme “involuntary movements” (theme 6), reported by two participants, was only described in relation to a limb affected by CRPS. This observation is consistent with the findings of a large observational study that investigated predictors of self-reported neglect-like symptoms and involuntary movements among individuals with various chronic pain conditions. This study found that respondents with CRPS were 4.55 times more likely to report involuntary movements than respondents with other types of limb pain.35 Similarly, the sub-theme “weight” (theme 1), reported by 13 participants, was consistently described as a sensation of heaviness in the painful limb, except for one participant (P07) who mentioned that he sometimes felt that his phantom leg was lighter than his other leg, depending on the pain. Similar accounts were reported in a study investigating body image and perception in lower limb amputees; participants without phantom limb pain tended to perceive the phantom leg as lighter, whereas participants with phantom limb pain tended to perceive the phantom leg as heavier.36
Furthermore, although investigating the relationships between body perception disturbances and other clinical variables (eg, pain intensity or duration) was not the aim of the present study, some observations can be made. First, our findings do not point toward obvious relationships between body perception disturbances and pain duration (ie, manifestations of body perception disturbances do not differ between participants with shorter or longer pain durations). These findings are consistent with those of a recent systematic review and meta-analysis on the Fremantle Back Awareness Questionnaire – a self-reported questionnaire assessing body perception disturbances in individuals with CLBP – and its region-specific adaptations. This study found no association between pain duration and the scores obtained for these questionnaires in individuals with CLBP, chronic neck pain, chronic shoulder pain, and knee osteoarthritis.37 Similarly, Ten Brink and collaborators found that disease duration was not associated with the score obtained using the revised Bath Body Perception Disturbance Scale in individuals with CRPS.38 Regarding the relationship between pain intensity and body perception disturbances, Budzisz and collaborators found a positive association between pain intensity and the different Fremantle Awareness Questionnaires scores,37 and Ten Brink and collaborators found that pain intensity was a predictor for body perception disturbances in individuals with CRPS.38 Although this tendency was not apparent in our sample (ie, participants with more severe pain did not report more disturbances than participants with less severe pain), participants did report having more disturbances during episodes of greater pain intensity. This suggests that body perception disturbances may not be a stable, unchanging phenomenon, but could fluctuate in response to different variables, such as pain flare-ups. In a recent qualitative study investigating the impact of the worst pain episodes on the minimal self (ie, pre-reflective self-awareness which reflects one’s in-the-moment experience),39 participants reported a disruption to their sense of agency, body ownership and awareness, as well as a distorted perception of time during these episodes.40 These findings echo the accounts of some of our participants who described their experiences of body perception disturbances. Future work could focus on identifying disturbances that are experienced stably, as opposed to transitory disturbances that occur in specific instances (eg, pain flare-ups).
Taken together, these observations suggest that body perception disturbances are a common phenomenon in chronic non-cancer pain that is not limited to individuals with more severe pain or longer pain duration. Furthermore, some manifestations of body perception disturbances may be transversally experienced in chronic non-cancer pain (ie, across different pain conditions), while others may be associated with specific pain conditions. Finally, some disturbances could fluctuate with pain flare-ups.
Research and Clinical Implications
Underlying Mechanisms
Future research should investigate the underlying mechanisms of the different manifestations of body perception disturbances. Previous work suggests that neuroplastic changes and perturbed sensorimotor integration could be at play; notably, distortions of perceived body characteristics like the shape or size of a painful limb/body part, and neglect-like symptoms could be closely related to neuroplastic changes in the central nervous system in chronic pain states like CRPS, phantom limb pain, and CLBP (see1 and41 for narrative reviews). Such neuroplastic changes could also account for disturbances related to proprioceptive and postural awareness in individuals with chronic pain. For instance, a recent study found that proprioceptive impairment was widespread – rather than localized – in participants with chronic neck pain and CLBP, lending further credibility to the involvement of central nervous system neuroplasticity.42 Disruptions of the sense of agency could be attributed to perturbed sensorimotor integration documented in chronic pain states like CRPS43–45 and fibromyalgia,44 as the sense of agency is thought to rely heavily on internal sensorimotor cues.46 In contrast, a shifted focus toward or away from the pain and perturbed emotions and beliefs about the body most likely rely on cognitive and affective adaptations to chronic pain. Several studies have investigated the role of hypervigilance in pain-related avoidance behaviors and its contribution to poorer clinical outcomes.47–49 Recent work suggests that the lived experience of chronic pain influences the affective and cognitive dimensions of body perception.50 Indeed, chronic pain has been reported to perturb individuals’ relationship to their body and self-concept in CLBP, persistent musculoskeletal pain, and endometriosis.16,51–53 Other authors in the field of pain-related behavior have proposed the concept of bodily doubt to conceptualize how the experience of chronic pain fragilizes one’s faith toward their body.54 As such, it could be hypothesized that psychological factors such as depression, fear of movement and catastrophizing – which are commonly reported in chronic pain –55 could contribute to explain body perception disturbances, as these variables have been associated with worse body perception in various musculoskeletal pain conditions (see56 for a scoping review).
Therefore, future research should investigate the relationships between body perception disturbances and their underlying causes at the sensorimotor, cognitive, and affective levels.
Reflecting on the Importance of Addressing Body Perception Disturbances
Our findings suggest that body perception disturbances are common among individuals with chronic non-cancer pain. This means that many patients receiving chronic pain care may experience these disturbances. As such, assessing body perception disturbances in this population should be incorporated into the biopsychosocial approach to chronic pain.57 Furthermore, body perception disturbances are known to be associated with pain, and normalization of such disturbances is thought to parallel pain reduction.14,58 Consequently, documenting body perception disturbances could provide valuable clinical insight into patients’ recovery. Moreover, in a recent study of early CRPS patients, the majority displayed moderate-to-high levels of body perception disturbances, and the results suggest that greater levels of disturbance are associated with poorer outcomes.59 Body perception disturbances could thus be considered a negative prognostic factor that should be considered in the management of chronic pain patients. This lends weight to the view that body perception disturbances are a valuable clinical outcome that warrants specific assessment and treatment. For example, some interventions like mirror visual feedback and body ownership paradigms have been shown to decrease body perception disturbances in individuals with CRPS.60,61
Study Limitations
This study has some limitations that should be considered when interpreting the results. Firstly, as previously mentioned, the interviews were led by a junior researcher who is new to qualitative research (MD), which could have impacted the depth of the interviews. However, this lack of experience was compensated for by the support of an expert in qualitative research, as well as by thorough preparation (eg, practice interviews). Another aspect to consider regarding the transferability of the study findings is the small sample size. Indeed, the intrinsic heterogeneity of the chronic pain population makes purposive sampling quite challenging. Nevertheless, efforts in participants recruitment were made to ensure sample diversity (age, gender, pain condition(s), pain severity, work status). Moreover, our findings revealed many similarities – and few differences – in body perception disturbances across participants, which suggests that this phenomenon could be transversally associated with chronic pain. However, it is worth pointing out that our sample of 15 individuals consisted of eleven women and four men. While this imbalance is not surprising considering the greater prevalence of chronic pain conditions among women,62 it may limit the generalizability of the results presented here. Finally, we cannot exclude the possibility of a selection bias; in fact, it is possible that individuals with more severe manifestations of body perception disturbances, or individuals who are keen to express themselves, had more interest in participating in this kind of study than less severely impaired or more reserved individuals. This should be taken into consideration when interpreting the results.
Conclusion
The present findings emphasize the common occurrence of body perception disturbances in individuals living with chronic non-cancer pain. They also highlight the importance of addressing this phenomenon, which should be part of the biopsychosocial treatment approach of chronic pain. The present study identified six main themes related to body perception disturbances in chronic non-cancer pain, which could serve as a starting point for a new conceptual framework for understanding body perception disturbances in heterogeneous pain populations. Future research should aim to investigate underlying mechanisms and to describe this phenomenon in large cohorts of heterogeneous chronic pain conditions to further build on current knowledge.
Data Sharing Statement
The raw data supporting the findings of this article will be made available by the corresponding author upon reasonable request, without undue restriction.
Acknowledgments
The authors thank all research participants, as well as David Bouchard, coordinator of the Methodological platform for qualitative research at the Center for Interdisciplinary Research in Rehabilitation and Social Integration (Cirris), and Catherine Bernier (CB), research intern, for her help with coding the first interviews.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Canada Research Chair in Sensori Motor Rehabilitation and Pain (CRC-2022-00093) awarded to CM. MD is supported by a scholarship from the Fonds de Recherche du Québec (FRQ; https://doi.org/10.69777/315881).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lotze M, Moseley GL. Role of distorted body image in pain. Curr Rheumatol Rep. 2007;9(6):488–18. doi:10.1007/s11926-007-0079-x
2. de Vignemont F. Body schema and body image-Pros and cons. Neuropsychologia. 2010;48(3):669–680. doi:10.1016/j.neuropsychologia.2009.09.022
3. Gallagher S. Body image and body schema: a conceptual clarification. J Mind and Behav. 1986;December.
4. de Vignemont F, Pitron V, Alsmith A. What is the body schema? Body Schema Body Image. 2021.
5. Gallagher S. How the Body Shapes the Mind. Oxford Academic; 2005.
6. Pitron V, Alsmith A, de Vignemont F. How do the body schema and the body image interact? Consciousness Cogn. 2018;65(August):352–358. doi:10.1016/j.concog.2018.08.007
7. Valenzuela-Moguillansky C. Chronic pain and disturbances in body awareness. Revista Chilena de Neuropsicologia. 2012;7(1):26–37.
8. Martinez E, Aira Z, Buesa I, Aizpurua I, Rada D, Azkue JJ. Embodied pain in fibromyalgia: disturbed somatorepresentations and increased plasticity of the body schema. PLoS One. 2018;13(4):e0194534. doi:10.1371/journal.pone.0194534
9. Acapo S, Dupeyron A, Nizard J. Disturbances in the representation and perception of the body in complex regional pain syndrome. Article. Douleurs. 2024;25(2):60–66. doi:10.1016/j.douler.2024.02.003
10. Wand BM, Catley MJ, Rabey MI, O’Sullivan PB, O’Connell NE, Smith AJ. Disrupted self-perception in people with chronic low back pain. Further evaluation of the fremantle back awareness questionnaire. J Pain. 2016;17(9):1001–1012. doi:10.1016/j.jpain.2016.06.003
11. Di Pietro F, McAuley JH, Parkitny L, et al. Primary somatosensory cortex function in complex regional pain syndrome: a systematic review and meta-analysis. J Pain. 2013;14(10):1001–1018. doi:10.1016/j.jpain.2013.04.001
12. Vittersø AD, Halicka M, Buckingham G, Proulx MJ, Bultitude JH. The sensorimotor theory of pathological pain revisited. Neurosci Biobehav Rev. 2022;139(May). doi:10.1016/j.neubiorev.2022.104735
13. Harris AJ. Cortical origin of pathological pain. Lancet. 1999;354(9188):1464–1466. doi:10.1016/S0140-6736(99)05003-5
14. Flor H. Cortical reorganisation and chronic pain: implications for rehabilitation. J Rehabili Med. 2003;35(Suppl. 41):66–72. doi:10.1080/16501960310010179
15. Wand BM, James M, Abbaszadeh S, et al. Assessing self-perception in patients with chronic low back pain: development of a back-specific body-perception questionnaire. J Back Musculoskelet Rehabil. 2014;27(4):463–473. doi:10.3233/BMR-140467
16. Osborn M, Smith JA. Living with a body separate from the self. The experience of the body in chronic benign low back pain: an interpretative phenomenological analysis. Scand J Caring Sci. 2006;20(2):216–222. doi:10.1111/j.1471-6712.2006.00399.x
17. Lewis JS, Schweinhardt P. Perceptions of the painful body: the relationship between body perception disturbance, pain and tactile discrimination in complex regional pain syndrome. Physical & Somatoform & Psychogenic Disorders 3290. Eur. J. Pain. 2012;16(9):1320–1330. doi:10.1002/j.1532-2149.2012.00120.x
18. Lewis J, McCabe C. Body Perception Disturbance (BPD) in CRPS. Practical Pain Manag. 2010;60–66.
19. Augière T, Metral M, Simoneau M, Mercier C. Preserved tactile distance estimation despite body representation distortions in individuals with fibromyalgia. Front Pain Res. 2024;1–12. doi:10.3389/fpain.2024.1414927
20. Förderreuther S, Sailer U, Straube A. Impaired self-perception of the hand in complex regional pain syndrome (CRPS). Pain. 2004;110(3):756–761. doi:10.1016/j.pain.2004.05.019
21. Halicka M, Vittersø AD, Proulx MJ, Bultitude JH. Neuropsychological changes in complex regional pain syndrome (CRPS). Review. Behav Neurol. 2020;2020:1–30. doi:10.1155/2020/4561831
22. Schwoebel J, Friedman R, Duda N, Coslett HB. Pain and the body schema. Brain. 2001;124:2098–2104. doi:10.1093/brain/124.10.2098
23. Martinez E, Guillen V, Buesa I, Azkue JJ. A distorted body schema and susceptibility to experiencing anomalous somatosensory sensations in fibromyalgia syndrome. Clin J Pain. 2019;35(11):887–893. doi:10.1097/AJP.0000000000000754
24. Halicka M, Cousins OR, Brink AFT, Vittersø AD, Proulx MJ, Bultitude JH. Reduced visuospatial attention in personal space is not limited to the affected limb in complex regional pain syndrome. Article. J Pain Res. 2024;17:1519–1529. doi:10.2147/JPR.S437366
25. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
26. Dagenais M, Proulx C, Augière T, Roy JS, Mercier C. Self-reported questionnaires assessing body perception disturbances in adults with chronic non-cancer pain: a scoping review. Front Pain Res. 2025;6. doi:10.3389/fpain.2025.1497328
27. Bennett MI, Kaasa S, Barke A, et al. The IASP classification of chronic pain for ICD-11: chronic cancer-related pain. Pain. 2019;160(1):38–44. doi:10.1097/j.pain.0000000000001363
28. Gokce Ceylan G, Gok Metin Z. Symptom status, body perception, and risk of anxiety and depression in breast cancer patients receiving paclitaxel: a prospective longitudinal study. Article. Support Care Cancer. 2022;30(3):2069–2079. doi:10.1007/s00520-021-06619-6
29. Brederecke J, Heise A, Zimmermann T. Body image in patients with different types of cancer. PLoS One. 2021;16(11):e0260602. doi:10.1371/journal.pone.0260602
30. Proudfoot K. Inductive/deductive hybrid thematic analysis in mixed methods research. J Mixed Methods Res. 2023;17(3):308–326. doi:10.1177/15586898221126816
31. Galer BS, Jensen M. Neglect-like symptoms in complex regional pain syndrome: results of a self-administered survey. J Pain Sympt Manage. 1999;18(3):213–217. doi:10.1016/S0885-3924(99)00076-7
32. Gecas V. The Self-Concept. Annu Rev Sociol. 1982;8:1–33. doi:10.1146/annurev.so.08.080182.000245
33. Haggard P. Sense of agency in the human brain. Nat Rev Neurosci. 2017;18:197–208. doi:10.1038/nrn.2017.14
34. Moore JW. What is the sense of agency and why does it matter? Frontiers in Psychology. 2016;7(AUG):1–9. doi:10.3389/fpsyg.2016.01272
35. Ten Brink AF, Bultitude JH. Predictors of self-reported neglect-like symptoms and involuntary movements in complex regional pain syndrome compared to other chronic limb pain conditions. Article. Pain Med. 2021;22(10):2337–2349. doi:10.1093/pm/pnab226
36. Beisheim-Ryan EH, Hicks GE, Pohlig RT, Medina J, Sions JM. Body image and perception among adults with and without phantom limb pain. Article in Press. PM R. 2021. doi:10.1002/pmrj.12750
37. Budzisz A, Jung A, Adamczyk WM, et al. Body image measured via the fremantle awareness questionnaire in individuals with and without pain: a systematic review and meta-analysis. J Pain. 2024;25(8):104530. doi:10.1016/j.jpain.2024.104530
38. Ten Brink AF, Halicka M, Vittersø AD, Jones HG, Stanton TR, Bultitude JH. Validation of the bath CRPS body perception disturbance scale. J Pain. 2021;22(11):1371–1384. doi:10.1016/j.jpain.2021.04.007
39. Colombetti G. Varieties of pre-reflective self-awareness: foreground and background bodily feelings in emotion experience. Inquiry. 2011;54(3):293–313. doi:10.1080/0020174X.2011.575003
40. Stilwell P, Gagnon-Mailhot M, Hudon A, et al. When pain overwhelms the self: a phenomenological study of a new mode of suffering, based on adults’ recollections of their worst pain episodes. J Pain. 2025;32:105413. doi:10.1016/j.jpain.2025.105413
41. Kuttikat A, Noreika V, Shenker N, Chennu S, Bekinschtein T, Brown CA. Neurocognitive and neuroplastic mechanisms of novel signs in CRPS. Front Human Neurosci. 2016;10(16):1–13. doi:10.3389/fnhum.2016.00016
42. Poesl M, Carvalho GF, Adamczyk WM, et al. Widespread proprioceptive acuity impairment in chronic back pain: a cross-sectional study. Arch Phys Med Rehabil. 2023;104:1439–1446. doi:10.1016/j.apmr.2023.02.016
43. McCabe CS, Blake DR. Evidence for a mismatch between the brain’s movement control system and sensory system as an explanation for some pain-related disorders. Current Pain Headache Rep. 2007;11(2):104–108. doi:10.1007/s11916-007-0006-x
44. McCabe CS, Cohen H, Hall J, Lewis J, Rodham K, Harris N. Somatosensory conflicts in complex regional pain syndrome type 1 and fibromyalgia syndrome. Curr Rheumatol Rep. 2009;11(6):461–465. doi:10.1007/s11926-009-0067-4
45. Bultitude JH, Petrini K. Altered visuomotor integration in complex regional pain syndrome. Behav Brain Res. 2021;397:1–12. doi:10.1016/j.bbr.2020.112922
46. Moore JW, Fletcher PC. Sense of agency in health and disease: a review of cue integration approaches. Consciousness Cognition. 2012;21:59–68. doi:10.1016/j.concog.2011.08.010
47. Herbert MS, Goodin BR, STt P, et al. Pain hypervigilance is associated with greater clinical pain severity and enhanced experimental pain sensitivity among adults with symptomatic knee osteoarthritis. Ann Behav Med. 2014;48(1):50–60. doi:10.1007/s12160-013-9563-x
48. Zhang W, Löffler M, Usai K, Mišić M, Nees F, Flor H. Hypervigilance to pain may predict the transition from subacute to chronic back pain: a longitudinal observational study. J Pain Res. 2025;2025(18):3141–3158. doi:10.2147/JPR.S512911
49. Shigetoh H. Hypervigilance to pain affects activities of daily living: an examination using the Japanese version of the pain vigilance awareness questionnaire. J Phys Ther Sci. 2017;29(12):2094–2096. doi:10.1589/jpts.29.2094
50. Sündermann O, Flink I, Linton SJ. My body is not working right: a cognitive behavioral model of body image and chronic pain. Pain. 2020;161(6):1136–1139. doi:10.1097/j.pain.0000000000001822
51. Crowe M, Whitehead L, Gagan MJ, Baxter GD, Pankhurst A, Valledor V. Listening to the body and talking to myself - the impact of chronic lower back pain: a qualitative study. Int J Nurs Studies. 2010;47(5):586–592. doi:10.1016/j.ijnurstu.2009.09.012
52. Sündermann O, Rydberg K, Linder L, Linton SJ. “when i feel the worst pain, i look like shit” - Body image concerns in persistent pain. Article. Scand J Pain. 2018;18(3):379–388. doi:10.1515/sjpain-2017-0163
53. Sayer-Jones K, Sherman KA. “My body…tends to betray me sometimes”: a qualitative analysis of affective and perceptual body image in individuals living with endometriosis. article in press. Int J Behav Med. 2022. doi:10.1007/s12529-022-10118-1
54. Fernandez AV, Hartvigsen J, Ravn SL, Stilwell P, Kongsted A. Reconceptualizing pain-related behaviour: introducing the concept of bodily doubt. Eur. J. Pain. 2023;27(6):666–667. doi:10.1002/ejp.2105
55. Rogers AH, Farris SG. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur. J. Pain. 2022;26(8):1611–1635. doi:10.1002/ejp.1994
56. Oliveira I, Garrido MV, Bernardes SF. On the body-mind nexus in chronic musculoskeletal pain: a scoping review. Eur. J. Pain. 2022;26(6):1186–1202. doi:10.1002/ejp.1944
57. Gatchel RJ, Haggard R, Thomas C, Howard KJ. Biopsychosocial approaches to understanding chronic pain and disability. In: Moore RJ, editor. Handbook of Pain and Palliative Care. Springer Nature; 2018.
58. Lewis JS, Kellett S, McCullough R, et al. Body perception disturbance and pain reduction in longstanding complex regional pain syndrome following a multidisciplinary rehabilitation program. Pain Med. 2019;20(11):2213–2219. doi:10.1093/pm/pnz176
59. Louis M-H, Legrain V, Aron V, et al. Early CRPS is a heterogeneous condition: results from a Latent Class Analysis. Eur. J. Pain. 2025;29(2):1–24. doi:10.1002/ejp.4785
60. Lewis JS, McCabe CS, Taylor G, Smith M. Visual illusions modulate body perception disturbance and pain in complex regional pain syndrome: a randomized trial. Eur. J. Pain. 2021;1–13. doi:10.1002/ejp.1766
61. Hwang H, Cho S, Lee J-H. The effect of virtual body swapping with mental rehearsal on pain intensity and body perception disturbance in complex regional pain syndrome. Int J Rehabi Res. 2014;37(2):167–172. doi:10.1097/MRR.0000000000000053
62. Meana M, Cho R, DesMeules M. Chronic pain: the extra burden on Canadian women. BMC Women’s Health. 2004;4(Suppl 1):1–11. doi:10.1186/1472-6874-4-S1-S17
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.