Back to Journals » Patient Preference and Adherence » Volume 17
I-PreFer Study: A Questionnaire to Explore Patient, Caregiver and Pulmonologist Preferences of Idiopathic Pulmonary Fibrosis Treatment Options
Authors Hollmen M, Bromilow T ![]() , Smith AB
, Smith AB ![]() , Mealing S
, Mealing S ![]() , Lewis D
, Lewis D ![]() , Galvin L, Jones S, Pacheco L, Soulard S, Froidure A
, Galvin L, Jones S, Pacheco L, Soulard S, Froidure A
Received 23 February 2023
Accepted for publication 19 June 2023
Published 4 August 2023 Volume 2023:17 Pages 1621—1639
DOI https://doi.org/10.2147/PPA.S408857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Maria Hollmen,1 Tom Bromilow,2 Adam B Smith,2 Stuart Mealing,2 Damian Lewis,2 Liam Galvin,3 Steve Jones,3 Luís Pacheco,4 Stéphane Soulard,4 Antoine Froidure5,6
1Faculty of Medicine, University of Helsinki, Helsinki, Finland; 2York Health Economics Consortium (YHEC), York, UK; 3European Pulmonary Fibrosis & Related Disorders Federation, Overijse, Belgium; 4Boehringer Ingelheim, Amsterdam, the Netherlands; 5Service de Pneumologie, Cliniques Universitaires Saint-Luc, Brussels, Belgium; 6Institut de Recherche Expérimentale et Clinique, UCLouvain, Ottignies-Louvain-la-Neuve, Belgium
Correspondence: Maria Hollmen, Faculty of Medicine, University of Helsinki, Helsinki, Finland, Email [email protected]
Introduction: Idiopathic Pulmonary Fibrosis (IPF) is a rare disease that causes shortness of breath, dry cough, and tiredness. While there is no cure for IPF, current therapeutic treatments aim to slow lung degeneration while managing side effects. There is little known about patient experience and attitude with regards to their disease and medication.
Purpose: To understand the perceptions, behaviors and drivers of treatment decision-making among patients, caregivers and pulmonologists in IPF.
Patients and Methods: Online surveys to patients with IPF, caregivers and pulmonologists were developed and administered in Belgium, Finland, France, Greece (pulmonologists only), the Netherlands, Ireland and the United Kingdom between November 2021 and January 2022.
Results: A total of 111 patients, 22 caregivers and 140 pulmonologists participated. Half (47%) of patients rated their disease as “severe”, while pulmonologists reported that a quarter of their patients had a low Forced Vital Capacity (FVC) (below 50% of the predicted value). Between 21% and 42% of the patients do not take an IPF medication (patients’ perception) or antifibrotic (physicians’ perception). Pulmonologists reported that a total of 58% of their patients were receiving antifibrotic medication, any IPF medication, while around 53%, 55%, 35% and 73% of the patients limited their exposure (sometimes or often) to the sun due to IPF, considered taking medication against diarrhea, nausea/vomiting and heartburn, respectively. Treatment adherence was relatively high (81%), in line with the caregivers’ view and the pulmonologists’ expectations. Overall, cultural, clinical or socio-demographic factors impacted patients’ perceptions or behaviors.
Conclusion: This study shows there is a significant proportion of IPF patients who remain untreated, a misalignment of disease severity between patients and their physicians and patient background impacts behavior. Overall, more in-depth patient–physician communication is needed to improve treatment experience.
Keywords: online survey, antifibrotic, adherence, behavior, lung disease, outcomes research
Introduction
Idiopathic pulmonary fibrosis (IPF) is the most common form of interstitial pneumonia. It is a chronic, progressive, and ultimately fatal lung disease associated with scarring of the tissue surrounding the alveoli.1–3 This causes impaired lung function, leading to shortness of breath, dry cough, and tiredness.4 While the specific etiology of IPF remains unknown, it is generally regarded as a consequence of multiple interacting genetic and environmental factors.3 IPF is considered a rare disease, more commonly affecting older age groups and men. However, the incidence of IPF has risen over time.5,6
IPF is typically diagnosed via a combination of pulmonary function tests, chest X-rays, high-resolution computed tomography scans and bronchoscopies, although diagnosis is often difficult due to its similarity to other lung conditions.2,4 Additionally, disease management is complicated by common comorbidities, such as lung cancer, pulmonary emphysema, gastroesophageal reflux, pulmonary hypertension, and obstructive sleep apnea.7
There is currently no cure for IPF. Common non-pharmacological treatment practices include pulmonary rehabilitation (ie breathing techniques) to foster respiratory strength2 and lung transplant in some cases. However, few people with IPF are suitable candidates, and donor lungs are scarce.4 With a median survival of 3–5 years from diagnosis for those not treated,8 the primary treatments for patients aim to slow the disease and maintain quality of life. There are two antifibrotic pharmacotherapies currently available for IPF: pirfenidone and nintedanib. Both treatments aim to slow the process of scarring thereby delaying lung degeneration. These treatments increase the average survival time for IPF patients. For example, a 2022 study estimated the mean survival time for nintedanib patients was around 6 years versus around 3 years for matched placebo patients.9 Similarly, a 2019 study found that pirfenidone significantly improved five-year survival versus no anti-fibrotic treatment (55.9% vs 31.5% alive, p = 0.002).10 While efficacious, both pharmacotherapies are associated with frequent adverse events, such as diarrhea and photosensitivity.11,12 However, Maher et al found that IPF patients wanted more information about the pharmacological treatment options at diagnosis and were more concerned about preventing disease progression than avoiding medication side effects.13 Therefore, stakeholders must consider which treatment is most appropriate while maintaining quality of life.
Aims
This study aims to understand the key drivers of treatment decision-making among patients, caregivers and pulmonologists in IPF and explore how to improve patient–pulmonologist discussions on treatment options. The need for improvement in patient–pulmonologist communication had previously been identified in Maher et al.13 Stakeholder preferences were elicited through a combination of discrete choice experiments (DCEs)14 and questionnaires. The DCE and questionnaires were collectively referred to as the “I-PreFer” (Preferences for Treatment Options in Idiopathic Pulmonary Fibrosis) study. The specific objective of the patient questionnaire was to develop knowledge of the patient experience when dealing with IPF and antifibrotic treatments.
Materials and Methods
Three online surveys were developed, one for each stakeholder, consisting of two parts, a DCE asking preferences on drug attributes,14 and a questionnaire collecting socio-demographic data and data specific to the type of stakeholder.
The study was administered in seven countries: Belgium, Finland, France, Greece (pulmonologists only), the Netherlands, the Republic of Ireland (ROI) and the United Kingdom (UK). The surveys were developed in English and translated using a medical translation firm, validated by native speakers.
The European Pulmonary Fibrosis & Related Disorders Federation (EU-PFF) and three expert clinicians assisted with the design and distribution of the surveys. The organization running the study, York Health Economics Consortium, is wholly owned by the University of York and seeks ethical approval for studies involving human subjects from the University. As such, the I-PreFer study and associated surveys were granted ethical approval by the University of York Health Sciences Research Governance Committee (HSRGC/2021/448/D: I-PreFer, letter dated 14 April 2021) and conformed to all relevant pharmacovigilance rules and reporting standards. A study information page was included at the start of the survey to inform stakeholders of the aims of the research, any potential risks of participation, the anonymous nature of the study and where the data would be stored. This was followed by a question asking for their voluntary consent to participate. If consent was given, the survey continued. Otherwise, the survey ended. Additionally, this study was conducted in accordance with the principles laid out by the 18th World Medical Assembly (Helsinki, 1964) and all subsequent amendments.
Questionnaire Design
A summary of the questions included in each survey is shown in Table 1. The full, final questionnaires for each stakeholder can be found in the Supplementary Material 1.
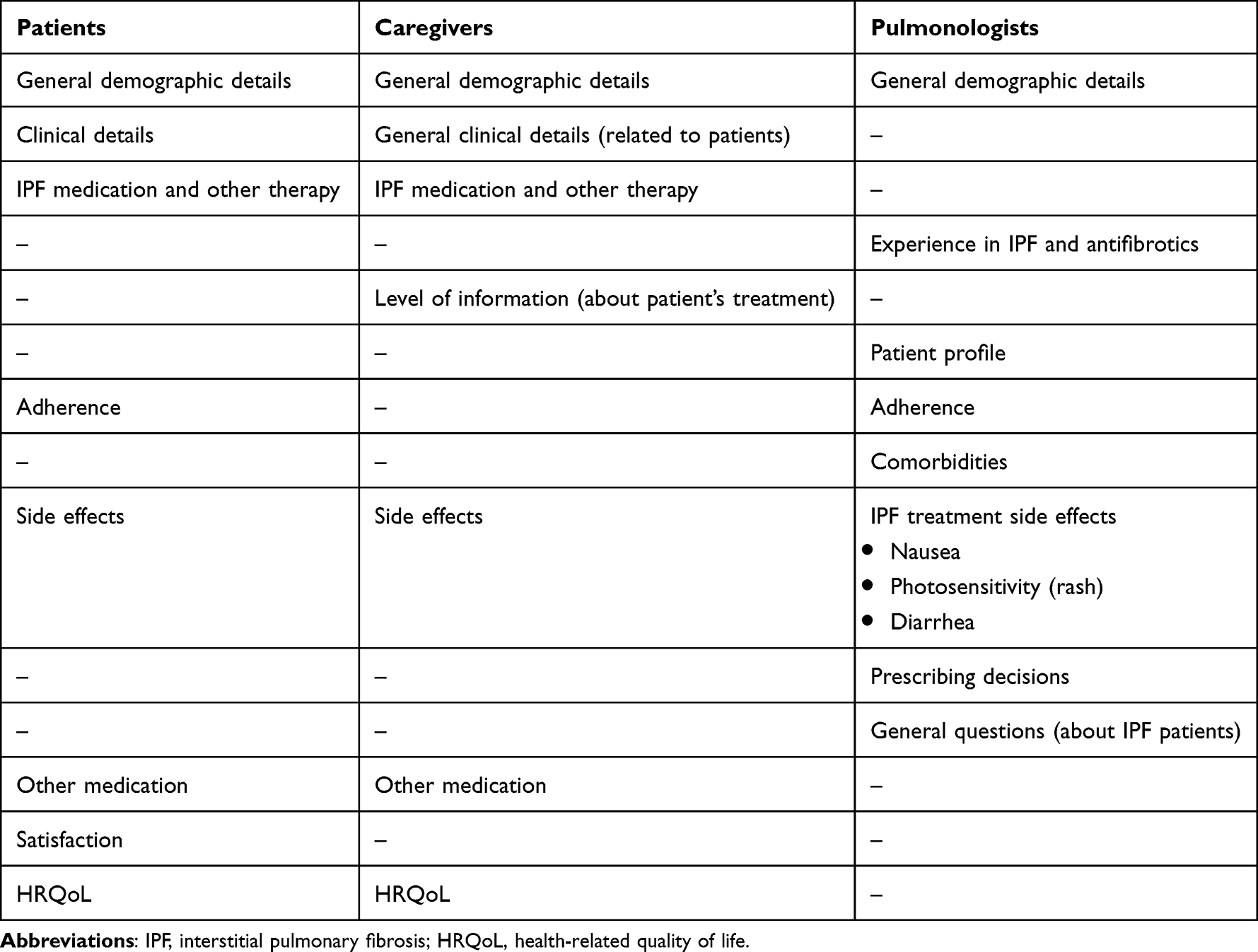 |
Table 1 Summary of Included Questions Categories |
Patient Questionnaire
To develop the questionnaire, a discussion panel was held to identify the most pertinent categories of questions and develop the initial questions. Two patient advocates from EU-PFF (one patient and one caregiver) co-developed the questionnaire (as well as the caregiver questionnaire). The advocates helped determine the set of questions to include and reworded the questions and responses into language that the general population would more easily understand. The questions regarding treatment adherence and treatment satisfaction were informed by a targeted literature review of existing generic and condition-specific instruments. Ultimately, a final questionnaire was produced that aimed to capture the nuances of the patient experience. To establish the health-related quality of life (HRQoL) of the patient, they were asked to rate their health in five different categories on a 0–100 answer scale.
Caregiver Questionnaire
The caregiver and patient questionnaires were similar, but the main difference was that the caregiver questionnaire also aimed to gain an understanding of the effect of different IPF treatments and treatment decisions on the caregiver. This meant that questions regarding the level of information that a caregiver received, their view on the condition of the person they care for, and caregiver-specific quality of life were included. To inform the development of these questions, a pragmatic literature review of existing caregiver-specific instruments was conducted.
Pulmonologist Questionnaire
The objective of the pulmonologist questionnaire was to capture how and why pulmonologists decide between IPF treatments, and to describe the patient population that each pulmonologist treats. To facilitate this, the summary of product characteristics (SmPCs) for pirfenidone and nintedanib were compared, to differentiate between the key characteristics of each treatment.15,16 In addition, a Delphi consensus study conducted by Rahaghi et al17 was reviewed. These documents were used to develop specific questions on prescription decisions and pulmonologist experience in treating IPF. The remaining questions were developed in an iterative process, similar to the patient and caregiver surveys.
Recruitment
All data were collected via an online survey platform (Qualtrics LLP). Participants were recruited between mid-November 2021 and mid-January 2022. If a participant declined to participate, the survey was terminated.
Recruitment varied across participant type and country. The patient and caregiver surveys were distributed by EU-PFF and local patient groups. In addition, the survey was distributed by local nurses in Belgium and the Netherlands. There was no patient or caregiver survey for Greece due to the difficulty in distributing the survey using an online survey platform. There were no exclusion criteria implemented for the patient and caregiver surveys; the only requirements were that a patient had to presently be diagnosed with IPF, or a caregiver must currently treat, or have treated, a patient with IPF. There were no incentives offered for patients or caregivers; however, EU-PFF received a nominal payment from Boehringer Ingelheim for every participant recorded.
The pulmonologist surveys were distributed by a third-party market research company (IQVIA). For the UK, ROI and Belgium, pulmonologists received letters that included survey information and a QR code linked to the survey. For the Netherlands, France, Finland and Greece, IQVIA emailed pulmonologists the survey information and survey link. In addition, three expert clinicians shared the brief and survey link with their colleagues. To be eligible to complete the survey, pulmonologists were required to see at least three IPF patients per year. The pulmonologists received payment from the study sponsor at a fair market rate to incentivize participation. The study sponsor was not involved in the selection of the recruited pulmonologists.
Data Analysis
Data were stored on the Qualtrics project database until the surveys were closed. Subsequently, data were downloaded from the database and cleaned and analyzed in the R Studio software package.18 Data from different countries were pooled to increase the power of the analysis, though some sub-group analyses were possible.
Descriptive summary statistics were generated by detailing the frequency of categorical variables and the mean of numerical variables. The answers to the five HRQoL questions in the patient questionnaire were mapped to utility values using the mapping algorithm developed by Oddershede et al.19
In addition to descriptive statistics, sub-group analysis was undertaken to describe and compare different sample populations. Sub-populations were derived by country, age, sex, the current drug taken by a patient, ethnicity, level of education and the prescription rates of the pulmonologists. For each sub-group, descriptive statistics were attained, and simple tests for differences between the samples were employed. These tests included the chi-squared test or Fisher’s test (dependent on sample size) for questions with categorical variables and tests for differences between means for numerical questions.
Results
Recruitment and Socio-Demographic Data
Patients
A total of 111 patients were recruited into the study; 95 of these completed the survey in full (85.6%). Most patients were recruited from Finland and France.
Table 2 shows a country breakdown by sociodemographic status. Most patients were male (62%), aged above 50 years (99%), identified as white (91%) and were living with their spouse/partner without children (69%). The majority of patients (71%) had been diagnosed within the past 5 years. Severity of disease was perceived as mainly moderate (41%) or severe (47%).
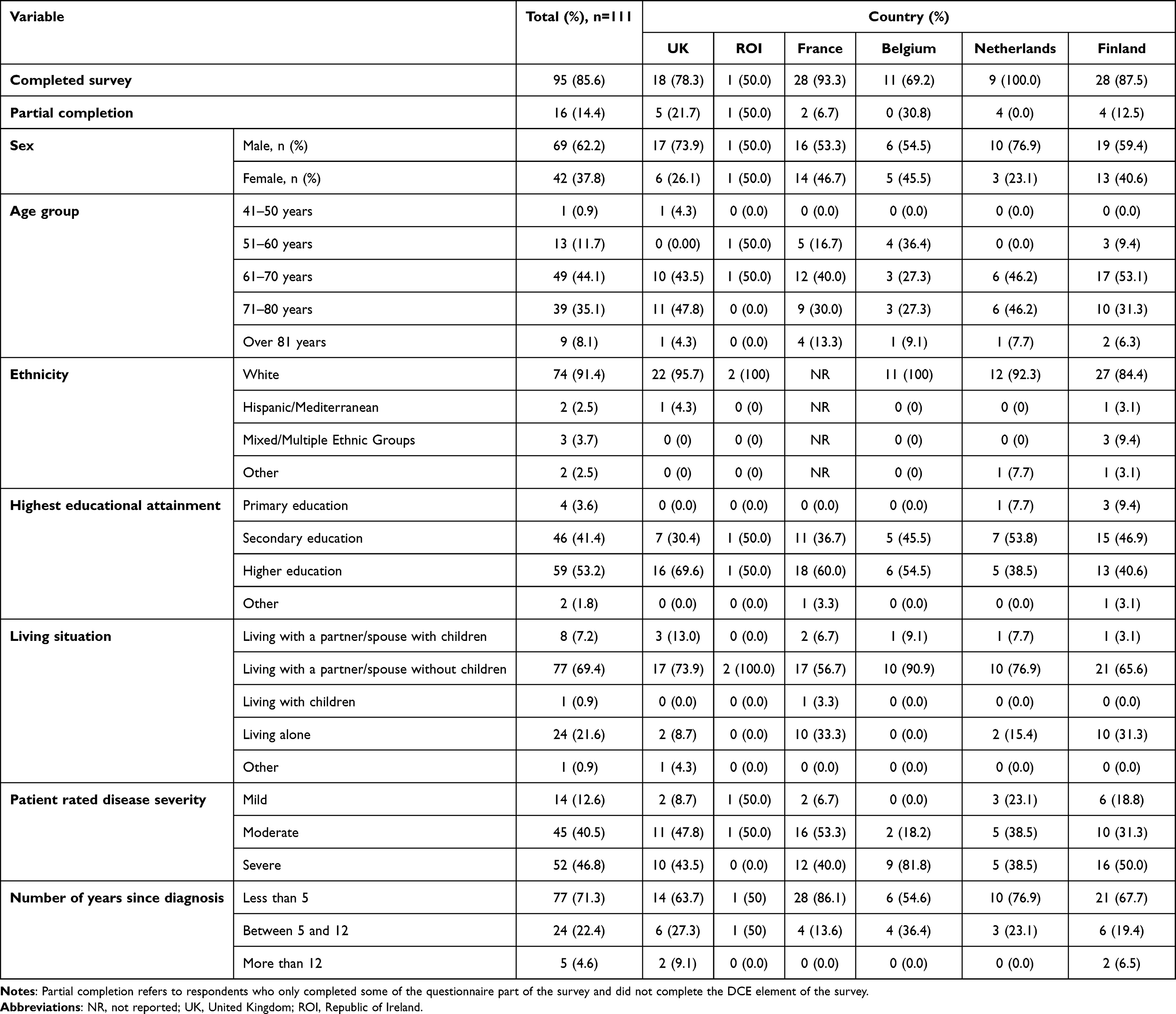 |
Table 2 Patient Respondents’ Socio-Demographic Characteristics |
Caregivers
A total of 22 caregivers completed the survey with the UK and France being the most represented countries (Table 3). The majority of caregivers were women aged between 51 and 70 years, living with the patient (82%) (their partner/spouse, 91%). In a minority of cases caregivers were involved in fewer than 3 hours of care per week (41%), but for the majority the level of care was three or more hours every week.
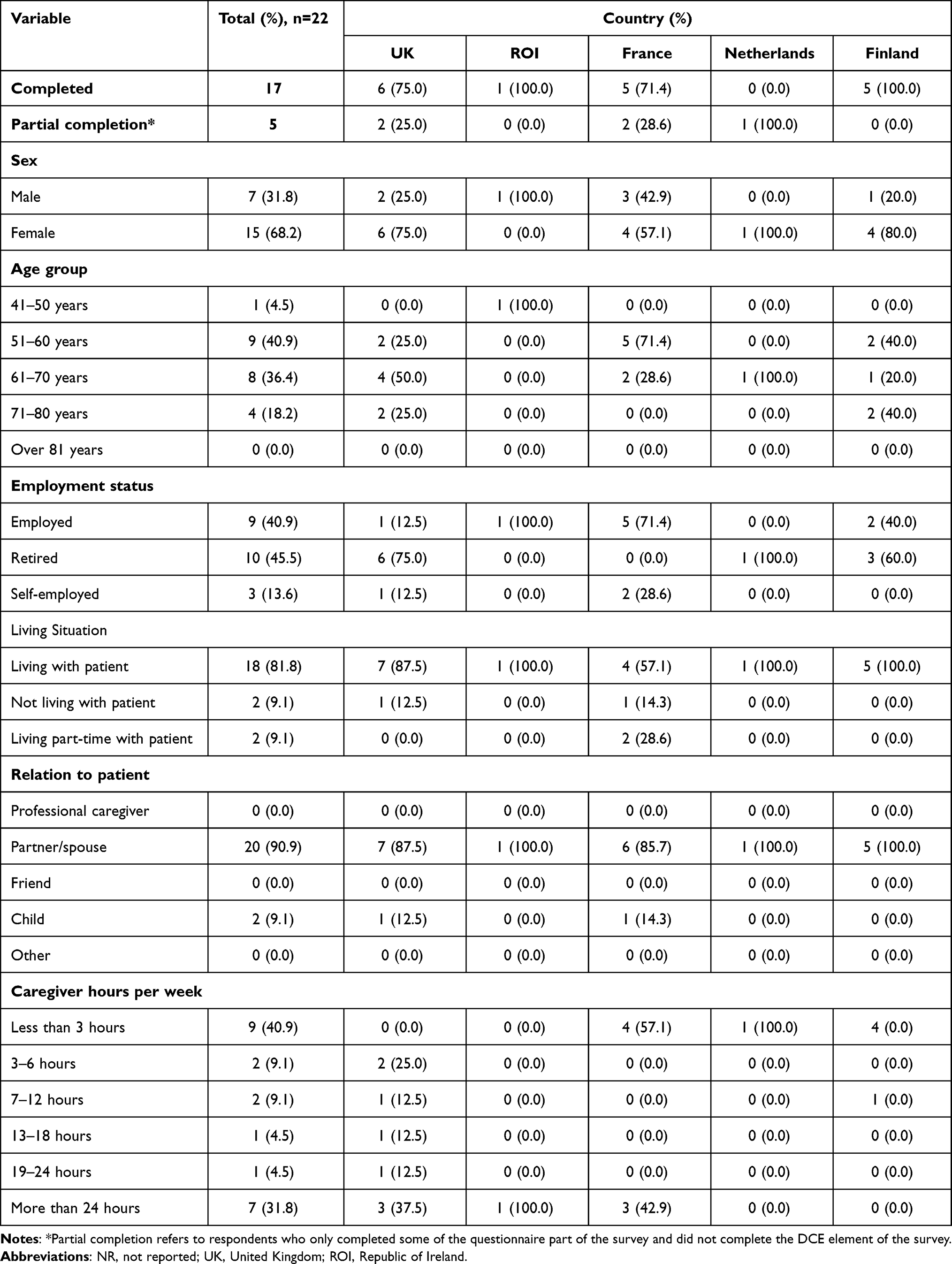 |
Table 3 Caregiver Respondents and Associated Completion Status per Country |
Pulmonologists
A total of 140 pulmonologists completed the survey, of whom 115 (82%) completed the entire survey (Table 4). The largest number of pulmonologists were recruited from the UK (51%). The majority of pulmonologists were in public practice (80%), and 55% had experience in managing IPF for up to 10 years.
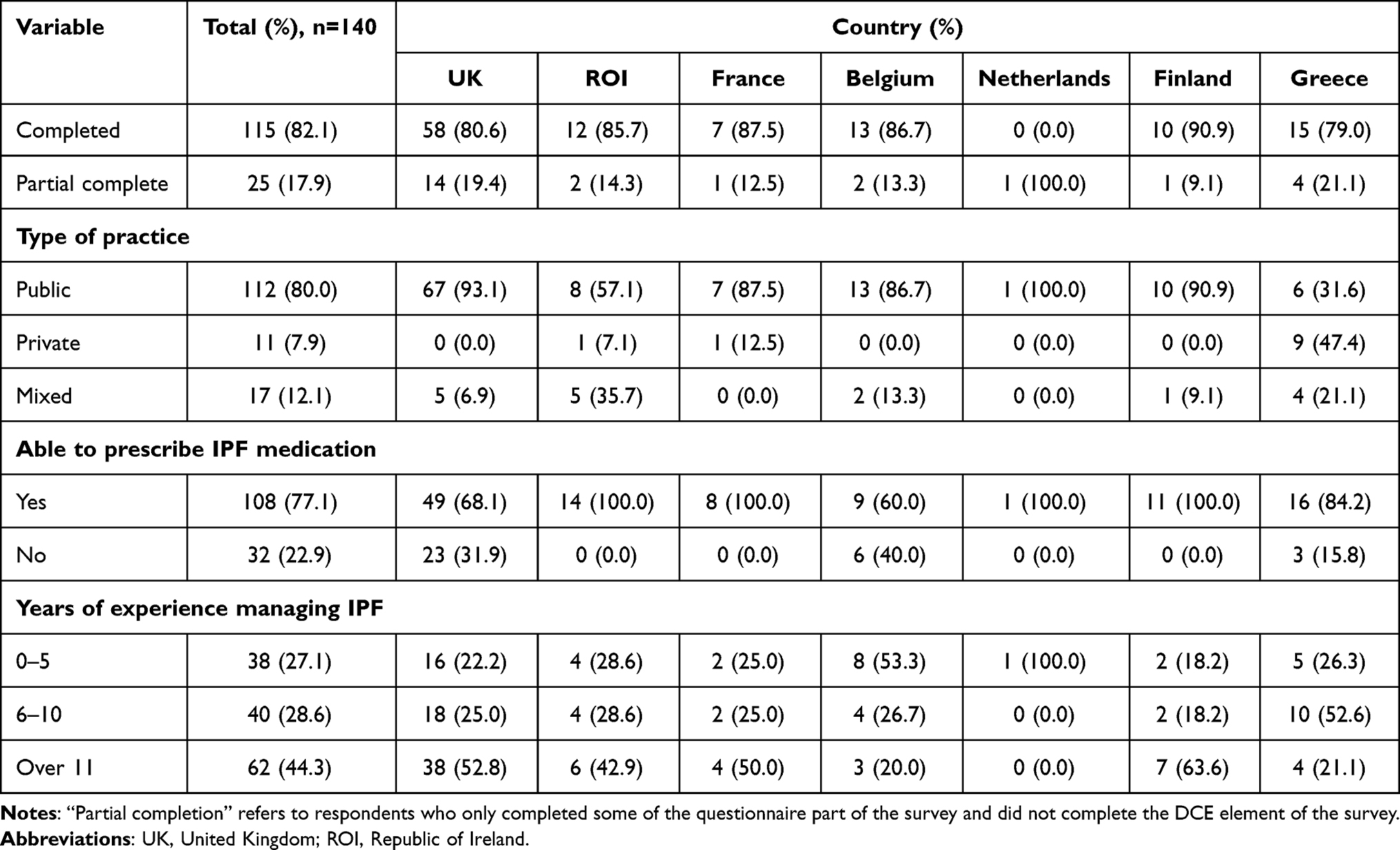 |
Table 4 Pulmonologist Respondents and Associated Completion Status per Country |
Around 41% of the pulmonologists saw 0 to 10 newly diagnosed IPF patients per year and most pulmonologists (63%) saw up to 50 IPF patients per year.
Clinical Status of Patients and Burden of Disease
Overall, 13%, 41% and 47% of the patients considered their IPF to be mild, moderate and severe, respectively. Twenty-two percent of the patients were on oxygen therapy and 16% were receiving pulmonary rehabilitation. Conversely, around a fifth of patients did not have any other medical support. Around 30% of the patients restricted their time outside to 1–3 hours; 58% restricted outdoor time to under 1 hour. Shortness of breath had prevented around 80% of the patients from daily activities in the past 4 weeks; similarly coughing had prevented around 60% of the patients from their daily activities.
In almost all cases, caregivers believed their partner’s disease to be severe (82%). They declared that the two main additional non-drug therapies consisted of oxygen therapy (29%) and pulmonary rehabilitation (35%). In terms of quality of life, a majority of caregivers (80%) noted that they were more stressed or significantly more stressed since the patient’s diagnosis. That said, the impact on self-reported mental wellbeing was small or had no effect in 60% of the caregivers. A similar pattern was also observed for physical wellbeing.
Although considerable variations of FVC were observed by country, pulmonologists reported that overall, 25%, 60% and 16% of their patients had FVC <50%, FVC 50–90% and FVC >90%, respectively. They declared that just over a third of patients were receiving oxygen therapy and 46% were receiving pulmonary rehabilitation. Pulmonologists recorded that 18% of their patients smoked. Regarding co-morbidities, pulmonologists noted that just under 40% of the patients had another pulmonary pathology and 48% had cardiovascular-related comorbidities. Mental health problems were recorded for a third of patients with 28% of the patients also having a metabolic disease. Other comorbidities were recorded in just under 30% of the patients with only 13% of the patients not having any comorbidities.
Treatment Details
Almost 80% of the patients reported currently taking IPF medication (Supplementary Table 1). Of those who had previous IPF treatment, there was roughly an equal split between those patients who had received nintedanib and those who had received pirfenidone. There were slightly more patients currently taking nintedanib compared with pirfenidone (53% versus 42%). Just over a third of patients (35.4%) had been on their current treatment for 3 or more years. The majority of patients (79%) had not received any IPF medication prior to their current regimen. For those who had changed to a different regimen, the main reason for this was side effects (45%) with a further 25% of the patients having changed medication due to their pulmonologist proposing an alternate treatment strategy (Supplementary Table 2). Patient satisfaction with their current treatment was moderate, with an average score of around 6 (out of 10).
Virtually all caregivers noted that their partner was currently taking antifibrotic medication for their IPF. The current treatment duration was up to 24 months in 55% of the patients. According to the caregivers, the majority of patients were taking nintedanib (64%), and three-quarters of patients had not received any previous IPF medication. Two-thirds of caregivers noted they had not been involved in any IPF treatment choice. Primary responsibility for organizing and ensuring IPF medication was taken correctly rested with the caregiver in 85% of the cases and 76% of the caregivers reported that the patient remained on top of their medication all of the time.
Pulmonologists reported that a total of 58% of their patients were receiving antifibrotic medication, although these numbers varied considerably by country with Finland having the largest proportion of patients not receiving this medication, and the Netherlands the lowest proportion. Of those patients taking antifibrotic medication, just under 56% were receiving nintedanib compared with 42% on pirfenidone. Pulmonologists also noted that around 26% of their patients were no longer taking pharmacological treatment. In the majority of cases, this was following a joint decision by the pulmonologist and patient. Adverse drug reactions were the most common reasons for treatment cessation followed by the patient no longer wishing to take medication.
Drug Interactions
A total of 134 unique concomitant medications were mentioned by patients. Two-thirds of patients reported they had not received any advice from their pulmonologist regarding the avoidance of certain foods or drinks, and almost three-quarters had not received any advice regarding the avoidance of certain medications (Supplementary Table 3).
When asked what other medications were also taken, the most mentioned one was pantoprazole, mentioned 13 times. When searching potential interactions through the drugs.com database,20 it was found that one patient on nintedanib could experience a drug–drug interaction with concomitant diltiazem and clopidogrel; three patients on pirfenidone could experience a drug–drug interaction with concomitant lansoprazole, and another patient with concomitant esomeprazole.
Just over 55% of the caregivers noted that there were no foods or drinks which the patient should avoid due to their IPF medication.
With regards to pulmonologists, 73% were either fairly confident or very confident of their knowledge of potential drug interactions for antifibrotics.
Adherence
Adherence to medication was high. The majority (81%) of patients were adherent in terms of not forgetting to take their medication (Supplementary Table 4). Similarly, 85% of the patients indicated “no” to the question: “have you decided not to take your medication in the past two weeks”. Virtually all patients had not forgotten to take their medication with them when travelling or leaving home, 86% had taken their medication the previous day and almost all patients (bar one) would continue to take medication even when symptoms were under control. Just under 80% of the patients reported never or rarely having difficulty remembering to take (all of) their medication.
Patient adherence to treatment was reported to be either very good or good by 84% of the pulmonologists. Factors affecting treatment adherence negatively were lower HRQoL, greater distance to the treatment center from home, patients being older with more comorbidities and being less well informed about IPF. More adverse drug reactions, lower perceptions of disease severity, living alone, frequent dosing schedules, and lower coping ability were all also deemed by pulmonologists to negatively impact on treatment adherence by patients as shown in Figure 1.
 |
Figure 1 Pulmonologist rating of factors on patient adherence. |
Adverse Events
The majority of patients (78%) had experienced an adverse event from the current therapy (Supplementary Table 5). Around half of patients (53%) limited their exposure (sometimes or often) to the sun due to IPF. Patients taking pirfenidone were significantly more likely than patients taking nintedanib to consider limiting their exposure to the sun (pirfenidone: 97%; nintedanib: 19%; p-value: <0.001).
Around 55% of the patients had considered taking medication against diarrhea (sometimes or often), and patients taking nintedanib were significantly more likely than patients taking pirfenidone to consider taking medication against diarrhea (pirfenidone: 33%; nintedanib: 74%; p-value: <0.001).
Just over a third (35%) had considered taking medication against nausea/vomiting, whereas 73% had considered taking medication to treat heartburn.
Adverse events were recorded by 65% of the caregivers; 40% of the caregivers noted that patients often limited their exposure to the sun due to IPF (conversely 40% also noted that patients never do this). Anti-diarrheal medication was recorded as being taken (by the patient) sometimes or often by 80% of the caregivers, and 55% noted that medication against nausea/vomiting was never taken.
Sixty-seven percent of the pulmonologists felt nausea was important or quite important in prescribing nintedanib, whereas 73% felt this was important or very important in prescribing pirfenidone. Nausea was considered most likely to occur at the start of treatment (73% pulmonologists) and was deemed to be moderate or severe in a quarter of cases. Thirty percent of the pulmonologists noted they would prescribe an additional secondary treatment for moderate-to-severe nausea and 36% would reduce the dosage.
Photosensitivity was noted as important or quite important for nintedanib by 50% of the pulmonologists and by 75% of the pulmonologists for pirfenidone. Photosensitivity was considered to be consistent throughout treatment by 42% of the pulmonologists and to be moderate to severe in 20% of the cases. The use of sun protection and a reduction in sun exposure were advocated for the treatment of moderate-to-severe photosensitivity.
Diarrhea was thought to be important to quite important by 91% of the pulmonologists in prescribing nintedanib and 63% of the pulmonologists in prescribing pirfenidone. Diarrhea was thought to occur at the beginning of treatment by 38% of the pulmonologists and consistently throughout treatment by 50% of the pulmonologists. In 30% of the cases, diarrhea was considered to be moderate to severe. Additional secondary treatment would be prescribed by 26% pulmonologists, 23% would reduce the dosage and 23% would interrupt treatment.
The vast majority (85%) of pulmonologists would extend the dose titration period for pirfenidone in elderly patients or for those with adverse drug reactions in all, to some, cases. The management of nausea, photosensitivity and diarrhea was considered difficult to manage for less than a third of pulmonologists, with no difference across side effects.
Source of Information
With respect to sources of information regarding current treatment choices, 77% of the patients received information from their pulmonologist and just under 10% from a nurse. In terms of information about the disease and treatment, the main source was the pulmonologist (44%), followed by the patient association (18%) and internet searches (15%) (see Supplementary Table 6).
Caregivers’ opinion was that overall levels of information about available IPF treatments were moderate.
Prescribing Decision Factors
Most pulmonologists believed the patient’s aspartate/alanine transaminase (AST/ALT) levels and potential interactions with concomitant medication (for both nintedanib and pirfenidone) were either important or quite important factors affecting prescribing decisions between the two molecules. Other important factors in prescribing were whether the patient required P-glycoprotein (P-gp) inhibitors/inducers or a cytochrome P450 (CYP1A2) inhibitor, the patient’s opinion on treatment options and their lifestyle (for both nintedanib and pirfenidone), the predicted FVC, the adverse drug reaction profile and the need for dose titration (pirfenidone). (See Supplementary Table 7).
The most preferred option for treatment changes following comorbidity in a stable patient was a decrease in the dose of current medication or treatment interruption for both renal and hepatic impairment (see Supplementary Table 8).
Impact of Patient Characteristics on Behavior
The impact of socio-demographic and clinical factors is summarized in Table 5. Age and level of education were the only factors that did not have a statistically significant impact on outcomes, but trends were observed. Belgian/Dutch patients were more satisfied with their treatment and were more frequently treated with pirfenidone compared with patients from other countries. French patients were less satisfied with their treatment and were more likely to be treated with nintedanib. However, no statistically significant difference in treatment satisfaction was observed between the two treatments Table 6. Nevertheless, nintedanib was associated with more diarrhea and pirfenidone with more limitation to sun exposure.
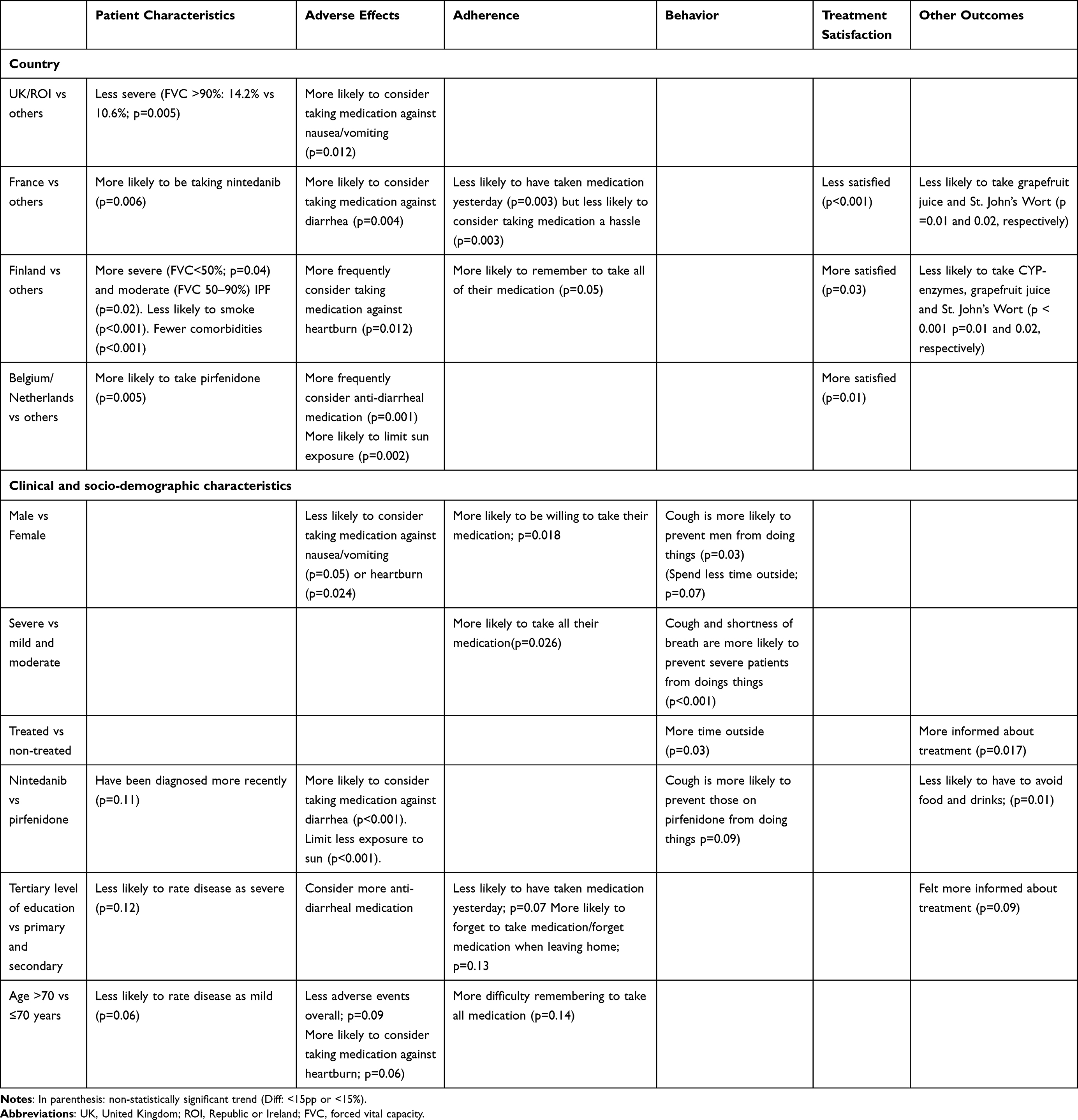 |
Table 5 Statistically Significant Differences in Questionnaire Findings Between Subgroups |
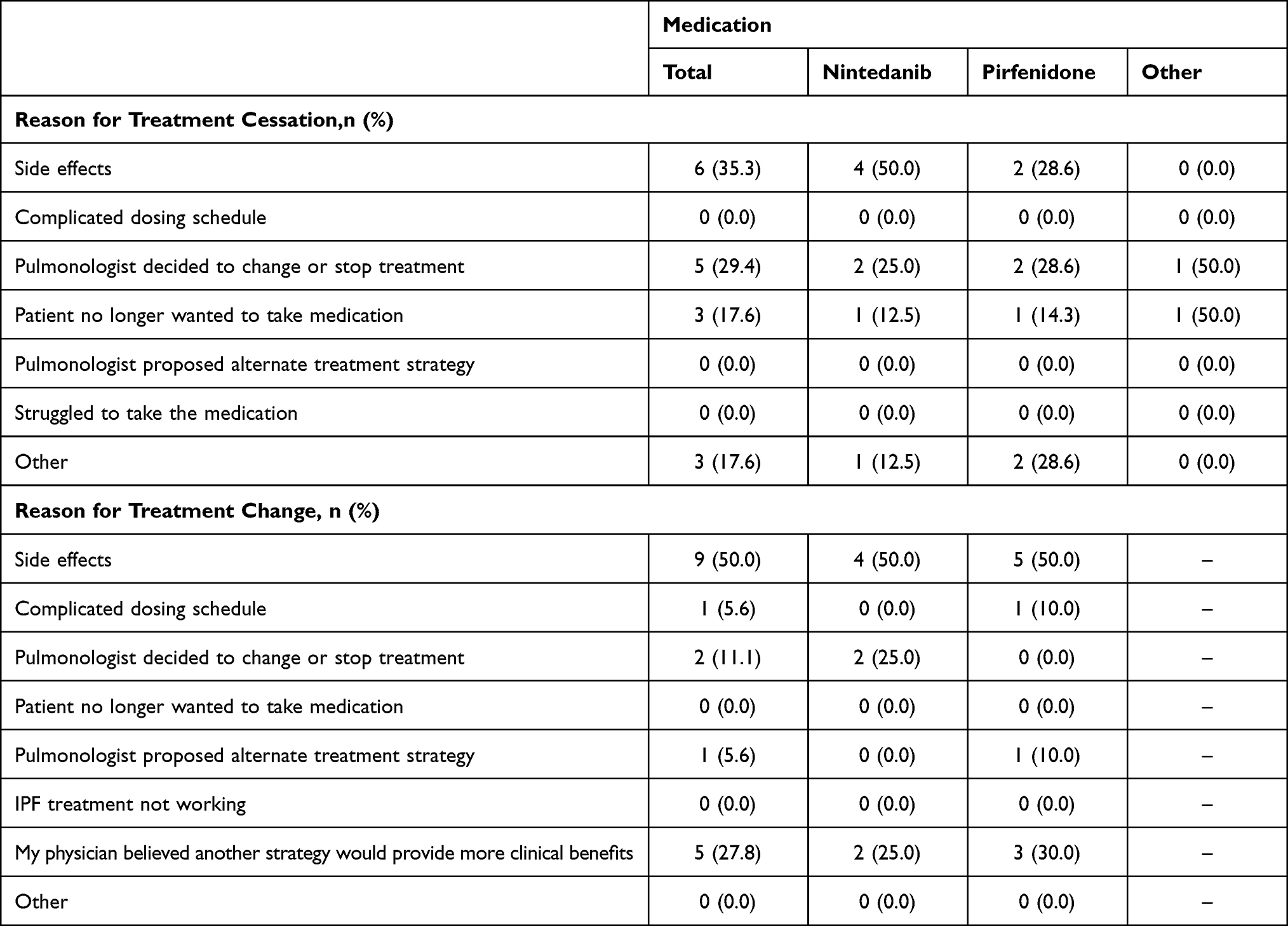 |
Table 6 Reported Reasons for Treatment Cessation and Change |
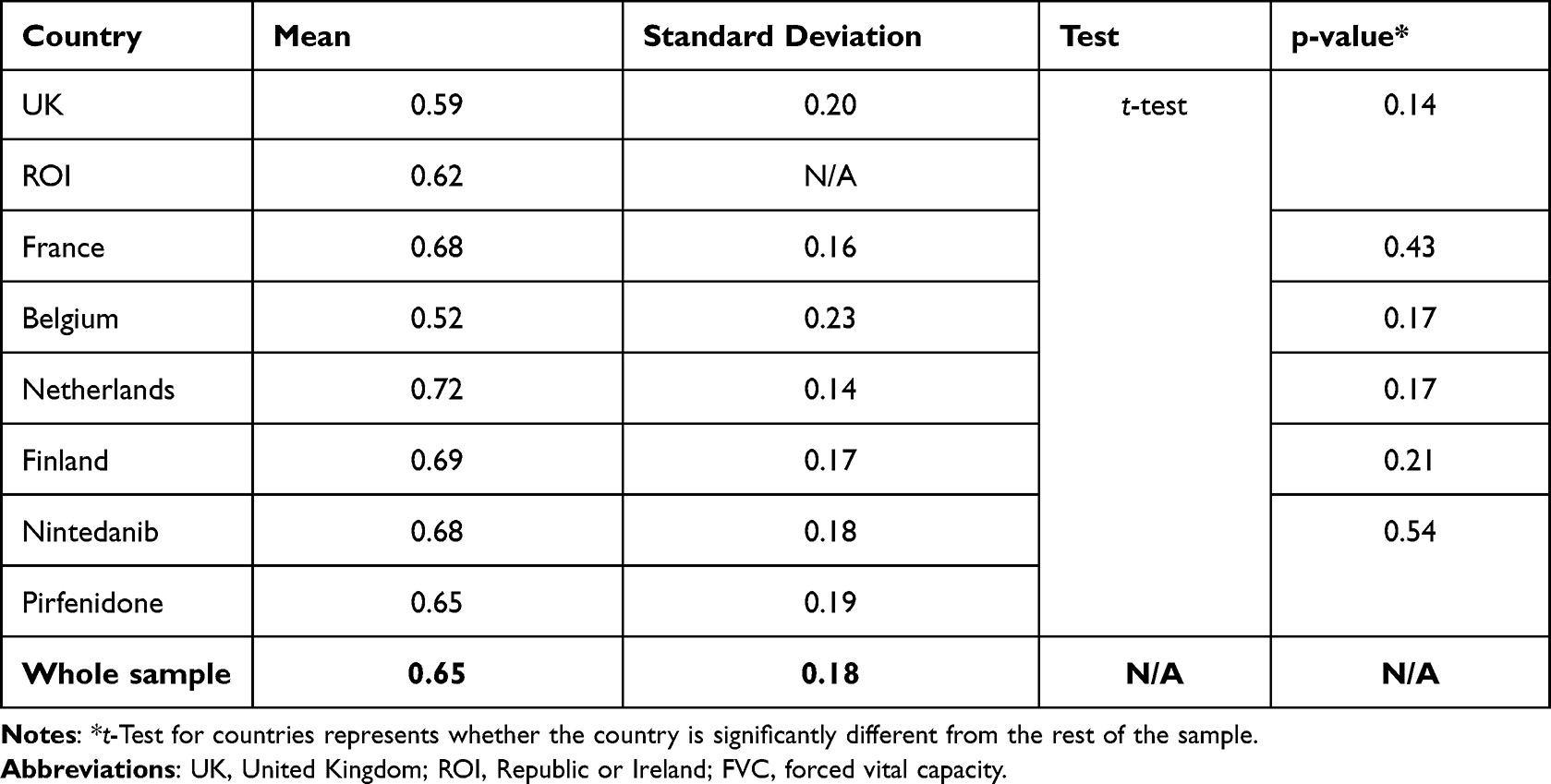 |
Table 7 Mean Utilities Stratified by Medication |
For patients currently on nintedanib, one patient had previously received nintedanib and seven patients had previously received pirfenidone. Among those currently on pirfenidone, five patients were previously receiving nintedanib. The most common reason for treatment change or cessation was side effects (Table 6).
Table 7 shows that there were cross-country differences in levels of HRQoL with Belgian participants reporting the lowest levels of HRQoL (0.52) and the Netherlands the highest level (0.72), although none of these differences were statistically significant. A small difference in HRQoL levels was observed between those patients on nintedanib (0.68) and those on pirfenidone (0.65), although again, these differences were not statistically significant.
Discussion
Over 100 patients participated in the study, mainly drawn from Finland (30%), France (27%), and the UK (21%). The proportion of females in the cohort (37%) was similar to that reported in epidemiological data from the UK (36%).21 The median age group of participants was 61–70 years and 53% reported a higher educational attainment. Based on incidence data from the European IPF registry, this was in line with the mean age of IPF patients in Europe (68 years).21
While 47% of the patients rated their disease as “severe”, 82% of the caregivers believed their partner’s disease was severe, implying a slight difference in perception of disease severity between the two stakeholders. This suggests that increased communication between patients, caregivers and pulmonologists around the impact of symptoms on quality of life is needed to better define the severity of IPF. However, it is important to note that self-reported severity was collected how and why the patients and caregivers classified the disease severity the way they did was not explored. Pulmonologists declared that only a quarter of their patients had a low FVC (below 50% of the predicted value), whereas data from various registries and real-world studies suggest that just 11% of the patients have an FVC <50% and that mean FVC in IPF patients is 78–81%.22–24 Interestingly, pulmonologists reported more oxygen therapy or physical therapy than the patients did. These findings suggest that IPF is perceived to be more severe among the three surveyed stakeholders than real world (registry) data imply.
It seemed unusual that for a relatively young cohort, with high educational attainment, just 32% of the patients reported receiving information about IPF mainly from the internet. This contrasted with a French study in which 60% (34 out of 57) of IPF patients reported using the internet for IPF research between 2016 and 2017.25 However, in the French study, patients were only asked about their internet use in a “yes/no” format. Given the multichoice nature of the I-Prefer questionnaire, it is possible that the results of this questionnaire are more reflective of the “true” IPF patient experience.
Slightly more patients were currently on nintedanib compared with pirfenidone (54% vs 42%), and just under a third had been on their current treatment for more than 3 years. However, 21% of the patients reported that they were not currently taking IPF medication and pulmonologists reported that 42% of their patients were not treated. While this seemed like a high level of unmedicated patients, it appears to reflect other studies, such as a Finnish study where only 35% of the patients received either nintedanib or pirfenidone.26 The results from the caregivers were broadly reflective of those from the patients in terms of the management of the disease.
In this study, 74% of the patients reported receiving no advice from their pulmonologist to avoid certain medications, and 66% did not receive advice on avoiding certain food or drink. A similar proportion of caregivers (55%) noted that there were no food or drinks to be avoided with AF medications. During the concomitant treatment analysis, it was found that one patient on nintedanib and four patients receiving pirfenidone were taking concomitant medications with potential interactions, as reported by the drugs interactions checker from drugs.com, the tool used in this study. According to the European SmPC, nintedanib is a substrate of P-gp. Inhibitors or inducers of P-gp such as ketoconazole, erythromycin, cyclosporin, rifampicin, carbamazepine, phenytoin and St. John’s Wort could increase or decrease exposure to nintedanib and cause increased adverse effects or reduced efficacy.15 Pirfenidone is metabolized via CYP1A2 with minor contributions from other CYP isoenzymes including CYP2C9, 2C19, 2D6, and 2E1. Therefore, fluvoxamine, enoxacin, ciprofloxacin, rifampicin, amiodarone, fluconazole, chloramphenicol, fluoxetine, paroxetine, omeprazole, grapefruit juice or cigarette smoking could modify exposure to pirfenidone, affecting the safety or efficacy of the treatment.16 When asking pulmonologists, the vast majority considered potential interactions with concomitant medication important, but for 19% of them, these interactions have little impact on their choice of antifibrotic treatment. Nineteen percent of the pulmonologists also mentioned that they had an alert system for drug interactions.
In this study, 97% of the patients taking pirfenidone sometimes or often limited their exposure to the sun to protect their skin due to IPF and 74% of the patients taking nintedanib sometimes, or often, considered taking medication against diarrhea. Only a third of patients considered taking medication against nausea/vomiting, with no difference between the two AF medicines. While the occurrence of diarrhea with nintedanib was in line with what is observed in clinical trials, the occurrence of rash or photosensitivity with pirfenidone was higher than that reported in the trials (29%),27 than that reported in a survey of IPF outpatients (59% of the patients).28 Nevertheless, in our study physicians believed that adverse events (nausea, diarrhea or photosensitivity) were difficult to manage in less than a third of their patients. In this study, around 30% of the surveyed pulmonologists considered photosensitivity, diarrhea, or nausea difficult or quite difficult to manage and the most frequent patient-reported reason for treatment cessation was side effects (33%). This indicates that more guidance should be given to pulmonologists and patients on the management of adverse reactions linked to IPF treatment. Using a modified Delphi process, Rahaghi et al collated clinical recommendations on the management of adverse events related to the use of nintedanib and pirfenidone. To manage rash with pirfenidone, it was recommended that the rash should be assessed for other causes, patients should ensure the use of sun protection and reduce sun exposure, and finally, pirfenidone should be temporarily stopped or discontinued treatment entirely if the rash is serious and persistent. To manage diarrhea with nintedanib, taking nintedanib with food or large meals with increased fiber and adequate hydration, taking therapies such as loperamide or diphenoxylate/atropine, interrupting then reducing the dose if the patient feels the symptoms are significant and finally, discontinuing treatment was recommended if the diarrhea was persistent and problematic.29,30
Treatment adherence was relatively high (81%), but this was in line with the caregivers' view (85%) and the pulmonologists' expectations, who noted that patients who continue their treatment regimen after the initial 3 months are generally adherent. Forgetting to take pills, being unwilling to take the medication, and considering the treatment plan a hassle were the most frequently reported reasons of lower adherence. This highlights the need to educate patients on the benefits of the medications and to teach patients techniques for remembering to take their medication. Pulmonologists also thought that treatment adherence was high, and that higher disease severity and a longer time on treatment were drivers for better adherence. In a Belgian study on adherence in IPF, it was found that a high dosing adherence seemed necessary to maintain lung function. Knowledge about the disease was associated with higher adherence, but adherence significantly decreased over time.31 In our study, we also saw that patients who were Finnish, male, younger (≤70 years) with severe disease tended to adhere more to their medication. Regardless of the patient profile, pulmonologists should continue to insist on the importance of taking medication to ensure high adherence, even if the medication does not improve symptoms.
HRQoL for patients with IPF was lower than that for the age-adjusted general populations. For example, in this study, the mean utility for Finland was 0.69, whereas the published mean utilities for 65 to 74 year-olds in Finland is 0.82 (roughly corresponding to the 61–70 age category in this study).32 Similarly, the UK mean of 0.59 in this study was much lower than the English mean utilities of 0.862 (across age categories) and 0.79 for the age category 65–74 years.32 These results clearly indicate the major impact IPF has on HRQoL. While caregivers also reported more stress since the patient’s diagnosis, the impact on self-reported mental wellbeing was small for these stakeholders.
Limitations
There were some limitations in this study, firstly, the sample was too small to draw meaningful conclusions about caregiver characteristics. Additionally, the questionnaires were distributed by patient organizations, which may have limited the selection of patients to those who are more involved or informed about their disease than patients usually seen in clinical practice.
Another limitation of the study was that there was no defined link between the three samples of stakeholders. Ideally, the study would include the set of caregivers that care for, and the set of pulmonologists that manage, the sample of patients. As this is not the case, the interpretation of observed differences in perceptions should be made carefully. For example, the difference in perceptions between patients and pulmonologists could be due to the over-representation of UK pulmonologists and/or an over-representation of French and Finnish patients in our study.
A final limitation is that insights were not collected from other clinical practitioners that are involved in the management of IPF alongside pulmonologists. For example, physiotherapists and nurses could provide an insight into the day-to-day management of IPF which would complement the perceptions of pulmonologists.
Conclusion
The results from these stakeholder questionnaires have shown that patients and pulmonologists are not quite aligned in terms of perceived disease severity.
There is also a suggestion that IPF patients are under treated given that pulmonologists declared that almost 40% of their patients were not treated with either nintedanib or pirfenidone, the only two treatments that are approved for the treatment of the disease. While IPF prognosis is poor, both nintedanib and pirfenidone have been shown to reduce the decline in lung function, with benefits on survival.27,33,34 Both drugs have different but manageable adverse reactions, with nintedanib being associated with diarrhea and nausea and pirfenidone associated with skin rash/photosensitivity, nausea and decreased appetite. Strategies to mitigate these adverse reactions should be tested first before changing or discontinuing treatment.
The exploratory sub-analyses suggested that some disease and patient characteristics influence medication use and treatment adherence. In this study, patients who rated their disease as severe were more adherent to their therapy, male patients less frequently decided to skip medication but were less likely to take medication against nausea or heartburn than females, and untreated patients were less informed about treatment. Several country-specific findings were found to be statistically significant, but conclusions should be taken cautiously due to the limited number of respondents per country. Nevertheless, these findings could hint the impact of cultural, clinical or socio-demographic factors on patients’ perceptions or behaviors. To our knowledge, this study is the first to explore behaviors per sub-group of patients and further investigation with higher numbers of participants is needed to fully understand these implications.
Such findings should be disseminated to patient–physician groups to improve the inclusion of the patient voice in treatment decision-making, especially in reflection of the fact that the majority of pulmonologists considered patient opinion on treatment options to be important or quite important (91%).
Acknowledgments
EU-PFF received a financial compensation to help support the design of the questionnaire, disseminate the survey and analyse the results.
Funding
This manuscript is supported and funded by Boehringer Ingelheim International GmbH (BI). BI was given the opportunity to review the abstract for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
Stephane Soulard and Luis Pacheco are employees of Boehringer Ingelheim. Steve Jones is President of EU-PFF and a patient. Liam Galvin is Chief Executive of EU-PFF and was a carer. Liam Galvin also reports organizational grants from Boehringer Ingelheim, Chiesi, Trevi Therapeutics, The Roche Group, CSL Behring, Vicore Pharma, Bristol Meyer Squibb; travel supports from European Lung Foundation and ERN-Lung, outside the submitted work. Tom Bromilow, Stuart Mealing, Adam B Smith, and Damian Lewis are employees of York Health Economics Consortium and provided writing, editorial support, and formatting assistance, which was contracted and funded by Boehringer Ingelheim. Maria Hollmen and Antoine Froidure received payment from Boehringer Ingelheim for helping to develop and review the questionnaire and DCE and comment on the study results. Antoine Froidure discloses consultancy and speakers fees from GlaxoSmithKline, Roche and Boehringer Ingelheim, outside the submitted work. Antoine Froidure’s institution has received unrestricted research grants from Roche and Boehringer Ingelheim. The authors report no other conflicts of interest in this work.
References
1. King TE Jr, Pardo A, Selman M. Idiopathic pulmonary fibrosis. Lancet. 2011;378(9807):1949–1961. doi:10.1016/S0140-6736(11)60052-4
2. National Heart Lung and Blood Institute. Idiopathic pulmonary fibrosis. Available from: https://www.nhlbi.nih.gov/health-topics/idiopathic-pulmonary-fibrosis.
3. Richeldi L, Collard HR, Jones MG. Idiopathic pulmonary fibrosis. Lancet. 2017;389(10082):1941–1952. doi:10.1016/S0140-6736(17)30866-8
4. National Health Service. Idiopathic pulmonary fibrosis; 2019. Available from: https://www.nhs.uk/conditions/idiopathic-pulmonary-fibrosis/.
5. Hilberg O, Hoffmann-Vold A-M, Smith V, et al. Epidemiology of ILDs and their progressive-fibrosing behaviour in six European countries. ERJ Open Res. 2021;00597–02021. doi:10.1183/23120541.00597-2021
6. Ley B, Collard HR. Epidemiology of idiopathic pulmonary fibrosis. Clin Epidemiol. 2013;5:483. doi:10.2147/CLEP.S54815
7. Cano-Jiménez E, Hernández González F, Peloche GB. Comorbidities and complications in idiopathic pulmonary fibrosis. Med Sci. 2018;6(3):71. doi:10.3390/medsci6030071
8. Fernández Fabrellas E, Peris Sánchez R, Sabater Abad C, Juan Samper G. Prognosis and follow-up of idiopathic pulmonary fibrosis. Med Sci. 2018;6(2):51. doi:10.3390/medsci6020051
9. Langford B, Diamantopoulos A, Maher TM, Inoue Y, Rohr KB, Baldwin M. Using data on survival with idiopathic pulmonary fibrosis to estimate survival with other types of progressive fibrosis interstitial lung disease: a bayesian framework. Adv Ther. 2022;39(2):1045–1054. doi:10.1007/s12325-021-02014-z
10. Zurkova M, Kriegova E, Kolek V, et al. Effect of pirfenidone on lung function decline and survival: 5-yr experience from a real-life IPF cohort from the Czech EMPIRE registry. Respir Res. 2019;20(1):16. doi:10.1186/s12931-019-0977-2
11. King TE, Bradford WZ, Castro-Bernardini S, et al. A Phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2083–2092. doi:10.1056/NEJMoa1402582
12. Richeldi L, Du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–2082. doi:10.1056/NEJMoa1402584
13. Maher TM, Swigris JJ, Kreuter M, et al. Identifying barriers to idiopathic pulmonary fibrosis treatment: a survey of patient and physician views. Respiration. 2018;96(6):514–524. doi:10.1159/000490667
14. Hollmen M, Wijsenbeek M, Bromilow T, et al. I-PreFer Study: A Discrete Choice Experiment to Explore Patient, Caregiver and Pulmonologist Preferences of Idiopathic Pulmonary Fibrosis Pharmacological Treatment Options. Patient Prefer Adher. 2023;17:1895–1906. doi: 10.2147/PPA.S409767
15. Electronic Medicines Compendium (EMC). Ofev 100 mg soft capsules; 2021. Available from: https://www.medicines.org.uk/emc/product/1786/smpc.
16. Electronic Medicines Compendium (EMC). Esbriet 267 mg film-coated tablets SmPC; 2022. Available from: https://www.medicines.org.uk/emc/product/2731/smpc.
17. Rahaghi FF, Safdar Z, Brown AW, et al. Expert consensus on the management of adverse events and prescribing practices associated with the treatment of patients taking pirfenidone for idiopathic pulmonary fibrosis: a Delphi consensus study. BMC Pulm Med. 2020;20(1):1–3. doi:10.1186/s12890-020-01209-4
18. R Core Team. R: a language and environment for statistical computing. R foundation for statistical computing; 2022. Available from: https://www.R-project.org.
19. Oddershede L, Andreasen JJ, Ehlers L. Estimation of utility values from visual analog scale measures of health in patients undergoing cardiac surgery. Clinicoecon Outcomes Res. 2014;6:21–27. doi:10.2147/CEOR.S55899
20. Drugs.com. Nintedanib; 2022. Available from: https://www.drugs.com/nintedanib.html#interactions.
21. Asthma and Lung UK. Idiopathic pulmonary fibrosis statistics; 2012. Available from: https://www.blf.org.uk/support-for-you/idiopathic-pulmonary-fibrosis-ipf/statistics.
22. Cano-Jiménez E, Romero Ortiz AD, Villar A, Rodríguez-Nieto MJ, Ramon A, Armengol S. Clinical management and acute exacerbations in patients with idiopathic pulmonary fibrosis in Spain: results from the OASIS study. Respir Res. 2022;23(1):235. doi:10.1186/s12931-022-02154-y
23. Wuyts WA, Dahlqvist C, Slabbynck H, et al. Baseline clinical characteristics, comorbidities and prescribed medication in a real-world population of patients with idiopathic pulmonary fibrosis: the PROOF registry. BMJ Open Respir Res. 2018;5(1):e000331. doi:10.1136/bmjresp-2018-000331
24. Spencer LG, Loughenbury M, Chaudhuri N, Spiteri M, Parfrey H. Idiopathic pulmonary fibrosis in the UK: analysis of the British Thoracic Society electronic registry between 2013 and 2019. ERJ Open Res. 2021;7(1):00187–02020. doi:10.1183/23120541.00187-2020
25. Le Garrec M, Rousseau C, Thépault F, Kerjouan M, Salé A, Jouneau S. Prevalence, predicting factors and impact of internet use by patients with idiopathic pulmonary fibrosis: a cross-sectional observational study. Respir Med Res. 2021;79:100818. doi:10.1016/j.resmer.2021.100818
26. Salonen J, Purokivi M, Hodgson U, Kaarteenaho R. National data on prevalence of idiopathic pulmonary fibrosis and antifibrotic drug use in Finnish specialised care. Eur Respir J. 2022;60(suppl 66):4357.
27. Troy LK, Corte TJ. Therapy for idiopathic pulmonary fibrosis: lessons from pooled data analyses. Eur Respir J. 2016;47(1):27. doi:10.1183/13993003.01669-2015
28. Moor CC, Mostard RLM, Grutters JC, et al. Patient expectations, experiences and satisfaction with nintedanib and pirfenidone in idiopathic pulmonary fibrosis: a quantitative study. Respir Res. 2020;21(1):196. doi:10.1186/s12931-020-01458-1
29. Faverio P, Bocchino M, Caminati A, et al. Nutrition in patients with idiopathic pulmonary fibrosis: critical issues analysis and future research directions. Nutrients. 2020;12(4):1131. doi:10.3390/nu12041131
30. Rahaghi F, Belperio JA, Fitzgerald J, et al. Delphi consensus recommendations on management of dosing, adverse events, and comorbidities in the treatment of idiopathic pulmonary fibrosis with nintedanib. Clin Med Insights Circ Respir Pulm Med. 2021;15:11795484211006050. doi:10.1177/11795484211006050
31. Delameillieure A, Wuyts WA, Pironet A, Dobbels F. Electronically monitored medication adherence in idiopathic pulmonary fibrosis: prevalence, predictors and outcomes. ERJ Open Res. 2022;8(3):00030–02022. doi:10.1183/23120541.00030-2022
32. Szende AJB, Cabases J, editors. Self-Reported Population Health: An International Perspective Based on EQ-5D. Dordrecht (NL): Springer; 2014.
33. Roskell N, Saunders O, Lee D, Fisher M. Long-term survival analysis: pirfenidone compared to standard care for the treatment of patients with idiopathic pulmonary fibrosis. Eur Respir J. 2014;44(Suppl 58):1905.
34. Lancaster L, Crestani B, Hernandez P, et al. Safety and survival data in patients with idiopathic pulmonary fibrosis treated with nintedanib: pooled data from six clinical trials. BMJ Open Respir Res. 2019;6(1):e000397. doi:10.1136/bmjresp-2018-000397
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.