")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 12
Hyponatremia as an Inflammatory Marker of Lupus Activity Is a Fact or Fad: A Cross-Sectional Study
Authors Yamany A, Behiry ME , Ahmed SA
Received 3 November 2019
Accepted for publication 24 January 2020
Published 12 March 2020 Volume 2020:12 Pages 29—34
DOI https://doi.org/10.2147/OARRR.S237168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Ahmed Yamany, Mervat E Behiry, Sahar A Ahmed
Faculty of Medicine, Cairo University, Cairo, Egypt
Correspondence: Mervat E Behiry Tel +20 1124205071
Fax +20 26 28 884
Email [email protected]
Purpose: Systemic lupus erythematosus (SLE) is an autoimmune disease with multi-organ involvement. Hyponatremia is common in inflammatory diseases such as meningitis. Also, it has been found to be strongly associated with the degree of inflammation. However, it has not been fully evaluated in lupus. This study aimed to assess the inflammatory impact of hyponatremia in SLE patients and investigate its relationship with SLE disease activity.
Patients and Methods: A total of 101 patients with SLE were enrolled in this study and divided into two groups according to Na level; a normo-natremic group and a hyponatremic group. Demographic and clinical data were collected. SLE activity was assessed by the systemic lupus erythematosus disease activity index (SLEDAI). The estimated sedimentation rate (ESR) as well as levels of C-reactive protein (CRP) and complements (C3 and C4) were measured.
Results: The majority of patients were females (98 subjects) (97%) with a mean age of 33± 8 years. Out of 101 participants, 40 patients (39.6%) were hyponatremic with a mean Na level of 131.58± 3.11 mmol/L. There was a statistically negative correlation between both ESR and SLEADI score and Na level (r=− 0.436 and − 0.436, respectively) with p=0.002, whereas Na level was positively correlated with complements, Cl, and albumin levels (r=0.653, 0.314, and 0.460, respectively) (p=0.000, 0.027, and > 0.001, respectively). CRP was not correlated with Na level. ESR was independently correlated with hyponatremia at the 95% CI for Exp B (0.997– 0.058) with a p-value of 0.048.
Conclusion: Hyponatremia could be used as an indicator of SLE activity. Also, it might be an easily and rapidly detected as well as a prognostically useful marker of inflammation.
Keywords: lupus erythematosus, activity, hyponatremia, complement, inflammation
Introduction
Systemic lupus erythematosus (SLE) is a multi-systemic autoimmune disease that encompasses several clinical manifestations and has different laboratory characteristics.1 The pathogenesis of SLE remains indefinable, but it mainly depends on the interplay of genetic, environmental, and hormonal factors.2 Besides, identified cytokines such as interleukin-6 (IL-6), IL-1, and tumor necrosis factor-alpha (TNF-α) give rise to immune dysregulation, tissue inflammation, and organ injury in lupus disease.3
SLE is associated with water and electrolyte disorders such as hypokalemia, hyper/hyponatremia, calcium disturbance, and acid–base balance disturbance. These disorders are mostly due to drug-related drawbacks and to a lesser extent direct effects of lupus disease. For example, lupus nephritis which becomes more complicated with tubulointerstitial damage may be attributed to such electrolyte abnormalities.4
Hyponatremia is infrequently observed among lupus patients. Nevertheless, in the clinical setting of CNS-related lupus activity, there is an increased IL-6 production resulting from the inappropriate cerebral secretion of antidiuretic hormone5,6 through non-osmotic stimulation of vasopressin by many stimuli such as pain and inflammation.7
Hyponatremia is not well investigated in lupus in terms of its incidence, pathophysiology, or relation to the disease activity. Far too little attention was paid to sodium abnormalities in SLE. In literature, previous two cohorts showed that hyponatremia could reflect the disease activity and could also be related to acute inflammatory markers.8 A recent study suggested that hyponatremia is associated with higher disease activity, fatigue development, and perception in lupus patients.9
There is scarcity of data on the association of hyponatremia with lupus. Therefore, this descriptive cross-sectional study was conducted to determine the prevalence of hyponatremia in lupus patients as well as its correlation with the disease activity and explore a new area of inquiry.
Materials and Methods
Study Design and Population
A cross-sectional study was conducted on 101 patients with SLE who were fulfilling the American College of Rheumatology (ACR) revised classification10 and aged >18 years. These patients were recruited consecutively from the rheumatology outpatient clinics of the internal medicine department of Cairo University hospital during the study period (January 2017-December 2017). Patients with severe hepatic or cardiac dysfunction, tubular injury proved by renal biopsy, concurrent infections, diarrhea, or vomiting as well as patients on diuretics medications and pregnant females were ruled out form the study.
According to Na level, the included patients in this study were divided into 2 groups; group (I) which included patients with normo-natremia (61 subjects) and group (II) which included patients with hyponatremia (40 patients). Hyponatremia patients are defined as those having serum Na <135 mmol/L.
All patients enrolled in the study were subjected to full history taking and complete physical examination with a special highlight on the manifestations of lupus activity which was assessed by systemic lupus erythematosus disease activity index (SLEDAI) score.11 The SLEDAI is a physician-administered instrument measuring SLE activity during the last 10 days. It evaluates 16 clinical features and 8 laboratory indices. The weight which is/was applied to each index gives this tool a range of 0–105 points.
The study protocol corroborates to the ethical guidelines of the Helsinki declaration. It was reviewed and approved by the ethical committee. Written informed consents were obtained from the study participants.
Blood Collection and Sample Preparation
Fresh peripheral blood was collected from SLE patients who were fasting overnight by sterile syringes. All laboratory analyses were performed within one hour after the collection of samples. The samples were centrifuged, and serum sodium and potassium assays were analyzed using the ion-selective electrode method by auto-analyzer microprocessor-controlled electrolyte system (EasyLyte Instrument Inc., Medica Corporation, 5 Oak Park Drive, Bedford, MA 01730, USA).
Complete blood count was estimated using cell counter by Cell Dyn machine; erythrocyte sedimentation rate (ESR) was estimated by Westergren’s method, C-reactive protein (CRP) was estimated by nephelometry DN100, Anti-nuclear antibody (ANA) was estimated by indirect immunofluorescence, and complements (C3, C4) were estimated by radial immunodiffusion. Estimation of serum creatinine and liver enzymes was done by the kinetic method over the automation system by Dimension machine, urine analysis, and 24 hr urinary protein were measured.
Data Analysis and Statistical Methodology
Microsoft excel 2013 was used for data entry and the statistical package for social science (SPSS version 24) was used for data analysis. Simple descriptive statistics (arithmetic mean and standard deviation) were used for the summary of normal quantitative data, while frequencies were used for qualitative data. The bivariate relationship was displayed in cross-tabulations and comparison of proportions was performed using the Chi-square test and Fisher’s exact test where appropriate. T-independent test was used for comparing normally distributed quantitative data. The factors that were significantly associated with hyponatremia in bivariate analysis (P<0.05) were included in the multivariate logistic regression model. Receiver operating characteristic (ROC) curve analysis was carried out to test the diagnostic performance of hyponatremia predictors.
Results
A total number of 101 systemic lupus patients were enrolled in the current study; most of them were females (98 subjects) (97%) with a mean age of 33±8. All patients were on steroids at a dose ranging from 5mg/d to 40mg/d. The mean (SD) value of steroid intake duration was 4.5 (3.8) yrs. The mean (SD) value of plasma osmolarity for all the studied patients was 384 (11.04) mOsm/Kg. Forty-six participants (45.5%) were presented with severe disease activity (SLEADI ≥12) with a mean SLEDAI value of 12 ±10.
The demographic, clinical, and laboratory characteristics of the studied population are demonstrated in Table 1.
The data depicted in Table 2 revealed the significantly higher ESR and CRP levels as well as lower complement levels in patients with hyponatremia compared to those with normo-natremia. Hyponatremic patients demonstrated higher SLE activity and SLEDAI (16.1±10.136) compared to normo-natremic patients (7.02±6.568) (p=<0.001).
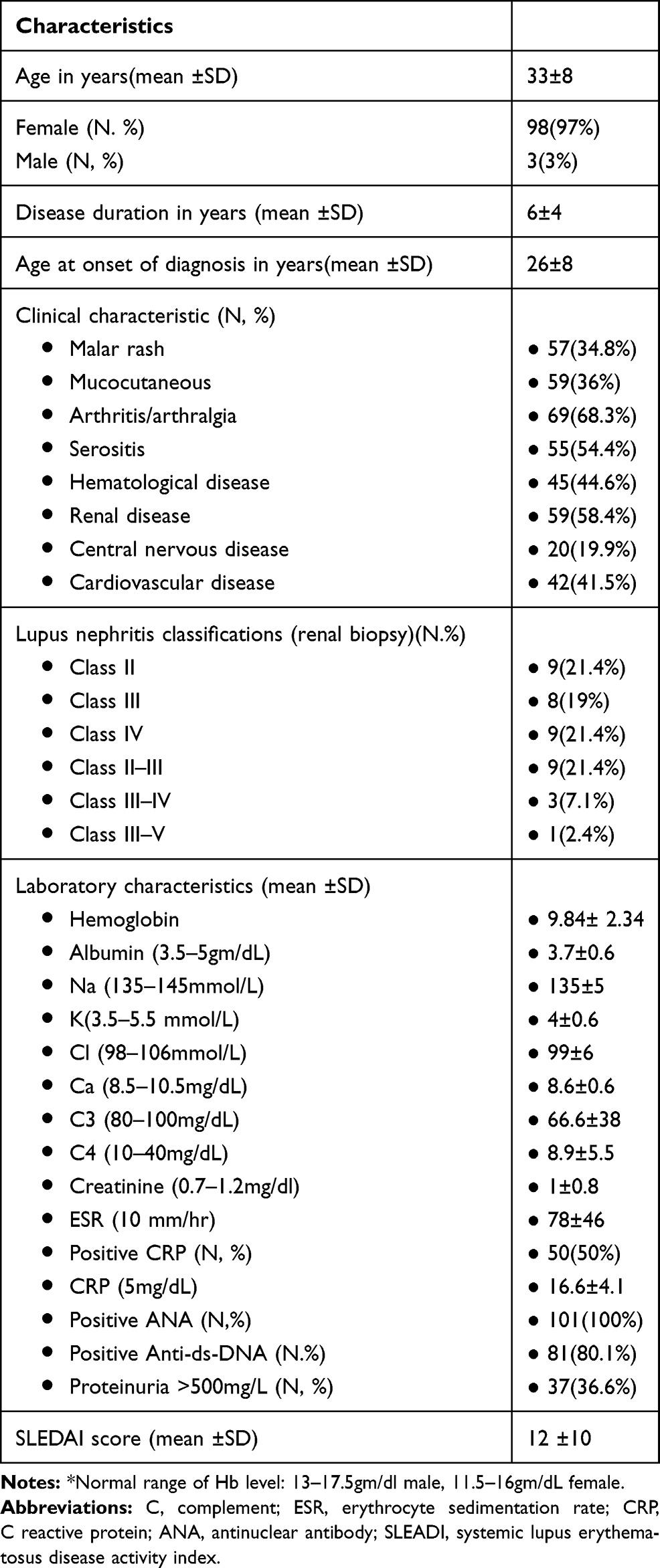 |
Table 1 Demographic, Clinical and Laboratory Characteristics of the Studied Group |
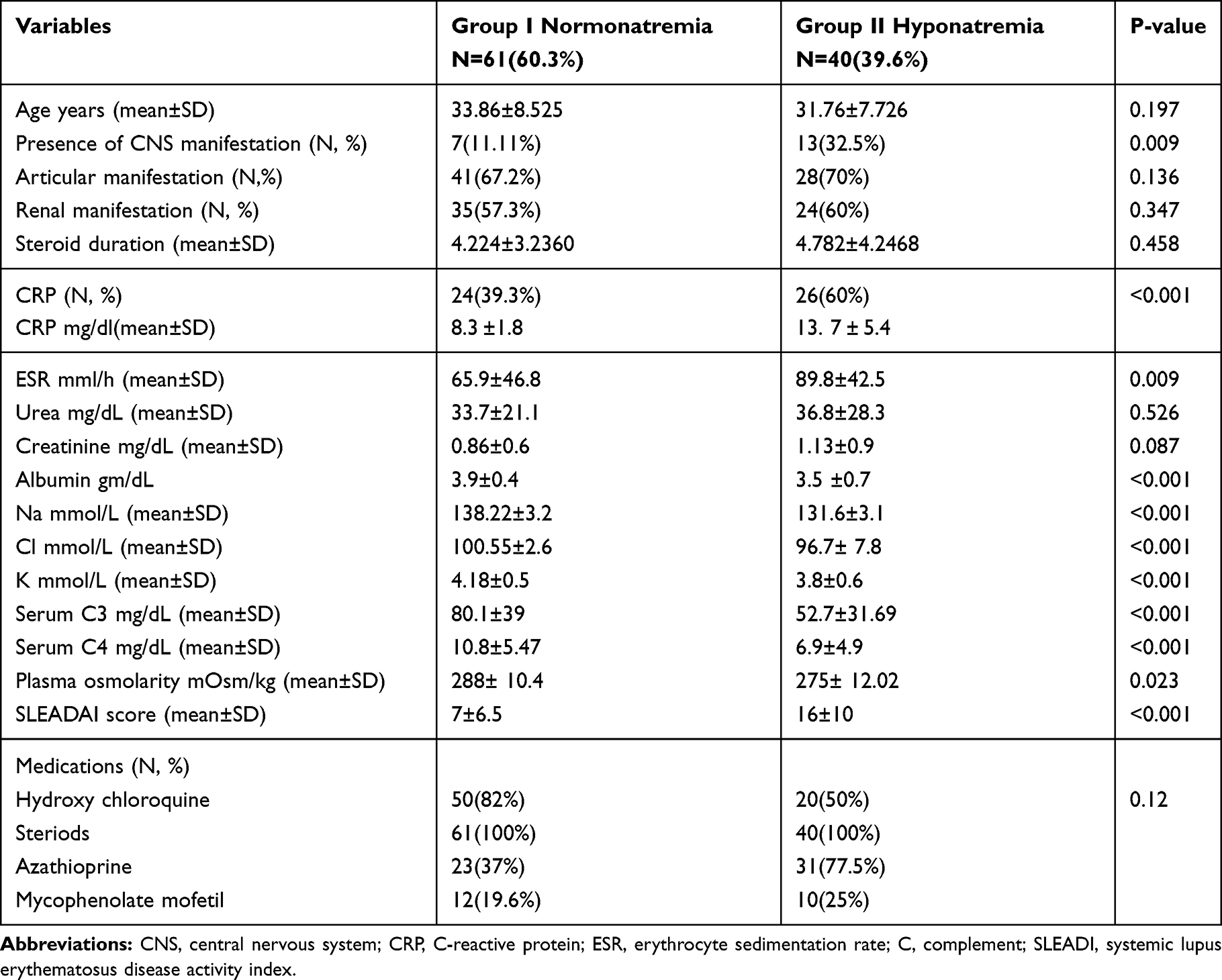 |
Table 2 Comparison Between Normonatremic and Hyponatremic Lupus Patients Regarding Clinical and Laboratory Parameters |
CNS manifestations were significantly expressed in hyponatremic patients (32.5%), while other clinical manifestations, disease duration, or types of medications were not different in both groups.
The current study data demonstrated a statistically negative correlation between each of ESR and SLEADI score with Na level (r - 0.542 and −0.697, respectively) (p=0.001), while the Na level was positively correlated with C3, C4, Cl, and albumin levels (r=0.586, 0.555, 0. 417, and 0.508, respectively) with a statistical significance as shown in Table 3. Sodium level was found to be not correlated to the CRP level.
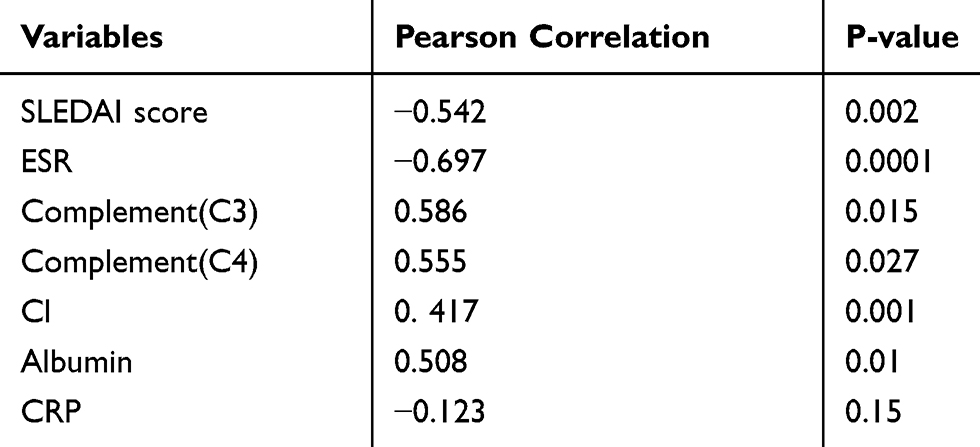 |
Table 3 Correlations Between Sodium Level and Other Variables |
Multiple logistic regression test yielded that ESR is the only parameter that could be an independent risk factor of hyponatremia with an odds ratio of 1.103% and 95% CI for Exp B of 0.997–0.058 (p-value=0.048).
ROC curve analysis was performed to evaluate the discriminant validity of SLEDAI, ESR, and serum albumin as predictors of hyponatremia in lupus patients. The highest AUC was for ESR (0.744) at a criterion of 35 with 100% sensitivity and 90% specificity, while SLEADI, albumin, and CRP showed fair performance in hyponatremia prediction (Table 4).
 |
Table 4 ROC Analyses of Prediction of Hyponatremia in Lupus Patients Based on Our Study Data |
Discussion
The current work hypothesized that low serum sodium level could be a determinant of lupus inflammatory activity. Hence, the aim of the study design was to evaluate the prevalence of hyponatremia and its clinical significance among lupus patients.
In the current study, the mean age of participants was 33±8. In addition, the most frequent presenting manifestations of SLE were musculoskeletal, mucocutaneous, and renal involvement. Hyponatremic patients had consensually lower levels of plasma osmolarity, chloride, and potassium compared to normo-natremic patients.
Hyponatremia in lupus disease could be related to variable factors including medications, namely diuretics, and renal sodium loss due to renal tubular injury through the immune-mediated pathways by the infiltration of interstitium with inflammatory complexes and tubular membrane damage, leading to acute kidney injury (AKI).12 So, patients with tubulointerstitial nephritis proven by renal biopsy were excluded from this study.
Hyponatremia has been widely observed in different inflammatory conditions13 such as pneumonia, tuberculosis, meningitis, and encephalitis. Also, it was reported in a case of Kawasaki.14 However, it is not well addressed in connective tissue diseases.
Although the pathoetiology is not fully understood, there is growing evidence that stimulatory cytokines, notably IL-6 which is produced in the setting of inflammation, augment the central release and peripheral action of vasopressin hormone which in turn stimulates vasopressin receptors in the collecting tubules of kidney acting on aquaporins channels. This results in water retention and dilutional hyponatremia.15–17 Besides, IL-1 and TNF-α have been indicted for hyponatremia as they impair sodium transport at the basolateral membrane of the tubule via dysregulation of epithelial sodium channel and sodium-potassium ATPase mediated by nitric oxide (NO) & prostaglandin E2 (PGE2), leading to the increase of natruresis.18
As regards the inflammatory markers, the present study demonstrated a significant difference between both two groups regarding the CRP level. Moreover, ESR was higher in patients with hyponatremia than those with normo-natremia, while albumin was significantly lower in patients with hyponatremia which might be attributed to the disease activity as a negative phase reactant or proteinuria. In the current study, C3 and C4 were more consumed in patients with hyponatremia. This is consistent with an earlier premier study which was set out on children and adult lupus in two centers; the authors reported that elevated CRP, ESR, and SLEDAI levels as well as decreased serum albumin and C3 concentrations were strongly related to hyponatremia. Furthermore, they estimated IL-6 as a surrogate player of inflammation and detected its higher level in the group of patients with hyponatremia compared to those without hyponatremia.8
Interestingly, in our study, hyponatremia was significantly related to patients manifesting with CNS lupus. This finding is congruous with few case reports on CNS lupus patients (lupus cerebritis and vascular thrombosis) where hyponatremia was attributed to vasopressin overstimulation in this clinical status.5,6,19,20 Also, in the current study, it was found that hyponatremia is related to proteinuria in contrast to the study of Shin et al stating that proteinuria was comparable in hyponatremic and normo-natremic lupus patients.8
However, in the current study, we noticed that other clinical presentations, disease duration, and type of medications did not significantly differ in both groups.
Attempting to correlate hyponatremia with inflammatory markers and disease activity profile, the present study showed a significant inverse correlation between Na level and ESR, a positive correlation between Na concentration and each of C3, C4, and albumin levels as well as SLEDAI score, indicating that low sodium concentration is strongly associated with disease activity and might be used as marker for inflammation in lupus disease. These findings are similar to the results of the aforementioned studies which concluded that hyponatremia in SLE is linked to higher SLE activity.8,9 Yet, our results noted that the CRP level was not significantly correlated with sodium level; this contradicts with what was reported by other studies that considered the association between hyponatremia and CRP in inflammatory conditions in general acute illness through a transient stimulation of vasopressin secretion.19,21 Meanwhile, our study revealed that only ESR was independently a risk factor for hyponatremia; this is inconsistent with the conclusion of EL-Badawy et al who demonstrated that CRP, SLEDAI, and consumed C4 were independent risk factors for hyponatremia.9
Our data showed that steroid intake had no impact on the hyponatremia group. ESR was found to be a better predictor of hyponatremia with good performance at a cut-off value of 35. This finding is matching with a recent study that stated that ESR can predict hyponatremia with best sensitivity (100%) and specificity (80%) but at a lower value (ESR ≥ 17.5).9
In the light of these facts, we speculate the conception that lupus as an inflammatory disease is characterized by enhanced cytokines that may cause hyponatremia and high disease activity.22 This observation may impact the clinical approach of hyponatremia management. Hence, treating the immune-inflammatory cascade aggressively among lupus patients is essential to correct the status of patients appropriately.
The main limitations of our study lie in its cross-sectional nature, the small scale of the participants, and lack of measuring cytokines and urine osmolarity for more affirmative results. We recommend further studies with great focus to investigate hyponatremia-related lupus and establish a better degree of accuracy in this matter.
Conclusions
Hyponatremia could reflect SLE disease activity and might be used as a simple inflammatory marker.
Acknowledgments
The authors thank all the participants in the study.
Disclosure
The authors report no funds and no conflicts of interest in this work.
References
1. Yilmaz-Oner S, Oner C, Dogukan FM, et al. Health-related quality of life assessed by LupusQoL questionnaire and SF-36 in Turkish patients with systemic lupus erythematosus. Clin Rheumatol. 2016;35(3):617–622. doi:10.1007/s10067-015-2930-1
2. Park S, Shin J. Inflammation and hyponatremia: an underrecognized condition? Korean J Pediatr. 2013;56(12):519–522. doi:10.3345/kjp.2013.56.12.519
3. Ohl K, Tenbrock K. Inflammatory cytokines in systemic lupus erythematosus. J Biomed Biotechnol. 2011;16:432595.
4. Joyce E, Glasner P, Ranganathan S, Swiatecka-Urban A. Tubulointerstitial nephritis: diagnosis, treatment, and monitoring. Pediatr Nephrol. 2017;32(4):577–587. doi:10.1007/s00467-016-3394-5
5. Leventhal LJ, Kobrin S, Callegari PE. Systemic lupus erythematosus and the syndrome of inappropriate secretion of antidiuretic hormone. J Rheumatol. 1991;14(5):578–579.
6. Hara H, Hasegawa H, Iwanaga M, et al. A case of the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) associated with lupus erythematosus in the central nervous system. CEN Case Rep. 2013;2:17–22. doi:10.1007/s13730-012-0031-4
7. Swart RM, Hoorn EJ, Betjes MG, Zietse R. Hyponatremia and inflammation: the emerging role of interleukin-6 in osmoregulation. Nephron Physiol. 2011;118(2):45–52. doi:10.1159/000322238
8. Shin J, Park SJ, Suh C-H, et al. Hyponatremia in patients with systemic lupus erythematosus. Sci Rep. 2016;6(1):25566. doi:10.1038/srep25566
9. El-Badawy MA, El-Mahdi AR, El-Sherbiny DA, Bawad SAH. Hyponatremia in systemic lupus erythematosus patients: relation to disease activity and fatigue. The Egyptian Rheumatologist; January 2019, doi:10.1016/j.ejr.2019.01.001.
10. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40:1725. doi:10.1002/art.1780400928
11. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH. Derivation of the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis Rheum. 1992;35(6):630–640. doi:10.1002/(ISSN)1529-0131
12. Kinloch AJ, Chang A, Ko K, et al. Vimentin is a dominant target of in situ humoral immunity in human lupus tubulointerstitial nephritis. Arthritis Rheum. 2014;66(12):3359–3370. doi:10.1002/art.v66.12
13. Hoorn E, Lindemans J, Zietse R. Development of severe hyponatremia in hospitalized patients: treatment-related risk factors and inadequate management. Nephrol Dial Transplant. 2006;21:70–76. doi:10.1093/ndt/gfi082
14. Lim GW, Lee M, Kim HS, Hong YM, Sohn S. Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion in Kawasaki disease. Korean Circ J. 2010;40(10):507. doi:10.4070/kcj.2010.40.10.507
15. Palin K,L, Moreau M, Sauvant J, et al. Interleukin-6 activates arginine vasopressin neurons in the supraoptic nucleus during immune challenge in rats. Am J Physiol Endocrinol Metab. 2009;296:E1289–99. doi:10.1152/ajpendo.90489.2008
16. Mastorakos G, Weber JS, Gunn H, Chrousos GP. Hypothalamic-pituitary-adrenal axis activation and stimulation of systemic vasopressin secretion by recombinant interleukin-6 in humans: potential implications for the syndrome of inappropriate vasopressin secretion. J Clin Endocrinol Metab. 1994;79:934–939. doi:10.1210/jcem.79.4.7962300
17. Papanicolaou DA, Wilder RL, Manolagas SC, Chrousos GP. The pathophysiologic roles of interleukin-6 in human disease. Ann Intern Med. 1998;128(2):127–137. doi:10.7326/0003-4819-128-2-199801150-00009
18. Eisenhut M. Changes in ion transport in inflammatory disease. J Inflamm. 2006;3:1487–1488. doi:10.1186/1476-9255-3-5
19. Park SJ, Oh YS, Choi MJ, Shin JI, Kim KH. Hyponatremia may reflect severe inflammation in children with febrile urinary tract infection. Pediatr Nephrol. 2012;27(12):2261–2267. doi:10.1007/s00467-012-2267-9
20. Elisaf MS, Milionis HJ, Drosos AA. Hyponatremia due to inappropriate secretion of antidiuretic hormone in a patient with systemic lupus erythematosus. Clin Exp Rheumatol. 1999;17(2):223–226.
21. Poddighe D. Common finding of mild hyponatremia in children evaluated at the Emergency Department and its correlation with plasma C-reactive protein values. Minerva Pediatr. 2016;68(3):173–176.
22. Kishimoto T. INTERLEUKIN-6: from basic science to medicine—40 years in immunology. Annu Rev Immunol. 2004;23(1):1–21. doi:10.1146/annurev.immunol.23.021704.115806
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.