Back to Journals » Cancer Management and Research » Volume 17

Hypofractionated Radiotherapy for Prostate Cancer: A Comparative Study of Clinical Outcomes and Dosimetry Between Proton and Photon Therapy
Authors Wu CT, Chen WC, Wu YY, Chen MF ![]()
Received 13 June 2025
Accepted for publication 11 October 2025
Published 30 October 2025 Volume 2025:17 Pages 2589—2599
DOI https://doi.org/10.2147/CMAR.S546959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Chun-Te Wu,1 Wen-Cheng Chen,2 Yao-Yu Wu,3 Miao-Fen Chen3
1Department of Urology, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2Department of Radiation Oncology, Chang Gung Memorial Hospital, Chiayi, Taiwan; 3Department of Radiation Oncology, Chang Gung Memorial Hospital, Taoyuan, Taiwan
Correspondence: Miao-Fen Chen, Department of Radiation Oncology, Chang Gung Memorial Hospital, Taoyuan, Taiwan, Email [email protected]
Background: Hypofractionated radiation therapy (HFRT) is increasingly accepted for prostate cancer. This prospective study compared clinical outcomes, early prostate-specific antigen (PSA) dynamics, and dosimetry between proton and photon HFRT for high-risk prostate cancer.
Methods: A total of 118 patients with high-risk prostate cancer were treated with HFRT (70Gy in 28 fractions) between 2022– 2024, receiving either intensity-modulated proton therapy (IMPT, n = 36) or photon therapy (VMAT, n = 82). All patients received long-term androgen deprivation therapy (ADT). Primary endpoints included biochemical control, PSA nadir at 6 months post-treatment, and genitourinary (GU) and gastrointestinal (GI) toxicities. Dosimetric comparisons were performed in silico.
Results: While biochemical control rates were comparable, a significantly higher proportion of patients receiving proton therapy achieved a PSA nadir < 0.1 ng/mL within 6 months. Proton therapy was associated with reduced GU toxicity compared to photon therapy, based on assessments from both physicians and patients. Dosimetric analysis confirmed that proton therapy provided excellent target coverage with superior organ-at risk (bladder and rectum) sparing. We further identified dosimetric parameter to determine the cuff-off value for GU events. The data revealed the percentage volume of bladder receiving ≥ 90% prescribed dose (V90%) ≥ 11% has the predictive value for the development of grade ≥ 2 genitourinary toxicity.
Conclusion: Two-year biochemical control was comparable between proton- and photon- based HFRT in high-risk prostate cancer. Proton therapy demonstrated improved early PSA kinetics and reduced GU toxicity, supported by favorable dosimetric profiles. The identification of bladder V90% < 11% as a planning constraint may guide treatment optimization. Further studies with longer follow-up are warranted to validate these benefits.
Keywords: prostate cancer, hypofractionated radiotherapy, proton therapy
Introduction
Treatment selection for prostate cancer is influenced by multiple factors, including tumor risk stratification, treatment efficacy, side effect profiles, and patient quality of life.1 For patients with high-risk prostate cancer, radiation therapy (RT) in combination with androgen deprivation therapy (ADT) represents a standard-of-care approach.
In recent years, hypofractionated radiation therapy (HFRT), which delivers larger doses per fraction over a shorter treatment duration, has gained clinical acceptance as an alternative to conventionally fractionated RT (CFRT).2,3 Multiple randomized trials have demonstrated the non-inferiority of HFRT in terms of biochemical control, with potential benefits in patient convenience and healthcare resource utilization. HFRT has been extensively validated in low- and intermediate-risk prostate cancer, but evidence for its application in high-risk patients remains relatively scarce. Given the aggressive nature of high-risk disease, it is particularly pertinent to investigate whether HFRT in this subgroup provides comparable efficacy and safety. Furthermore, the concerns persist regarding its association with increased genitourinary (GU) and gastrointestinal (GI) toxicity.4–7 Prior studies have identified several clinical and dosimetric factors8–11 that may influence the risk of radiation-induced cystitis and proctitis, underscoring the importance of careful treatment planning and dose constraint optimization. The issue regarding GI and GU toxicities associated with HFRT needs further investigation.
Proton therapy (PT) offers a promising advancement due to its distinct physical properties, which allow for superior dose conformality and reduced radiation exposure to surrounding normal tissues.12–14 The role of proton therapy in prostate cancer has been increasingly studied. In low-risk and favorable intermediate-risk disease, both photon-based therapy and proton therapy provide excellent long-term biochemical control. In contrast, high-risk prostate cancer presents a greater challenge. Evidence for HFRT in this group is still evolving, and direct comparisons between proton and photon therapy are limited. Available studies suggest that while both modalities achieve comparable disease control, proton therapy may offer dosimetric advantages in reducing rectum and bladder exposure. However, whether these dosimetric advantages translate into measurable clinical benefits remains under active investigation.
Regarding prostate tumor control, previous studies have suggested that early PSA kinetics have been shown to correlate with long-term outcomes and may serve as an early surrogate marker of treatment efficacy.15–18 In this prospective study, we compared clinical outcomes, toxicity profiles, and dosimetric parameters in patients with high-risk prostate cancer treated with HFRT using either proton or photon therapy. We also evaluated early PSA kinetics and conducted an in silico analysis to quantify the relative dosimetric advantages of PT. These findings may help clarify the clinical value of PT in the context of modern prostate cancer radiotherapy and support evidence-based selection of radiation modalities.
Materials and Methods
Patient Characteristics and Treatment Techniques
This prospective study was approved by the institutional review board of our hospital (No. 202201558B0). This study adhered to strict confidentiality guidelines and in compliance with regulations regarding personal electronic data protection and the Declaration of Helsinki. A total of 118 high-risk prostate cancer patients who received hypofractionated radiotherapy (HFRT) since 2022 were enrolled. Informed consent was obtained from all participants prior to enrollment. All patients received long-term androgen deprivation therapy (ADT), typically 2 years of LHRH analogue monotherapy. HFRT was administered at a dose of 70 Gy in 28 fractions over six weeks. Patients were stratified by treatment modality into either the proton or photon therapy group. Treatment allocation was based on patient preference, not randomization. Photon therapy was delivered using volumetric modulated arc therapy (VMAT), while proton therapy was administered via intensity-modulated proton therapy (IMPT). All patients underwent treatment planning using modern standard-of-care techniques, including computed tomography (CT) simulation and motion management protocols.19 For IMPT, an endorectal balloon was used during simulation and each daily session to ensure consistent rectal positioning.14 Patients were instructed to maintain a comfortably full bladder at the time of simulation and during treatment. Immobilization was achieved in the supine position, and daily cone beam CT (CBCT) imaging was used for image-guided treatment and to monitor anatomical changes. The clinical target volume (CTV) included the prostate and regional high-risk pelvic areas, while the bladder, rectum, bowel, and femoral heads were designated as organs at risk (OARs). Treatment plans were optimized based on CTV coverage, dose homogeneity, and sparing of adjacent normal tissues.
Clinical Assessment
Toxicities were assessed using the Radiation Therapy Oncology Group (RTOG) toxicity scale on a weekly basis during treatment, at 1 month post-treatment, and subsequently at 3-month follow-up visits. Acute toxicities were defined as adverse events occurring within 90 days following the completion of radiotherapy. In addition to toxicity evaluation, each follow-up visit included a serum prostate-specific antigen (PSA) test, as well as the completion of the International Prostate Symptom Score (IPSS) and the Urinary Distress Inventory (UDI-6) questionnaires. Biochemical-clinical failure (BCF) was defined as the earliest occurrence of either clinical failure—including local recurrence, regional recurrence, or distant metastasis—or biochemical failure, according to the Phoenix definition (an increase in PSA ≥ 2 ng/mL above the nadir).
Proton Treatment Planning and In Silico Analysis
A relative biological effectiveness (RBE) value of 1.1 was assumed for proton therapy.10 At our institution, proton therapy was delivered using a cyclotron system (Sumitomo Heavy Industries, Ltd). capable of producing a continuous, high-intensity proton beam. For the in silico dosimetric comparison, CT simulation data from 36 patients in the proton group were retrospectively collected to generate corresponding photon-based plans. Target volumes and OARs were delineated on the CT images. For each patient, two treatment plans were created: one using VMAT and one using IMPT. The prescribed dose for both modalities was 70 Gy (RBE) delivered in 28 fractions.
Statistical Analyses
Student’s t-tests were used to analyze the associations between RT-induced toxicity, dosimetric parameters, and clinical characteristics and to compare the dose distribution between the plans. Dose reduction to the OAR was compared between the VMAT and proton therapy plans. p-values for two-tailed tests with a 95% confidence interval was used. Linear regression analyses were performed using SPSS version 17.0. Receiver operating characteristic (ROC) curves were generated for various dose levels, and the area under the curve (AUC) values were calculated. The volumetric constraint for the optimal dosimetric parameters were obtained through analyzing RT-induced toxicity sensitivity and specificity values.
Results
Clinical Outcomes: Proton vs Photon HFRT
A total of 118 high-risk prostate cancer patients treated with HFRT between 2022 and 2024 were prospectively analyzed, including 82 patients who received VMAT (photon group) and 36 who underwent IMPT (proton group). The 2-year biochemical control rates were comparable between the two groups (90% in the proton group vs 83% in the photon group; p = 0.742) (Figure 1a). Baseline clinical characteristics—including T-stage, PSA at diagnosis, and Gleason score—were similarly distributed between groups (Table 1). Dosimetric analyses demonstrated superior target coverage in the proton group, with a higher proportion of the clinical target volume (CTV) receiving both 95% and 100% of the prescribed dose compared to the photon group (Table 2).
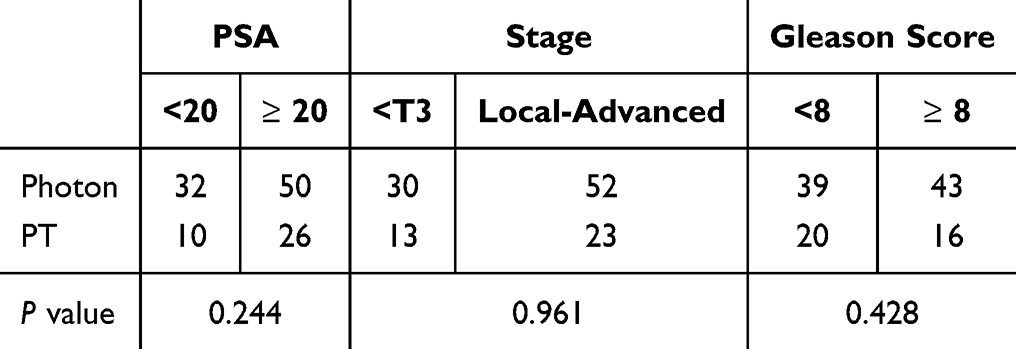 |
Table 1 The Clinical Characteristics of High-Risk Prostate Cancer Patients Treated with HFRT Between the PT and Photon Groups |
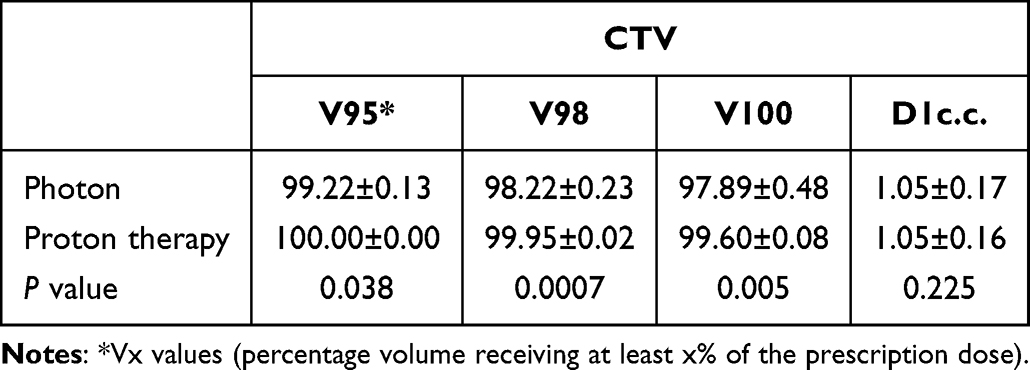 |
Table 2 Dosimetric Comparison of Target Coverage (CTV) Between the PT and Photon Groups |
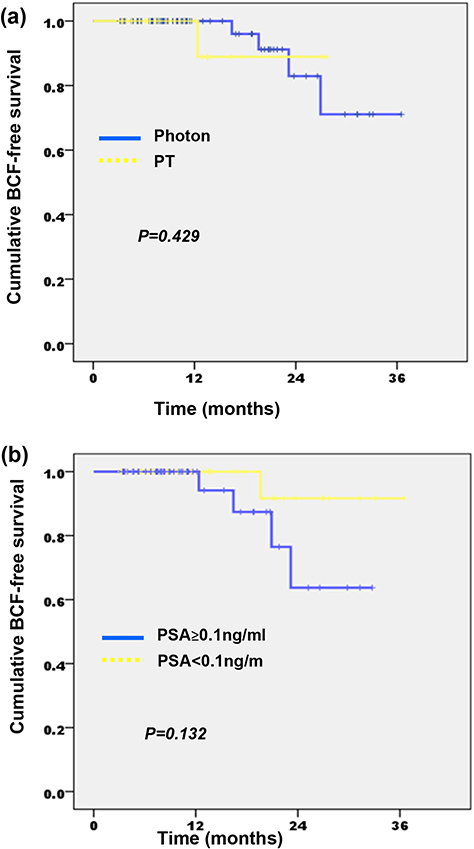 |
Figure 1 Clinical outcomes following HFRT in high-risk prostate cancer. (a) Biochemical control was assessed by plotting BCF-free survival curves, comparing proton therapy to photon-based radiotherapy. (b) Biochemical control was assessed by plotting BCF-free survival curves, comparing PSA nadir<0.1ng/mL to PSA nadir≥0.1ng/mL. |
In this study, PSA levels within six months following treatment were analyzed. Among the patients, 53 (45%) had a nadir PSA level of ≥0.1 ng/mL. Although not statistically significant, patients with a nadir PSA <0.1 ng/mL demonstrated a trend toward improved 2-year biochemical control rates compared to those with higher nadir levels (92% vs 64%, respectively; Figure 1b). Furthermore, a significantly higher proportion of patients in the proton group reached this low PSA threshold (Table 3, P = 0.004). Additionally, baseline PSA levels (≥20 ng/mL vs <20 ng/mL) were significantly associated with early PSA nadir outcomes, suggesting that both treatment modality and initial disease burden influence early biochemical response.
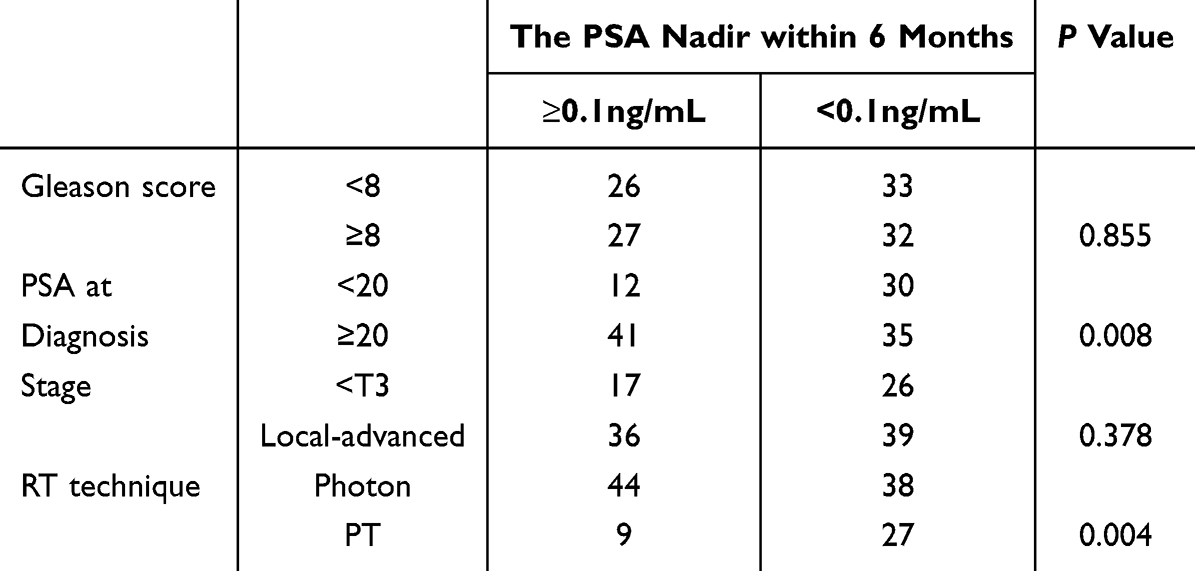 |
Table 3 The Correlation Between the Lowest PSA Value Within 6 months and Clinical Characteristics |
Clinical RT-Induced Toxicity
Patients receiving HFRT with proton therapy experienced significantly lower rates of acute GU toxicity compared to those treated with photon therapy (p = 0.002), while no significant differences were observed in acute gastrointestinal (GI) toxicity (p = 0.06) between the two groups (Figure 2a). To further characterize acute GU toxicity from the patient’s perspective, we analyzed symptom burden using the IPSS and UDI-6 questionnaires at baseline, at the end of radiotherapy, and at 1 and 3 months post-treatment. These validated tools assess urinary symptoms—including nocturia, frequency, and incontinence—with higher scores indicating more severe symptoms. Both groups exhibited a transient increase in urinary symptoms at the end of treatment, which improved by 3 months post-RT (Figure 2b). Notably, the proportion of patients reporting moderate-to-severe urinary symptoms (including nocturia and frequency) was lower in the proton group (p = 0.018). In terms of late toxicity, proton therapy was associated with a significantly reduced incidence of late GU toxicity (p = 0.013), whereas no significant difference was observed for late GI toxicity (p = 0.81) (Figure 2c). Importantly, physician-reported toxicities were consistent with patient-reported outcomes, underscoring the reliability of the findings across assessment methods (Table 4).
 |
Table 4 Concordance Between Physician-Reported GU Toxicities and Patient-Reported Outcomes Following HFRT |
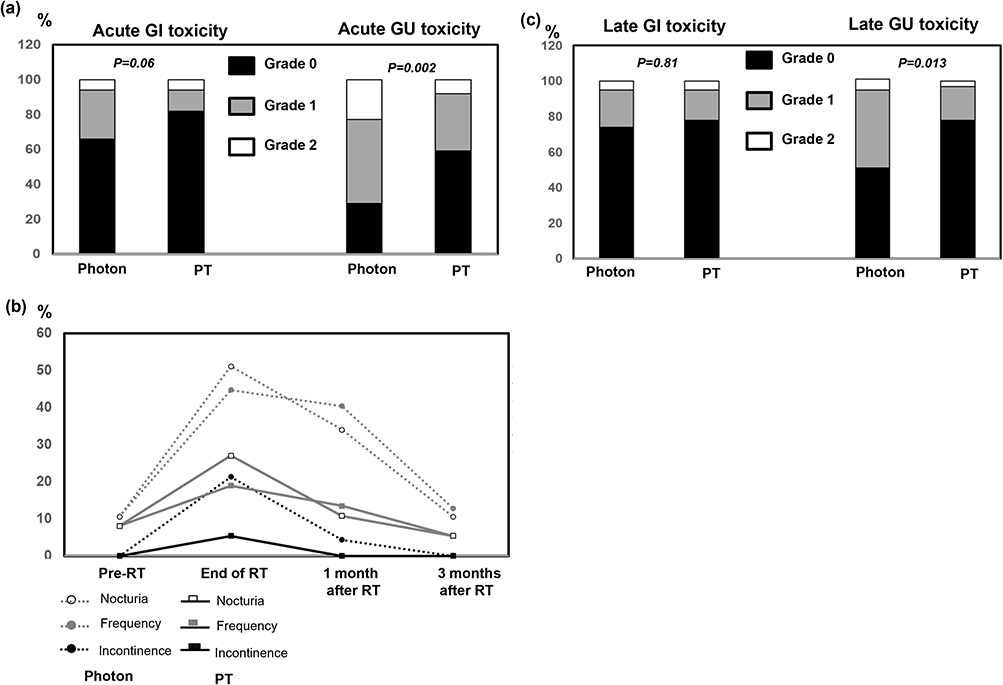 |
Figure 2 Acute and Late Toxicities Following HFRT. (a) Physician-reported acute gastrointestinal (GI) and genitourinary (GU) toxicities were compared between the PT and photon groups. (b) Patient-reported GU symptoms (nocturia, frequency, incontinence) were assessed using validated questionnaires. The severity of symptoms was normalized to baseline levels. (c) Incidence of physician-reported late GI and GU toxicities was compared across modalities. |
Dosimetric Factors Associated with Radiation-Induced GU Toxicity
Previous studies have demonstrated that bladder dose metrics—including total, maximal, mean doses, and specific dose-volume percentages—are closely associated with radiation-induced GU toxicity during pelvic irradiation. In the present analysis, proton therapy significantly reduced bladder volume across the 50%–100% isodose levels, as shown by dose-volume histogram (DVH) comparisons (Figure 3a and b). Univariate analysis identified proton therapy (P=0.043) and a reduction in bladder V50% to V100% (P<0.001) as being significantly associated with a lower incidence of acute grade ≥2 GU toxicity. As shown in Supplementary Table 1 and Supplementary Figure 1, ROC curve analysis further confirmed bladder V90 as a strong predictor of GU toxicity, with an area under the curve (AUC) exceeding 0.80. A V90 threshold of 10.99% was identified as the optimal cutoff for predicting ≥ grade 2 GU toxicity (Table 5). Patients with a bladder V90 <11% experienced significantly lower rates of moderate-to-severe GU symptoms (Table 6). Importantly, patients treated with proton therapy exhibited significantly lower bladder V90 values compared to those receiving photon therapy, supporting the dosimetric advantage of proton therapy in minimizing radiation-induced GU toxicity.
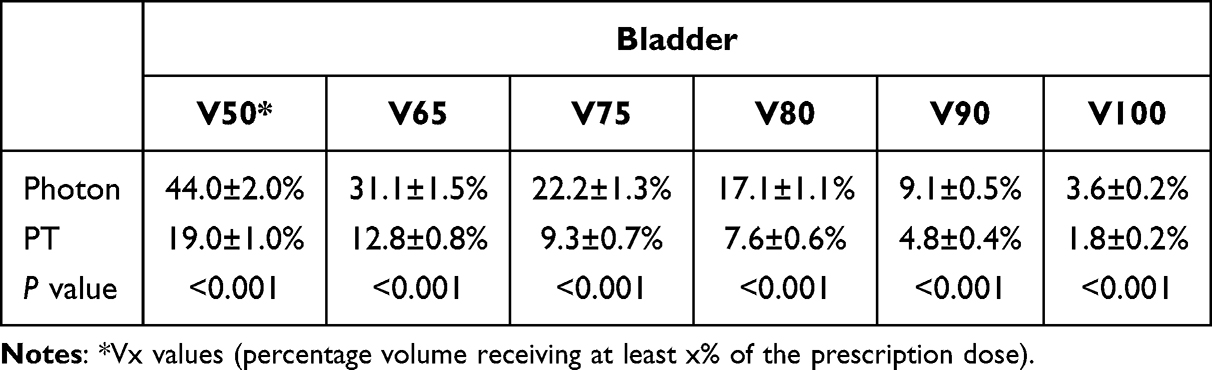 |
Table 5 The Dose Parameter for Bladder for Between Photon and Proton Groups |
 |
Table 6 Correlation Between Bladder V90% Values and Physician- and Patient-Reported ≥ Grade 2 GU Toxicity Incidence |
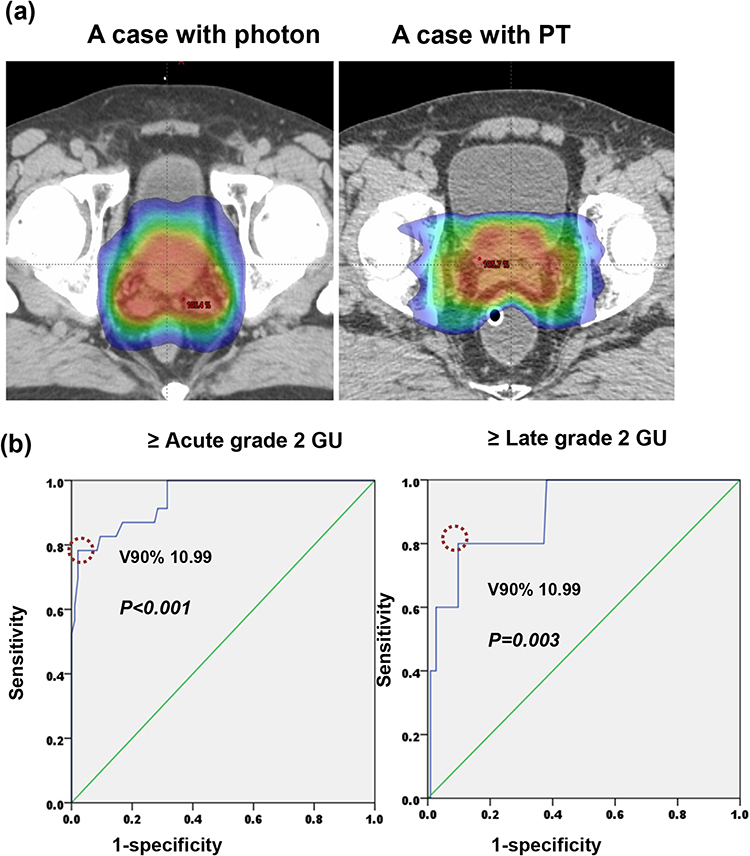 |
Figure 3 Dosimetric Predictors of Radiation-Induced GU Toxicity. (a) Representative isodose distributions from patients treated with photon and proton therapy. (b) The ROC curves analysis. The dotted circle indicates the optimal cutoff value (Bladder V90% =10.99) for predicting ≥ grade 2 acute and late GU toxicity. |
Treatment Plan Comparison by In Silico Analysis
To further assess the dosimetric benefits of proton therapy, an in silico analysis was performed using CT simulation data from 36 patients treated with proton therapy. For each patient, treatment plans were generated for both VMAT and IMPT, utilizing identical target delineations and dose prescriptions. All plans achieved adequate target coverage, with at least 95% of the CTV receiving 100% of the prescribed dose. Compared to photon-based VMAT plans, proton therapy consistently demonstrated superior sparing of OARs, including the bladder, rectum, and penile bulb (Figure 4 and Table 7). These results underscore the dosimetric advantage of proton therapy in reducing radiation exposure to surrounding normal tissues.
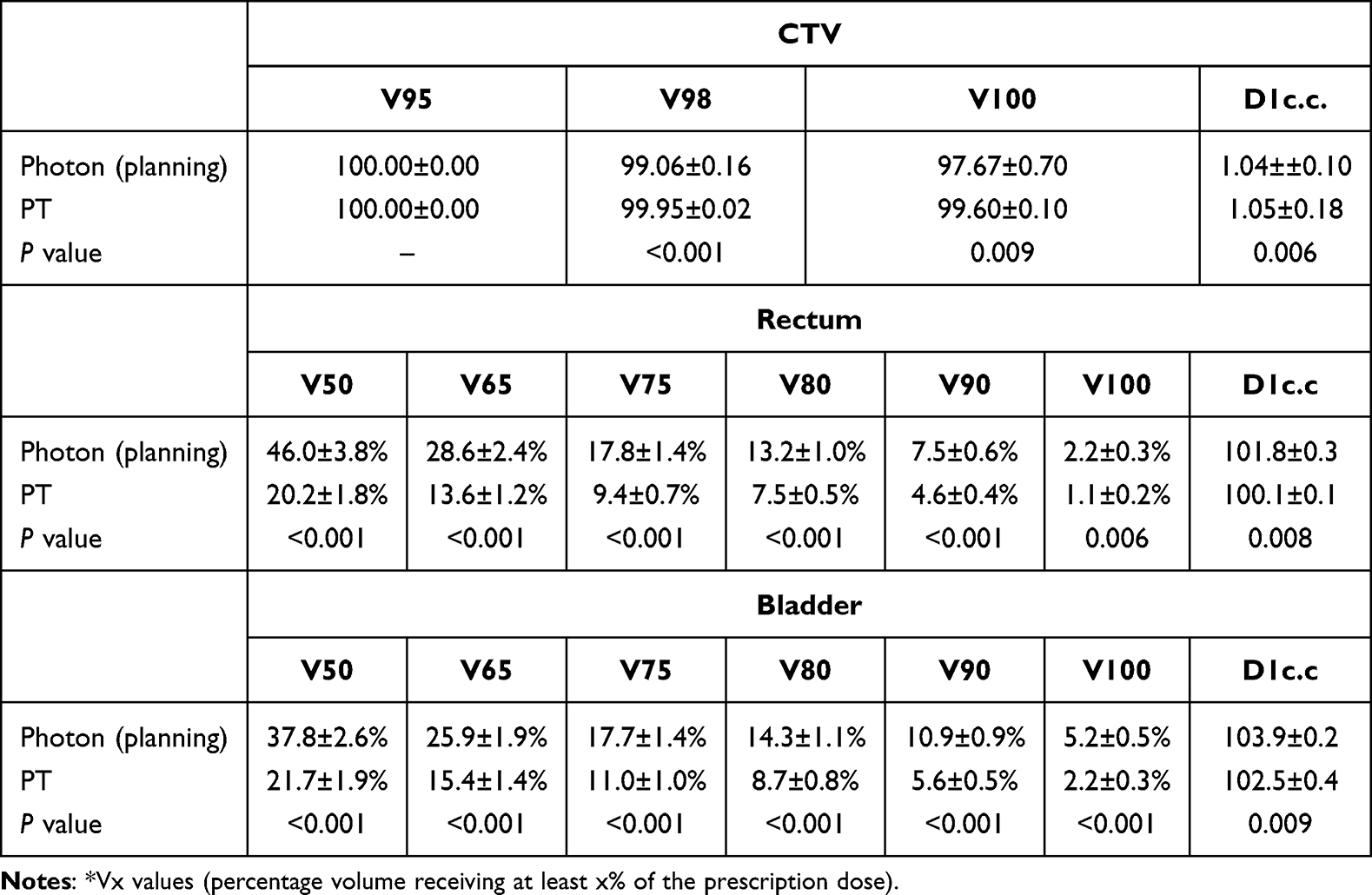 |
Table 7 In Silico Dosimetric Comparison Between VMAT (Photon Planning) and IMPT (Proton) |
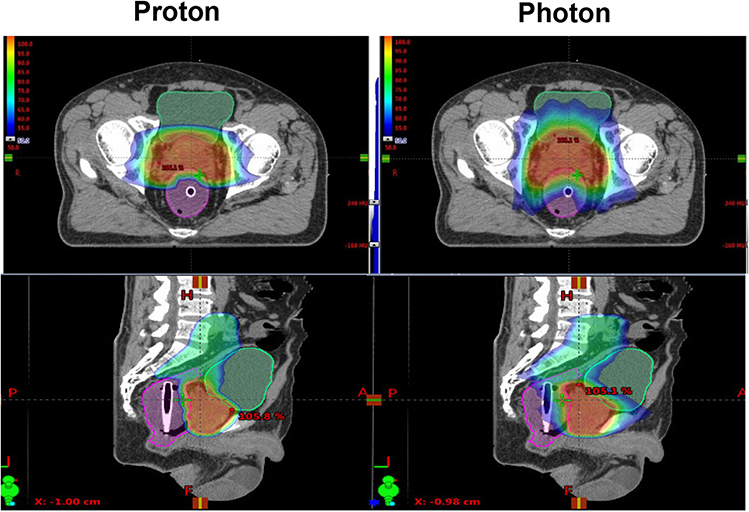 |
Figure 4 In Silico Dosimetric Comparison of Proton and Photon Therapy. Representative isodose distribution from comparative planning (A: anterior; P: posterior; H: head; F: foot; R: right). |
Discussion
The growing adoption of HFRT for prostate cancer is supported by the radiobiological rationale that prostate tumors possess a low α/β ratio, rendering them more sensitive to larger fraction sizes. Multiple randomized trials have validated HFRT as a safe and effective alternative to CFRT, demonstrating comparable tumor control and acceptable toxicity profiles.20–23 However, concerns persist regarding the potential for increased GU and GI toxicity, particularly in high-dose regions.
Proton therapy (PT), owing to its favorable physical properties—including reduced exit dose and improved dose conformality—has been proposed as a strategy to optimize HFRT by enhancing target coverage while minimizing exposure to adjacent normal tissues. While PT has demonstrated dosimetric benefits in a variety of malignancies, including hepatocellular carcinoma, pediatric cancers, and central nervous system tumors,24–26 its clinical utility in prostate cancer remains under investigation. The lack of robust long-term outcome data and the high cost of PT continue to limit its widespread implementation.13,14 In this prospective study, we compared HFRT delivered via photon-based VMAT versus proton-based IMPT in patients with high-risk prostate cancer. Our findings revealed comparable biochemical control between the two groups, with a trend toward improved prostate-specific antigen (PSA) response in the proton cohort. Notably, a significantly higher proportion of patients in the proton group achieved a PSA nadir <0.1 ng/mL within 6 months post-treatment—an early surrogate endpoint that has been associated with improved metastasis-free and cancer-specific survival.15–18 Although PSA at 6 months largely reflects the suppressive effect of ADT, early PSA kinetics remain prognostically informative. Prior studies have demonstrated that early PSA decline is predictive of durable disease control, even in high-risk patients. Moreover, consistent reporting of PSA at 6 months provides a standardized reference point for longitudinal monitoring. Therefore, this favorable PSA kinetics noted in our study may reflect the superior target coverage provided by IMPT, which is particularly critical in high-risk patients requiring dose escalation with strict normal tissue constraints. Future studies with longer follow-up and stratified analyses according to ADT duration are warranted to better isolate the effect of proton therapy.
In terms of toxicity, proton therapy was associated with significantly lower rates of both acute and late GU toxicity compared to photon-based HFRT. This reduction was consistently observed across physician-reported outcomes and patient-reported symptom scores, the latter offering a more patient-centered evaluation of treatment-related morbidity. These findings align with previous comparative studies demonstrating reduced GU toxicity with PT, although variability remains across the literature, likely due to differences in radiation techniques, follow-up durations, and patient selection.27–30
Our dosimetric analysis further substantiates these clinical outcomes. Proton therapy significantly decreased the irradiated volumes of both the bladder and rectum across clinically relevant dose thresholds. Importantly, bladder V90 ≥11% emerged as a significant predictor of ≥ grade 2 GU toxicity, with this threshold validated through receiver operating characteristic (ROC) analysis (AUC ≥0.80). Patients with bladder V90 <11% had significantly lower rates of moderate-to-severe urinary symptoms, highlighting the application of this parameter as a planning constraint in clinical practice.
Interestingly, despite substantial rectal dose sparing achieved with IMPT, we did not observe a corresponding reduction in GI toxicity. This may be due to the low baseline incidence of rectal events or the use of rectal balloons in both groups, which are known to reduce rectal dose independent of radiation modality. Future studies incorporating additional dose-modifying strategies, such as hydrogel spacers, may further mitigate rectal toxicity and warrant investigation.
A key strength of this study is its comparison of IMPT and VMAT for delivering HFRT in a high-risk prostate cancer population. These findings contribute to the growing body of evidence informing modality selection in the management of high-risk prostate cancer.
This study has several limitations. The sample size was relatively small and derived from a single institution, potentially limiting generalizability. Moreover, the median follow-up duration may be insufficient to fully assess long-term oncologic outcomes and late toxicities. Our findings provide prospective evidence supporting the clinical and dosimetric benefits of proton-based HFRT in the management of high-risk prostate cancer. Although the proton group sample size was smaller, the study provides prospective data that could be validated in future larger trial.
Conclusion
In the prospective study of high-risk prostate cancer, HFRT using either photon or proton therapy are effective options when combined with ADT. Proton therapy was associated with reduced GU toxicity and more favorable early PSA kinetics, while GI toxicity outcomes were comparable. The identification of bladder V90% <11% as a predictor of GU toxicity provides a practical dosimetric guideline for clinical planning. Although the sample size of proton cohort was limited, these findings suggest that proton-based HFRT may offer both dosimetric and clinical advantages. Further large-scale, long-term investigations are needed to confirm these benefits.
Data Sharing Statement
Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
Ethics Approval and Consent to Participate
This prospective study was approved by the institutional review board of Chang Gung Memorial Hospital (No. 202201558B0). Informed consent forms were signed by patients prior to their participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was support by National Science and Technology Council, Grant 113-2314-B-182A-137- (to C.T. Wu).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schaeffer EM, Srinivas S, Adra N. et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023;21(10):1067–1096. doi:10.6004/jnccn.2023.0050
2. Langrand-Escure J, de Crevoisier R, Llagostera C, et al. Dose constraints for moderate hypofractionated radiotherapy for prostate cancer: the French genito-urinary group (GETUG) recommendations. Cancer Radiother. 2018;22(2):193–198. doi:10.1016/j.canrad.2017.11.004
3. Lapierre A, Hennequin C, Beneux A, et al. Highly hypofractionated schedules for localized prostate cancer: recommendations of the GETUG radiation oncology group. Crit Rev Oncol Hematol. 2022;173:103661. doi:10.1016/j.critrevonc.2022.103661
4. Catton CN, Lukka H, Gu CS, et al. Randomized Trial of a Hypofractionated Radiation Regimen for the Treatment of Localized Prostate Cancer. J Clin Oncol. 2017;35(17):1884–1890. doi:10.1200/JCO.2016.71.7397
5. Dearnaley D, Syndikus I, Mossop H, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, Phase 3 CHHiP trial. Lancet Oncol. 2016;17(8):1047–1060. doi:10.1016/S1470-2045(16)30102-4
6. Lee WR, Dignam JJ, Amin MB, et al. Randomized Phase III Noninferiority Study Comparing Two Radiotherapy Fractionation Schedules in Patients With Low-Risk Prostate Cancer. J Clin Oncol. 2016;34(20):2325–2332. doi:10.1200/JCO.2016.67.0448
7. Incrocci L, Wortel RC, Alemayehu WG, et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17(8):1061–1069. doi:10.1016/S1470-2045(16)30070-5
8. Zelefsky MJ, Levin EJ, Hunt M, et al. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70(4):1124–1129. doi:10.1016/j.ijrobp.2007.11.044
9. Heemsbergen WD, Peeters ST, Koper PC, Hoogeman MS, Lebesque JV. Acute and late gastrointestinal toxicity after radiotherapy in prostate cancer patients: consequential late damage. Int J Radiat Oncol Biol Phys. 2006;66(1):3–10. doi:10.1016/j.ijrobp.2006.03.055
10. Vargas C, Martinez A, Kestin LL, et al. Dose-volume analysis of predictors for chronic rectal toxicity after treatment of prostate cancer with adaptive image-guided radiotherapy. Int J Radiat Oncol Biol Phys. 2005;62(5):1297–1308. doi:10.1016/j.ijrobp.2004.12.052
11. Michalski JM, Winter K, Purdy JA, et al. Toxicity after three-dimensional radiotherapy for prostate cancer on RTOG 9406 dose Level V. Int J Radiat Oncol Biol Phys. 2005;62(3):706–713. doi:10.1016/j.ijrobp.2004.11.028
12. Royce TJ, Efstathiou JA. Proton therapy for prostate cancer: a review of the rationale, evidence, and current state. Urol Oncol. 2019;37(9):628–636. doi:10.1016/j.urolonc.2018.11.012
13. Poon DMC, Wu S, Ho L, Cheung KY, Yu B. Proton Therapy for Prostate Cancer: challenges and Opportunities. Cancers. 2022;14(4):925. doi:10.3390/cancers14040925
14. Wu YY, Fan KH. Proton therapy for prostate cancer: current state and future perspectives. Br J Radiol. 2022;95(1131):20210670. doi:10.1259/bjr.20210670
15. Bitterman DS, Chen MH, Wu J, et al. Prostate-specific antigen nadir and testosterone level at prostate-specific antigen failure following radiation and androgen suppression therapy for unfavorable-risk prostate cancer and the risk of all-cause and prostate cancer-specific mortality. Cancer. 2021;127(15):2623–2630. doi:10.1002/cncr.33543
16. Naik M, Reddy CA, Stephans KL, et al. Posttreatment Prostate-Specific Antigen 6 Months After Radiation With Androgen Deprivation Therapy Predicts for Distant Metastasis-Free Survival and Prostate Cancer-Specific Mortality. Int J Radiat Oncol Biol Phys. 2016;96(3):617–623. doi:10.1016/j.ijrobp.2016.07.009
17. Hallemeier CL, Zhang P, Pisansky TM, et al. Prostate-Specific Antigen After Neoadjuvant Androgen Suppression in Prostate Cancer Patients Receiving Short-Term Androgen Suppression and External Beam Radiation Therapy: pooled Analysis of Four NRG Oncology Radiation Therapy Oncology Group Randomized Clinical Trials. Int J Radiat Oncol Biol Phys. 2019;104(5):1057–1065. doi:10.1016/j.ijrobp.2019.03.049
18. Kwak L, Ravi P, Armstrong JG, et al. Prognostic Impact of Prostate-Specific Antigen at 6 Months After Radiotherapy in Localized Prostate Cancer: an Individual Patient Data Analysis of Randomized Trials. J Clin Oncol. 2024;42(18):2132–2138. doi:10.1200/JCO.23.00762
19. Bryant CM, Henderson RH, Nichols RC, et al. Consensus Statement on Proton Therapy for Prostate Cancer. Int J Part Ther. 2021;8(2):1–16. doi:10.14338/IJPT-20-00031.1
20. Miralbell R, Roberts SA, Zubizarreta E, Hendry JH. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: alpha/beta = 1.4 (0.9-2.2) Gy. Int J Radiat Oncol Biol Phys. 2012;82(1):e17–24. doi:10.1016/j.ijrobp.2010.10.075
21. Dasu A, Toma-Dasu I. Prostate alpha/beta revisited -- an analysis of clinical results from 14 168 patients. Acta Oncol. 2012;51(8):963–974. doi:10.3109/0284186X.2012.719635
22. Pollack A, Walker G, Horwitz EM, et al. Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer. J Clin Oncol. 2013;31(31):3860–3868. doi:10.1200/JCO.2013.51.1972
23. Francolini G, Detti B, Becherini C, et al. Toxicity after moderately hypofractionated versus conventionally fractionated prostate radiotherapy: a systematic review and meta-analysis of the current literature. Crit Rev Oncol Hematol. 2021;165:103432. doi:10.1016/j.critrevonc.2021.103432
24. Mohan R, Grosshans D. Proton therapy - Present and future. Adv Drug Deliv Rev. 2017;109:26–44. doi:10.1016/j.addr.2016.11.006
25. Sanford NN, Pursley J, Noe B, et al. Protons versus Photons for Unresectable Hepatocellular Carcinoma: liver Decompensation and Overall Survival. Int J Radiat Oncol Biol Phys. 2019;105(1):64–72. doi:10.1016/j.ijrobp.2019.01.076
26. Yock TI, Bhat S, Szymonifka J, et al. Quality of life outcomes in proton and photon treated pediatric brain tumor survivors. Radiother Oncol. 2014;113(1):89–94. doi:10.1016/j.radonc.2014.08.017
27. Fang P, Mick R, Deville C, et al. A case-matched study of toxicity outcomes after proton therapy and intensity-modulated radiation therapy for prostate cancer. Cancer. 2015;121(7):1118–1127. doi:10.1002/cncr.29148
28. Mendenhall NP, Hoppe BS, Nichols RC, et al. Five-year outcomes from 3 prospective trials of image-guided proton therapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2014;88(3):596–602. doi:10.1016/j.ijrobp.2013.11.007
29. Liu YM, Shiau CY, Lee ML, et al. The role and strategy of IMRT in radiotherapy of pelvic tumors: dose escalation and critical organ sparing in prostate cancer. Int J Radiat Oncol Biol Phys. 2007;67(4):1113–1123. doi:10.1016/j.ijrobp.2006.10.009
30. Ojerholm E, Bekelman JE. Finding Value for Protons: the Case of Prostate Cancer? Semin Radiat Oncol. 2018;28(2):131–137. doi:10.1016/j.semradonc.2017.11.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.