Back to Journals » Cancer Management and Research » Volume 14
Hypofractionated Postoperative Radiotherapy in Prostate Cancer with Ialuril Soft Gels®: Toxicity and Efficacy Analysis on a Retrospective Series of 305 Patients
Authors Nicosia L, Vitale C, Cuccia F, Figlia V ![]() , Giaj-Levra N, Mazzola R, Ricchetti F
, Giaj-Levra N, Mazzola R, Ricchetti F ![]() , Rigo M, Ruggieri R, Cavalleri S, Alongi F
, Rigo M, Ruggieri R, Cavalleri S, Alongi F
Received 10 February 2022
Accepted for publication 18 July 2022
Published 20 September 2022 Volume 2022:14 Pages 2839—2846
DOI https://doi.org/10.2147/CMAR.S357814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Luca Nicosia,1 Claudio Vitale,1 Francesco Cuccia,1 Vanessa Figlia,1 Niccolò Giaj-Levra,1 Rosario Mazzola,1 Francesco Ricchetti,1 Michele Rigo,1 Ruggero Ruggieri,1 Stefano Cavalleri,2 Filippo Alongi1,3
1Advanced Radiation Oncology Department, IRCCS Sacro Cuore Don Calabria Hospital, Cancer Care Center, Verona, Negrar, Italy; 2Urology Division, IRCCS Sacro Cuore Don Calabria Hospital, Verona, Negrar, Italy; 3University of Brescia, Brescia, Italy
Correspondence: Luca Nicosia, Advanced Radiation Oncology Department, IRCCS Sacro Cuore Don Calabria Hospital, Cancer Care Center, via Don Sempreboni 5, 37034, Verona, Negrar, Italy, Tel +39 045-6014800, Fax +045-60148071, Email [email protected]
Aim: To evaluate the impact of Ialuril soft Gels® (HA) in reducing acute genito-urinary (GU) toxicity in patients treated with adjuvant or salvage radiotherapy for a prostate cancer relapse.
Material and Methods: The data of 305 patients were retrospectively collected. One hundred and five patients underwent adjuvant radiotherapy (aRT), while 200 a salvage treatment (sRT). GU toxicity was evaluated according to CTCAE v5.0. Every patient received RT combined with HA.
Results: Grade 1– 2 GU toxicity during RT was represented by: urgency (36%), dysuria (23%), increased urinary frequency (12.1%), and urinary retention (11.8%). Nevertheless, the majority of symptoms were present at the baseline. Grade 3 severe toxicity was represented by 10 (3.2%) cases of incontinence and 3 (1%) cases of urgency. The incidence of any-grade RT-related GU toxicity was significantly higher in the aRT group than the salvage group (esRT + sRT) (83.8% versus 64.5%). When comparing the incidence of any-grade RT-related GU toxicity in the aRT, esRT, and sRT groups we observed a significant correlation favoring sRT, over esRT, and aRT.
Conclusion: Postoperative hypofractionated radiotherapy is safe and not correlated with increase of unexpected toxicity when administered with oral hyaluronic acid. A prospective study is necessary to confirm these results.
Keywords: prostate cancer, hyaluronic acid, postoperative radiotherapy, salvage radiotherapy, hypofractionation, toxicity
Introduction
Prostate cancer (PCa) is the first neoplasia in the male population, therefore it has several oncological, psychological and economic issues.1–3 Radical prostatectomy (RP), with or without lymphadenectomy (LAD) according to risk factors is one of the treatments of choice for the localized and locally advanced disease. Despite surgery ensures disease control in the majority of the cases, 17–40% of the patients can experience a relapse, which might be located within the prostate bed.1 Then, patients can be evaluated for postoperative treatment including adjuvant radiotherapy (aRT), when postoperative PSA is not detectable or salvage radiotherapy (sRT) when PSA becomes detectable.2
The results from three randomized Phase III trials (RADICALS, RAVES e GETUG-AFU17) and the meta analysis ARTISTIC showed that a delayed postoperative RT administered in case of biochemical failure, called early salvage RT (esRT), has the same oncological outcome of adjuvant radiotherapy (aRT), with a safer toxicity profile.3–6
The treatment volume of the prostate bed is a virtual volume inside the pelvis, between bladder and rectum and its delineation was recently revised by the francophone group.7 Since the treatment volume includes the bladder neck, genitourinary toxicity might be improved only to a limited extent using advanced RT treatment techniques.8
Given the known radiobiological properties of PCa as a tumor with a low α/β ratio, thus more sensitive to higher doses per fraction,9 the application of hypofractionation in the post-operative setting has been favorably reported in the literature, despite being under-represented when compared to the definitive setting.10,11 Nonetheless, some studies have pointed out some caution when adopting hypofractionated schedules for the post-operative setting, as reported by Cozzarini et al who recorded a higher risk of severe genitourinary toxicity when >2.55 Gy/fx regimens are adopted.12
Therefore, great interest is addressed to the topic of reducing treatment-related toxicities, especially in the case of the bladder and rectum. In the healthy bladder, there is a natural glycosaminoglycan (GAG) barrier that protects the bladder lining from the urine. When this barrier is damaged, urine comes into direct contact with the bladder lining tissue causing damage over time. This can lead to several symptoms, such as pain, urinary urgency and frequency. Ialuril Soft Gels® (HA) contains curcumin, quercetin, hyaluronic acid and chondroitin sulfate able to repair the damage to the GAG layer and restore the bladder’s protective coating, relieving these symptoms.
A previous reported experience with the use of HA showed improved toxicity in the setting of definitive RT.13 On the other hand, the evidence in the postoperative scenario is limited to intravesical hyaluronic acid instillation,14 which requires invasive and repeated procedures. RT-related urinary toxicity is generally higher in the postoperative setting than in the definitive one, since the treatment volume includes the bladder neck; therefore, the possibility to reduce urinary toxicity in a non-invasive way might represent an opportunity for the patients. The study aims to report the urinary toxicity in patients treated with postoperative hypofractionated radiotherapy using Ialuril softGels®.
Materials and Methods
From December 2013 to December 2019, a series of patients receiving post-operative RT was retrospectively reviewed. Ialuril softGels® was orally administered (2 capsules per day from the first day of RT to one month after the end of RT). Pre-treatment evaluation consisted of documented history, postoperative PSA and physical examination, including performance status and digital rectal examination. Eligibility criteria were a) Eastern Cooperative Oncology Group (ECOG) performance status 0–2, b) PCa patients treated with radical prostatectomy, c) pathological stage pT2–4 and pN0-1, d) no detected distant metastases.
Patients received aRT or sRT according to the following risk factors: pathological stage (pT3 or higher), post-operative PSA, Gleason score 8 or higher, and positive surgical margin. Pelvic irradiation was performed according to the following histopathological characteristics: lymph nodal dissection <10 lymph nodes and/or pN1 and/or Gleason score ≥8. aRT was performed in case undetectable post-operative PSA (<0.1 ng/mL), esRT when PSA was ≤0.2 ng/mL, and sRT when PSA was ≥0.2 ng/mL. In the case of detectable post-operative PSA value, pre-treatment staging was performed using metabolic imaging with Choline or PSMA-PET. Androgen deprivation therapy (ADT) was prescribed according to risk factors. The study was conducted in accordance with the principles set forth in the Helsinki Declaration and review by IRCSS Sacro Cuore Don Calabria Internal Ethical Committee. Specific informed consent was not required for retrospective study analysis.
Treatment Procedures
A simulation CT (3 mm slice thickness) without contrast medium was acquired in the supine position and with the arms on the chest with Combifix (Kalona, IA, USA). The clinical target volume (CTV) delineation was performed as follows: the CTV1 was the prostate bed only and included the bladder-urethral anastomosis, the bladder neck, and the retro-bladder space, as defined by EORTC guidelines.15 Patients were requested to have their rectum empty, and to drink 500 mL of water just after having emptied the bladder and 30 min before each treatment session. When available, surgical clips were used to define better the prostate bed. The CTV2 was the pelvis and included the following nodal stations: common iliac, external and internal iliac, obturator, and presacral (above S2-S3). The planning target volume (PTV)1 was obtained from CTV1 by adding 8 mm in all direction and 6 superiorly and posteriorly. The PTV2 was obtained from CTV2 by adding 6–7 mm in all directions. Moreover, the following organs at risk (OARs) were contoured: the rectum, the bladder, the small bowel, the femoral heads, and the penile bulb. Treatment was performed in 30 fractions 5 times per week with a mild hypofractionation schedule as follows: 66 Gy or 67.5 Gy to the prostatic bed in the adjuvant and salvage setting, respectively; 51–52.5 Gy to the pelvic lymph nodes.
The planning endpoint was to cover 95% of each PTV with at least 95% of prescribed dose. Maximum dose <107% was requested for PTV1 only. OAR planning objectives were as follows: for bladder V60 Gy <35%; for rectum V50 Gy <45%, V60 Gy <30%, V65 Gy <20%, Dmax <70 Gy; for femurs (specifically femoral heads) D1cc <50 Gy; for bowels the entirety of the intestinal cavity was outlined, and V20 Gy <40%, Dmean <20 Gy, Dmax <48 Gy.13
RapidArc plans consisted of one or two full arcs using 6-MV photon beams. All dose distributions were calculated with the Anisotropic Analytical Algorithm on an Eclipse treatment planning system (Varian Medical Systems, Palo Alto, USA), setting a dose grid size of 2.5 mm (version 10.0.28). Daily con beam CT (CBCT) before treatment was performed to account for setup errors, and to assess appropriate bladder filling and rectal emptying. In case of inadequate setup, patients repeated pelvic preparation.
Toxicity Assessment, End-Point and Statistics
Baseline toxicity was assessed on the first day of treatment by the treating physician; thereafter, patients were visited weekly to assess toxicity during treatment. In case of severe urinary incontinence 1 month after surgery, postoperative radiotherapy could have been deferred up to 3 months to allow rehabilitation of the pelvic floor. Moreover, patients were encouraged to continue pelvic exercises also during RT. Supportive therapy was modulated in case of 1 degree increase in toxicity compared to the baseline. HA was administered continuously also in case of toxicity increase. The first follow-up was performed 60 days after the end of the RT, and PSA and toxicity were collected. Afterwards, the follow-up was performed every 3 months of the first year, every 6 months in the second and third year and then once a year.
Acute and late toxicities were recorded according to the Common Terminology Criteria for Adverse Events (CTCAE version 5.0), and urinary incontinence was measured with the Pad test measuring the numbers of pads per day both through weekly interview during treatment and at each follow-up after treatment, reported in a specific form and stored internally. More specifically, acute toxicity was defined as any event occurred within 90 days from the RT treatment while late toxicity was defined as any event recorded after this time. Acute and late toxicities were scored in terms of organ-not-specific toxicity (genitourinary and gastrointestinal) and organ-specific toxicity (dysuria, urgency, frequency, incontinence, urinary retention, proctitis, and diarrhea). Acute toxicity was considered as severe for grade ≥3.
Statistical analysis was performed using SPSS version 20.0 software (IBM, Chicago, IL). Additionally, patients were classified into 3 groups for each treatment setting: aRT, esRT, and sRT. Then, a univariate model using a χ2 test (in contingency tables) was performed to associate the previous groups combined (aRT versus esRT + sRT; aRT versus esRT versus sRT) to the overall acute (G0 versus G≥1, and G0 versus G≥3), organ-not-specific acute toxicity, organ-specific acute toxicity, urinary incontinence, and overall late toxicity. Additional univariate analysis included the comparison between baseline toxicity and toxicity during treatment. A p-value ≤0.05 indicated a significant association.
Results
Patients’ Characteristics
Three-hundred and five (305) patients affected by PCa were treated with post-operative hypofractionated RT, associated to HA. The median age was 68 years old (range 47–83). One hundred and five (34.5%) patients were treated with aRT, 77 (25%) with esRT, and 123 (40%) with sRT. Median PSA before RT was 0.03 ng/mL (range, 0–0.09 ng/mL) in the adjuvant setting and 0.385 ng/mL (range, 0.1–13.59 ng/mL) in the sRT group. ADT was administered in 27 (25.5%) aRT patients and in 98 (49.5%) sRT cases. Patients’ characteristics are described in Table 1.
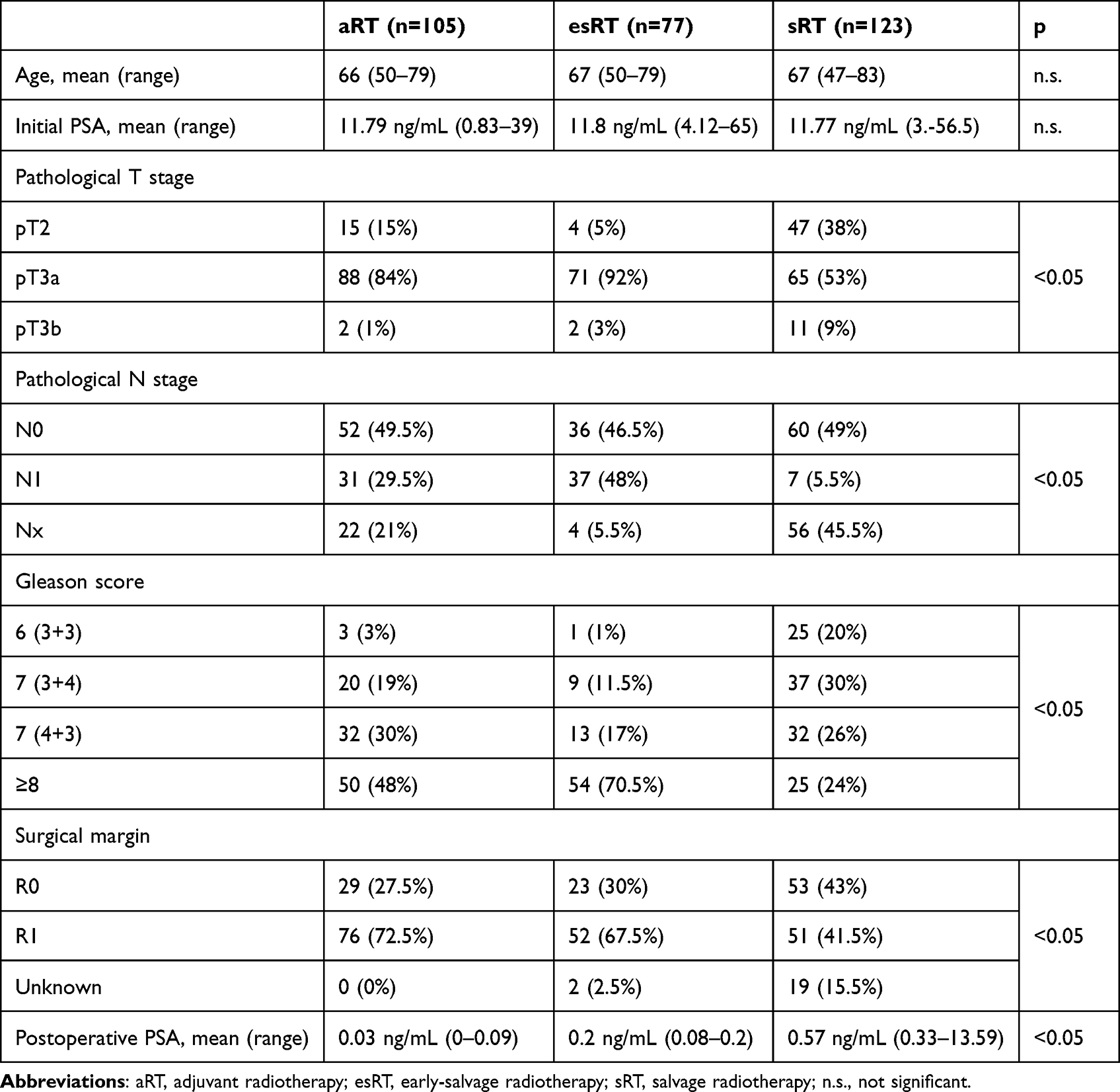 |
Table 1 Patients’ Characteristics (N = 305) |
Baseline Urinary Symptoms
Baseline symptom assessment showed that 197 (65%) patients had GU symptoms. Patients might have one or more symptoms simultaneously. Grade 1–2 GU symptoms at baseline were represented as follows: 163 (53.5%) urinary incontinence, 47 (15.5%) urgency, 30 (10%) increased urinary frequency, 15 (4.5%) urinary retention, and 11 (3.5%) cases of dysuria. Grade 3 GU toxicity before RT was represented by 12 (4%) urinary incontinence and 3 (1%) urgency events. Toxicity is reported in Table 2.
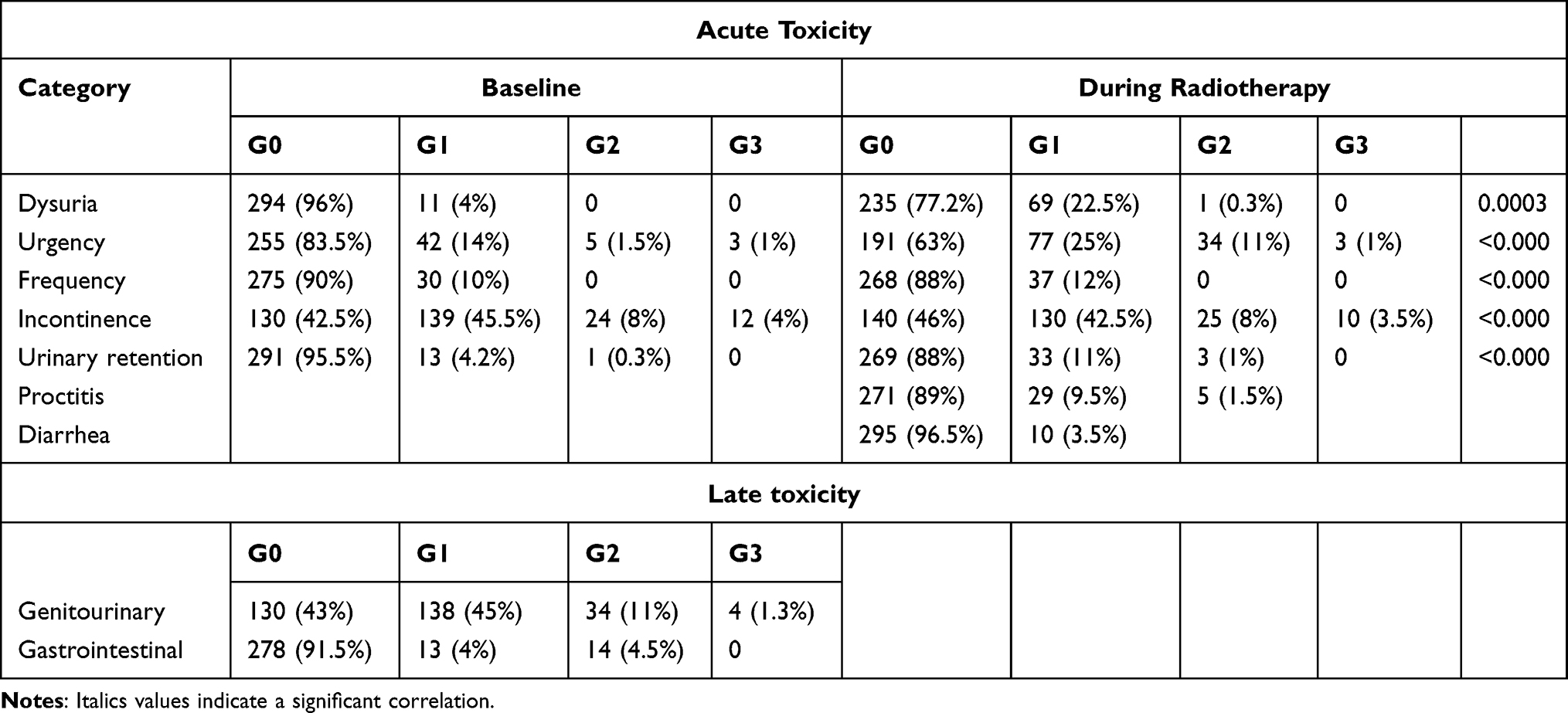 |
Table 2 Acute and Late Toxicity in the Overall Population (N = 305) |
Acute Toxicity During RT
The most common GU side effects were worsening incontinence, urgency and increased urinary frequency. There was an increase in GU symptoms during radiotherapy as compared to the baseline. Globally, grade 1–2 urinary incontinence during RT occurred in 155 (51%) patients, urgency occurred in 111 (36%) patients, dysuria in 70 (23%) cases, increased urinary frequency in 37 (12.1%) cases, and urinary retention in 36 (11.8%) cases. Grade 3 severe toxicity was represented by 10 (3.2%) cases of incontinence and 3 (1%) cases of urgency. The majority of symptoms were present at baseline. Globally, postoperative RT contributed to a modification of grade 1–2 GU toxicity as follows: dysuria + 18.8%, urgency + 20.5%, frequency + 2%, incontinence −3%, urinary retention + 7.5%.
Late Toxicity
Late toxicity was represented by 138 (45%) cases of grade 1 and 34 (11%) cases of grade 2 GU toxicity. Grade 1–2 late proctitis occurred in 27 (8.5%) cases. Severe late toxicity was represented by 4 cases (1.3%) of urinary incontinence. No grade 4 or higher toxicity occurred. Late toxicity is reported in Table 2
Toxicity in the Different Treatment Settings
Globally, the incidence of any-grade RT-related GU toxicity was higher in the aRT group than the salvage group (esRT + sRT) (83.8% versus 64.5%; p = 0.000). The incidence of grade 3 GU toxicity was higher in the aRT group, despite the correlation was at the limit of the statistical significance (6.7% versus 2%; p = 0.052). Interestingly, incontinence was the only GU toxicity significantly different based to treatment setting. The incidence of any-grade incontinence was significantly higher in the aRT group than in the entirety of the salvage group (p = 0.000).
When comparing the incidence of any-grade RT-related GU toxicity in the aRT, esRT, and sRT groups we observed a significant correlation favoring sRT, over esRT, and aRT (p = 0.000) (Table 3). Nevertheless, the correlation was not significant when considering grade 3 toxicity only (p = 0.061). Moreover, a significant correlation was found in the three treatment groups for what concerns urinary incontinence (p = 0.000). The other acute GU symptoms, GI toxicity and late toxicity did not correlate with treatment modality. See results from the univariate analysis in Table 3.
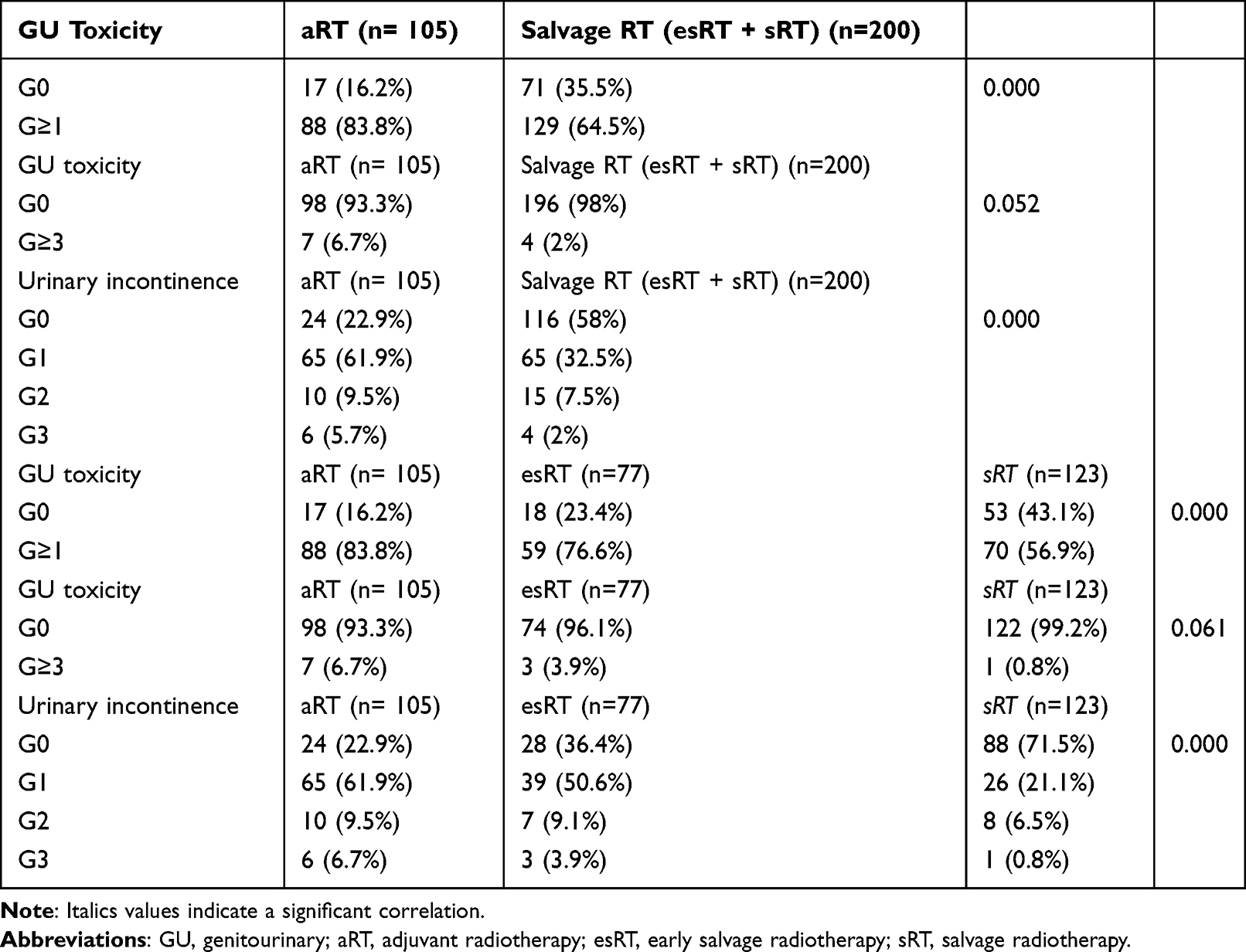 |
Table 3 Univariate Analysis of Toxicity According to Treatment Setting |
Discussion
Post-operative adjuvant RT for PCa is generally performed according to risk factors (pT3, pN1, R+). Alternatively, PSA can be followed over time, and only when it begins to present values >0.2 ng/mL in two consecutive dosages, a salvage RT can be done.16 Some studies have shown that salvage radiotherapy is not inferior to adjuvant radiotherapy in terms of oncological outcomes, and moreover it would seem to ensure lower toxicity.6 Currently, urinary toxicity remains one of the main clinical issue in this scenario, being the bladder neck part of the treatment volume. A recent experience demonstrated no toxicity improvement between 3D conformal radiotherapy and intensity modulated RT, questioning how clinicians can improve the safety of the postoperative treatment.17
Gacci et al14 reported their experience with chondroitin sulfate (CS) and hyaluronic acid (HA) bladder instillation in patients treated with definitive or aRT. They observed that after RT about one-third of patients suffered from cystitis or urinary retention, and HA instillation might significantly improve urinary symptoms. However, intra-vescical therapies are still an invasive procedure and can be troublesome or not accepted by the patient. Therefore, an attempt was made to evaluate the effectiveness of HA replacement no longer invasively, but orally. In a prospective study by Fersino et al,13 HA was evaluated in patients treated with prostate definitive RT. The results showed that the use of HA seems to reduce GU toxicities, especially grade 3.
The results of our study demonstrated limited RT-related toxicity in a post-operative scenario. The majority of the symptoms were present at the baseline and were mainly represented by urinary incontinence and urgency. The incidence of grade 3 urinary incontinence was 4.5%. Our results compare similar to those of the randomized trial RAVES that reported a rate of grade 3 urinary incontinence of 4.8% and 4% in the aRT and esRT group.3
A previous experience with postoperative PCa RT hypofractionation showed a high incidence of severe grade 3–4 late toxicity, especially when a dose per fraction >2.55 Gy is applied.12 In the present study, we used a moderate hypofractionation with 2.2–2.25 Gy per fraction and reported very limited late toxicity events (1.3%). The incidence of GU and GI grade 2 late toxicity were 11% and 4.5%, respectively. Our results are in line with other studies with similar mild hypofractionation. In the study of Barra et al18 the incidence of grade 3 GU toxicity was 3.3%. Similarly, in another study with the use of helical tomotherapy19 the incidence of late GU and GI grade 2 toxicity were 5.3% and 6.6%, respectively. The substantial comparable toxicity pattern of hypofractionated schedules is confirmed also by a retrospective comparison study published by Tandberg et al.20
To the best of our knowledge, the present study is the first to evaluate the use of HA in the PCa postoperative setting. Moreover, it is the first experience assessing the impact of this supportive therapy applied to a hypofractionated post-operative radiotherapy schedule.
Further evidence in terms of toxicity and clinical outcomes will be provided by the ongoing prospective randomized trial NRG GU003. Nonetheless, our series presents several limitations: the study concept is retrospective, however toxicity data collection was performed prospectively through specific internal questionnaire by a dedicated team and at specified time interval during and after treatment. Furthermore, this study lacks a comparison cohort, as a method to better assess the real impact of hyaluronic acid on GU toxicity incidence. Another limitation is the absence of patients’ reported outcome whose use might have contributed to better assess the toxicity.
Conclusion
HA administration might be a useful tool for mitigating the incidence of genitourinary toxicity in patients treated with postoperative radiotherapy. We did not record unacceptable severe toxicity using a mild hypofractionation schedule. A prospective study is however necessary to confirm these data.
Funding
Publication fees has been supported by IBSA Farmaceutici Italia SRL.
Disclosure
The authors declare no conflict of interest.
References
1. Bruni A, Ingrosso G, Trippa F, et al. Macroscopic locoregional relapse from prostate cancer: which role for salvage radiotherapy? Clin Transl Oncol. 2019;21(11):1532–1537. doi:10.1007/s12094-019-02084-0
2. Arcangeli S, Ramella S, De bari B, Franco P, Alongi F, D’Angelillo RM. A cast of shadow on adjuvant radiotherapy for prostate cancer: a critical review based on a methodological perspective. Crit Rev Oncol Hematol. 2016;97:322–327. doi:10.1016/j.critrevonc.2015.09.005
3. Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): a randomised, controlled, Phase 3, non-inferiority trial. Lancet Oncol. 2020;21(10):1331–1340. doi:10.1016/S1470-2045(20)30456-3
4. Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): a randomised, phase 3 trial. Lancet Oncol. 2020;21(10):1341–1352. doi:10.1016/S1470-2045(20)30454-X
5. Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): a randomised, controlled phase 3 trial. Lancet. 2020;396(10260):1413–1421. doi:10.1016/S0140-6736(20)31553-1
6. Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet. 2020;396(10260):1422–1431. doi:10.1016/S0140-6736(20)31952-8
7. Robin S, Jolicoeur M, Palumbo S, et al. Prostate bed delineation guidelines for postoperative radiation therapy: on behalf of the Francophone Group of Urological Radiation Therapy. Int J Radiat Oncol Biol Phys. 2020;109:1243–1253. doi:10.1016/j.ijrobp.2020.11.010
8. Alongi F, Cozzi L, Fogliata A, et al. Hypofractionation with VMAT versus 3DCRT in post-operative patients with prostate cancer. Anticancer Res. 2013;33(10):4537–4543.
9. Dasu A, Toma-Dasu I. Prostate alpha/beta revisited – an analysis of clinical results from 14 168 patients. Acta Oncol. 2012;51(8):963–974. doi:10.3109/0284186X.2012.719635
10. Picardi C, Perret I, Miralbell R, Zilli T. Hypofractionated radiotherapy for prostate cancer in the postoperative setting: what is the evidence so far? Cancer Treat Rev. 2018;62:91–96. doi:10.1016/j.ctrv.2017.11.004
11. Chin S, Fatimilehin A, Walshaw R, et al. Ten-year outcomes of moderately hypofractionated salvage postprostatectomy radiation therapy and external validation of a contemporary multivariable nomogram for biochemical failure. Int J Radiat Oncol Biol Phys. 2020;107(2):288–296. doi:10.1016/j.ijrobp.2020.01.008
12. Cozzarini C, Fiorino C, Deantoni C, et al. Higher-than-expected severe (Grade 3-4) late urinary toxicity after postprostatectomy hypofractionated radiotherapy: a single-institution analysis of 1176 patients. Eur Urol. 2014;66(6):1024–1030. doi:10.1016/j.eururo.2014.06.012
13. Fersino S, Fiorentino A, Giaj Levra N, et al. Impact of Ialuril Soft Gels in reducing urinary toxicity during radical hypofractionated radiotherapy in prostate cancer: a preliminary experience. Minerva Urol Nefrol. 2016;68(1):9–13.
14. Gacci M, Saleh O, Giannessi C, et al. Bladder instillation therapy with hyaluronic acid and chondroitin sulfate improves symptoms of postradiation cystitis: prospective pilot study. Clin Genitourin Cancer. 2016;14(5):444–449. doi:10.1016/j.clgc.2016.01.016
15. Poortmans P, Bossi A, Vandeputte K, et al. Guidelines for target volume definition in post-operative radiotherapy for prostate cancer, on behalf of the EORTC Radiation Oncology Group. Radiother Oncol. 2007;84(2):121–127. doi:10.1016/j.radonc.2007.07.017
16. Francolini G, Timon G, Matrone F, et al. Postoperative radiotherapy after upfront radical prostatectomy: debated issues at a turning point-A survey exploring management trends on behalf of AIRO (Italian Association of Radiotherapy and Clinical Oncology). Clin Transl Oncol. 2021;23(12):2568–2578. doi:10.1007/s12094-021-02665-y
17. Flores-Balcázar CH, Urías-Arce DM, Bourlon MT, et al. Transitioning from conformal radiotherapy to intensity-modulated radiotherapy after radical prostatectomy: clinical benefit, oncologic outcomes and incidence of gastrointestinal and urinary toxicities. Rep Pract Oncol Radiother. 2020;25(4):568–573. doi:10.1016/j.rpor.2020.04.018
18. Barra S, Belgioia L, Marcenaro M, et al. Moderate hypofractionated radiotherapy after prostatectomy for cancer patients: toxicity and clinical outcome. Cancer Manag Res. 2018;10:473–480. doi:10.2147/CMAR.S146131
19. Cuccia F, Mortellaro G, Serretta V, et al. Hypofractionated postoperative helical tomotherapy in prostate cancer: a mono-institutional report of toxicity and clinical outcomes. Cancer Manag Res. 2018;10:5053–5060. doi:10.2147/CMAR.S182016
20. Tandberg DJ, Oyekunle T, Lee WR, Wu Y, Salama JK, Koontz BF. Postoperative radiation therapy for prostate cancer: comparison of conventional versus hypofractionated radiation regimens. Int J Radiat Oncol Biol Phys. 2018;101(2):396–405. doi:10.1016/j.ijrobp.2018.02.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.