")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Hypertension and Its Associated Factors Among Cancer Patients at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: Hospital-Based Cross-Sectional Study
Authors Kibret AK , Aragie H , Belay DG , Molla MD , Teferi ET , Melese EB , Worku YB, Wolde HF , Adugna DG
Received 2 December 2021
Accepted for publication 4 April 2022
Published 14 April 2022 Volume 2022:15 Pages 793—803
DOI https://doi.org/10.2147/JMDH.S352114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anteneh Ayelign Kibret,1 Hailu Aragie,1 Daniel Gashaneh Belay,1,2 Meseret Derbew Molla,3 Ephrem Tafesse Teferi,4 Endalkachew Belayneh Melese,4 Yilkal Belete Worku,4 Haileab Fekadu Wolde,2 Dagnew Getnet Adugna1
1Department of Human Anatomy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Biochemistry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Internal Medicine, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Dagnew Getnet Adugna, Department of Human Anatomy, School of Medicine, College of Medicine and Health Science, University of Gondar, P.O.Box 196, Gondar, Ethiopia, Tel +2510932223887, Email [email protected]
Introduction: Hypertension is the most common comorbidities in adult cancer patients. Although hypertension is a leading cause of cancer-related death and disability, there is no evidence about its prevalence and associated factors among cancer patients in Ethiopia. Therefore, this study aimed to assess the prevalence and associated factors of hypertension among cancer patients.
Methods: Hospital-based cross-sectional study was conducted among cancer patients from January to March 2021. A systematic random sampling technique was performed to select 403 study participants. To collect the data, structured interviewer-administered questionnaires were used. Both bi-variable and multivariable binary logistic regression analyses were used to identify factors associated with hypertension. In the multivariable logistic regression analysis, adjusted odds ratios (AOR) with 95% confidence interval (CI) and P-value of less than 0.05 were used to determine significant factors.
Results: The final result was based on 384 cancer patients. In this study, the prevalence of hypertension among adult cancer patients was 36.2% [95% CI: (31.5, 41.2)]. In the multivariable logistic regression analysis, age greater than 57 years [AOR = 5.0; 95% CI (1.7, 14.9)] and having a family history of hypertension [AOR 10.9; 95% CI (5.5, 21.6)] were found to be significantly associated with hypertension.
Conclusion: The prevalence of hypertension among cancer patients was considerably high. Age > 57 years and family history of hypertension were found to increase the odds of having hypertension among cancer patients. Therefore, it is important to emphasize cancer patients that are at high risk of hypertension and develop preventive strategies to decrease the burden of this disease. There is a need for routine screening for hypertension for those having a positive family history of hypertension and older age, as they have an increased likelihood of developing high blood pressure among cancer patients.
Keywords: hypertension, prevalence, cancer, associated factors, Ethiopia
Introduction
Hypertension (HTN) is defined as a systolic blood pressure (SBP) of ≥140 mmHg and/or a diastolic pressure (DBP) of ≥90 mmHg.1 It is a major public health problem due to its high prevalence and concomitant risks of cardiovascular and renal diseases like heart disease, strokes, and kidney dysfunction. Globally, around 35 million people died due to non-communicable diseases (NCDs), with 80% of deaths occurring in developing countries.2 HTN is predicted to cause the death of 1.75 million people each year, accounting for 12.8% of all deaths in Sub-Saharan Africa.3,4
HTN and cancer are complex, severe, and chronic NCDs. HTN has been associated with an increased likelihood of developing certain malignancies and patients with HTN experienced a high rate of cancer-related mortality.5,6 Cancer is also one of the main causes of morbidity and mortality in the world. In 2018, there were over 18 million new cancer cases and 9.6 million cancer-related mortality worldwide, and these figures are expected to increase in the next two decades.7 As a result, if high blood pressure and/or HTN are linked to an increased risk of cancer, this could have serious public health implications. Many cancers and chemotherapeutic drugs directly or indirectly cause HTN; thus, cancer patients have a higher risk of developing HTN when compared to the general population.8 In the previous years, the survival rate of cancer patients enhanced dramatically. However, toxicities of chemotherapeutic treatment, a high number of aging patients with several comorbid diseases, accompanied by lack of adequate knowledge and risk factors’ treatment, causes an increased incidence of HTN in cancer patients.9 Cardiovascular disease is becoming the second most common cause of morbidity and mortality in cancer patients.9 An increased prevalence of cardiovascular diseases in cancer patients is observed because of the overlapping of risk factors to both cancer and cardiovascular diseases.10
Furthermore, the association between HTN, cancer diseases, and other cardiovascular diseases are multidimensional and they share many common risk factors such as smoking, diabetes mellitus, and obesity.11,12 The co-occurrence of risk factors permits the application of harmonized preventive strategies to many NCDs.13 HTN has been reported as the most common comorbidities in adult cancer patients and the estimated prevalence among cancer patients is particularly higher compared with the general population.14–19 As result, HTN is the foremost modifiable risk factor for the development of cardiovascular diseases, which is quickly emerging as one of the main causes of death and disability in adult cancer patients.5,19 Prior to the administration of chemotherapeutic drugs, HTN prevalence in cancer patients was similar to the general adult population (29%).20,21 However, a higher prevalence is seen after starting certain chemotherapeutic drugs like angiogenesis inhibitors (17–80%), alkylating agents (36–39%), and immunodepressants after stem-cell transplantation (30–80%).22–24 Therefore, many chemotherapeutic drugs have been associated with the development of new-onset HTN or worsening of previously well-controlled HTN because of the direct influences of these drugs on vascular endothelial growth factors, sympathetic function, and renal toxicity.8 The co-occurrence of HTN and cancer is common in adult patients and the prevalence of both diseases is increased with advanced age.14,25,26
In 2020, a systematic and meta-analysis was conducted in Ethiopia and the overall prevalence of HTN in the adult population was 21.81%.27 However, awareness about the management and prevention of HTN is very low in Ethiopia. Previous studies indicated that several factors have been associated with HTN. These include age, obesity, diabetes mellitus, physical inactivity, alcohol use, positive family history of HTN and diabetes mellitus, chat chewing, cigarette smoking, and socioeconomic status.27–30
HTN is becoming a main public health issue in low- and middle-income countries including Ethiopia since it is the main risk factor for coronary heart disease, stroke, heart failure, and end-stage renal disease.21 However, there is no evidence about the prevalence and associated factors of HTN among cancer patients in developing countries, particularly in Ethiopia. Besides, documented data on the prevalence and associated factors of HTN among cancer patients is very crucial for understanding the burden of the diseases, identifying high-risk groups, and developing effective curative and preventive strategies. Therefore, this study aimed to assess the prevalence of HTN and its associated factors among adult cancer patients visiting the oncology unit, in the University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia.
Methods
Study Area and Period
The study was conducted among adult cancer patients visiting the Oncology unit at the University of Gondar Comprehensive Specialized Hospital from January to March 2021. The hospital was founded in 1954 and is located in the Central Gondar Zone of the Amhara National Regional State, which is far around 750 km from Addis Ababa, the capital city of Ethiopia. According to the 2015 population projection of major cities in Ethiopia, the overall population size of Gondar town was around 323,900. Today, Gondar town has 9 public health institutions (one Comprehensive Specialized Hospital and eight Health Centers). University of Gondar Comprehensive Specialized Hospital is a teaching hospital, which serves more than 7.5 million people of the Central Gondar Zone and neighboring regions. This hospital has one Oncology ward. The ward serves more than 1500 cancer patients every year. The oncology unit currently has 15 beds for the treatment of patients with cancer.
Study Design
A hospital-based cross-sectional study was employed.
Population
All adult cancer patients visiting the Oncology unit at the University of Gondar Comprehensive Specialized Hospital were the source population. The study population was all adult cancer patients who visited the Oncology unit at the University of Gondar Comprehensive Specialized Hospital during the study period.
Inclusion and Exclusion Criteria
All adult cancer patients whose age is greater than 18 years and visiting the hospital were included in the study. Critically ill patients who were unable to respond were excluded.
Sample Size Determination and Sampling Procedure
The sample size was calculated using a single population proportion formula by considering the following parameters: confidence level (95%), the margin of error = 5%, and proportion of HTN among adult cancer patients taken as 50% since no previous study in the area. By adding a non-response rate of 5%, the required sample size was 403. A systematic random sampling technique was performed to select study participants. The average number of patients visiting the Oncology unit within the previous three months was calculated and was 630. The sampling interval (K) was calculated by dividing the average number of patients visiting oncology unit per three months by sample size (630/403), which is approximately 2. The 1st respondent was chosen by lottery method. Finally, every other second respondent was selected and interviewed until the required sample size was achieved.
Variables of the Study
The outcome variable for this study was HTN.
Independent Variables
Socio-demographic factors of the participants like age, sex, religion, marital status, occupational status, residence, and income were assessed. Besides, behavioral factors such as alcohol consumption, khat chewing, cigarette smoking, physical inactivity, and use of oil were also assessed. Moreover, cancer-related clinical factors like stage of cancer, types of cancer, site of cancer, metastasis, cancer treatment, and duration of treatment were assessed. Anthropometric characteristics such as weight, height, body mass index (BMI), and waist circumference were measured.
Data Collection Procedure and Tools
The data were collected by interviewing the patients and reviewing their medical records using a structured interviewer-administered questionnaire. Patients were interviewed by four general practitioners working in the oncology department under the supervision of the principal investigator and one oncology specialist doctor. The questionnaire was initially developed in English, and translated into Amharic language by experts, and then back into English by a panel of professionals who are fluent in both languages. Blood pressure (BP) was measured in the left arm using a standard mercury sphygmomanometers BP cuff with participants sitting after resting for at least 5 minutes. Patients were asked if they had consumed any caffeinated product, such as tea or coffee, had a cigarette, or engaged in any high-intensity physical activity 30 minutes before measurement; if they did, their BP was taken after 30 minutes of initial consumption. Three BP measurements were taken in every 5-minute intervals between consecutive measurements. The average systolic and diastolic BP of the three consecutive records was analyzed. HTN was defined as a SBP of ≥130 mmHg or DPB of ≥80 mmHg or previous diagnosis of HTN or the use of antihypertensive medications on regular basis.31 Blood sugar of the patients was measured using CareSenseN glucometer and diabetes mellitus was diagnosed based on WHO guideline which is fasting blood sugar ≥126 mg/dl or random blood sugar ≥200 mg/dl or self-report of the previous diagnosis of diabetes mellitus by physicians or recent use of diabetes medication.32 The participants’ heights were measured in a standing upright position with bare feet. Participants’ weight was also measured using a calibrated weight scale while wearing light clothing. BMI was determined accordingly and was classified as underweight (<18.5 kg/m2), normal (18.5–24.99 kg/m2), overweight (25–29.99 kg/m2), and obese (≥30kg/m2). The waist circumference was measured using flexible plastic tape with light closing at an approximate mid-point between the lower edge of the lowest palpable rib and the top of the iliac crest. A waist circumference of ≥ 80 for females and ≥ 94 for males was considered as high risk.
Data Quality Control
Two-days training were provided for data collectors and supervisors about the content of questionnaires, data collection technique, and measurement procedures. Before data collection, a pretest was done among 5% of the sample size to see the effectiveness of the questionnaire. The principal investigator supervised the data collectors daily, and the collected data were reviewed for completeness, accuracy, and clarity before being entered.
Data Processing and Analysis
Data was entered to Epidata version 4.6 and analyzed by STATA software version 14. Descriptive statistics such as percentages, proportions, mean and standard deviations were calculated for selected variables. The results were presented using tables and text. A chi-square assumption was tested for all categorical explanatory variables. Binary logistic regression analysis was used to examine independent variables associated with HTN. Bi-variable and multivariable logistic regression models were used. Variables with a p-value of less than 0.2 at the bivariable analyses were entered into multivariable logistic regression analysis. In the multivariable logistic regression analysis, adjusted odds ratios (AOR) with 95% confidence interval (CI) and P-value of less than 0.05 were used to determine significant factors. The Hosmer–Lemeshow goodness of fit test was used to check model fitness.
Ethical Considerations
The study protocol was approved by the Ethical Review Board of University of Gondar. Permission letter was taken from the University of Gondar Comprehensive Specialized Hospital, Department of Oncology. Informed consent was obtained from all participants enrolled in the study. Participants’ names and other personal identifiers were not included to maintain confidentiality and the data were password protected. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of Adult Cancer Patients
A total of 384 participants were included in the study with a response rate of 95%. The mean (SD) age of the respondents was (49±13) years. About 56.8% were in between 38 and 57 age groups. Of the total participants, about 51.3% were women, 64.4% were urban dwellers and 64.6% had medium-level income. Regarding marital status, nearly half (49.7%) of participants were married (Table 1).
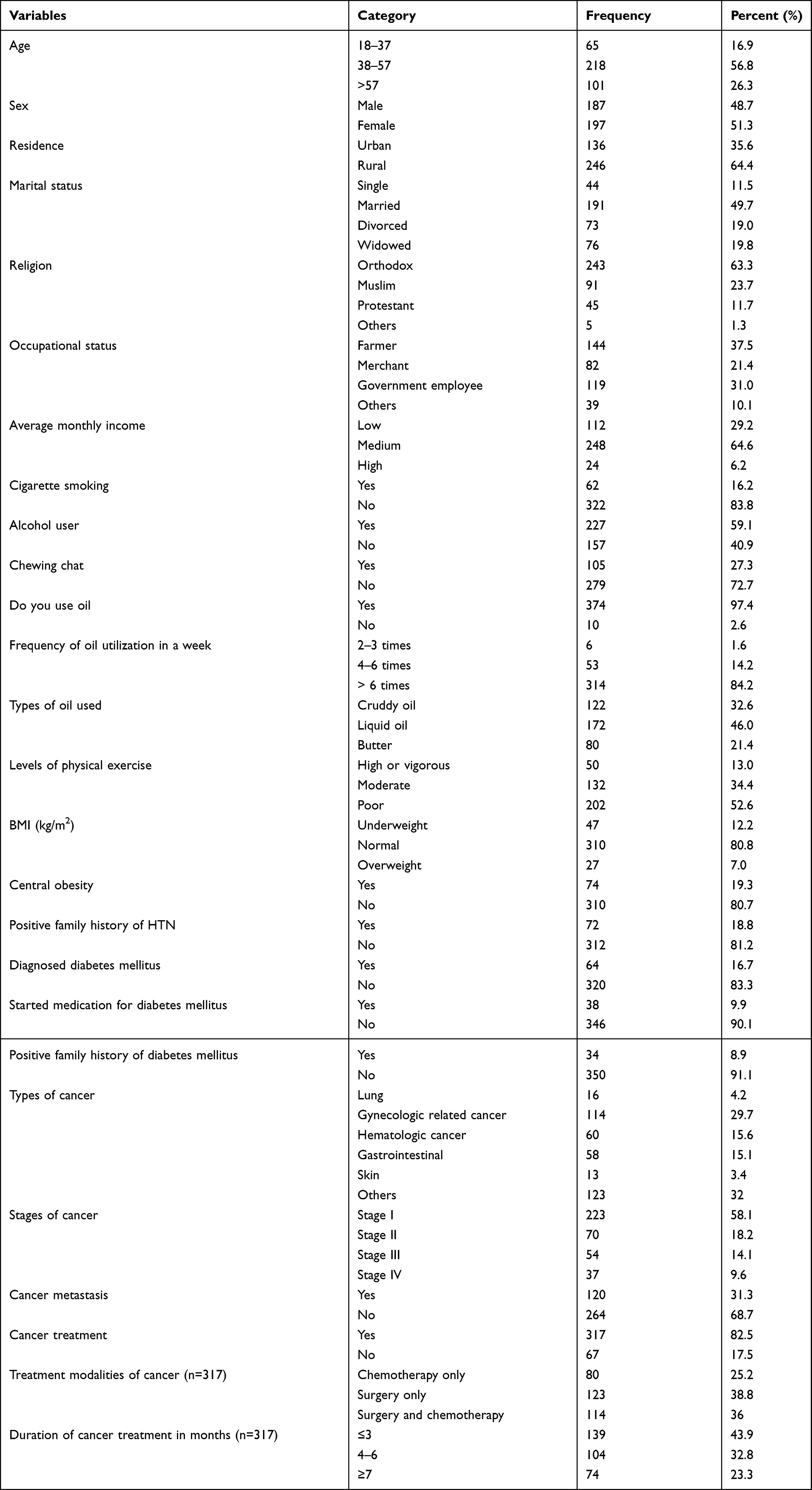 |
Table 1 Socio-Demographic, Behavioral, Dietary, and Cancer-Related Clinical Characteristics of Adult Cancer Patients at Oncology Unit in University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia, 2021 |
Anthropometric Measurements of Study Participants
The mean (±SD) heights of the study participants were 1.6 3 (±0.6) m while the mean (±SD) weights of the study participants were 56.8 (±7) kg. Thus, the mean (SD) BMI of the study participants was 21.2 (±2.5) kg/m2. Moreover, the mean (±SD) waist circumferences of the study participants were 76.5 (±9.9) cm. Regarding central obesity of participants, about 19.3% had central obesity. About 80.7% of participants had normal BMI.
Behavioral and Dietary Characteristics of Study Participants
Of the total study participants, 6.2%, 59.1%, and 27.3% had a habit of smoking, alcohol drinking, and chewing khat, respectively. Regarding oil utilization, majority 97.4% of respondents were oil users. Of this, about 46% were liquid oil consumers. Among all study participants, 18.8% had a family history of HTN, 6.8% had a family history of diabetes mellitus, and 16.7% had diabetes mellitus (Table 1).
Cancer-Related Clinical Characteristics of Study Participants
Of the total cancer patients, about 29.7% were gynecological-related cancers, 58.1% had stage I cancer and 31.1% have metastasis. Concerning the treatment of cancer, 82.5% have already started anti-cancer treatments and of these, 38.8% had undergone surgery (Table 1).
Prevalence of HTN Among Cancer Patients
In this study, the prevalence of HTN among adult cancer patients was 36.2% [95% CI: (31.5, 41.2)]. The frequency of HTN among various types of cancer patients was as follows: lung cancer patients (43.7%), gynecologic-related cancer (38%), gastrointestinal tract cancer (20%), and hematologic cancer (14%). The mean systolic and diastolic BP records were 121.3 (±11 SD) and 74 (±7.5SD) mmHg respectively. Among the total hypertensive patients, 49.64% were taking antihypertensive medications currently. Of all study participants, 17.7% had a previous history of HTN.
Factors Associated with HTN
In the bivariable analysis: age, marital status, alcohol taking, having a positive family history of HTN, family history of diabetes mellitus, presence of diabetes mellitus, presence of metastasis of cancer were significantly associated with HTN. However, other variables such as cigarette smoking, khat chewing, BMI, waist circumference, and cancer treatment did not show any significant association in this study (Table 2).
 |
Table 2 Bivariable Analysis for Factors Associated with HTN Among Adult Cancer Patients at Oncology Unit in University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia, 2021 |
In the multivariable logistic regression analysis, only age greater than 57 years and having a family history of HTN were identified as statistically significant risk factors of HTN.
In this study, age groups of greater than 57 years, proved to have an independently significant association with HTN. Cancer patients in the age group of greater than 57 years were 5 times more likely to develop HTN when compared to those in the age group between 18 and 37 years [AOR = 5.0; 95% CI (1.7,14.9)]. Moreover, having a positive family history of HTN was significantly associated with HTN. Patients who had a family history of HTN were about 10.9 times high likely to be hypertensive than those who have not [AOR 10.9; 95% CI (5.5, 21.6)] (Table 3).
 |
Table 3 Multivariable Analysis for Factors Associated with HTN Among Adult Cancer Patients at Oncology Unit in University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia, 2021 |
Discussion
In Ethiopia, HTN is becoming one of the most common NCDs. It has a significant contribution to a high burden of cardiac diseases.33 This hospital-based study investigated the prevalence of HTN and its associated factors among cancer patients at oncology unit, University of Gondar, Comprehensive Specialized Hospital. Therefore, the overall prevalence of HTN among cancer patients in this study was 36.2% [95% CI: (31.5, 41.2)]. The current finding is similar with previous studies done in Oman (42%),34 Malaysia (34.8%),35 Australia (39%),36 and Poland (37%).37 However, the prevalence of HTN in this study is significantly higher than the prospective cohort study conducted in Iran (13.38%).38 The possible discrepancy for this might be due to the study design, time, areas, and population difference. The proportion of HTN is also much higher than other community-based studies conducted in Ethiopia which reported the prevalence of HTN to be 28.3%,29 22.4%,28 14%,30 and 27.9%.39 The first reason for this discrepancy might be due to the difference in the study population because the study participants in the present study are only adult cancer patients while others are conducted on the general adult population. Secondly, HTN and cancer have many common risk factors such as smoking, diabetes mellitus, obesity, and low physical activity;11,12 hence this could increase the prevalence of HTN among cancer patients. The third possible explanation for the higher prevalence in this study could be due to the use of angiogenesis inhibitors in cancer treatment. Many cancer treatments are highly associated with the development or worsening of HTN; thus, HTN is the most serious complication in cancer patients receiving chemotherapy.21 For instance, angiogenesis inhibitors such as vascular endothelial growth factor signaling pathway inhibitors (bevacizumab) directly block vascular endothelial growth factors from binding to its specific receptors, while small molecule inhibitors of tyrosine kinase (sorafenib and sunitinib) block tyrosine kinases activated by the vascular endothelial growth factors pathway.40 The exact mechanism by which these chemotherapies cause HTN is not fully understood but may be directly related to the inhibition of vascular endothelial growth factors signaling via tyrosine kinase.41 Vascular endothelial growth factor signaling pathway is required for optimal endothelial function and the production of nitric oxide; so its inhibition induces vasoconstriction which in turn causes HTN.10,41
The current finding is lower than the study conducted in Poland with a prevalence of 62%.42 The difference between the current study and the previous study might be due to the difference in study population since the previous study considered only colorectal cancer patients which increase the prevalence of HTN. Epidemiological studies suggested that certain types of cancers such as colorectal cancer have been highly associated with HTN.43,44 Another possible explanation might be due to the presence of age differences between the two study populations. The mean age of study populations in the previous study conducted in Poland was (67 ±11) years,42 leading to a higher prevalence of HTN, while the mean age of study participants in the present study was (49±13) years. This might increase the magnitude of HTN in the previous study. Besides, genetic differences may probably affect the prevalence of HTN.
In our study, cancer patients in the age group of greater than 57 years were found to have increased odds of having elevated BP compared to those in the age group between 18 and 37 years. This is supported by other studies conducted in Ethiopia,28,39,45 and elsewhere.46–48 This could be because of the biological effect of increased vascular resistance due to arterial thickening as one becomes older. As age increases, arterial blood vessels gradually lose some of their elasticity, which can lead to high BP.
Moreover, positive family history of HTN was significantly associated with the development of high BP. Patients who had a family history of HTN were about 10.9 times high likely to be hypertensive than their counterparts. Previous studies indicated that family history of HTN was a risk factor for high BP.28,29,49–51 This could be explained by genetic factors. Blood relatives may share many similar genes which can expose an individual to HTN, cardiac diseases, and stroke.52,53 Furthermore, family members may also share some of the risky lifestyles which could have a contribution to this association.
Previous studies have reported that cigarette smoking was significantly associated with high BP.30,39,54 However, in our study, cigarette smoking has no significant association with high BP. The possible discrepancy of this finding might be due to the low prevalence of this risk factor in cancer patients.
As strength, this study is the first of its kind in Ethiopia. So, it provides the opportunity of evaluating the prevalence of HTN in a rarely studied population (adult cancer patients). The main limitation of the study is the cross-sectional nature of the study design, which may not indicate the cause and effect relationship. In addition, the study did not include some factors such as salt intake, renal function test, and use of contraceptive drugs. Moreover, this study will be a base for future researchers to carry out better study designs such as prospective cohort and experimental studies in this area to bring results with better validity.
Conclusion
In this study, the prevalence of HTN among cancer patients was considerably higher than findings from other countries. Age >57 years old and family history of HTN were found to increase the odds of having HTN among cancer patients. The findings of this study have indicated that HTN is becoming a main public health problem among cancer patients in Ethiopia. Therefore, it is important to emphasize cancer patients that are at high risk of HTN and develop preventive strategies to decrease the burden of this disease. We recommend cancer and HTN clinics should work together to provide comprehensive care, which can improve the treatment outcome and prognosis of these diseases. There is a need for routine screening and monitoring for HTN for those with a positive family history of HTN and older age, as they have an increased likelihood of developing high BP among cancer patients.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; BP, blood pressure; CI, confidence interval; COR, crude odds ratio; DBP, diastolic blood pressure; HTN, hypertension; NCD, non-communicable disease; SBP, systolic blood pressure.
Data Sharing Statements
The data will be available from the corresponding author based on your request with the email address of “[email protected]”.
Acknowledgments
First, we would like to thank the study participants and data collectors. We would also like to acknowledge the University of Gondar for giving us ethical clearance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflicts of interest related to this work.
References
1. Adeniyi OV, Yogeswaran P, Longo-Mbenza B, Ter Goon D. uncontrolled hypertension and its determinants in patients with concomitant Type 2 Diabetes Mellitus (T2DM) in Rural South Africa. PLoS One. 2016;11(3):e0150033. doi:10.1371/journal.pone.0150033
2. Hu B, Liu X, Yin S, Fan H, Feng F, Yuan J. Effects of psychological stress on hypertension in middle-aged Chinese: a cross-sectional study. PLoS One. 2015;10(6):e0129163. doi:10.1371/journal.pone.0129163
3. Addo J, Smeeth L, Leon DA. Hypertension in sub-saharan Africa: a systematic review. Hypertension. 2007;50(6):1012–1018. doi:10.1161/HYPERTENSIONAHA.107.093336
4. Organization WH, Canada PHAo, Canada CPHAo. Preventing Chronic Diseases: A Vital Investment. World Health Organization; 2005.
5. Mohammed T, Singh M, Tiu JG, Kim AS. Etiology and management of hypertension in patients with cancer. Cardio-Oncology. 2021;7(1):1–13. doi:10.1186/s40959-021-00101-2
6. Grossman E, Messerli FH, Boyko V, Goldbourt U. Is there an association between hypertension and cancer mortality? Am J Med. 2002;112(6):479–486. doi:10.1016/S0002-9343(02)01049-5
7. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
8. Cohen JB, Geara AS, Hogan JJ, Townsend RR. Hypertension in cancer patients and survivors: epidemiology, diagnosis, and management. Cardio Oncol. 2019;1(2):238–251.
9. Jemal A, Ward E, Thun M. Declining death rates reflect progress against cancer. PLoS One. 2010;5(3):e9584. doi:10.1371/journal.pone.0009584
10. Rosa LV, Issa JS, Salemi VMC, Younes RN, Kalil Filho R. Epidemiologia das doenças cardiovasculares e neoplasias: quando vai ocorrer o cruzamento das curvas? Rev Soc Cardiol Estado de Säo Paulo. 2009;19:526–534.
11. Kantor AF, Li FP, Janov AJ, Tarbell NJ, Sallan SE. Hypertension in long-term survivors of childhood renal cancers. Am J Clin Oncol. 1989;7(7):912–915. doi:10.1200/JCO.1989.7.7.912
12. Cohen JB. Hypertension in obesity and the impact of weight loss. Curr Cardiol Rep. 2017;19(10):98. doi:10.1007/s11886-017-0912-4
13. de Andrade Martins W, Moço ET-SM. Cardio-oncologia: o preço do envelhecimento. Rev Bras Cardiol. 2012;25:3.
14. Yancik R, Wesley MN, Ries LA, Havlik RJ, Edwards BK, Yates JW. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA. 2001;285(7):885–892. doi:10.1001/jama.285.7.885
15. Fraeman KH, Nordstrom BL, Luo W, Landis SH, Shantakumar S. Incidence of new-onset hypertension in cancer patients: a retrospective cohort study. Int J Hypertens. 2013;2013:379252
16. Ko C, Chaudhry S. The need for a multidisciplinary approach to cancer care. J Surg Res. 2002;105(1):53–57. doi:10.1006/jsre.2002.6449
17. Tammemagi CM, Nerenz D, Neslund-Dudas C, Feldkamp C, Nathanson D. Comorbidity and survival disparities among black and white patients with breast cancer. JAMA. 2005;294(14):1765–1772. doi:10.1001/jama.294.14.1765
18. Piccirillo JF, Tierney RM, Costas I, Grove L, Spitznagel JEL. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA. 2004;291(20):2441–2447. doi:10.1001/jama.291.20.2441
19. Armstrong GT, Oeffinger KC, Chen Y, et al. Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. Am J Clin Oncol. 2013;31(29):3673–3680. doi:10.1200/JCO.2013.49.3205
20. Kalil Filho R, Hajjar LA, Bacal F, et al. Brasileira de cardio-oncologia da Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2011;96(2):01–52. doi:10.1590/S0066-782X2011000700001
21. Izzedine H, Ederhy S, Goldwasser F, et al. Management of hypertension in angiogenesis inhibitor-treated patients. Ann Oncol. 2009;20(5):807–815. doi:10.1093/annonc/mdn713
22. Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356(2):125–134. doi:10.1056/NEJMoa060655
23. Meinardi M, Gietema J, Van der Graaf W, et al. Cardiovascular morbidity in long-term survivors of metastatic testicular cancer. J Clin Oncol. 2000;18(8):1725–1732. doi:10.1200/JCO.2000.18.8.1725
24. Mouhayar E, Salahudeen A. Hypertension in cancer patients. Tex Heart Inst J. 2011;38(3):263.
25. Yancik R, Wesley MN, Ries LA, et al. Comorbidity and age as predictors of risk for early mortality of male and female colon carcinoma patients: a population‐based study. J Am Cancer Soc. 1998;82(11):2123–2134. doi:10.1002/(SICI)1097-0142(19980601)82:11<2123:AID-CNCR6>3.0.CO;2-W
26. Janssen-Heijnen ML, Smulders S, Lemmens V, Smeenk FW, Van Geffen H, Coebergh J. Effect of comorbidity on the treatment and prognosis of elderly patients with non-small cell lung cancer. Thorax. 2004;59(7):602–607. doi:10.1136/thx.2003.018044
27. Tiruneh SA, Bukayaw YA, Yigizaw ST, Angaw DA. Prevalence of hypertension and its determinants in Ethiopia: a systematic review and meta-analysis. PLoS One. 2020;15(12):e0244642. doi:10.1371/journal.pone.0244642
28. Helelo TP, Gelaw YA, Adane AA. Prevalence and associated factors of hypertension among adults in Durame Town, Southern Ethiopia. PLoS One. 2014;9(11):e112790. doi:10.1371/journal.pone.0112790
29. Asresahegn H, Tadesse F, Beyene E. Prevalence and associated factors of hypertension among adults in Ethiopia: a community based cross-sectional study. BMC Res Notes. 2017;10(1):1–8. doi:10.1186/s13104-017-2966-1
30. Haye TB, Tolera Agama B. Prevalence of hypertension and associated factors among the outpatient Department in Akaki Kality Subcity Health Centers, Addis Ababa, Ethiopia. Int J Hypertens. 2020;2020:7960578.
31. Carey RM, Whelton PK, Committee* AAHGW. Prevention, detection, evaluation, and management of high blood pressure in adults: synopsis of the 2017 American College of Cardiology/American Heart Association Hypertension Guideline. Ann Intern Med. 2018;168(5):351–358. doi:10.7326/M17-3203
32. Riley L, Guthold R, Cowan M, et al. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: methods, challenges, and opportunities. Am J Public Health. 2016;106(1):74–78. doi:10.2105/AJPH.2015.302962
33. World Health Organization. The WHO STEPwise approach to chronic disease risk factor surveillance (STEPS) 20 Avenue Appia, 1211, Geneva 27. Switzerland: 2005. Avaiable from: wwwwhoint/chp/steps.
34. Kumar S, Burney IA, Zahid KF, et al. Colorectal cancer patient characteristics, treatment and survival in Oman-a single center study. Pac J Cancer Prev. 2015;16(12):4853–4858. doi:10.7314/APJCP.2015.16.12.4853
35. Othman NH, Zin A. Association of colorectal carcinoma with metabolic diseases; experience with 138 cases from Kelantan, Malaysia. Pac J Cancer Prev. 2008;9(4):747–751.
36. Mahumud RA, Alam K, Dunn J, Gow J. The burden of chronic diseases among Australian cancer patients: evidence from a longitudinal exploration, 2007–2017. PLoS One. 2020;15(2):e0228744. doi:10.1371/journal.pone.0228744
37. Kozłowska K, Kozłowski L, Małyszko J. Hypertension prevalence in early breast cancer patients undergoing primary surgery. Adv Med Sci. 2019;64(1):32–36. doi:10.1016/j.advms.2018.10.003
38. Ahmadi A, Mobasheri M, Hashemi-Nazari SS, Baradaran A, Choobini ZM. Prevalence of hypertension and type 2 diabetes mellitus in patients with colorectal cancer and their median survival time: a cohort study. J Res Med Sci. 2014;19(9):850.
39. Abebe SM, Berhane Y, Worku A, Getachew A. Prevalence and associated factors of hypertension: a crossectional community based study in northwest Ethiopia. PLoS One. 2015;10(4):e0125210. doi:10.1371/journal.pone.0125210
40. Essa H, Dobson R, Wright D, Lip GY. Hypertension management in cardio-oncology. J Hum Hypertens. 2020;34(10):673–681. doi:10.1038/s41371-020-0391-8
41. Suter TM, Ewer MS. Cancer drugs and the heart: importance and management. Eur Heart J. 2013;34(15):1102–1111. doi:10.1093/eurheartj/ehs181
42. Kozłowski L, Kozłowska K, Małyszko J. Hypertension and chronic kidney disease is highly prevalent in elderly patients with colorectal cancer undergoing primary surgery. Adv Clin Exp Med. 2019;28(10):1425–1428. doi:10.17219/acem/104537
43. Christakoudi S, Kakourou A, Markozannes G, et al. Blood pressure and risk of cancer in the European prospective investigation into cancer and nutrition. Inter j Cancer. 2020;146(10):2680–2693. doi:10.1002/ijc.32576
44. Xuan K, Zhao T, Sun C, et al. The association between hypertension and colorectal cancer: a meta-analysis of observational studies. Eur J Cancer Prev. 2021;30(1):84–96. doi:10.1097/CEJ.0000000000000578
45. Kebede B, Ayele G, Haftu D, Gebremichael G. The prevalence and associated factors of hypertension among adults in Southern Ethiopia. Int J Chronic Dis 2020;2020:8020129. doi:10.1155/2020/8020129
46. Mufunda J, Mebrahtu G, Usman A, et al. The prevalence of hypertension and its relationship with obesity: results from a national blood pressure survey in Eritrea. J Hum Hypertens. 2006;20(1):59–65. doi:10.1038/sj.jhh.1001924
47. Olatunbosun ST, Kaufman JS, Cooper RS, Bella AF. Hypertension in a black population: prevalence and biosocial determinants of high blood pressure in a group of urban Nigerians. J Hum Hypertens. 2000;14(4):249–257. doi:10.1038/sj.jhh.1000975
48. Longo-Mbenza B, Nkoy Belila J, Vangu Ngoma D, Mbungu S. Prevalence and risk factors of arterial hypertension among urban Africans in workplace: the obsolete role of body mass index. Niger J Med. 2007;16(1):42–49. doi:10.4314/njm.v16i1.37280
49. Awoke A, Awoke T, Alemu S, Megabiaw B. Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovasc Disord. 2012;12:113. doi:10.1186/1471-2261-12-113
50. Giday A, Tadesse B. Prevalence and determinants of hypertension in rural and urban areas of southern Ethiopia. Ethiop Med J. 2011;49(2):139–147.
51. Gudina EK, Michael Y, Assegid S. Prevalence of hypertension and its risk factors in southwest Ethiopia: a hospital-based cross-sectional survey. Integr Blood Press Control. 2013;6:111–117. doi:10.2147/IBPC.S47298
52. Corvol P, Jeunemaitre X, Charru A, Soubrier F. Can the genetic factors influence the treatment of systemic hypertension? The case of the renin-angiotensin-aldosterone system. Am J Cardiol. 1992;70(12):14d–20d. doi:10.1016/0002-9149(92)90267-3
53. Carmelli D, Robinette D, Fabsitz R. Concordance, discordance and prevalence of hypertension in World War II male veteran twins. J Hypertens. 1994;12(3):323–328. doi:10.1097/00004872-199403000-00015
54. Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. 2010;16(23):2518–2525. doi:10.2174/138161210792062920
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.