Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Hyperkalemia Is an Underestimated Risk Factor in COPD
Authors Mäenpää J, Anderson I, Owen CA, Emerath U, Hughes R, Sultana SR, Olsson M
Received 3 October 2024
Accepted for publication 23 February 2025
Published 15 March 2025 Volume 2025:20 Pages 723—734
DOI https://doi.org/10.2147/COPD.S490620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jukka Mäenpää,1 Isobel Anderson,2 Caroline A Owen,3 Ulrika Emerath,1 Rod Hughes,4 Stefan R Sultana,5 Marita Olsson6
1Chief Medical Office, Research & Development, Patient Safety Biopharma, AstraZeneca, Gothenburg, Sweden; 2Patient Safety Operations, Technology & Analytics, Global Patient Safety, AstraZeneca, Macclesfield, UK; 3BioPharmaceuticals, Early Clinical Development, AstraZeneca, Gaithersburg, MD, USA; 4BioPharmaceuticals Medical, AstraZeneca, Cambridge, UK; 5Cardiovascular Safety Center of Excellence and Safety Knowledge Groups, Global Patient Safety, AstraZeneca, Cambridge, UK; 6BioPharma Late-Stage Development Respiratory & Immunology, Biometrics and Statistical Innovation, AstraZeneca, Gothenburg, Sweden
Correspondence: Jukka Mäenpää, Chief Medical Office, Research & Development, Patient Safety Biopharma, AstraZeneca, Gothenburg, SE-431 83, Sweden, Tel +46-730-715488, Email [email protected]
Background: Hyperkalemia increases mortality in various patient populations. The risk of hyperkalemia in COPD patients is poorly recognized. Hyperkalemia may increase cardiovascular mortality during and soon after COPD exacerbations.
Patients and Methods: A cohort based on two clinical trials comprising 7968 patients with moderate-to-very severe COPD was analysed retrospectively for associations between hyperkalemia and common comorbidities such as chronic kidney disease, diabetes mellitus (DM), or renin-angiotensin-aldosterone system inhibitor use.
Results: Overall, 6.4% of 7968 patients had hyperkalemia (5.3% Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2, 6.8% GOLD 3, and 8.0% GOLD 4). COPD severity was associated with significantly higher hyperkalemia risk in GOLD 3 (odds ratio [OR]=1.28, 95% CI 1.04– 1.58) and GOLD 4 (OR=1.64, 95% CI 1.19– 2.22) versus GOLD 2 patients. Hyperkalemia cases increased with decreasing renal function. Patients with moderate-to-severe renal impairment had > 2-fold increased hyperkalemia risk versus those with normal renal function (OR=2.29, 95% CI 1.71– 3.04). DM was associated with increased hyperkalemia risk (OR=1.28, 95% CI 1.02– 1.59). Angiotensin-converting-enzyme inhibitor (ACEi) use increased hyperkalemia risk (OR=1.25, 95% CI 1.02– 1.53). Unexpectedly, the association between hyperkalemia and renin-angiotensin-aldosterone system inhibitor use was statistically significant only in the normal renal function group (OR=1.63, 95% CI 1.13– 2.34).
Conclusion: Hyperkalemia risk is higher in severe and very severe COPD patients than patients with moderate COPD. Hyperkalemia was also associated with decreasing kidney function, DM, and ACEi use. Serum potassium levels should be monitored regularly in patients with COPD, particularly those with GOLD-3 and 4.
Keywords: cardiac arrhythmias, chronic kidney disease, angiotensin-converting-enzyme inhibitor, renin-angiotensin-aldosterone system inhibitors, serum bicarbonates
Introduction
Hyperkalemia (serum potassium ≥5.0 mmol/L) is associated with an increase in all-cause mortality (Supplementary Figure 1).1,2 Hyperkalemia contributes to mortality by triggering serious cardiac dysrhythmias, cardiac arrest, and sudden cardiac death.1,3 Chronic obstructive pulmonary disease (COPD) also increases the risk of cardiac dysrhythmias especially during acute exacerbations.4,5 Hyperkalemia risk has been extensively studied in common comorbidities of COPD, such as heart failure (HF), diabetes mellitus (DM), and chronic kidney disease (CKD).1 However, the risk of hyperkalemia in moderate to very severe COPD patients is poorly recognised.
In one recent study, comorbid COPD was shown to be a predictor of hyperkalemia in patients with heart failure (HF).6 Additionally, a study of 1747 patients (combining data from several clinical trials) showed that ~7% of patients with COPD had hyperkalemia.7 It is not known whether the severity of COPD may affect the risk of hyperkalemia. Thus, additional studies are warranted to establish the frequency of hyperkalemia in patients with COPD in various GOLD categories and identify subgroups at increased risk of having hyperkalemia.
Hypertension is also a common comorbidity in COPD.8 Many COPD patients take medications to treat hypertension, HF, and other comorbidities. They include renin-angiotensin-aldosterone system inhibitors (RAASis), including angiotensin-converting-enzyme inhibitors (ACEis), which increase the risk of hyperkalemia by attenuating RAAS (Supplementary Figure 2).9 Furthermore, patients with COPD often use medications that may potentiate the pro-arrhythmic effects of hyperkalemia, such as beta-agonists, long-acting anti-cholinergics, and methylxanthines.10
The primary aim of this study was to investigate the frequency of hyperkalemia (as defined by a serum potassium ≥5.5 mmol/l) in COPD patients. Secondary aims were to assess whether known risk factors of hyperkalemia were present/more frequent/elevated in COPD patients with hyperkalemia events, and to determine whether hyperkalemia events were more common in patients with severe (Global Initiative for Chronic Obstructive Lung Disease; GOLD 3) and/or very severe (GOLD 4) COPD versus moderately severe (GOLD 2) disease. Two COPD Phase 3 trials (ETHOS and KRONOS) provided data on a cohort of 7968 White patients with moderate-to-severe (GOLD stage 2, 3 and 4) COPD.11,12 Access to patient-level clinical trial data made it possible to study potential hyperkalemia risk factors, some of which are also common comorbidities of COPD.
Methods
Study Designs and Participants
This retrospective cohort study analysed data from two interventional clinical trials in patients with moderate-to-very-severe COPD. ETHOS11 and KRONOS12 were phase 3, randomized, double-blind, parallel-group studies investigating a new triple-therapy combination comprising budesonide, glycopyrrolate, and formoterol. Eligibility criteria of both studies were similar, although ETHOS recruited patients with more severe COPD. Data from these studies were combined into one cohort of 7968 White patients. Other race groups were too small to provide representative estimates (Supplementary Table 1). The studies were conducted in accordance with the Declaration of Helsinki.
Assessments
In the current study, a serum potassium ≥5.5 mmol/L was the threshold for hyperkalemia, as this threshold has commonly been used in prior clinical trials13–15 and has been linked to adverse clinical outcomes including a higher mortality rate within 1 day of the measurement with an odd ratio of 10.32 in participants without CKD.14 Furthermore, Goyal et al16 showed in their retrospective trial with over 38000 in-hospital acute myocardial infarction patients that rates of ventricular fibrillation, ventricular flutter or cardiac arrest were increased most significantly in patients having hyperkalemia ≥5.5 mmol/L. We classified hyperkalemia cases as patients having at least one serum potassium value ≥5.5 mmol/L measured at screening or pre-dose at any scheduled visit during the study period. Severe hyperkalemia was considered if serum plasma potassium was ≥6.0 mmol/L.13,14 COPD severity was categorized according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) into moderate (GOLD 2), severe (GOLD 3) or very severe (GOLD 4).10 The clinical trial data on DM did not separate type 1 from type 2. However, considering the age range in both trials was 40–80 years, it is likely that most patients with DM had type 2. Patients with a history of HF had HF of NYHA Class I/II. The estimated glomerular filtration rate (eGFR) was calculated using the CKD-Epidemiology Collaboration equation.17 There were only 25 patients with eGFR<30 mL/min/1.73 m2 and therefore eGFR was analysed by the following three categories;18 eGFR <60 mL/min/1.73 m2 (moderate-to-severe renal impairment), 60–89 mL/min/1.73 m2 (mild renal impairment), and ≥90 mL/min/1.73 m2 (normal or high renal function). Serum bicarbonate levels were measured at the same visits as the potassium value for 99% of the patients and analysed as low (<22 mmol/L), or normal-high (≥22 mmol/L),18,19 since the high (>30 mmol/L) group contained only 143 patients.
Concomitant Medications
Concomitant drugs (defined as drugs taken at randomization or prescribed during the trial) of special interest in our study were RAASis, including ACEis, angiotensin II receptor blockers (ARBs), and mineralocorticoid receptor antagonists (MRAs) (Supplementary Figure 2). In addition, the effect of selective and non-selective beta-blockers on hyperkalemia risk was investigated (Supplementary Table 2).9 Other drugs that may increase serum potassium levels were also explored (Supplementary Table 2).
Statistical Analyses
Associations between hyperkalemia and potential risk factors were assessed as adjusted odds ratios (ORs) with 95% CI and estimated using logistic regression models. Risk factors considered were sex, age (<65 and ≥65 years), renal function (eGFR <60, 60–89, and ≥90 mL/min/1.73 m2), COPD severity (GOLD 2, GOLD 3, and GOLD 4), DM, HF history, and concomitant use of RAASis and beta-blockers. In the final model all factors but age (excluded due to co-linearity with eGFR), were included together with a random effect on data source (ETHOS, KRONOS). Adjusted ORs with p-values ≤ 5% were considered statistically significant. For reference, unadjusted ORs were calculated for each potential risk factor.
A subgroup analysis was conducted to investigate whether the association between hyperkalemia and use of RAASis (use of ACEi, ARB or MRA combined), and between hyperkalemia and use of beta-blockers, differed between eGFR categories. Subgroup-specific ORs were estimated from a model including main effects and interaction for drug class and eGFR category, and a random effect on data source. Because of limited size of subgroups, the model was only adjusted for DM. In addition, frequencies of users and non-users by subgroup and by hyperkalemia status were calculated.
Serum bicarbonate levels (<22 or ≥22 mmol/L) were explored as a potential risk factor for hyperkalemia by means of descriptive statistics. Patients with missing serum bicarbonate records (98 patients) were excluded from the analysis.
Analyses used R version 3.5.1.
Supplementary material includes further details on methods.
Results
Study Population
A total of 7968 patients from the ETHOS and KRONOS studies met the criteria for this retrospective analysis (Table 1). The population was evenly distributed between age categories, with 4112 (51.6%) patients aged ≥65 years. DM and mild HF comorbidities were present in 1433 (18.0%) and 245 (3.1%) of 7968 patients, respectively. Overall, 3542 (45.5%) of 7968 patients were on at least one ACEi, ARB, or MRA medication: 2220 (27.9%), 1338 (16.8%), and 181 (2.3%) of 71968 patients, respectively. The percentage of patients without comorbidities was similar over the COPD severity categories; 43% in GOLD 2, 46% in GOLD 3, and 51% in GOLD 4 (Figure 1).
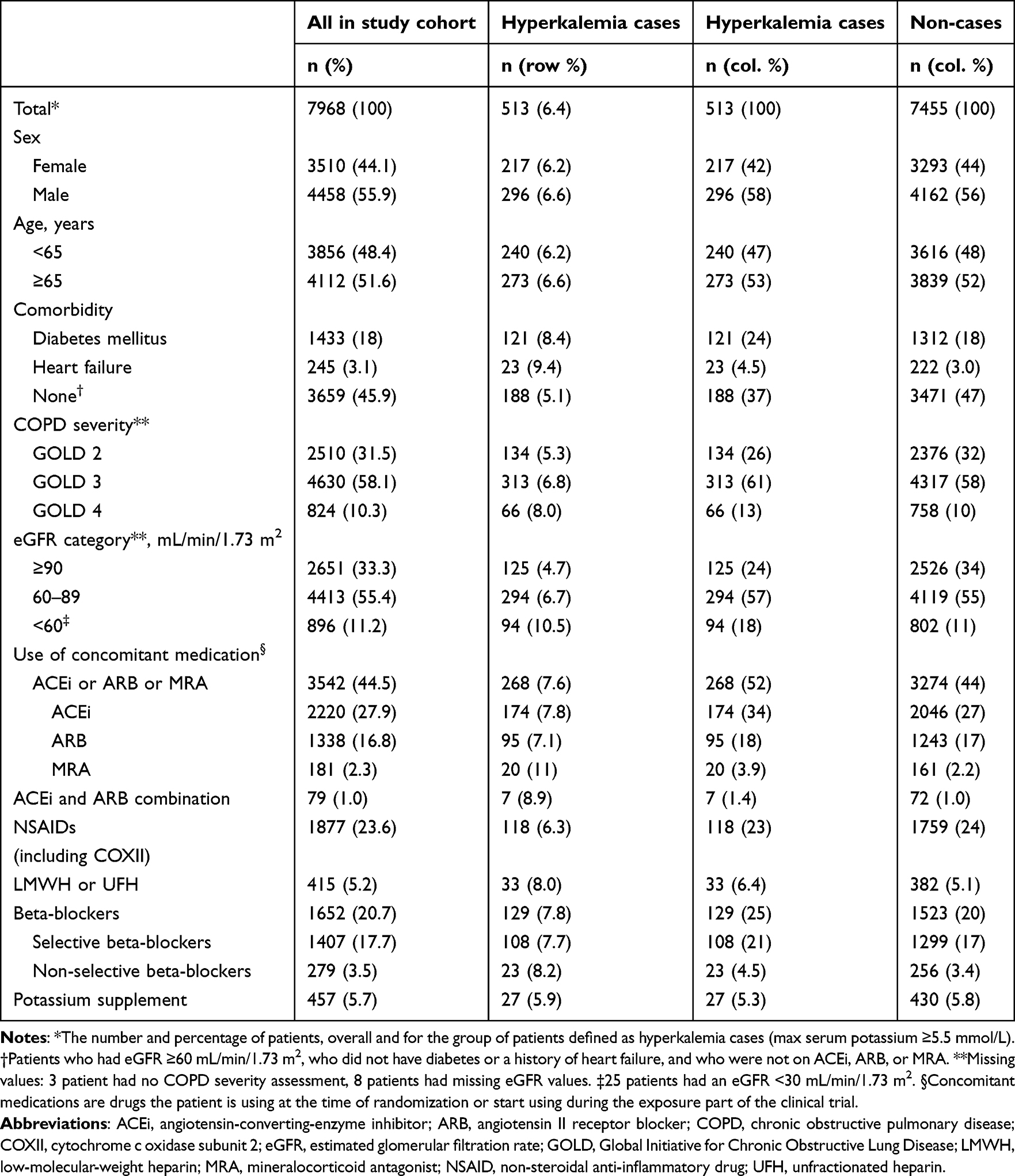 |
Table 1 Patient Demographics, Clinical Characteristics, and Concomitant Medications |
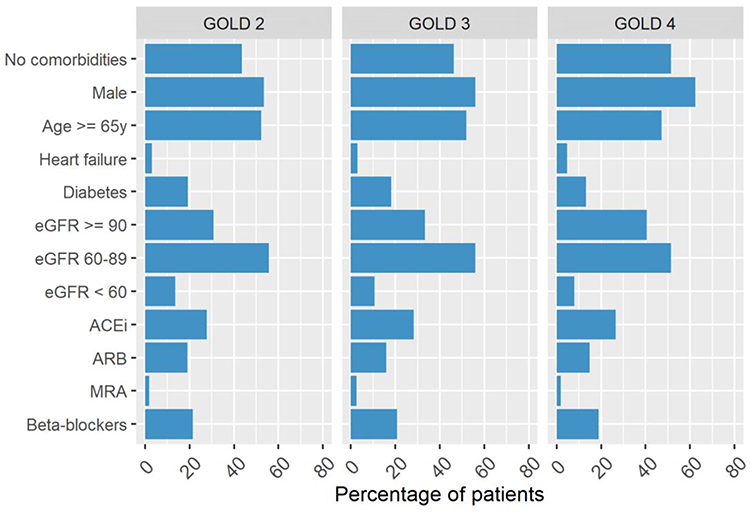 |
Figure 1 Distribution of risk factors over COPD severity categories. Bars represent the percentage of patients within the COPD severity subgroup who have the risk factor / are on drug. Abbreviations: ACEi, angiotensin-converting-enzyme inhibitor; ARB, angiotensin receptor blocker; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MRA, mineralocorticoid receptor antagonist; y, years. Note: No comorbidity includes those who had eGFR ≥60 mL/min/1.73 m2, were not diagnosed with HF or with diabetes, and did not use ACEs, ARBs, or MRAs. |
Cross tabulation of GOLD-stage COPD and eGFR categories showed a similar distribution of GOLD stages 2–4 COPD within each eGFR category (Figure 1, Figure 2). However, there was a trend of decreasing percentage of patients with GOLD-4 COPD and an increasing percentage of patients with GOLD-2 COPD, with worsening renal function.
 |
Figure 2 Percentage of patients per Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage by estimated glomerular filtration rate (eGFR, in mL/min/1.73 m2) category. Abbreviations: eGFR, estimated glomerular filtration rate (in mL/min/1.73 m2). |
Hyperkalemia was identified in 513 (6.4%) of 7968 patients and in 188 (5.1%) of 3659 patients with no comorbidities (Table 1). Severe hyperkalemia was reported in 52 (0.65%) of patients.
The incidence of hyperkalemia increased with increasing COPD severity, from 134 (5.3%) of 2511 patients with GOLD stage 2 COPD to 66 (8%) of 824 patients with GOLD stage 4 COPD. Severe hyperkalemia was reported most commonly in GOLD 3 patients (0.80%) (Supplementary Table 3).
The percentage of hyperkalemia cases showed a monotonic increase with decreasing renal function, from 125 (4.7%) of 2651 patients with eGFR ≥90 mL/min/1.73 m2 to 94 (10.5%) of 896 patients with eGFR <60 mL/min/1.73 m2. Severe hyperkalemia was reported in 0.41%, 0.52% and 2.0% of patients with normal-to-high renal function, mild renal impairment and moderate-to-severe renal impairment, respectively (Supplementary Table 3).
The incidence of hyperkalemia was generally comparable between patients who used ACEis (174 [7.8%] of 2220) or ARBs (95 [7.1%] of 1338), and slightly higher for MRA users (20 [11.0%] of 181).
Relationship Between Hyperkalemia and Patients With Various COPD Severities (GOLD 2-4)
The increase in hyperkalemia risk for GOLD stages 3 and 4 COPD compared with GOLD stage 2 COPD was 28% (OR 1.28, 95% CI 1.04–1.58) and 64% (OR 1.64, 95% CI 1.19–2.22), respectively (Figure 3).
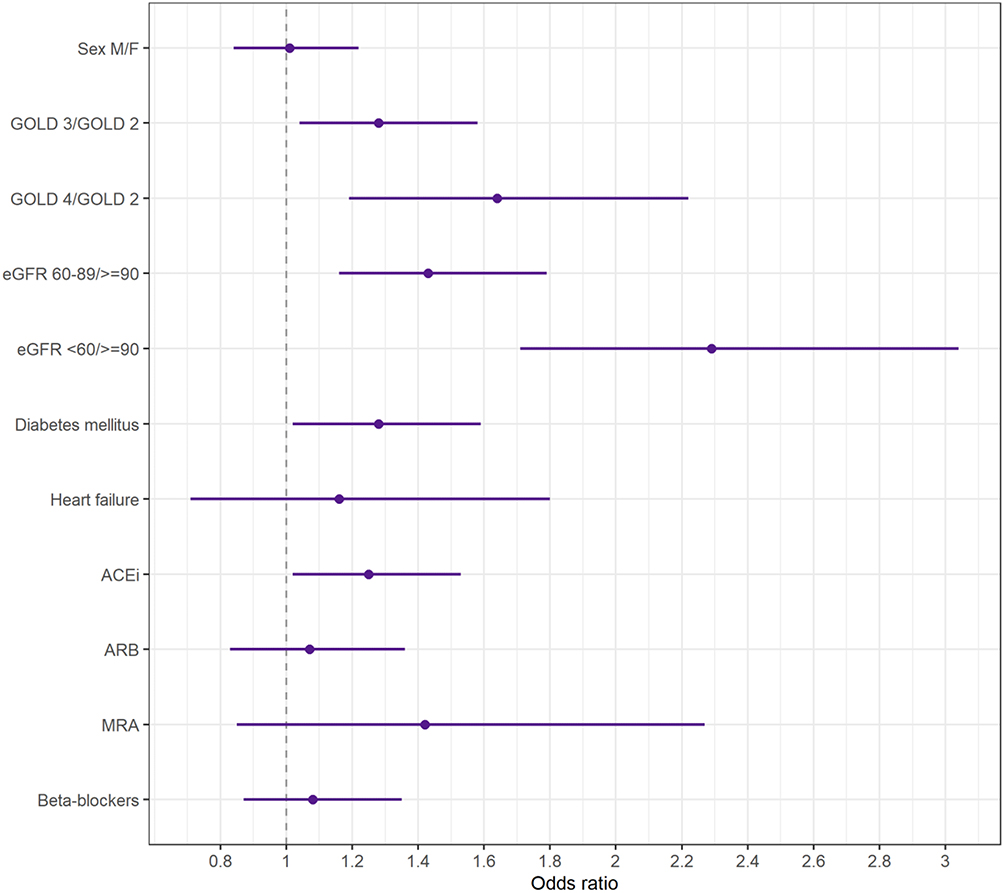 |
Figure 3 Adjusted odds ratio (OR) estimates of association between hyperkalemia and risk factors of main interest. ORs were estimated from a multivariate logistic regression model including all factors in the graph. Bars show 95% confidence intervals. Abbreviations: ACEi, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II receptor blocker; eGFR, estimated glomerular filtration rate (mL/min/1.73 m2); F, female; GOLD, Global Initiative for Chronic Obstructive Lung Disease; M, male: MRA, mineralocorticoid antagonist. |
Relationship Between Hyperkalemia and Other Risk Factors
Statistically significant associations of hyperkalemia with comorbidities were also shown for decreasing renal function and DM diagnosis (Figure 3).
Patients with moderate-to-severe renal impairment (eGFR <60 mL/min/1.73 m2) had a >2-fold increased risk for hyperkalemia compared with those with normal-to-high renal function (eGFR ≥90 mL/min/1.73 m2; OR 2.29, 95% CI 1.71–3.04). Patients with mild renal impairment (eGFR 60–89 mL/min/1.73 m2) had an estimated risk increase of 43% compared with those with normal-to-high renal function (eGFR ≥90 mL/min/1.73 m2; OR 1.43, 95% CI 1.16–1.79).
Patients with DM had 28% higher risk for incidence of hyperkalemia than patients without a diagnosis of DM (OR 1.28, 95% CI 1.02–1.59). The proportion of patients with DM was similar in the GOLD 2 and 3 groups and lower in GOLD 4 (Figure 1). It was not possible to determine or correct for the impact of hyperglycemia or insulin usage on serum potassium levels.
In patients who used ACEis, there was a 25% increased risk of hyperkalemia (OR 1.25, 95% CI 1.02–1.53) (Figure 3, Supplementary Table 4). The proportion of patients using ACEis was similar in all GOLD 2–4 grades (Figure 1). In contrast, ARBs did not increase risk of hyperkalemia. Use of MRAs showed a numerically higher OR of 1.42 (95% CI 0.85–2.27) but was not statistically significant, likely due to the low frequency of use (181 [2.3%] of 7968).
All ORs of association between hyperkalemia and the risk factors included in the main multiple logistic regression analysis are found in Supplementary Table 4. For reference, unadjusted OR estimates based on univariate logistic regression models are shown in Supplementary Table 5.
Risk of Hyperkalemia With Use of RAASi Within eGFR Categories
The association between hyperkalemia and RAASi (ACEi, ARB, or MRA) use was statistically significant in the normal-to-high renal function group (eGFR ≥90 mL/min/1.73 m2; OR 1.63, 95% CI 1.13–2.34) (Figure 4, Supplementary Table 6). In the mild renal impairment group (eGFR 60–89 mL/min/1.73 m2) and the moderate-to-severe renal impairment group (eGFR <60 mL/min/1.73 m2), patients who used RAASis had no increased risk for the incidence of hyperkalemia (OR 1.07, 95% CI 0.84–1.36 and OR 1.19, 95% CI 0.76–1.88, respectively) (Figure 4, Supplementary Table 6).
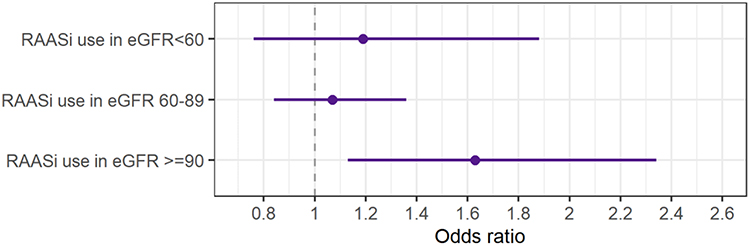 |
Figure 4 Subgroup-specific odds ratio (OR) estimates of association between hyperkalemia and renin-angiotensin-aldosterone system inhibitor (RAASi) use, by estimated glomerular filtration rate (eGFR, in mL/min/1.73 m2) categories. ORs were estimated from a multivariate logistic regression model and adjusted for diabetes mellitus diagnosis. Bars show 95% confidence intervals. |
Additional investigations of the eGFR subgroup results are described in Supplementary Table 7.
Hyperkalemia Incidence Within Serum Bicarbonate Subgroups
About 22% of all COPD patients in the current study had serum bicarbonate levels <22 mmol/L. Evaluation of the percentage of hyperkalemia cases over the GOLD stages showed similar percentage cases (3.6%-4.3%) among patients with low serum bicarbonate levels (<22 mmol/L), while an increasing trend, from 5.9% cases in GOLD 2 to 8.5% cases in GOLD 4, was observed among those with normal-high serum bicarbonate (≥22 mmol/L; Figure 5, Supplementary Table 8).
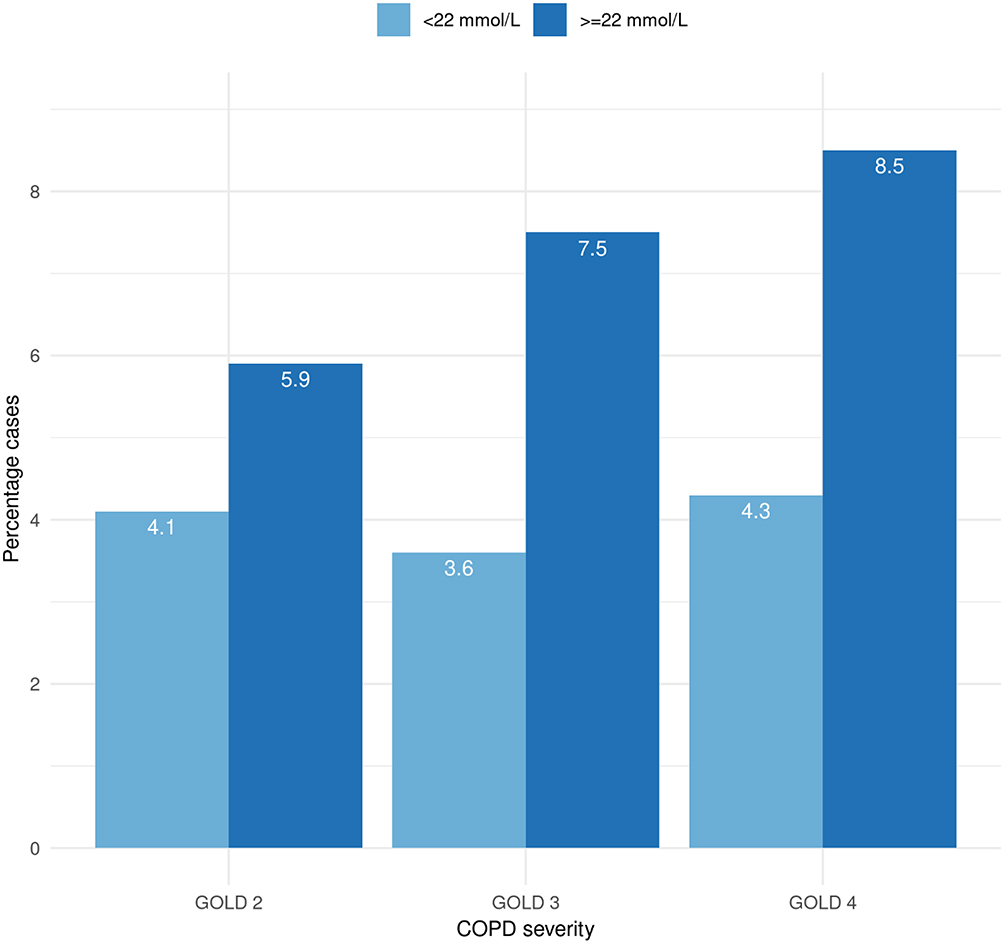 |
Figure 5 Percentage of hyperkalemia cases within each Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage and by bicarbonate level low (<22 mmol/L) and normal–high (≥22 mmol/L). Abbreviation: COPD, chronic obstructive pulmonary disease. |
Additional results from exploratory analyses of serum bicarbonate subgroups are provided in the Supplementary Material.
Discussion
Hyperkalemia is associated with increased all-cause mortality due to its life-threatening arrhythmia risk.2 The risk of developing comorbid hyperkalemia has been extensively studied in patients with HF, DM, and CKD during the past two decades.20–22 To our knowledge, this is the first study evaluating the risk of hyperkalemia in a large number of patients with COPD.
The results of this study showed that 6.4% of patients with COPD had at least one hyperkalemia event during their participation in the ETHOS and KRONOS clinical trials, and the risk was increased by severe or very severe COPD, a diagnosis of DM or CKD and by ACEi use. Relatively high proportion of COPD patients (almost 50%) had no comorbidities (no CKD, DM, or HF) and were not on treatment with ACEis, ARBs, or MRAs. It is considered to be due to the strict exclusion criteria.11,12 However, hyperkalemia was still present in 188 (5.1%) of 3659 patients in this subgroup of COPD patients. This is a relatively high percentage compared with the ~3200 patients with asthma and ~20,000 patients with pneumonia, among whom only 1.2% and 2%, respectively, had a hyperkalemia event during a clinical trial and at admission to the emergency department, respectively.7,23
Among our findings the link between hyperkalemia events and COPD severity was of special interest as this identifies a sub-group of COPD patients that may be of increased risk of hyperkalemia events (and hence ventricular arrhythmias and their associated increased mortality). It is alarming that hyperkalemia risk was significantly increased in GOLD 3- and 4 patients compared with GOLD 2 patients. Hyperkalemia may manifest with various serious arrhythmias including ventricular tachycardia.1,24 Non-sustained and sustained ventricular tachycardia have been shown to be increased with worsening COPD severity, which are suggested to play a role in increased risk of cardiovascular mortality with COPD.25 During an exacerbation, the risk of arrhythmias doubles, while cardiovascular events and mortality have been shown to be increased during and soon after COPD exacerbations.5,26,27
Hypoxemia, acidosis, and poor respiratory function have been claimed to be likely related to increased arrhythmia risk in COPD patients.4 Data from the current study suggest that hyperkalemia is another significant factor that increases the risk of arrhythmias in patients with COPD. Further research should focus on the potential of chronic hyperkalemia to contribute to cardiovascular mortality in COPD patients across the GOLD stages.
Several findings in the current study suggest that COPD-related factors may contribute to hyperkalemia. First, the incidence of hyperkalemia increased with worsening COPD severity. Second, hyperkalemia risk was common even in patients with no major risk factors for hyperkalemia (ie, no CKD, DM, HF, or those who were not on ACEis, ARBs, or MRAs). Third, there was a similar distribution of GOLD stages within each eGFR category suggesting that renal function had a similar role in hyperkalemia frequency in various GOLD stages. Also, we noted that the proportion of diabetic patients was lower in GOLD stage 4 than in GOLD 2–3 and the proportion of patients using ACEis was similar in all GOLD grades.
In the absence of CKD, serum bicarbonate levels in patients with mild-to-moderate COPD are thought to be similar to those of healthy populations. However, patients with COPD commonly have respiratory acidosis, which is related to worsened lung function and hypercapnia, and associated with increased serum bicarbonate levels.28,29 Furthermore, hyperkalemia is associated with raised blood pCO2 values in chronic respiratory acidosis in COPD and during surgery.30–33 In the current study, cases of hyperkalemia tended to increase with increased GOLD stage (5.9–8.5%) among the patients with normal or elevated bicarbonate levels. We hypothesize that the increase in hyperkalemia events, especially in patients with GOLD-4 COPD, could be partly due to COPD-related respiratory acidosis. However, it is not possible to confirm this hypothesis as arterial blood gas analyses were not performed during the study and future studies assessing the frequency, severity, cause, and impact of hyperkalemia in patients with COPD should include arterial blood gas analyses.
In patients with CKD, lower eGFR, older age, and male sex are considered disease-specific risk factors causing hyperkalemia.34 Here, hyperkalemia was reported in 11% of patients with COPD who had moderate-to-severe renal impairment. Furthermore, patients with COPD and mild renal impairment (eGFR 60–89 mL/min/1.73 m2) had a higher risk of developing hyperkalemia than patients with COPD and normal renal function. A recent report found a similar increase in hyperkalemia risk in patients with mild renal impairment.35 Together, these results suggest that reduced renal function is one of the key factors driving the development of hyperkalemia in patients with COPD.
Hyperkalemia is an uncommon (≤2%) complication of RAASi monotherapy in patients with hypertension and normal renal function.36 By contrast, the current study showed that in the normal-to-high renal function group (eGFR ≥90 mL/min/1.73 m2), patients who used RAASis (ACEis, ARBs, or MRAs) showed a 63% increased risk of hyperkalemia versus those who did not use RAASis. It is possible that the physicians in the clinical trials analysed in the current study were generally in favour of using RAASis at higher doses in COPD patients without CKD in whom hyperkalemia risk was considered less of a concern.
Alternatively, results from the CKD subgroup (eGFR <60 and 60–89 mL/min/1.73 m2) showed no significantly increased hyperkalemia risk among patients who did or did not use RAASis (ACEis, ARBs, or MRAs). However, the available data did not allow us to investigate eGFR <30 mL/min/1.73 m2 as a separate category, in which the likelihood of developing hyperkalemia substantially increases.20 Two additional studies have also reported that hyperkalemia risk was not higher in patients with CKD who use RAASis, and in patients hospitalized for acute kidney injury compared with non-users.14,37
Treating physicians may have played a critical role in decreasing the hyperkalemia risk in patients with CKD through regular serum potassium monitoring prior to patient inclusion in the trials included in the current analysis. Furthermore, RAASis may have been discontinued in patients with CKD, or dosing reduced, as needed, or overall potassium intake limited.
Worse NYHA functional class was associated with hyperkalemia in a study of patients with HF.6 Among patients with a history of HF (NYHA I/II) in our study population, almost 10% had hyperkalemia. However, HF was not shown to be an independent risk factor for hyperkalemia. Plausible explanations are the low number of patients with a history of HF and the absence of patients with NYHA class III and IV, which was an exclusion criterion in both the ETHOS and KRONOS studies.
This study had several limitations. The retrospective nature of this study did not allow for assessment of any relationship between hyperkalemia and mortality. Further, this study included a restricted number of patients who were eligible for and were enrolled in a clinical trial and, therefore, may not be representative of the wider population of patients with COPD. Additionally, these analyses included only White patients because of the limited number of non-White patients included in ETHOS and KRONOS. The number of patients taking an MRA was too low to determine whether MRA use was associated with hyperkalemia. It was not possible to determine what RAASi doses patients received, which prevented a more granular investigation on the association between RAASi and hyperkalemia. Due to the retrospective study design we were unable to fully confirm that all patients were using concomitant medications such as RAASis in the same visit of the observed hyperkalemia. Since it was not possible to determine or correct for the impact of hyperglycemia or insulin usage on serum potassium levels, future studies evaluating hyperkalemia in patients with COPD should include control of DM and insulin usage and adjust analyses for these covariates. Finally, blood gas analyses were not available to enable assessment of an association between respiratory acidosis and hyperkalemia.
Conclusion
In conclusion, hyperkalemia was relatively frequent in the study population. Patients with severe and very severe COPD (GOLD-3 and 4) were at a significantly higher risk of hyperkalemia compared with moderate COPD (GOLD 2) patients. It may be particularly lethal in the debilitated COPD population, who are also at increased risk of cardiovascular mortality. The mechanism by which COPD may directly increase the risk of hyperkalemia requires further investigation. Hyperkalemia was also associated with decreasing renal function, comorbid DM, and use of ACEis. It is highly recommended that serum potassium levels are regularly monitored in patients with COPD, particularly those with GOLD-3 and 4. Clinicians should exhibit caution before initiating agents that may precipitate hyperkalemia in such patients without knowing their baseline serum potassium level.
Data Sharing Statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data-sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure. Data for studies directly listed on Vivli can be requested through Vivli at www.vivli.org. Data for studies not listed on Vivli could be requested through Vivli at https://vivli.org/members/enquiries-about-studies-not-listed-on-the-vivli-platform/. AstraZeneca Vivli member page is also available outlining further details: https://vivli.org/ourmember/astrazeneca/.
Ethics Approval and Informed Consent
The study protocols and informed consent forms were approved by the appropriate institutional review board, independent ethics committee (Supplementary Tables 9 and 10), and written informed consent was obtained from all patients before screening.
Any secondary use of data is assessed by AstraZeneca R&D Data Office for alignment with the patients’ consent, by reviewing the language on future use of data in the Informed Consent Form.
Acknowledgments
Medical writing support under guidance of the authors was provided by Melissa Fernandez PhD and Michael Howell PhD of Core, London, UK, according to Good Publication Practice guidelines. The abstract of this paper was presented at the European Respiratory Society (ERS) Congress 2023 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in European Respiratory Journal: DOI 10.1183/13993003.congress-2023.PA614.
Funding
This study was funded by AstraZeneca. ETHOS and KRONOS clinical trials were funded by AstraZeneca and Pearl—a member of the AstraZeneca Group, respectively.
Disclosure
All authors are employees of AstraZeneca. The authors report no other conflicts of interest in this work.
References
1. Kovesdy CP. Updates in hyperkalemia: outcomes and therapeutic strategies. Rev Endocr Metab Disord. 2017;18(1):41–47. doi:10.1007/s11154-016-9384-x
2. Collins AJ, Pitt B, Reaven N, et al. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am J Nephrol. 2017;46(3):213–221. doi:10.1159/000479802
3. Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84(12):934–942. doi:10.3949/ccjm.84a.17056
4. Falk JA, Kadiev S, Criner GJ, et al. Cardiac disease in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):543–548. doi:10.1513/pats.200708-142ET
5. Celli BR, Fabbri LM, Aaron SD, et al. Differential diagnosis of suspected chronic obstructive pulmonary disease exacerbations in the acute care setting: best practice. Am J Respir Crit Care Med. 2023;207(9):1134–1144. doi:10.1164/rccm.202209-1795CI
6. Savarese G, Xu H, Trevisan M, et al. Incidence, predictors, and outcome associations of dyskalemia in heart failure with preserved, mid-range, and reduced ejection fraction. JACC Heart Fail. 2019;7(1):65–76. doi:10.1016/j.jchf.2018.10.003
7. Mäenpää J, Emerath U, Sultana S, et al. The risk of hyperkalemia in COPD and asthma patients. Eur Respir J. 2019;54:PA4334. doi:10.1183/13993003.congress-2019.PA4334
8. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
9. Salem BC, Badreddine A, Fathallah N, et al. Drug-induced hyperkalemia. Drug Saf. 2014;37(9):677–692. doi:10.1007/s40264-014-0196-1
10. Global Initiative for Chronic Obstructive Lung Disease. GLOBAL STRATEGY FOR PREVENTION, DIAGNOSIS AND MANAGEMENT OF COPD:2023 Report, 2023.
11. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
12. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
13. Michel A, Martín-Pérez M, Ruigómez A, et al. Risk factors for hyperkalaemia in a cohort of patients with newly diagnosed heart failure: a nested case–control study in UK general practice. Eur J Heart Fail. 2015;17(2):205–213. doi:10.1002/ejhf.226
14. Einhorn LM, Zhan M, Hsu VD, et al. The frequency of hyperkalemia and its significance in chronic kidney disease. Arch Intern Med. 2009;169(12):1156–1162. doi:10.1001/archinternmed.2009.132
15. Kristensson C, Åstrand A, Donaldson S, et al. AZD5634, an inhaled ENaC inhibitor, in healthy subjects and patients with cystic fibrosis. J Cyst Fibros. 2022;21(4):684–690. doi:10.1016/j.jcf.2022.02.010
16. Goyal A, Spertus JA, Gosch K, et al. Serum potassium levels and mortality in acute myocardial infarction. JAMA. 2012;307(2):157–164. doi:10.1001/jama.2011.1967
17. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
18. Kidney Disease Improving Global Outcomes. KDIGO 2012. Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:5–14.
19. Kraut JA, Madias NE. Metabolic acidosis: pathophysiology, diagnosis and management. Nat Rev Nephrol. 2010;6(5):274–285. doi:10.1038/nrneph.2010.33
20. Palmer BF. Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. N Engl J Med. 2004;351(6):585–592. doi:10.1056/NEJMra035279
21. Palmer BF, Clegg DJ. Electrolyte and acid-base disturbances in patients with diabetes mellitus. N Engl J Med. 2015;373(6):548–559. doi:10.1056/NEJMra1503102
22. Sarwar CMS, Papadimitriou L, Pitt B, et al. Hyperkalemia in heart failure. J Am Coll Cardiol. 2016;68(14):1575–1589. doi:10.1016/j.jacc.2016.06.060
23. Ravioli S, Gygli R, Funk GC, et al. Prevalence and impact on outcome of sodium and potassium disorders in patients with community-acquired pneumonia: a retrospective analysis. Eur J Intern Med. 2021;85:63–67. doi:10.1016/j.ejim.2020.12.003
24. Hunter RW, Bailey MA. Hyperkalemia: pathophysiology, risk factors and consequences. Nephrol Dial Transplant. 2019;34(Suppl 3):iii2–iii11. doi:10.1093/ndt/gfz206
25. Konecny T, Park JY, Somers KR, et al. Relation of chronic obstructive pulmonary disease to atrial and ventricular arrhythmias. Am J Cardiol. 2014;114(2):272e277. doi:10.1016/j.amjcard.2014.04.030
26. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of Chronic Obstructive Pulmonary Disease and Cardiac Events. A Post Hoc Cohort Analysis from the SUMMIT Randomized Clinical Trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
27. Donaldson GC, Hurst JR, Smith CJ, et al. Increased risk of myocardial infarction and stroke following exacerbation of COPD. CHEST. 2010;137(5):1091–1097. doi:10.1378/chest.09-2029
28. Epstein SK, Singh N. Respiratory acidosis. Respir Care. 2001;46(4):366–383.
29. Palmer BF, Clegg DJ. Respiratory acidosis and respiratory alkalosis: core curriculum. Am J Kidney Dis. 2023;82(3):347–359. doi:10.1053/j.ajkd.2023.02.004
30. Dulfano MJ, Ishikawa S. Hypercapnia: mental changes and extrapulmonary complication. An expanded concept of the “CO-2 intoxication” syndrome. Ann Intern Med. 1965;63(5):829–841. doi:10.7326/0003-4819-63-5-829
31. Edwards R, Winnie AP, Ramamurthy S. Acute hypocapneic hypokalemia: an latrogenic anesthetic complication. Anesth Analg. 1977;56(6):786–792. doi:10.1213/00000539-197711000-00009
32. Hassan H, Gjessing J, Tomlin PJ. Hypercapnia and hyperkalaemia. Anaesthesia. 1979;34(9):897–899. doi:10.1111/j.1365-2044.1979.tb08543.x
33. Weinberg L, Lee DK, Gan C, et al. The association of acute hypercarbia and plasma potassium concentration during laparoscopic surgery: a retrospective observational study. BMC Surg. 2021;21(1):31. doi:10.1186/s12893-020-01034-w
34. Seliger SL. Hyperkalemia in patients with chronic renal failure. Nephrol Dial Transplant. 2019;34(Supplement_3):iii12–iii8. doi:10.1093/ndt/gfz231
35. Sriperumbuduri S, McArthur E, Hundemer GL, et al. Initial and recurrent hyperkalemia events in patients with CKD in older adults: a population-based cohort study. Can J Kidney Health Dis. 2021;8:20543581211017408. doi:10.1177/20543581211017408
36. Weir MR, Rolfe M. Potassium homeostasis and renin-angiotensin-aldosterone system inhibitors. Clin J Am Soc Nephrol. 2010;5(3):531–548. doi:10.2215/CJN.07821109
37. Villain C, Metzger M, Liabeuf S, et al. Effectiveness and tolerance of renin-angiotensin system inhibitors with aging in chronic kidney disease. J Am Med Dir Assoc. 2022;23(6):998–1004.e7. doi:10.1016/j.jamda.2021.10.019
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.