Back to Journals » Infection and Drug Resistance » Volume 19
Hyperbaric Oxygen Treatment as a Novel Add-on in Selected Patients with Infective Endocarditis – A Safety and Feasibility Trial
Authors Pries-Heje MM ![]() , Lerche CJ, Fosbøl E, Forchhammer M, Hasselbalch RB, Schwartz F, Siebert ASL, Jensen PØ
, Lerche CJ, Fosbøl E, Forchhammer M, Hasselbalch RB, Schwartz F, Siebert ASL, Jensen PØ ![]() , Rottensten H, Iversen K
, Rottensten H, Iversen K ![]() , Bundgaard H, Hyldegaard O
, Bundgaard H, Hyldegaard O ![]() , Moser C
, Moser C
Received 24 September 2025
Accepted for publication 17 March 2026
Published 22 May 2026 Volume 2026:19 568123
DOI https://doi.org/10.2147/IDR.S568123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mia Marie Pries-Heje,1 Christian Johann Lerche,2 Emil Fosbøl,1,3 Martin Forchhammer,4,5 Rasmus Bo Hasselbalch,1,5 Franziska Schwartz,2 Anne Sofie L Siebert,2 Peter Østrup Jensen,2,6,7 Henrik Rottensten,4 Kasper Iversen,3,5,8 Henning Bundgaard,1,3 Ole Hyldegaard,3,4 Claus Moser2,6
1Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; 2Department of Clinical Microbiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; 3Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 4Department of Anaesthesiology, Centre of Head and Orthopedics, Rigshospitalet, Copenhagen University, Copenhagen, Denmark; 5Department of Cardiology, Herlev-Gentofte Hospital, Copenhagen University Hospital, Herlev, Denmark; 6Department of Immunology and Microbiology, University of Copenhagen, Copenhagen, Denmark; 7Center for Rheumatology and Spine Diseases, Institute for Inflammation Research, Rigshospitalet, Copenhagen University Hospital, Copenhagen; 8Department of Emergency Medicine, Herlev-Gentofte Hospital, Copenhagen University Hospital, Herlev, Denmark
Correspondence: Mia Marie Pries-Heje, Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Blegdamsvej 9, Copenhagen, 2100, Denmark, Tel +45 35 45 23 40, Email [email protected]
Background: Infective endocarditis (IE) is associated with a high morbidity and mortality. Adjunctive hyperbaric oxygen (HBO2) treatment may enhance bactericidal effects of antibiotics and improve outcomes in patients with IE We conducted an open label, feasibility, and safety trial, including exploratory biomarker analyses, to evaluate HBO2-therapy in patients with IE.
Methods: This Phase I/II feasibility and safety trial included patients aged > 18 years, with left-sided IE caused by Gram-positive cocci. The intervention consisted of six consecutive HBO2-sessions at 2.4 atm. Antibiotics were administered 1 hour before each HBO2-session.
Results: Of 26 screened patients, 13 patients were included and 10 (77%) completed the HBO2-therapy (age 80 years (IQR 73– 83); 70% male). Median time from diagnosis of IE to first HBO2 session was 6 days (IQR 5– 7). No serious adverse events or suspected unexpected serious adverse reactions were recorded. Pre- and post-HBO2 blood samples revealed significant changes in biomarkers: reduced median CRP levels (22 vs 15 mmol/L, p=0.043) and hemoglobin levels (6.4 vs 5.8 mmol/L, p=0.021); increased mean serum VCAM-1 (1.22x106 vs. 1.29x106 pg/mL, p=0.0003) and E-selectin (5.7x104 vs. 6.41x104 pg/mL, p=0.044); and a decrease in G-CSF levels (73.85 vs 72.93 pg/mL, p=0.021), activated platelets (193.7 vs 169.8 MFI, p=0.015), and platelet-neutrophil complexes (2747 vs 1916 MFI, p=0.003).
Conclusion: Adjunctive HBO2 therapy was feasible and safe in selected patients with IE. Significant changes in biochemical markers suggest potential immunomodulatory effects of HBO2-therapy. Randomized controlled trials are required to evaluate the clinical efficacy of HBO2 as an adjunct to standard care in IE.
Study Id: EudraCT (2019– 000857-29). Danish Medicines Agency (2019030362). Infographic on hyperbaric oxygen treatment for adults with left-sided IE. Includes population, intervention, sample collection and findings.
Keywords: infective endocarditis, hyperbaric oxygen, adjunctive therapy, biofilm infection
Introduction
The incidence of infective endocarditis (IE) is increasing,1–3 with in-hospital mortality largely unchanged at 20%4–6 and a 35–50% all-cause mortality at 3–5 years follow-up.7–9
Antibiotics may have reduced efficacy in valvular vegetation biofilm infections,10 abscesses, and peripheral tissue with poor oxygenation, due to reduced bacterial killing by reactive oxygen species (ROS) and polymorphonuclear neutrophils.11
Hyperbaric oxygen (HBO2) treatment is commonly applied in repeated sessions of 1–1.5 hours, in a pressure chamber where the patient breathes pure oxygen, resulting in estimated oxygen levels at 6–10 fold higher than normal physiological tissue-levels.11,12 Improvement of antibacterial effects of certain antibiotics through HBO2 treatment has shown promise in in vitro biofilm models, as well as in animal models with Staphylococcus aureus IE.10,13 Possible positive effects of adjunctive HBO2 treatment include (i) decreased tissue hypoxia, (ii) reduced biofilm, (iii) reduced microbial growth and virulence, (iv) reduced pro-inflammatory cytokines and adhesins, and (v) enhanced growth factors and anti-inflammatory cytokines.11
To our knowledge, HBO2 treatment has not previously been studied in patients with IE. The safety profile of HBO2 treatment in an IE patient population remains unknown and implementing the therapy during the active phase of IE is organizationally challenging. Based on these considerations, we initiated a phase I/II trial (ENDOHOT trial) to evaluate the safety and feasibility of adjunctive HBO2 treatment in hemodynamically stable patients with left-sided IE caused by Gram-positive cocci, which account for 85% of all IE cases4,14 Additionally, exploratory biomarker analyses were performed to provide a foundation for the design of a large-scaled randomized controlled trial of HBO2 treatment of patients with IE.
Materials and Method
Trial Design and Oversight
The ENDOHOT trial (Hyperbaric oxygen treatment in humans with Gram-positive cocci endocarditis) was an open label, non-randomized single-arm phase I/II trial performed at the Copenhagen University Hospital, Rigshospitalet and Herlev-Gentofte Hospital, Denmark. The study was approved by the Danish Medicines Agency (Journal file no.: 2019030362), the Danish Data Protection Agency (Journal file no.: VD-2019-149) and the regional ethical committee of the Capitol Region of Denmark (Journal file.no: H-19024913). The study was registered on EudraCT (2019–000857-29). The trial was overseen by the Copenhagen University GCP-Unit and complied with WHO GCP criteria for good clinical research practice and was performed in accordance with the principles of the Declaration and Helsinki. All participants provided written informed consent. All the authors vouch for the completeness and accuracy of the data and analyses presented.
Patient Population
Inclusion of 10 patients with a completed course of HBO2 treatments was planned. Eligible patients were adults (≥18 years), fulfilling the modified Duke criteria for left-sided definitive IE, including positive blood cultures with Gram-positive cocci. Patients needed to be respiratory and hemodynamically stable, with no need of mechanical support or inotropes and/or vasopressor support, able to perform Valsalva’s maneuver or accepting either tympanic paracentesis- or tubulation if needed, and able to be seated for duration of treatment. Only patients where HBO2 treatment could be initiated within 2 weeks after the diagnosis of IE with concurrent initiation of appropriate antibiotic treatment were eligible for inclusion.
Patients were excluded if they suffered from severe claustrophobia, were clinically or hemodynamically unstable, had 2nd or 3rd degree AV-block without a temporary pacemaker, had signs of pneumothorax on X-ray or CT, or were planned for cardiac surgery within the same timeframe as planned HBO2 treatment.
Hyperbaric Oxygen Treatment
Patients were scheduled for six consecutive HBO2 sessions over a maximum of 5 days, with one to two sessions per day and at least a six-hour interval between sessions. Each session consisted of placement in an HBO2 multi-place chamber with 100% oxygen at 2.4 atmospheres absolute (ATA, or 243 kPa)) for 90 min at a time including two air brakes of 5 minutes each (Figure S1). Intravenous antibiotic treatment was administered <1 hour prior to HBO2 treatment. Patients’ vital signs including electrocardiogram, oxygen saturation, pulse rate, level of consciousness and respiratory rate were continuously monitored during treatment. All patients were monitored with telemetry, daily labs, and blood cultures and vital signs during hospitalization in the IE ward, in addition to standard care.
Observations and Outcomes
The primary feasibility outcomes of the trial were (I) patient compliance (tolerance/acceptance of the treatment) and (II) practical feasibility of completing all six HBO2 treatment sessions. A successful session required ≥60 min of HBO2 at 2.4 ATA, and adequate treatment was defined as ≥4 completed session.
Primary safety endpoint was assessed by monitoring and reporting of serious adverse events (SAE’s) and suspected unexpected serious adverse reactions (SUSAR’s), according to the Clinical Study Serious Adverse Event Report Form and the Danish Health and Medicines Authority’s form for SUSAR’s.
Secondary endpoints included assessment of changes on imaging by echocardiography <48 hours before and after first and last HBO2 session, biochemistry including C-reactive protein (CRP), procalcitonin, white blood cell count, haemoglobin, coagulation parameters, D-dimer, kidney and liver parameters, serum biomarkers, daily blood cultures and whole blood for flow cytometrical analysis of neutrophils, platelets, and their complexes.
Samples
Blood was drawn from participants via 21G butterfly needle or from a central venous catheter. All patients had blood drawn before (max 1 hour) and directly after HBO2 treatment (±15 min post-treatment).
Serum Cytokines
For multiplex analysis, a human cytokine assay (Bio-Rad, Hercules, CA) was used on a LUMINEX® 200TM platform (Luminex Corporation, Austin, TX). Granulocyte–colony stimulating factor (G-CSF),15 urokinase plasminogen activator surface receptor (uPAR, CD87),16 interleukin (IL)-1β and IL-8,15,17 vascular endothelial growth factor (VEGF),18 intercellular adhesion molecule 1 (ICAM-1),19 vascular cell adhesion protein 1 (VCAM-1)20 and E-selectin20 were measured (purchased from R&D systems, Abingdon, UK). Missing samples and sample outliers with values beyond ±2 standard deviations were excluded for analysis.
Flow Cytometry
To measure total leukocyte count (data not shown) and neutrophils (Panel 1), 50 µL of citrate whole blood were added to counting tubes (BD Trucount™ tube, 340334) placed on ice followed by addition of 10 µL each of the following antibodies: CD11b Monoclonal Antibody (M1/70), APC, eBioscience™, CD15 Monoclonal Antibody (HI98), FITC, eBioscience, and CD45 Monoclonal Antibody (HI30), eFluor 450, eBioscience. The samples were incubated in the dark for 30 min and added 1 mL FACS lysing solution (BD FACS™ lysing Solution) dilute 1:10 in MilliQH2O for simultaneous lysing of erythrocytes and fixation. After incubation for 10 minutes, the samples were analyzed by flow cytometry.
For estimating platelet-neutrophil-complexes (Panel 2), 100 µL of citrate whole blood was added to a 5 mL falcon tube (Corning Science México S.A. de C.V. Ref 352054) placed on ice followed by addition of 10 µL each of the following antibodies: CD11b Monoclonal Antibody (ICRF44), Super Bright 600, eBioscience, CD15 Monoclonal Antibody (HI98), eFluor 450, eBioscience, CD42b Monoclonal Antibody (HIP1), FITC, eBioscience, and CD62P (P-Selectin) Monoclonal Antibody (Psel.KO2.3), APC, eBioscience. The samples were incubated in the dark for 30 min and diluted 1000 times in cold PBS filtered through a 0.22 µm filter before flow cytometrical analysis on an Attune NxT flow cytometer (Thermo Fisher Scientific, Waltham, MA, USA).
Samples from panel 1 were recorded using standard filter settings and samples from panel 2 were recorded using the Attune NxT No-Wash No-Lyse Filter Kit (Thermo Fisher Scientific).21 Missing and failed samples and outliers with values beyond ±2 standard deviations were excluded from the analysis.
Statistical Analysis
Continuous variables are presented as means and standard deviations or medians and interquartile ranges, as appropriate. Categorical variables are expressed as absolute numbers and frequencies. Parametric data were assessed for normality using the D’Agostino and Pearson omnibus normality test and analyzed using paired t-tests (pooled data). For non-parametric data, the Wilcoxon matched-pairs signed-rank test was applied, with correction for multiple comparisons.22 Two-sided P-values of less than 0.05 were considered statistically significant. Analyses were performed with the use of R software (R Foundation for Statistical Computing). Statistical analyses of serum cytokines and flow cytometry data were performed using GraphPad Prism v.10.1.2 (GraphPad Software, Inc., San Diego, CA).
Results
Patient Inclusion and Feasibility
A total of 26 patients were screened for inclusion. Of these, 13 patients were excluded prior to initiation of HBO2 treatment; one (8%) due to pneumothorax, two (15%) due to hemodynamic instability, two (15%) could not be initiated within the first 14 days of relevant antibiotic treatment and eight (62%) declined to participate (Figure 1). For the remaining 13 patients, 62 HBO2 sessions in total were initiated, with intravenous antibiotics administered ≤ 1 hour before HBO2 treatment in 60 sessions (97%). Two (15%) patients were excluded without completion of any HBO2 sessions due to claustrophobia and one (8%) patient was excluded after completion of the 1st HBO2 session due to subacute cardiac surgery, leaving 10 patients who completed treatment. Eight patients (80%) completed all six sessions of 90 mins duration. One (10%) patient completed five sessions, before early termination of HBO2 treatment due to planned subacute cardiac surgery. One (10%) patient completed four sessions of 90 minutes, 40 min of a 5th session (terminated due to diarrhea related to preparation for colonoscopy). Final session was omitted due patient fatigue. Details of treatment-related side-effects and patient tolerance are provided in the supplementary (Table S1).
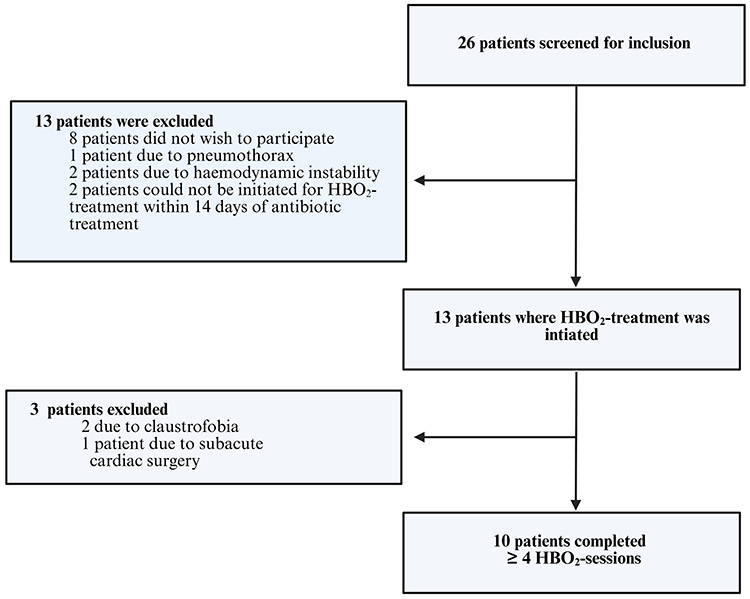 |
Figure 1 Inclusion and exclusion of patients. Abbreviation: HBO2, Hyperbaric oxygen. |
Baseline Characteristics
Of the 10 patients completing HBO2 treatment, the majority were men (n=7, 70%) and the median age was 80 years (IQR 73–83) (Table 1). All patients were assessed by transesophageal echocardiography at time of diagnosis. Median time from diagnosis to first HBO2 session was 6 days (IQR 5–7). The pathogens were Streptococcus spp. (n = 5, 50%) followed by Enterococcus faecalis (n= 4, 40%) and Staphylococcus aureus (n=1, 10%). Half of the patients (n=5, 50%) had a prosthetic heart valve at baseline. The most common affected valve was the aortic valve (n = 8, 80%) and four (40%) patients had cardiac abscess formation, three of which were not considered surgical candidates and were discharged as terminally ill. Echocardiographic variables before and after HBO2 treatment are shown in Table S2. No patients underwent cardiac surgery prior to inclusion in the trial. The median level of CRP at inclusion was 26 mmol/L (IQR 15–58 mmol/L). Baseline lab values can be seen in Table S3.
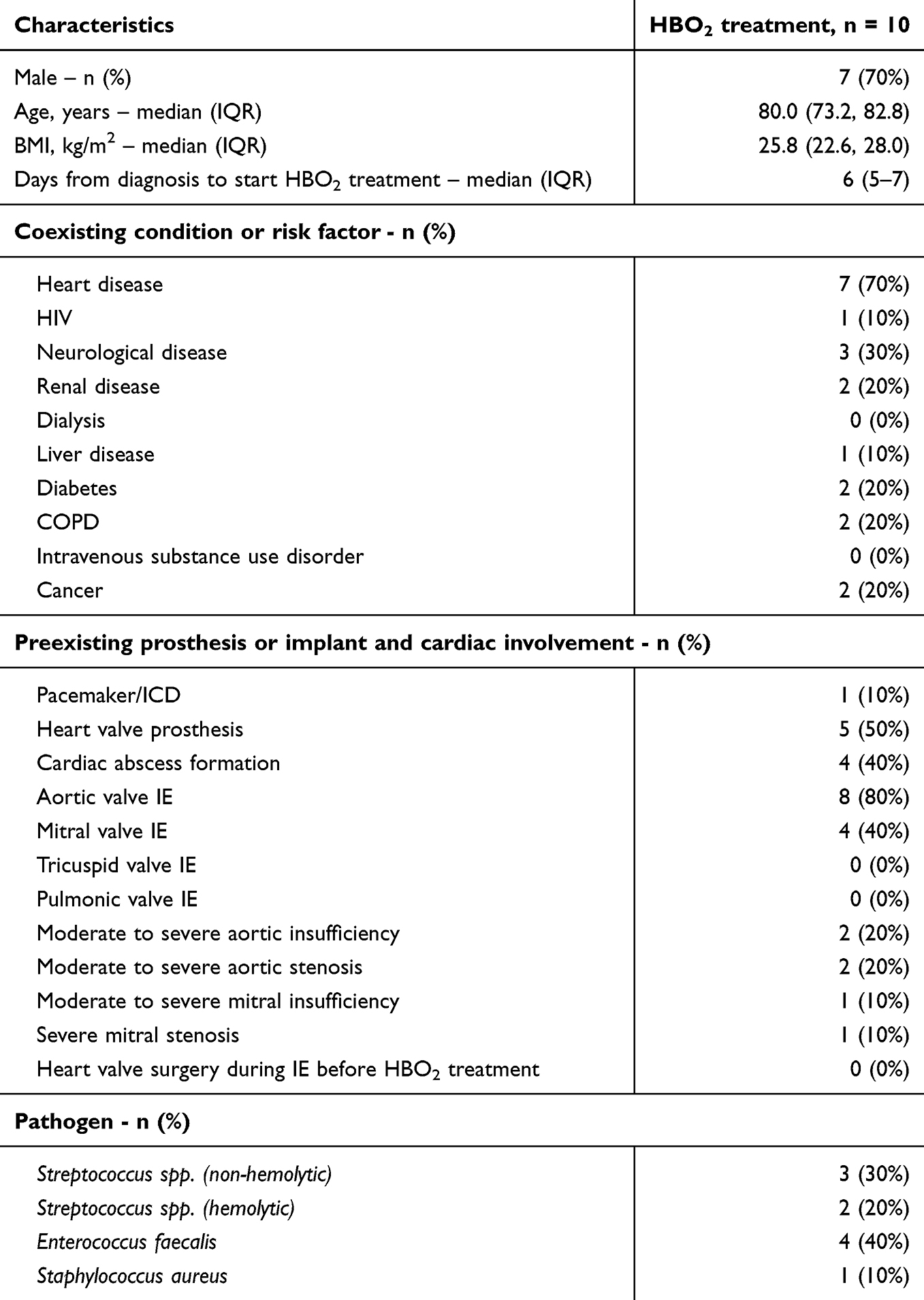 |
Table 1 Clinical Characteristics of Patients |
Safety and Secondary Outcomes
There were no SAE’s or SUSARs registered, and no deaths considered related to HBO2 therapy. Echocardiographic parameters before and after HBO2 treatment were largely unchanged (Table S2). There were no relapses of positive blood cultures and no new surgical indications identified. One patient (10%) died within 30 days of HBO2 treatment, due to heart failure caused by IE complicated by severe valvular heart disease with no surgical options and the patients had been discharged to palliative care. Outcome was not considered related to HBO2 treatment.
Biochemistry before and after HBO2 treatment can be seen in Supplementary Figure S2. After HBO2 treatment, there were significant reductions in CRP levels (pre-HBO2 CRP: 22 mmol/L (IQR 14–46) vs post-HBO2 CRP: 15 mmol/L (IQR 9–21), p=0.043) and in hemoglobin levels (pre-HBO2 Hgb: 6.4 mmol/L (IQR 5.9–7.6) vs post-HBO2 Hgb: 5.8 mmol/L (IQR 5.5 −7.6), p=0.021). There were no significant differences in WBC or eGFR.
Serum Cytokines and Adhesins
The concentrations of serum cytokines and adhesion markers measured pre- and post-HBO2 treatment over the entire treatment period are presented in Figures 2 and S3.
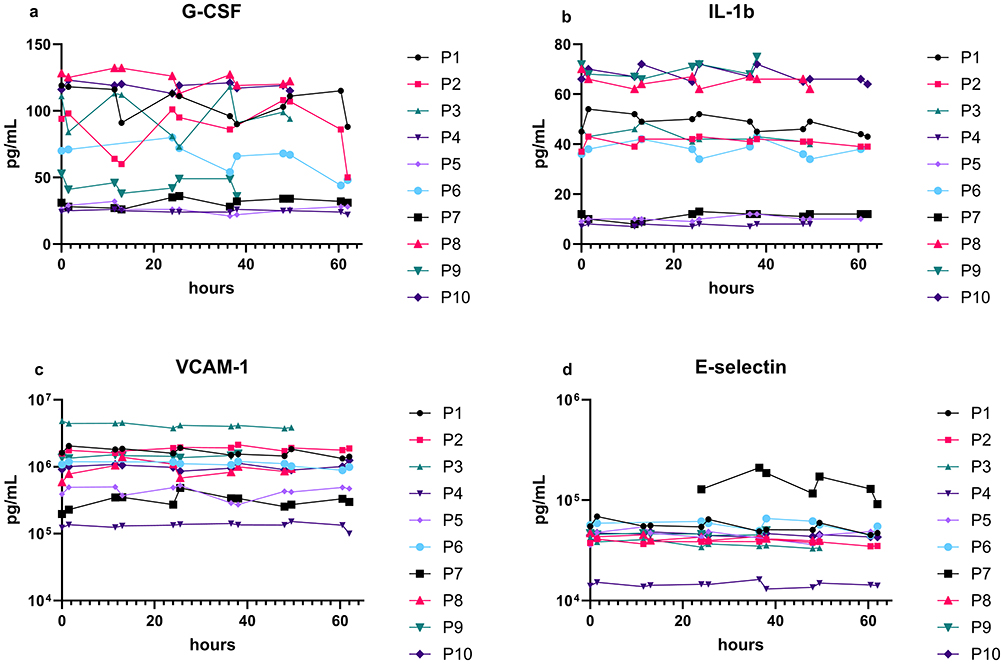 |
Figure 2 Serum cytokine and adhesion molecule levels pre- and post-HBO2 treatment. Serum levels of granulocyte colony-stimulating factor (G-CSF) (a), interleukin-1β (IL-1β) (b), vascular cell adhesion protein 1 (VCAM-1) (c), and E-selectin (d) were measured before (pre) and after (post) each hyperbaric oxygen (HBO2) treatment. Concentrations are presented in pg/mL. The number of patients included in the analysis for each HBO2 session was as follows: session 1 (n=9), session 2 (n=7), session 3 (n=8), session 4 (n=9), session 5 (n=9), and session 6 (n=7). Samples were excluded if missing or identified as outliers beyond ± standard deviations. Statistical analysis was not performed. |
Pooled pre- and post-HBO2 treatment data demonstrated a significant increase in VCAM-1 and E-selectin levels, accompanied by a decrease in G-CSF. VCAM-1 increased from a mean of 1.22 × 106 ± 1.09 × 106 pg/mL (95% CI 9.25–15.16 × 106) to 1.29 × 106 ± 1.11 × 106 pg/mL (95% CI 9.90–15.91 × 106; p = 0.0003, n = 55). E-selectin increased from 5.70 × 104 ± 7.42 × 104 pg/mL (95%CI 3.76–7.77 × 104) to 6.41 × 104 ± 9.83 × 104 pg/mL (95% CI 3.76–9.07 × 104; p = 0.044, n = 55). In contrast, G-CSF levels decreased from 73.85 ± 39.86 pg/mL (95% CI 63.08–84.63) to 72.93 ± 47.40 pg/mL (95% CI 60.11–85.74; p = 0.021, n = 55) (Figure S4). For other measured cytokines and adhesion markers no significant differences were found (data not shown).
Neutrophil Count, Neutrophil, and Platelets Activation and Platelets-Neutrophil Complex Formation
Flow cytometry analysis of neutrophils revealed a non-significant increase at pre- vs. post-HBO2 treatment for sessions 1, 3, and 5 based on paired analysis. Specifically, for session 1 (S1): pre-treatment: 5.52 ×109 ± 1.59 ×109 vs. post-treatment: 5.57 ×109 ±1.96 ×109, p=0.92; for session 3: pre-treatment: 4.84 ×109 ±1.65 ×109 vs. post-treatment: 5.28 ×109 ±1.63 ×109, p=0.32; and for session 5: pre-treatment: 4.86 ×109 ±1.63 ×109 vs. post-treatment: 5.40 ×109 ±1.43 ×109, p=0.35. Similarly, activated neutrophils showed no significant change across sessions (S1 pre-treatment: 2505 ± 1292 vs. S1 post-treatment: 2357 ±828, p=0.50; S3 pre-treatment: 2707 ±1504 vs. S3 post-treatment: 2469 ±1479, p=0.47; S5 pre-treatment: 2228 ±908 vs. S5 post-treatment: 2338 ±1482, p=0.70) (Figure S5a and b).
Activated platelets exhibited a decrease at session 3, with a reduction in mean fluorescence intensity (MFI) from pre-HBO2 (193.4 ±44.81) to post-HBO2 treatment (176.3 ±37.47 MFI), p=0.037. A non-significant reduction was observed at sessions 1 and 5 (p=0.34 and p=0.12, respectively). Platelet-neutrophil complexes showed a reduction at sessions 3 (pre-treatment (2931 ±1548 MFI) vs. post-treatment (1893 ±665 MFI), p=0.050) and 5 (pre-treatment (2463 ±1032 MFI) vs. post-treatment (1349 ±257 MFI, p=0.03) (Figure 3). Paired analysis of all individual values (pooled data, n=23) revealed a non-significant increase in the total number of neutrophils comparing pre- vs. post-HBO2 treatment (5.12 ×109 ±1.58 ×109 vs. 5.42 ×109 ±1.66 ×109 neutrophils /L, p=0.28) (Figure S6a). Whole blood analysis for activated neutrophils, as indicated by CD11b expression, showed a non-significant reduction after HBO2 treatment (2314 ±1083 vs. 2181 ±1016 fluorescence intensity (MFI), p=0.35) (Figure S6b). In contrast, activated platelets, as indicated by CD62p expression, showed a significant reduction after HBO2 treatment (193.7 ±46 vs. 169.8 ±33 MFI, p=0.015) (Figure S6c). Additionally, analysis of whole blood platelet-neutrophil complexes revealed a significant reduction post-HBO2 (2747 ±1631 vs. 1916 ±1271 MFI, p=0.003) (Figure S6d).
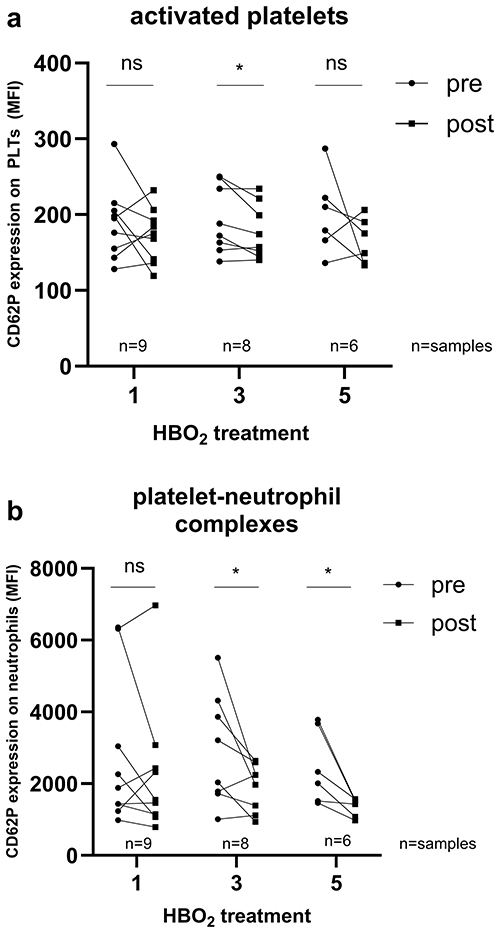 |
Figure 3 Flow cytometry analysis of whole blood pre- and post-HBO2 treatment. Flow cytometry was used to analyze whole blood samples collected pre and post HBO2 treatment, at session 1, 3 and 5. Activated platelets (panel a) and platelet-neutrophil complexes (panel b) we quantified. A paired t-test was used to compare pre- and post-HBO2 measurements. n=samples for analysis. Significant decreases are indicated by asterisks (*P ≤ 0.05). Abbreviations: MFI, mean fluorescent index; ns, non-significant. |
Discussion
In this phase I/II feasibility trial of HBO2 treatment as adjunctive therapy in patients with left-sided IE, we found that this treatment was feasible in 62% of the patients, with partial completion in an additional 15% of patients. No SAE’s or SUSARs were seen in relation to HBO2 treatment. The main side effect specifically related to HBO2 treatment was claustrophobia. Based on these findings, HBO2 treatment as adjunctive therapy in patients with IE is regarded feasible and safe in the majority of patients. The exploratory analysis of biomarkers measured before and after each session of HBO2-treatment showed significant changes in a proportion of several markers, yet might be confounded by antibiotic treatment and reflect the natural disease course. Larger randomized trials are needed to assess the impact of HBO2 on clinical outcomes, including efficacy on pathogen eradication, risk of IE relapse, and need of later surgical intervention in addition to effect on short- and long-term mortality, and also on risk of relapse of infection and need for surgery.
Undertaking six sessions of HBO2 treatment twice daily during the early critical treatment phase of IE23 was organizationally challenging and affected the timing of other procedures. This was reflected in the need to expand the initial timeframe for completion of six sessions within 3 days to a maximum of 5 days, allowing for initiation of treatment in the evening and restricting HBO2 treatment to one session on days where other diagnostic procedures such as PET-CT and endoscopies were performed. For one patient, it was only possible to complete four full sessions and one 40-min session due to the patient’s clinical condition. The initial protocol planned to include patients within 1 week of initiation of antibiotic therapy. This timeframe was expanded to 2 weeks by the trial investigators, to allow for higher recruiting rate. Considering the large resource allocation associated with completing all six HBOT sessions as per protocol, further knowledge on the benefits of HBO2 treatment is needed to assess the gain from adjunctive therapy of HBO2 treatment. However, we identified a potential benefit of HBO2 therapy for patients with IE. If adjunctive therapy with HBO2 was found to enhance antibiotic efficacy and improve bacterial eradication in randomized clinical trials, it might be of clinical value in selected patients, eg. those who are not surgical candidates or with abscess formation, prosthetic material in the heart, or reduced kidney function, to reduce risk of relapse or possibly reduce the total daily antibiotic dosage.
We found that CRP levels were significantly lower at the end of HBO2 treatment; however the patients already had low levels at time of treatment. This might reflect the natural treatment course of the disease over time and is difficult to interpret in relation to the anti-inflammatory effect of HBO2 treatment measured by serum cytokines. A randomized study including patients both in the early and the septic phase of IE could provide valuable insights into the effects of HBO2 treatment. This approach has shown promise in an experimental rat models of S. aureus IE,13 undergoing 6 consecutive sessions with HBO2 treatment at 280 kPA pressure HBO2 treatment has also been demonstrated beneficial in patients with infection caused by other severe biofilm-forming infections such as necrotizing soft tissue infections, including a study of 114 patients with septic shock, undergoing daily HBO2 treatment at 284 kPA pressure19,24,25 We also found significantly lower hemoglobin levels which might reflect a response to treatment, but might also be related to development of inflammatory anemia caused by the infection,26 in combination with iatrogenic anemia caused by multiple blood tests.
No significant changes were seen in sequential measurements of the serum cytokines and adhesion molecules during HBO2 treatment. This could be explained by the stability and low inflammation seen in patient at the state of inclusion (baseline biochemistry) contrary to other observations in HBO2 treated patients with sepsis and septic shock27 and after several day of antibiotic treatment. Pooled data showed a temporary elevation of serum VCAM-1 and E-selectin and decline of G-CSF after HBO2 exposure. VCAM‑1 and E‑selectin are co‑regulated markers of endothelial activation and leukocyte recruitment, frequently elevated together in cardiovascular and inflammatory disease.28 The impact of this temporary elevation of VCAM-1 and E-selectin remains uncertain and should be interpreted with caution. Evidence is limited, but it may reflect endothelial activation that promotes leukocyte recruitment, including VCAM-1–mediated rolling, firm adhesion, and subsequent transmigration to the site of infection. The temporary decline of G-CSF could reflect reduced inflammation. However, these serum markers are surrogate markers for the actual inflammation in the surrounding of the endothelium of the heart valves and could indicate the extensive activation of endothelial and the dominating source of VCAM-1 and E-selectin cells during infection. Elevation of these soluble serum markers could also be a consequence of shredding from the endothelial line in the regeneration and healing process of the endothelium induced by HBO2, which has also been observed in vitro endothelial cell study.29 Another explanation for the transient rise in VCAM-1 and E-selectin post HBO2 sessions may reflect short-term endothelial activation or “priming” in response to hyperoxia and oxidative signals, without implying harmful or sustained vascular injury.30 Söderquist et al20 have also shown that VCAM-1 and E-selectin are elevated in patients with S. aureus IE and S aureus bacteremia. These adhesions molecules are expressed by several cell types that play key roles in both the innate immune and adaptive immune response.31,32 The local response in the heart valves could for obvious reasons not be investigated in this trial but was assessed by consecutive echocardiography. However, the previous mention precursor of this trial, a pre-clinical study of S. aureus IE, suggest that HBO2 treatment can reduce levels of several proinflammatory cytokines and adhesins in infected valves.13
In response to HBO2 treatment we found no significant differences in total PMNs count and activated leukocytes, although there was a trend of elevated leukocytes after HBO2 treatment. Previous studies have shown that the HBO2 treatment can mobilize stem cells from the bone marrow especially CD34+ progenitor cells (pluripotent) by stimulating NO synthesis,33,34 but importantly our trial found no adverse effects on the PMNs. Activated platelets play a crucial role in the innate immune response during intravascular infection and platelet-neutrophil complexes are essential for infection control. However, in IE, an exaggerate immune response or inadequate infection control may promote the formation of platelet-neutrophil complexes, contributing to septic thrombosis.35 We observed that the number of activated platelets was decreased post-HBO2 and significantly at session 3 of HBO2 treatment. The number of platelet-neutrophil complexes was also decreased significantly at session 3 and 5, which could indicate a beneficial and protective immune response by HBO2 treatment, in regards oto thrombosis.
Strengths and Limitations
This trial is a phase I/II trial of the feasibility and safety of adjunctive HBO2 treatment in humans with IE, performed at two large centers in the Capital Region of Denmark. While we found that HBO2 treatment was feasible, with no registered SAE or SUSARs, the design and small number of patients and the lack of control group limits assessment the clinical effect, as the single-arm, non-comparative design does not allow for causal inference of the treatment and changes seen in biomarkers.
Median time from diagnosis to initiation of HBO2 treatment was 6 days due to inclusion criteria, practical setup in the hyperbaric chamber, and need for transfer of patients to the tertiary centre for inclusion. While all patients were considered to be in the initial stage of treatment for endocarditis, most were clinically stable with a CRP < 50 mmol/L. The timing of initiation of treatment might have influenced the effect of the HBO2 treatment and yielded smaller changes in biomarkers than if initiated immediately after diagnosis, yet might also decrease confounding from initiation of antibiotic treatment.
Conclusion
This phase I/II trial found HBO2 treatment for IE in selected patients to be feasible with no adverse effects. Significant changes were observed in biomarkers and key inflammatory markers, which might reflect effects from HBO2 treatment. Further studies are needed to verify these findings and determine if adjunctive HBO2 could help reduce IE’s high complication and mortality rates.
Data Sharing Statement
Due to Danish national legislation (Data Protection Act §10 and the Data Disclosure Proclamation Act), public deposition of raw data is not permitted. Pseudonymized data and study protocol can be made available upon reasonable request to corresponding author until June 2027, following approval by the Danish Data Protection Agency and in compliance with Capital Region data governance. Please contact corresponding authors for further information.
Acknowledgments
The assistance from the technical staff (chamber operators and tenders) at the pressure chamber unit is gratefully appreciated. Henning Bundgaard, Ole Hyldegaard, and Claus Moser shared last authorship.
Funding
This work was supported by “Rigshospitalets research foundation” under an unrestricted grant (no grant number). OH was supported by the PERAID (grant 8114-00005B), which is funded by Innovation Fund Denmark and NORDFORSK (Project 90456) and a research grant from Denmark’s Ellab-Fonden. CM has received funding from Novo Nordisk Fonden with ‘Borregaard Clinical Scientist Grant’ (Grant no. NNF17OC0025074). The funders had no role in the study’s data collection, analysis, or interpretation. Similarly, the funders and sponsors had no involvement in the study’s design, manuscript preparation, review and approval, or decision to submit the paper for publication.
Disclosure
EF reports grants from Novo Nordisk Foundation and the Danish Heart Association (unrelated to study). HB reports lecture fee from Amgen, MSD, BMS, Sanofi and Pfizer and grant from the Novo Nordic Foundation (unrelated to this study). CTP reports a grant from Bayer for a randomized study, and a grant from Novo Nordisk for an epidemiological study (unrelated to study). OH was supported by the PERAID (grant 8114-00005B), which is funded by Innovation Fund Denmark and NORDFORSK (Project 90456) and a research grant from Denmark’s Ellab-Fonden. CM reports payment for speaking engagements from AstraZeneca, GSK, MSD, and Pfizer; co-authorship of the Danish Treatment Guidelines for Infective Endocarditis and of the ESCMID guidelines for prevention, treatment, and diagnosis of biofilm infections; and service as a board member of the European Society for Clinical Microbiology Study Group (ESCMID) for Biofilms (ESGB). The authors report no other competing interests in this work.
References
1. Hammond-haley M, Hartley A, Al-khayatt BM, et al. Trends in the incidence and mortality of infective endocarditis in high-income countries between 1990 and 2019. Int J Cardiol. 2022;371:441–12. doi:10.1016/j.ijcard.2022.09.061
2. Hill EE, Herijgers P, Claus P, Vanderschueren S, Herregods M, Peetermans WE. Infective endocarditis: changing epidemiology and predictors of 6-month mortality: a prospective cohort study. European Heart Journal. 2007;28(2):196–203. doi:10.1093/eurheartj/ehl427
3. Erichsen P, Gislason GH, Bruun NE. The increasing incidence of infective endocarditis in Denmark, 1994–2011. Eur J Intern Med. 2016;35:95–99. doi:10.1016/j.ejim.2016.05.021
4. Østergaard L, Voldstedlund M, Bruun NE, et al. Temporal changes, patient characteristics, and mortality, according to microbiological cause of infective endocarditis: a nationwide study. J Am Heart Assoc. 2022;11(16). doi:10.1161/JAHA.122.025801
5. Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis. Eur Heart J. 2015;36(44):3075–3123. doi:10.1093/eurheartj/ehv319
6. Park LP, Chu VH, Peterson G, et al. Validated risk score for predicting 6-month mortality in infective endocarditis. J Am Heart Assoc. 2016;5(4):1–13. doi:10.1161/JAHA.115.003016
7. Østergaard L, Oestergaard LB, Lauridsen TK, et al. Long-term causes of death in patients with infective endocarditis who undergo medical therapy only or surgical treatment: a nationwide population-based study. Eur J Cardiothorac Surg. 2018;54(5):860–866. doi:10.1093/ejcts/ezy156
8. Thuny F, Giorgi R, Habachi R, et al. Excess mortality and morbidity in patients surviving infective endocarditis. Am Heart J. 2012;164(1):94–101. doi:10.1016/j.ahj.2012.04.003
9. Pries-Heje MM, Wiingaard C, Ihlemann N, et al. Five-Year Outcomes of the Partial Oral Treatment of Endocarditis (POET) trial. N Engl J Med. 2022;386(6):601–602. doi:10.1056/NEJMc2114046
10. Lerche CJ, Schwartz F, Theut M, et al. Anti-biofilm approach in infective endocarditis exposes new treatment strategies for improved outcome. Front Cell Dev Biol. 2021;9(June):1–25. doi:10.3389/fcell.2021.643335
11. Lerche CJ, Schwartz F, Pries-Heje MM, et al. Potential advances of adjunctive hyperbaric oxygen therapy in infective endocarditis. Front Cell Infect Microbiol. 2022;12(February):1–12. doi:10.3389/fcimb.2022.805964
12. Richard E, Moon M; Undersea and Hyperbaric Medical Society. Hyperbaric Oxygen Committee. Hyperbaric Oxygen Therapy Indications. 14th Ed. North Palm Beach, FL, USA: Best Publishing Company; 2019.
13. Lerche CJ, Christophersen LJ, Kolpen M, et al. Hyperbaric oxygen therapy augments tobramycin efficacy in experimental Staphylococcus aureus endocarditis. Int J Antimicrob Agents. 2017;50(3):406–412. doi:10.1016/j.ijantimicag.2017.04.025
14. Habib G, Erba PA, Iung B, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. 2019;40(39):3222–3232B. doi:10.1093/eurheartj/ehz620
15. Browne SK, Holland SM. Anticytokine autoantibodies in infectious diseases: pathogenesis and mechanisms. Lancet Infect Dis. 2010;10(12):875–885. doi:10.1016/S1473-3099(10)70196-1
16. Alfano D, Franco P, Stoppelli MP. Modulation of cellular function by the urokinase receptor signalling: a mechanistic view. Front Cell Dev Biol. 2022;10(April):1–20. doi:10.3389/fcell.2022.818616
17. Veloso TR, Chaouch A, Roger T, et al. Use of a human-like low-grade bacteremia model of experimental endocarditis to study the role of Staphylococcus aureus adhesins and platelet aggregation in early endocarditis. Infect Immun. 2013;81(3):697–703. doi:10.1128/IAI.01030-12
18. Apte RS, Chen DS, Ferrara N. VEGF in signaling and disease: beyond discovery and development. Cell. 2019;176(6):1248–1264. doi:10.1016/j.cell.2019.01.021
19. Hedetoft M, Moser C, Jensen PØ, Vinkel J, Hyldegaard O. Soluble ICAM-1 is modulated by hyperbaric oxygen treatment and correlates with disease severity and mortality in patients with necrotizing soft-tissue infection. J Appl Physiol. 2021;130(3):729–736. doi:10.1152/japplphysiol.00844.2020
20. Söderquist B, Sundqvist KG, Vikerfors T. Adhesion molecules (E-selectin, intercellular adhesion molecule-1 (ICAM- 1) and vascular cell adhesion molecule-1 (VCAM-1)) in sera from patients with Staphylococcus aureus bacteraemia with or without endocarditis. Clin Exp Immunol. 1999;118(3):408–411. doi:10.1046/j.1365-2249.1999.01081.x
21. Petriz J, Bradford JA, Ward MD. No lyse no wash flow cytometry for maximizing minimal sample preparation. Methods. 2018;134–135:149–163. doi:10.1016/j.ymeth.2017.12.012
22. Noble WS. How does multiple testing correction work? Nat Biotechnol. 2009;27(12):1135–1137. doi:10.1038/nbt1209-1135
23. Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC guidelines for the management of endocarditis. Eur Heart J. 2023;133(5):65–116. doi:10.1093/eurheartj/ehad193/7243107
24. Hedetoft M, Garred P, Madsen MB, Hyldegaard O. Hyperbaric oxygen treatment is associated with a decrease in cytokine levels in patients with necrotizing soft-tissue infection. Physiol Rep. 2021;9(6). doi:10.14814/phy2.14757
25. Vinkel J, Rib L, Buil A, Hedetoft M, Hyldegaard O. Key pathways and genes that are altered during treatment with hyperbaric oxygen in patients with sepsis due to necrotizing soft tissue infection (HBOmic study). Eur J Med Res. 2023;28(1):507. doi:10.1186/s40001-023-01466-z
26. Pries-Heje MM, Hasselbalch RB, Wiingaard C, et al. Severity of anaemia and association with all-cause mortality in patients with medically managed left-sided endocarditis. Heart. 2022;108(11):882–888. doi:10.1136/heartjnl-2021-319637
27. Vinkel J, Arenkiel B, Hyldegaard O. The mechanisms of action of hyperbaric oxygen in restoring host homeostasis during sepsis. Biomolecules. 2023;13(8):1228. doi:10.3390/biom13081228
28. Machoń NJ, Zdanowska N, Klimek-Trojan P, Owczarczyk-Saczonek A. Vascular cell adhesion molecule 1 and e-selectin as potential cardiovascular risk biomarkers in psoriasis. Int J Mol Sci. 2025;26(2):792. doi:10.3390/ijms26020792
29. Kendall AC, Whatmore JL, Winyard PG, Smerdon GR, Eggleton P. Hyperbaric oxygen treatment reduces neutrophil-endothelial adhesion in chronic wound conditions through S-nitrosation. Wound Repair Regen. 2013;21(6):860–868. doi:10.1111/wrr.12108
30. Buras JA, Stahl GL, Svoboda KKH, Reenstra WR. Hyperbaric oxygen downregulates ICAM-1 expression induced by hypoxia and hypoglycemia: the role of NOS. Am J Physiol Physiol. 2000;278(2):C292–302. doi:10.1152/ajpcell.2000.278.2.C292
31. Hemingway I, Pigoit R. Soluble forms of vascular pathological significance. Most. 0865:324–331.
32. Carlos BTM, Harlan JM. Leukocyte-endothelia1 adhesion molecules. Blood. 1994;84(7):2068–2101.
33. Thom SR, Bhopale VM, Velazquez OC, Goldstein LJ, Thom LH, Buerk DG. Stem cell mobilization by hyperbaric oxygen. Am J Physiol - Hear Circ Physiol. 2006;290(4):1378–1386. doi:10.1152/ajpheart.00888.2005
34. Heyboer M, Milovanova TN, Wojcik S, et al. CD34+/CD45-dim stem cell mobilization by hyperbaric oxygen - Changes with oxygen dosage. Stem Cell Res. 2014;12(3):638–645. doi:10.1016/j.scr.2014.02.005
35. Scherlinger M, Richez C, Tsokos GC, Boilard E, Blanco P. The role of platelets in immune-mediated inflammatory diseases. Nat Rev Immunol. 2023;23(8):495–510. doi:10.1038/s41577-023-00834-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.