")
Back to Journals » International Journal of General Medicine » Volume 16
Human Poisoning with Chlorpyrifos and Cypermethrin Pesticide Mixture: Assessment of Clinical Outcome of Cases Admitted in a Tertiary Care Hospital in Taiwan
Authors Wu YJ, Chang SS, Chen HY, Tsai KF, Lee WC, Wang IK , Lee CH , Chen CY, Liu SH, Weng CH , Huang WH, Hsu CW, Yen TH
Received 29 July 2023
Accepted for publication 12 October 2023
Published 26 October 2023 Volume 2023:16 Pages 4795—4804
DOI https://doi.org/10.2147/IJGM.S432861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandul Yasobant
Yi-Jan Wu,1,2 Shu-Sen Chang,3 Hsien-Yi Chen,4 Kai-Fan Tsai,2,5 Wen-Chin Lee,2,5 I-Kuan Wang,6,7 Chern-Horng Lee,8 Chao-Yu Chen,1,2 Shou-Hsuan Liu,1,2 Cheng-Hao Weng,1,2 Wen-Hung Huang,1,2 Ching-Wei Hsu,1,2 Tzung-Hai Yen1,2
1Department of Nephrology, Clinical Poison Center, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan City, Taiwan; 3Institute of Health Behaviors and Community Sciences, Department of Public Health, College of Public Health, National Taiwan University, Taipei City, Taiwan; 4Department of Emergency Medicine, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan; 5Division of Nephrology, Department of Internal Medicine, Chang Gung Memorial Hospital, Kaohsiung Branch, Kaohsiung City, Taiwan; 6Department of Nephrology, China Medical University Hospital, Taichung City, Taiwan; 7College of Medicine, China Medical University, Taichung City, Taiwan; 8Division of General Internal Medicine and Geriatrics, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan
Correspondence: Tzung-Hai Yen, Department of Nephrology, Clinical Poison Center, Chang Gung Memorial Hospital, Linkou Branch, 5 Fu-Hsing Street, Kweishan, Taoyuan City, Taiwan, Tel +886 3 3281200 ext 8181, Fax +886 3 3282173, Email [email protected]
Background and Purpose: There is an overall paucity of data regarding the human toxicity of chlorpyrifos and cypermethrin pesticide mixture. Both organophosphate and pyrethroid insecticides are metabolized by carboxylesterases. Thus, its pesticide combination, organophosphates may boost the toxicity of pyrethroids via inhibited its detoxification by carboxylesterases. This study examined the clinical course, laboratory tests, and outcomes of patients with chlorpyrifos, cypermethrin or their pesticide mixture poisoning, and to determine what association, if any, might exist between these findings.
Patients and Methods: Between 2000 and 2021, 121 patients poisoned with chlorpyrifos, cypermethrin, or their pesticide mixture were treated at Chang Gung Memorial Hospital. Patients were categorized as chlorpyrifos (n=82), cypermethrin (n=27) or chlorpyrifos and cypermethrin (n=12) groups. Demographic, clinical, laboratory and mortality data were collected for analysis.
Results: The patients experienced a broad range of clinical symptoms, including aspiration pneumonia (44.6%), salivation (42.5%), acute respiratory failure (41.3%), acute kidney injury (13.9%), seizures (7.5%), hypotension (2.6%), etc. Leukocytosis (12,700± 6600 /uL) and elevated serum C-reactive protein level (36.8± 50.4 mg/L) were common. The acute respiratory failure rate was 41.3%, comprising 48.8% in chlorpyrifos, 11.1% in cypermethrin as well as 58.3% in chlorpyrifos and cypermethrin poisoning. Patients with chlorpyrifos and cypermethrin pesticide mixture poisoning suffered higher rates of acute respiratory failure (P=0.001) and salivation (P=0.001), but lower Glasgow Coma Scale score (P=0.011) and serum cholinesterase level (P< 0.001) than other groups. A total of 17 (14.0%) patients expired. The mortality rate was 14.0%, including 17.1% in chlorpyrifos, 3.7% in cypermethrin as well as 16.7% in chlorpyrifos and cypermethrin poisoning. No significant differences in mortality rate were noted (P=0.214).
Conclusion: Chlorpyrifos pesticide accounted for the major toxicity of the pesticide mixture. While the data show a higher rate of respiratory failure in the chlorpyrifos and cypermethrin pesticide mixture group than others, other measures of toxicity such as mortality and length of stay were not increased.
Keywords: chlorpyrifos, cypermethrin, pesticide mixture, poisoning, acute respiratory failure, mortality
Introduction
Organophosphate pesticides such as chlorpyrifos are powerful cholinesterase inhibitors that are able to induce severe cholinergic toxicity by skin contact, inhalation, or gastrointestinal ingestion.1 These chemicals work by inhibiting the activity of the enzyme acetylcholinesterase, leading to an excess of the neurotransmitter acetylcholine in the body.2 Chlorpyrifos is a widespread name for the chemical 0,0-diethyl 0-(3,5,6-trichloro-2-pyridinyl)-phosphorothioate. The initial step in the metabolism of organophosphate compounds involves the liver enzyme cytochrome P450 (CYP450)-dependent oxidative desulfuration, which converts them into chlorpyrifos-oxon, an active anticholinesterase compound. Subsequently, paraoxonase, an A-esterase, hydrolyzes chlorpyrifos-oxon into 3,5,6-trichloro-2-pyridinol (TCPy), an inactive metabolite that serves as the primary metabolite of chlorpyrifos, which is specific enough to be used as a biomarker of exposure. TCPy is then preferentially eliminated from the body through urine. Diethylphosphate, diethylthiophosphate could also be generated in this metabolic pathway.3
Acute cholinergic crisis happens speedily after organophosphate exposure owing to the acetylcholinesterase inhibition and the features involve nicotinic and muscarinic signs and symptoms.4
Pyrethrin pesticides are derived from the flower of Chrysanthemum cinerariifolium.5 The pyrethrins work by targeting the nervous systems of insects, but are considered less poisonous to mammals than organophosphates.5 Pyrethroid is an organic composite that derived from natural pyrethrins. Synthetic pyrethroids such as cypermethrin have been used as an insecticide in agricultural sector. It behaves as a fast-acting neurotoxin in insects. The effects of which are mediated through preventing the closure of the voltage-gated of sodium channels in the axonal membranes.5 Symptoms of acute poisoning may manifest as dizziness, loss of appetite, fatigue, nausea, vomiting, and unusual sensations in the face.6 These abnormal facial sensations are often described as burning, itching, or tingling, and they can become more intense when sweating or washing with warm water.6 Fortunately, they typically subside within a few hours to a day after exposure. The more serious cases developed coarse muscular fasciculations in large muscles of extremities, conscious disturbance, twilight state or coma.6
In 2006, Tripathi et al7 reported the outcomes of eight Nepal patients due to suicidal ingestion of an illegal mixing pesticide of organophosphate and pyrethroid. The details of the pesticide were not described. After treatment, seven of the patients recovered without chronic complications. One patient died of aspiration pneumonia. As shown in Table 1, clinical research on the toxicity of chlorpyrifos and cypermethrin pesticide mixture poisoning are sparse in the literature, and confined to one original research.1,8–13 In a retrospective study of pesticide poisoning database, Iyyadurai et al12 presented that patients with chlorpyrifos and cypermethrin pesticide mixture poisoning suffered lesser ventilator-free days than patients poisoned by either of the pesticides alone. The mortality rate was not significantly different among the three groups. Furthermore, Srinivasan et al14 reported a case of a 23-year-old Indian female chlorpyrifos and cypermethrin pesticide mixture poisoning who suffered delayed neuropathy for two years. Moreover, Gupta et al15 described a 13-year-old Indian girl of chlorpyrifos and cypermethrin pesticide mixture poisoning, where the cholinergic features continued manifesting till 3 weeks after exposure of poison.
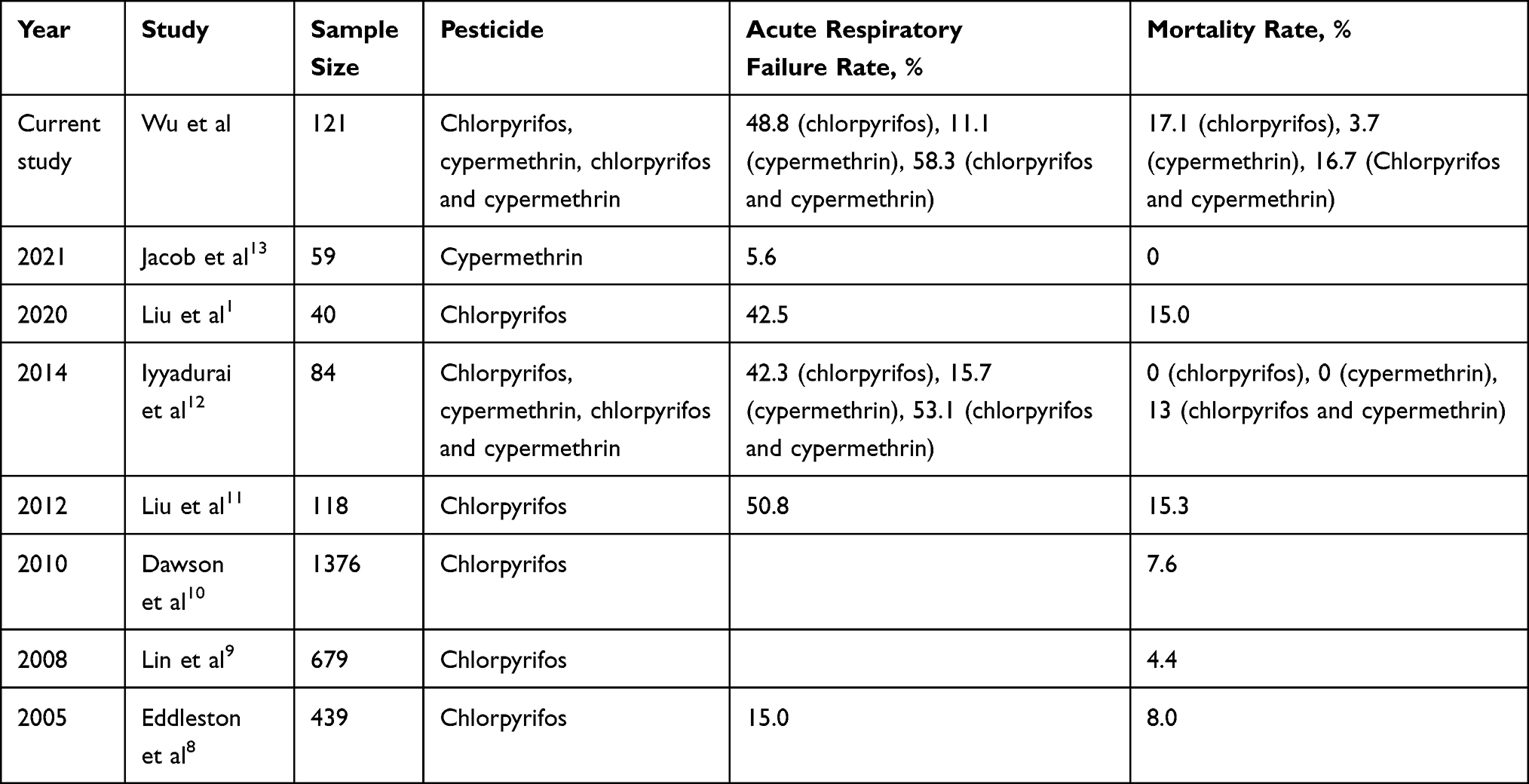 |
Table 1 Published Literatures on the Medical Complications of Chlorpyrifos and Cypermethrin Poisoning |
In Taiwan, pesticide poisoning remains a prevalent concern. According to epidemiological data spanning from 1985 to 1993, documented by The Taiwan National Poison Center, there were 6872 reported cases of human pesticide exposure within an eight-year period. Pesticide exposures constituted the biggest single category, accounting for 29.3% of all reported toxic substances exposures in Taiwan. This category encompassed various types of pesticides, including insecticides, rodenticides, and herbicides.16 A more recent study covering the period from July 1985 to December 2006 revealed 4799 cases of human organophosphate exposure over approximately 21 years, as reported by Taiwan’s Poison Control Center. This highlights the ongoing significance of this issue and underscores the need for continued vigilance and attention to pesticide-related health risks.9 On the contrary, in Japan, there were 221 fatalities due to pesticide poisoning in 2019, which marked a significant decrease from the 2648 fatalities reported in 1986. This remarkable reduction of 92% over a span of 33 years can likely be attributed to a combination of factors, including the decreased utilization of highly hazardous pesticides and the adoption of lower-concentration formulations.17
The rationale for this research was based on an important, but as yet unanswered, question that arose for many chlorpyrifos-poisoned patients receiving treatment at our hospital. Organophosphate compound could be absorbed via the inhalation, skin, and in the digestive tract.18 Human organophosphate poisoning could contribute to serious outcomes, which depended on ingested amount. Symptoms of organophosphate poisoning comprise muscle twitching, weakness, excessive bronchial secretions and respiratory failure. Neuromuscular blockade and cerebral depression may also develop and contribute to respiratory failure, consciousness disturbance and mortality.4,19 Pyrethroids, on the other hand are considered safer, although some respiratory failure or mortality cases have been described. Nevertheless, reports on the human toxicity of chlorpyrifos and cypermethrin pesticide mixture have been limited and inconclusive. Pyrethroid insecticides are typically broken down by carboxylesterases into inactive metabolites. However, in the case of chlorpyrifos, it can be converted into chlorpyrifos oxon, a potent inhibitor of carboxylesterases. As a result, chlorpyrifos oxon has the potential to effectively block the initial breakdown of permethrin, leading to an increase in its insecticidal effectiveness.20
Organophosphates may boost the toxicity of pyrethroids via inhibited its detoxification by carboxylesterases.20 Therefore, this hospital-based retrospective study examined the clinical course, laboratory tests, and outcomes of patients with chlorpyrifos, cypermethrin or their pesticide mixture poisoning, and to determine what association, if any, might exist between these findings.
Materials and Methods
Institutional Review Board Statement
The analyses in this retrospective cohort study complied with the guidelines of the Declaration of Helsinki and were approved by the Medical Ethics Committee of Chang Gung Memorial Hospital (Institutional Review Board No.: 202002502B0). As this was a retrospective study based on the assessment of existing data, the committee waived the requirement for informed consent from the patients. All personal data were available only to the investigators and were secured by delinking the recognition information from the main dataset.
Patients
Between 2000 and 2021, a total of 121 patients poisoned with chlorpyrifos, cypermethrin, or their pesticide mixture were treated at Chang Gung Memorial Hospital, a tertiary referral hospital that had a capacity of nearly 3700 beds and approximately 100,000 annual admissions in Taiwan. Patients were classified into three groups based on the type of pesticide, as chlorpyrifos (n = 82), cypermethrin (n = 27) or chlorpyrifos and cypermethrin (n = 12). All exposures were via the oral route. Demographic, clinical, laboratory and mortality data were recorded for analysis.
Inclusion and Exclusion Criteria
All patients were analyzed. Patients were excluded if they had ingested pesticides other than chlorpyrifos or cypermethrin, or if their exposure was not via oral route.
Diagnosis of Pesticide Poisoning
The diagnosis was based on the exposure history, clinical features, physical examinations, and laboratory results. According to database of Animal and Plant Health Inspection Agency, Ministry of Agriculture in Taiwan, chlorpyrifos pesticide was normally supplied as 22.5%, 25%, 40.8%, 44.9% or 50% (w/w). Cypermethrin pesticide was normally supplied as 5% or 10% (w/w). On the other hand, chlorpyrifos and cypermethrin pesticide mixture was available as 25% or 50% (w/w).21 To determine serum cholinesterase levels, an enzymatic method (DF51, Siemens Healthcare Diagnostics, Newark, Delaware, USA) was applied, with a normal levels of 7–19 U/mL and a detection level of 0.8 U/mL.1 The serum cholinesterase activity was used to diagnose organophosphate poisoning, but the test was not specific to chlorpyrifos. Due to blood chlorpyrifos and cypermethrin measurements were unavailable at our hospital, a thorough clinical exposure history was taken, which incorporated questioning the patient and family about the pesticide label image and asking the pesticide bottle for confirmation.
Detoxification Protocols
Gastric lavage was performed if the patient arrived within 1 hour after pesticide ingestion. The contraindications for gastric lavage comprise loss of airway protective reflexes, ingestion of a strong acid or alkali, or risk of gastrointestinal bleeding due to an underlying illness.22 Chlorpyrifos patients with acute cholinergic crisis were treated with anticholinergic and oxime drugs, including atropine (2 mg, intravenously, increased as required to resolve bronchial secretions and bronchospasm) and pralidoxime (1 g every 4 hours, intravenously). There is no antidote available for cypermethrin poisoning, and its treatment was largely symptomatic and supportive.
Statistical Analysis
Comparisons of categorical variable among the three pesticide groups were conducted using trend estimation. A one-way analysis of variance was used when assessing for differences in one continuous variable between the three groups. The criterion for significance was a 95% confidence interval to reject the null hypothesis. All analyses were performed with SPSS 19.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
As shown in Table 2, the patients aged 55.2 ± 17.5 years and most were male (69.5%). The majority of patients ingested the pesticides by intention (94.2%), and they arrived 4.6 ± 9.2 hours after pesticide ingestion. The reason for patients who accidentally ingesting pesticides (5.8%) was they forgot and simply grab the pesticides that were previously stored in a bottle. Their occupations were mainly non-farmer 95 (81.9%). There were 87 (75%) married, and 29 (25%) unmarried, divorced, widowed. There were no significant differences in baseline demographic variables between three groups.
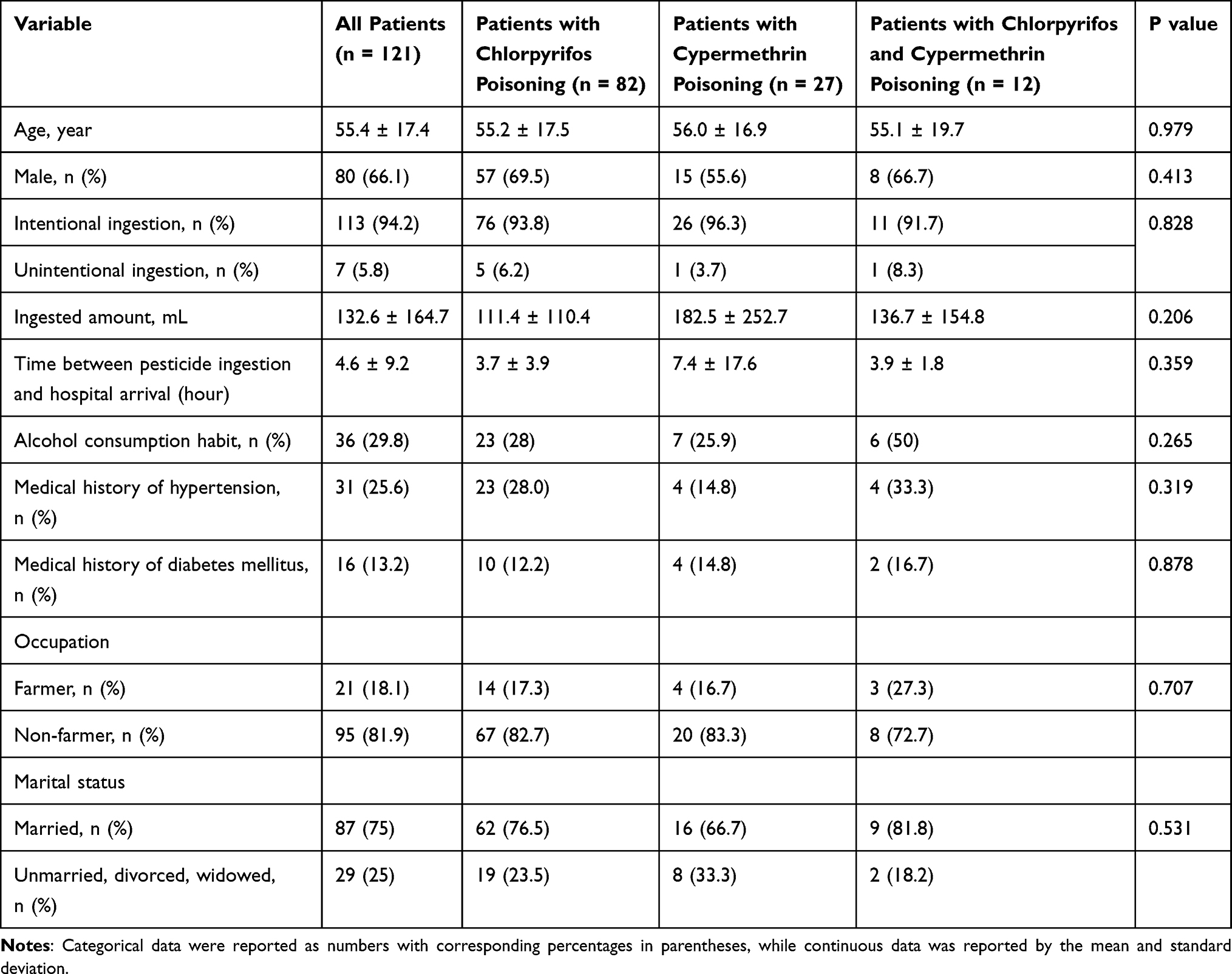 |
Table 2 Baseline Characteristics of Patients with Pesticide Poisoning, Stratified by Type of Pesticide (n = 121) |
Following ingestion (Table 3), the patients experienced a broad range of clinical symptoms, including aspiration pneumonia (44.6%), salivation (42.5%), acute respiratory failure (41.3%), acute kidney injury (13.9%), seizures (7.5%), hypotension (2.6%), etc. After analysis, it was found that patients with chlorpyrifos and cypermethrin pesticide mixture poisoning suffered higher rates of salivation (P = 0.001) and acute respiratory failure (P = 0.001), but lower Glasgow Coma Scale score (P = 0.011) than other groups. Furthermore, patients with chlorpyrifos poisoning suffered higher rates of aspiration pneumonia (P < 0.001) and salivation (P < 0.001) than other groups. No significant differences were observed for other clinical variables.
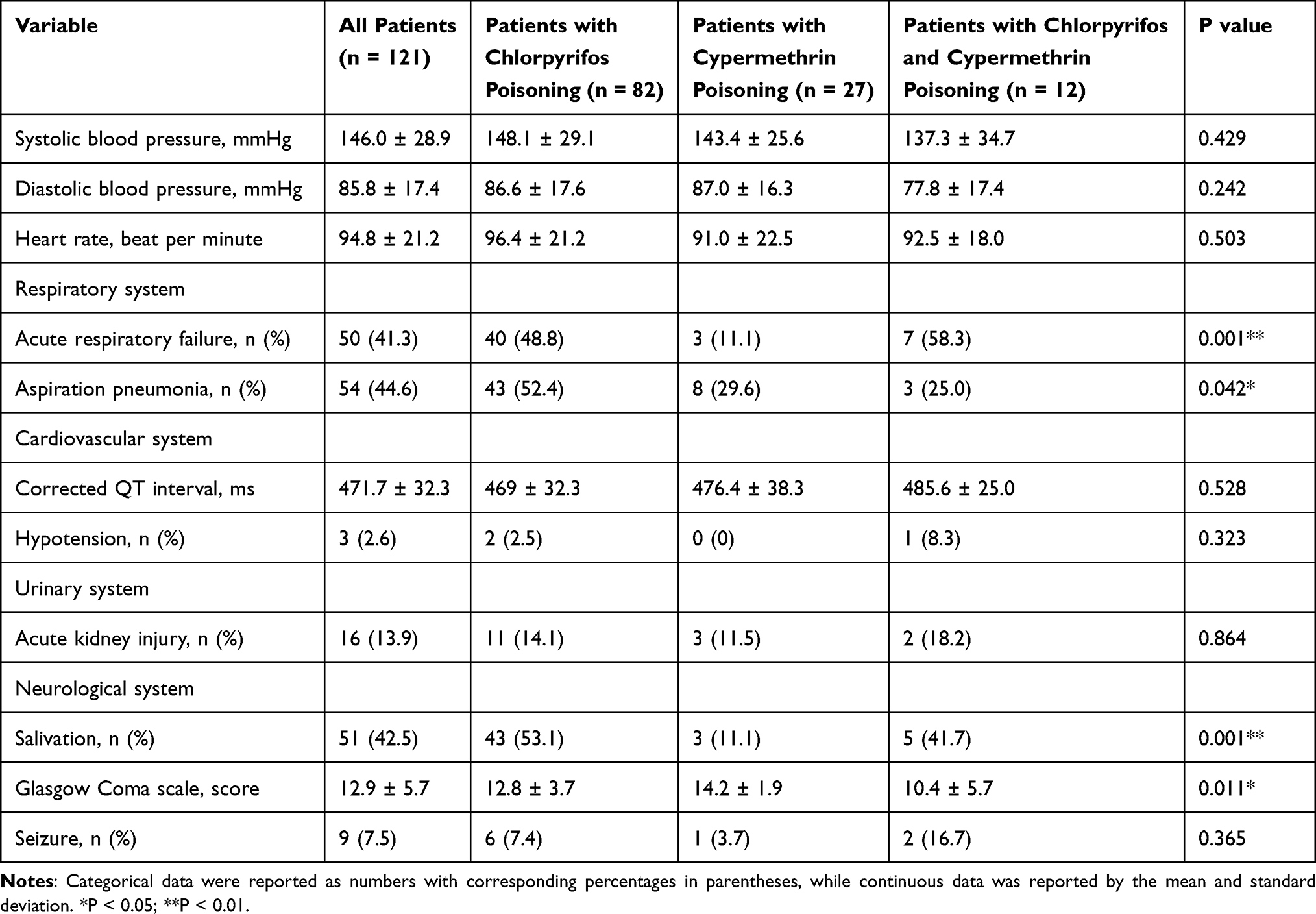 |
Table 3 Clinical Manifestations of Patients with Pesticide Poisoning, Stratified by Type of Pesticide (n = 121) |
Table 4 showed that leukocytosis (12,700 ± 6600 /uL) and elevated serum C-reactive protein level (36.8 ± 50.4 mg/L) were common after pesticide poisoning. Furthermore, it was found that patients with chlorpyrifos poisoning suffered lower serum cholinesterase level than other groups (P < 0.001). No significant differences were observed for other laboratory variables.
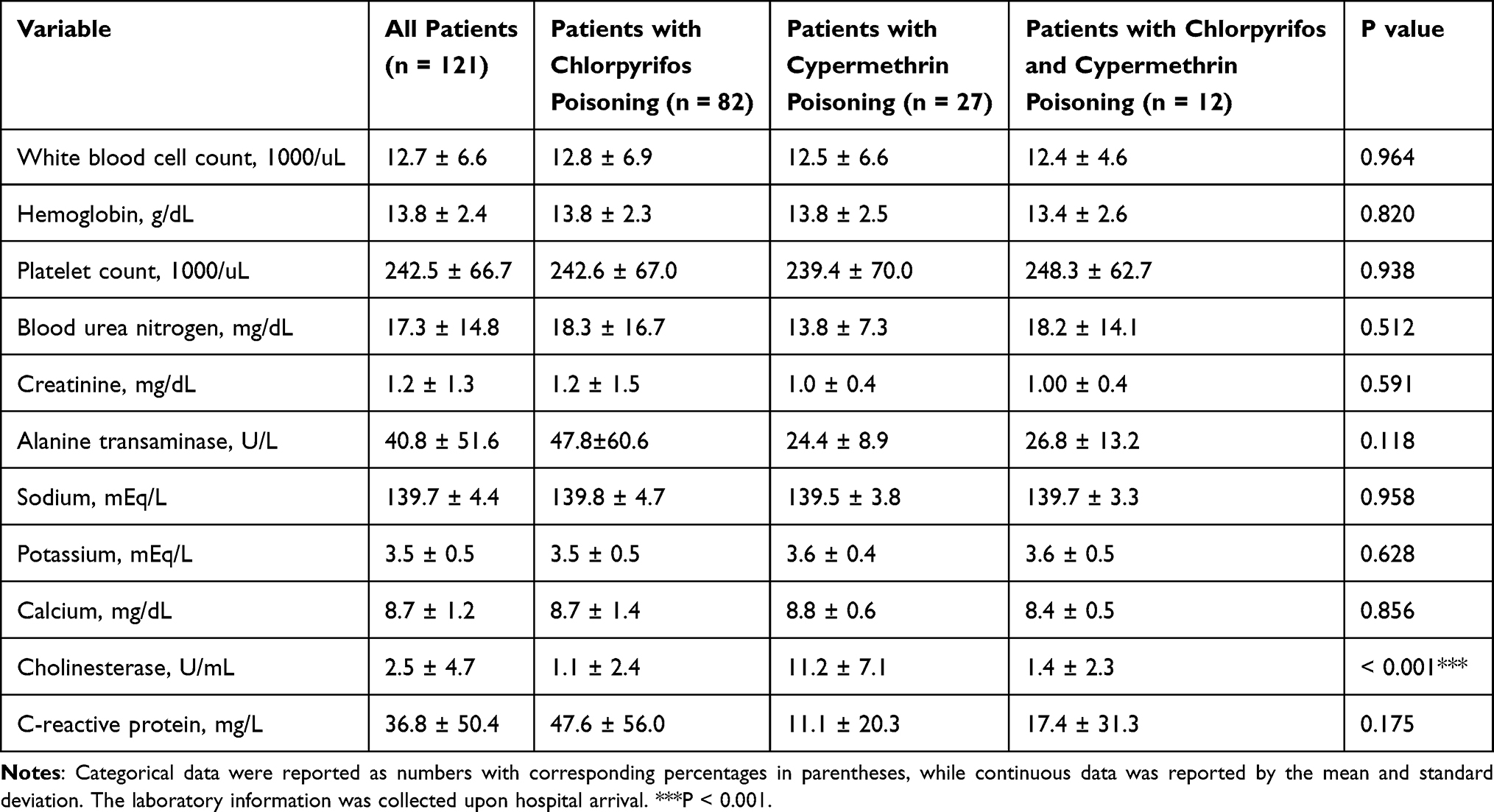 |
Table 4 Laboratory Data of Patients with Pesticide Poisoning, Stratified by Type of Pesticide (n = 121) |
As shown in Table 5, a total of 17 (14.0%) patients expired. The mean duration of hospitalization was 17.9 ± 15.8 days, and the mean duration of intensive care unit hospitalization was 9.4 ± 10.1 days. After analysis, it was found that patients with chlorpyrifos poisoning had longer duration of hospitalization than other groups (P = 0.001). Nevertheless, there were no significant differences in mortality rate among the three groups (P = 0.214).
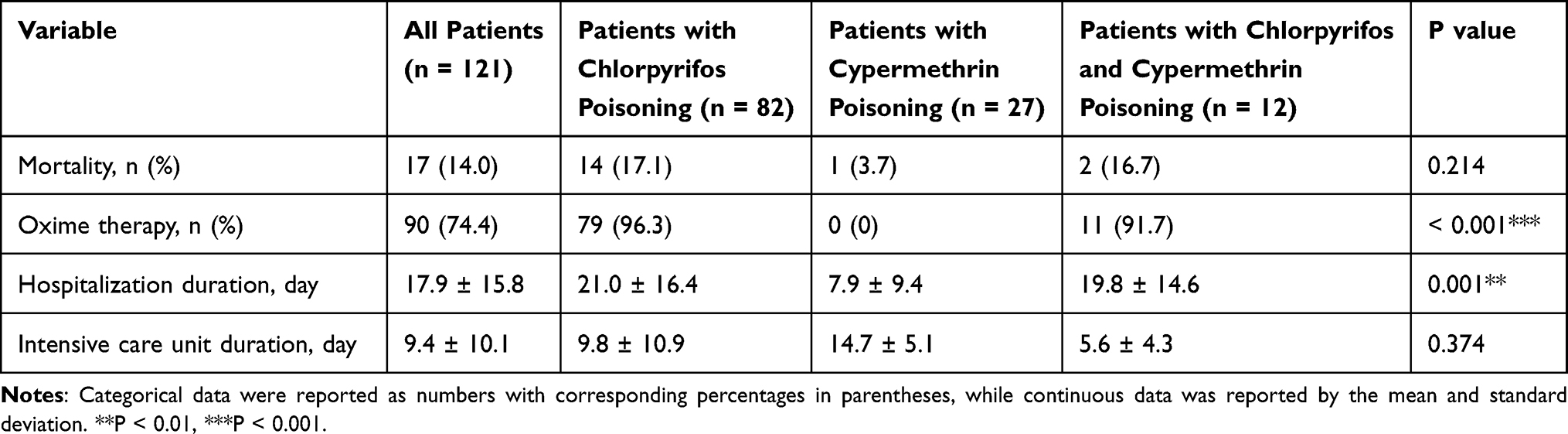 |
Table 5 Outcomes of Patients with Pesticide Poisoning, Stratified by Type of Pesticide (n = 121) |
Discussion
Chlorpyrifos was the most widely used pesticide in agricultural sector in the world, but is also one of the most controversial pesticides in its use.23 The debate appears to be the inconsistency between the clinical findings and the conclusions drawn for the pesticide’s approval in data reporting the toxicity of chlorpyrifos on human health.24 In Taiwan, the Agricultural Chemicals and Toxic Substances Research Institute released a ban on the production of chlorpyrifos, which took effect in April 2022.25 Additionally, the government will ban the usage of this pesticide by January 2026. Similarly, the chlorpyrifos and cypermethrin pesticide mixture had been banned from production in December 2022, and will be banned from use in April 2024. In August 2021, the Environmental Protection Agency (EPA) had forbidden the use of chlorpyrifos on food crops in the United States.26 In December 2019, the European Union announced that it would no longer permit sales of chlorpyrifos after January 2020.27
As shown in Table 2, the acute respiratory failure rate was 41.3%, comprising 48.8% in chlorpyrifos, 11.1% in cypermethrin as well as 58.3% in chlorpyrifos and cypermethrin poisoning. The respiratory failure rate was lower in cypermethrin group than other groups, and this was in line with other studies. In the study by Iyyadurai et al,12 the respiratory failure rates were 42.3%, 15.7%, and 53.1%, in chlorpyrifos, cypermethrin as well as chlorpyrifos and cypermethrin, respectively. The respiratory failure rates were 15.0%, 50.8%, and 42.5% after chlorpyrifos poisoning in three other studies.1,8,11 Moreover, Jacob et al13 disclosed that only 5.6% of patients with cypermethrin poisoning developed acute respiratory failure. Chlorpyrifos associated respiratory failure can be classified into two types depending on the time of onset after exposure.19 Central and peripheral mechanisms are implicated the pathogenesis of respiration inhibition. Studies have proposed that the major mechanisms regulating early respiratory failure associated with organophosphate absorption are in the central nerve system. Excess acetylcholine can depress respiratory activity in the respiratory center, which induces respiratory paralysis.19 On the other hand, mechanisms for late respiratory failure consist of peripheral dysfunction due to the continued overstimulation of the neuromuscular junction. Peripheral acetylcholine at neuromuscular junction produces voluntary muscle weakness and fasciculations, which inducing late respiratory failure.28
Nearly half of the patients (44.6%) developed aspiration pneumonia in this study. Aspiration pneumonia is a common complication of pesticide poisoning, which may contribute to acute lung injury and mortality. Published incidence rates of aspiration pneumonia following organophosphate intoxication range from 21% to 43.5%.29–31 Reddy et al32 reported 16 cases of respiratory distress to aspiration pneumonia in young children after accidental ingestion of mosquito repellants containing pyrethroid, but the study attributed the pulmonary complication to hydrocarbon ingredients rather than pyrethroid as the causative agent. Excess mucosal fluid secretion, vomiting and consciousness change increased the possibility of aspiration pneumonia after pesticide exposure.33,34
As shown in Table 5, the mortality rate was 14.0%, including 17.1% in chlorpyrifos, 3.7% in cypermethrin as well as 16.7% in chlorpyrifos and cypermethrin poisoning. Nevertheless, there were no significant differences in mortality rates among the three pesticide groups (P = 0.214). The mortality rate was lower in cypermethrin group than other groups, and this was in line with other studies (Table 1). Iyyadurai et al12 found that patients with chlorpyrifos, cypermethrin as well as chlorpyrifos and cypermethrin poisoning suffered mortality rate of 0%, 0%, and 13.0%, respectively. The mortality rates were ranged between 4.4 and 15.3% following chlorpyrifos poisoning according to other studies.1,8–11 None of the cypermethrin patients expired according to the Jacob study.13
Leukocytosis (12,700 ± 6600 per uL) and elevated serum C-reactive protein level (36.8 ± 50.4 mg/L) were common after pesticide poisoning (Table 4). Furthermore, chlorpyrifos and cypermethrin pesticide mixture group suffered higher incidences of salivation (P = 0.001) and lower Glasgow Coma Scale score (P = 0.011) and serum cholinesterase level (P < 0.001) than other groups (Tables 3 and 4). The observations could be explained by the toxicity of pesticide compounds. Salivation may develop after acute cholinergic crisis, neuromuscular blockade and cerebral depression. Acute cholinergic crisis always develops promptly after organophosphate exposure. Neuromuscular blockade and brain depression may develop and contribute to respiratory failure, consciousness disturbance and mortality.19 Besides, type II pyrethroids can produce a severe syndrome typified by salivation and choreoathetosis in laboratory animals.35 In addition, Lin et al36 also presented that the death organophosphate group had a higher white blood cell count than the survival group.
Pesticide self-poisoning is a widely used means of suicide, and one of the most popular approaches of suicide worldwide.37 It comprises an important public health issue in Asian nations.38 Suicide by intentional ingestion of pesticides is common in Taiwan because of easy access.39,40 Pesticide poisoning accounted for the third most common suicide method in Taiwan during 2002–2009.40 In this study, it was found that the occupation of farming was relatively low (18.1%). In contrast, the percentage of intentional poisoning was relatively high (94.2%). The results of the study were in line with previous researches on pesticide poisoning in Taiwan, which reported that the percentage of pesticide poisoning among farmers (20%–32.4%) was lower compared to non-farmers (67.6%–80.0%).1,34 This maybe shows that non-agricultural Taiwanese have access to pesticide, and can easily gain pesticide for self-poisoning.40 Previous analysis from our group38 also revealed that the selection of pesticides employed in self-poisoning is associated with pesticide availability rather than intentional selection. Thus, it is suggested that the government should take proper measure to not only forbidding highly poisonous pesticides, but also to control access to pesticides for prevention of self-poisoning.41
The standard approach to treating organophosphate poisoning consists of two primary phases. The first stage involves supportive care, which encompasses resuscitation, mechanical ventilation, decontamination, and, when necessary, hemodialysis.42 The second stage involves pharmacological interventions. The treatments for organophosphate poisoning include atropine as the initial antidote, oximes for reactivating acetylcholinesterase, typically administered in conjunction with atropine, benzodiazepines for managing seizures, and pyridostigmine as the primary prophylactic agent.42 On the other hand, the treatment approach for pyrethroid poisoning primarily involves providing supportive and symptomatic care. Ensuring the optimization of the patient’s airway, breathing, and circulation is of utmost importance, as it is for any individual with acute poisoning. While immediate decontamination of the skin with soap and water can be taken into consideration, it’s worth noting that there is no conclusive evidence demonstrating its effectiveness in reducing toxicity.5 In cases of pyrethroid ingestion, it is advisable to avoid gastric lavage due to the heightened risk of aspiration pneumonia associated with the solvent. The use of activated charcoal has limited supporting evidence; however, it can be considered if the patient seeks medical attention within one hour of ingestion.5 Our study revealed that 96.3% of patients with chlorpyrifos poisoning received oxime therapy at our hospital, and 91.7% of patients with chlorpyrifos and cypermethrin poisoning underwent the same treatment. This underscores the high level of vigilance and expertise in our emergency department when it comes to pesticide poisoning. Once the specific pesticide poisoning type is confirmed, our medical team promptly administers the appropriate treatment.
Our study contributed to expanding the current limited understanding of the human toxicity of chlorpyrifos and cypermethrin pesticide mixture by reporting on the medical complications and mortality data. Nevertheless, this study was limited by retrospective study design, small sample size and short follow-up duration. Meanwhile, the lack of information on blood chlorpyrifos and cypermethrin concentrations as well as pesticide surfactant analysis may limit the extrapolation of the findings of our study. Further research is needed.
Conclusion
Chlorpyrifos pesticide accounted for the major toxicity of the pesticide mixture. While the data show a higher rate of respiratory failure in the chlorpyrifos and cypermethrin pesticide mixture group than others, other measures of toxicity such as mortality and length of stay were not increased.
Funding
This research was funded by Chang Gung Memorial Hospital, grant number CORPG3M0391 and CORPG3K0194.
Disclosure
The authors report no conflict of interest.
References
1. Liu HF, Ku CH, Chang SS, et al. Outcome of patients with chlorpyrifos intoxication. Hum Exp Toxicol. 2020;39(10):1291–1300. doi:10.1177/0960327120920911
2. Kwong TC Organophosphate pesticides: biochemistry and clinical toxicology. Ther Drug Monit. 2002;24(1):144–149. doi:10.1097/00007691-200202000-00022
3. Wielgomas B, Krechniak J. Toxicokinetic Interactions of α-Cypermethrin and Chlorpyrifos in Rats. Pol J Environ. 2007;16(2):267–274.
4. Chung YL, Hou YC, Wang IK, Lu KC, Yen TH. Organophosphate pesticides and new-onset diabetes mellitus: from molecular mechanisms to a possible therapeutic perspective. World J Diabetes. 2021;12(11):1818–1831. doi:10.4239/wjd.v12.i11.1818
5. Ramchandra AM, Chacko B, Victor PJ. Pyrethroid Poisoning. Indian J Crit Care Med. 2019;23(4):S267–S271. doi:10.5005/jp-journals-10071-23304
6. He F, Wang S, Liu L, Chen S, Zhang Z, Sun J. Clinical manifestations and diagnosis of acute pyrethroid poisoning. Arch Toxicol. 1989;63(1):54–58. doi:10.1007/bf00334635
7. Tripathi M, Pandey R, Ambesh SP, Pandey M. A mixture of organophosphate and pyrethroid intoxication requiring intensive care unit admission: a diagnostic dilemma and therapeutic approach. Anesth Analg. 2006;103(2):410–2. doi:10.1213/01.ane.0000222470.89210.5a
8. Eddleston M, Eyer P, Worek F, et al. Differences between organophosphorus insecticides in human self-poisoning: a prospective cohort study. Lancet. 2005;366(9495):1452–9. doi:10.1016/S0140-6736(05)67598-8
9. Lin TJ, Walter FG, Hung DZ, et al. Epidemiology of organophosphate pesticide poisoning in Taiwan. Clin Toxicol (Phila). 2008;46(9):794–801. doi:10.1080/15563650801986695
10. Dawson AH, Eddleston M, Senarathna L, et al. Acute human lethal toxicity of agricultural pesticides: a prospective cohort study. PLoS Med. 2010;7(10):e1000357. doi:10.1371/journal.pmed.1000357
11. Liu SH, Lin JL, Weng CH, et al. Heart rate-corrected QT interval helps predict mortality after intentional organophosphate poisoning. PLoS One. 2012;7(5):e36576. doi:10.1371/journal.pone.0036576
12. Iyyadurai R, Peter JV, Immanuel S, et al. Organophosphate-pyrethroid combination pesticides may be associated with increased toxicity in human poisoning compared to either pesticide alone. Clin Toxicol. 2014. 52(5):538–541. doi:10.3109/15563650.2014.909933
13. Jacob MS, Iyyadurai R, Jose A, et al. Clinical presentation of type 1 and type 2 pyrethroid poisoning in humans. Clin Toxicol. 2022;60(4):464–471. doi:10.1080/15563650.2021.1994145
14. Srinivasan M, Amin R, Thunga G, Nagiri SK, Kudru CU. Pharmacokinetic potentiation of mixed organophosphate and pyrethroid poison leading to prolonged delayed neuropathy. J Clin Diagn Res. 2016;10(11):FD01–FD02. doi:10.7860/JCDR/2016/22756.8773
15. Gupta B, Kerai S, Khan I. Organophosphate-pyrethroid combined poisoning may be associated with prolonged cholinergic symptoms compared to either poison alone. Indian J Anaesth. 2018;62(11):903–905. doi:10.4103/ija.IJA_338_18
16. Yang CC, Wu JF, Ong HC, et al. Taiwan national poison center: epidemiologic data 1985–1993. J Toxicol Clin Toxicol. 1996;34(6):651–663. doi:10.3109/15563659609013825
17. Eddleston M, Nagami H, Lin CY, Davis ML, Chang SS. Pesticide use, agricultural outputs, and pesticide poisoning deaths in Japan. Clin Toxicol (Phila). 2022;60(8):933–941. doi:10.1080/15563650.2022.2064868
18. Robb EL, Baker MB. Organophosphate Toxicity. StatPearls; 2023.
19. Giyanwani PR, Zubair U, Salam O, Zubair Z. Respiratory failure following organophosphate poisoning: a literature review. Cureus. 2017;9(9):e1651. doi:10.7759/cureus.1651
20. Hernandez AF, Parron T, Tsatsakis AM, Requena M, Alarcon R, Lopez-Guarnido O. Toxic effects of pesticide mixtures at a molecular level: their relevance to human health. Toxicology. 2013;307:136–145. doi:10.1016/j.tox.2012.06.009
21. Taiwan Aaphiamoai. Animal and plant health inspection agency ministry of agriculture in Taiwan. Available from: https://pesticide.aphia.gov.tw/information/Query/Pesticide. Accessed September 22, 2023.
22. Vale JA, Kulig K. Position paper: gastric lavage. J Toxicol Clin Toxicol. 2004;42(7):933–943.
23. Sheppard L, McGrew S, Fenske RA. Flawed analysis of an intentional human dosing study and its impact on chlorpyrifos risk assessments. Environ Int. 2020;143:105905. doi:10.1016/j.envint.2020.105905
24. Wolejko E, Lozowicka B, Jablonska-Trypuc A, Pietruszynska M, Wydro U. Chlorpyrifos occurrence and toxicological risk assessment: a review. Int J Environ Res Public Health. 2022;19:19. doi:10.3390/ijerph191912209
25. Taiwan Agricultural Chemicals and Toxic Substances Research Institute. 歷年政府禁用農藥一覽表 [List of banned pesticides in Taiwan]. Artcle in Mandarin. Available from: https://www.tactri.gov.tw/Item/Detail/.
26. U.S. Environmental Protection Agency. Chlorpyrifos. Available from: https://www.epa.gov/ingredients-used-pesticide-products/chlorpyrifos.
27. European Union to Ban Chlorpyrifos after January 31, 2020. Available from: https://pesticideblog.lawbc.com/entry/european-union-to-ban-chlorpyrifos-after-january-31-2020.
28. Gupta RC, Dettbarn WD. Potential of memantine, D-tubocurarine, and atropine in preventing acute toxic myopathy induced by organophosphate nerve agents: soman, sarin, tabun and VX. Neurotoxicology Fall. 1992;13(3):649–661.
29. Wang CY, Wu CL, Tsan YT, Hsu JY, Hung DZ, Wang CH. Early onset pneumonia in patients with cholinesterase inhibitor poisoning. Respirology. 2010;15(6):961–968. doi:10.1111/j.1440-1843.2010.01806.x
30. Moon J, Chun B, Song K. An exploratory study; the therapeutic effects of premixed activated charcoal-sorbitol administration in patients poisoned with organophosphate pesticide. Clin Toxicol (Phila). 2015;53(2):119–126. doi:10.3109/15563650.2014.1001516
31. Sun IO, Yoon HJ, Lee KY. Prognostic factors in cholinesterase inhibitor poisoning. Med Sci Monit. 2015;21:2900–2904. doi:10.12659/MSM.894287
32. Reddy MV, Ganesan SL, Narayanan K, et al. Liquid mosquito repellent ingestion in children. Indian J Pediatr. 2020;87(1):12–16. doi:10.1007/s12098-019-03088-y
33. Hulse EJ, Clutton RE, Drummond G, et al. Lung injury caused by aspiration of organophosphorus insecticide and gastric contents in pigs. Clin Toxicol (Phila). 2022;60(6):725–736. doi:10.1080/15563650.2022.2028803
34. Yu JR, Hou YC, Fu JF, et al. Outcomes of elderly patients with organophosphate intoxication. Sci Rep. 2021;11(1):11615. doi:10.1038/s41598-021-91230-2
35. Martinez-Larranaga MR, Anadon A, Martinez MA, Martinez M, Castellano VJ, Diaz MJ. 5-HT loss in rat brain by type II pyrethroid insecticides. Toxicol Ind Health. 2003;19(7–10):147–155. doi:10.1191/0748233703th184oa
36. Lin TJ, Jiang DD, Chan HM, Hung DZ, Li HP. Prognostic factors of organophosphate poisoning between the death and survival groups. Kaohsiung J Med Sci. 2007;23(4):176–182. doi:10.1016/S1607-551X(09)70394-8
37. Huang WC, Yen TH, Lin L, et al. Clinical characteristics of pesticide self-harm as associated with suicide attempt repetition status. Neuropsychiatr Dis Treat. 2020;16:1717–1726. doi:10.2147/NDT.S258475
38. Tu CY, Yen TH, Chang CM, et al. Characteristics and psychopathology of 1086 patients who self-poisoned using pesticides in Taiwan (2012–2019): a comparison across pesticide groups. J Affect Disord. 2022;300:17–26. doi:10.1016/j.jad.2021.12.058
39. Yen JS, Wang IK, Liang CC, et al. Cytokine changes in fatal cases of paraquat poisoning. Am J Transl Res. 2021;13(10):11571–11584.
40. Chang SS, Lu TH, Sterne JA, Eddleston M, Lin JJ, Gunnell D. The impact of pesticide suicide on the geographic distribution of suicide in Taiwan: a spatial analysis. BMC Public Health. 2012;12(1):260. doi:10.1186/1471-2458-12-260
41. Liang CA, Chang SS, Chen HY, et al. Human poisoning with methomyl and cypermethrin pesticide mixture. Toxics. 2023;11:4. doi:10.3390/toxics11040372
42. Alozi M, Rawas-Qalaji M. Treating organophosphates poisoning: management challenges and potential solutions. Crit Rev Toxicol. 2020;50(9):764–779. doi:10.1080/10408444.2020.1837069
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.