")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
How Ready are Pediatricians and Family Physicians in Saudi Arabia to Perform Clinical Screening of Developmental Dysplasia of the Hip?
Authors Suqaty R , Alomran AK , Alkhalifah MK , Aldughaythir SS , Albeshry AM, Aldilaijan Y , Alzahrani MT , Alhussainan T
Received 10 April 2023
Accepted for publication 21 August 2023
Published 30 August 2023 Volume 2023:16 Pages 2567—2576
DOI https://doi.org/10.2147/JMDH.S416459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rayyan Suqaty,1 Ammar K Alomran,2 Mohammed K Alkhalifah,3 Saad S Aldughaythir,4 Abdulrahman M Albeshry,5 Yousif Aldilaijan,6 Mohammed T Alzahrani,1 Thamer Alhussainan1
1Department of Orthopedic Surgery, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia; 2Department of Orthopedics, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 3Department of Family Medicine & Polyclinics King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; 4Department of Pediatrics, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; 5Department of Family and Community Medicine, Faculty of Medicine, University of Jeddah, Jeddah, Saudi Arabia; 6Primary Health Care Centers, Eastern Health Cluster, Khobar, Saudi Arabia
Correspondence: Thamer Alhussainan, Department of Orthopedic Surgery, King Faisal Specialist Hospital & Research Center, Al Mathar Ash Shamali, Riyadh, 11564, Saudi Arabia, Tel +966504181881, Fax +96614414839, Email [email protected]
Background: Developmental dysplasia of the hip (DDH) is one of the most common hip pathologies in pediatric age group and late diagnosis remains a major concern in Saudi Arabia.
Objective: The aim of this study is to examine the ability of Saudi Arabian pediatricians and family physicians to conduct clinical screening for (DDH) by estimating their clinical knowledge and skills and analyzing the gaps therein to determine whether there is potential to launch a national screening protocol for DDH in Saudi Arabia.
Methods: This is a multicenter cross-sectional study from three major regions in Saudi Arabia (Central, Eastern and Western provinces). The assessed aspects are risk factors, age of screening, incidence in Saudi Arabia, physical signs and diagnostic markers, and treatment, along with their ‘clinical knowledge and skills’ score.
Results: Half of the participants were pediatricians, while the rest were family physicians. More than a third of the participants were considered to have adequate knowledge, ie, above the mean score. Dimensions with the most significant knowledge gaps included the incidence of DDH in Saudi Arabia, adverse effects of swaddling, and the management of a high-risk infants presenting with a negative physical examination. Additionally, there were relatively low rates of awareness regarding positive risk factors as well as a generally poor ability to identify physical signs. Clinical knowledge and skill levels were significantly lower among family physicians.
Conclusion: Pediatricians and family physicians in Saudi Arabia still need further training to improve their clinical skills for DDH screening. The proper administration of training programs could eventually enable the gradual implementation of a national systematic screening program.
Keywords: orthopedic, pediatrics, observational study, pediatricians, family physicians, developmental dysplasia of the hip
A Letter to the Editor has been published for this article.
Introduction
Developmental dysplasia of the hip (DDH) is one of the most common developmental defects leading to childhood disability. It is defined by clinical and subclinical abnormalities in the shape, size, and/or orientation of the femoral head, acetabulum, or both, leading to postnatal developmental problems with hip articulation and, ultimately, function.1–3 The incidence of DDH varies greatly across countries and ethnic groups; reported cases have increased dramatically in the past few decades due to the use of ultrasound imaging and systematic screening.2 Recently, incidence rates of 2.4–6.7 per 1000 newborns have been reported in Europe and the United States.4–8 In Saudi Arabia, a systematic review found an average prevalence of DDH of 10.5 per 1000 newborns during the period 1980–2018, with most cases being diagnosed late, after 12 months of age, due to inadequate screening. This increased prevalence was associated with high rates of consanguinity and family history.8
Although mild forms of DDH, which cause minor hip instability, commonly resolve before the third month of life, severely unstable and dislocated forms progress and lead to other anatomical and functional changes in soft tissue and bone structures.9,10 Therefore, early diagnosis and timely management are essential to improve functional prognosis and prevent long-term complications. Systematic screening programs using different approaches that combine clinical examinations and imaging have been implemented worldwide and show efficacy in improving early detection and reducing the complications associated with late-detected or uncorrected DDH.11 Although comparative studies of different screening approaches suggested no superiority of any method over the other,11,12 an international interdisciplinary consensus, in 2019, advocated for universal ultrasound-based screening of DDH, notably by using the Graf method both to diagnose and classify the defect.13 However, regardless of the method adopted, successful screening is based above all on the physicians’ knowledge of DDH risk factors and on their clinical skills in performing adequate physical examinations to detect abnormal signs and assess their significance.1,3,10,14
In current practice, and despite the presumably high prevalence of DDH in Saudi Arabia, the clinical screening of DDH follows no clear guidelines. It is usually conducted either by nurses or physicians (family physicians or pediatricians) responsible for the well-baby clinic. It usually occurs during the systematic assessment and screening of the infant for other diseases and the completion of mandatory vaccination. In a view to improve the practice, this study examined the preparedness of Saudi pediatricians and family physicians to conduct clinical screening for DDH with the goal of evaluating the potential and assets to a national screening program. The levels of knowledge about the risk factors, gaps therein, basic physical examination skills, and management parameters were explored and compared between disciplines.
Methods
Design and Population
A national cross-sectional study was conducted in August 2019 and informed consent was obtained before starting the Supplementary Questionnaire from the specialists, consultant pediatricians, and family physicians working in the public or private sectors of three regions of the Central, Eastern and Western provinces of Saudi Arabia from January 2019 to May 2020. The study was approved by the institutional review board of our institution.
The sample size (N=65) was calculated to detect an unknown percentage (p=0.5) of participants with adequate knowledge and skills in DDH screening among family physicians and pediatricians in Saudi Arabia with a 95% confidence interval (CI), 80% statistical power, and 20% type 2 error. A stratified sampling was used to include an equivalent number of family physicians and pediatricians (~200 in each group). Every center in each region participated in the study.
Data Collection
A structured Supplementary Questionnaire was designed to assess the clinical knowledge and skills (CKS) of these physicians in the detection of DDH. The survey included 11 questions covering the following topics: one question on the incidence of DDH in Saudi Arabia (one correct answer out of five); one question on the appropriate age for screening (one correct answer out of five); two questions on risk factors, including one on previously suggested factors (seven correct answers out of 13), and another on those that should dictate further evaluation (two correct answers out of 13); two questions regarding physical examination, including one about physical signs (five correct answers out of eight), and another about the diagnostic value of hip click (two correct answers out of four); two questions regarding the most appropriate management of two different presentations, one with risk factors but with a negative physical examination (one correct answer out of five) and another with a positive physical examination (one correct answer out of four); two questions about swaddling, including one about awareness of its effects on the development of the hip and lower limb (one correct option out of four) and another regarding the practical attitude and advice the participant should give the mother of a swaddled infant (one correct option out of three); and one question on self-assessed confidence in performing hip instability tests, including Ortolani and Barlow maneuvers (four levels of confidence).
The Supplementary Questionnaire was verified in terms of structure and content by two independent pediatricians and a pilot test was carried out among 10 physicians to test the clarity of its items.
The Supplementary Questionnaire also collected data on the sex and home region of the participants, as well as on their professional and academic credentials, including specialty (pediatrician versus family physician), academic level (specialist, consultant), and exposure to DDH screening in routine practice.
The Supplementary Questionnaire was edited for use online and was administered through the REDCap survey platform of KFSH&RC.
Statistical Methods
Statistical analysis was performed with SPSS version 21 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to examine the responses to the different parts of the Supplementary Questionnaire. Categorical variables are presented as frequencies and percentages, while numerical variables are presented as means ± standard deviation (SD).
An accuracy score (range 0–1) was calculated for each of the 11 questions as the number of correct answers divided by the total number of possible answers to a given question. Accuracy scores were compared between pediatricians and family physicians using an independent t-test; results are presented as mean (SD). A CKS score (range 0–100) was calculated as the sum of accuracy scores divided by 11 and multiplied by 100; the higher the score, the higher the expertise of the participant. An adequate CKS level was defined as a CKS score above the mean population score or the theoretical mean (50/100), whichever is higher. The factors relative to the CKS were analyzed by comparing both CKS scores and the percentage of overall adequate CKS scores between regions, sex, disciplines, academic levels and exposure to DDH screening programs using one-way ANOVA or independent t-tests and chi-square, respectively. A p-value <0.05 was considered to reject the null hypothesis.
Results
Characteristics of the Participants
A total of 410 participants completed the survey, 56.3% of whom were women. There was a low participation rate for residents (8.5%) and a high participation rate for consultants (56.3%). The distribution of participants was fair in both disciplines and regions, as shown in Table 1.
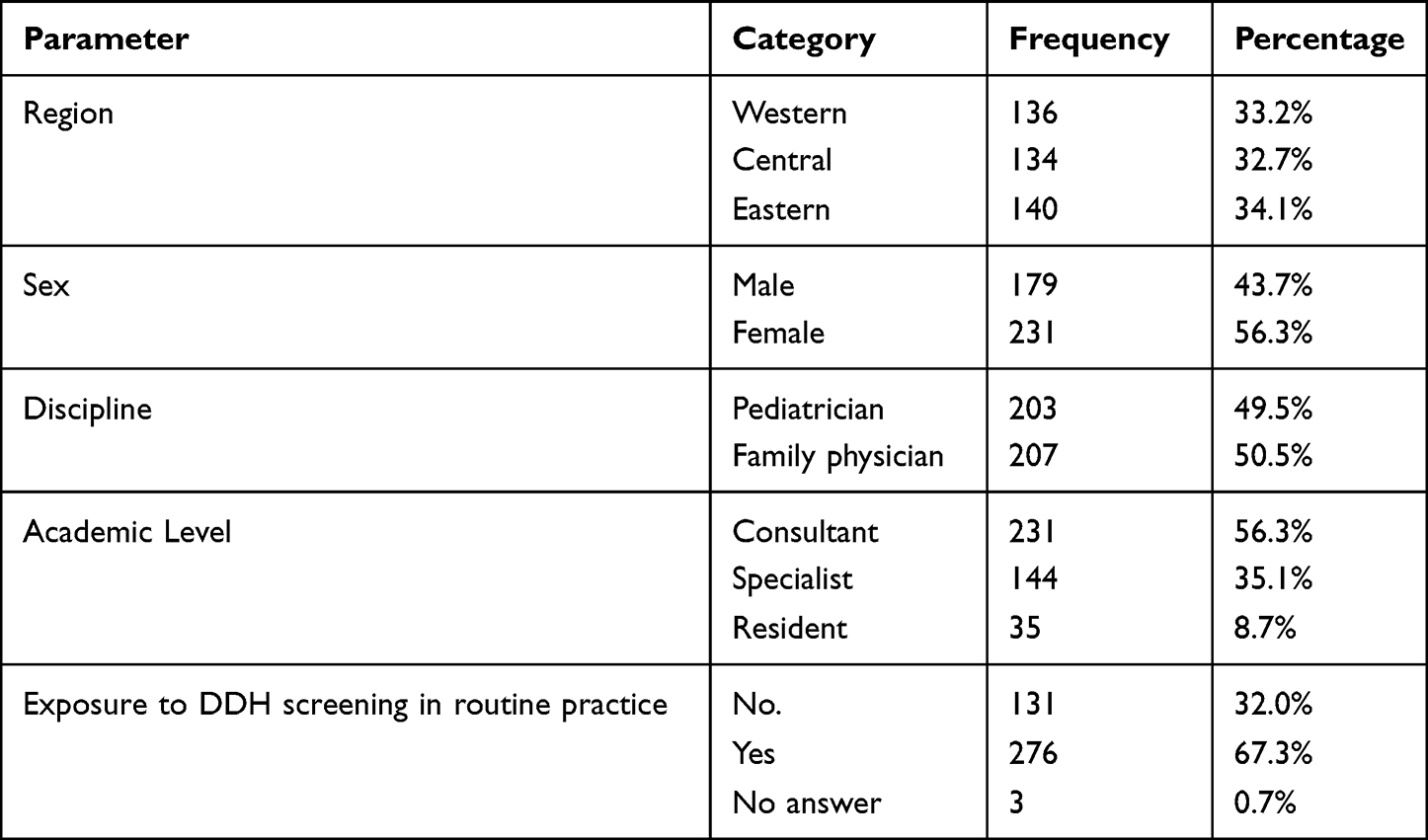 |
Table 1 Participant Characteristics |
Assessment of Knowledge and Skills
The mean CKS score of the study population was 53.8 (SD=11.6); the mean was significantly higher among pediatricians (57.5 [SD=12.1]) than among family physicians (50.2 [SD=9.9]) (P<0.001). The dimensions with the most significant knowledge and skill gaps included the incidence of DDH in Saudi Arabia (mean=0.10), adverse effects of swaddling (0.22), and the management of a high-risk infant presenting with a negative physical examination (0.24). Family physicians scored lower than pediatricians in these categories, but statistical significance was only observed in the latter two. The dimension with the highest score was the identification of currently considered risk factors (mean= 0.83), with no observable differences between the two disciplines (P=0.903) (Table 2). The percentage of participants who achieved adequate CKS (defined as a CKS score <54/100) in the detection of DDH was 41%.
 |
Table 2 Accuracy of Responses in Different Knowledge Dimensions in the Total Study Population and in Pediatricians versus Family Physicians |
Specific knowledge about currently considered risk factors (among 13 suggestions) and physical signs (among 8 suggestions) are presented in Figures 1 and 2, respectively. Figure 1 shows the relatively low rates of correct identification of the following currently considered risk factors: breech delivery/breech position in the third trimester (68.5%), family history of DDH (65.9%), and correct exclusion of female sex (55.9%) as a risk factor. All other factors were correctly excluded by >70% of the participants. Figure 2 shows the lower rates of correct identification of the five physical signs of DDH (30.7–60.2%); all other signs were correctly excluded by >90% of the participants.
 |
Figure 1 Knowledge among pediatricians and family physicians in Saudi Arabia about the risk factors currently considered for Hip developmental dysplasia in infants. Bars represent the percentage of participants who correctly identified (dark bars) or correctly excluded (light bars) the given factor. |
 |
Figure 2 Knowledge among pediatricians and family physicians in Saudi Arabia about physical signs of developmental dysplasia of the Hip in infants. Bars represent the percentage of participants who correctly identified (dark bars) or correctly excluded (light bars) the given sign. |
Factors Associated with Overall Knowledge and Skills
The levels of CKS in DDH screening were significantly higher among pediatricians (P<0.001 and P<0.001) participants from the Central region (P<0.001 and P=0.008), and those who are routinely exposed to DDH screening (P<0.001 and P<0.001); this was determined by comparing their scores with their counterparts and by comparing both CKS scores and adequacy rates, respectively.
Furthermore, the level of self-reported confidence in performing Ortolani and Barlow maneuvers was significantly predictive of both the CKS score (P<0.001) and the adequacy rate (P<0.001) (Table 3). To explain the higher levels of CKS in the Central region, a contingency table analysis showed a fair distribution of discipline by region with a chi-square P-value=0.765.
 |
Table 3 Factors Associated with Clinical Knowledge and Skills in Screening for Developmental Dysplasia of the Hip in Infants |
Discussion
Several DDH screening programs have been implemented using different techniques but without much evidence-based support, leading to controversy, particularly regarding imaging criteria and discrimination between abnormal findings and normal developmental variants of the hip.15 Therefore, clinical screening remains a key investigation in the absence of national guidelines. This national survey estimated the preparedness of pediatricians and family physicians to perform clinical screening for DDH in Saudi Arabian infants. It showed low levels of CKS among nearly 60% of the participants, with relatively higher proficiencies among pediatricians and participants from the central region of the country. Most participants indicated inadequate knowledge of the position of the breech and positive family history as risk factors, as well as physical signs of DDH. Exposure to DDH screening in routine practice was associated with better knowledge and skills, and the level of self-reported confidence in performing Ortolani and Barlow maneuvers was positively correlated with the level of overall CKS.
The most significant knowledge gap was related to the incidence of DDH in Saudi Arabia, which was correctly identified by only 10% of the participants. Notwithstanding the methodological limitations of national studies, DDH incidence is reported to be 1.5-times higher in Saudi Arabia than in international studies; a dramatically higher proportion of these cases are diagnosed with functional disorders at walking age.4–8 Furthermore, in terms of the apparently low detection rates and the specific epidemiological and social factors, which combine high consanguinity rates and the public prevalence of swaddling,8,16 these incidence rates, although very high, may underestimate the real figures. As such, DDH should be considered a public health problem in Saudi Arabia and would benefit from significant interest from authorities and healthcare providers.
The second most significant gap concerned the negative effect of swaddling, which was correctly identified by 22% of the participants. Swaddling, especially when done tightly and involving the lower extremities, is considered a risk factor for DDH and predisposing to dysplasia.17–19 Infant swaddling is common in the Middle East, including Saudi Arabia, where majority of the mothers are unaware of its relationship with DDH.20 Furthermore, a study using dynamic ultrasound estimated the effect of different swaddling techniques on hip instability and showed that swaddling restricting leg motion is associated with an increased risk of hip instability and dislocation.21 Inadequate awareness of physicians about these negative effects observed in this study could impact the education of the mothers. In our survey, providing accurate advice on swaddling yielded a very low knowledge score, which stresses the need to educate physicians, especially those in primary pediatric and obstetric care, in order to increase patient awareness of the general adverse effects of swaddling while emphasizing incorrect techniques.
The third most significant gap was related to the management of a high-risk infant presenting a normal physical examination; only 24% of the participants (29% of pediatricians and 20% of family physicians) indicated that they would request an ultrasound examination of the hip and refer the infant to pediatric orthopedics at six weeks of age for further examination. Although little evidence supports this practice, the 2019 International Consensus recommended universal screening between 4 and 6 weeks of age, in the absence of risk factors.13 Early referral to specialists is encouraged to optimize diagnosis and treatment and prevent reconstructive surgery.15,22 This practice should be promoted even more in Saudi Arabia given the inadequate levels of clinical skills among primary care pediatricians and family physicians, as confirmed in this study. Furthermore, the sensitivity of the physical examination has not been well documented, and once undertaken, great variations are to be expected based on the level of expertise and skills of the physician. A recent Italian study, based on the International Consensus, demonstrated a very low sensitivity of clinical examination in diagnosing DDH, with reference to universal ultrasound screening.23 Authors incriminated the lack of adequate training in pediatrics schools on DDH, which is consistent with our observations. Local data indicate that the diagnosis of DDH is delayed in most cases, which is attributable to social factors and inadequate parental awareness, but also to limited screening due to the absence of a national screening program.8,16,24 The present study complements these data and highlights the need to enhance the knowledge and skills of primary physicians to create a foundation for a successful screening program.
Although several factors have been associated with DDH, the most recent evidence suggests that breech presentation in the third trimester and a positive family history are the most significant. These two factors are associated with DDH with an odds ratio of 5.7 and 4.8, respectively, as demonstrated by a meta-analysis.14 In the present study, approximately one-third of the physicians failed to identify these two risk factors. More importantly, a high percentage of breech infants are found to have residual dysplasia at approximately six months of age, even with an initially stable hip and negative early ultrasound.10,25 This provides strong justification for intensifying the investigation and monitoring of such babies to secure their hips while awaiting definitive diagnosis. Similarly, a positive family history should be systematically determined, especially in populations with high rates of consanguinity, such as Saudi Arabia, where high percentages of familial forms of DDH have been reported.18,19,26 Several studies have established the association of pedigrees from families with DDH with a number of gene variants, such as COL1A1, GDF5, HOXB9, IL6, and HOXD9, and in chemokine receptor genes (CX3CR1).27 In the Saudi population, the SNP rs143383 variant of the GDF5 gene in both its homozygous and heterozygous forms has been associated with a higher risk of DDH.28 This further indicates the relevance of genetic screening and counseling in populations with high rates of family history of DDH.
Besides stressing awareness and active investigation of risk factors as keys to enhancing proper clinical screening, our observations raise the prognostic value of these risk factors, even with negative findings in early physical examination and ultrasound imaging. Most pediatricians and family physicians did not identify the proper management in case of normal physical examination of a high-risk infant. Conversely, most clinicians indicated that they would request ultrasound imaging and refer the infant to pediatric orthopedics in case of abnormal physical examination. This suggests that, for the participants, finding of the physical examination prevail over the diagnostic and prognostic values of the major risk factors. This misconception should be addressed, as it de-emphasizes high-risk patients with negative early screenings. Furthermore, findings of the physical examination are operator-dependent and depend on the physician’s competency, which reduces their reliability. Therefore, in the context of Saudi Arabia, early and systematic referral of high-risk patients to experts and pediatric orthopedists should be promoted.
On the other hand, our study revealed a moderate-to-fair level of knowledge of physical signs and relatively high self-reported confidence in performing Ortolani and Barlow maneuvers, which are simple methods used to assess hip stability and to detect a dislocated femoral head, respectively.15,29 Approximately 60% of the participants in this study considered a hip click as a positive sign of DDH; its clinical significance was correctly associated with the Ortolani and Barlow maneuvers with an accuracy score=0.63/1. These findings could be considered encouraging, except that there was a weak correlation between the two questions (Pearson’s coefficient=0.30, P<0.001) in the responses of the participants. Furthermore, neither of the two questions was correlated with the confidence in performing the maneuvers (Pearson’s correlation<0.1, P>0.500), which signifies that the physicians most confident in performing these maneuvers are not those who are most aware of the importance of hip click. This indicates an inconsistency in the knowledge of physical examinations and the unreliability of self-reported levels of practice, which affects the trustworthiness of the most optimistic findings in this dimension. Further studies are warranted to provide a more accurate assessment of the levels of practice in clinical screening for DDH and to address this inconsistency between theoretical knowledge and self-reported practice.
There was a significant difference in CKS levels in DDH between pediatricians and family physicians: 52.2% of pediatricians had an adequate level of CKS compared to only 30% of family physicians. The most significant knowledge gaps among family physicians compared to pediatricians (>.1-score difference) were related to appropriate screening age, effects of swaddling, and the management of infants with positive physical examination, in addition to self-reported confidence in performing Ortolani and Barlow maneuvers. These differences may reflect the levels of exposure to DDH screening in routine practice. Further subgroup analysis showed a higher exposure to DDH screening in pediatricians (73.1%) as compared to family physicians (62.6%), with a statistically significant difference (P=0.023). In our opinion, and in view of the other findings, these differences are not large enough to justify specific measures for family physicians. Rather, both disciplines should be involved in national training programs to increase awareness and skills of physicians to the required level for an appropriate clinical screening. This program should be completed with the implementation of a standard decision tree and a reliable referral system to optimize early diagnosis and management.
The method used to determine the levels of knowledge and skills and the set of included questions could lead to validity concerns and impact the generalizability of the findings. The major limitation is that the Supplementary Questionnaire and its related scale are not validated by the scientific community, which may hinder the external consistency of the findings. Nevertheless, the Supplementary Questionnaire was designed to cover the most important basic and practical issues that physicians must consider estimating their readiness to perform DDH screening; it was not intended to provide an accurate evaluation of their level of practice. The latter issue requires additional studies, as mentioned above.
Conclusions
Pediatricians and family physicians in Saudi Arabia are currently not ready to perform clinical screenings for DDH due to inadequacies and inconsistencies in their knowledge and skills. More remarkably, there is suboptimal awareness of risk factors and their diagnostic value, and inconsistent knowledge of physical examination and indications of different clinical signs. Given the high incidence of DDH in Saudi Arabia, it is urgent to implement a stepwise national strategy that culminates in an effective and systematic screening program. This process should begin with efficient training of primary care physicians involved in newborn assessment to improve their awareness of the condition and its risk factors, as well as their clinical screening practices. This should be supported by the implementation of a standard decision tree and a reliable referral system to optimize early diagnosis and management. Well-trained physicians could educate parents about the risk factors for DDH, especially swaddling and a positive family history, which in turn would trigger their participation in prophylaxis and monitoring of high-risk infants. Obstetricians and healthcare providers who work in family planning and antenatal care could be involved in a multidisciplinary approach and have also become involved in parental education and genetic counseling.
Strengths and Limitations
- This was a national study that involved participants from 3 regions of the Kingdom.
- Level of knowledge was assessed using a multidimensional scale covering the most important basic and practical issues about DDH.
- The reliability of the assessment of practice and skills may be questionable.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available upon request to the corresponding author Thamer S. Alhussainan ([email protected]).
Ethics Approval and Consent to Participate
All methods were performed in accordance with the relevant guidelines of Research Ethical Committee of King Faisal Hospital and Research center – Riyadh Saudi Arabia (Approval Number: RAC#2191282).
An electronic informed consent was obtained before starting the Supplementary Questionnaire from survey participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Noordin S, Umer M, Hafeez K, et al. Developmental dysplasia of the Hip. Orthop Rev. 2010;2:e19. doi:10.4081/or.2010.e19
2. Dezateux C, Rosendahl K. Developmental dysplasia of the Hip. Lancet. 2007;369:1541–1552. doi:10.1016/S0140-6736(07)60710-7
3. Kotlarsky P. Developmental dysplasia of the Hip: what has changed in the last 20 years? World J Orthop. 2015;6:886–901. doi:10.5312/wjo.v6.i11.886
4. Woodacre T, Ball T, Cox P. Epidemiology of developmental dysplasia of the Hip within the UK: refining the risk factors. J Child Orthop. 2016;10:633–642. doi:10.1007/s11832-016-0798-5
5. Pollet V, Percy V, Prior HJ. Relative risk and incidence for developmental dysplasia of the Hip. J Pediatr. 2017;181:202–207. doi:10.1016/j.jpeds.2016.10.017
6. Loder RT, Skopelja EN. The epidemiology and demographics of Hip dysplasia. ISRN Orthop. 2011;238607. doi:10.5402/2011/238607
7. Kolb A, Schweiger N, Mailath-Pokorny M, et al. Low incidence of early developmental dysplasia of the Hip in universal ultrasonographic screening of newborns: analysis and evaluation of risk factors. Int Orthop. 2016;40:123–127. doi:10.1007/s00264-015-2799-2
8. Sadat-Ali M. Developmental dysplasia of the Hip (DDH) in Saudi Arabia: time to wake up. A systematic review (1980–2018). Open J Epidemiol. 2020;10:125–131. doi:10.4236/ojepi.2020.102011
9. Vitale MG, Skaggs DL. Developmental dysplasia of the Hip from six months to four years of age. J Am Acad Orthop Surg. 2001;9:401–411. doi:10.5435/00124635-200111000-00005
10. Schwend RM, Shaw BA, Segal LS. Evaluation and treatment of developmental Hip dysplasia in the newborn and infant. Pediatr Clin North Am. 2014;61:1095–1107. doi:10.1016/j.pcl.2014.08.008
11. Shorter D, Hong T, Osborn DA. Cochrane review: screening programmes for developmental dysplasia of the Hip in newborn infants. Evid Based Child Health. 2013;8:11–54. doi:10.1002/ebch.1891
12. Sewell MD, Eastwood DM. Screening and treatment in developmental dysplasia of the Hip—where do we go from here? Int Orthop. 2011;35:1359–1367. doi:10.1007/s00264-011-1257-z
13. O’Beirne JG, Chlapoutakis K, Alshryda S, et al. International interdisciplinary consensus meeting on the evaluation of developmental dysplasia of the Hip. Ultraschall Med. 2019;40:454–464. doi:10.1055/a-0924-5491
14. de Hundt M, Vlemmix F, Bais JMJ, et al. Risk factors for developmental dysplasia of the Hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2012;165:8–17. doi:10.1016/j.ejogrb.2012.06.030
15. Shaw BA, Segal LS, Otsuka NY. Evaluation and referral for developmental dysplasia of the Hip in infants. Pediatrics. 2016;138:e20163107. doi:10.1542/peds.2016-3107
16. Al-Mohrej O, Alsarhani W, Al-Ayedh N, et al. Characteristics of developmental dysplasia of the Hip at a tertiary hospital in Riyadh, Saudi Arabia. J Health Special. 2017;5:87. doi:10.4103/2468-6360.205076
17. Clarke NMP. Swaddling and Hip dysplasia: an orthopaedic perspective. Arch Dis Child. 2014;99:5–6. doi:10.1136/archdischild-2013-304143
18. Kutlu A, Memik R, Mutlu M, et al. Congenital dislocation of the Hip and its relation to swaddling used in Turkey. J Pediatr Orthop. 1992;12:598–602. doi:10.1097/01241398-199209000-00006
19. Guner SI, Guner S, Peker E, et al. Are consanguineous marriage and swaddling the risk factors of developmental dysplasia of the Hip? J Membr Biol. 2013;246:115–119. doi:10.1007/s00232-012-9509-4
20. Almahdi H, Almukhlifi R, Alahmadi R, et al. Assessment of the awareness among females in Saudi Arabia about the relationship of swaddling to developmental dysplasia of the hips. J Musculoskelet Surg Res. 2017;1(1):44–48. doi:10.4103/jmsr.jmsr_22_17
21. Harcke HT, Karatas AF, Cummings S, Bowen JR. Sonographic assessment of Hip swaddling techniques in infants with and without DDH. J Pediatr Orthop. 2016;36:232–238. doi:10.1097/BPO.0000000000000446
22. Murphy RF, Kim Y-J. Surgical management of pediatric developmental dysplasia of the Hip. J Am Acad Orthop Surg. 2016;24:615–624. doi:10.5435/JAAOS-D-15-00154
23. Buonsenso D, Curatola A, Lazzareschi I, et al. Developmental dysplasia of the Hip: real world data from a retrospective analysis to evaluate the effectiveness of universal screening. J Ultrasound. 2021;24:403–410. doi:10.1007/s40477-020-00463-w
24. Kremli MK, Alshahid AH, Khoshhal KI, et al. The pattern of developmental dysplasia of the Hip. Saudi Medical J. 2003;24:1118–1120.
25. Imrie M, Scott V, Stearns P, et al. Is ultrasound screening for DDH in babies born breech sufficient? J Child Orthop. 2010;4:3–8. doi:10.1007/s11832-009-0217-2
26. Mirdad T. Incidence and pattern of congenital dislocation of the Hip in Aseer Region of Saudi Arabia. West Afr J Med. 2004;21:218–222. doi:10.4314/wajm.v21i3.28034
27. Zamborsky R, Kokavec M, Harsanyi S, Attia D, Danisovic L. Developmental dysplasia of the Hip: perspectives in genetic screening. Med Sci. 2019;7:59. doi:10.3390/medsci7040059
28. Sadat-Ali M, Al-Habdan IM, Bubshait DA. Genetic influence in developmental dysplasia of the Hip in Saudi Arabian children due to GDF5 polymorphism. Biochem Genet. 2018;56:618–626. doi:10.1007/s10528-018-9864-7
29. Vaquero-Picado A, González-Morán G, Garay EG, et al. Developmental dysplasia of the Hip: update of management. EFORT Open Rev. 2019;4:548–556. doi:10.1302/2058-5241.4.180019
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.