")
Back to Journals » International Journal of General Medicine » Volume 14
How Much Benefit Can Patients Acquire from Enhanced Recovery After Surgery Protocols with Percutaneous Endoscopic Lumbar Interbody Fusion?
Authors Gong J, Luo L, Liu H, Li C, Tang Y, Zhou Y
Received 6 May 2021
Accepted for publication 16 June 2021
Published 2 July 2021 Volume 2021:14 Pages 3125—3132
DOI https://doi.org/10.2147/IJGM.S318876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Junfeng Gong,* Liwen Luo,* Huan Liu, Changqing Li, Yu Tang, Yue Zhou
Department of Orthopedics, The Second Affiliated Xinqiao Hospital of Army Military Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Zhou; Yu Tang
Department of Orthopedics, The Second Affiliated Xinqiao Hospital of Army Military Medical University, Xinqiao Street, Shapingba District, Chongqing, People’s Republic of China
Tel +86 13908390792; +86 18623422628
Fax +86 23-68755012
Email [email protected]; [email protected]
Purpose: We aimed to explore the role of enhanced recovery after surgery (ERAS) in patients who underwent percutaneous endoscopic lumbar interbody fusion (PELIF).
Patients and Methods: We performed a retrospective, observational, cohort study on 91 patients who underwent PELIF for degenerative disc disease. The primary outcomes were postoperative opioid consumption, hospital length of stay (LOS), and hospital cost.
Results: Forty-six patients comprised the ERAS group, and 45 patients comprised the pre-ERAS group (control group). The groups had comparable demographic characteristics. Good compliance with the ERAS pathway was observed in the ERAS group. Patients in the ERAS group used significantly fewer morphine equivalents compared with the pre-ERAS group (25.0 vs 33.3, respectively; p = 0.017). Hospital LOS did not decrease significantly in the ERAS group compared with the pre-ERAS group (3.1days vs 3.4 days, respectively; p = 0.096). Likewise, there was no significant difference in hospital cost between the pre-ERAS group and the ERAS group ($10,598.60 vs $10,384.50, respectively; p = 0.468).
Conclusion: In the present study, the benefit of ERAS in the context of PELIF was limited. Although a multidisciplinary ERAS protocol can improve analgesia and decrease opioid consumption, no significant reduction in hospital LOS and cost was observed.
Keywords: enhanced recovery after surgery, hospital length of stay, opioid use, hospital costs, percutaneous endoscopic spine surgery
Introduction
In the 1990s, enhanced recovery after surgery (ERAS) was proposed by Kehlet to improve patient care and outcomes and accelerate postoperative recovery time.1 ERAS is a multimodal and multidisciplinary approach aimed at reducing surgical stress by applying preoperative, perioperative, and postoperative protocols to ameliorate the surgical stress response and associated increases in glucose and protein catabolism.2,3 Implementation of ERAS requires involvement of a multidisciplinary group comprised of surgeons, anesthetists, nurses, and other care staff. Although some elements differ between ERAS protocols, all protocols share the common principle that benefit is achieved by aggregating marginal gains.4
ERAS protocols have been widely implemented in most surgical specialties and have proven to optimize patient outcomes, such as reducing opioid use, hospital length of stay (LOS), and hospital costs. In addition, ERAS protocols ease the burden on the health care system.5–9 Given the success of ERAS protocols in other types of surgery, it is not surprising that their implementation has received increasing interest in the field of spinal surgery.10,11 However, ERAS in spinal surgery is still in the early stages compared with other surgical specialties. Variations in the extent of the surgical stress response and availability of multiple surgical and anesthetic approaches suggest that no same pathway is appropriate for all cases of spinal surgery. Therefore, protocols might be best tailored to different types of spinal procedure. In a previous study, authors reported their 18-month experience with an ERAS pathway in spinal surgery. Postoperative opioid consumption was significantly reduced in the ERAS group, as was hospital LOS.12 In 2020, Yang et al studied the clinical outcomes of ERAS protocols for minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF). The results suggest that ERAS protocols decrease hospital LOS and provide relief from back pain.13 Our previous results using ERAS in MIS-TLIF were similar; specifically, hospital LOS decreased from 7 days to 5 days.14 In a recent randomized controlled trial on ERAS for lumbar spine fusion, the results showed significant gains in early recovery with ERAS.15
Percutaneous endoscopic lumbar interbody fusion (PELIF), which is another minimally invasive surgical technique, is used to treat degenerative lumbar disease with satisfactory clinical and radiological results.16–18 PELIF is advantageous in terms of its short hospitalization duration, smaller volume of intraoperative bleeding, and ability to minimize structural damage, but whether ERAS protocols benefit patients undergoing PELIF remains unclear. Therefore, in this study, we aimed to investigate whether ERAS protocols reduce opioid consumption, hospital LOS, and hospital cost in patients with degenerative lumbar disease undergoing PELIF surgery.
Materials and Methods
This study adopted a retrospective observational design. The study was performed in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Army Medical University. All participants provided written informed consent, and all patients’ details were anonymized during collection and analysis. Patients who underwent PELIF at our institution before (pre-ERAS group) and after (ERAS group) implementation of ERAS protocols in May 2019 were enrolled. Selection criteria included 1) typical clinical symptoms and homologous imaging evidence supporting the need for lumbar fusion; 2) unsatisfaction with conservative treatment; 3) the ability to understand the ERAS protocol and to actively participate in its implementation. Patients with lumbar spondylolisthesis of Meyerding classification grade II or above, severely deformed intervertebral foramina, low-exiting nerve roots, and exiting nerve root variability were excluded. All procedures were performed by the same orthopedic surgeons (Y. Z., Y. T., and CQ. L.) during the study period at our institution, and lumbar degenerative disease types did not change before and after implementing ERAS (Table 1). All data of patients and procedures were collected from the hospital database. The following patient demographics were reviewed using electronic medical data: age; sex; body mass index (BMI); preoperative pain score (evaluated using the Visual Analog Scale [VAS]); and medical comorbidities, including hypertension, diabetes mellitus, coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), asthma, and liver disease. We hypothesized that implementing the ERAS protocol in patients undergoing PELIF would reduce hospital LOS; therefore, this variable was chosen as the primary outcome. All routes of opioid use were converted to the morphine equivalent dose for standardization, and the ratios have been described previously.19 Hospital LOS was defined as the time from completion of surgery to hospital discharge. Secondary outcomes included volume of intraoperative blood loss, postoperative surgical dram drainage, postoperative patient pain score, surgical complications, and 30-day readmission. Most pain occurred on postoperative days (PODs) 0 and 1, decreasing in later days. Therefore, we recorded patients’ VAS scores on PODs 0 and 1.
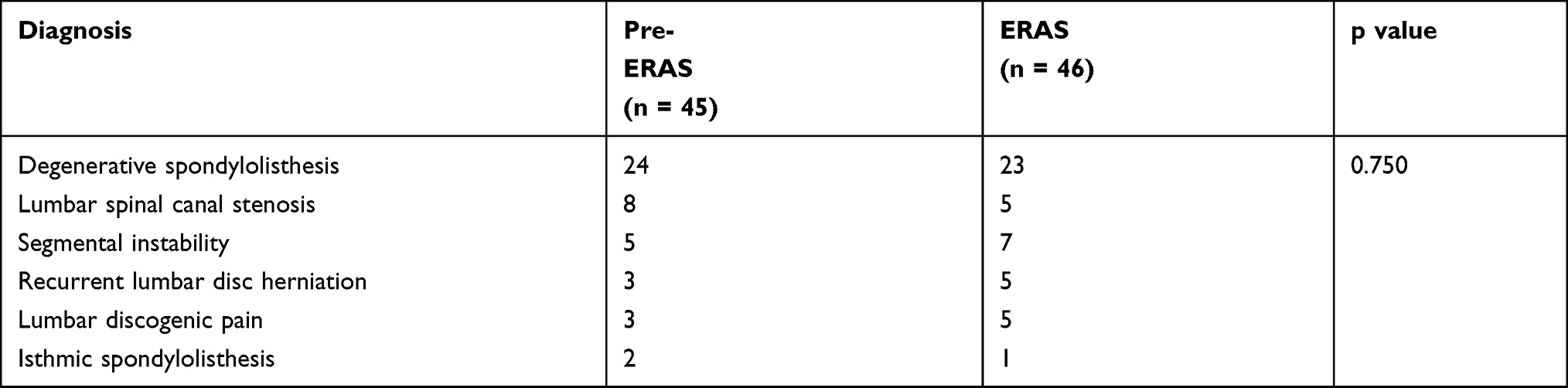 |
Table 1 Lumbar Degenerative Disease Types |
ERAS Protocol
After reviewing the literature on successful ERAS protocols and adjusting our protocol accordingly, the ERAS protocol was implemented in patients who underwent PELIF at our institution from May 2019 (Table 2). In the preoperative period, patients were educated about the ERAS protocol and PELIF surgery, and we responded to any questions raised. The nutritional status of patients was assessed by a dietitian who prescribed nutritional supplements containing protein, glucose, omega-3 fatty acids, and specific amino acids (glutamine and arginine), if necessary. Pre-emptive oral analgesics, including celecoxib, eperisone, extended-release tramadol, and pregabalin, were used on the day of admission according to the condition of the patient. Unlike routine bowel preparation, clear carbohydrate-rich drink was provided before surgery, which patients were required to drink 4 hours preoperatively. Intraoperatively, the ERAS protocol consisted of prophylactic antibiotics, surgical wound local anesthetic, and intraoperative temperature and fluid management. Antibiotics were administered proactively 30 minutes before incision, and peak concentrations were achieved at the time of surgery. Skin blocks using local anesthesia were performed around the skin incision, which relieved surgical wound pain. Body temperature was monitored constantly throughout surgery, and an air-warming device and warmed intravenous fluids were used to prevent intraoperative hypothermia. To avoid excessive or insufficient use of intravenous fluids, goal-directed fluid therapy was applied for fluid management. The anesthetist adjusted the fluid infusion based on intraoperative changes in hemodynamics. In the postoperative period, multimodal analgesia was implemented for pain management. Patients received intravenous parecoxib immediately after surgery, and oral pain medications (celecoxib, acetaminophen, and, if necessary, pregabalin) were administered from POD 1. Intravenous or intramuscular morphine was used if pain was not well controlled. Patients were permitted to eat liquid food on POD 0 and switched to eating solid food on POD 1. Foley catheters were removed on POD 1 unless close monitoring of urine output was necessary. Subfascial drains were routinely placed intraoperatively and were removed when the drain output was <20 mL/24 h. Early ambulation and mobilization using a brace were encouraged, but patients were required to avoid bending or weight lifting.
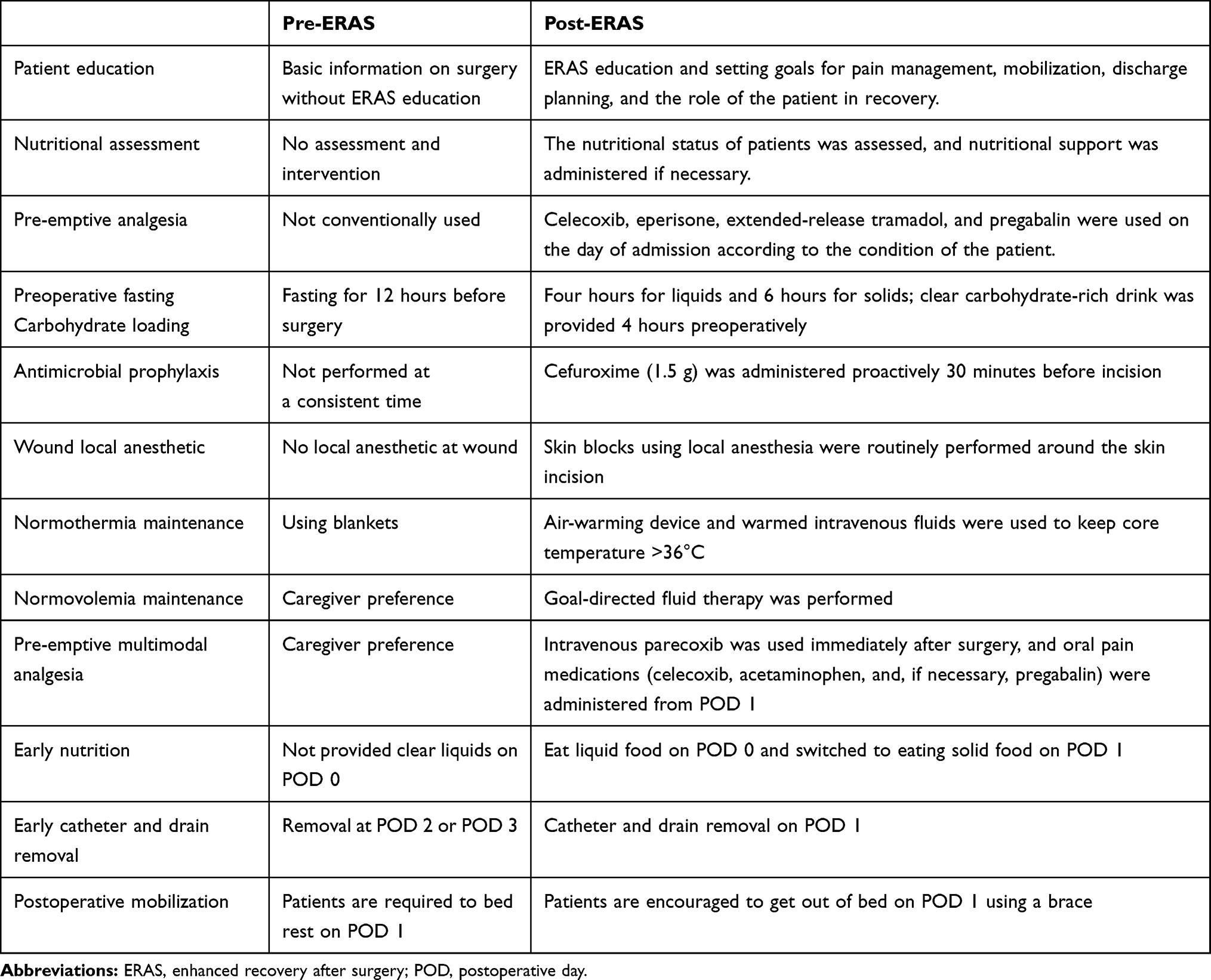 |
Table 2 Items Included in pre-ERAS and Post-ERAS Care |
Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median (range). Categorical variables are presented as frequencies or percentages. If parametric assumptions were met, a two-tailed Student’s t-test was employed to compare continuous variables between the pre-ERAS group and the ERAS group; otherwise, the Mann–Whitney U-test was used. Categorical variables between the pre-ERAS group and the ERAS group were compared using the χ2 test. Significant differences were determined using a p value of <0.05, and all analyses were performed using SPSS software 25.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 91 patients who underwent PELIF were enrolled in this study. Forty-five patients were allocated to the pre-ERAS group, and 46 patients were allocated to the ERAS group. The demographics of patients in the pre-ERAS and ERAS groups were similar. There were no significant differences in sex, age, BMI, preoperative pain score, or medical comorbidities (such as hypertension, diabetes mellitus, CAD, COPD, asthma, and liver disease) between groups (Table 3). A greater number of patients were female than were male in both groups (26 female patients in the pre-ERAS group and 30 female patients in the ERAS group). In the pre-ERAS group, 41 patients received one level of fusion, and 4 patients received two levels of fusion. In the ERAS group, 45 patients underwent one level of fusion, and 1 patient underwent two levels of fusion. There was no significant difference in surgical level between the two groups. Surgical duration and volume of intraoperative blood loss were similar between the pre-ERAS and ERAS groups (Table 4).
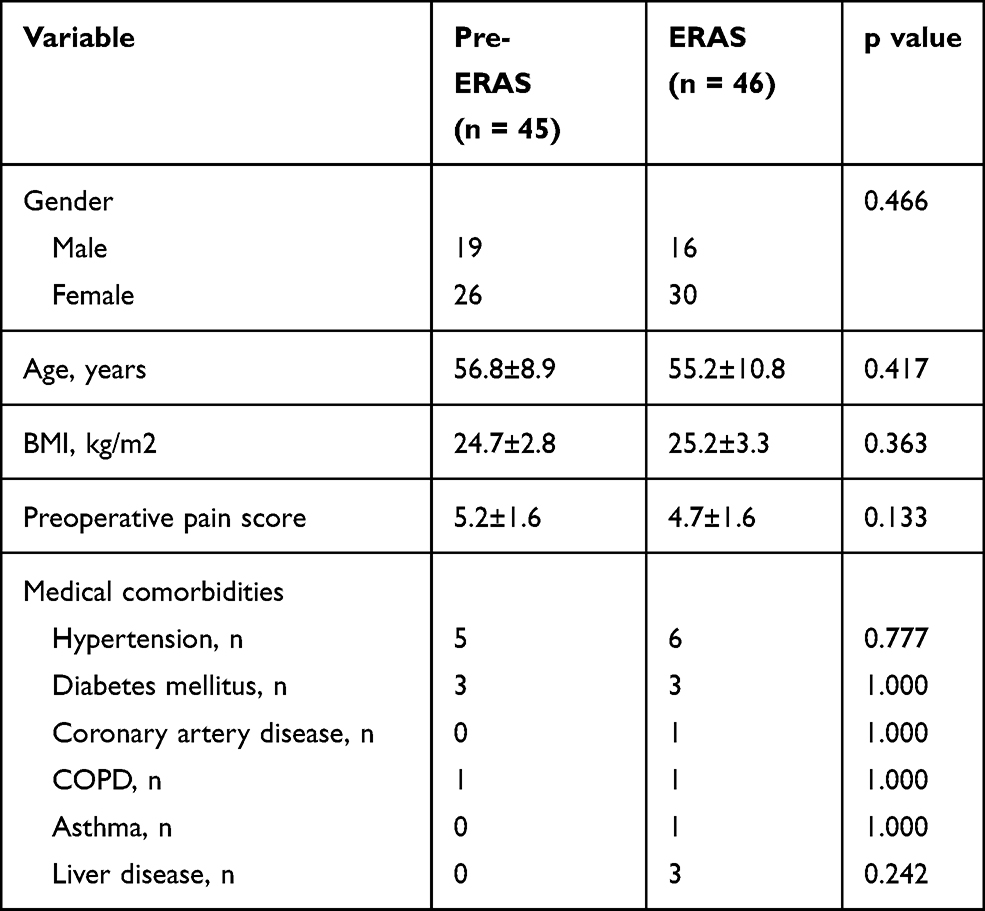 |
Table 3 Patient Demographics |
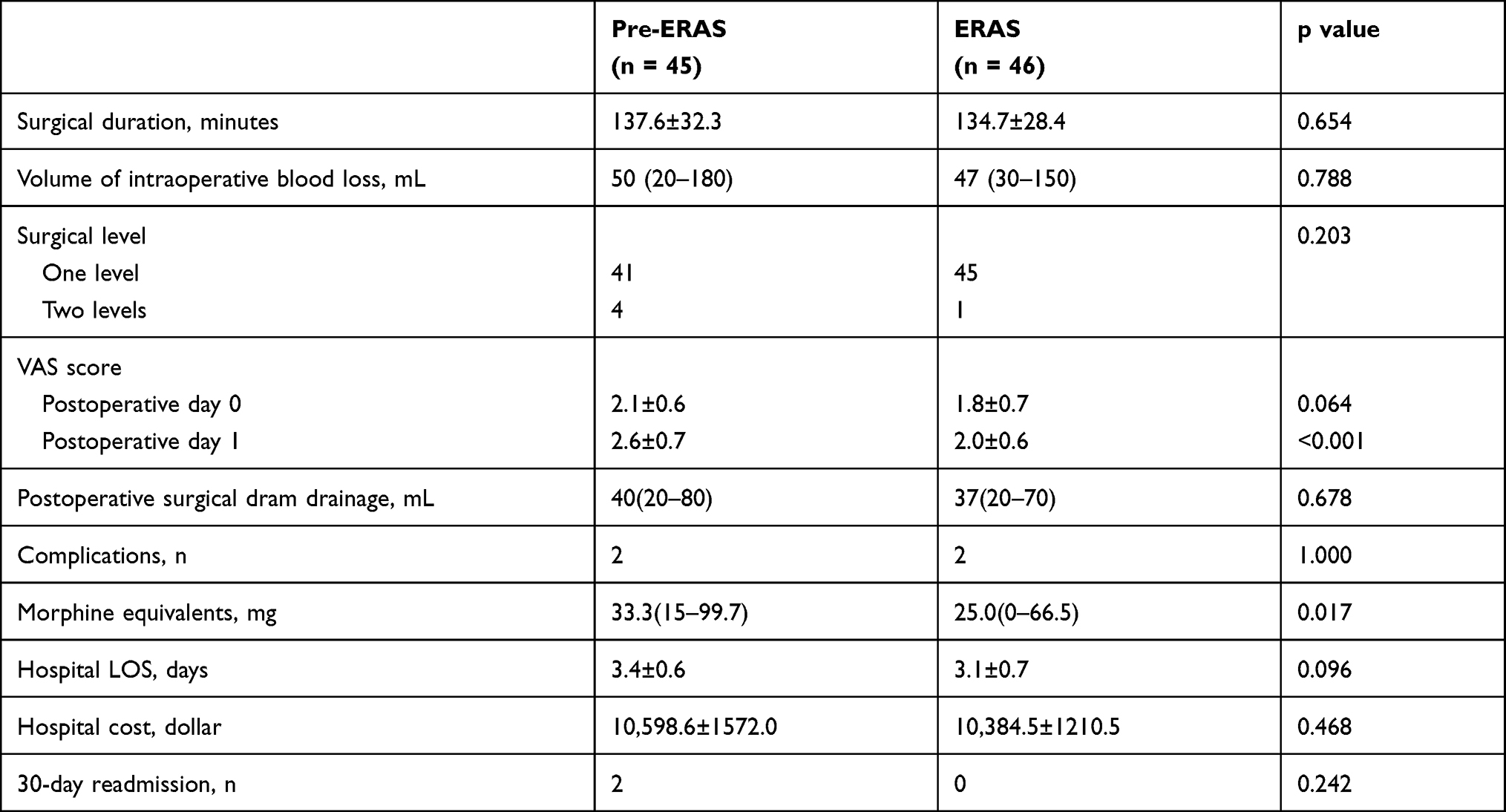 |
Table 4 Intraoperative and Postoperative Variables |
Fifteen ERAS elements were tracked in the ERAS group. Most items were used in 100% of cases, such as patient education, nutritional status assessment, nutritional intervention, antimicrobial prophylaxis, wound local anesthetic, active warming, early oral nutrition, early ambulation, and early catheter removal. Other items with high compliance were preemptive analgesia (96%), preoperative fasting and carbohydrate loading (98%), goal-directed fluid therapy (91%), and multimodal analgesia (93%).
Although no significant differences between groups were detected according to VAS score on POD 0, VAS score on POD 1 in the ERAS group was lower compared with that in the pre-ERAS group (2.0 vs 2.6, respectively; p < 0.001). Postoperative surgical dram drainage did not differ significantly between patients in the pre-ERAS group and patients in the ERAS group. Patients in the ERAS group used significantly fewer morphine equivalents compared with the pre-ERAS group (25.0 vs 33.3, respectively; p = 0.017). Hospital LOS did not decrease significantly in the ERAS group compared with the pre-ERAS group (3.1 days vs 3.4 days, respectively; p = 0.096). Likewise, there was no significant difference in hospital cost between the pre-ERAS group and the ERAS group ($10,598.60 vs $10,384.50, respectively; p = 0.468). One case of dural tear and one case of temporary ipsilateral dysesthesia were observed in the pre-ERAS group. The patient who experienced cage migration underwent a second surgery at readmission. There was also one case of dural tear and one case of temporary ipsilateral dysesthesia in the ERAS group. No differences were noted in complications and 30-day readmission between groups (Table 4).
Discussion
An increasing number of people who suffer from degenerative disc disease undergo lumbar fusion surgery worldwide. Since MIS-TLIF was introduced in the early 2000s, spinal surgeons have shown great enthusiasm for this procedure. MIS-TLIF demonstrates less intraoperative blood loss, a shorter hospital stay, a faster recovery time, and less postoperative narcotic use with similar clinical outcomes and fusion rates compared with open TLIF.20–22 Wainwright et al first proposed that ERAS protocols could promote patient recovery and improve outcomes in major spinal surgery.23 Since then, ERAS protocols have been gradually implemented in patients who undergo minimally invasive spinal surgery.24,25 Yang et al reported that patients who undergo MIS-TILF gain benefit from ERAS in terms of a shorter LOS, lower opioid use, and earlier recovery of daily activity.13 In another recent ERAS MIS-TLIF cohort study, ERAS achieved a significant decrease in LOS and opioid use in the immediate perioperative and postoperative periods.26 These studies indicate that ERAS plays an important role in decreasing LOS and opioid use without increasing complications. However, no studies have reported ERAS protocols tailored for PELIF. Therefore, we implemented the ERAS protocol in patients undergoing PELIF and determined how much benefit can be acquired by patients.
In the present study, although basic patient demographics and disease types were similar between the pre-ERAS and ERAS groups, non-significant decreases in hospital LOS and hospital cost were observed in our research, which contradicts previous studies. This discrepancy may be due to two reasons. First, our study sample size was small and could not be unpowered to detect a significant difference in hospital LOS between groups. Second, the minimal invasiveness of PELIF may have influenced hospital LOS in our research. In previous research, a minimally invasive technique was used as a component of the ERAS protocol.25,27 Compared with open-surgery approaches, minimally invasive approaches cause less surgical stress and improve perioperative immune function in esophageal, rectal, and gastric procedures.28–30 PELIF, as a new surgical technique, is performed through Kambin’s triangle without destroying the paravertebral structure. Thus, patients experience less postoperative pain, mobilize more quickly, and are discharged earlier compared with patients who undergo MIS-TLIF, suggesting that PELIF is less invasive compared with MIS-TLIF.18 Therefore, the benefit of ERAS may not be well reflected in terms of reducing hospital LOS.
Recently, regulating the prescription of opioids to reduce opioid use has attracted attention because of increased opioid-related morbidity and mortality.31 There are many different side effects of opioid use. Multiple organ systems are affected by opioids, which can result in serious complications, such as respiratory depression and/or obstruction, cognitive dysfunction, and even death. Sedation, hormonal changes, hyperalgesia, and immunological depression are related to opioid use.32,33 Patients are also at risk of developing tolerance and dependence on account of opioid addiction. Therefore, it is necessary to decrease opioid use in surgical patients. In our ERAS protocol, pre-emptive and multimodal analgesia were used for postoperative pain management. Pre-emptive and multimodal analgesia are two pain management methods used to effectively control pain. These approaches involve taking oral analgesics before the procedure, preventing central nervous system hyperexcitation and effectively relieving pain. Multimodal analgesia provides more effective analgesia and fewer side effects using equivalent or reduced doses of a combination of analgesics that work via different mechanisms and at various sites in the pain-producing pathway. In addition, local anesthetics are injected at the surgical site to relieve wound pain.
In the current study, opioid consumption was significantly lower in the ERAS group (25.0 mg) compared with the pre-ERAS group (33.3 mg). Moreover, this reduction did not cause higher VAS pain scores, but rather it improved pain on POD 1. These data are consistent with previous studies, indicating that implementation of ERAS could successfully reduce opioid use in the postoperative period without negatively increasing pain scores.12,34,35 Our results also suggest that ERAS protocols in spinal surgery are safe. A non-significant decrease in complications was observed in the ERAS group compared with the pre-ERAS group (2 vs 3, respectively; p = 0.627). Only one patient underwent a second surgery. All other patients’ symptoms disappeared within 1–3 days after surgery.
There are some limitations of the present study that should be noted. First, the study was a small-sample retrospective study that may be unpowered to detect significant differences in hospital LOS and hospital cost between the two groups. Second, the study adopted a “before-and-after” study design, which may cause bias associated with implementing a particular policy or intervention. Next, some patients in the pre-ERAS group may have already undergone certain ERAS protocol elements before formally implementing the protocol. This could also explain why a reduction in hospital LOS was not observed. Moreover, postoperative opioid use could only be monitored when patients were at hospital, and rapid exhaustion of refill prescriptions at home and prescriptions from outside institutions could not be measured.
Conclusion
In this study, we report use of an ERAS protocol in patients undergoing PELIF. The benefits of the ERAS protocol in patients undergoing PELIF were limited. Although the multidisciplinary ERAS protocol improved the effect of analgesia and decreased opioid consumption, we did not observe a significant reduction in hospital LOS and cost. The present study indicates that it is not necessary to implement ERAS in PELIF surgery. However, elements of ERAS need to be optimized and improved, and large-scale randomized controlled trials should be performed to assess the benefits of the ERAS protocol for patients undergoing PELIF in the future.
Acknowledgments
All authors thank all the staff members in the Xinqiao Hospital of Army Military Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–617. doi:10.1093/bja/78.5.606
2. Carli F. Physiologic considerations of Enhanced Recovery After Surgery (ERAS) programs: implications of the stress response. Can J Anaesth. 2015;62(2):110–119. doi:10.1007/s12630-014-0264-0
3. Fearon KCH. Overview: key elements and the impact of enhanced recovery care. In: Francis N, Kennedy RH, Ljungqvist O, Mythen MG, editors. Manual of Fast Track Recovery for Colorectal Surgery. London: Springer-Verlag; 2012:1–13.
4. Lumb AB, McLure HA. AAGBI recommendations for standards of monitoring during anaesthesia and recovery 2015 - a further example of ‘aggregation of marginal gains’. Anaesthesia. 2016;71(1):3–6. doi:10.1111/anae.13327
5. Christelis N, Wallace S, Sage CE, et al. An enhanced recovery after surgery program for hip and knee arthroplasty. Med J Aust. 2015;202(7):363–368. doi:10.5694/mja14.00601
6. Geltzeiler CB, Rotramel A, Wilson C, Deng L, Whiteford MH, Frankhouse J. Prospective study of colorectal enhanced recovery after surgery in a community hospital. JAMA Surg. 2014;149(9):955–961. doi:10.1001/jamasurg.2014.675
7. Kowalsky SJ, Zenati MS, Steve J, et al. A combination of robotic approach and ERAS pathway optimizes outcomes and cost for pancreatoduodenectomy. Ann Surg. 2019;269(6):1138–1145. doi:10.1097/SLA.0000000000002707
8. Parise P, Ferrari C, Cossu A, et al. Enhanced Recovery After Surgery (ERAS) pathway in esophagectomy: is a reasonable prediction of hospital stay possible? Ann Surg. 2019;270(1):77–83. doi:10.1097/SLA.0000000000002775
9. Harrison RF, Li Y, Guzman A, et al. Impact of implementation of an enhanced recovery program in gynecologic surgery on healthcare costs. Am J Obstet Gynecol. 2020;222(1):
10. Dietz N, Sharma M, Adams S, et al. Enhanced Recovery After Surgery (ERAS) for spine surgery: a systematic review. World Neurosurg. 2019;130:415–426. doi:10.1016/j.wneu.2019.06.181
11. Zaed I, Bossi B, Ganau M, Tinterri B, Giordano M, Chibbaro S. Current state of benefits of Enhanced Recovery After Surgery (ERAS) in spinal surgeries: a systematic review of the literature. Neuro-Chirurgie. 2021. doi:10.1016/j.neuchi.2021.04.007
12. Flanders TM, Ifrach J, Sinha S, et al. Reduction of postoperative opioid use after elective spine and peripheral nerve surgery using an enhanced recovery after surgery program. Pain Med. 2020;21(12):3283–3291. doi:10.1093/pm/pnaa233
13. Yang Y, Wu X, Wu W, et al. Enhanced recovery after surgery (ERAS) pathway for microendoscopy-assisted minimally invasive transforaminal lumbar interbody fusion. Clin Neurol Neurosurg. 2020;196:106003. doi:10.1016/j.clineuro.2020.106003
14. Feng C, Zhang Y, Chong F, et al. Establishment and Implementation of an Enhanced Recovery After Surgery (ERAS) pathway tailored for minimally invasive transforaminal lumbar interbody fusion surgery. World Neurosurg. 2019;129:e317–e323. doi:10.1016/j.wneu.2019.05.139
15. Soffin EM, Beckman JD, Tseng A, et al. Enhanced recovery after lumbar spine fusion: a randomized controlled trial to assess the quality of patient recovery. Anesthesiology. 2020;133(2):350–363. doi:10.1097/ALN.0000000000003346
16. Lee SH, Erken HY, Bae J. Percutaneous transforaminal endoscopic lumbar interbody fusion: clinical and radiological results of mean 46-month follow-up. Biomed Res Int. 2017;2017:3731983.
17. Kamson S, Lu D, Sampson PD, Zhang Y. Full-endoscopic lumbar fusion outcomes in patients with minimal deformities: a Retrospective Study of data collected between 2011 and 2015. Pain Physician. 2019;22(1):75–88. doi:10.36076/ppj/2019.22.75
18. Ao S, Zheng W, Wu J, et al. Comparison of preliminary clinical outcomes between percutaneous endoscopic and minimally invasive transforaminal lumbar interbody fusion for lumbar degenerative diseases in a tertiary hospital: is percutaneous endoscopic procedure superior to MIS-TLIF? A prospective cohort study. Int J Surg. 2020;76:136–143. doi:10.1016/j.ijsu.2020.02.043
19. Xu W, Daneshmand S, Bazargani ST, et al. Postoperative pain management after radical cystectomy: comparing traditional versus enhanced recovery protocol pathway. J Urol. 2015;194(5):1209–1213. doi:10.1016/j.juro.2015.05.083
20. Guan J, Bisson EF, Dailey AT, Hood RS, Schmidt MH. Comparison of clinical outcomes in the national neurosurgery quality and outcomes database for open versus minimally invasive transforaminal lumbar interbody fusion. Spine. 2016;41(7):E416–E421. doi:10.1097/BRS.0000000000001259
21. Wang J, Zhou Y, Zhang ZF, Li CQ, Zheng WJ, Liu J. Comparison of one-level minimally invasive and open transforaminal lumbar interbody fusion in degenerative and isthmic spondylolisthesis grades 1 and 2. Eur Spine J. 2010;19(10):1780–1784. doi:10.1007/s00586-010-1404-z
22. Khan NR, Clark AJ, Lee SL, Venable GT, Rossi NB, Foley KT. Surgical outcomes for minimally invasive vs open transforaminal lumbar interbody fusion: an updated systematic review and meta-analysis. Neurosurgery. 2015;77(6):
23. Wainwright TW, Immins T, Middleton RG. Enhanced recovery after surgery (ERAS) and its applicability for major spine surgery. Best Pract Res Clin Anaesthesiol. 2016;30(1):91–102. doi:10.1016/j.bpa.2015.11.001
24. Wang MY, Chang HK, Grossman J. Reduced acute care costs with the ERAS® minimally invasive transforaminal lumbar interbody fusion compared with conventional minimally invasive transforaminal lumbar interbody fusion. Neurosurgery. 2018;83(4):827–834. doi:10.1093/neuros/nyx400
25. Wang MY, Chang P-Y, Grossman J. Development of an Enhanced Recovery After Surgery (ERAS) approach for lumbar spinal fusion. J Neurosurg Spine. 2017;26(4):411–418. doi:10.3171/2016.9.SPINE16375
26. Kerolus MG, Yerneni K, Witiw CD, et al. Enhanced recovery after surgery pathway for single-level minimally invasive transforaminal lumbar interbody fusion decreases length of stay and opioid consumption. Neurosurgery. 2021;88(3):648–657. doi:10.1093/neuros/nyaa493
27. Soffin EM, Vaishnav AS, Wetmore DS, et al. Design and IMPLEMENTATION of an Enhanced Recovery After Surgery (ERAS) program for minimally invasive lumbar decompression spine surgery: initial experience. Spine. 2019;44(9):E561–E570. doi:10.1097/BRS.0000000000002905
28. Veenhof AA, Sietses C, von Blomberg BM, et al. The surgical stress response and postoperative immune function after laparoscopic or conventional total mesorectal excision in rectal cancer: a randomized trial. Int J Colorectal Dis. 2011;26(1):53–59. doi:10.1007/s00384-010-1056-9
29. Maas KW, Biere SS, van Hoogstraten IM, van der Peet DL, Cuesta MA. Immunological changes after minimally invasive or conventional esophageal resection for cancer: a randomized trial. World J Surg. 2014;38(1):131–137. doi:10.1007/s00268-013-2233-0
30. Okholm C, Goetze JP, Svendsen LB, Achiam MP. Inflammatory response in laparoscopic vs. open surgery for gastric cancer. Scand J Gastroenterol. 2014;49(9):1027–1034. doi:10.3109/00365521.2014.917698
31. Hill MV, McMahon ML, Stucke RS, Barth RJ
32. van Lersberghe C, Camu F, de Keersmaecker E, Sacré S. Continuous administration of fentanyl for postoperative pain: a comparison of the epidural, intravenous, and transdermal routes. J Clin Anesth. 1994;6(4):308–314. doi:10.1016/0952-8180(94)90078-7
33. Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. doi:10.36076/ppj.2008/11/S105
34. Young R, Cottrill E, Pennington Z, et al. Experience with an enhanced recovery after spine surgery protocol at an academic community hospital. J Neurosurg Spine. 2020:1–8. doi:10.3171/2020.7.SPINE20358
35. Ali ZS, Flanders TM, Ozturk AK, et al. Enhanced recovery after elective spinal and peripheral nerve surgery: pilot study from a single institution. J Neurosurg Spine. 2019:1–9. doi:10.3171/2018.9.SPINE18681
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.