Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
How Long After Coronary Artery Bypass Surgery Can Patients Have Elective Safer Non-Cardiac Surgery?
Authors Sung LC ![]() , Chang CC
, Chang CC ![]() , Yeh CC, Cherng YG
, Yeh CC, Cherng YG ![]() , Chen TL, Liao CC
, Chen TL, Liao CC ![]()
Received 14 December 2023
Accepted for publication 7 February 2024
Published 19 February 2024 Volume 2024:17 Pages 743—752
DOI https://doi.org/10.2147/JMDH.S449614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Li-Chin Sung,1– 4 Chuen-Chau Chang,5– 7 Chun-Chieh Yeh,8,9 Yih-Giun Cherng,5,10 Ta-Liang Chen,5,7,11 Chien-Chang Liao5– 7,12,13
1Division of Cardiology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 2Division of Cardiology, Department of Internal Medicine, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan; 3Taipei Heart Institute, Taipei Medical University, Taipei, Taiwan; 4Department of General Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 5Department of Anesthesiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 6Department of Anesthesiology, Taipei Medical University Hospital, Taipei, Taiwan; 7Anesthesiology and Health Policy Research Center, Taipei Medical University Hospital, Taipei, Taiwan; 8Department of Surgery, China Medical University Hospital, Taichung, Taiwan; 9Department of Surgery, University of Illinois, Chicago, IL, USA; 10Department of Anesthesiology, Shuang Ho Hospital, Taipei Medical University, Taipei, Taiwan; 11Department of Anesthesiology, Wang Fang Hospital, Taipei Medical University, Taipei, Taiwan; 12Research Center of Big Data and Meta‑Analysis, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 13School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan
Correspondence: Chien-Chang Liao, Department of Anesthesiology, Taipei Medical University Hospital, 252 Wuxing Street, Taipei, 11031, Taiwan, Tel +886-2-2737-2181, ext. 8310, Fax +886-2-2736-7344, Email [email protected]; [email protected]
Objective: To evaluate the complications and mortality after noncardiac surgeries in patients who underwent previous coronary artery bypass grafting (CABG).
Methods: We used insurance data and identified patients aged ≥ 20 years undergoing noncardiac surgeries between 2010 and 2017 in Taiwan. Based on propensity-score matching, we selected an adequate number of patients with a previous history of CABG (within preoperative 24 months) and those who did not have a CABG history, and both groups had balanced baseline characteristics. The association of CABG with the risk of postoperative complications and mortality was estimated (odds ratio [OR] and 95% confidence interval [CI]) using multiple logistic regression analysis.
Results: The matching procedure generated 2327 matched pairs for analyses. CABG significantly increased the risks of 30-day in-hospital mortality (OR 2.28, 95% CI 1.36– 3.84), postoperative pneumonia (OR 1.49, 95% CI 1.12– 1.98), sepsis (OR 1.49, 95% CI 1.17– 1.89), stroke (OR 1.53, 95% CI 1.17– 1.99) and admission to the intensive care unit (OR, 1.75, 95% CI 1.50– 2.05). The findings were generally consistent across most of the evaluated subgroups. A noncardiac surgery performed within 1 month after CABG was associated with the highest risk for adverse events, which declined over time.
Conclusion: Prior history of CABG was associated with postoperative pneumonia, sepsis, stroke, and mortality in patients undergoing noncardiac surgeries. Although we raised the possibility regarding deferral of non-critical elective noncardiac surgeries among patients had recent CABG when considering the risks, critical or emergency surgeries were not in the consideration of delay surgery, especially cancer surgery.
Keywords: adverse events, coronary artery bypass surgery, noncardiac surgeries, postoperative complications, postoperative mortality
Introduction
Cardiovascular disease is one of the leading causes of death worldwide, and half of all deaths are due to coronary artery disease (CAD).1,2 Coronary artery bypass grafting (CABG), a surgical procedure that effectively treats angina and prolongs life, is a major therapy for patients with severe CAD. CABG is a common cardiac surgical procedure (243 cases per million adults in 2011) in the United States.3 Some patients with a prior history of CABG require noncardiac surgeries.4
Two previous post hoc analyses of randomized trials showed a low postoperative risk, ranging from 1.3% to 1.7% in post-CABG patients.5,6 From the Coronary Artery Surgery Study database, prior history of CABG was associated with fewer postoperative deaths and myocardial infarctions than medical treatment for CAD.5 The clinical practice guideline on perioperative cardiac assessment recommends no further cardiac evaluation is needed in asymptomatic CAD patients who have good functional capacity.7 Theoretically, clinically stable patients who have undergone CABG within the last 6 years are relatively “protected” from experiencing a myocardial infarction as a complication of noncardiac surgeries.5
Patients undergoing CABG have increasingly complex conditions, including multiple noncardiac comorbidities.8 These comorbidities not only impact long-term prognosis after CABG but also increase the surgical risks. Atrial fibrillation and pulmonary artery systolic pressure were recommended to be high risk factors among patients undergoing noncardiac surgery.9,10 In the clinical settings, physicians frequently encounter noncardiac surgeries in patients with a prior history of CABG. Although two studies suggested that noncardiac surgery is often required early after CABG and carries very low risk for major complications,4,11 we still suggested that a electrocardiographic based or clinical based score should be formed in order to determine patients with highest risk12 Although the revised cardiac risk index has been used to predict perioperative cardiac complications following noncardiac surgeries,13,14 the index cannot identify risks in patients who have been treated with CABG.
Until recently, studies on the outcomes after noncardiac surgeries in CABG patients compared with normal controls are still lacking. The purpose of our investigation is to investigate the complications and mortality after noncardiac surgeries in patients who underwent previous CABG.
Methods
Source of Data
We used insurance data of the Health and Welfare Data Science Center of all populations (23 million people), obtained from the Ministry of Health and Welfare of Taiwan. Detailed information on this insurance program is described in previous reports.15,16 This study was evaluated and approved by the Research Ethics Committee of Taipei Medical University (TMU-JIRB-201710033; TMU-JIRB-201902053; TMU-JIRB-201905042) and was exempted from the requirement for informed patient consent. The data accessed complied with relevant data protection and privacy regulations.
Study Design
In this surgical cohort study, we identified 3,498,909 surgical patients aged ≥ 20 years who underwent noncardiac surgeries from 2010 to 2017, and 5622 of them had a CABG history within preoperative 24 months. To balance the baseline characteristics of surgical patients, with and without a previous history of CABG, we conducted propensity-score matching and selected 2327 patients who had a previous history of CABG and 2327 patients without a history of CABG for comparison. The postoperative complications, mortality, admission to the intensive care unit, length of hospital stay, and medical expenditure during surgical admission were considered as outcomes that were evaluated and compared between the CABG group and the non-CABG control group.
Definition and Measures
For identifying patients with CABG, we used insurance payment codes of CABG and the records of surgical hospitalization due to CABG in the national insurance research database in Taiwan. In this study, we defined the target population CABG group as patients who received CABG within 24 months before the noncardiac surgery. The non-CABG group was defined as patients who had no experienced CABG within 24 months before the noncardiac surgery. All noncardiac surgeries were surgical procedures that could be performed with general anesthesia, neuraxial anesthesia or general anesthesia. We included a history of disease (within the preoperative 24 months), such as hypertension, diabetes, hyperlipidemia, heart failure, ischemic heart disease, chronic obstructive pulmonary disease, liver cirrhosis, Parkinson’s disease, and renal dialysis, as comorbidities that might be associated with postoperative outcomes. Postoperative complications that occurred during surgical admission, including postoperative bleeding, pneumonia, sepsis, urinary tract infection, deep wound infection, stroke, acute myocardial infarction, acute renal failure and pulmonary embolism, were evaluated. In this study, the definition of postoperative adverse events included postoperative pneumonia, sepsis, stroke, and mortality.
Statistical Analysis
In this surgical cohort study, data analysis first compared baseline distributions of demographic status, comorbidities and propensity scores between each pair of CABG and non-CABG groups. Comparisons of characteristics between surgical patients, with and without a previous CABG history, used the absolute standardized mean difference, with a value greater than 10% used to define a clinically important imbalance.
For the balance of baseline characteristics between patients with and without prior CABG in this study, a nonparsimonious multivariable logistic regression model was used to estimate a propensity score for patients who had or had not prior CABG. Age, sex, low income, types of surgery, types of anesthesia, hypertension, diabetes, hyperlipidemia, heart failure, ischemic heart disease, chronic obstructive pulmonary disease, liver cirrhosis, Parkinson’s disease, and renal dialysis were considered as clinical significance guided the initial choice of covariates in this matching model. Each variable was analyzed individually. We matched patients with prior CABG to non-CABG patients using a greedy matching algorithm (without replacement) with a caliper width of 0.2 SD of the log odds of the estimated propensity score. This method was used in our previous studies.15,16
The incidence of postoperative complications and mortality were calculated in patients with and without a previous CABG history. Adjusted odds ratios (ORs) of postoperative complications and mortality associated with a previous CABG history were estimated using multiple logistic regression models. The stratified analysis (by age, sex, medical conditions, types of surgery, and types of anesthesia) for the relationship between CABG and postoperative adverse events was also conducted by using multiple logistic regression models.
Results
In this propensity-score matched study, 4654 surgical patients were included and analyzed (Table 1). We found similar baseline characteristics, including socioeconomics, medical conditions, types of noncardiac surgeries, and anesthesia types, between the CABG group and the non-CABG group.
 |
Table 1 Characteristics of Surgical Patients with and without CABG (After Propensity-Score Matching) |
Compared with the controls, which were the individuals without a CABG history (Table 2), the CABG group had increased risks of postoperative pneumonia (OR 1.49, 95% CI 1.12–1.98), sepsis (OR 1.49, 95% CI 1.17–1.89), stroke (OR 1.53, 95% CI 1.17–1.99), and mortality (OR 2.28, 95% CI 1.36–3.84).
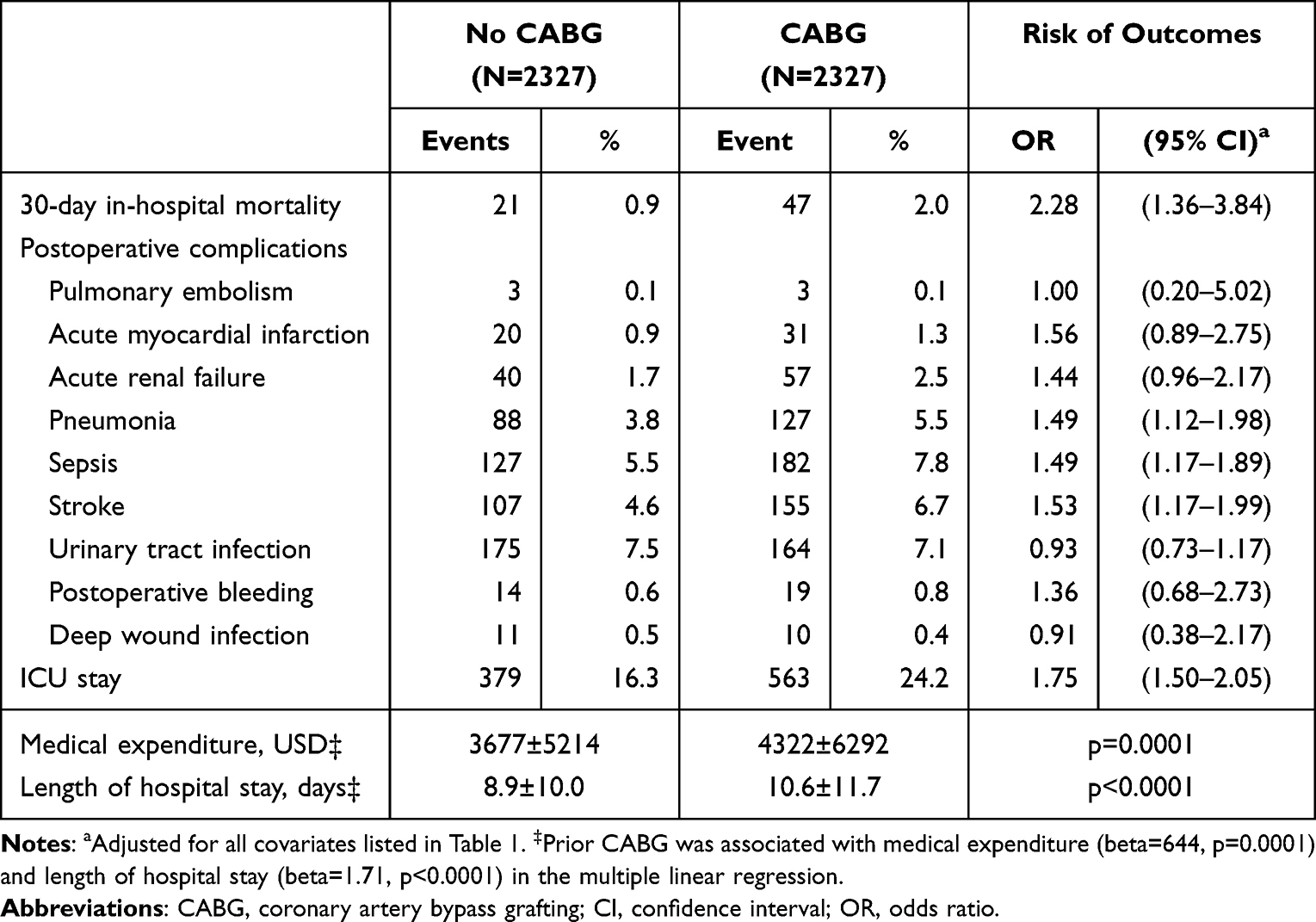 |
Table 2 Adverse Outcomes After Non-Cardiac Surgeries in Patients with and without Previous CABG |
In Table 3, prior CABG was associated with adverse events after noncardiac surgeries in women (OR 1.74, 95% CI 1.21–2.51) and men (OR 1.64, 95% CI 1.36–1.98). Among patients aged 20–49 years, patients with CABG had an increased risk of postoperative adverse events compared with patients without CABG (OR 6.75, 95% CI 1.59–28.6). The adjusted OR of postoperative adverse events associated with CABG for patients with age of 50–59 years, 60–69 years, and 70–79 years were 3.31 (95% CI 1.93–5.70), 1.78 (95% CI 1.35–2.35), and 1.37 (95% CI 1.03–1.80), respectively. The rate of postoperative adverse events rise steady with age in the non-CABG group but not in the CABG group, resulting in a steep decline in OR. CABG was also associated adverse events after musculoskeletal surgeries (OR 1.50, 95% CI 1.09–2.07), digestive surgeries (OR 1.50, 95% CI 1.09–2.08) and neurosurgeries (OR 1.78, 95% CI 1.21–2.63). Prolonged hospital stay, elevated medical expenditure, and increased risk of intensive care unit admission were also found in the CABG group. Supplementary Table S1 presented the stratified analysis for the relationship between CABG and postoperative adverse events by hypertension, diabetes, hyperlipidemia, heart failure, ischemic heart disease, chronic obstructive pulmonary disease, liver cirrhosis, Parkinson’s disease, renal dialysis, types of surgery, and types of anesthesia.
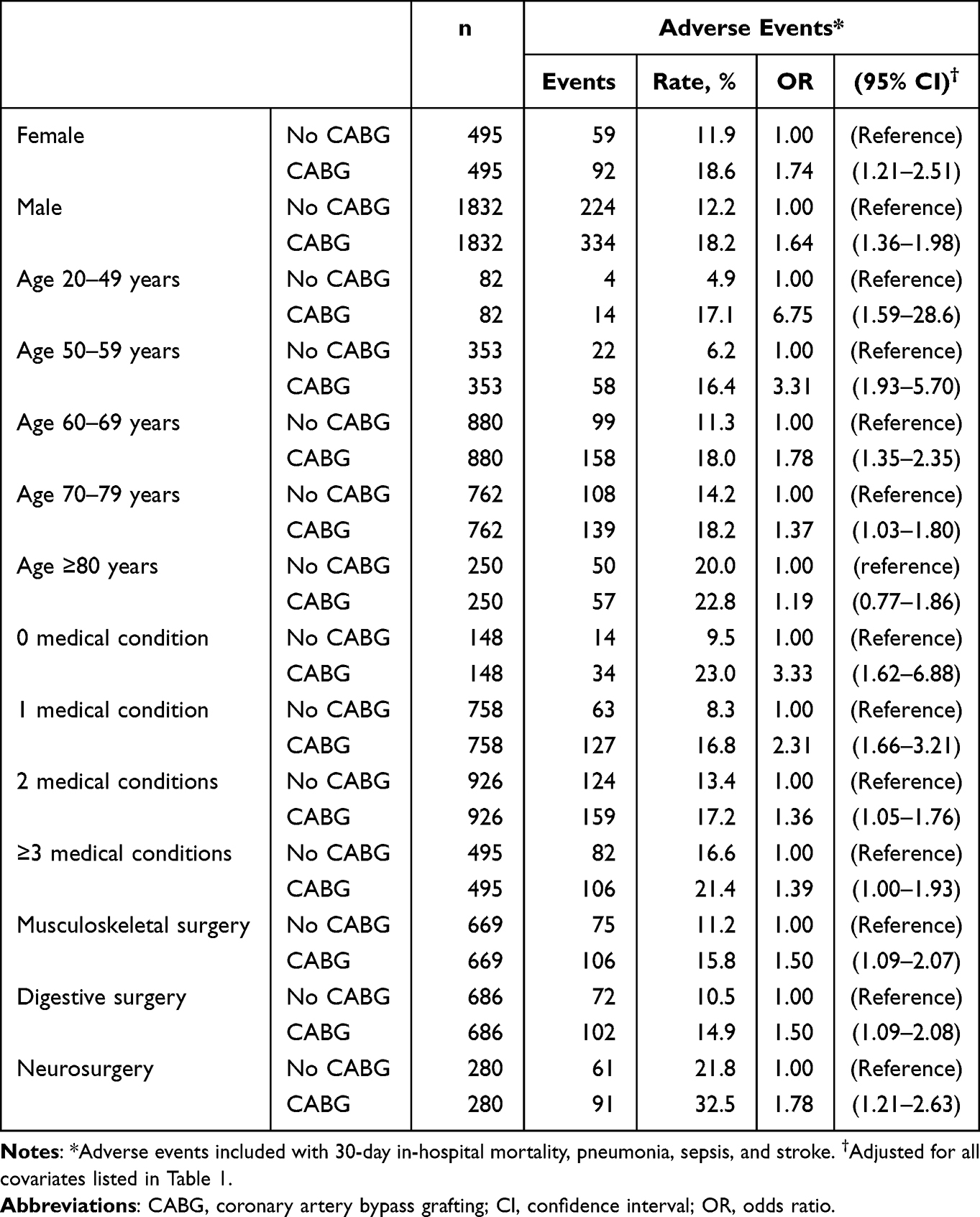 |
Table 3 The Stratified Analysis for the Association Between Postoperative Adverse Events and Previous CABG |
In Table 4, the adjusted ORs of adverse events after noncardiac surgeries for patients with preoperative 1-month, 2-month, 3-month, 6-month, and 12-month CABG were 7.94 (95% CI 3.70–17.0), 6.28 (95% CI 3.96–9.96), 4.32 (95% CI 2.99–6.23), 2.83 (95% CI 2.11–3.80), and 2.13 (95% CI 1.68–2.70), respectively.
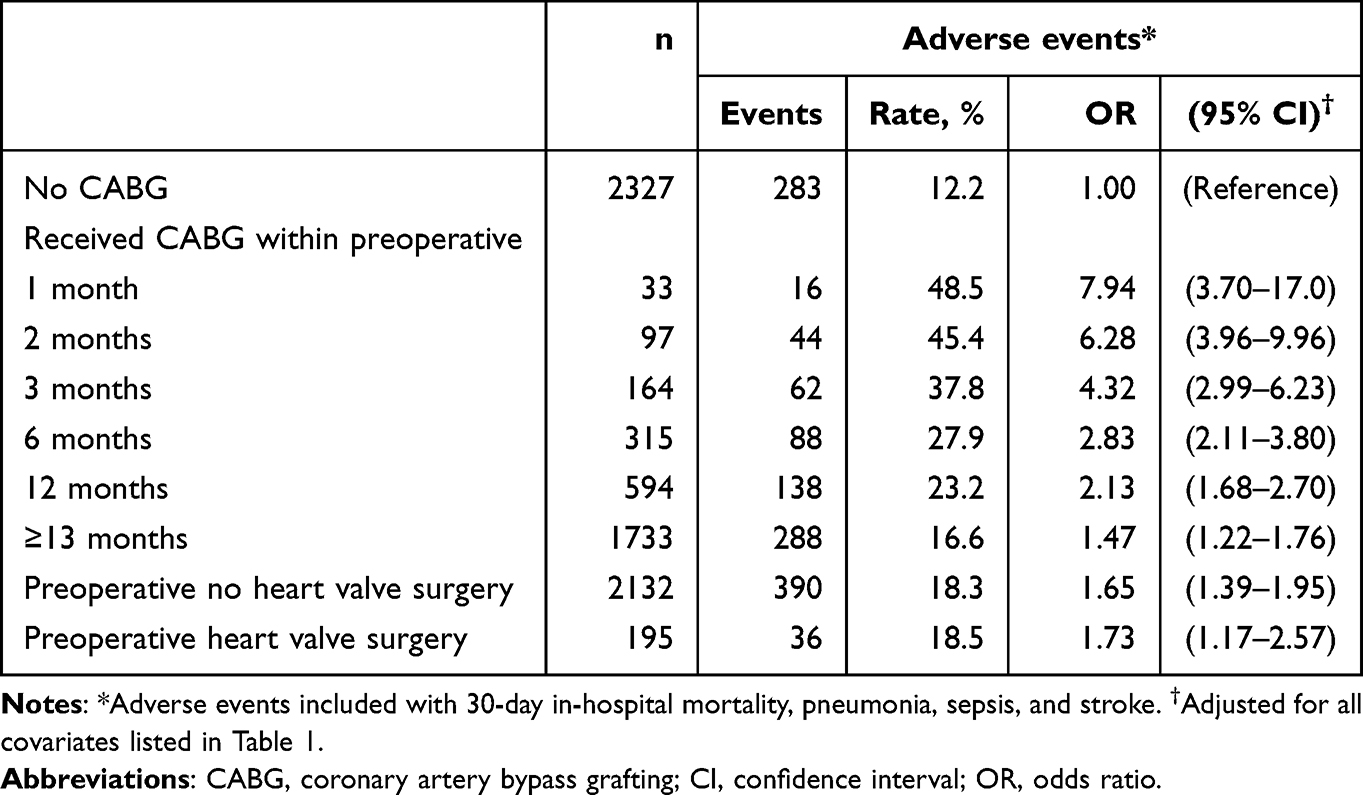 |
Table 4 The Risk of Postoperative Adverse Events Associated with the Characteristics of Previous CABG |
Discussion
In this nationwide population-based study matched by propensity score, we found that patients with prior CABG histories and who underwent noncardiac surgeries had increased risks of stroke, pneumonia, sepsis, intensive care, and 30-day in-hospital mortality. CABG patients had higher medical expenditures and longer lengths of hospital stay than the control group. The association between CABG and postoperative complications remained significant in various subgroup analyses. Furthermore, patients who received CABG less than 1 month prior exhibited the highest risks for noncardiac surgeries and continued to decline over time. The present study involved the largest CABG cohort that has been investigated to assess the postoperative risks of noncardiac surgeries thus far.4–6,11,17
In previous studies, patients with CABG and who underwent noncardiac surgeries have a similarly low 30-day mortality rate compared to those with angioplasty and even lower than those with only medically managed CAD.5,6 These data support the current practice guidelines that indicate that patients do not require preoperative cardiovascular assessment in the absence of unstable angina symptoms.7,18 However, after propensity-score matching, our study found that the postoperative complications after noncardiac surgeries were increased in CABG groups compared to those without CAD. Several possible factors should be discussed.
The surgeries induced stress responses, including acute inflammation, impaired immune function, hypermetabolism and hypercatabolism.19 Acute myocardial infarction and stroke after noncardiac surgeries are believed to share similar pathophysiological processes: plaque rupture, erosion and thrombus formation, which may be due to perioperative processes such as cardiovascular stress, hemodynamic instability, infection, activation of the sympathetic nervous system and renin-angiotensin-aldosterone system, and disseminated hypercoagulability.19–21 Risk of carotid artery stenosis is increased in a linear manner and proportional to the severity of CAD. The prevalence of significant carotid plaques in patients undergoing CABG has been reported to be high, ranging from 9% to 17%.22 CABG provides protection against vessel occlusions of the coronary artery but not of the carotid artery, which might explain the higher risk of postoperative stroke without myocardial infarction in the present study. Another possible cause of stroke is postoperative atrial fibrillation, which occurs in approximately 10% of patients following noncardiac surgeries.23 Postoperative stroke is an independent predictor of 30-day in-hospital mortality and is a risk factor for developing pulmonary complications (such as aspiration pneumonia).21,23,24 The optimal strategy to reduce stroke risk (identifying carotid artery stenosis and monitoring for atrial fibrillation) needs to be clarified in future studies. In this study, more postoperative infections were noted in patients with CABG. It was suggested that surgeries impact the immune system, which may increase the risk of sepsis.19 In addition, CABG patients had a higher incidence of postoperative intensive care, which might also explain the higher infection rate in these patients. It was well documented that intensive care-acquired infections such as pneumonia and bacteremia were common in patients who had a stay in the intensive care unit,21,25 which is consistent with the findings in this study. The pathophysiology of acute renal failure after surgery is multifactorial, including inflammation, hemodynamic compromise, postoperative urine retention, and nephrotoxic agents.21 A risk predictive model for acute renal failure after noncardiac surgeries has been reported.26 In the present study, we observed a higher incidence of postoperative acute renal failure without statistical significance in the CABG groups. These findings may be partially attributed to the lack of an increase in the risk of urinary tract infection.
The practice guidelines recommend statins and antiplatelet agents for all CABG patients without contraindications.27,28 Dual antiplatelet therapy should be used in patients undergoing off-pump bypass surgery.28 Statins also inhibited the development of vein graft occlusion and improved patency.29 The guidelines also recommend that patients should be on angiotensin-converting enzyme inhibitors or angiotensin receptor blockers if they have a history of previous myocardial infarction or left ventricular dysfunction.27,28 The cohort studies have shown that statins have pleiotropic effects, which results in a reduced risk of pneumonia in the general population as well as in patients with coronary artery disease.30,31 It has been previously shown that patients are less likely to receive medications that provide full benefits after CABG. There are several possible causes. First, concomitant conditions, such as advanced age (especially those over the age of 75), bleeding tendency, renal toxicity, hepatotoxicity, or hypotensive status, prevented the use of some of these medications. Second, there was a lack of long-term focus on the secondary prevention of cardiovascular diseases by primary care physicians. Both cardiologists and cardiovascular surgeons should be involved in the long-term care of CABG patients. In addition, the perioperative management of patients who receive antiplatelet therapy is another important issue. Unfortunately, there are no specific, widely accepted recommendations for the perioperative management of CABG patients who receive antiplatelet therapy. The continuation or discontinuation of antiplatelet agents, either too early (>10 days) or too late (≤3 days), before noncardiac surgeries may impact postoperative outcomes.32,33 The decision to stop one of the dual antiplatelet agents after multidisciplinary considerations, and subsequently evaluating the individual thrombotic and bleeding risk, is important. In addition, prophylactic therapy with β-blockers and surveillance for postoperative atrial fibrillation are also important.23
In this study, the rate of postoperative adverse events rise steady with age in the non-CABG group but not in the CABG group, resulting in a steep decline in OR. Older age is a significant risk factor for postoperative complications and mortality in our current and previous studies.15,16,21 It is reasonable that the effect of CABG on postoperative adverse events was diluted with the increasing age. Our results also showed that the OR of postoperative adverse events associated with prior CABG decreased with the number of medical conditions increased. Similar with the effects of age, more number of medical conditions represents personal critical status and it also may dilute the influence of CABG on the postoperative adverse events. Smoking cessation, cardiopulmonary rehabilitation, diet, and exercise are just as important after CABG. Lifestyle changes need to be made to prevent disease progression and, thus, improve patients’ health to combat future stress.34 However, there is a lack of data on the lifestyle impact of CABG patients undergoing noncardiac surgeries.
The other postoperative complications associated with CABG include stroke, arrhythmia, kidney injury, respiratory infection, sternal wound infection, gastrointestinal events and pericardial effusion.35 Post-CABG complications were associated with or predisposed to future adverse events when elective surgery was arranged shortly after CABG. We raised the possibility regarding deferral of elective noncardiac surgeries among patients received CABG when considering the risks, particularly for those had CABG within previous 12 months. However, critical or emergency surgeries were not in the consideration of delay surgery, especially cancer surgery.
Some limitations of our study warrant caution. First, information on the individual’s lifestyle (such as smoking, physical activity level), nutrition status, physical examination, and laboratory measures was unavailable in Taiwan’s public health insurance records. Second, the severity of CAD, presence of vascular atherosclerosis and intraoperative choice to receive bypass grafts were unknown in the current database. Failure to consider the aforementioned variables may have led to a certain degree of residual bias. Third, the true relationship between postoperative atrial fibrillation, carotid artery stenosis and stroke remains unknown in the database. However, our principal objective was to address a simple clinical question regarding the impact of prior CABG surgery on adverse postoperative outcomes in patients receiving noncardiac surgeries. In addition, the poor prognosis in patients with a history of CABG could not be totally due to the major recent surgery. Previous history included carotid stenosis, atrial fibrillation, or other medical conditions may be risk factors for postoperative adverse outcomes in this study. We admitted that residual confounding possibly existed in this study since we were unable to control all potential confounding factors in the current analysis. Finally, the present study only enrolled Taiwanese population, so determining whether the results can be extrapolated to other populations remain uncertain.
In conclusion, patients with CABG had increased risks of complications and mortality after noncardiac surgeries compared with those without CABG. Although we raised the possibility regarding deferral of non-critical elective noncardiac surgeries among patients had recent CABG when considering the risks, critical or emergency surgeries were not in the consideration of delay surgery, especially cancer surgery. Further well-designed prospective studies are needed to clarify the impact of CABG on postoperative outcomes.
Abbreviations
CABG, coronary artery bypass grafting; CAD, coronary artery disease; CI, confidence interval; ICD-9-CM, International Code of Diseases, Ninth Edition, Clinical Modification; OR, odds ratio.
Data Sharing Statement
The data underlying this study is from the Health and Welfare Data Science Center. Interested researchers can obtain the data through formal application to the Health and Welfare Data Science Center, Department of Statistics, Ministry of Health and Welfare, Taiwan (http://dep.mohw.gov.tw/DOS/np-2497-113.html) and contact the agency with email ([email protected]). Under the regulations from the Health and Welfare Data Science Center, we have made the formal application (included application documents, study proposals, and ethics approval of the institutional review board) of the current insurance data from in 2019. The authors of the present study had no special access privileges in accessing the data which other interested researchers would not have.
Acknowledgments
This study is based on data obtained from Health and Welfare Information Science Center, Ministry of Health and Welfare, Taiwan. The interpretation and conclusions in this paper do not represent Ministry of Health and Welfare, Taiwan. The authors deeply thank Prof. Chun-Chuan Shih who contributed very much to this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. TLC has equal contribution with the corresponding author.
Funding
This study was supported in part by the National Science and Technology Council, Taiwan (NSTC112-2314-B-038-141; MOST111-2320-B-532-001-MY3; MOST110-2314-B-038-108-MY2; MOST108-2320-B-038-070-MY3).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health and Welfare, ROC. 2016 statistics of causes of death; 2017 Available from: https://www.mohw.gov.tw/cp-115-33347-2.html.
2. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
3. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
4. Daye J, Boatman D, Peters C, et al. Perioperative risk of patients undergoing noncardiac surgery after coronary artery bypass surgery. J Investig Med. 2008;56(6):878–881. doi:10.2310/JIM.0b013e318182081f
5. Eagle KA, Rihal CS, Mickel MC, et al. Cardiac risk of noncardiac surgery: influence of coronary disease and type of surgery in 3368 operations. CASS Investigators and University of Michigan Heart Care Program. Coronary Artery Surgery Study. Circulation. 1997;96(6):1882–1887. doi:10.1161/01.CIR.96.6.1882
6. Hassan SA, Hlatky MA, Boothroyd DB, et al. Outcomes of noncardiac surgery after coronary bypass surgery or coronary angioplasty in the Bypass Angioplasty Revascularization Investigation (Bari). Am J Med. 2001;110(4):260–266. doi:10.1016/S0002-9343(00)00717-8
7. Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014;64(22):e77–e137. doi:10.1016/j.jacc.2014.07.944
8. Alexander JH, Smith PK. Coronary-artery bypass grafting. N Engl J Med. 2016;375(10):e22. doi:10.1056/NEJMc1608042
9. Çiçek V, Cinar T, Hayiroglu MI, et al. Preoperative cardiac risk factors associated with in-hospital mortality in elderly patients without heart failure undergoing Hip fracture surgery: a single-centre study. Postgrad Med J. 2021;97(1153):701–705. doi:10.1136/postgradmedj-2020-138679
10. Orhan AL, Çınar T, Hayıroğlu Mİ, et al. Atrial fibrillation as a preoperative risk factor predicts long-term mortality in elderly patients without heart failure and undergoing Hip fracture surgery. Rev Assoc Med Bras. 2021;67(11):1633–1638. doi:10.1590/1806-9282.20210686
11. Back MR, Stordahl N, Cuthbertson D, et al. Limitations in the cardiac risk reduction provided by coronary revascularization prior to elective vascular surgery. J Vasc Surg. 2002;36(3):526–533. doi:10.1067/mva.2002.126560
12. Hayıroğlu Mİ, Çınar T, Çiçek V, et al. A simple formula to predict echocardiographic diastolic dysfunction-electrocardiographic diastolic index. Herz. 2021;46(Suppl 2):159–165. doi:10.1007/s00059-020-04972-6
13. Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med. 2010;152(1):26–35. doi:10.7326/0003-4819-152-1-201001050-00007
14. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043–1049. doi:10.1161/01.CIR.100.10.1043
15. Sung LC, Chang CC, Yeh CC, et al. The effects of regular dental scaling on the complications and mortality after stroke: a retrospective cohort study based on a real-world database. BMC Oral Health. 2023;23(1):487. doi:10.1186/s12903-023-03178-6
16. Lin CS, Chang CC, Yeh CC, et al. Outcomes following diabetes admission in patients who had influenza vaccination: a population-based cohort study. Diabet Res Clin Pract. 2022;189:109930. doi:10.1016/j.diabres.2022.109930
17. Mahar LJ, Steen PA, Tinker JH, et al. Perioperative myocardial infarction in patients with coronary artery disease with and without aorta--coronary artery bypass grafts. J Thorac Cardiovasc Surg. 1978;76(4):533–537. doi:10.1016/S0022-5223(19)41084-2
18. Kristensen SD, Knuuti J, Saraste A, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: the Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383–2431. doi:10.1093/eurheartj/ehu282
19. Finnerty CC, Mabvuure NT, Ali A, et al. The surgically induced stress response. JPEN J Parenter Enteral Nutr. 2013;37(5 Suppl):21S–29S. doi:10.1177/0148607113496117
20. Kikura M, Oikawa F, Yamamoto K, et al. Myocardial infarction and cerebrovascular accident following non-cardiac surgery: differences in postoperative temporal distribution and risk factors. J Thromb Haemost. 2008;6(5):742–748. doi:10.1111/j.1538-7836.2008.02948.x
21. Lo PH, Chang CC, Yeh CC, et al. Adverse outcomes after non-cardiac surgeries in patients with heart failure: a propensity-score matched study. J Clin Med. 2021;10(7):1501. doi:10.3390/jcm10071501
22. Wang LJ, Ergul EA, Mohebali J, et al. The effect of combining coronary bypass with carotid endarterectomy in patients with unrevascularized severe coronary disease. J Vasc Surg. 2019;70(3):815–823. doi:10.1016/j.jvs.2018.12.026
23. Lin MH, Kamel H, Singer DE, et al. Perioperative/postoperative atrial fibrillation and risk of subsequent stroke and/or mortality. Stroke. 2019;50(6):1364–1371. doi:10.1161/STROKEAHA.118.023921
24. Lewis DJ, Al-Ghazawi SS, Al-Robaidi KA, et al. Perioperative stroke associated in-hospital morbidity and in-hospital mortality in common non-vascular non-neurological surgery. J Clin Neurosci. 2019;67:32–39. doi:10.1016/j.jocn.2019.06.034
25. Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–2329. doi:10.1001/jama.2009.1754
26. Wilson TA, de Koning L, Quinn RR, et al. Derivation and external validation of a risk index for predicting acute kidney injury requiring kidney replacement therapy after noncardiac surgery. JAMA Network Open. 2021;4(8):e2121901. doi:10.1001/jamanetworkopen.2021.21901
27. Sousa-Uva M, Head SJ, Milojevic M, et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur J Cardiothorac Surg. 2018;53(1):5–33. doi:10.1093/ejcts/ezx314
28. Kulik A, Ruel M, Jneid H, et al. Secondary prevention after coronary artery bypass graft surgery: a scientific statement from the American Heart Association. Circulation. 2015;131(10):927–964. doi:10.1161/CIR.0000000000000182
29. Kulik A, Voisine P, Mathieu P, et al. Statin therapy and saphenous vein graft disease after coronary bypass surgery: analysis from the CASCADE randomized trial. Ann Thorac Surg. 2011;92(4):1284–1290. doi:10.1016/j.athoracsur.2011.04.107
30. Nielsen AG, Nielsen RB, Riis AH, et al. The impact of statin use on pneumonia risk and outcome: a combined population-based case-control and cohort study. Crit Care. 2012;16(4):R122. doi:10.1186/cc11418
31. Lin CF, Chang YH, Liu JC, et al. Statin use associated with a reduced risk of pneumonia requiring hospitalization in patients with myocardial infarction: a nested case-control study. BMC Cardiovasc Disord. 2016;16(1):24. doi:10.1186/s12872-016-0202-x
32. Oscarsson A, Gupta A, Fredrikson M, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010;104(3):305–312. doi:10.1093/bja/aeq003
33. Sundström J, Hedberg J, Thuresson M, et al. Low-dose aspirin discontinuation and risk of cardiovascular events: a Swedish nationwide, population-based cohort study. Circulation. 2017;136(13):1183–1192. doi:10.1161/CIRCULATIONAHA.117.028321
34. Niebauer J. Is there a role for cardiac rehabilitation after coronary artery bypass grafting? Treatment after coronary artery bypass surgery remains incomplete without rehabilitation. Circulation. 2016;133(24):2529–2537. doi:10.1161/CIRCULATIONAHA.116.021348
35. Montrief T, Koyfman A, Long B. Coronary artery bypass graft surgery complications: a review for emergency clinicians. Am J Emerg Med. 2018;36(12):2289–2297. doi:10.1016/j.ajem.2018.09.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.