Back to Journals » Risk Management and Healthcare Policy » Volume 19
How Does Social Frailty Evolve Among Patients with Prostate Cancer? Evidence from Regression Models versus Fuzzy Set Qualitative Comparative Analysis
Authors Wan Y, Li N, Zhuang S, Gu Y, Shen L, Ye J
Received 20 January 2026
Accepted for publication 6 April 2026
Published 14 April 2026 Volume 2026:19 597629
DOI https://doi.org/10.2147/RMHP.S597629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Yueting Wan,* Na Li,* Shiwei Zhuang, Yuanchun Gu, Linjie Shen, Jing Ye
Department of Urology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, 200129, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Ye, Department of Urology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, 200129, People’s Republic of China, Email [email protected]
Background: Social frailty is a critical indicator of declining social functioning and affects quality of life in older adults. Prostate cancer patients face greater challenges in social frailty than the general elderly population, due to the physical burden of the disease, treatment-related adverse effects, and psychological stress. However, its multidimensional influencing factors and risk patterns remain unclear.
Objective: To identify key factors and configurations associated with social frailty in patients with prostate cancer.
Methods: This study was guided by the Health Ecology Model and used a cross-sectional design. A total of 211 patients were recruited from Shanghai East Hospital between April and September 2025. Structured questionnaires assessed sociodemographic characteristics, family function, living space, depressive symptoms, and social frailty. Data were analyzed using hierarchical regression and fuzzy-set qualitative comparative analysis (fsQCA), enabling the examination of both net effects and complex configurational pathways.
Results: The mean age of participants was (69.20 ± 5.63) years, and the prevalence of social frailty was 39.81%. The final regression model was significant (F=101.37, P< 0.001) and explained 80.1% of the variance in social frailty. Depression, exercise frequency, family function, living space, and residence location were retained in the final model as factors associated with social frailty. FsQCA identified four configurations associated with social frailty (overall consistency=0.899; coverage=0.468). The configuration with the highest coverage included low education, urban residence, insufficient exercise, poor family function, high depression, and restricted living space (consistency=0.873).
Conclusion: Social frailty among patients with prostate cancer reflects the influence of psychosocial, behavioral, and environmental conditions. Social frailty was significantly associated with depression, family function, living space, residence, and exercise frequency. High social frailty was associated with specific configurations of these factors. These results advance understanding of social frailty from isolated risk factors to combined pathway patterns. They help inform targeted screening and tailored intervention strategies for this population.
Keywords: social frailty, prostate cancer, fuzzy set qualitative comparative analysis, life space, health ecology model
Introduction
Research Background
Prostate cancer is one of the most common malignancies among men and predominantly affects older adults.1 The incidence of prostate cancer in China rose from 10.2 per 100,000 in 2015 to 18.6 per 100,000 in 2022,2,3 showing a steady upward trend. Advances in diagnostic and therapeutic technologies have led to substantial improvements in the survival of patients. However, “living longer” does not mean “living better”. Many patients exhibit typical characteristics of social frailty during the stages of diagnosis, treatment, and rehabilitation.4 The concept of social frailty was first proposed by Bunt in 2017.4 It refers to a multidimensional state involving a gradual decline in social participation, social support, and social role functioning. As an emerging health concept following physical and psychological frailty, social frailty has attracted increasing attention in the fields of geriatrics and public health. Previous studies have linked social frailty to adverse outcomes, including disability, functional dependence, sarcopenia, and even all-cause mortality.5–8
Patients with prostate cancer may be particularly vulnerable to social frailty.9 Compared with the general older population, they often face additional challenges across physiological, psychological, and social domains. Physiologically, prostate cancer and its treatments may lead to complications such as urinary incontinence and sexual dysfunction, which restrict daily activities and social participation.10 Psychologically, patients frequently experience anxiety and depression during disease progression and treatment.11 Socially, illness-related stigma and reduced social engagement may further limit access to external support.12 Therefore, social frailty in this population reflects not only aging but also the combined influence of disease, treatment, and psychosocial conditions. Investigating social frailty among patients with prostate cancer is essential for developing targeted interventions to improve quality of life.
Existing evidence suggests that social frailty is influenced by multiple factors. Demographic characteristics such as age and education may affect access to social resources and participation opportunities.13 Behavioral factors, particularly regular physical exercise, help maintain physical function and social engagement.14 Psychosocial conditions are also important; depressive symptoms and poor family functioning have been associated with increased vulnerability to social frailty.15–18 Environmental factors, including residential context and living space, may further shape opportunities for social participation. Based on this evidence, this study included demographic characteristics (age and education), behavioral factors (exercise frequency), psychosocial factors (depression and family function), and environmental conditions (residential area and living space) as candidate variables.
Despite growing interest in frailty among patients with prostate cancer, most studies have focused on physical or psychological frailty, while social frailty has received far less attention.19 In particular, limited evidence exists regarding its risk and protective factors, and little is known about how multiple factors interact to shape social frailty in this population. Methodologically, previous studies have mainly relied on regression analysis or structural equation modeling, which may not fully capture the complex interactions among multiple conditions. Fuzzy Set Qualitative Comparative Analysis (fsQCA) provides a useful complement because it can identify configurational pathways through which multiple factors jointly contribute to an outcome.
This study hypothesized that social frailty among patients with prostate cancer is not attributable to a single factor but rather reflects the combined influence of demographic characteristics, disease-related conditions, and psychosocial resources. Different combinations of these conditions may be associated with a high risk of social frailty. Identifying these configurations may provide evidence for developing targeted social rehabilitation interventions in clinical practice.
Theoretical Framework
To better understand the mechanisms underlying social frailty among patients with prostate cancer, this study adopted the Health Ecology Model as the theoretical framework. The model proposed by McLeroy et al20 emphasizes that health outcomes are shaped by multiple ecological levels, including individual characteristics, interpersonal relationships, and broader environmental contexts. Guided by this framework, the variables in this study were classified into three ecological levels: (1) the micro level (individual and behavioral factors), including age, education, depression, and exercise frequency; (2) the meso level (interpersonal relationships), represented by family function; and (3) the macro level (environmental context), including residential area and living space. Applying this model allows examination of how factors across ecological levels interact to form configurational pathways leading to social frailty.
Methods
Study Design, Setting, and Sample
A cross-sectional study design was adopted, and self-reported data were collected through both online and paper-based questionnaires. Participants were recruited using a consecutive sampling method from patients with prostate cancer who attended the Department of Urology at Shanghai East Hospital. The inclusion criteria were: (1) a confirmed diagnosis of prostate cancer based on the 2020 European Association of Urology (EAU) Guidelines; (2) adequate comprehension and communication abilities; and (3) awareness of their condition and voluntary participation. The exclusion criteria were: (1) concurrent malignant tumors or severe organic diseases; and (2) severe cognitive impairment or psychiatric disorders that hindered understanding or cooperation.
Measurement
Demographic Information
To summarize participants’ characteristics, the research team developed a questionnaire that included sociodemographic variables such as age, educational level, residential area, and exercise frequency. Residential area was classified as urban or rural according to participants’ self-reported current place of residence based on the Chinese administrative division system. Exercise frequency referred to the number of aerobic exercise sessions per week. Participants were informed that aerobic exercise included activities such as walking, brisk walking, jogging, and square dancing. One exercise session was defined as aerobic physical activity lasting at least 30 minutes.
Social Frailty
Social frailty was assessed using the HALFT (Help, Participation, Loneliness, Financial, and Talk) scale. The scale was developed by Ma et al21 using data from a longitudinal study of older adults in Chinese communities and has been widely used in China. The HALFT scale includes five dimensions with one item in each, assessing help to others, social participation, loneliness, financial sufficiency, and daily communication with family or friends. For scoring, one point was assigned for a “yes” response to item 3 (Loneliness) and zero for “no”. For the remaining items, a “no” response was assigned one point and a “yes” response was assigned zero. The total score ranged from 1 to 5, with a score of 3 or higher indicating the presence of social frailty. In this study, the Cronbach’s α coefficient for the scale was 0.788.
Life Space
The Life Space Assessment (LSA) was used to evaluate participants’ mobility range and level of independence. The scale was developed by Baker et al22 and translated into Chinese by Ji et al23 It consists of five levels representing progressively wider geographic areas, from within the home to the broader community. The total LSA score is calculated as the sum of the product of life-space level, independence, and frequency scores, yielding a range from 1 to 120, with higher scores indicating greater mobility. Scores below 60 suggest restricted life space. In this study, the LSA demonstrated good reliability (Cronbach’s α = 0.772).
Family Function
Family function was assessed using the Adaptability, Partnership, Growth, Affection, and Resolve (APGAR) scale. The scale was developed by Smilkstein at the University of Washington in 197824 to comprehensively evaluate individuals’ subjective satisfaction with family functioning across five dimensions. The APGAR scale consists of five items and adopts a three-point Likert scoring system. Each item is rated as “almost always” (2 points), “sometimes” (1 point), or “hardly ever” (0 points). All items are negatively scored, and the total score ranges from 0 to 10, with higher scores indicating better family function. Specifically, total scores of 0–3 indicate severe family dysfunction, 4–6 indicate moderate dysfunction, and 7–10 represent good family function. The scale has demonstrated good reliability and validity, with a Cronbach’s α coefficient of 0.803 in this study.
Depression
Depressive symptoms were measured using the Hospital Depression Scale (HDS), which was developed by Zigmond and Snaith in 1983.25 The scale consists of seven items that assess how frequently patients experienced depressive feelings over the past month. Each item is rated on a four-point scale ranging from 0 to 3, with the total score being the sum of all item scores. The total score ranges from 0 to 21, with higher scores indicating more severe depressive symptoms. According to the total score, depression severity was categorized into four levels: 0–7 as normal, 8–10 as mild, 11–14 as moderate, and 15–21 as severe. In this study, the scale demonstrated satisfactory reliability, with a Cronbach’s α coefficient of 0.840.
Data Collection
Before the investigation, all members involved in data collection received standardized training. For patients who met the inclusion criteria, data were collected within 24 hours after hospital admission. The survey was conducted using a combination of offline paper questionnaires and online electronic forms. Prior to questionnaire distribution, the researchers explained the study objectives, content, estimated completion time, and data confidentiality principles to all participants. The survey was administered only after obtaining informed consent. For any items that patients did not understand, standardized terminology was used to provide clarification. During the online survey, clear instructions were included in the questionnaire. The researchers’ contact information was also provided so that participants could seek assistance when needed. After completion, all questionnaires were immediately checked by the research team to ensure data completeness and reliability.
Statistical Analysis
Descriptive and regression analyses of all variables were conducted using IBM SPSS version 25. Fuzzy-set qualitative comparative analysis (fsQCA) was performed with fsQCA software version 3.0 to identify the necessary and sufficient conditions leading to specific outcomes. Before the analysis, raw data were converted into fuzzy-set membership scores to reflect the degree to which each individual belonged to a given condition set. Following the recommendations of Ragin,26 three calibration thresholds were selected: full membership (1.0), full non-membership (0.0), and a crossover point (0.5). All scale scores were calibrated accordingly. A necessity analysis was first conducted. A condition with a consistency score greater than 0.90 was considered a necessary condition for the occurrence of the outcome. Subsequently, a truth table was constructed, and the thresholds for consistency and coverage were set to generate all possible combinations of conditions. Based on these results, the complex, parsimonious, and intermediate solutions were obtained. Raw coverage was used to evaluate the proportion of cases explained by each configuration, unique coverage represented the extent to which a specific configuration uniquely explained the outcome, and consistency indicated the reliability and goodness of fit of each configuration in explaining the outcome.
Results
Sample Characteristics
The study was initiated in April 2025, and data collection lasted for approximately six months. A total of 211 valid samples were obtained. Participants ranged in age from 62 to 87 years, with a mean age of (69.20 ± 5.63) years. In terms of educational background, most participants had a middle school education (54.5%). Urban residents accounted for 60.19% of the total sample, and the average exercise frequency was (4.05 ± 1.65) times per week. The mean social frailty score among participants was (2.11 ± 0.88), and 39.81% met the criteria for social frailty. Detailed characteristics of the participants are presented in Table 1.
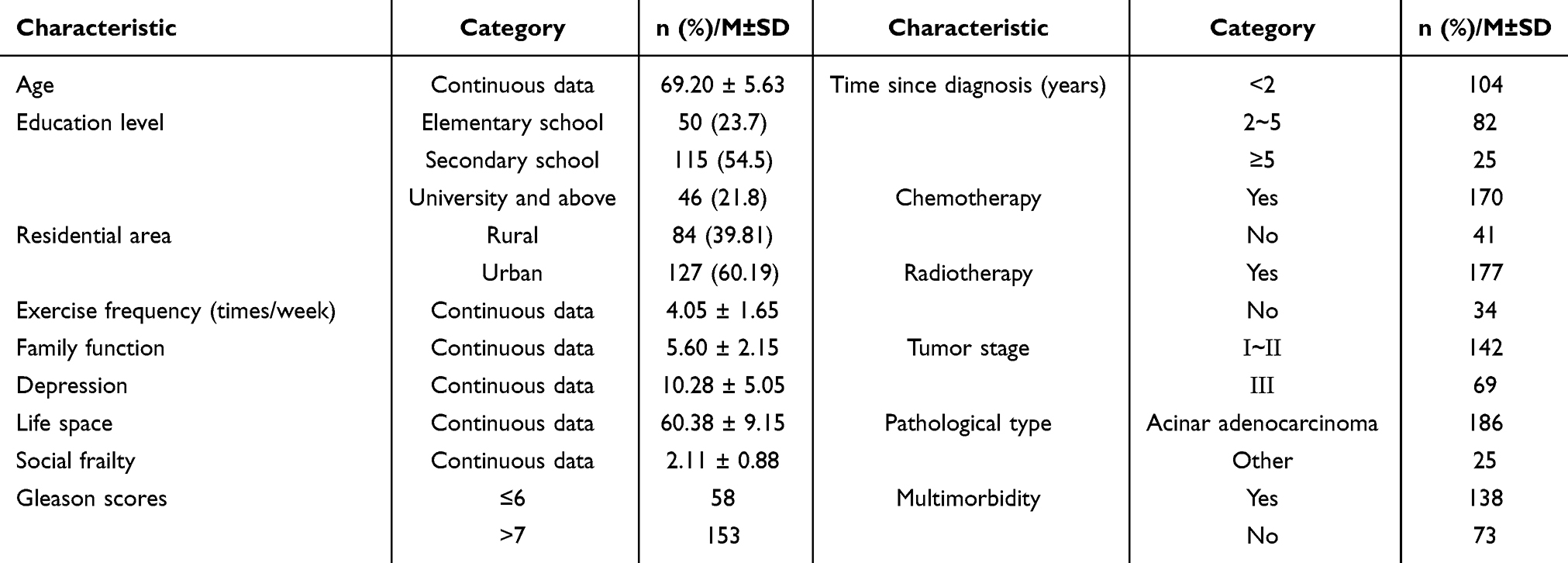 |
Table 1 Descriptive Statistics of Participants’s Characteristics (n=211) |
Hierarchical Regression Models
A hierarchical regression analysis was conducted to examine the predictive effects of individual and behavioral variables, interpersonal relationship variables, and environmental variables on social frailty. As shown in Table 2, after entering individual and behavioral variables (age, education level, exercise frequency, and depression) into the first model, the R2 value was 0.735 (F=113.517, P<0.001). Among these, exercise frequency (β =–0.522, P<0.001) and depression (β=0.448, P<0.001) were significant predictors. When the interpersonal relationship variable (family function) was added to the second model, the R2 value increased to 0.771 (F=114.151, P<0.001), with a ΔR2 of 0.036. Family function was identified as a significant negative predictor (β=–0.257, P<0.001). In the third model, the environmental variables (residence and living space) were included, and the R2 value further increased to 0.801 (F=101.374, P<0.001), with a ΔR2 of 0.030. Both living space and residence had significant effects on social frailty (β =–0.237, P<0.01; β=0.075, P<0.05, respectively). Multicollinearity diagnostics for the final model indicated no evidence of serious collinearity among the predictors (tolerance = 0.440~0.977; VIF = 1.021~2.273).
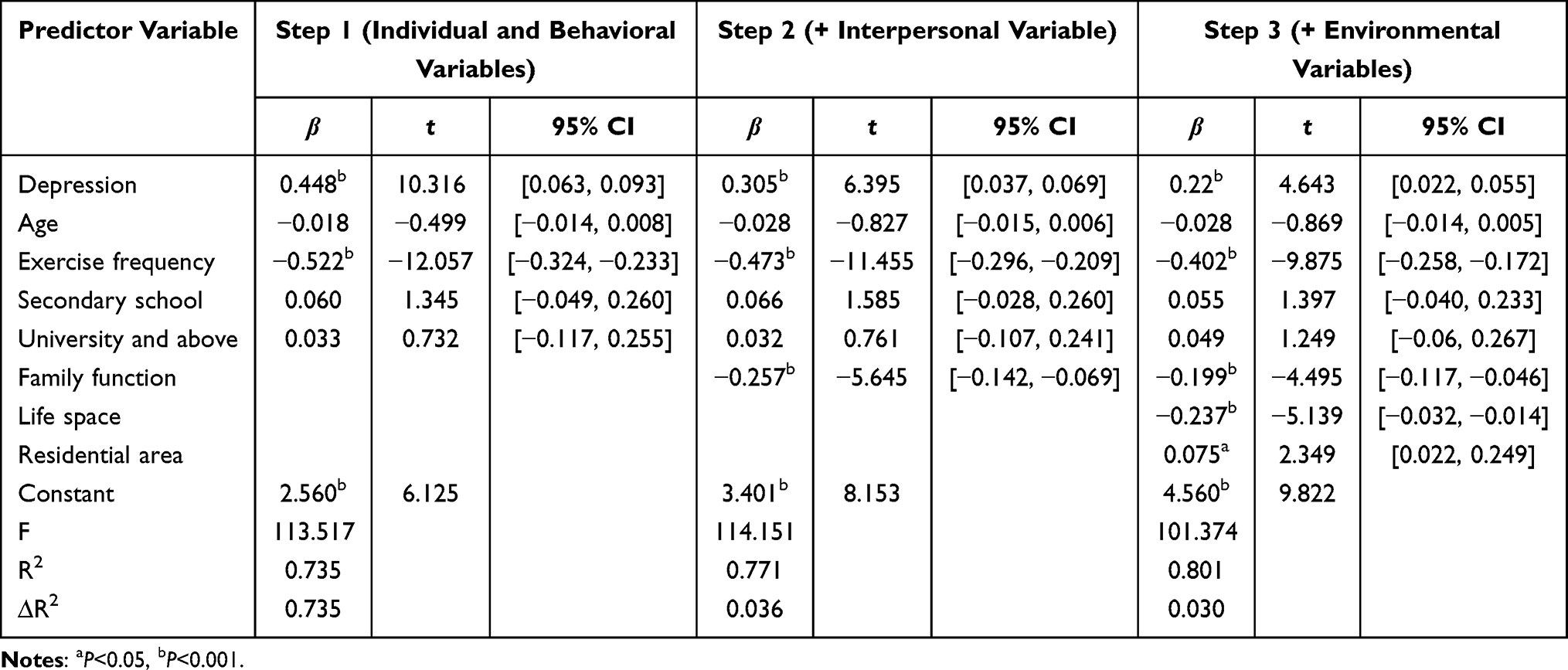 |
Table 2 Hierarchical Regression Results for Predictors of Social Frailty (n=211) |
FsQCA
Calibration
Calibration converts raw data into set membership scores ranging from 0 to 1. For continuous variables, we used a percentile-based calibration approach. Full membership was set at the 75th percentile. The crossover point was set at the 50th percentile, and full non-membership at the 25th percentile. Dichotomous variables were coded as 0 or 1. A small constant (0.001) was added to avoid excluding cases with a membership score of exactly 0.5.27 Supplementary Materials 1 presents the calibration thresholds for all conditions and the outcome.
Necessary Analysis
Before performing fsQCA, each condition was examined to determine whether it constituted a necessary condition.28 As shown in Table 3, for the outcome variable of social frailty, the consistency values of all conditions were below 0.9. Based on this result, it was concluded that none of the individual conditions served as a necessary condition influencing social frailty.
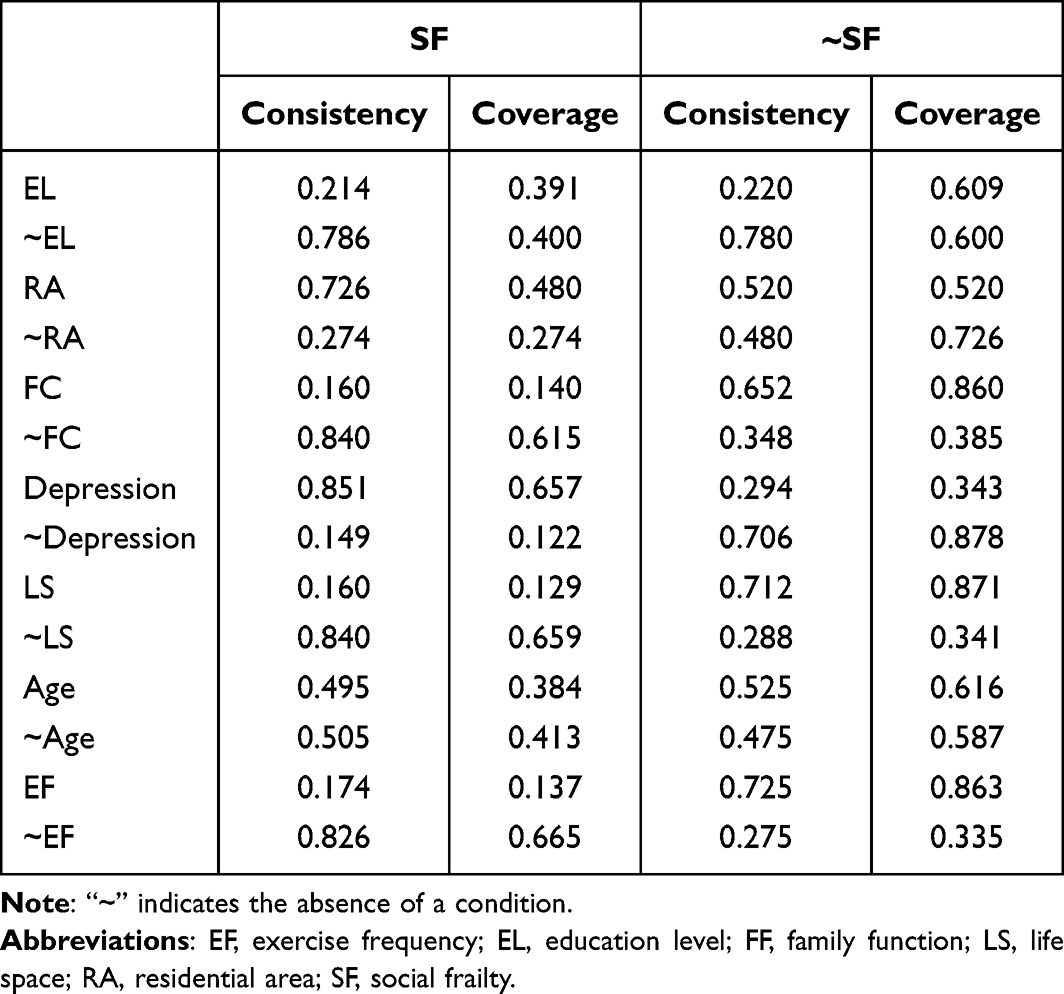 |
Table 3 Univariate Necessity Analysis |
Sufficiency Analysis
A truth table was constructed to identify configurations associated with high social frailty. Following Fiss’s recommendations,29,30 we set the frequency threshold at 3 based on the sample size. The consistency and Proportional Reduction in Inconsistency (PRI) thresholds were set at 0.8 and 0.7, respectively. The Quine–McCluskey algorithm was then applied to generate three types of solutions. We selected the intermediate solution for interpreting the final configurations. Core conditions were those that appeared in both the intermediate and parsimonious solutions. Peripheral conditions appeared only in the intermediate solution.29,31
The fsQCA results yielded four configurations associated with high social frailty (overall solution coverage = 0.468, consistency = 0.899). These configurations together explained nearly half of the cases with high social frailty. Table 4 presents the core and peripheral conditions for each configuration, following Pappas and Woodside’s recommendation.30
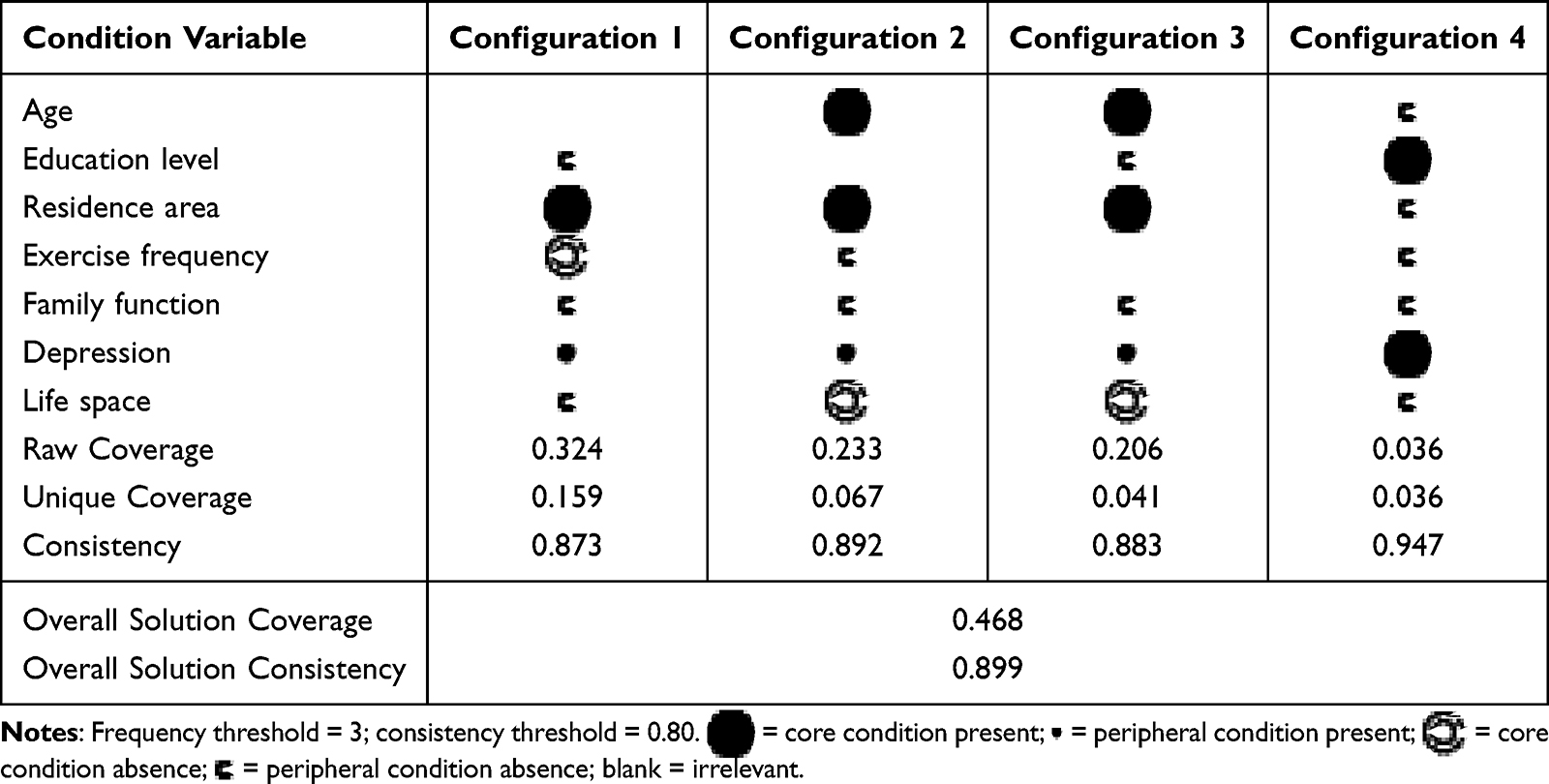 |
Table 4 Configurations for High Social Frailty |
Configuration 1 was the most common pathway (raw coverage = 32.4%). It captured urban patients with lower education who faced multiple concurrent challenges: lack of exercise, insufficient family support, high depression, and restricted living space.
Configuration 2 described a similar urban profile but highlighted older age as an additional factor, alongside the same combination of insufficient exercise, poor family support, high depression, and restricted living space.
Configuration 3 also pertained to urban patients, combining older age, lower education, insufficient family care, depression, and restricted living space.
Configuration 4 showed that even younger, rural, and higher-educated patients could develop high social frailty when they lacked exercise, had inadequate family support, experienced high depression, and faced restricted living space.
Robustness Test
To test the robustness of the fsQCA results, the consistency threshold was increased from 0.8 to 0.85 and the analysis was repeated. As shown in Supplementary Materials 2, three configurations were repeated across both analyses. These findings indicate that the initially configurational model demonstrated acceptable robustness.
Discussion
Main Findings
Guided by the Health Ecology Model, this study examined influencing factors influencing social frailty among prostate cancer patients across individual, interpersonal, and environmental levels. Using hierarchical regression and fsQCA, we identified both independent effects and multiple pathways leading to high social frailty.
Both hierarchical regression and fsQCA analyses identified high depression and limited living space as key risk factors for social frailty in prostate cancer patients. Limited living space is likely multifactorial. Physical limitations may stem from the disease itself or its treatment, including urinary dysfunction, fatigue, and chronic pain. These limitations are linked to reduced participation in daily activities and social interactions.32 Psychological stress related to illness may further reduce patients’ willingness to engage with the outside world.33 Confinement to closed environments limits opportunities for social interaction and emotional support, which is associated with higher depression and greater social frailty.34 Depressive symptoms such as low mood and fatigue may reduce motivation to go outdoors. This can lead to a cycle where reduced mobility and limited social engagement reinforce each other.35 Interventions aimed at expanding patients’ accessible environment could help restore their sense of agency. Such interventions may include home modifications or mobility support. Sustained psychological care should also be provided to slow this decline.
The regression model indicated that better family function and more frequent exercise were associated with lower levels of social frailty. These factors may partially mitigate the adverse effects of depression and restricted living space. This finding provides a potential direction for intervention. In the Chinese cultural context, the family represents the primary source of support for many patients with chronic diseases.36 It often serves as an important social resource that helps maintain social connectedness when external engagement declines.37 Concurrently, exercise has well documented physiological and psychological benefits. It can improve physical function and has been associated with reduced depressive symptoms through mechanisms such as endorphin release.38 Family support and regular exercise may work together to help maintain social engagement among prostate cancer patients. Family encouragement may facilitate adherence to physical activity, while improved physical capacity may help patients sustain participation in social life. These observations suggest that interventions addressing social frailty may benefit from integrating family support, physical activity promotion, and psychological care. For example, family-based empowerment programs or co-exercise activities could be considered to support social functioning in this population.
Notably, the fsQCA results revealed a more nuanced picture of urban–rural differences than previously reported. Earlier studies have suggested that urban residents generally exhibit lower levels of social frailty due to greater social opportunities and access to resources.13 However, our findings suggest that urban residence also be associated with social frailty when combined with insufficient family support, restricted living space, and high depression. This pattern indicates that social frailty is not determined by urban–rural status alone. Rather, it appears to reflect the interaction between environmental conditions and individual vulnerability factors. In urban contexts, limited family support, constrained living environments, and psychological distress may jointly shape the experience of social disconnection.39,40 By contrast, rural areas often have fewer institutional resources. However, stronger family ties and closer neighborhood relationships may provide everyday forms of support that help maintain social connectedness. This perspective draws attention to the possibility of “hidden social frailty” among urban patients, a phenomenon that may be overlooked in resource-rich environments. Future studies could further examine how processes of urbanization reshape social support structures and how these changes relate to patterns of social connectedness and vulnerability.
Through fsQCA, two configurations leading to social frailty were identified among prostate cancer patients living in urban areas. Although these configurations shared common features such as insufficient family support, prominent depressive symptoms, and restricted living space, they differed in their dominant conditions. One configuration was characterized by reduced exercise frequency and was referred to as the “behaviorally constrained type” (Configuration 2). The other was associated with lower educational attainment and was termed the “low cognitive resource type” (Configuration 3). These findings suggest that social frailty among prostate cancer patients may arise through different pathways shaped by behavioral and cognitive constraints. From a practical perspective, patients in the behaviorally constrained group may benefit from rehabilitation programs that emphasize safety, feasibility, and privacy. For patients in the cognitively constrained group, clear and accessible educational materials may help improve understanding and engagement with available social resources.
Strengths and Limitations
Guided by the Health Ecology Model, we systematically integrated multilevel factors including individual characteristics and behaviors, interpersonal support, and living environment. This framework enabled us to explore the formation mechanisms of social frailty among patients with prostate cancer from a multidimensional perspective. Hierarchical regression was applied to estimate individual predictors of social frailty, and fsQCA was used to capture complex causal configurations. Together, these approaches address the constraints of linear analysis.
Despite these strengths, several limitations should be acknowledged. First, the cross-sectional design, single-center sampling, and self-reported data may limit the generalizability of the findings. Second, clinical variables were not included in the analytical model. Finally, although no evidence of multicollinearity was detected, the relatively high explanatory power of the regression model may be partly attributable to the theory-driven selection of variables and the relatively homogeneous sample. Therefore, the findings should be interpreted with caution. Future studies should adopt longitudinal, multicenter designs, incorporate clinical indicators, and aim to provide more comprehensive evidence on factors associated with social frailty in prostate cancer patients.
Conclusion
Based on the Health Ecology Model, this study identified multiple factors associated with social frailty among patients with prostate cancer. Depression, restricted living space, and urban residence were positively associated with social frailty, whereas better family functioning and regular exercise were negatively associated with social frailty. The fsQCA findings further suggested that social frailty may reflect the combined influence of multiple conditions, particularly the co-occurrence of high depression, low family functioning, and restricted living space. Overall, these findings highlight the multifactorial nature of social frailty and may inform the development of tailored interventions. Further longitudinal studies are needed to confirm these associations.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of Shanghai East Hospital (No. 2025YS-106) and was conducted in strict accordance with the principles of the Declaration of Helsinki. All participants were informed of the study’s purpose and procedures before participation and provided written informed consent. Participants’ privacy and anonymity were fully protected throughout the study, and all data were stored in an anonymized format.
Acknowledgments
The authors would like to express their sincere gratitude to all the patients who generously participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no funding or conflicts of interest to disclose.
References
1. Ribeiro CH, Campelo BBF, de Souza VMG, et al. Câncer de próstata: atualizações em diagnóstico e tratamento-revisão integrativa. Braz J Implantol Health Sci. 2024;6(9):400–10. doi:10.36557/2674-8169.2024v6n9p400-409
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Zhang S, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2015. J Natl Cancer Cent. 2021;1(1):2–11. doi:10.1016/j.jncc.2020.12.001
4. Bunt S, Steverink N, Olthof J, et al. Social frailty in older adults: a scoping review. Eur J Ageing. 2017;14:323–334. doi:10.1007/s10433-017-0414-7
5. Ko Y, Lee K. Social frailty and health-related quality of life in community-dwelling older adults. Int J Environ Res Public Health. 2022;19(9):5659. doi:10.3390/ijerph19095659
6. Teo N, Gao Q, Nyunt MSZ, et al. Social frailty and functional disability: findings from the Singapore longitudinal ageing studies. J Am Med Directors Assoc. 2017;18(7):
7. Makizako H, Kubozono T, Kiyama R, et al. Associations of social frailty with loss of muscle mass and muscle weakness among community‐dwelling older adults. Geriatr Gerontol Int. 2019;19(1):76–80. doi:10.1111/ggi.13571
8. Ragusa FS, Veronese N, Smith L, et al. Social frailty increases the risk of all-cause mortality: a longitudinal analysis of the English Longitudinal Study of Ageing. Exp Gerontology. 2022;167:111901. doi:10.1016/j.exger.2022.111901
9. Bentefouet L, Jalloh M, Thiam NM, et al. Prostate cancer in the thies region, senegal: epidemiological, diagnostic and therapeutic aspects. Open J Urol. 2024;14(2):71–82. doi:10.4236/oju.2024.142008
10. Ryan CJ, Small EJ. Advances in prostate cancer. Curr Opin Oncol. 2004;16(3):242–246. doi:10.1097/00001622-200405000-00009
11. Irusen H, Fernandez P, Van der Merwe A, et al. Depression, Anxiety, and their association to health-related quality of life in men commencing prostate cancer treatment at tertiary hospitals in cape town, South Africa. Cancer Control. 2022;29:10732748221125561. doi:10.1177/10732748221125561
12. Roberts C, Toohey K, Paterson C. The experiences and unmet supportive care needs of partners of men diagnosed with prostate cancer: a meta-aggregation systematic review. Cancer Nurs. 2024;47(3):E168–E80. doi:10.1097/NCC.0000000000001172
13. Qi X, Jia N, Hu J, et al. Analysis of the status of social frailty in Chinese older adults with cardiovascular and cerebrovascular diseases: a National Cross-Sectional Study. Front Public Health. 2023;11:1022208. doi:10.3389/fpubh.2023.1022208
14. Makizako H, Tsutsumimoto K, Shimada H, et al. Social frailty among community-dwelling older adults: recommended assessments and implications. Ann Geriatr Med Res. 2018;22(1):3–8. doi:10.4235/agmr.2018.22.1.3
15. Wang J, Xu S, Liu J, et al. The mediating effects of social support and depressive symptoms on activities of daily living and social frailty in older patients with chronic heart failure. Geriatric Nurs. 2023;53:301–306. doi:10.1016/j.gerinurse.2023.08.003
16. Inoue T, Maeda K, Satake S, et al. Osteosarcopenia, the co-existence of osteoporosis and sarcopenia, is associated with social frailty in older adults. Aging Clin Exp Res. 2022;34(3):535–543. doi:10.1007/S40520-021-01968-Y
17. Schmahl O, Jeuring H, Aprahamian I, et al. Impact of childhood trauma on multidimensional frailty in older patients with a unipolar depressive-, anxiety-or somatic symptom disorder. Arch Gerontol Geriatr. 2021;96:104452. doi:10.1016/j.archger.2021.104452
18. Silva A, Ottaviani AC, Orlandi FS, et al. Social support perceived by elderly people in social vulnerability according to family functionality: a cross-sectional study. Revista da Escola de Enfermagem da U S P. 2023;57:e20220475. doi:10.1590/1980-220X-REEUSP-2022-0475en
19. Chambers SK, Chung E, Wittert G, et al. Erectile dysfunction, masculinity, and psychosocial outcomes: a review of the experiences of men after prostate cancer treatment. Transl Androl Urol. 2017;6(1):60–68. doi:10.21037/tau.2016.08.12
20. McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi:10.1177/10901981880150040
21. Ma L, Sun F, Tang Z. Social frailty is associated with physical functioning, cognition, and depression, and predicts mortality. J Nutr Health Aging. 2018;22(8):989–995. doi:10.1007/s12603-018-1054-0
22. Baker PS, Bodner EV, Allman RM. Measuring life-space mobility in community-dwelling older adults. J Am Geriatr Soc. 2003;51(11):1610–1614. doi:10.1046/j.1532-5415.2003.51512.x
23. Ji M, Zhou Y, Liao J, et al. Pilot study on the Chinese version of the life space assessment among community-dwelling elderly. Arch Gerontol Geriatrics. 2015;61(2):301–306. doi:10.1016/j.archger.2015.06.012
24. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978;6(6):1231–1239.
25. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 1983;67(6):361–370. doi:10.1111/J.1600-0447.1983.Tb09716.X
26. Rihoux B, Ragin CC. Configurational Comparative Methods: Qualitative Comparative Analysis (QCA) and Related Techniques. Sage; 2009.
27. Crilly D, Zollo M, Hansen MT. Faking it or muddling through? Understanding decoupling in response to stakeholder pressures. Acad Manage J. 2012;55(6):1429–1448. doi:10.5465/amj.2010.0697
28. Ragin CC. Redesigning Social Inquiry: Fuzzy Sets and Beyond. University of Chicago Press; 2009.
29. Fiss PC. Building better causal theories: a fuzzy set approach to typologies in organization research. Acad Manage J. 2011;54(2):393–420. doi:10.5465/amj.2011.60263120
30. Pappas IO, Woodside AG. Fuzzy-set Qualitative Comparative Analysis (fsQCA): guidelines for research practice in Information Systems and marketing. Int J Inf Manage. 2021;58:102310. doi:10.1016/j.ijinfomgt.2021.102310
31. Kourouthanassis PE, Mikalef P, Pappas IO, et al. Explaining travellers online information satisfaction: a complexity theory approach on information needs, barriers, sources and personal characteristics. Inf Manage. 2017;54(6):814–824. doi:10.1016/j.im.2017.03.004
32. Marsicano FP, Petroianu A. Impact of advanced prostatic cancer treatment on quality of life and sexual function. Braz J Oncol. 2023;19:e–20230438. doi:10.5935/2526-8732.20230438
33. Bowie J, Brunckhorst O, Stewart R, et al. Body image, self-esteem, and sense of masculinity in patients with prostate cancer: a qualitative meta-synthesis. J Cancer Survivorship. 2022;16(1):95–110. doi:10.1007/s11764-021-01007-9
34. Polku H, Mikkola TM, Portegijs E, et al. Life-space mobility and dimensions of depressive symptoms among community-dwelling older adults. Aging Mental Health. 2015;19(9):781–789. doi:10.1080/13607863.2014.977768
35. Fuchs T, Jaspers K. Psychopathology of depression and mania: symptoms, phenomena and syndromes. Off J Ital Soc Psychopathol. 2014;20:404–413.
36. Yusuf H, Subardhini M, Andari S, et al. Role of family and community support in the eliminating restraint of persons with mental illness. Int J Health Sci. 2022;6(2):987–1000. doi:10.53730/ijhs.v6n2.9697
37. Gurusinga R, Afrizal A, Bachtiar A, et al. Family support pattern for treatment adherence among tuberculosis patients in deli serdang regency: a qualitative study. Jurnal Ilmu Kesehatan Masyarakat. 2024;15(2):220–233. doi:10.26553/jikm.2024.15.2.220-233
38. Hird EJ, Slanina-Davies A, Lewis G, et al. From movement to motivation: a proposed framework to understand the antidepressant effect of exercise. Transl Psychiatry. 2024;14(1):273. doi:10.1038/s41398-024-02922-y
39. Liu JY. Ageing and familial support: a three-generation portrait from urban China. Ageing Soc. 2024;44(5):1204–1230. doi:10.1017/S0144686X22000861
40. Lo TW, Chan GH. Understanding the life experiences of elderly in social isolation from the social systems perspective: using Hong Kong as an illustrating example. Front Psychiatry. 2023;14:1114135. doi:10.3389/fpsyt.2023.1114135
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.