Back to Journals » Infection and Drug Resistance » Volume 15
How Does Helicobacter pylori Infection Cause Gastric Mucosal Atrophy
Authors Wang YK, Zhou JL, Meng NL, Zhu CY, Wang SN, Chen XD
Received 6 January 2022
Accepted for publication 5 May 2022
Published 7 July 2022 Volume 2022:15 Pages 3619—3629
DOI https://doi.org/10.2147/IDR.S355981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yang-Kun Wang,1 Jun-Ling Zhou,2 Nian-Long Meng,3 Chao-Ya Zhu,4 Su-Nan Wang,5 Xiao-Dong Chen1
1Department of Pathology, Foresea Life Insurance Guangzhou General Hospital, Guangzhou, 511300, People’s Republic of China; 2Shenzhen Nanshan District People’s Hospital, Shenzhen, 518067, People’s Republic of China; 3Department of Pathology, The 989th Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army, Luoyang, Henan, 471031, People’s Republic of China; 4Department of Pathology, Third Affiliated Hospital, Zhengzhou University, Zhengzhou, 450052, People’s Republic of China; 5Shenzhen Polytechnic, Shenzhen, 518055, People’s Republic of China
Correspondence: Su-Nan Wang, Shenzhen Polytechnic, Bank of Xili Lake, Xilihu Town, Nanshan District, Shenzhen City, 518055, People’s Republic of China, Tel/Fax +86-0755-26731494, Email [email protected] Xiao-Dong Chen, Department of Pathology, Foresea Life Insurance Guangzhou General Hospital, No. 703, New Town Avenue, Zengcheng District, Guangzhou, 511300, People’s Republic of China, Tel/Fax +86-020-32169999, Email [email protected]
Objective: To investigate the occurrence and development of gastric mucosal atrophy due to Helicobacter pylori (Hp) infection and the accompanying histomorphological features.
Methods: Detailed histological observations and immunohistochemical examinations were conducted via 197 endoscopic biopsies and endoscopic submucosal dissection specimens of gastric mucosal atrophic lesions with gastric Hp infection. Detailed observation was made of columnar cells in the proliferative region of the deep gastric pit and the isthmus of the gastric gland, as well as the upper part of the glandular cervix.
Results: The infection of the gastric mucosa by Hp firstly led to the proliferative disorder of stem cells in the normal proliferative region of the gastric mucosa. This caused substantial propagation of cells in the proliferative region of the deep gastric pit and the isthmus of the gastric gland, as well as the upper part of the glandular cervix, as a means to replenish the damaged surface mucus cells. However, the propagation of stem cells in the proliferative region was insufficient for downward migration, and the normal physiological process of differentiation into fundic/pyloric gland cells was disrupted, resulting in glandular atrophy of the intrinsic layer of the gastric mucosa. Persistent Hp infection and disruption of stem cell proliferation in the proliferative region subsequently resulted in extensive segmental hyperplasia of the gastric mucosa and glandular atrophy of the lamina propria.
Conclusion: The occurrence, development, and histomorphological features of gastric mucosal atrophy due to gastric Hp infection provide a reliable pathological basis for precise treatment by clinicians and are of great significance for controlling the development of gastric cancer.
Keywords: gastric tumor, Helicobacter pylori, mucosal atrophy, histopathology, immunohistochemistry
Introduction
Gastric cancer (GC) is one of the most common types of cancer worldwide, and gastric mucosal atrophy is clearly correlated with its occurrence.1,2 Many factors can cause gastric mucosa atrophy such as infection, long-term drug stimulation, as well as immune and genetic factors.1,3,4 In recent years, the incidence of Helicobacter pylori (Hp) infection, as well as its correlation with chronic atrophic gastritis, and intestinal epithelial metaplasia, has been investigated in the literature by pathological biopsies. Studies have also compared the prevalence of atrophy and intestinal epithelial metaplasia with the prevalence of GC in different countries, with the investigation of 1906 patients with Hp infection in seven countries reflecting the prevalence of GC in different geographical regions.5–7 Gastric Hp infection can lead to gastric mucosal atrophy and intestinal epithelial metaplasia, and studies have verified the correlation between the degree of gastric mucosal atrophy and the risk of carcinogenesis. With the progression of gastric mucosal atrophy, the number of gastric differentiated and undifferentiated cancers continues to increase.1–3,8
It was revealed in our previous study that gastric mucosal atrophy can be classified as simple, proliferative, intestinal metaplasia, and intraepithelial neoplastic atrophy.9 Helicobacter pylori infection can lead to a papillary proliferation of the surface epithelial cells.10 However, how Hp infection leads to gastric mucosa atrophy and the histological structural, as well as the cellular morphological changes that occur during its onset and development, have not been reported. This study aimed to investigate the occurrence and development of Hp infection and its histomorphological features, providing a reliable pathological basis for precise treatment by clinicians.
Materials and Methods
Materials
This study included 197 patient cases resected by gastroscopic biopsy and endoscopic submucosal dissection (ESD) with gastric mucosal atrophic lesions due to Hp infection. Patients were diagnosed by histopathological examination and were selected from July 2019 to July 2021 from Foresea Life Insurance Guangzhou General Hospital, Shenzhen Nanshan Hospital, No.989 Hospital of the PLA Joint Logistics Support Force, and the Third Affiliated Hospital of Zhengzhou University. There were 121 males and 76 females. Among the patients, 6 cases were pathologically diagnosed with extensive segmental hyperplasia of the gastric mucosa and atrophy of the lamina propria, accompanied by focal high-grade intraepithelial neoplasia. The six cases were all underwent ESD. The cancer sites were as follows: 48 cases in the gastric angle, 88 cases in the gastric antrum, 39 cases in the gastric body, and 22 cases in the gastric fundus. Between 3 and 5 sections of mucosal tissue were clamped from each site. The specimens were fixed in 10% neutral formalin, routinely dehydrated, paraffin-embedded, and sections with a thickness of 4 μm were prepared. Hematoxylin and eosin (H&E) and immunohistochemistry staining were conducted. The specific treatment of patients is shown in Table 1.
 |
Table 1 Specific Treatment Protocol for H. pylori Infection of the Gastric Mucosa |
Immunohistochemistry Staining
The EnVision two-step method was adopted, and the tissue sections were deparaffinized, hydrated, and rinsed with distilled water. The slices were then placed in tris-buffered saline (TBS) for 10 minutes. Endogenous peroxidase was blocked for another 5 minutes, and then the sections were treated with TBS for 10 minutes. Each primary antibody (MUC5AC, MUC6, villin, CDX2, p53, ki-67) was incubated with the sections for 30 minutes at room temperature, respectively. After washing in TBS for 10 minutes, the sections were incubated in En VisionTM. The sections were washed in TBS for 10 minutes and incubated with a secondary antibody for 10 minutes, respectively. The sections were incubated with a chromogenic substrate solution for 10 minutes, then rinsed with distilled water. Diaminobenzidine (DAB) was used to develop color and stained again with hematoxylin. The gastric mucosal sections with a definitive diagnosis were used as the positive controls, and a phosphate-buffered saline (PBS) buffer was adopted as a negative control instead of the primary antibody. The working solutions were purchased from Shenzhen Dartmon Biotechnology Co., Ltd., and the operational steps were carried out in strict accordance with the kit instructions.
Statistical Analysis
The SPSS Statistics 22.0 software package was adopted for statistical analysis. The chi-square test was employed for statistical analysis of gender and age; P < 0.05 was considered statistically significant.
Results
Clinical Characteristics
There were 121 males (61.6%) and 76 females (38.3%) with Hp infection. The time of Hp infection onset was ≤60 in 108 cases (54.8%) and >60 in 89 cases (45.2%), as shown in Table 2.
 |
Table 2 The Relationship Between the Age of Onset and Gender in the Occurrence and Development of Atrophic Lesions Due to Hp Infection in the Gastric Mucosa |
The Occurrence and Development of Gastric Mucosal Atrophy Due to Hp Infection
Initially, Hp colonized the mucus layer covered by gastric mucosal epithelium, then penetrated the mucus layer and specifically and selectively adhered to the surface mucus cytoplasm, and could also involve the proliferating cervical mucus cells. The infection of the gastric mucosa by Hp first led to the widespread disorder of stem cells in the normal proliferative region of the gastric mucosa. On the one hand, this caused massive propagation of cells in the proliferative region of the deep gastric pit and the isthmus of the gastric gland, as well as the upper part of the glandular cervix, aimed at replenishing the damaged surface mucus cells. However, the propagation of stem cells in the proliferative region was insufficient for downward migration, and the normal physiological process of differentiation into fundic/pyloric gland cells was disrupted, resulting in glandular atrophy of the intrinsic layer of the gastric mucosa. Persistent Hp infection and the disruption of stem cell proliferation in the proliferative region eventually resulted in extensive segmental hyperplasia of the gastric mucosa and glandular atrophy of the lamina propria (see Figure 1).
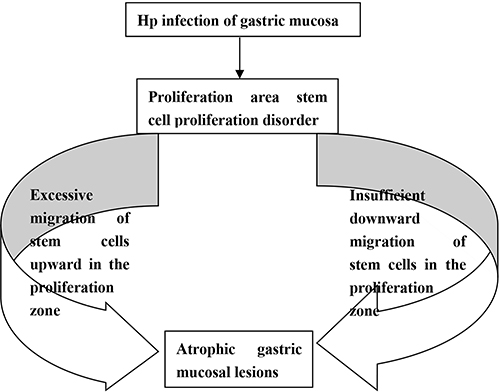 |
Figure 1 A flow chart: occurrence and development of mucosal atrophy caused by Hp infection in gastric mucosa. |
The Histomorphological Features of Gastric Mucosa Atrophy Due to Hp Infection
Helicobacter pylori selectively destroyed the cytoplasm of surface mucus cells, causing cytoplasmic swelling and vacuolar degeneration (Figure 2A). In the early stages of Hp infection, the lesions were mainly in the superficial layer of the gastric mucosa, and the cytoplasm of the Hp-infected surface epithelial cells was destroyed, with the remaining cytoplasm surrounding the nucleus in a radial structure (and the infiltration of numerous neutrophilic leukocytes and some lymphocytes in the interstitium) and forming the characteristic Hp-infected band visible under low magnification (Figure 2B). Large amounts of Hp adhered to the cytoplasm of the surface epithelial cells, leading to substantial cell proliferation and transformation in the deep region of the gastric pit and the isthmus of the gastric gland, as well as in the proliferative region of the upper part of the glandular cervix (Figure 2C). This subsequently led to disorder in stem cell propagation in the proliferating region and considerable Hp adhesion on the cytoplasm of the surface epithelium. The proliferating glands were mildly enlarged, with a poorly defined cytoplasm boundary, increased basophils, and diffused acute and chronic inflammation of the interstitium (Figure 3A). Cytologically, the cytoplasm was poorly defined, with increased basophils and an enlarged nucleus, one-to-two times the size of the normal nucleus, together with small nucleoli. The nuclei were elongated, mildly to moderately heterogeneous, with increased nuclear chromatin and small to medium-sized nucleoli visible in approximately 20% to 30% of the nuclei (Figure 3B). The persistent and massive proliferation of cells in the proliferating areas of the deep gastric pit, the isthmus of the gastric gland, and the upper part of the glandular cervix supplemented the damaged surface mucus cells, resulting in the formation of histologically characteristic papilloma-like structures (Figure 4A). The nuclei of the proliferated cells were enlarged and elongated, one-to-two times the size of the normal nuclei, with mild to moderate heterogeneity (Figure 4B). The normal physiological differentiation process of the stem cells in the proliferative region into fundic/pyloric gland cells, as well as downward migration, was disrupted due to the significant disruption in the proliferative region, resulting in glandular atrophy in the lamina propria of the gastric mucosa. Histomorphologically, the glands of the lamina propria were significantly smaller and reduced (Figure 5A). The intrinsic lamina glands decreased or vanished with hyperplasia of fibrous connective and smooth muscle tissue, as well as hyperplasia of lymphoid tissue (Figure 5B). Persistent Hp adhesion and the persistent propagation disorder of the proliferative regions/proliferative bands of the gastric mucosa led to the formation of widespread segmental papillary hyperplasia and atrophy of the lamina propria glands. The proliferation of epithelial cells on the surface of the gastric mucosa and the atrophy of the lamina propria glands alternated in a relatively regular high/low-level pattern, similar to the undulating waves of an ocean (Figure 6A). Mild to moderate heterogeneity remained in the areas of extensive segmental hyperplasia (Figure 6B). In the region with extensive segmental lamina propria gland atrophy, the fundic glands were almost completely absent (Figure 6C). In severe regions, there existed only a thin layer of surface mucus cells (Figure 6D) as shown in Figure 7.
 |
Figure 2 Degeneration of the surface epithelial cells on the gastric mucosa in the presence of Hp infection. (A) Massive adherence of Hp on the mucus layer and surface epithelial cells covered by the gastric mucosal surface epithelium; H&E staining, × 400. (B) A characteristic Hp infection band was visible on the routine pathological section under low magnification; H&E staining, ×10. (C) Cobweb-like vacuolar degeneration of the cytoplasm of the surface epithelial cells. With different degrees of cytoplasmic destruction and detachment, a small amount of cytoplasm remained around the nucleus in a radial structure; finally, the nucleus also degenerated and detached; H&E staining, ×400. (D) Positive for Hp, EnVision method, ×400. |
 |
Figure 3 Proliferative disorder of the stem cells in the proliferative region. (A) The hyperplastic glands were mildly enlarged, with poorly defined cytoplasm, increased basophilia, and diffused acute and chronic inflammation of the interstitium; H&E staining, ×100. (B) The nuclei were elongated, mildly to moderately heterogeneous, with increased nuclear chromatin and small-to-medium-sized nucleoli in approximately 20% to 30% of the nuclei; H&E staining, ×200. (C) Positive for Hp, EnVision method, ×100. (D) Formation of the tubular and branched structures by significant cell proliferation in the deep gastric pit and isthmus of the gastric glands, as well as in the proliferating areas of the upper part of the glandular cervix. The proliferating glands were surface epithelial cells with the positive expression of MUC5AC; EnVision method, ×200. |
 |
Figure 4 Excessive upward migration of the stem cells in the proliferative region. (A) Massive propagation of cells in the proliferating region resulted in the formation of a histologically characteristic papilloma-like structure; H&E staining, ×100. (B) Enlarged nuclei, one-to-two times the size of the nuclei in the normal surface epithelial cells, with mild to moderate heterotypy; H&E staining, ×400. (C) Positive for MUC5AC, EnVision method, ×200. (D) Positive for CDX2, EnVision method, ×100. |
 |
Figure 5 Insufficient downward migration of the stem cells in the proliferative region. (A) Proliferative disorder of the proliferative region, reduction in the number and size of glands in the lamina propria; H&E staining, ×200. (B) Almost complete disappearance of the glands in areas with severe atrophy, with only a thin layer of surface mucus cells, hyperplasia of the fibrous connective and smooth muscle tissue, and hyperplasia of lymphoid tissue; H&E staining, ×100. (C) Positive for MUC6, EnVision method, ×200. (D) Positive for p53, EnVision method, ×200. |
 |
Figure 6 Formation of the characteristic wave-like shape due to extensive atrophy of the intrinsic laminar glands. (A) The widespread segmental papillary hyperplasia and atrophy of the gastric mucosa manifested as relatively regular alternating highs and lows, similar to the undulating waves of an ocean; accordingly, this was labeled the characteristic wave-like shape of Hp infection; H&E staining, ×100. (B) Widespread segmental hyperplasia areas retaining mild to moderate heterogeneity; H&E staining, ×200. (C) Areas of extensive segmental atrophy showing the almost complete disappearance of the fundic glands and only a thin layer of surface mucus cells; H&E staining, ×200. (D) Severe areas with only a thin layer of surface mucus cells; H&E staining, ×200. |
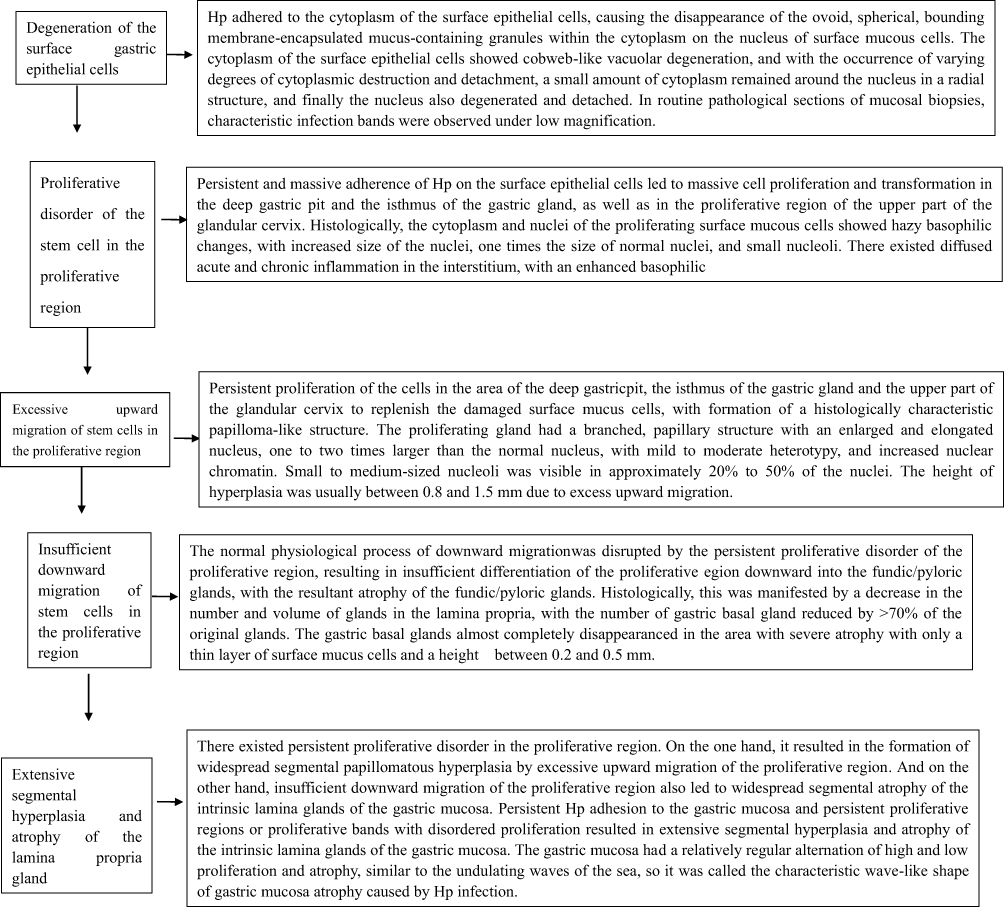 |
Figure 7 Onset and development of atrophic lesions due to Hp infection in the gastric mucosa and the characteristic histomorphological immunophenotypes. |
The Results of Immunohistochemistry Staining
Degeneration of the mucus cells was present in the gastric mucosal surface, mainly with reduced positive expression of MUC5AC and MUC6. Varying degrees of the positive expression of CEA and HER2 manifested, and the presence of Hp was strongly positive (Figure 2D). In the proliferating region, disturbed stem cell proliferation was observed, together with the proliferation of surface epithelial cells and diffused inflammation of the mesenchyme, as well as strong Hp positivity (Figure 3C) and the positive expression of MUC5AC (Figure 3D). The stem cells in the proliferation region migrated upward excessively, and the proliferation of surface epithelial cells showed the positive expression of MUC5AC (Figure 4C) and the decreased positive expression of MUC6. Different degrees of positive expression of CDX2 (Figure 4D), villin, and p53 were observed. The stem cells in the proliferation region failed to migrate downward sufficiently, with decreased positive expression of MUC6 (Figure 5C) and varying degrees of positive expression of CDX2, villin, and p53 (Figure 5D) as illustrated in Table 3.
 |
Table 3 Results of Immunohistochemical Staining of Atrophic Lesions of the Gastric Mucosa |
Discussion
Histologically, three-to-five glands are connected to the base of each gastric pit, which is the basic structural unit of the gastric mucosa. These are called gastric units, and they have a structure that is of monoclonal origin.11 The gastric unit comprises the gastric pit and gastric glands and can be divided, in order, into the isthmus, the glandular cervix, and the fundus. The deeper part of the gastric pit, the upper part of the isthmus, and the cervix of the gastric gland are called the proliferative region, or the proliferative zone. From the top of the fundus gland to the deep part of the gastric pit, the cells are small in low columnar shapes, which primarily comprise proliferating stem cells. Some cells migrate upward and differentiate into surface mucous cells; some remain local or migrate downward and differentiate into other fundic gland cells.12–15
The present study found that the occurrence of gastric mucosal atrophy due to Hp infection was mainly caused by the failure of stem cells in the proliferative region of the gastric mucosa to differentiate and migrate normally. Additionally, based on the results of this study, the formation process of gastric mucosal atrophy is proposed as follows via the observation of 197 cases with atrophic gastric mucosal lesions. First, atrophy was caused by proliferative disorders in the proliferative zone/region. On the one hand, there was an excessive upward migration of the increasing stem cells in the proliferative region. The persistent proliferation of cells in the area of the deep gastric pit, the isthmus of the gastric gland, and the upper part of the glandular cervix could replenish the damaged surface mucus cells, resulting in the formation of histologically characteristic papilloma-like structures. Histomorphologically, the hyperplastic glands had a branched, papillary structure with enlarged and elongated nuclei, one-to-two times the size of the normal nuclei, with mild to moderate heterogeneity, increased nuclear chromatin, and small-to-medium-sized nucleoli visible in approximately 20% to 50% of the nuclei. On the other hand, the downward migration of multiplying stem cells in the proliferative zone was inadequate. The normal physiological process of downward migration was interrupted by the persistent disruption of the proliferative band in the proliferative region, resulting in insufficient downward differentiation of the proliferative region into the fundic/pyloric glands, leading to atrophy of these glands. Histomorphologically, atrophy manifested as a decrease in the number and size of glands in the lamina propria, with almost complete disappearance of these glands in areas with severe atrophy and only a thin layer of surface mucus cells. There was a persistent disturbance in the proliferative region, and excessive upward migration of the proliferative region resulted in extensive segmental papillomatous hyperplasia. The insufficient downward migration of the proliferative region also resulted in extensive segmental atrophy of the glands in the lamina propria of the gastric mucosa. This will result in an atrophic lesion of the gastric mucosa with the formation of alternating high and low waves resembling the undulating waves of an ocean; accordingly, this was labeled the characteristic wave-like shape of gastric mucosal atrophy caused by Hp infection. Change of immunohistochemical of biomarkers was investigated. In the degeneration stage of gastric mucosal surface mucus cells, the positive expression of MUC5AC and MUC6 decreased. CEA and HER2 were positively expressed in different degrees and Hp was strongly positive. When excessive upward migration of stem cells in the proliferative region happened, proliferation of surface epithelial cells led to increased expression of MUC5A, decreased expression of MUC6, with different levels of positive expression of CDX2, villin, and p53. In the stage of insufficient downward migration of stem cells in the proliferative region, positive expression of MUC6 decreased, while positive expression of CDX2, villin, p53, and ki67 increased. In the present study, the occurrence and development of gastric mucosal atrophic lesions caused by Hp infection in the gastric mucosa, as well as the histomorphological features and immunophenotype involved were proposed. This provides new information for investigating gastric mucosal atrophy.
Helicobacter pylori represent the most common type of bacteria worldwide and represent a flagellar pathogen. It is a unipolar, multiflagella, Gram-negative bacterium with blunt ends and spirally curved ends. Its length is 2.5–4.0 μm and it has a width of 0.5–41.0μm. Helicobacter pylori have a high level of genetic diversity for adapting to the nature of the host’s gastric juices and undergoes spherical deformation in unsuitable environments or after drug therapy. Spherical Hp has a complete membrane-like structure with flagella, which is viable and can lead to repeated infections.16,17 Helicobacter pylori is a spiral, flagella-like, microaerobic Gram-negative bacteria. Infection with the bacteria can easily be identified in HE-stained sections. The bacteria have been reported to colonize the gastric mucosa, and reports also indicate that Hp colonizes the gastric and duodenal mucosa in humans.5,18–20 The present study found that Hp initially colonized the mucus layer covered by the gastric mucosal epithelium, then penetrated the mucus layer, and specifically adhered to the cytoplasm of the surface mucus cells before destroying them, causing cobweb-like vacuolar degeneration of the cytoplasm. With varying degrees of cytoplasmic destruction and detachment, a small amount of cytoplasm remained surrounding the nucleus in a radial structure; finally, the nucleus also degenerated and detached. In the routine pathological sections of mucosal biopsies, characteristic Hp infection bands were observed under low magnification, suggesting that the appearance of these bands may reflect early lesions of Hp infection. These early lesions, when found in gastric mucosal biopsies by pathologists during clinical practice, should be included in the clinical pathology test report, which can help guide clinicians to provide early treatment, control, or even eradicate Hp infection and prevent its further development to the stage of becoming a stem cell disorder in the proliferative region. This will, in turn, serve as an important step for controlling the occurrence and development of atrophic lesions of the gastric mucosa.
Helicobacter pylori reflect unique toxic factors that allow it to colonize the cytoplasm of epithelial cells on the surface of the gastric mucosa, including urease, helix shapes, flagella, and adhesion molecules.21–23 Persistent Hp infection has been fully verified as a risk factor for gastric mucosal atrophy and GC.24,25 Although the eradication of Hp infection has been shown to reduce the incidence of GC, it was suggested that the history of Hp infection after eradication, or a history of having had a Hp infection, remains a risk factor for developing GC.26,27 It was also suggested that patients who developed GC after treatment for an Hp infection had a history of precancerous lesions prior to Hp infection.28
The present study showed that persistent Hp infection led to irreversible changes in the proliferative region with disordered propagation, excess upward migration, or the insufficient downward migration of stem cells with lesion progression in the proliferative region, and extensive segmental atrophy of the lamina propria glands of the gastric mucosa. This study concluded that gastric mucosal atrophy caused by Hp infection may be an irreversible injury, and the occurrence of GC could still be caused by the atrophic lesions of the gastric mucosa, even after Hp eradication. The mechanism of gastric mucosa atrophy caused by Hp infection need further clinical studies enrolling more cases or with more follow-up data and further basic research of molecular biology.
Conclusion
This study proposed how Hp infection caused gastric mucosal atrophy especially the histopathological features of the occurrence and development of gastric atrophy. In addition, it revealed that failure to control or eradicate Hp infection in time would lead to irreversible gastric mucosal atrophy.
Abbreviations
HP, helicobacter pylori; GC, gastric cancer; ESD, endoscopic submucosal dissection; H&E, Hematoxylin and eosin; TBS, tris-buffered saline; DAB, diaminobenzidine; PBS, phosphate-buffered saline.
Ethical Statement
This study was conducted with approval from the Ethics Committee of Foresea Life Insurance Guangzhou General Hospital, Ethics Committee of Shenzhen Nanshan Hospital, Ethics Committee of No.989 Hospital of the PLA Joint Logistics Support Force, and Ethics Committee of the Third Affiliated Hospital of Zhengzhou University. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
Supported by the Key Scientific and Technological Research Project of Henan Province, No. 132102310008.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Akbari M, Tabrizi R, Kardeh S, Lankarani KB. Gastric cancer in patients with gastric atrophy and intestinal metaplasia: a systematic review and meta-analysis. PLoS One. 2019;14(7):e0219865. doi:10.1371/journal.pone.0219865
2. Song JH, Kim SG, Jin EH, Lim JH, Yang SY. Risk factors for gastric tumorigenesis in underlying gastric mucosal atrophy. Gut Liver. 2017;11(5):612–619. doi:10.5009/gnl16488
3. Masuyama H, Yoshitake N, Sasai T, et al. Relationship between the degree of endoscopic atrophy of the gastric mucosa and carcinogenic risk. Digestion. 2015;91(1):30–36. doi:10.1159/000368807
4. Kim HJ, Kim N, Yun CY, Lee HS. The clinical meaning of the “indefinite for atrophy” lesions within gastric mucosa biopsy specimens in a region with a high prevalence of gastric cancer. Helicobacter. 2019;24(5):e12605. doi:10.1111/hel.12605
5. Quach DT, Vilaichone RK, Vu KV, Yamaoka Y, Sugano K, Mahachai V. Helicobacter pylori infection and related gastrointestinal diseases in Southeast Asian Countries: an expert opinion survey. Asian Pac J Cancer Prev. 2018;19(12):3565–3569. doi:10.31557/APJCP.2018.19.12.3565
6. El-Zimaity HM, Graham DY. Evaluation of gastric mucosal biopsy site and number for identification of Helicobacter pylori or intestinal metaplasia: role of the Sydney system. Hum Pathol. 1999;30(1):72–77. doi:10.1016/S0046-8177(99)90303-9
7. Udoh MO, Obaseki DE. Histopathological evaluation of H. pylori associated gastric lesions in Benin City, Nigeria. East Afr Med J. 2012;89(12):408–413.
8. Khatoon J, Prasad KN, Prakash Rai R, Ghoshal UC, Krishnani N. Association of heterogenicity of Helicobacter pylori cag pathogenicity island with peptic ulcer diseases and gastric cancer. Br J Biomed Sci. 2017;74(3):121–126. doi:10.1080/09674845.2017.1278887
9. Wang Y-K, Shen L, Yun T, Yang B-F, Zhu C-Y, Wang S-N. Histopathological classification and follow-up analysis of chronic atrophic gastritis.World. J Clin Cases. 2021;9(16):3838–3847. doi:10.12998/wjcc.v9.i16.3838
10. Wang Y, Shen L, Zhao G, et al. Histomorphological characteristics and pathological types of hyperproliferation of gastric surface epithelial cells. Gastroenterol Res Pract. 2021;2021:8828326. doi:10.1155/2021/8828326
11. Russi S, Calice G, Ruggieri V, et al. Gastric normal adjacent mucosa versus healthy and cancer tissues: distinctive transcriptomic profiles and biological features. Cancers. 2019;11(9):1248. doi:10.3390/cancers11091248
12. Matysiak-Budnik T, Camargo MC, Piazuelo MB, Leja M. Recent guidelines on the management of patients with gastric atrophy: common points and controversies. Dig Dis Sci. 2020;65(7):1899–1903. doi:10.1007/s10620-020-06272-9
13. Souza SM, Valiente AEF, Sá KM, et al. Immunoexpression of LGR4 and beta-catenin in gastric cancer and normal gastric mucosa. Asian Pac J Cancer Prev. 2019;20(2):519–527. doi:10.31557/APJCP.2019.20.2.519
14. Tarnawski AS, Ahluwalia A. Increased susceptibility of aging gastric mucosa to injury and delayed healing: clinical implications. World J Gastroenterol. 2018;24(42):4721–4727. doi:10.3748/wjg.v24.i42.4721
15. Heidari Z, Mahmoudzadeh-Sagheb H, Narouei M. Quantitative changes of gastric mucosa during carcinogenesis using stereological methods. J BUON. 2017;22(4):905–910.
16. Gu H. Role of flagella in the pathogenesis of Helicobacter pylori. Curr Microbiol. 2017;74(7):863–869. doi:10.1007/s00284-017-1256-4
17. Koido S, Odahara S, Mitsunaga M, et al. Diagnosis of Helicobacter pylori infection: comparison with gold standard. Rinsho Byori. 2008;56(11):1007–1013.
18. Sgambato D, Miranda A, Romano L, Romano M. Gut microbiota and gastric disease. Minerva Gastroenterol Dietol. 2017;63(4):345–354. doi:10.23736/S1121-421X.17.02380-7
19. Malfertheiner P, Megraud F, O’Morain CA, et al. European Helicobacter and microbiota study group and consensus panel. Management of Helicobacter pylori infection-The Maastricht V/Florence consensus report. Gut. 2017;66(1):6–30. doi:10.1136/gutjnl-2016-312288
20. Sabbagh P, Mohammadnia-Afrouzi M, Javanian M, et al. Diagnostic methods for Helicobacter pylori infection: ideals, options, and limitations. Eur J Clin Microbiol Infect Dis. 2019;38(1):55–66. doi:10.1007/s10096-018-3414-4
21. Roesler BM, Rabelo-Gonçalves EM, Zeitune JM. Virulence factors of Helicobacter pylori: a review. Clin Med Insights Gastroenterol. 2014;27(7):9–17.
22. Allen LA. Phagocytosis and persistence of Helicobacter pylori. Cell Microbiol. 2007;9(4):817–828. doi:10.1111/j.1462-5822.2007.00906.x
23. Šterbenc A, Jarc E, Poljak M, Homan M. Helicobacter pylori virulence genes. World J Gastroenterol. 2019;25(33):4870–4884. doi:10.3748/wjg.v25.i33.4870
24. Kao CY, Sheu BS, Wu JJ. Helicobacter pylori infection: an overview of bacterial virulence factors and pathogenesis. Biomed J. 2016;39(1):14–23. doi:10.1016/j.bj.2015.06.002
25. Toyoshima O, Yamaji Y, Yoshida S, et al. Endoscopic gastric atrophy is strongly associated with gastric cancer development after Helicobacter pylori eradication. Surg Endosc. 2017;31(5):2140–2148. doi:10.1007/s00464-016-5211-4
26. Kodama M, Murakami K, Okimoto T, et al. Histological characteristics of gastric mucosa prior to Helicobacter pylori eradication may predict gastric cancer. Scand J Gastroenterol. 2013;48(11):1249–1256. doi:10.3109/00365521.2013.838994
27. Lee YC, Chiang TH, Chou CK, et al. Association between Helicobacter pylori eradication and gastric cancer incidence: a systematic review and meta-analysis. Gastroenterology. 2016;150(5):1113–1124.e5. doi:10.1053/j.gastro.2016.01.028
28. Watari J, Chen N, Amenta PS, et al. Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World J Gastroenterol. 2014;20(18):5461–5473. doi:10.3748/wjg.v20.i18.5461
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.