Back to Journals » Advances in Medical Education and Practice » Volume 13
How Do Clinical Supervisors and Managers in Swedish Primary Care Perceive Their Opportunities to Meet the Learning Needs of Medical Students?
Authors Milos Nymberg V ![]() , Jakobsson U
, Jakobsson U
Received 5 November 2021
Accepted for publication 12 March 2022
Published 17 May 2022 Volume 2022:13 Pages 521—533
DOI https://doi.org/10.2147/AMEP.S348012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Veronica Milos Nymberg, Ulf Jakobsson
Department of Clinical Sciences, Lund University, Malmö, Sweden
Correspondence: Veronica Milos Nymberg, Department of Clinical Sciences, Lund University, Building 28, Floor 11, Jan Waldenströms Street 35, 205 02, Malmö, Sweden, Tel +46-767700240, Email [email protected]
Introduction: Primary health care centers (PHCCs) in Sweden are struggling to maintain a balance between increasing demands of service and supervision and learning activities for a growing number of students. We sought a deeper understanding of primary care physicians and managers behavioral intention towards supervising, and their perceptions of the structural preconditions and support needed.
Methods: The study combines two theoretical approaches, the Theory of Planned Behavior (TPB) and Social Practice Theory. A questionnaire with 22 items including an open-ended question was designed to collect quantitative and qualitative data and sent to clinical supervisors and managers at PHCCs in Southern Sweden. The aim was to map a) participants’ behavioral intention and perceived capacity to act to improve supervision and b) their perceptions of structural prerequisites and support needed to sustain and develop clinical supervision practice.
Results: A total of 181 questionnaires were returned, with a total response rate of 60.7%. Behavior predictors (attitudes, subjective norms, and perceived behavioral control) were positively correlated to behavioral intention towards supervising and building supervising competence. Three themes emerged from the content analysis of the qualitative data: ”Time and distribution”, ”Improved communication and support systems” and ”Elimination of structural barriers.”.
Discussion: The manager and supervisor reports suggest that the intentions and capacity of individuals (individuals’ agency) is not a strong barrier to high-quality supervising and teaching in PHCC. Organizational preconditions for sustaining and developing supervision practice exist, and structural barriers for exercising agency could be eliminated according to PHCC managers and supervisors. However, a conclusion of our study from a practice theory perspective is that how and to what degree primary care physicians engage in supervision and competence building is determined by how the workplace – and the medical school – afford participation in supervision-related workplace activities. Improved communication between medical school, managers and supervising physicians and on-site faculty development integrated in daily clinical work were described as important facilitators of a favorable supervision and learning environment.
Keywords: supervision competence, primary care, behavior predictors, questionnaire
Background
A global priority for society and health systems today is the necessary scale-up of Primary Health Care (PHC) and the growth of the PHC workforce including the supply of primary care physicians.1–3 Medical schools can contribute to ensure the ongoing education of the primary care workforce by stimulating medical students’ interest in PHC as a career choice.4 Some evidence suggests that students’ later choices of career and work location are influenced by the quality of the learning environment in the clinical rotations they experience in medical school.5,6 Also, there is evidence suggesting that medical students regard family medicine as a career of low interest and prestige.7–9 Consequently, efforts to improve the supervising and teaching of medical students in primary care placements is of not only educational interest but also a major public policy concern since it may increase the likelihood of young physicians choosing primary care careers.
While the preconditions for optimizing clinical learning environments largely vary and students’ learning needs may fluctuate across years of clinical training, the medical education literature suggests that a favorable clinical learning environment, among other things, include opportunities of active, experience-based learning; inclusion in workplace teams; autonomy support; opportunities to be observed during patient meetings; recurrent personalized feedback; teaching models for developing clinical reasoning skills; physical space and relevant resources for participation in work activities.2,10–13 Due to its constant rapid flow of patients needing to be managed, often independently, and with a high variety of complaints, primary care is potentially an excellent environment for practicing clinical skills under supervision and for experienced-based learning, and for developing clinical reasoning in the later stages of medical education.14 Students perceive the interaction with primary care physicians as having a crucial impact on their learning outcomes, particularly for developing communication skills and rapport with patients.15
Moreover, students report of improved broad clinical diagnostic reasoning skills through regular GP-facilitated teaching at various stages of student education.16 In a recent Swedish study, medical students found the relationship with the individual primary care physician supervisor as the central determinant for the outcome and meaningfulness of a placement in PHC.17
However, in Sweden, which is the setting of the present study, primary health care centers (PHCCs) are struggling to maintain a balance between increasing demands of service and supervision and learning activities for a growing number of students. As in many other countries, engaging PHCCs and primary care physicians in the clinical education of medical students is problematic in an already overburdened primary care.18 Moving services from hospital care towards outpatient care and primary care facilities have further affected the conditions for undergraduate education in primary care.19 Barriers to clinical training of medical students in primary care such as heavy workload, limited time and resources, financial constraints, lack of confidence in supervising, lack of feedback on supervision and lack of support from medical school and faculty are consistent with findings in earlier research, dating from the 90ʹs.20–22 Increasingly stressful working conditions for primary healthcare staff and little time for supervising is no surprise considering the ongoing substantial structural changes in the healthcare delivery system. Moreover, many primary care physicians feel isolated and do not identify as members of the medical school teaching community which influences commitment and confidence21. Other recent studies suggest that primary care clinical supervisors wish for supervision guidance and a variety of options for developing as clinical teachers and supervisors.20,23
A reason for initiating this study was the authors’ involvement in recruiting and supporting PHC for student clinical training. Despite long-term affiliation agreements between medical education programs and primary care, recruiting PHCCs willing to receive students has been difficult. Although previous research have identified barriers for offering medical students training we found a paucity of studies exploring perceptions of barriers related to both to the agency of individual supervisors’ or managers’ (the capacity of individuals to act and exercise power to make a difference) and environmental (structural and sociocultural) preconditions for the development of supervising practices in primary care.24 While there is a body of research exploring the perceptions of clinical teachers and supervisors in primary care, studies of the attitudes and perceptions of managers related to student training in primary care are scarce. In Sweden, PHCC managers’ primary role is an administrative, managerial role. Being in control of the scheduling and planning of supervision, PHCC managers highly influence students’ access to patient encounters and supervision. Managers are also in control of how the information from the medical school is disseminated and communicated among the physician staff. An understanding of primary care physicians and managers behavioral intentions, how they think of their capacity to act, and how contextual conditions might support, or limit actions is necessary to address the needs of PHC centers effectively and provide meaningful support from medical school and relevant forms of faculty development activities.
Aim and Theoretical Approach
The overarching aim of the present study was to map, on the one hand, PHC physicians’ and managers’ behavioral intentions related to teaching and clinical supervising of medical students and on the other hand, their perceptions of structural preconditions and support needed to sustain and develop clinical supervision practice.
The theoretical grounding of the present study is a combination of the Theory of Planned Behavior25 and the Social Practice Theory of Billet.24 Behavioral intention has been studied in sociopsychological and medical research through the lens of cognitive behavioral theories.25–27 According to the Theory of Planned Behavior (TPB),25 individual’s behavioral intention in a certain situation can predict behavior. Although there is not a perfect correlation between behavioral intention and actual behavior, intention might be used as a proximal measure for behavior. Behavioral intention in turn can be predicted by individual’s attitudes, social norms, and perceived behavioral control.
Attitude toward a behavior has two components: beliefs about the consequences of the behavior and the corresponding positive or negative judgements about the behavior. Subjective norms are individuals’ own estimate of the social pressure to perform or not perform a behavior. Perceived behavioral control is the extent to which the individual feels able to perform a behavior, both in terms of self-efficacy and control beliefs about the power to influence situational or internal factors to inhibit or facilitate a behavior.28 TPB is therefore a useful model to describe, predict, and even alter behaviors. For instance, TPB-based questionnaires have been used to assess, predict, and influence primary care physician’s behavior in prescribing situations,29 their intention to use electronic learning tools30 or to assess residents’ intention to adopt a comprehensive scope of practice upon graduation.31
The insights of Practice Theory have offered perspectives on professional and workplace learning that take into consideration the reciprocal relationship between individual supervisors’ agency and environmental influences on student learning and supervision practices.24,32 Billet suggested that the workplaces’ invitational quality, ie the degree to which individuals are welcome or “invited” to participate in work is central to how learners experience the quality of a workplace learning environment.24 He stated that the learners who were afforded the richest opportunities for participation in combination with direct or indirect guidance reported the strongest development. At the same time, Billet stresses the capacity of individuals to exercise agency, and that the individual’s intentionality, agency, and interests influence the quality of learning. Guided participation alone cannot not guarantee that students learn. In the same way, an individual physician elects the level of engagement in the opportunities offered by the workplace to supervise and to build supervision competencies and supervision workplace social practices.24 As individual and contextual factors influencing the learning environment are intertwined, workplace conditions might affect the connection between attitudes, intention, and behavior. We present the theoretical framework of the study in Figure 1.
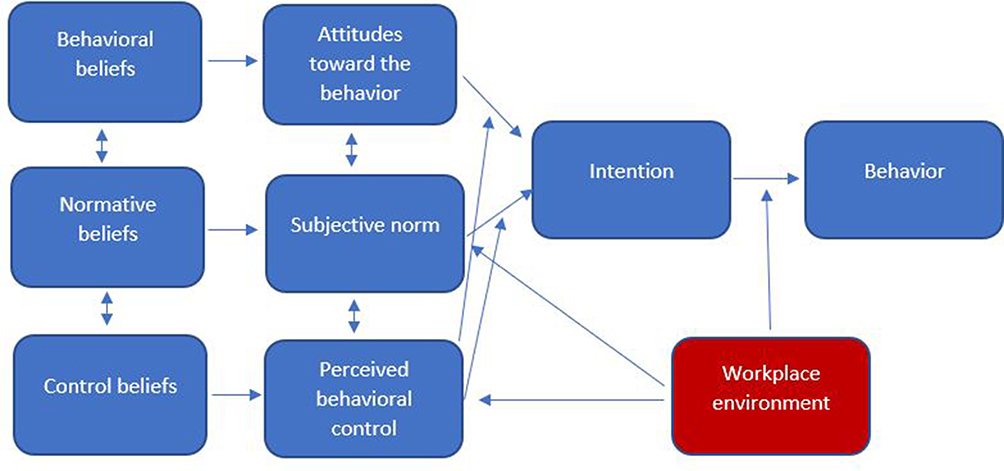 |
Figure 1 The theoretical framework of the study. Notes: Based on data from the theory of planned behavior by Ajzen25 and the social practice theory by Billet and Newton, 2010.24 |
Therefore, we wished to combine in this study the cognitive behavioral theory approach, analyzing intention and perceived capacity to act to improve supervision, with analysis of perceptions of environmental, mainly structural prerequisites for improving clinical supervision.
Method
A questionnaire was designed to collect quantitative data and open text comments. The 22 items questionnaire was based on a) TPB25 and b) Practice theory32 with a 5-point Likert scale ranging from ”fully disagree” to ”fully agree”. The middle position was labeled neutral.
A manual for health care services with instructions for constructing questionnaires based on the TPB was applied.28 Items were constructed by the first author using the manual, with the aim to target a) predictors of PHC physicians’ behavior related to supervising and the development of clinical (supervision) skills33 and b) structural prerequisites for clinical supervision.34 An open-ended question was included to collect free text answers describing support and resources needed to sustain and develop clinical supervision practice (”Give examples of support/resources you need to improve the clinical supervision and learning environment of medical students at the primary care center”).
Items that mapped out attitudes, social norms, or perceived behavioral control towards supervising medical students and towards developing clinical supervision competence were created. Every item resulted in a score on the Likert scale. The items targeting different theoretical constructs are shown in Table 1.
 |
Table 1 Focus Area, Items and Target Constructs Derived from the Theory of Planned Behavior and Practice Theory |
The items were pilot tested by the first author among primary care physicians (n = 14) from PHCCs involved in clinical teaching who discussed face validity and relevance of items and wordings. The feedback from the pilot group lead to final changes in wordings. The comments of the expert group lead to minor changes in the questionnaire.
Context
The setting of the study was Swedish PHCs in three regions in Southern Sweden where physicians and other staff are involved in the supervision and teaching of medical students at the university medical program. The students have limited interaction with primary care physicians and staff in year one, followed by short encounters with primary care during year three to five and a longer primary care placement of four weeks in their final semester.
Participants and Data Collection
E-mail invitations together with an information letter were sent to the same managers and the clinical supervisors who regularly received information from the medical program at the local university and with previous experience of training medical students. The faculty have access to e-mail addresses for one manager and/or one clinical supervisor responsible for student teaching at each PHCC. A total number of 298 primary care physicians and managers at 159 PHC centers from the contact list received an e-mail in which they were invited to participate in the study, with a link to the web-based survey. The participants were selected based on their role as managers or clinical supervisors at PHC centers which regularly received students from the local university. The main investigator informed primary care physicians about the survey at local conferences during the same period.
The survey was designed in REDCap,13 a secure web application used for building and managing online surveys. All responses were anonymous. The participants could submit the survey without fully completing the survey. It was not technically possible to do consistency or completeness checks before the questionnaire was submitted. Participants were able to review and change the answers with a ”back” button.
The survey ran from 8th May to 4th June 2020. Three consecutive reminders spaced each by one week were sent by e-mail during the data collection.
Data Analysis
Quantitative Data
All statistical analyses were performed using IBM SPSS statistics version 26 (IBM). Internal consistency of items was tested using Cronbach’s α coefficient. Acceptable alpha values range from 0.70 to 0.95.35
For each of the primary outcome variables (attitudes, subjective norms, perceived behavioral control, and behavioral intention) the mean of the item scores were calculated to give an overall score. Missing values were replaced with the mean value for the item (imputation). As the variables were not normally distributed, group comparison analyses were performed with Mann–Whitney’s test. Spearman’s rank order correlation was used to study associations between the different items.
Open-Text Comments
Inductive content analysis of the open-text answers was performed,36 transforming statements into themes and categories and illustrating the variety of thinking related to the open-ended question. Two researchers (VMN and PS) independently carried out initial condensation and pattern coding. The participants’ own words and expressions were used in the first phase of organizing and reorganizing the material. VMN and PS compared and revised the tentative pattern coding, constructed categories and themes, and then discussed and revised the analysis patterns until they reached consensus.
Ethical Considerations
The Swedish Ethical Review Authority reviewed the study plan/protocol (D no 2020–00429) and concluded that ethical approval and participant written consent was not necessary according to the Swedish Ethical Review Act (SFS 2003:460).
Results
A total number of 181 questionnaires were returned from 159 managers at PHCCs and 139 clinical supervisors resulting in a total response rate of 60.7%. The characteristics of the participants are summarized in Table 2. Cronbach’s α varied between 0.765 and 0.814, showing good reliability for all items.
 |
Table 2 Characteristics of the Respondents |
Response Rate, Correlations, and Distribution of Scores
The response rate for each item was 95–100% with a total of 23 missing answers. One item (” I am sufficiently competent to supervise students at the primary care center”) had a response rate of 95% with 10 missing answers. All questionnaire items and their corresponding Likert ranks are presented in Table 3. A large majority (85%) of the participants stated that they had attended a course to enhance their supervision skills. Most of the participants (93% of the managers and 94% of the supervisors) agreed or strongly agreed with the question: ”At our primary care center, we set aside time to supervise medical students”. A sub-group analysis of participants that answered with strongly disagree, disagree or neutral showed a distribution of 9 women and 3 men, 9 working at public health care centers and 3 at private PHCCs, 5 tutors and 4 managers. A majority of the participants strongly agreed (64%) or agreed (32%) with the statement: ”I have sufficient competence to supervise medical students” (self-efficacy).
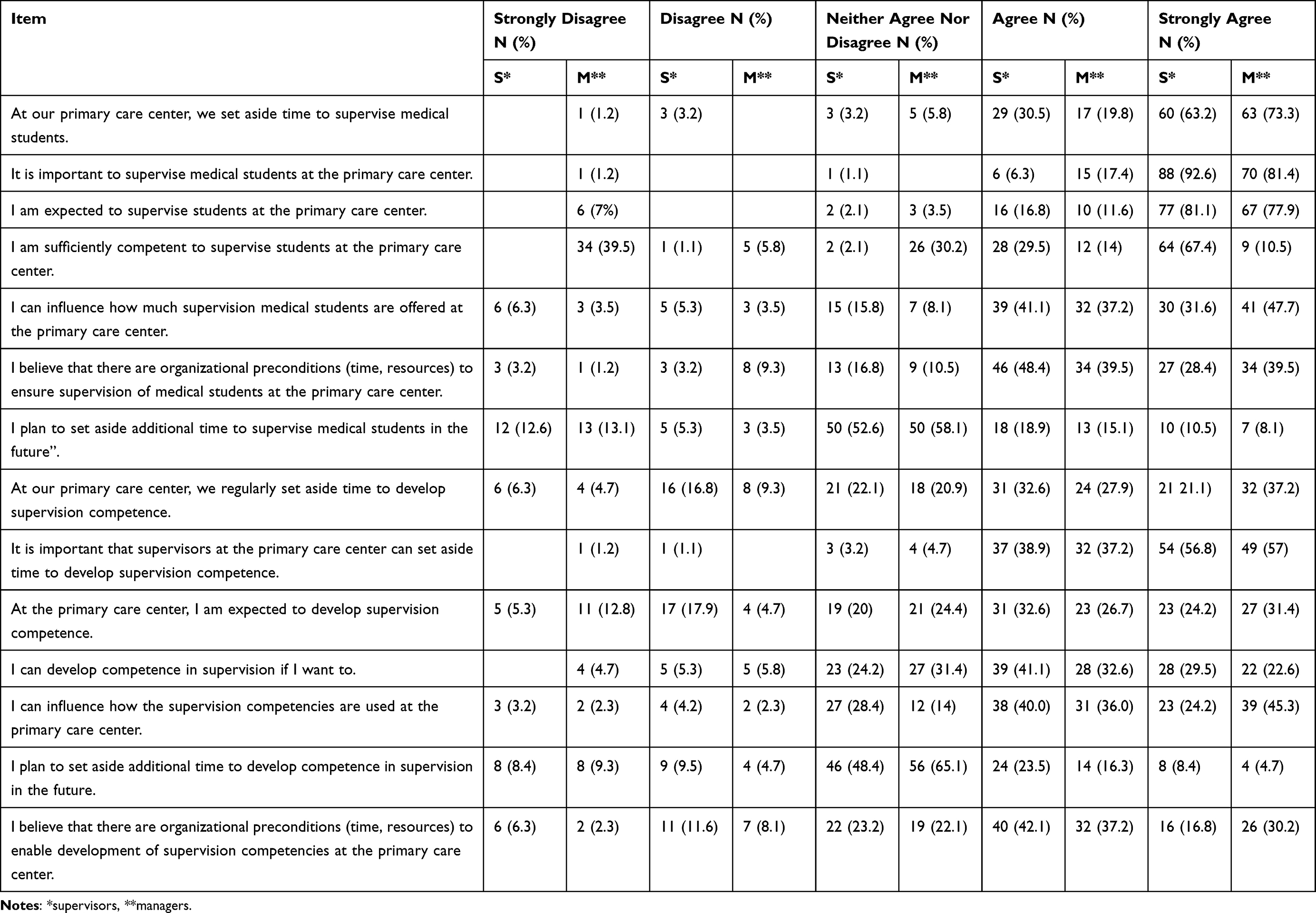 |
Table 3 Distribution of Answers on the Likert Scale for Supervisors (N = 95) and Managers (N = 86) |
Spearman’s rank-order correlations were used to identify item correlations (between predictors of behavior and behavioral intention) that conformed to the theoretical model of TPB. The item measuring intention to set aside more time for supervision correlated positively with work in a private setting (r = 0.147, p = 0.049, 95% CI −0.004-0.228), social norms (”I am expected to supervise students at the primary care center”, r = 0.193, p = 0.009, 95% CI 0.092-0.224) and controllability (”I can influence how much supervision medical students are offered at the primary care center”, r = 0.187, p = 0.012, 95% CI 0.055-0.293). The item measuring intention to develop supervision competence (”I plan to set aside additional time to develop competence in supervision in the future”) correlated with attitudes towards developing supervision competence (”At our primary care center, we regularly set aside time to enhance our competence in supervision”, r = 0.206, p = 0.005, 95% CI 0.016-0.307), social norms (”At the primary care center, I am expected to develop competence in supervision”, r = 0.161, p = 0.030, 95% CI 0.040-0.330), controllability (”I can enhance my competence if I want to”, r = 0.217, p = 0.003, 95% CI 0.079-0.367) and self-efficacy (”I am sufficiently competent to supervise students at the primary care center”, r = 0.162, p = 0.03, 95% CI 0.009-0.300).
Most participants agreed or strongly agreed that organizational preconditions to ensure supervision of medical students existed at their primary care center. The answers for the item measuring the possibility to develop supervision competencies at the PHCC are shown in Table 3.
No statistically significant differences (Mann Whitney’s test) were found between managers and supervisors for attitudes (U = 3484, p = 0.081), social norms (U = 3873, p = 0.534), perceived behavioral control (U = 3722, p = 0.291) and behavioral intentions (U = 3736, p = 0.271). In summary, behavior predictors derived from TPB were positively correlated to behavioral intention towards supervising and building supervising competence.
Open-Text Comments
While organizational pre-requisites where in place to ensure supervision of medical students at their primary care center”, the open-ended question rendered many suggestions of support and resources needed to utilize these prerequisites and improve the clinical supervision and learning environment of medical students. Three overarching themes emerged from the content analysis of open-text answers: ”Time and distribution”, ”Improved communication and support systems” and ”Elimination of structural barriers” (Table 4).
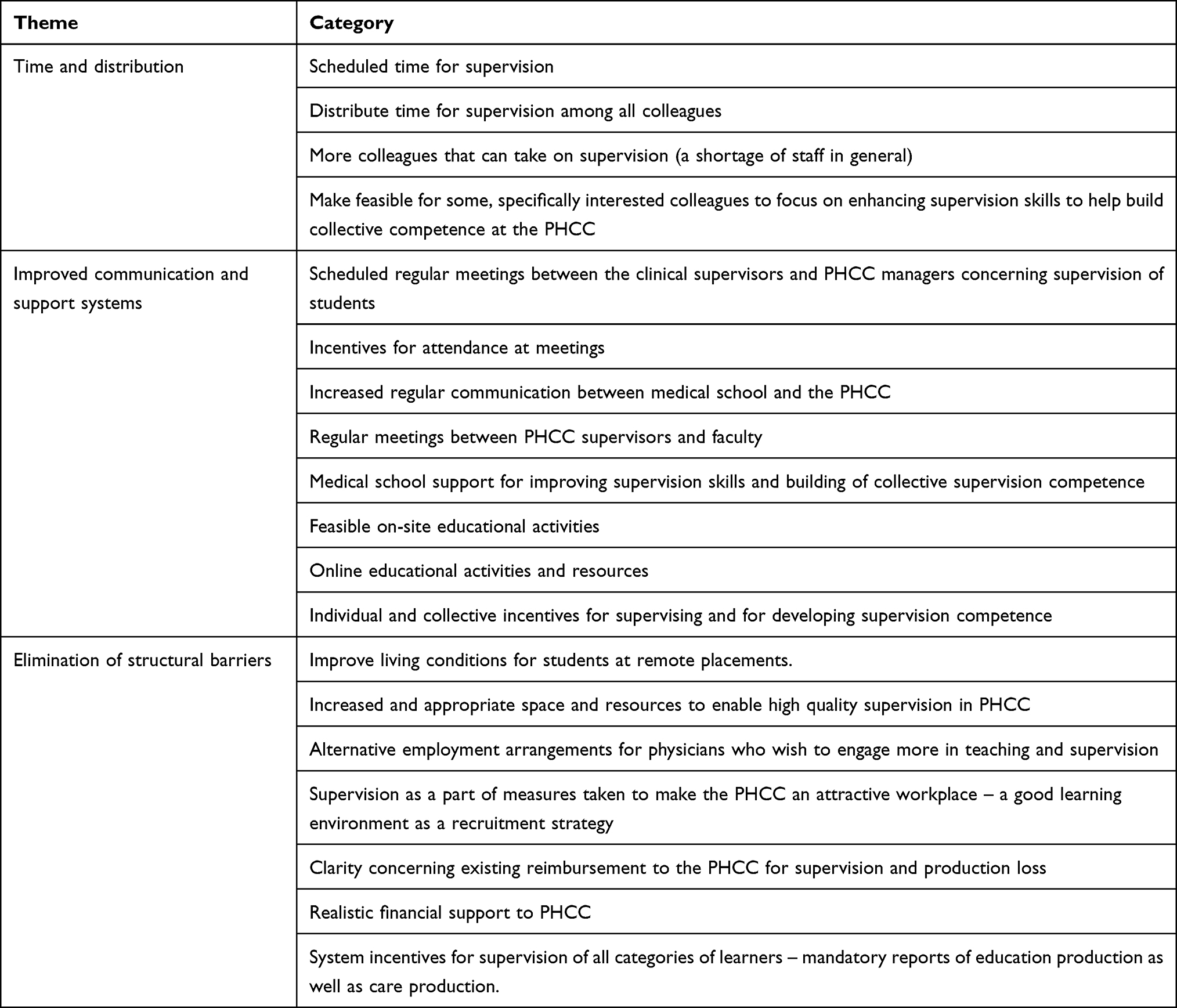 |
Table 4 Themes and Categories Emerged from the Content Analysis of the Open-Ended Question: ”Give Examples of Support/Resources You Need to Improve the Clinical Supervision and Learning Environment of Medical Students at the Primary Care Center” |
Time and Distribution
This theme reflected the frustration created by the shortage of staff in general in primary care and particularly the need for additional physicians. To distribute the task of supervising students among a larger number of physician colleagues would not only reduce the time and engagement needed of a supervisor but also enable sharing and discussing supervision practice. This theme included suggestions mostly from clinical supervisors of how physicians with additional, supervision competence could support colleagues on-site to improve supervision at the PHCC. This would save time and money.
Improved Communication and Support Systems
This theme reflected the need for improved communication between the involved stakeholders. Some clinical supervisors perceived that not all physicians were motivated to attend educational meetings with focus on student teaching: “Few people come to the annual teaching meeting, that’s a shame …” Both managers and supervisors made suggestions for improvement focused on regularity of meetings between managers and staff/faculty at medical school and clinical supervisors, to ensure that information from the medical school reached the staff and the supervisors. Among support systems that could increase competence and quality of supervision were more direct support to the PHCC for updates and training, feasible on-site activities, and easily available resources. Reasonable financial compensation for supervision and competence building was another recurrent category of support.
Elimination of Structural Barriers
This theme reflected the priority of care production over educational activities at the PHCC. The quantitative data suggested that the supervisors perceived control over how time was spent, but the free answers showed that time and space for developing supervision skills was not always prioritized due to pressure of producing care from the managerial office: ”It is of course within my control to improve my supervision skills and to take time for it, but it does not happen within the framework of my working hours. Every moment that is prioritized for supervision (whether it is students, nurses, medical colleagues) takes place through overtime work that is not compensated financially or with time off.”
This theme included PHCC managers idea of including supervision quality as a strategy for recruitment. Several additional categories (Table 4) reflected the need to eliminate structural barriers and adapt an organizational approach that integrates the support of and measuring of the quality of supervision and learning environments in the healthcare quality assurance system. Managers stressed incentives for supervision as one key indicator of quality of care among others. They also stressed the need to include reports of “education production” as well as of care production in mandatory quality report systems: ”A system where all training that takes place in parallel with healthcare production is made visible. Primary health care centers should be required to report the number of educational services and the different categories of students. How much time has been set aside for supervision and measures taken to train tomorrow’s physicians and healthcare staff?”
Managers also emphasized supervision among several measures taken to make the PHCC an attractive workplace – a good learning environment as a recruitment strategy: ”Taking good care of medical students is the best way of promoting the PHCC”.
Additional barriers (Table 4) that needed to be eliminated were lack of appropriate reimbursement, space and resources (eg computers for students, access of students to patient information, video cameras for educational purposes). PHCC units are in general undersized and to increase quality of supervision, adequate material resources and physical space are necessary.
Discussion
Principal Findings
The overarching aim of the present study was to map, on the one hand, PHC physicians’ and managers’ behavioral intentions related to clinical supervision of medical students and on the other hand, their perceptions of structural preconditions and support needed to sustain and develop clinical supervision practice. A majority of the participating PHC supervisors and managers reported positive attitudes towards supervising medical students and building supervision competence at their PHCC. Most participants strongly agreed or agreed that they had sufficient competence in supervision, that they were expected to supervise and could influence supervision practice and build competence if they wanted to, at their workplace. Attitudes, perceived behavioral control, self-efficacy, and social norms were positively correlated to behavioral intention i.e planning to set aside time for supervision and competence-building. Participants agreed that organizational preconditions for high-quality supervision and learning environments exist in the PHCC environment. However, the three themes that emerged from the content analysis of the open-text comments (”Time and distribution”, ”Improved communication and support systems” and ”Elimination of structural barriers”) described improvements and support needed for sustainable solutions and engagement.
In many aspects, our findings are in line with previous research on primary care physicians’ perceptions of undergraduate student supervision. For instance, in accordance with previous results on the supervision and teaching of undergraduate medical students in primary care21 we found that allocated time, adequate workload, availability of space and adequate financial compensation are measures that if taken would improve opportunities to build a more favorable supervision practice.
The self-reported supervision competence of the primary care physicians in our study is comparable to findings of a previous Swedish study.37 Experienced primary care physicians felt confident to supervise medical students although they felt they lacked skills for coordinating clinical clerkships or improve the overall learning environments.37
The same study found that the role as ambassador for primary care by increasing students’ interest for general medicine as a future specialty was a key incentive for primary care physicians to supervise medical students.37 In our study, primary care managers stressed the advantage of trying to create a favorable supervision and learning environment for medical students, and that would increase the opportunities to recruit future staff to primary care. This is in accordance with studies suggesting that career choices and work location are influenced by medical students’ experiences of learning environments.5,6 Our results support also previously reported findings suggesting that practice managers’ support and engagement is a significant and probably undervalued factor in the recruitment and retainment of undergraduate students in primary care.38
A contribution of our study to existing research is the combined theoretical lenses of theory of planned behavior and practice theory that allowed for an analysis of both behavioral intention and perceptions of workplace affordances related to the development of favorable supervision and learning environments of undergraduate medical students in primary care.
Our study indicates that the attitudes and agency of individuals or the social norms of the workplace are not the most prominent barriers for development. Positive behavioral intention towards developing high quality supervision practice is evident in our findings. Moreover, the organizational preconditions for supervision are perceived as sufficient and although structural impediments for exercising power to improve practice are strong, they could be eliminated. From a practice theory perspective, our findings suggest that many supervisors in primary care have the capacity to exercise agency but how and to what degree they engage in supervision and competence building is determined by how the workplace - and the medical school – afford participation in supervision-related workplace activities. In line with previous studies, we found that primary care physicians and managers felt marginalized, isolated from the rest of the medical school and teacher and supervisor community of practice.21 We also found that participants in our study in accordance with primary care physicians in other studies reported that not all clinical supervisors felt motivated to attend faculty development activities or central supervisor meetings.21 Among suggestions for improving practice in our study were recurrent allocated meetings at the workplace for communication with the medical school and support for competence building in on-site, collaborative group activities.
Implications for Practice
A possible implication of our findings is that measures taken to recruit and support primary care centers as medical student placements should involve infrastructures for increased, organized, and direct communication between medical school, managers, and supervising physicians. Our findings moreover suggest that traditional approaches to faculty development such as offering individual supervisors to attend courses or workshops to improve supervision skills might be less effective compared to collaborative learning activities on-site and on-line, focused on building collective, sustainable competence. Alternative employment arrangements and career paths where committed physicians combine patient care with educational responsibilities could be an effective way of improving supervision and learning environments and thereby serve as a recruitment strategy. As previously highlighted in the literature, measures taken to improve supervision practice in primary care as well as in other healthcare contexts should consider the distribution of affordances, space, and place for learning between groups of learners in a patient- and service-centred environments.39,40
Strengths and Limitations
The questionnaire was sent to all primary care practices in Southern Sweden, covering a large variety of settings with different characteristics regarding both staff and patient demography, which is a strength of this study. Researchers followed guidelines for development and dissemination of the questionnaire. The response rate was high, which is unusual in web-based surveys.41 This might be explained by the distribution method where e-mails were sent to managers and physicians with a specific responsibility for students’ placements. However, we did not use log-files or cookies to eliminate the risk that one single responder could fill the survey several times, a common problem of web-based surveys.42 The selection of respondents is likely to have influenced the results. The questionnaire was initially tested with face-validity among 14 primary care physicians with previous experience of student supervising. Other primary care physicians might have different attitudes toward supervision and building supervision competence. No managers were involved in the face-validity, which is also a limitation of the study.
A limitation of the study is that our findings represent a relatively narrow work in Swedish primary care. Information about PCHHs’ specific contexts as geography, size and staffing was not collected. Additional research is needed using methods that allow for the explorations of thoughts and meanings behind the interpretations of data on perceptions of PHCC supervision gained by the survey.
Addressing both clinical supervisors and managers as key facilitators of a favorable supervision learning environment is also a strength as most previous studies have focused solely on clinical supervisors’ attitudes and experiences.
Conclusion
Most participants in our study (managers and physicians in Swedish primary care) reported positive attitudes towards supervising medical students and sufficient competence to supervise. We conclude that the attitudes and agency of individuals or the social norms of the workplace are not the most prominent barriers for developing supervision practice in the Swedish primary care setting of our study. Analysis of correlations suggests that predictors are linked to positive behavioral intention towards developing high quality supervision practice in the studied primary care setting. However, while behavioral intention is a strong determinant of social behavior, it is beyond the reach of this study to make any assumptions of the actual behavior of the participating managers and supervisors. However, a conclusion of our study from a practice theory perspective24 is that many supervisors in primary care perceive that they have the capacity to exercise power to achieve changes but how and to what degree they engage in supervision and competence building is determined by how the workplace - and the medical school – afford participation in supervision-related workplace. Improved communication between medical school, managers and supervising physicians and on-site faculty development integrated in daily clinical work were described as important facilitators of favorable supervision and teaching of medical students in primary care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research or authorship of this article.
Disclosure
The authors declared no potential conflicts of interest in relation to this work.
References
1. WHO. The World Health Report 2008 - Primary Health Care (Now More Than Ever); 2008. Available from: https://www.who.int/whr/2008/en/.
2. Baird BCA, Honeyman M, Maguire D, Das P. Understanding Pressures in General Practice. London: King’s Fund; 2016.
3. Thistlethwaite JE, Kidd MR, Hudson JN. General practice: a leading provider of medical student education in the 21st century? Med J Aust. 2007;187(2):124–128.
4. Theobald M, Ruttter A, Steiner B, Morley CP. Preceptor Expansion Initiative Takes Multitactic Approach to Addressing Shortage of Clinical Training Sites. Fam Med. 2019;51(2):159–165.
5. Cleland J, Johnston PW, French FH, Needham G. Associations between medical school and career preferences in Year 1 medical students in Scotland. Med Educ. 2012;46(5):473–484.
6. Cleland JA, Johnston PW, Anthony M, Khan N, Scott NW. A survey of factors influencing career preference in new-entrant and exiting medical students from four UK medical schools. BMC Med Educ. 2014;14:151.
7. Selva Olid A, Zurro AM, Villa JJ, et al. Medical students’ perceptions and attitudes about family practice: a qualitative research synthesis. BMC Med Educ. 2012;12:81.
8. Barber S, Brettell R, Perera-Salazar R, Greenhalgh T, Harrington R. UK medical students’ attitudes towards their future careers and general practice: a cross-sectional survey and qualitative analysis of an Oxford cohort. BMC Med Educ. 2018;18(1):160.
9. Nicholson S, Hastings AM, McKinley RK. Influences on students’ career decisions concerning general practice: a focus group study. Br J Gen Pract. 2016;66(651):e768–75.
10. van der Hem-Stokroos HH, Daelmans HE, van der Vleuten CP, Haarman HJ, Scherpbier AJ. A qualitative study of constructive clinical learning experiences. Med Teach. 2003;25(2):120–126.
11. Dornan T, Conn R, Monaghan H, Kearney G, Gillespie H, Bennett D. Experience Based Learning (ExBL): clinical teaching for the twenty-first century. Med Teach. 2019;41(10):1098–1105.
12. Strand P, Edgren G, Borna P, Lindgren S, Wichmann-Hansen G, Stalmeijer RE. Conceptions of how a learning or teaching curriculum, workplace culture and agency of individuals shape medical student learning and supervisory practices in the clinical workplace. Adv Health Sci Educ Theory Pract. 2015;20(2):531–557.
13. Strand P, Sjöborg K, Stalmeijer RE, Wichmann-Hansen G, Jakobsson U, Edgren G. Development and Psychometric Evaluation of the Undergraduate Clinical Education Environment Measure (UCEEM). Med Teach. 2013;35(12):1014–1026.
14. Bansal A, Singh D, Thompson J, Kumra A, Jackson B. Developing Medical Students’ Broad Clinical Diagnostic Reasoning Through GP-Facilitated Teaching in Hospital Placements. Adv Med Educ Pract. 2020;11:379–388.
15. Chan SCC, Jetha N, Baid R. Tension in the primary-secondary care interface: changing medical students views on general practice. Med Educ. 2019;53(6):639.
16. van der Zwet J, Hanssen VG, Zwietering PJ, et al. Workplace learning in general practice: supervision, patient mix and Independence emerge from the black box once again. Med Teach. 2010;32(7):e294–9.
17. Salminen H, Ohman E, Stenfors-Hayes T. Medical students’ feedback regarding their clinical learning environment in primary healthcare: a qualitative study. BMC Med Educ. 2016;16(1):313.
18. En akut bild av Sverige. Kartläggning av akutsjukvårdens organisation och arbetsfördelning. Myndigheten för vård och omsorgsanalys. Swedish: Les Creatives Sthlm; 2018.
19. Anell A. Health Systems in Transition 2012. Available from: https://www.euro.who.int/__data/assets/pdf_file/0008/164096/e96455.pdf.
20. Hawken SJ, Henning MA, Pinnock R, Shulruf B, Bagg W. Clinical teachers working in primary care: what would they like changed in the medical school? J Prim Health Care. 2011;3(4):298–306.
21. Barber JRG, Park SE, Jensen K, et al. Facilitators and barriers to teaching undergraduate medical students in general practice. Med Educ. 2019;53(8):778–787.
22. Thomson J, Haesler E, Anderson K, Barnard A. What motivates general practitioners to teach. Clin Teach. 2014;11(2):124–130.
23. Irby DM. Excellence in clinical teaching: knowledge transformation and development required. Med Educ. 2014;48(8):776–784.
24. Billet S, Newton J. A learning practice. Conceptualising professional lifelone learning for the health-care sector. In: Bradbury H, Frost N, Kilminster S, Zukas M, editors. Beyond Reflective Practice: New approaches to professional lifelong learning. Oxon, England: Routledge; 2010:52–65.
25. Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health. 2011;26(9):1113–1127.
26. Lathia A, Rothberg M, Heflin M, Nottingham K, Messinger-Rapport B. Effect of a Novel Interdisciplinary Teaching Program in the Care-continuum on Medical Student Knowledge and Self-Efficacy. J Am Med Dir Assoc. 2015;16(10):848–854.
27. Lapkin S, Levett-Jones T, Gilligan C. Using the Theory of Planned Behaviour to examine health professional students’ behavioural intentions in relation to medication safety and collaborative practice. Nurse Educ Today. 2015;35(8):935–940.
28. Francis JJ, Eccles MP, Johnston M, et al. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers. Centre for Health Services Research, University of Newcastle; 2004.
29. Milos V, Jakobsson U, Westerlund T, Melander E, Molstad S, Midlov P. Theory-based interventions to reduce prescription of antibiotics–a randomized controlled trial in Sweden. Fam Pract. 2013;30(6):634–640.
30. Hadadgar A, Changiz T, Masiello I, Dehghani Z, Mirshahzadeh N, Zary N. Applicability of the theory of planned behavior in explaining the general practitioners eLearning use in continuing medical education. BMC Med Educ. 2016;16(1):215.
31. Grierson LE, Fowler N, Kwan MY. Family medicine residents’ practice intentions: theory of planned behaviour evaluation. Can Fam Physician. 2015;61(11):e524–31.
32. Schatzki TR. Practice theory. In: Schatzki TR, Knorr-Cetina K, von Savigny E, editors. The Practice Turn in Contemporary Theory. London/New York: Routledge; 2001.
33. Ajzen I. The Theory of Planned Behavior. Organ Behav Hum Decis Process. 1991;50(2):179–212.
34. Mulder H, Ter Braak E, Chen HC, Ten Cate O. Addressing the hidden curriculum in the clinical workplace: a practical tool for trainees and faculty. Med Teach. 2019;41(1):36–43.
35. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55.
36. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115.
37. Von Below B, Haffling AC, Brorsson A, Mattsson B, Wahlqvist M. Student-centred GP ambassadors: perceptions of experienced clinical tutors in general practice undergraduate training. Scand J Prim Health Care. 2015;33(2):142–149.
38. Wass V, Gregory S, Petty-Saphon K By choice - not by chance: supporting medical students towards future careers in general practice. 2016. https://www.medschools.ac.uk/media/2881/by-choice-not-by-chance.pdf.
39. Bleakley A. Professing medical identities in the liquid world of teams. Med Educ. 2011;45(12):1171–1173.
40. Kitto S, Nordquist J, Peller J, Grant R, Reeves S. The disconnections between space, place and learning in interprofessional education: an overview of key issues. J Interprof Care. 2013;27(Suppl 2):5–8.
41. Leece P, Bhandari M, Sprague S, et al. Internet versus mailed questionnaires: a randomized comparison (2). J Med Internet Res. 2004;6(3):e30.
42. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.