Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Hospital Cost Savings for Sequential COPD Patients Receiving Domiciliary Nasal High Flow Therapy
Authors Milne RJ ![]() , Hockey HU
, Hockey HU ![]() , Garrett J
, Garrett J
Received 7 December 2021
Accepted for publication 24 March 2022
Published 3 June 2022 Volume 2022:17 Pages 1311—1322
DOI https://doi.org/10.2147/COPD.S350267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Min Zhang
Richard J Milne,1,2 Hans-Ulrich Hockey,3 Jeffrey Garrett4
1Health Outcomes Associates Ltd, Auckland, New Zealand; 2School of Pharmacy, University of Auckland, Auckland, New Zealand; 3Biometrics Matters Ltd, Hamilton, New Zealand; 4Middlemore Hospital, Auckland, New Zealand
Correspondence: Richard J Milne, Health Outcomes Associates Ltd, 260 Major Hornbrook Road, Christchurch, 8081, New Zealand, Tel +64 21 02361114, Email [email protected]
Purpose: To estimate the 5-year budget impact to Aotearoa New Zealand (NZ) hospitals of domiciliary nasal high flow (NHF) therapy to patients with chronic obstructive pulmonary disease (COPD) who require long term oxygen therapy.
Methods: Hospital admission counts along with length of stay were obtained from hospital records of 200 COPD patients enrolled in a 12-month randomized clinical trial of NHF in Denmark, both over a 12-month baseline and then in the study period while on randomized treatment (control or NHF). NZ costings from similar COPD patients were estimated using data from Middlemore Hospital, Auckland and were applied to the Danish trial. The budget impact of NHF was estimated over the predicted 5-year lifetime of the device when used by patients sequentially.
Results: Fifty-five of 100 patients in the NHF group and 44 of 100 patients in the control group were admitted to hospital with a respiratory diagnosis during the baseline year. They had 108 admissions in the treatment group vs 89 in the control group, with 632 vs 438 days in hospital, and modeled annual costs of $9443 vs $6512 per patient, respectively. During the study period there were 38 vs 44 patients with 67 vs 80 admissions and 302 vs 526 days in hospital, at a modeled annual cost of $6961 vs $9565 per patient respectively. Taking into account capital expenditure and running costs, this resulted in cost savings of $5535 per patient-year (95% CI, -$36 to -$11,034). With 90% usage over the estimated five-year lifetime of the NHF device, amortized capital costs of $594 per year and annual running costs of $662, we estimate a 5-year undiscounted cost saving per NHF device of $18,626 ($16,934 when discounted to net present value at 5% per annum). There would still be annual cost savings over a wide range of assumptions.
Conclusion: Domiciliary NHF therapy for patients with severe COPD has the potential to provide substantial hospital cost savings over the five-year lifetime of the NHF device.
Keywords: cost, hospital admissions, nasal high flow, COPD, long term oxygen therapy, LTOT, budget impact, New Zealand
Corrigendum for this paper has been published.
Introduction
Respiratory disorders such as chronic obstructive pulmonary disease (COPD) place a large burden on hospital budgets. Community interventions that reduce exacerbations of bronchitis, improve quality of life and reduce the need for hospital admissions and length of stay have the potential to both enhance patients’ lives and to save healthcare costs. This is particularly important when hospital respiratory services are burdened with Covid-19 patients.
In Aotearoa New Zealand (NZ) there were 61,516 hospital admissions for COPD over the 5-year period July 1, 2008, to June 30, 2013, costing $300m.1,2 When adjusted for population and inflation in medical services costs, this amounts to $83m in 2020, assuming a stable incidence rate. Like many other chronic diseases, COPD disproportionately affects indigenous Māori and Pasifika peoples.1 Healthcare providers worldwide are seeking approaches to reduce costly hospital admissions.
Oxygen administered via NHF is used worldwide for managing critically ill patients hospitalized with hypoxaemic respiratory failure, which is not always feasible using ordinary face masks or standard nasal cannulae.3 AirvoTM NHF devices (Fisher & Paykel Healthcare Ltd, Auckland, NZ) are used in Middlemore Hospital, Auckland (MMH), and increasingly across other NZ hospitals, for managing patients suffering acute exacerbations of COPD, bronchiectasis, and pneumonia. They have also gained acceptance in managing patients admitted with SARS-CoV-2 pneumonitis, so long as patients are managed in a negative pressure environment to reduce the potential for cross infection. Indeed, of COPD patients admitted to MMH, 50% received NHF and 42% used continuous positive airway pressure, which have both been shown to reduce the need for intubation and intensive care unit admission.4,5
The Airvo NHF device allows warmed and humidified air to be delivered at high flow rates ranging from 10 to 60 L/min, thus increasing the fraction of inspired oxygen from 21% to 100% depending on patient requirement. In addition it provides a modest increase in end expiratory airway pressure of 2–5cm H2O, which increases carbon dioxide clearance and diminishes the work of breathing in both acute and chronic (ie home based) stable settings.3,6–10 The clinical and economic benefits of NHF for both COPD and bronchiectasis patients in the ambulatory care setting have also been evaluated in randomized controlled trials both in NZ11–13 and in Denmark.14,15 Subsequent economic evaluation in NZ showed this intervention to be cost effective by local criteria, with a cost per quality adjusted life year (QALY) of around $NZ20,000.11
A randomized, controlled, 12-month trial of NHF in 200 patients with COPD and chronic hypoxaemia in the North Jutland Region of Denmark between December 2013 and July 2015 demonstrated reduced frequency of both non-admitted and admitted exacerbations of COPD and a lower total score on the St. Georges Respiratory Questionnaire. The average use of the NHF device was 5.9 hours per day, varying from almost nil to 10 hours. Inclusion criteria were chronic hypoxic failure (ie, three arterial blood gasses during stable conditions demonstrating hypoxemia) and previously prescribed long-term oxygen therapy (LTOT) by a pulmonary medicine specialist. Exclusion criteria were malignant disease, terminal nonmalignant disease, unstable psychiatric disease, and long-term non-invasive ventilation.14
The NHF treatment group had a predicted annual exacerbation rate of 3.12 compared with 4.95 per annum in the control group (p<0.001), adjusted for baseline rate, age, and sex. Predicted hospital admission rates favoured the treatment group (1.08 versus 1.22/patient/year, p = 0.373). In addition, for both exacerbations and admissions there was a strong regression relationship between event rate and actual number of days of use of NHF. For hospital admissions, predicted rates were 0.79 versus 1.39/patient/year for 12 months versus zero use of NHF respectively. Subsequent economic analysis of the same study reported a substantial increase in quality of life based on the St George’s Respiratory Questionnaire and when mapped to quality adjusted life years (QALYs).14
In order to estimate economic costs and benefits of medical interventions, it is both cost effective and useful to apply the findings of a clinical study to a similar patient group in another country. In this paper we report the number of hospital admissions in the treatment and control groups in the year before and after inclusion in the Danish clinical trial. We then apply current NZ costings to hospital admissions for similar COPD patients, using data derived from Counties Manukau District Health Board (CMDHB) which serves a population of 580,000. A budget impact analysis was developed from this information.
Regional oxygen budgets reside within the hospital system of care, and patients are reviewed in the outpatient clinic or from an outreach system of care. Any reduction in hospital admission rates would offset the cost of acquiring and maintaining the NHF device. Therefore, the present study takes a hospital perspective, with a focus on hospital costs and potential savings over the estimated five-year lifetime of the NHF device.
Methods
The methods of the Danish clinical trial and the characteristics of the patients have been reported in detail.14,15 Briefly, 200 patients were randomized into usual care ± NHF. At inclusion, acute exacerbations of COPD and hospital admissions one year before inclusion, modified Medical Research Council (mMRC) score, St George’s Respiratory Questionnaire (SGRQ), forced expiratory volume in 1 second (FEV1), 6-minute walk test (6MWT) and arterial carbon dioxide (PaCO2) were recorded.
Inclusion criteria were COPD with chronic hypoxemic respiratory failure (ie three arterial blood gases during stable conditions demonstrating hypoxemia). Exclusion criteria were malignant disease, terminal nonmalignant disease, unstable psychiatric disease and home treatment with noninvasive ventilation (NIV) or a change in smoking habits during the study period.15
Enrolled patients had a self-care plan with prednisone and antibiotics available. They were recommended to use the myAirvoTM NHF system with OptiflowTM cannula (Fisher and Paykel Healthcare, Auckland, New Zealand) for at least 8 hours a day, preferably at night. After titration the temperature was set to 37°C and the average flow rate was 20 L/min. Patients in the myAirvo NHF group who ceased that treatment before 12 months were nevertheless encouraged to remain in the study for all scheduled assessments and event counts.
Hospital admissions data were obtained from hospital records. Hours of usage were retrieved electronically from the NHF device.
Intervention Costs
Capital costs and running costs were obtained from the manufacturer, along with the expected lifetime of the NHF device myAirvoTM (at least 5 years). The annual cost for consumables was based on six breathing tubes, six autofill chambers, and 12 OptiflowTM nasal cannulas per year. The cost of oxygen was excluded because all patients in both groups were already receiving oxygen from an oxygen concentrator, which would be passed on to the next patient.
Exacerbations of COPD
Published analysis of the clinical study showed a substantial reduction in exacerbations, as counted via patient diaries and phone calls.14,15 However, the available information does not clarify how non-admitted patients were managed, and detailed information about the timing of these exacerbations is not available. Therefore, in order to avoid double counting and the need to impute missing data, we excluded all patient-reported information from the current analysis. This is conservative (see Discussion).
Hospital Admissions and Costs
Hospital admissions with any diagnosis of COPD were counted from Danish hospital records for a 12-month period before and after inclusion in the study. In order to apply an economic evaluation of the Danish study to the NZ context, we required the cost of each hospital admission for each patient. This information was not available from Denmark and in any case is not necessarily relevant to NZ. Therefore, NZ costs for hospital admissions were obtained from a respiratory clinic database at Middlemore Hospital for patients with any diagnosis of COPD. None of these patients had received domiciliary NHF. In selecting patients, COPD diagnostic guidelines were stringently adhered to.16,17 Thirty percent of these patients had evidence of mild bronchiectasis on computerized tomography criteria, thought to be secondary to COPD, and 54% had blood eosinophil counts of >0.3 or 3% (eosinophil count /white blood count) implying an increased risk of exacerbations, and were on inhaled steroid therapy. The average life expectancy of this patient group is around 5 years, and all patients remain on LTOT indefinitely.
Thirty patients in the clinic database who had been receiving long-term oxygen therapy for at least three months were selected to correspond to the Danish cohort. All of these patients had been admitted at least once to Middlemore Hospital in the period April 1st, 2018, to April 1st, 2020, with a total of 79 hospital admissions.
Individual hospital admission costs are based on hours of stay per hospital ward, with different costs per ward and time of day depending on staffing ratios (eg, staffing ratios are lower at night). The cost of non-admitted Emergency Department visits were not included. However, most patients with severe COPD who present to the Emergency Department are admitted to hospital. Costs were adjusted to 2020 NZ dollars (NZD) using the NZ Consumers Price Index. The mean daily cost of an individual hospital admission for this patient group was obtained by linear regression of actual hospital cost, as determined by CMDHB analysts, on length of stay.
Analytical Methods
Baseline data included hospital admission counts in the 12-month period prior to inclusion in the study. About one-third of the patients withdrew from treatment before their 12-month study period ended and some others chose to continue treatment beyond 12 months, but data on hospital admissions beyond the 12-month study length were not available. In economic analyses we assumed that the device will be passed from one eligible patient to another when it is no longer required, with a delay between patients, and that process continues until the end of the five-year lifetime of the NHF device (see Discussion). For the base case analysis we assumed 90% usage (range 85% to 95%).
Hospital admissions with any diagnosis of COPD within a 12-month period before inclusion in the clinical study and from inclusion up to the time of withdrawal from treatment or from observation (in the control group) or 12 months, whichever was shorter, were counted from hospital records.
There were 100 patients in the control group and 100 patients in the treatment group. Hospital admissions, hospital days and cost per patient were calculated for each patient. Although the patients were randomized to treatment groups, in the year prior to inclusion the average hospital cost was considerably higher in the treatment group than the control group, due to more admissions. Hence treatment comparisons effectively use the change in annualized costs from the baseline year to the study period.
All baseline data were based on one year but not all study period data were. Hence study period costs per patient were annualized by division by the fraction of a year data was observed per patient. And in summation and analysis, weighting by the length of time observed was used so the annualized data contributed in proportion to how long a period occurred, typically one year, but not always.
Although there were only two sets of measurements per patient over time (pre- and post-treatment), a repeated measures mixed model was used so the 400 data points could each be correctly weighted.
Results
Treatment
Information was available for all 200 patients in the clinical trial, 100 in each treatment group. Clinical details are provided elsewhere.14,15 The NHF flow rate was titrated at the baseline visit from 15 L/min to 20 L/min. For the majority of patients, the supplementary O2 flow rate (of average 1.7 L/min) was not altered when on NHF compared to their oxygen therapy only. Fifty-six percent overall were female, and the mean age was 70.7 years. The randomized treatment groups were well-matched clinically except for a difference in modified Medical Research Council Dyspnoea (mMRC) score.
Most (66%) patients in the NHF treatment arm of the study continued with treatment for the duration of the 12-month study period although their usage was variable. Overall device compliance, defined as the average ratio of the number of days actually used compared with the number of days before treatment was terminated, was 92%. Within the 12-month study period, the mean period on treatment or observation (truncated to 12 months) was longer in the control arm than the NHF arm (307 days vs 249 days). However, NHF patients could remain in the study after ceasing active HFNC use, and the mean study observation period in both arms was almost equal. Nevertheless, because the device will be passed from one patient to another, our calculations are based on the actual period of use.
Hospital Admissions
Fifty-five patients in the treatment group and 44 patients in the control group were admitted to hospital during the 12-month baseline period. The information available to the researchers was by ward admissions, from which hospital admissions and days per patient were derived. In the total period under analysis (including baseline year) there were 413 ward admissions with a principal or secondary diagnosis classified as respiratory (ICD10 Jxxx using international notation) and 345 hospital admissions (Table 1). Almost one-half of the ward admissions had a principal diagnosis of “COPD with acute exacerbation, unspecified” (J441) whereas J440 (“COPD with acute lower respiratory infection”) dominated in a NZ study of a previous version of the same device for patients with moderate or severe COPD or bronchiectasis.11,12 Both studies had a similar frequency of J440 and J441 taken together. Pneumonia (ICD10 J189) comprised 7.7% of the principal diagnoses of ward admissions in the Danish study (Table 1). The distribution of principal diagnoses is similar to that of hospital admissions in the CMDHB (NZ) data set: J440 + J441, 39/79 (49.4%) and J47, 7/79 (8.9%).
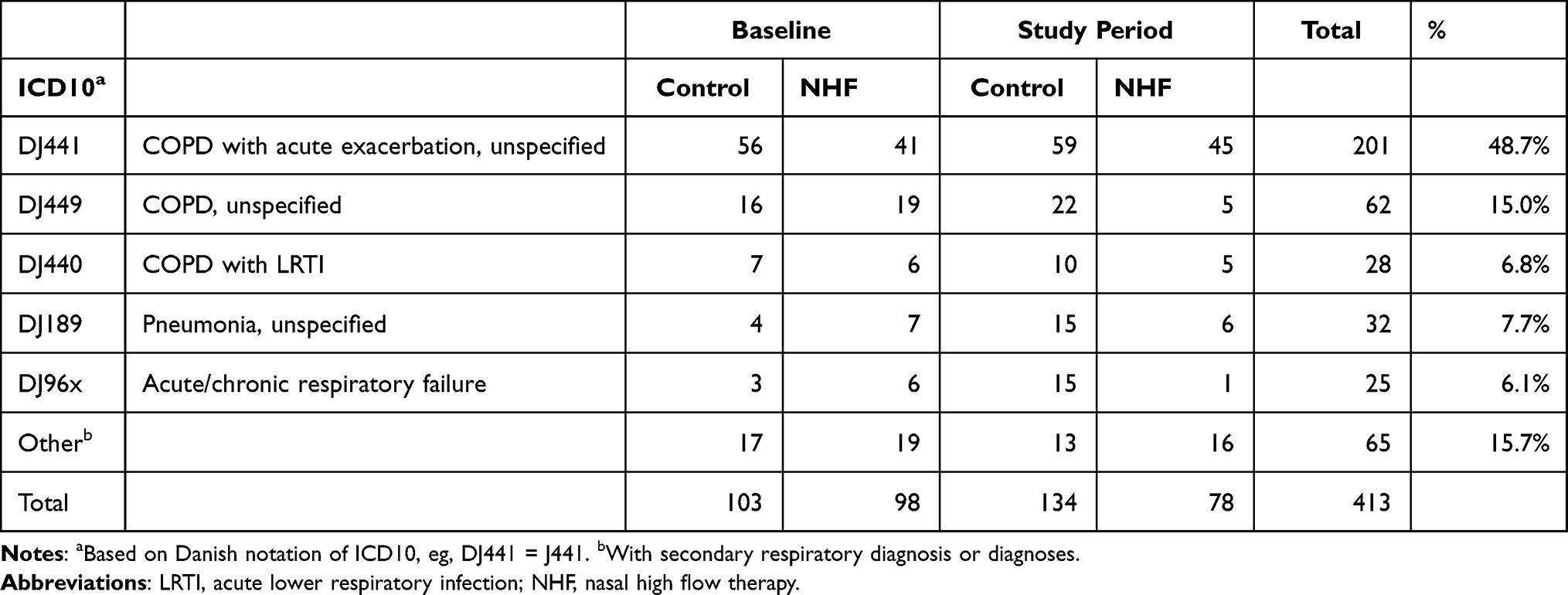 |
Table 1 Principal Diagnosis for 413 Ward Admissions in the Period 12 Months Before Treatment and During the Study Period |
Adherence
In the treatment group, daily usage of the NHF device varied considerably, with 37% using it for less than five hours a day on average during the treatment period. The mean duration of treatment, as measured by the device, was 5.6 hours per day over the treatment period (median 6.2 hours). Regardless, all patients receiving the device were included in the analysis and running costs were based on average daily usage.
Hospital Admission Costs in Aotearoa New Zealand
Because hospital admission costs were not provided in the Danish study and in any case are not directly relevant to NZ, we estimated NZ costs adjusted to December 2020 NZ dollars (NZD), with data from MMH for a similar patient group.
During the period April 1st, 2018, to April 1st, 2020, there were 79 hospital admissions by 30 patients who fulfilled the criteria (see Methods). Linear regression analysis on length of stay (LOS) gave the cost per admission of:
Cost = $478 + $1234×(LOS+1) [R2 = 0.83]
Both the LOS (discharge date minus admission date) and the hospital costs in the MMH data varied considerably, with a few long stayers, as also occurred in the Danish study. The two country cohorts were comparable in mean age and average length of stay (Table 2).
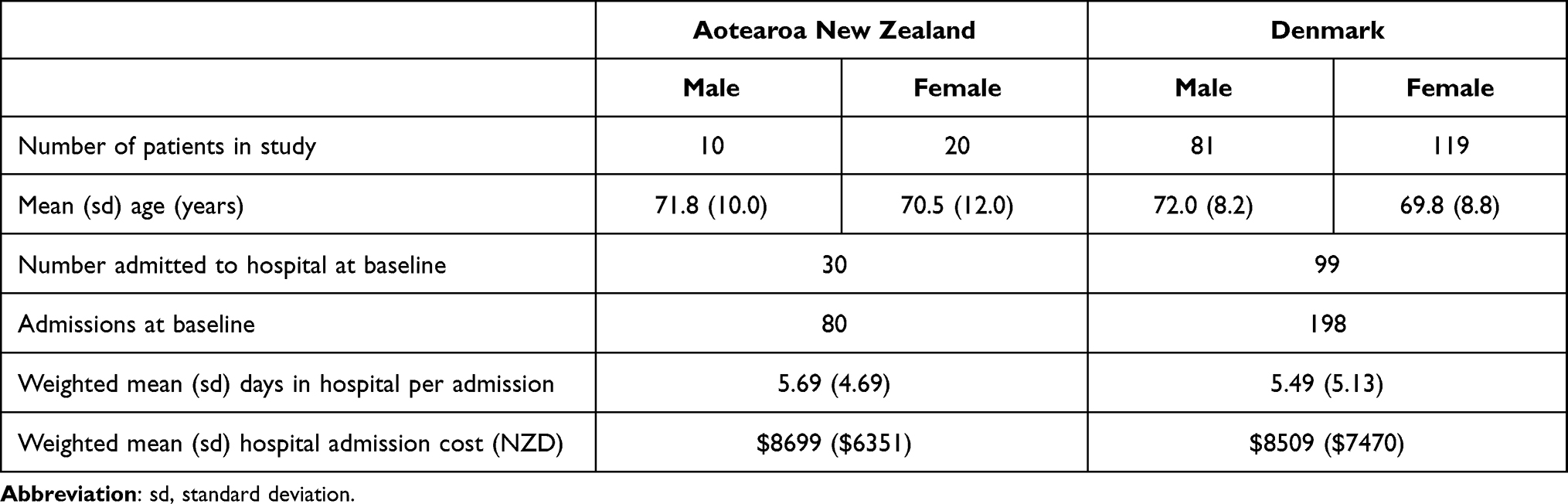 |
Table 2 Comparison of the New Zealand Cohort with the Danish Cohort at Baseline |
Hospital Admission Rates, Days, and Costs
All patients were included. Comparing the treatment period with the 12-month baseline period, hospital admission rates increased by 7% in the control group but declined by 9% in the treatment group. The annualized number of days in hospital increased by 43% in the control group but declined by 30% in the treatment group. Because of these changes, the modeled admission costs increased by 47% in the control group but declined by 26% in the treated group (Table 3).
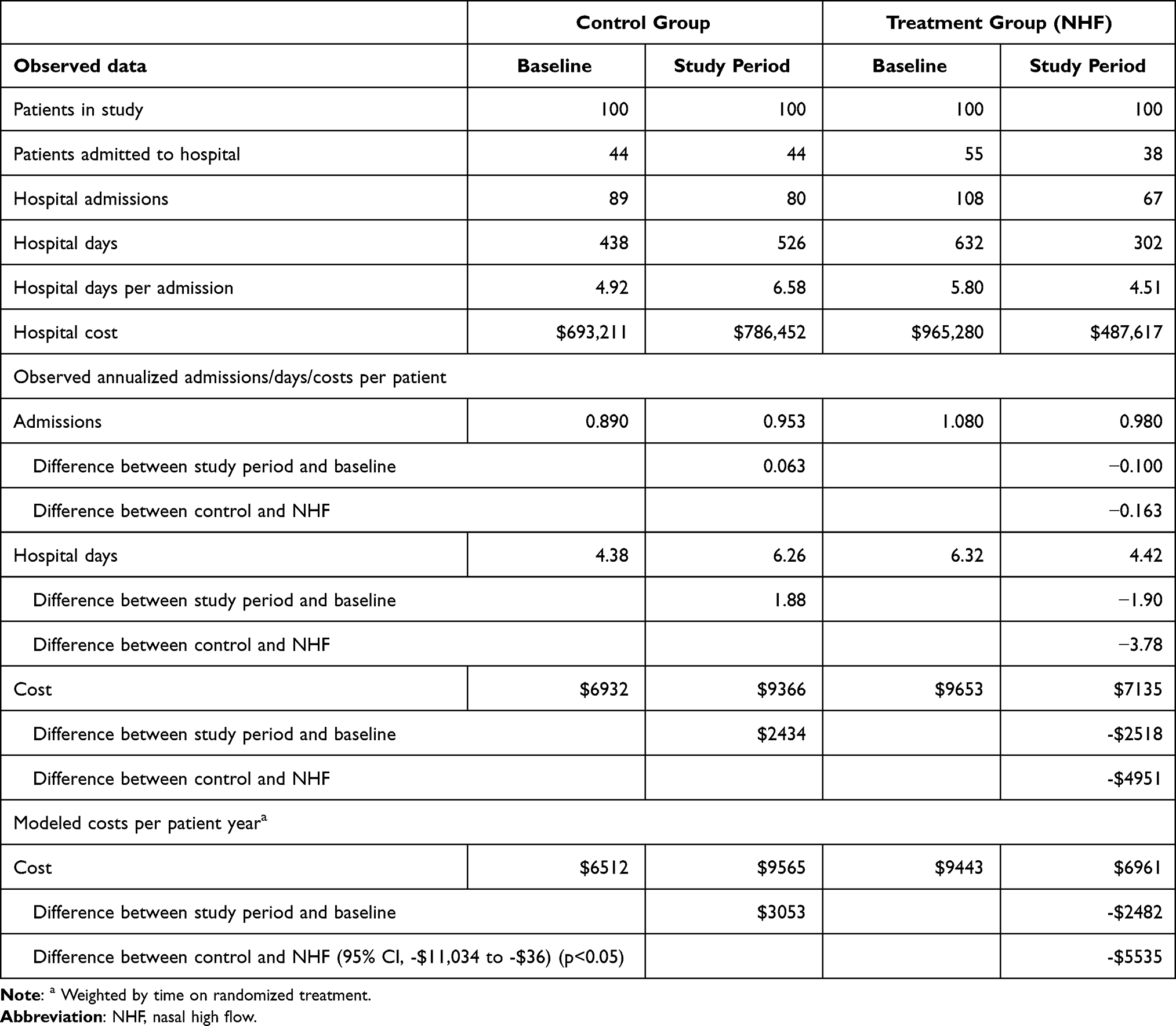 |
Table 3 Hospital Admissions, Hospital Days and Admission Costs (2020 NZD) Before and After the Treatment Period Began |
Intervention Costs
Because the treatment is self-administered, only the capital cost and running costs are relevant (Table 4). Setup costs for each patient, including deep cleaning, are included in the capital cost. Capital costs were amortized over 5 years at an interest rate of 5% per annum. For completeness, the cost to the household for electricity (not shown), assuming an average of 5.6 hours use per day (as measured from the NHF device) and 25c/kWh on the margin, is approximately $66 per year. Water costs are not relevant in NZ because the device uses potable tap water.
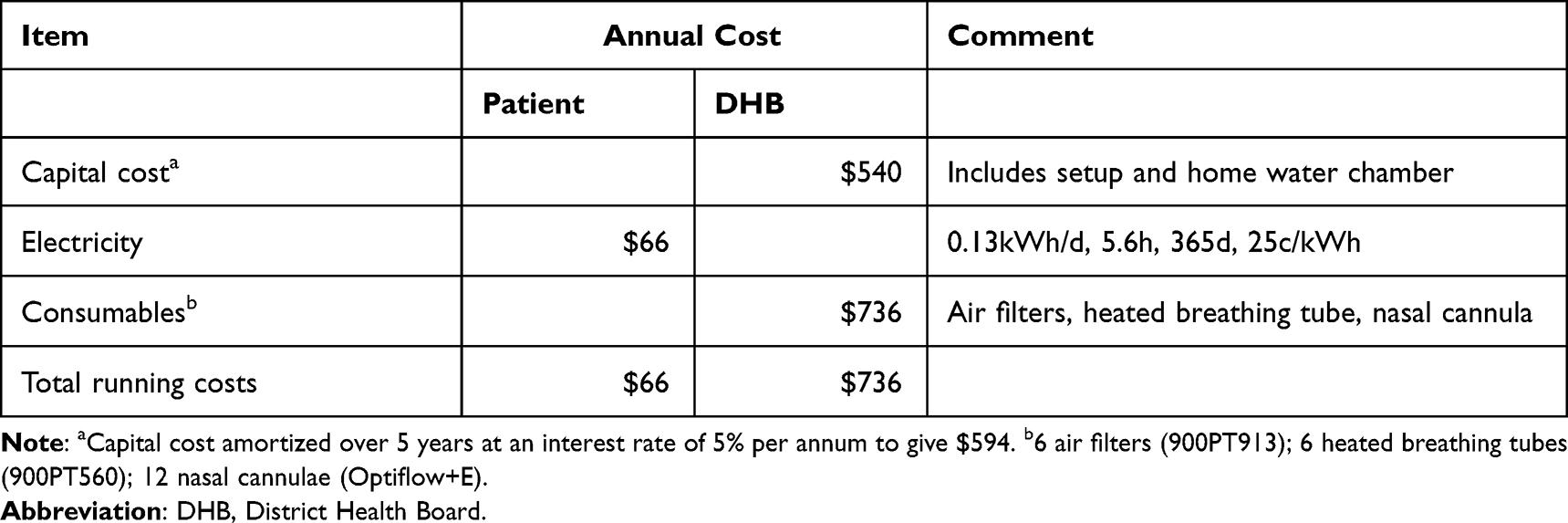 |
Table 4 Costs of the NHF Device Assuming Fulltime Use for 12 Months |
Hospital Budget Impact
In practice there will be administrative delays between sequential patients utilising the NHF device. In the base case analysis we assumed 90% usage with zero running costs or economic benefits when not in use. There are minimal transition costs because the setup cost is included in the purchase price. Based on hospital admissions alone, and assuming that the capital cost of the NHF device ($2700) is amortized over five years at an interest rate of 5% per annum, there would be substantial cost savings due to averted hospital admissions and reduced days in hospital (Table 5). The predicted 5-year cost saving is $18,626 per device if the device has 90% usage, or $17,426 for 85% usage or $19,826 for 95% usage (Table 5).
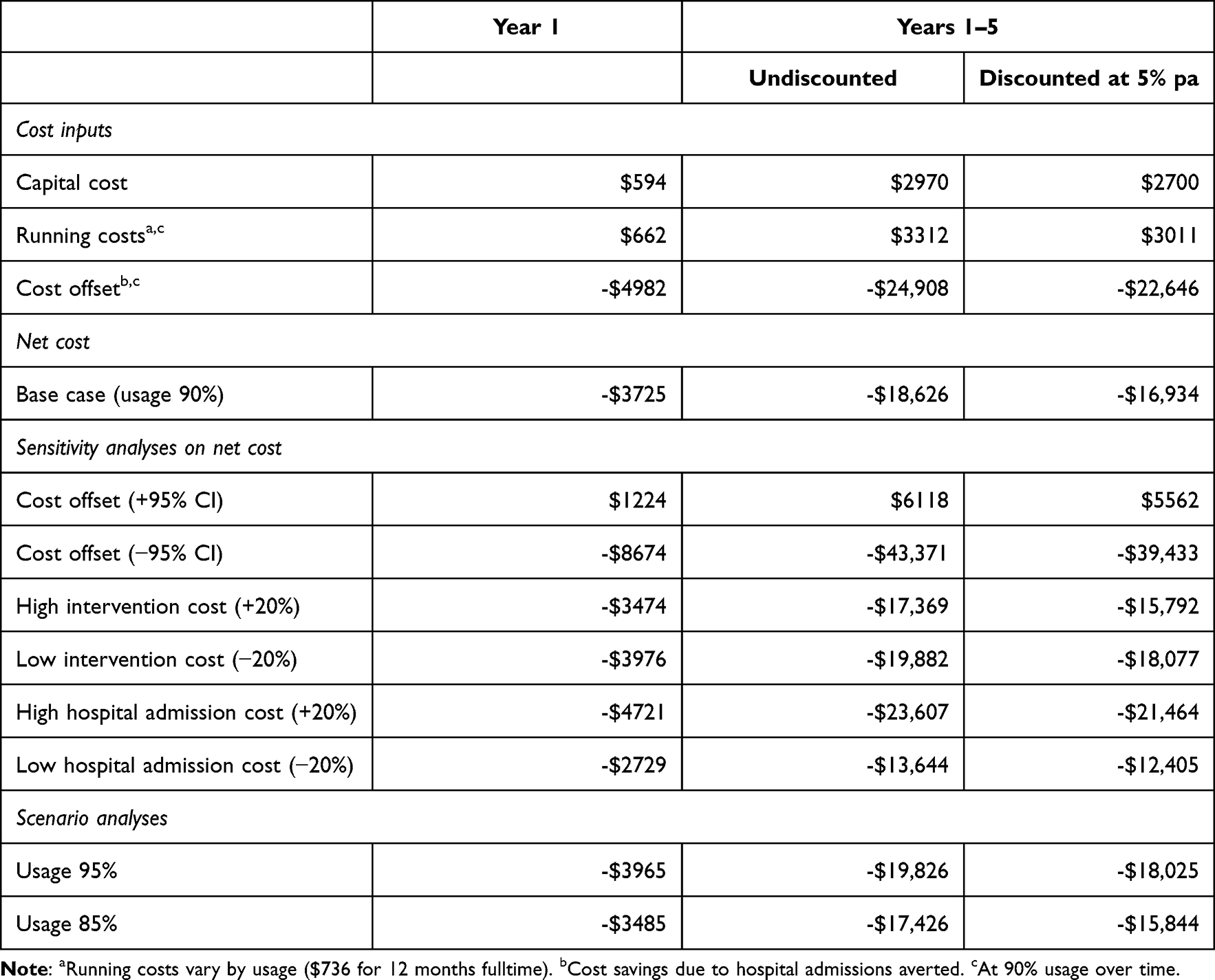 |
Table 5 Predicted Hospital Budget Impact per Device Over 5 Years (2020 $NZ) |
The budget impact varies considerably with the cost offset; and in the least favourable case (ie, at the high limit of the 95% confidence interval of the cost offset; see Table 3) it would cost the DHB $6118 per NHF device over a 5-year period. If the cost of a hospital admission is lower in Denmark relative to the local cost of the NHF device, the cost difference between treatment and control arms of the clinical study might not outweigh the cost of therapy. However, our sensitivity analysis showed that if the cost of a hospital admission was 20% lower there would still be a substantial cost savings over the lifetime of the device in the NZ context (Table 5). Furthermore, we showed that even an increase of 50% in the capital cost of the equipment would have only a minor effect on the cost savings. On the other hand, the economic outcome of the analysis is sensitive to the cost offset that was determined from the number of hospital admissions averted (Table 5).
In practice, the mean cost of hospital admissions for exacerbations of COPD is unlikely to be 20% more or less than that which we measured. The capital cost of the NHF equipment is realistic for the New Zealand market, although it was substantially higher for the Danish economic evaluation and it could differ across other markets.
If a decision needs to be made between purchasing the NHF device versus other hospital purchases within a given financial year, it is appropriate to discount future costs to net present value, independent of inflation. At net present value (NPV), all other variables being equal, and using a discount rate of 5% per annum, there is a predicted cost saving of $16,934 per device over its 5-year lifetime at 90% usage. In the least favourable case (ie at the high limit of the 95% confidence interval of the cost offset; Table 3), the device would cost the DHB $5562 over 5 years at net present value (Table 5).
Discussion
This is the first study to show that for sequential COPD patients receiving long-term oxygen therapy, NHF is very likely to be cost saving to the hospital budget. The cost saving to the overall healthcare budget is underestimated because the clinical trial showed a substantial reduction in exacerbations of COPD, a proportion of which were managed in the community but were not included in this analysis.15 However, self-managed exacerbations, primary care, medications and non-admitted Emergency Department visits (if any) would cost considerably less on average than the cost of a hospital admission; therefore, additional cost savings would be modest. Further, if patients were instructed to increase their use of NHF during an exacerbation they would potentially derive three specific benefits: (a) a reduction in the work of breathing (ie reduced positive end-expiratory pressure; PEEP)10,18 (b) a reduction in hypercapnia7–9,19 and (c) an increase in mucociliary clearance for those suffering symptoms of bronchitis.20 The Danish study did not attempt to amplify the positive effects of NHF by suggesting that usage be increased during exacerbations.
Findings of the clinical trial have been reported in detail previously and are not the main focus of this study.15 We have no direct information on why hospital admission rates differed at baseline or why they increased in the control group during the study period; but the increase is not unexpected because the patients had severe COPD which progresses over time. The contrast between the treatment group and control group is a strong indicator of the effectiveness of myAirvo NHF therapy, as reported previously.15
An increased need for hospitalization is a known risk factor for death for COPD patients on LTOT.21 Therefore, as shown in the control group (Table 3), it could be expected that the admission rate for the COPD cohort on LTOT would increase over time and specifically within the subgroup at highest risk of dying. The reduction in admission rates one year after starting treatment therefore is very favourable.
Our base case analysis applies to all patients who were given the NHF device, whether or not they used it as instructed. However, 37% of the patients used the device for less than 5 hours a day on average and others used it intermittently. Also, 11 patients (overlapping with the above group) discontinued therapy within the first month, some immediately. In practice, usage could be monitored for a few weeks while the patient adjusts to using the device and withdrawn if the patient is unable to tolerate it and/or is unwilling to use it. Transitioning to a new patient would be inexpensive because the cost of cleaning the NHF device and setting up for a new patient is included in the capital cost (see Table 4). Our previous analysis showed that the benefits were proportional to usage.15 Replacing a patient who underutilised the NHF device with another eligible patient would enhance both the net benefits and the potential cost savings of this therapy. Some patients were lost to the clinical study because they died, and others withdrew for various reasons including inconvenience. This does not affect the findings of our economic model, because each patient who withdraws is replaced by another eligible patient within the five-year lifetime of the NHF device.
In the base case analysis we assumed 90% usage, amounting to about one month delay between average patients. This is conservative for 2 reasons: (a) some patients utilized the device for more than 12 months, although information about their hospital admissions was not captured or included in this study; and (b) the number of patients on the LTOT register at MMH has remained constant over time, as patients who withdraw from NHF therapy are replaced by new registrants. In general, demand for the device is likely to outstrip supply. Indeed, acquisition of oxygen concentrators over the past 10 years have been provided as part of a replacement programme or to acquire more versatile concentrators (eg, capable of filling portable oxygen cylinders) rather than a need to keep pace with expanding demand. Adherence to NHF varied considerably from patient to patient. In the New Zealand context, the cost of NHF is covered by public funds and therefore is unlikely to make any difference to patient compliance.
This study could underestimate the costs at MMH because LTOT patients are severely ill and often require assisted ventilation on admission, which is not incorporated into the costs. Their average LOS is longer than average for respiratory patients and intriguingly, very similar to that of the Danish study (see Table 2).
The oxygen service in NZ and at MMH is funded by the budget for respiratory services. The service is run by specialist respiratory nurses with oversight by a designated respiratory physician. The nurses provide an outreach programme and apart from evaluating patients regularly within an ambulatory care setting are able to perform home visits when required. As above, the service could be used more often during subacute events such as in supporting patients with an exacerbation of COPD at home with further potential to reduce hospitalization. If NHF devices were available, adjustments in flow and in oxygen delivery could be made during exacerbations of COPD, which could amplify the economic impact of NHF outlined in this paper.
Study Strengths
This study, using secure hospital information without the need for data imputation or linkage, illustrates a generalisable methodology for applying clinical results from one country to budgetary considerations in another. This is much less costly than conducting an independent study. Unlike most economic evaluations of clinical trials, it considers the financial impact of the NHF device over its lifetime, with replacement of those patients who withdraw from therapy with other eligible patients. This is particularly important because of the high mortality of eligible patients. This information is valuable to hospital budget holders and decision makers.
Previous evaluation of the same clinical study, based on device use, showed a per-protocol benefit on admissions, but a comparison by randomized group (intention-to-treat) only favoured NHF non-significantly.15 However, that analysis underestimates the benefits because it counted COPD hospital admissions that occurred even after the NHF device was no longer in use by the patient.
Study Limitations
Our budget impact analysis was based on a moderately sized clinical study, in which about one-third of patients withdrew from therapy or from observation and some patients died during the 12-month study period. All risk factors for admissions, such as smoking history, were not directly considered in this economic analysis, but the trial was randomized and the number of pre-treatment admissions per patient will be a consequence of all risk factors. The study included COPD patients with a wide range of daily usage of NHF, as would be expected in real life. The economic model is based on the pragmatic assumption that the NHF equipment will be passed from one patient to another during the lifetime of the equipment; therefore, reasons for withdrawal from the study are not relevant to the economic conclusions of the study.
One limitation of this study is that it did not include the potential cost savings generated by non-admitted exacerbations of COPD.14,15 Inclusion of these would provide more cost savings, albeit mostly to the primary care budget and the household rather than to hospitals.
Inevitably, applying an economic analysis to a study in a different country with a different healthcare system is challenging. NZ data were used solely to generate costs that could be applied to the Danish study and are based on a carefully selected population of COPD patients who had been using LTOT for at least three months, as in the Danish study. One limitation of this methodology is that the NZ and Danish discharge criteria might differ. However, similarity of length of stay in the Danish study and NZ (Table 2) gives confidence that the study populations were similar.
Other Studies
While our economic evaluation was being completed, the Danish team published a comprehensive cost utility analysis of the same clinical study which included both hospital costs and primary care.14 Like our previous analysis of the same clinical trial,15 the Danish analysis was conducted as a 12-month intention-to-treat analysis14 but it did not model the pragmatic scenario of replacing one patient with another when the device is no longer being used. The Danish analysis relied on patient-specific database linkage, which is not feasible outside the country in which the trial was conducted.
The Danish analysis estimated a small incremental cost (GBP 304.4) over 12 months, with wide confidence intervals.14 In contrast, we estimate a net cost saving over 12 months of $NZ 5535 (GBP 2711), also with wide confidence intervals. The difference in means can be attributed partly to different capital costs of myAirvo in Denmark (approximately 43% higher at February 2022 exchange rates). However, the cost outcome in the NZ model is dominated by a difference in hospital admission rates and is not particularly sensitive to capital expenditure (Table 5).
More importantly, the two studies address different questions. The Danish study reported an intention-to-treat analysis of the clinical trial, during which a substantial proportion of treated patients died or withdrew from therapy for other reasons. The NZ economic model (this paper) replaces each patient who withdraws from therapy with another patient from the hospital waiting list, adjusting for equipment usage (transitional delays). There are also differences in the methodologies for adjusting for different baseline admission rates and duration of treatment. We believe that our 5-year economic model is more relevant to the practical use of NHF over the lifetime of the medical device, although it is limited to hospital admissions.
This study suggests that there is sufficient information to acquire NHF devices for the LTOT population or at the very least to conduct a Phase 4 prospective study to assess whether it is possible to improve upon the findings of the Danish study by maximizing the full potential of NHF. This could be done by providing it only to compliant patients and improving usage during exacerbations in the community. Information needs to be collected systematically to better identify those patients who exhibit obvious benefit (eg, reduced frequency of exacerbations or evidence of bronchiectasis at baseline) and to determine whether NHF used overnight whilst asleep20 leads to an improved outcome. Further, NHF may both increase the quality of sleep and also increase exercise capacity. Taken together, these benefits may increase the length of time that patients use LTOT. If such factors were apparent and were enhanced by NHF use, then they may also impact over time on mortality rates.
Conclusion
Domiciliary humidified oxygen enriched air applied through a warmed, nasal cannula to sequential patients with severe COPD has the potential to avert hospital admissions and provide substantial cost savings over the estimated five-year lifetime of the HFNC device.
Ethics Approval
Ethics approval for the clinical trial was obtained previously from the North Jutland Ethical Committee and the Danish Data Protection Agency and the clinical and economic findings have been published.14,15 The current study is based on anonymised data from this clinical trial. For New Zealand data, Counties Manukau District Health Board have advised that ethics approval is not required for this low-risk clinical audit of anonymised retrospective data. Use of New Zealand anonymised hospital admissions data also meets the expectations of the Ministry of Health for ethics approval.
Acknowledgments
Lila Prasad for providing NZ clinical data; Rosie Whittington for providing NZ cost data; William Good for assistance with referencing; Line Hust Storgaard, Ulla Møller Weinrich and Birgitte Schantz Laursen for providing the Danish clinical trial data.
Disclosure
Funding for this analysis was provided as consultancy fees to RJM and HUH by Fisher & Paykel Healthcare Ltd, supplier of the myAirvo nasal high flow device for the clinical trial. Fisher & Paykel Healthcare Ltd reviewed the manuscript but took no part in the experimental design, analysis or interpretation of the findings. RJM is Managing Director of Health Outcomes Associates Ltd. HUH is an employee and majority shareholder in Biometrics Matters Ltd. The authors report no other potential conflicts of interest for this work.
References
1. Milne RJ, Beasley R. Hospital admissions for chronic obstructive pulmonary disease. NZ Med J. 2015;128(1408):23–35.
2. Barnard L, Zhang J. The impact of respiratory disease in New Zealand: 2016 update; 2016 [cited October 7, 2021]. Available from: https://www.asthmafoundation.org.nz/research/the-impact-of-respiratory-disease-in-New-Zealand-2016-update.
3. Frat JP, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–2196. doi:10.1056/NEJMoa1503326
4. Ni YN, Luo J, Yu H, Liu D, Liang BM, Liang ZA. The effect of high-flow nasal cannula in reducing the mortality and the rate of endotracheal intubation when used before mechanical ventilation compared with conventional oxygen therapy and noninvasive positive pressure ventilation. A systematic review and meta-analysis. Am J Emerg Med. 2018;36(2):226–233. doi:10.1016/j.ajem.2017.07.083
5. Marini JJ, Gattinoni L. Management of COVID-19 respiratory distress. JAMA. 2020;323(22):2329–2330. doi:10.1001/jama.2020.6825
6. Sun J, Li Y, Ling B, et al. High flow nasal cannula oxygen therapy versus non-invasive ventilation for chronic obstructive pulmonary disease with acute-moderate hypercapnic respiratory failure: an observational cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:1229–1237. doi:10.2147/COPD.S206567
7. Nagata K, Kikuchi T, Horie T, et al. Domiciliary high-flow nasal cannula oxygen therapy for patients with stable hypercapnic chronic obstructive pulmonary disease. A multicenter randomized crossover trial. Ann Am Thorac Soc. 2018;15(4):432–439. doi:10.1513/AnnalsATS.201706-425OC
8. McKinstry S, Pilcher J, Bardsley G, et al. Nasal high flow therapy and PtCO2 in stable COPD: a randomized controlled cross-over trial. Respirology. 2018;23(4):378–384. doi:10.1111/resp.13185
9. Fraser JF, Spooner AJ, Dunster KR, Anstey CM, Corley A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and end-expiratory lung volumes: a randomised crossover trial. Thorax. 2016;71(8):759–761. doi:10.1136/thoraxjnl-2015-207962
10. Pisani L, Fasano L, Corcione N, et al. Change in pulmonary mechanics and the effect on breathing pattern of high flow oxygen therapy in stable hypercapnic COPD. Thorax. 2017;72(4):373–375. doi:10.1136/thoraxjnl-2016-209673
11. Milne RJ, Hockey H, Rea H. Long-term air humidification therapy is cost effective for patients with moderate or severe chronic obstructive pulmonary disease or bronchiectasis. Value Health. 2014;17(4):320–327. doi:10.1016/j.jval.2014.01.007
12. Rea H, McAuley S, Jayaram L, et al. The clinical utility of long-term humidification therapy in chronic airway disease. Respir Med. 2010;104(4):525–533. doi:10.1016/j.rmed.2009.12.016
13. Good WR, Garrett J, Hockey HUP, Jayaram L, Wong C, Rea H. The role of high-flow nasal therapy in bronchiectasis: a post hoc analysis. ERJ Open Res. 2021;7:1. doi:10.1183/23120541.00711-2020
14. Sorensen SS, Storgaard LH, Weinreich UM. Cost-effectiveness of domiciliary high flow nasal cannula treatment in COPD patients with chronic respiratory failure. ClinicoEcon. 2021;13:553–564.
15. Storgaard LH, Hockey HU, Laursen BS, Weinreich UM. Long-term effects of oxygen-enriched high-flow nasal cannula treatment in COPD patients with chronic hypoxemic respiratory failure. Int J Chron Obstruct Pulmon Dis. 2018;13:1195–1205. doi:10.2147/COPD.S159666
16. Asthma-Respiratory-Foundation-NZ. NZ COPD Guidelines 2021. Wellington, New Zealand; 2021 [cited September, 2021]. Available from: https://www.nzrespiratoryguidelines.co.nz/uploads/8/3/0/1/83014052/nz_copd_guidelines_web.pdf.
17. Augusti A, Beasley R, Celli B; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnoses, management, and prevention of COPD; [cited October 2021]. Available from: http://www.goldcopd.org.
18. Biselli PJ, Kirkness JP, Grote L, et al. Nasal high-flow therapy reduces work of breathing compared with oxygen during sleep in COPD and smoking controls: a prospective observational study. J Appl Physiol. 2017;122(1):82–88. doi:10.1152/japplphysiol.00279.2016
19. Nilius G, Franke KJ, Domanski U, Ruhle KH, Kirkness JP, Schneider H. Effects of nasal insufflation on arterial gas exchange and breathing pattern in patients with chronic obstructive pulmonary disease and hypercapnic respiratory failure. Adv Exp Med Biol. 2013;755:27–34.
20. Hasani A, Chapman TH, McCool D, Smith RE, Dilworth JP, Agnew JE. Domiciliary humidification improves lung mucociliary clearance in patients with bronchiectasis. Chron Respir Dis. 2008;5(2):81–86.
21. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.