Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
HIV/AIDS-Related Training Coverage Sponsored by Centers for Disease Control and Prevention and Associated Factors at Health Facilities Providing Antiretroviral Therapy in Southern Ethiopia
Received 25 August 2020
Accepted for publication 23 December 2020
Published 22 January 2021 Volume 2021:13 Pages 53—59
DOI https://doi.org/10.2147/HIV.S278179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Wolde Facha,1 Getahun Molla2
1Department of Epidemiology and Biostatistics, School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of Surgery, School of Medicine, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Wolde Facha
Department of Epidemiology and Biostatistics, School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, PO Box 138, Wolaita Sodo, Ethiopia
Tel +251-912025928
Fax +251- 465511500
Email [email protected]
Background: Large numbers of people living with HIV do not know their HIV status and are not on antiretroviral therapy (ART). In this regard, various gap filling in-service trainings were given for health professionals to achieve the global three ninety-five target by 2020. The objective of this study was to assess Centers for Disease Control and Prevention (CDC) sponsored training coverage and related factors at health facilities providing antiretroviral therapy in southern Ethiopia.
Methods: A facility-based cross-sectional study was conducted in 27 facilities (15 hospitals and 12 health centers) in five zones of southern Ethiopia who were providing ART services in October 2019. A total of 403 health professionals from the 27 facilities were included in the study. Quantitative data were collected, edited, coded, and entered into EpiData version 3.1 and transported to SPSS 20 statistical software for analysis. Descriptive statistics were conducted and data were summarized using tables.
Results: From a total of 403 eligible study participants, 396 were included in the study with the response rate of 98.2%. Our study revealed that only 105 (33.5%) took training to conduct HIV testing for patients who were living with the virus. Our study also showed that all 91 health professionals working in HIV care and the treatment unit took pieces of training related to the service. However, only 102 (45.7%) laboratory professionals had training related to sample collection, HIV testing service, and viral load monitoring. Shortages of supply and equipment, space and trained human resources were claimed by 82 (62.6%), 68 (51.9%), and 46 (35.1%) of respondents, respectively.
Conclusion: Our study showed that there was low coverage of trained staff to deliver HIV testing service and viral load monitoring. However, the coverage was good at HIV/AIDS care, treatment, and prevention units. Almost all health facilities have at least one trained staff member working at each service delivery point.
Keywords: training coverage, HIV/AIDS, CDC, southern Ethiopia
Introduction
Besides the COVID-19 pandemic, globally HIV/AIDS is still a public health problem and about 37.9 million people are living with HIV, 1.7 million new HIV infections, and 770,000 AIDS-related deaths occurred in 2018.1 The global HIV targets set for 2020 will not be reached.2 Of all the people living with HIV, only 81% knew their serostatus, 67% were receiving life-saving antiretroviral therapy, and 59% had suppressed viral loads in 2019.3 Despite gains in preventing new HIV infections, Sub-Saharan Africa remains the region most severely affected by the disease.1 Ethiopia adopted the ambitious global 95-95-95 target announced by UNAIDS in 2014, aiming to end the AIDS epidemic by 2030.4 This target aims that 95% of all people living with HIV will know their HIV status, 95% of those diagnosed with HIV infection will receive antiretroviral therapy (ART), and 95% of all people receiving ART will be virally suppressed by 2020.5 However, the achievement in the country was 79%, 81.1%, and 87.7%, respectively.2
Even though there are differences in prevalence among regions, the prevalence in Southern Nations, Nationalities, and People Region (SNNPR) was 0.42% in 2018.5,6 The country at large and the region specifically responded to the epidemic promptly by adopting HIV treatment guidelines since 2003, which has been regularly updated in 2005, 2007, 2014, and 2018.7 As part of the country, scaling up the number of treatment facilities and training health professionals were aggressively implemented in the southern part of Ethiopia. However, of all people living with HIV, only 59% know their status and 63% are taking ART in the region.6,8 This shows that still a large number of people living with HIV do not know their HIV status and are not on ART. Coverage of trained health professionals and their commitment to delivering appropriate services related to HIV care and treatment could be the main challenge to achieve the global target in the region. In this regard the Regional Health Bureau (RHB) was providing in-service training for health workers in collaboration with CDC to provide the service by trained health professionals. A total of 2,528 trainees took antiretroviral-related pieces of training in our training center for the past 4 years since 2014 and were expected to deliver quality health services for clients as per the training protocol. The training was aimed to deliver HIV prevention, care, and treatment by trained health professionals at all service delivery facilities. However, there was no post-training assessment to audit whether trained individuals were exactly working at a service delivery unit where they got training or not as per the investigators knowledge. Therefore, the objective of this study was to assess training coverage and related factors at health facilities providing antiretroviral therapy in southern Ethiopia in October 2019.
Methods and Materials
Study Design and Setting
A facility-based cross-sectional study was conducted in selected health facilities providing ART services at the central part of southern Ethiopia in October 2019. A total of 27 facilities (15 hospitals and 12 health centers) were randomly selected from 53 facilities (21 hospitals and 32 health centers) that were providing ART services in five zones of southern Ethiopia. A total number of 7,964 patients were currently on ART in these five zones (Wolaita, Dawro, Hadiya, KembataTembaro, and Halaba zones) in 2019.
Study Population
The study population was selected health professionals who took CDC sponsored training in the past 4 years from October 2015 to September 2019 at selected health facilities providing ART services and working in the ART unit, tuberculosis clinic, ART pharmacy unit, maternal and child health unit, outpatient department, and laboratory units. However, those individuals who took pieces of training not related to ART services and non-CDC sponsored were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined using a single population proportion formula with 95% confidence interval, 5% margin of error, assuming 50% appropriate service provision based on providers’ competence after taking CDC sponsored training. By considering a 5% non-response rate the minimum final sample size was 403. About half of health facilities providing ART services in five zones of southern Ethiopia were selected randomly. Based on the trainee pool, a total of 9,489 health workers took CDC sponsored training in the past 4 years in the region, which was used as a sampling frame. The calculated sample size was distributed to each facility based on the proportion of trained staff number. Respondents were selected randomly from trained individuals who were working at respective service delivery units.
Data Collection Methods and Quality Assurance
Interviewer administered questionnaires (Supplementary Material) were used to collect quantitative data from health professionals who took CDC sponsored training. The questionnaire (Supplementary Material) addressed providers’ socio-demographic-related factors, service area-related factors, training-related factors, and health facility-related factors. A data extraction checklist (Supplementary Material) was also used to collect information from the facility head and case team leader so as to identify the total number of professionals working at each department and those who took CDC sponsored training. Three teams were formed to collect data. Each team consists of three members (one from the training University, one from the respective zonal health department, and one from the southern Regional Health Bureau). Three days of training for nine data collectors and three supervisors were given by the principal investigator on how to collect data. The questionnaire (Supplementary Material) was pre-tested on 5% of trainees not included in the study. Discussion was held based on the result of the pre-test to make necessary corrections. Data was checked for completeness by supervisors on a daily basis during the data collection time. Double entry was done by the principal investigator before analysis.
Data Entry and Analysis
Data were edited, coded, and entered into EpiData version 3.1 and transported to SPSS 20 statistical software for analysis. Data were summarized using descriptive statistics like mean and presented by using frequency distribution tables.
Ethical Consideration
Ethical approval and clearance was obtained from the Institutional Research and Ethics Review Committee of Southern Regional Health Bureau and then a letter of cooperation was written to selected health facilities from the respective zonal health departments. Informed consent was obtained voluntarily from all participants to be enrolled in the study and the confidentiality of study participants was ensured in accordance with the Declaration of Helsinki.
Results
Health Professional-Related Factors
Socio-Demographic-Related Factors
From a total of 403 eligible study participants, 396 participants responded to a questionnaire with the response rate of 98.3%. About (203, 51.3%) respondents were from Wolaita zone and (352, 88.9%) were from public facilities. More than half of the respondents were male (209, 52.8%) and had a first degree (232, 58.6%). By profession the majority of the respondents were nurses (127, 32.1%), followed by public health officers (80, 20.2%). About one-third of study participants (146, 36.9%) had less than 5 years of service, and (142, 35.9%) had extra managerial duties at their facility in addition to clinical service provision (Table 1).
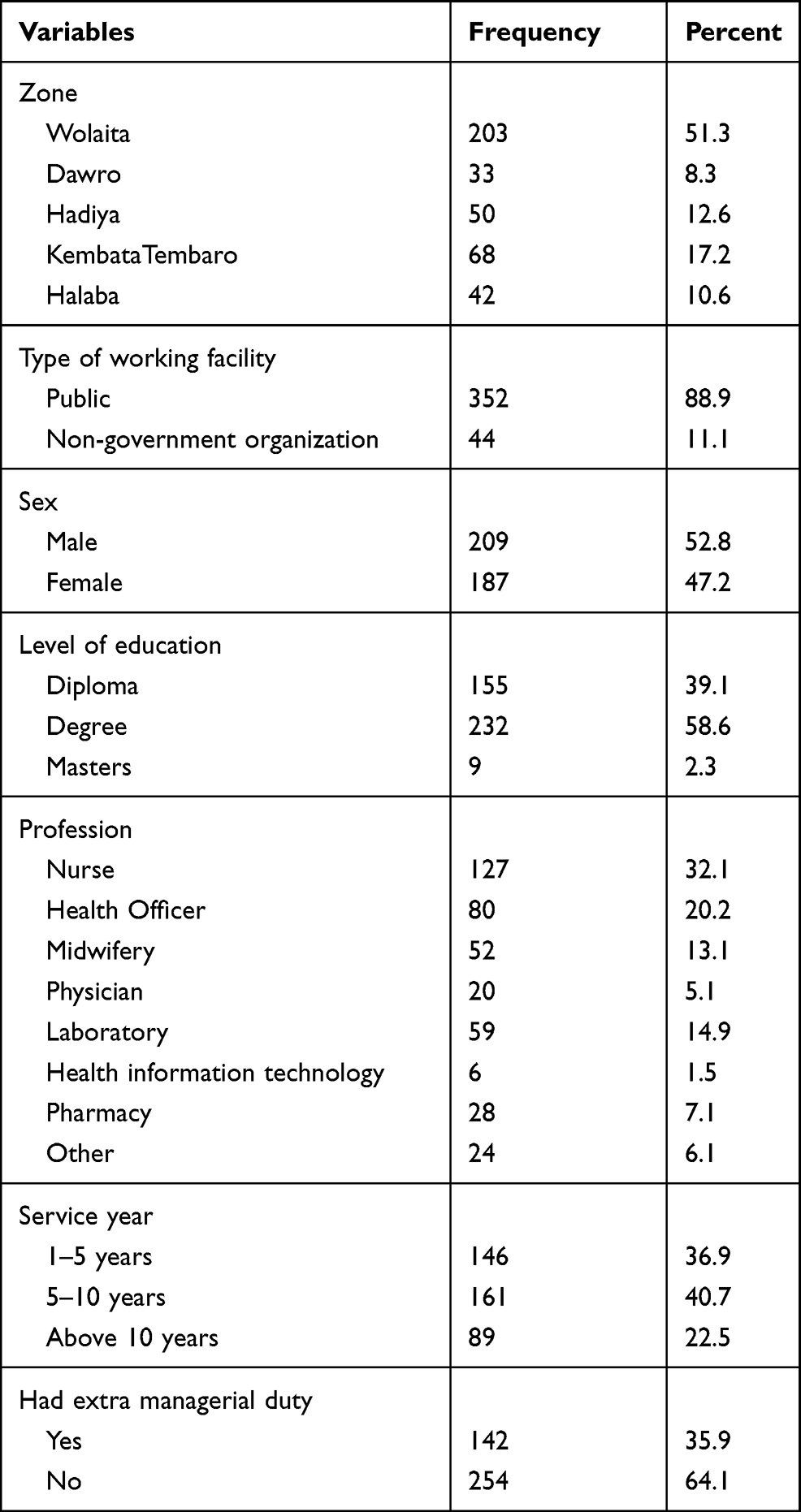 |
Table 1 Socio Demographic-Related Characteristics of Centers for Disease Control and Prevention Sponsored Training Participants in Five Zones of Southern Ethiopia, October 2019 |
Service Area-Related Factors
Of 396 participants included in the study, (85,1.5%) were from the ART unit, followed by the outpatient department (76, 19.2%). The majority of study participants (325, 82.1%) were currently working on units where they got training, and (357, 90.2%) were providing services for clients for at least 5 days per week. However, (109, 27.5%) took training before 2 years, (66, 16.7%) were not happy providing services in the area they got the training, and (159, 40.2%) were never mentored by a responsible body after training (Table 2).
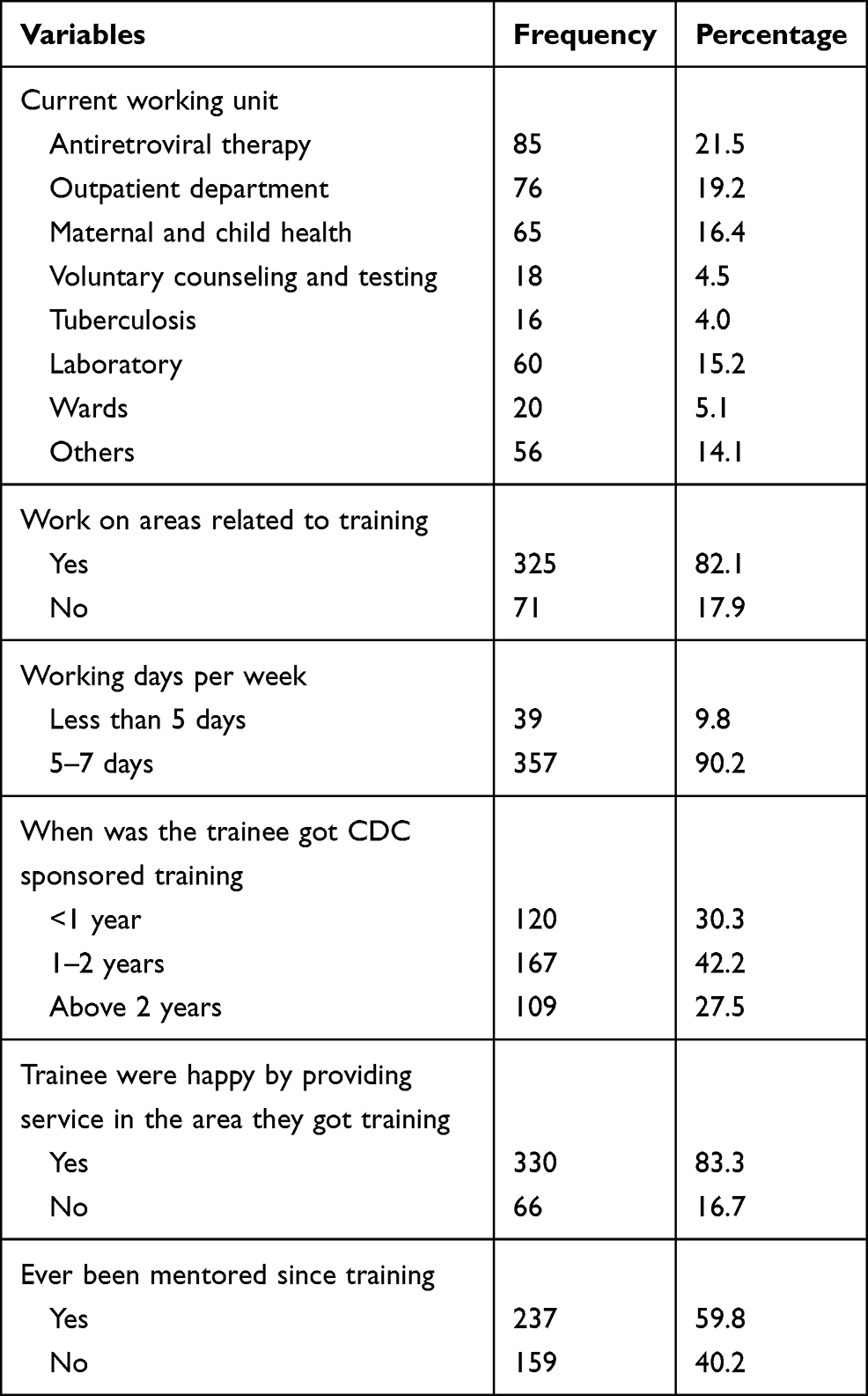 |
Table 2 Service Area-Related Factors of Centers for Disease Control and Prevention Sponsored Training in Five Zones of Southern Ethiopia, October 2019 |
Training-Related Factors
Of 396 participants, (153, 38.6%) were trained at Wolaita Sodo University training center, followed by (140, 35.4%) at Hawassa University training center. Two hundred and ninety-seven (75%) of the participants took only one CDC sponsored training and almost the entire group of trainees (386, 97.5%) were happy about the trainer's quality, as well as the conduciveness of the training environment (368, 92.9%). However, (131, 33.1%) of respondents were not happy in their working environment. Shortage of supply and equipment, space, and trained man power were claimed by (82, 62.6%), (68, 51.9%), and (46, 35.1%) of respondents, respectively. Almost all of respondents (378, 95.5%) recommend the Regional Health Bureau and training University to address untrained health professionals to provide quality service in the health sector (Table 3).
 |
Table 3 Training-Related Factors of Centers for Disease Control and Prevention Sponsored Training in Five Zones of Southern Ethiopia, October 2019 |
Health Facility-Related Findings
Pre-Training Activities
Out of 27 facilities, (25, 92.6%) facilities selected eligible trainees based on criteria set by training organizations as mentioned in an invitation letter before sending them to attend training. Facilities selected non-trained staff using orders given for them, using the lottery method, purposely determining competent and committed health workers from service units to attend the training. However, only (15, 55.6%) facilities have documents and minutes about the number and types of pieces of training taken by trainees in the organization (Table 4).
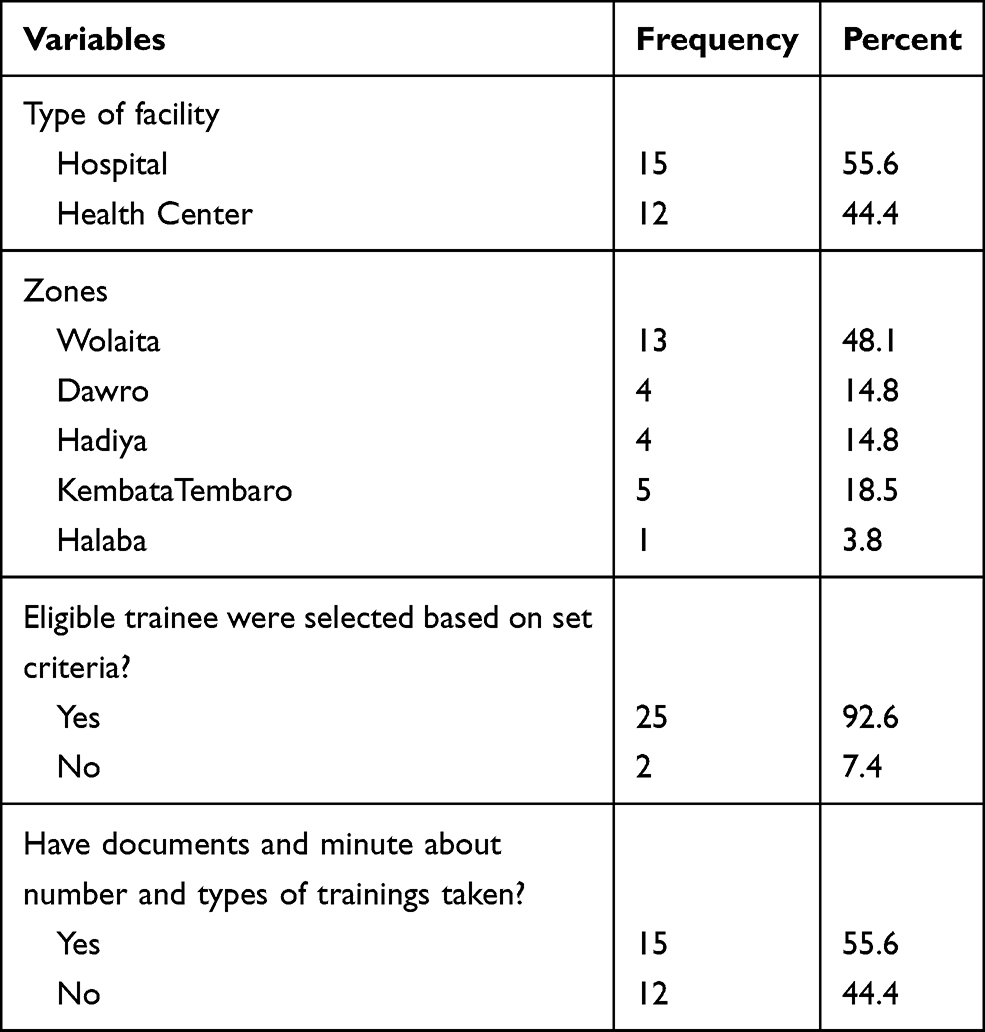 |
Table 4 Pre-Training-Related Factors of Centers for Disease Control and Prevention Sponsored Training in Five Zones of Southern Ethiopia, October 2019 |
Post-Training Activities
About two-thirds of facilities (18, 66.7%) were requesting trainees to put training manuals at the working unit for reference after they got training. However, only (15, 55.6%) of the facilities have training manuals at the working place for reference. For different reasons, three (11.1%) of the facilities assigned trained professionals out of service point where they got training. Trainees from more than half of the facilities (15, 55.6%) has no habit of giving orientation for other non-trained staff after training. Twenty-five (92.6%) facilities have a regular rotation program from one service delivery unit to another service delivery unit within the facility every 3–6 months for staff; however, two (7.4%) facilities did not consider trained staff to stay at the area where they got training. Among the 25 facilities that experienced a rotation program, (23, 85.2%) left trained staff at the service unit where he/she got training without being shifted to another service delivery unit. About half (14, 51.9%) of the facilities responded that they had a signed agreement between the selected trainee and the facility for before sending for pieces of training if the training was more than 1-week duration. However, three of 14 (21.4%) of the facilities have no documented agreement as to how long the trainee was expected to serve the facility (Table 5).
 |
Table 5 Post-Training-Related Factors of Health Facilities in Five Zones of Southern Ethiopia, October 2019 |
Trained Professionals at Service Delivery Unit
Maternal and Child Health (MCH) Unit
A total of 283 health workers are currently working at the MCH unit at 27 health facilities. A total of 63 (22.3%), 27 (9.5%), and 25 (8.8%) individuals took basic PMTCT, PMTCT Refresher, and Early Infant Diagnosis (EID) pieces of training. The numbers who took mother support group training for mentor mothers, mother support group training for site coordinators, PMTCT Mentorship, PMTCT cohort monitoring, and Gender-Based Violence were 13 (4.5%), 12 (4.3%), 11 (3.9%), 20 (7.1%), and 5 (1.8%), respectively.
ART Unit
A total of 91 health workers are currently working at the ART unit at 27 facilities. About 58 (63.7%), 30 (32.9%), 22 (24.2%), and 41 (45.1%) health professionals took essential ART, ART pharmacy, adherence supporter, and Dolutegravir (DTG) rollout training. In addition to that those who took Partner Notification Service/Index Case Testing, mental health for ART providers, and care managers, Psychosocial support and clinical system mentorship were 32 (35.2%), 18 (19.8%), 14 (15.4%), 16 (17.6%), and 23 (25.3%), respectively.
Outpatient Department (OPD), Voluntary Counseling and Testing (VCT), and Tuberculosis Units
Among 278 health professionals working at adult and emergency OPD, 70 (25.2%) individuals took PITC training and only 19 (6.8%) got STI training. From a total of 35 health professionals working in the Voluntary Counseling and Testing (VCT) unit, 20 (57.1%) individuals took HIV Testing Service (HTS) training. On the other hand, from a total of 49 health professionals working on TB units, 28 (57.14%) had TBL training.
Laboratory Unit
A total of 223 health workers were currently working at the laboratory unit at 27 health facilities. Among them, 24 (10.8%) laboratory professionals took ART lab monitoring training and only 14 (6.3%) participants got Dried Blood Sample (DBS) collection training. Regarding Strengthening Laboratory Management towards Accreditation (SLMTA) training, SLMTA I, II, and III training was given for 17 (7.6%), 12 (5.4%), and 15 (6.7%), respectively. Besides that, the number of individuals who got pieces of training on Sample Referral Linkage (SRL), Lab bio-safety, Laboratory Quality Management (LQM), and the New HIV testing algorithm were 28 (12.6%), 24 (10.8%), 34 (15.2%), and 36 (16.1%), respectively.
Cross-Cutting Issue
A total of 13 health workers got monitoring and evaluation-related Data Quality training, and seven participants were trained on continuous quality improvement (CQI) training. Currently, Case-Based Surveillance (CBS) and recency testing were given at each point of service delivery. In that regard, 23 (8.1%) were from the MCH unit and 59 (64.8%) from the ART unit got the training. Moreover, 45 (16.2%), five (14.3%), 10 (20.4%), and seven (3.1%) healthcare providers took case-based surveillance and recency testing training from the outpatient department, voluntary counseling and testing, tuberculosis and laboratory units, respectively.
Discussion
The study addressed 396 participants working in 12 hospitals and 15 health centers providing antiretroviral therapy in southern Ethiopia. Our study revealed that there was low training coverage in the study area to conduct HIV testing for patients who were living with the virus. In this regard, from a total of 313 health professionals, only 105 (33.5%) took training at outpatient department (OPD) and voluntary counseling and testing (VCT) units where HIV testing services were primarily conducted. Moreover, there was a lack of habit by trained staff to provide orientation for non-trained colleagues, a shortage of supply and equipment to conduct HIV tests, and assigning trained staff out of HIV service delivery units were some of the problems seen at facility level not to address all individuals to know their HIV status. This was a great challenge to identify all individuals who were living with HIV so as to enrol them into care and treatment. Therefore, facility heads should address these problems to achieve the global target on HIV testing uptake.
Our study showed that all 91 health professionals working on the HIV care and treatment unit took trainings related to HIV care and treatment. This showed that all care and treatment-related services were given by trained professionals in the study area. This should be maintained to deliver quality service to patients so as to retain them in care and treatment and reduce loss to follow-up once they were enrolled.
As per the national guidelines, all patients enrolled to care and treatment should regularly be monitored to assess the progress of treatment. However, in our study, only 102 (45.7%) laboratory professionals took training related to sample collection, HIV testing service, and viral load monitoring. This could be one of the reasons for low achievement for third 95 of the global target in the study area. Thus, facility heads and training organizations should consider training for laboratory professionals to overcome this problem.
Strength and Limitation of the Study
The study addressed both health centers and hospitals in urban and rural areas providing antiretroviral therapy. It also covered a large geographic area in the region. However, it lacks the analytic component due to the nature of the data study design.
Conclusion
Our study showed that there was low coverage of trained staff to deliver HIV testing service and viral load monitoring. Almost all health facilities have at least one trained staff member working at each service delivery point. However, some of them took training 2 years ago and need refresher training. Mentorship performance after training was not adequate. A gap has been seen on selecting appropriate trainees based on criteria mentioned on an invitation letter and documentation of trained staff profiles in some facilities. There was also a high turnover of trained staff and gaps in knowledge transfer by trained staff to non trained staff by delivering orientation on what has been trained and even sharing training manuals for reference.
Abbreviations
AIDS, acquired immunodeficiency syndrome; ART, antiretroviral therapy; CBS, case-based surveillance; CDC, Centers for Disease Control and Prevention; CQI, continuous quality improvement; HIT, health informatics technician; HIV, human immunodeficiency virus; LQM, laboratory quality management; MCH, maternal and child health; NGO, non-governmental organization; OPD, outpatient department; PITC, Provider Initiated HIV Testing and Counseling; PMTCT, prevention of mother to child transmission; PNS, Partner Notification Service; RHB, Regional Health Bureau; SLMTA, Strengthening Laboratory Management Towards Accreditation; SNNPR, Southern Nations, Nationalities and People Region; SPSS, Statistical Package for the Social Sciences; SRL, sample referral linkage; STI, sexual transmitted infection; TB, Tuberculosis; UNAIDS, United Nations Joint Program on HIV/AIDS; VCT, voluntary counselling and testing; WHO, World Health Organization.
Acknowledgments
The authors would like to acknowledge the Regional Health Bureau for technical support. The authors would also give sincere appreciation to data collectors, supervisors, and participants for their willingness to participate in the study.
Author Contributions
All authors contributed to the data analysis, drafting, or revising of the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. UNAIDS. UNAIDS data 2018; 2018:1–376.
2. UNAIDS. North P. Communities at the Heart? In Urban Renaissance?; 2017:121–138. doi:10.2307/j.ctt1t898kc.12
3. Communications and Global Advocacy UNAIDS. UNAIDS FACT SHEET. Global HIV statistics. End. AIDS epidemic; 2020:1–3.
4. Dimitrov D, Moore JR, Donnell DJ, Boily M. Achieving 95-95-95 may not be enough to end AIDS epidemic in South Africa; 2020:1068617
5. WHO. WHO - Global AIDS Monitoring 2020; 2020.
6. HIV related estimates and projections in Ethiopia for the year-2019 February 2020 Addis Ababa Table of Contents; 2020.
7. National Comprehensive HIV care and Treatment Training for Health Care Providers. Ministry of Health, Ethiopia. February, 2017.
8. Manual, P. National Comprehensive HIV Testing Services Training; (2018).
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.