")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
HIV Voluntary Counseling and Testing Uptake and Associated Factors Among Sexually Active Men in Ethiopia: Analysis of the 2016 Ethiopian Demographic and Health Survey Data
Authors Kabeta T , Belina M , Nigatu M
Received 21 May 2020
Accepted for publication 26 July 2020
Published 13 August 2020 Volume 2020:12 Pages 351—362
DOI https://doi.org/10.2147/HIV.S263851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Teshome Kabeta,1 Merga Belina,2 Mamo Nigatu1
1Jimma University, Institute of Health, Faculty of Public Health, Department of Epidemiology, Jimma, Oromia, Ethiopia; 2Addis Ababa University, College of Natural and Computational Sciences, Department of Statistics, Addis Ababa, Ethiopia
Correspondence: Teshome Kabeta
Jimma University, Institute of Health, Faculty of Public Health, Department of Epidemiology, Jimma, Ethiopia
Tel +251911794169
Email [email protected]
Background: Human immuno-deficiency virus (HIV) counseling affirms that people exercise the right to know their HIV status, which opens the gateway to care, treatment, and support for a person in need. HIV counseling and testing uptake among sexually active males in Ethiopia is too low. Moreover, existing studies were not done at country level and the contributing factors were not well studied. Therefore, the aim of this study is to determine the status of uptake and identify its correlates using the 2016 Ethiopia Demographic and Health Survey.
Methods: Data on 12,688 participants were utilized in this study. Descriptive statistics and multilevel logistic regression were used to summarize the data and investigate the associations between predictors and HIV counseling and testing uptake.
Results: The overall HIV voluntary counseling and testing uptake among sexually active men in Ethiopia was 45.69%; 95% CI [43.08%, 48.33%]. About 13% of the variation in the likelihood of being tested for HIV was due to the variation among the regions. On the other hand, age, religion, education, occupation, marital status, HIV knowledge, health insurance coverage, wealth status, risky sexual behavior, family planning discussion with health workers, owning a mobile, frequency of watching television, and listening to the radio were significantly associated with the uptake of HIV voluntary counseling and testing.
Conclusion: HIV voluntary counseling and testing uptake in Ethiopia is still low and varies across the regions, which might hamper the ambitious plan of Ethiopia to end AIDS as a public health threat by 2030. Therefore, giving due consideration to scale up HIV knowledge to avoid risky sexual behavior, improving access to health insurance and media, and working on the significant modifiable sociodemographic determinants are worthy to boost HIV voluntary counselling and testing uptake, which is an integral component of the strategies to efficiently prevent and control HIV.
Keywords: Ethiopia, risky sexual behavior, sexually active men, voluntary HIV counseling and testing
Background
There is a strong consensus within the global community to end acquired immune deficiency syndrome (AIDS) by 2030.1 Closing the book on the AIDS epidemic is a momentous opportunity to lay a foundation for a healthier and equitable world for future generations, which is impossible without available and accessible human immuno-deficiency virus (HIV) treatment to all who need it.2 HIV voluntary counseling and testing (VCT) creates the gateway to care, treatment, and support for a person in need.3,4 To affirm that people exercise their right to know their HIV status and benefit from antiretroviral treatment (ART), HIV VCT must be radically scaled up.5
All forms of HIV VCT should be voluntary and adhere to the five Cs: consent, confidentiality, counseling, correct test results, and connections to care, treatment and prevention services.6
In 2014, the Joint United Nations Program on HIV/AIDS (UNAIDS) and other partners launched the 90–90–90 target with a three-pronged strategy; diagnosing 90% of all HIV-positive persons, providing ART for 90% of those diagnosed, and achieving viral suppression for 90% of those treated by 2020.2 The 2019 UNAIDS global HIV statistics report on world AIDS day showed that 37.9 million people were living with HIV and 1.7 million were newly infected while 770,000 people died from it at the end of 2018.7 Many people with HIV also remain unaware of their HIV status and start HIV treatment after their immunity is already depleted, resulting in poor prognosis and transmission of the disease to vulnerable individuals due to late HIV VCT.3 According to the 2015 World Health Organization (WHO) estimate, only 54% of people living with HIV know their HIV status.8 HIV VCT uptake in Africa ranges from 10% in Burkina Faso9 to 69.9% in Malawi.10 In Ethiopia, the uptake of HIV VCT is relatively low.4 A time series study done in Ethiopia concluded that Ethiopia will not achieve the first 90% target, without which the control of the epidemic will not be achieved.11 The 2016 Ethiopia Demographic and Health Survey (EDHS) report also showed that 20% of women and 19% of men had been tested for HIV and received the most recent test results.12
According to the 2015 WHO report, less than one-third of adult males receive HIV testing services while more than two-thirds of adult females receive the service, which shows gender disparity in HIV VCT uptake.8 Different studies done in sub-Saharan Africa (SSA) also showed that HIV VCT is relatively lower among males than females.13,14
Different studies also show that age, gender, region of residence, marital status, being covered by health insurance, age at first sex, stigma toward the HIV patient, comprehensive HIV knowledge, discussion about HIV with partner, HIV risky behavior, wealth index, educational status, religion, and distance from the nearest health facility were significantly associated with HIV VCT uptake.9,10,13-17
Although HIV VCT uptake is alarmingly low among males residing in Ethiopia, existing studies were not done at country level and the contributing factors were not well studied. Therefore, the current study objectives were to determine the status of uptake and identify the predictors of HIV VCT among sexually active males in Ethiopia using the nationally representative 2016 EDHS data. Moreover, this study assessed the regional variability of HIV VCT among sexually active males in Ethiopia.
Methods
Data Sources
The 2016 EDHS, the fourth Demographic and Health Survey (DHS), data were collected by the Central Statistical Agency (CSA) of Ethiopia and other stakeholders, and processed and organized by ICF International into different datasets. The authors accessed these public domain datasets from the MEASURE DHS website by permission. Variables related to VCT of HIV were extracted and processed for secondary analysis. Standard protocols and three types of tools were used for collecting DHS data, namely the Household Questionnaire, the Woman’s Questionnaire, and the Man’s Questionnaire. Further standardization and contextualization of the questionnaires were also done by governmental and non-governmental shareholders to maintain the validity of the tools.
Study Population and Sampling Procedures for 2016 EDHS
Ethiopia has been administratively divided into nine regions and two town administrative units. Regions are divided into Zones, and Zones into administrative units known as Weredas. Each Wereda is further subdivided into the lowest administrative units, called Kebele. During the 2007 census, each Kebele was subdivided into census enumeration areas (EAs), which were convenient for the implementation of the census and subsequent surveys.12 The 2016 EDHS followed a two-stage sampling design with stratification into urban and rural. At the first stage of the sampling, 645 EAs, 202 from urban and 443 from rural, were selected on the basis of the 2007 Ethiopian population and housing census sampling frame called EAs. For the Man’s Questionnaire, males aged from 15 to 59 in the selected EAs of the selected households were eligible. The second stage of the sampling involved selection from complete listing of households in each selected EAs by a probability proportionate to the size (PPS) of each cluster. Approximately, 28 households from each cluster (giving a total of 18,008 households), of which 17,067 households were occupied, and 12,688 eligible males were identified and interviewed.12
Measurements
The outcome variable along with all other sociodemographic variables (region, sex, age, religion, wealth status, marital status, occupational status, place of residence, sex of household head, and education level), discussion about family planning with a health worker, coverage status of health insurance, owning a mobile telephone, use of internet, frequency of using internet within a month, frequency of reading a newspaper or magazine in a month, frequency of listening to the radio in a month, frequency of watching television, relationship with most recent sex partner, decisions on personal health care, decisions on large household purchases and decisions on how to spend respondent’s earnings, and respondent’s involvement during check-ups for most recent child were measured by respective direct questions asked of the respondents. The three other explanatory variables, namely risky sexual behavior, stigma status, and knowledge of HIV, were indirectly measured by asking different indicator questions for each of the three variables and scoring and grouping were done to measure the generic variables.
Operational Definitions
HIV-related risky sexual behavior was considered to be practiced by study participants if they either have multiple sexual partners, having more than one sexual partner until the survey, or if they have additional sex partners other than spouse in one year before the interview, or if they fail to use a condom consistently with the three most recent non-spouse or non-girlfriend partners. On the other hand, levels of stigma and HIV knowledge were developed by composite questions to measure each appropriately. The stigma score from seven questions was calculated and then groupings of the scores were performed. The variables from which scoring was done were whether the respondents were ashamed if someone in the family had HIV, buy vegetables from a vendor with HIV, whether attending school together with children living with HIV is right or not, hesitation to take HIV test, afraid of a bad label about people with or believed to have HIV, afraid of loss of respect from other people if positive for HIV, and afraid to get HIV from contact with saliva from an infected person. The scores calculated from these questions range from 0 to 7 and were grouped into four classes. Consequently, score 0 shows no stigma, score from 1–3 shows low stigma, score 4 was considered to be moderate stigma, and score 5–7 as high stigma. By a similar method, “knowledge about HIV” was constructed by combining the responses to nine sets of questions. Scores were computed from questions that ask whether the respondents ever heard about HIV/AIDS, whether the respondent know about reducing risk of getting HIV by always using condoms during sex, whether the respondent know about reducing risk of getting HIV by having one sex partner only, who has no other partners, whether the respondents answered the right answer on transmission of HIV via mosquito bites and by sharing food with a person who has AIDS, whether the respondents know that a healthy-looking person can have HIV, and whether the respondents know that HIV can be transmitted during pregnancy, delivery, and breastfeeding. These nine questions were added together and the minimum sum was 1 and with the maximum of 9. After scoring, grouping of scores were performed to form “HIV knowledge” levels of the respondents. The average score was 7, and scores strictly less than average were categorized to have low “knowledge on HIV” and the respondents with scores 7 and 8 were categorized to have high knowledge on HIV while respondents with score 9 were grouped as those having comprehensive knowledge of VCT HIV.
Other definitions, specific to this paper, were also given. Respondents in the age groups of 15–29 were considered as youths, those in the age group of 30–44 are adults, and those 45–59 were considered as late adults.
Agricultural Workers
Refers to those males who were market-oriented skilled agricultural workers, market-oriented skilled forestry, fishery, and hunting, and agricultural, forestry, and fishery laborers.
Professional Workers
Includes chief executives, senior officials and legislators, administrative and commercial managers, production and specialized services managers, science and engineering professionals, health professionals, teaching professionals, and other professionals.
Trade or Sales Workers
Encloses sales workers, building and related trades workers, excluding electricians, metal, machinery and related traders, handicraft and printing workers, and electrical and electronic traders.
Elementary Occupation
Covers cleaners and helpers, laborers in mining, construction, manufacturing, and transport, food preparation assistants, street and related sales and service workers, and refuse workers and other elementary workers.
Other Workers
Consists of hospitality, retail, and other services managers, general and keyboard clerks, numerical and material recording clerks, and other workers.
Data Analysis
Extraction of relevant variables, data exploration, cleaning, coding, and recoding, generating new important variables, and descriptive and inferential statistics were done using Stata 14.2 statistical software. A multilevel logistic regression model was fitted to assess regional variation of HIV VCT uptake and to identify its determinants. The DHS surveys often follow a hierarchical data structure as the surveys are based on multistage stratified cluster sampling.12 Models used for analysis of this type of data must account for associations among observations within clusters to make efficient and valid inferences.
In the analysis of multilevel regression, the clustering effect plays a great role in estimation of the parameters and this clustering effect can be quantified by intraclass correlation (ICC). ICC is the proportion of total variation in the response variable that is accounted by between-group variation. ICC can also be thought as the correlation among units within the same group.18 In the current study, all predictors are at level 1 and the clustering variable is the region where the subjects were residing.
All the outputs for descriptive analysis were done using weights provided in EDHS 2016 data as per the recommendations by the DHS program. In fact, the way weights are used vary based on the purpose of the analysis. In order to carry out multilevel analysis, the weights from the DHS are adjusted as per the recommendation by Carle.19 Subsequently, we checked the goodness of fit after weighting the dataset by both candidate weights. As expected, the multilevel logistic regression fitted by using the adjusted weights resulted in lower AIC=9162.102 and BIC=9233.47 as compared to the results from unadjusted weights with AIC=10,492.85 and BIC=10,564.22. In addition to the choice of the weights, the principle of parsimony dictates us to go for a model with fewer number of variables in the model. Consequently, significant variables retained in our final model have smaller AIC and BIC, and the results are presented in Table 1.
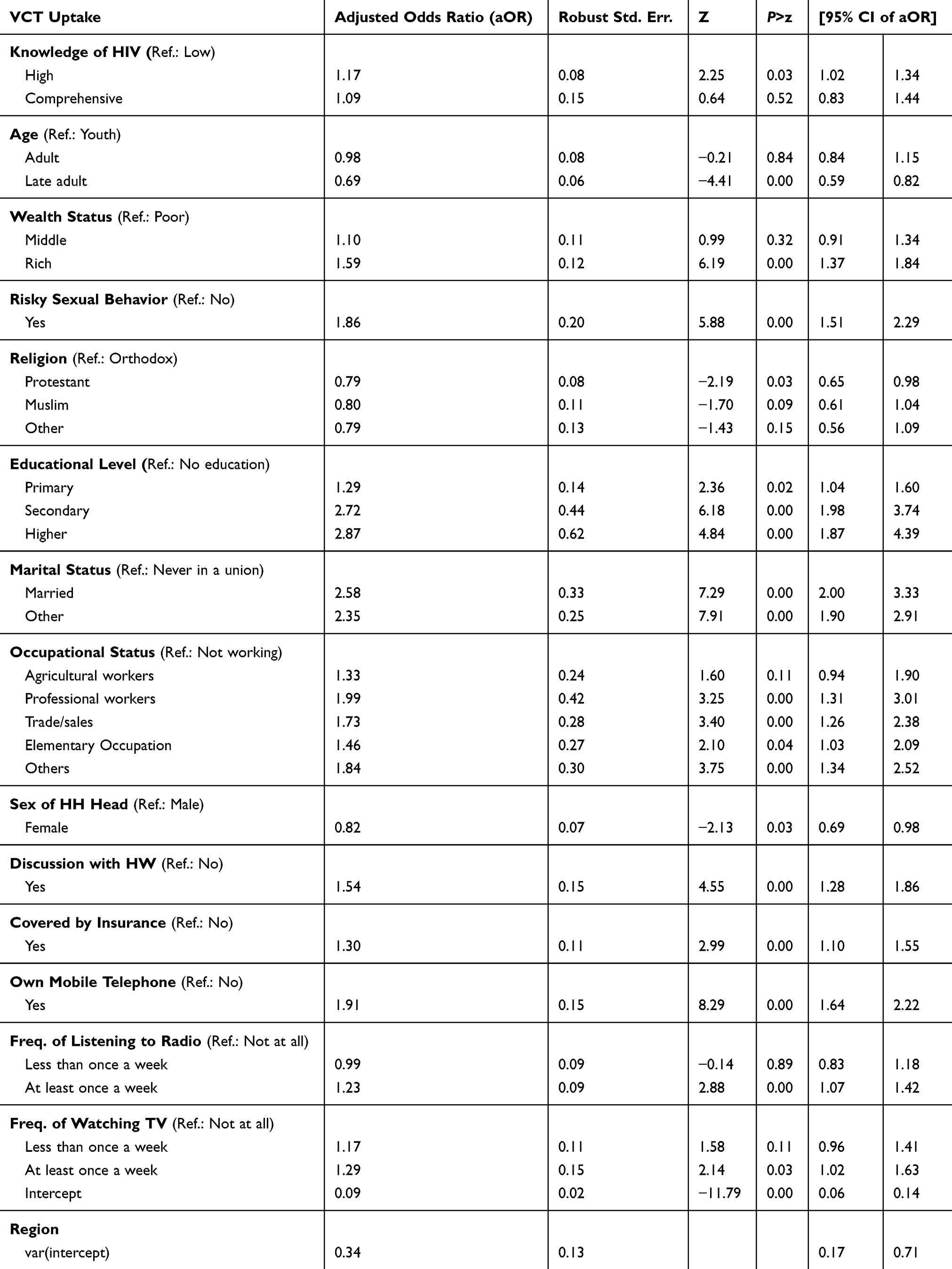 |
Table 1 Results from Multilevel Logistic Regression on Sexually Active Ethiopian Males, 2016 EDHS |
Ethical Consideration
The EDHS 2016 survey protocol, including biomarker collection, was reviewed and approved by the Federal Democratic Republic of Ethiopia Ministry of Science and Technology and the Institutional Review Board of ICF International. Additionally, written consent was obtained from each respondent. For analysis, the investigators received permission from the public domain MEASURE DHS website and reanalyzed the dataset on male respondents.
Results
Characteristics of the Participants
Twelve thousand six hundred and eighty-eight male respondents were included in the analysis of this 2016 EDHS national survey and the mean age (±SD) of the respondents was 30.92 (±0.16) years. About 50.69% of the participants were youths aged from 15 to 29 years. The majority (55.54%) of the participants were married and nearly half of them were in the rich economic status. The dominancy of males was seen by this study, 87.66% of them were from male-headed households. Agriculture is the leading type of occupation, constituting 66.34% of all types of work captured in the survey. The majority (80.29%) of the respondents were rural dwellers (Table 2).
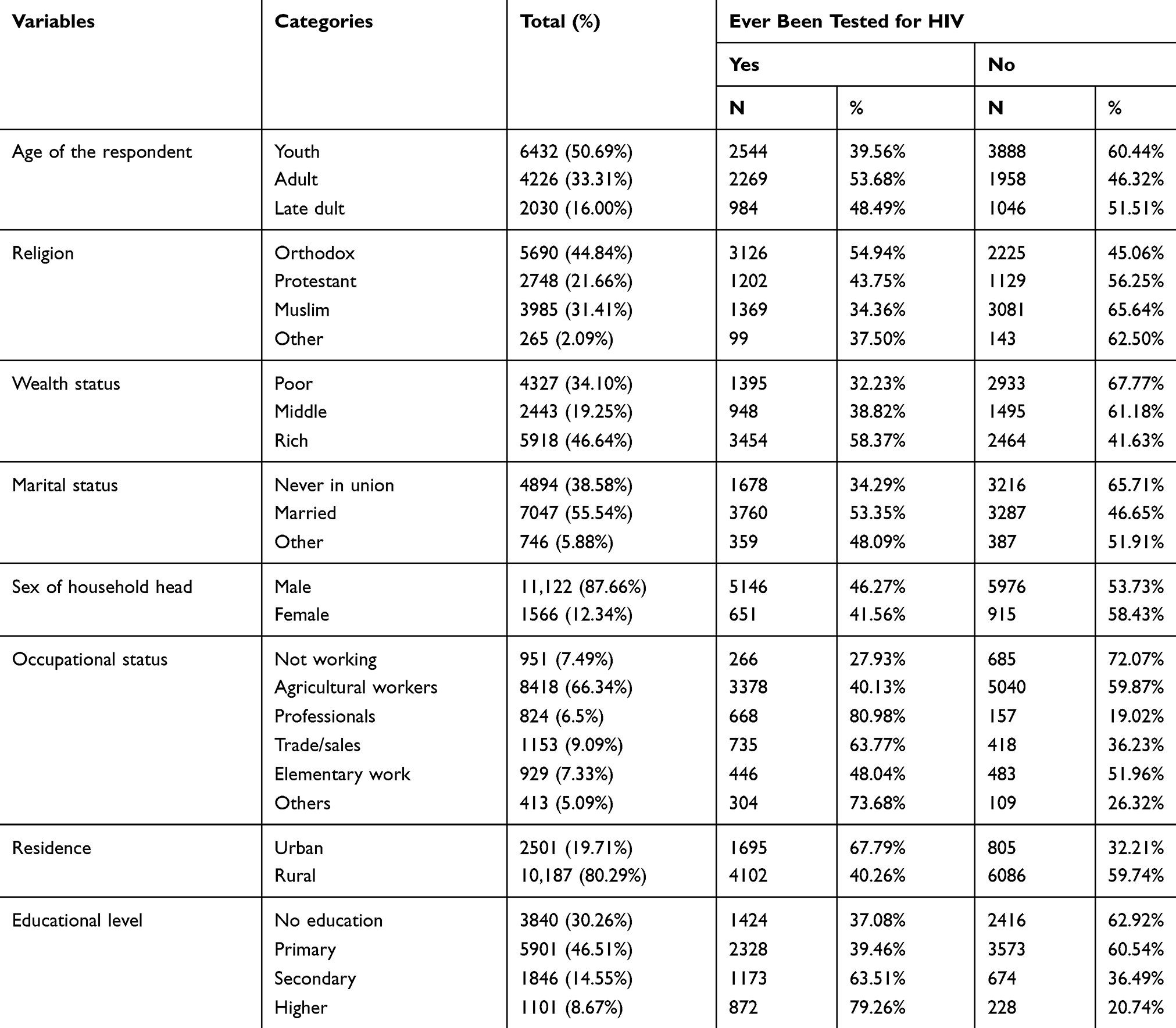 |
Table 2 Sociodemographic Characteristics of Sexually Active Ethiopian Males, EDHS 2016 |
Behavioral and Individual Characteristics of Ethiopian Males, EDHS 2016
In relation to the three indicators, namely about risky sexual behaviors, feeling of stigma about PLWHIV, and knowledge about HIV/AIDS, 40.84% of the participants were showing risky sexual behavior, about 78.4% had high feeling of stigma on PLWHIV, and only 3.83% had comprehensive knowledge about HIV. Whereas about one-third (29.41%) of the interviewed males had low knowledge about HIV. From the total respondents, only one-fourth of them discussed FP with health workers in the last few months before the interview. Regarding health insurance, only 6.53% were covered with health insurance from the total participants. Of all participants, 69.41% and 77.03% of participants were from households where respondents and their wives or their partners were jointly deciding on respondents’ health care and large households’ purchase respectively (Table 3).
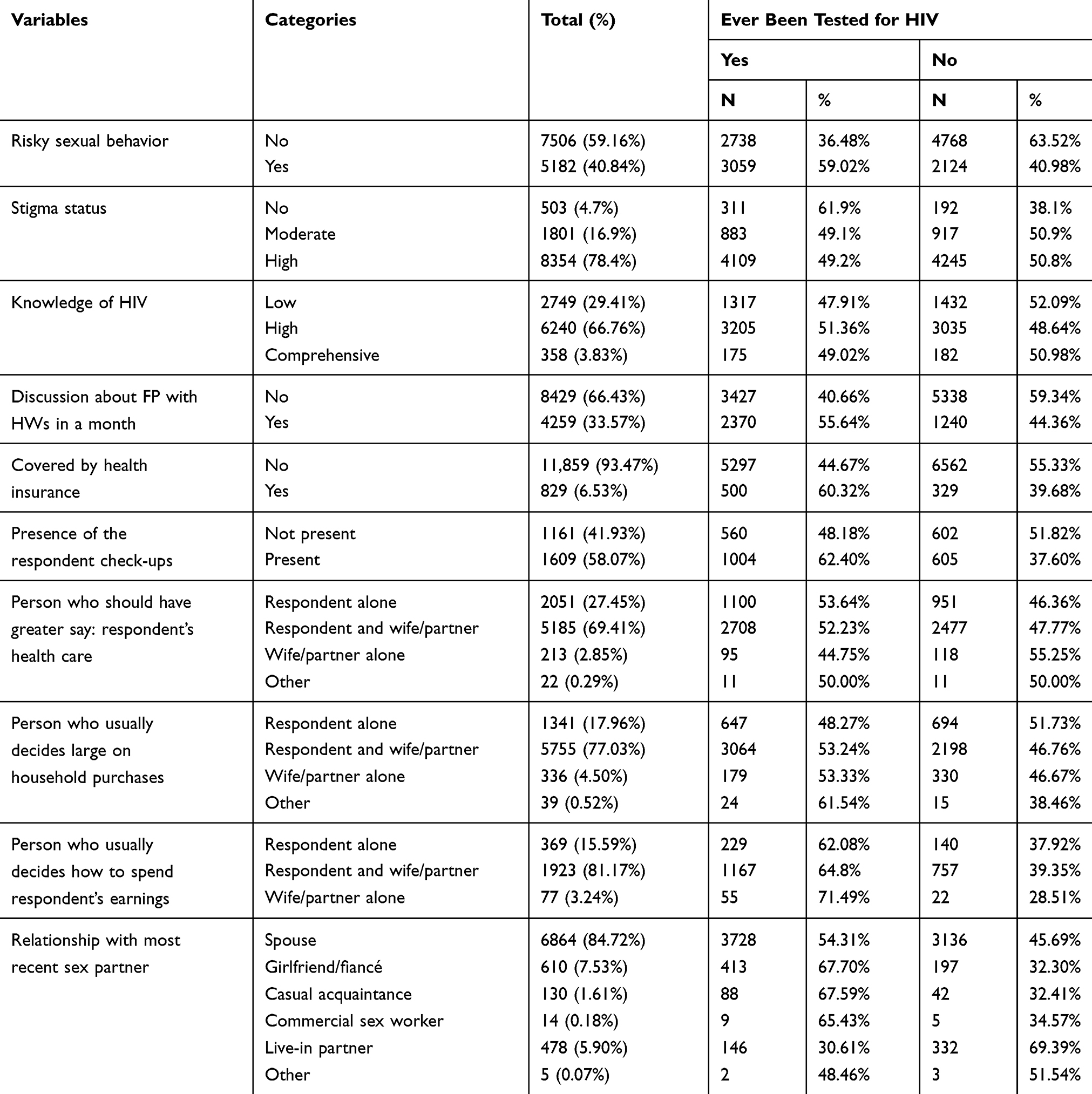 |
Table 3 Behavioral and Individual Characteristics of Sexually Active Ethiopian Males, 2016 EDHS |
HIV VCT Uptake Among Sexually Active Men in Ethiopia, EDHS 2016
The current study revealed that HIV VCT uptake among sexually active men in Ethiopia from the 2016 EDHS was 45.69%; 95% CI [43.08%, 48.33%]. The narrow confidence interval with the range of 5.25 implies that the study yielded quite a precise estimate of HIV VCT uptake among sexually active men in Ethiopia that should have been reported but missed from the 2016 EDHS report. The 2016 EDHS summary report only included descriptive figures for those who were tested and received their results. The distribution of HIV VCT uptake across regions is presented in Figure 1.
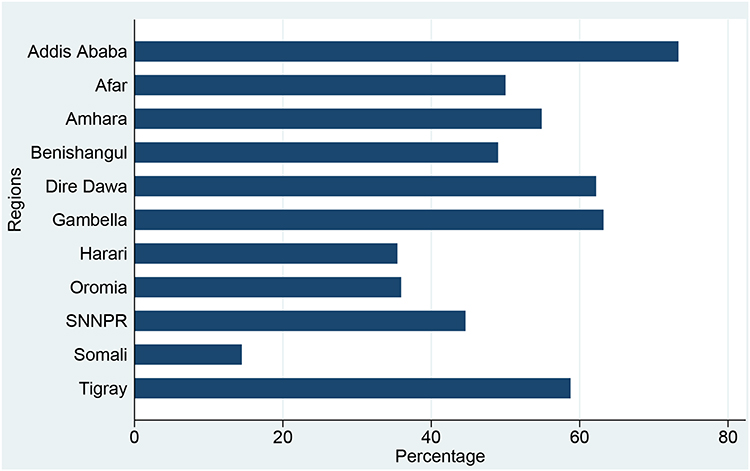 |
Figure 1 HIV VCT uptake among sexually active men by regions in Ethiopia, 2016 EDHS. |
Factors Associated with VCT
The result of ICC with its SD (0.13173±0.06041) shows that about 13% of the variation in the likelihood of being tested for HIV/AIDS was explained by the variation among the regions in Ethiopia. As we can see from the 95% CI [0.05113, 0.29931], the variation among the regions is statistically significant and hence any estimation without considering this effect will result in a biased estimate.
Being in the late adult age group (45–59) was significantly associated with decreased HIV VCT uptake as compared to the youths aged 15–29 (AOR=0.69406; 95% CI [0.59011, 0.81634]). The odds of being tested for HIV among Protestants is AOR=0.79434; 95% CI [0.64669, 0.97571] compared to those who were following Orthodox religion. Attending primary, secondary, and higher education (AOR=1.29468; 95% CI [1.04475, 1.60439], AOR=2.72233; 95% CI [1.98135, 3.74042], and AOR=2.86842; 95% CI [1.87277, 4.39341] respectively) were also significantly associated with the uptake compared with those who never attended school. The odds of being tested for HIV among married and males who were in the other form of union were AOR= 2.57830; 95% CI [1.99872, 3.32595] and AOR=2.35340; 95% CI [1.90368, 2.90937] respectively compared to those who never married. Respondents engaged in professional work (AOR=1.98924; 95% CI [1.31471, 3.00986]), trading or sales (AOR=1.73206; 95% CI [1.26195, 2.3773]), elementary occupation (AOR=1.46256; 95% CI [1.02507, 2.08676]), and other occupation (AOR=1.83561; 95% CI [1.33627, 2.52153]) were significantly associated with outcome variable compared to the not working counterpart. Sex of the household head was also the significant predictor from the sociodemographic variables with AOR=0.82377; 95% CI [0.68918, 0.98465] compared to males from male-headed households.
From the other non-sociodemographic variables, having high knowledge about HIV compared to having low knowledge (AOR=1.169523; 95% CI [1.02009, 1.34085]), the rich compared to the poor (AOR=1.58591; 95% CI [1.37055, 1.83510]), experiencing risky sexual behavior compared to non-experiencing (AOR=1.861432; 95% CI [1.51341, 2.28949]), having discussion with HW about family planning with respect to not having (AOR=1.54497; 95% CI [1.28109, 1.86322]), being covered by health insurance (AOR=1.30135 95% CI [1.09512, 1.54642]), owning a mobile telephone (AOR=1.90564; 95% CI [1.63622, 2.21943]), listening to the radio at least once a week compared to those who do not listen at all (AOR=1.23201; 95% CI [1.06910, 1.41975]), and watching television at least once a week (AOR=1.29040; 95% CI [1.02128, 1.63044]) compared to those who do not watch at all were the significant variables associated with HIV VCT uptake.
Discussion
HIV VCT uptake among sexually active men in Ethiopia was estimated to be 45.69%; 95% CI [43.08%, 48.33%]. The magnitude from our study is greater than many findings from studies done in Burkina Faso, Ethiopia, Cambodia, and South Africa.9,15,20-23 But the current figure is less than the result drawn from the study done in Malawi.10 Most of the studies reviewed clarified that the majority of the figures were less than those of the results obtained by the current study and this may have linkage with the duration when the studies were conducted, meaning that they were mostly done before the year of this study since in the most recent times the VCT for HIV uptake is expected to increase. On the other hand, the uptake of HIV VCT among males was less than that of the females in this study24 although the result obtained for females’ HIV VCT uptake might not be reliable since they did not report whether they applied weighting before doing the analysis, which should be done for DHS data.
In this study, while identifying the factors associated with the uptake of VCT the authors were also interested to see the effect of regional variability on the prevalence of the uptake. In order to account for this effect, ICC among regions was computed and was found to be about 13%, which is a very good reason to consider fitting a multilevel logistic regression model instead of ordinary binary logistic regression. ICC of at least 2% is suggestive of a potential higher-level effect and worth considering a multilevel setup.25
This study uncovered that there is reasonable evidence on knowledge of HIV/AIDS. Compared to those who have low knowledge about HIV/AIDS, males who have high knowledge of HIV/AIDS are more likely to get tested for HIV/AIDS. In fact, regarding males who have high knowledge of HIV/AIDS, the odds of being tested for HIV/AIDS is 17% more than those with no knowledge of HIV/AIDS. This finding is consistent with the results of other studies.16,24,26,27 This could be due to the fact that men who do have comprehensive HIV knowledge may also have better insight on the potential risks associated with the disease, and need to be tested to know their HIV status to prevent themselves from the disease and to prevent the disease’s future sequels.
The odds of accepting HIV VCT for late adult men within the age group of 45–59 was lower by about 30.6% than the youths aged 15–29. This finding is in accordance with the study done in Burkina Faso which reported that males in the young age group were more likely to be tested for HIV.9 The findings from the current study formed evidence that difference in knowledge about HIV across different age groups is the most likely reason for this to happen, since among the males who have comprehensive and high knowledge, 55% and 52% were youths respectively. However, this result is different from the study done in Arusha, Tanzania that discovered the VCT uptake was three times higher among those aged 18 years and above as compared to those below 18 years.15,30 The possibility of the difference can be related to the way age grouping was done; in the current study it is more specific in order to contain those similar populations together than that done in the Tanzania study.
Regarding wealth status, the odds of getting tested for HIV/AIDS for the rich males was 58.6% higher than for the poor. Different studies14–16,20,28 also showed that rich people are more likely to accept HIV VCT as compared to the poor. This could be explained by different reasons. Rich people might have more access to media and have better awareness on HIV than the poor. Similarly, rich men may have better access to a health facility than poor men.
According to these findings, people who exhibit risky sexual behavior are more likely to get tested for HIV/AIDS. Moreover, the odds of getting tested for HIV/AIDS for males who exhibit risky sexual behavior is 86.1% more than males who were not exercising risky sexual behavior. This is concordant with the findings from Cambodia,15 rural Ethiopia,16 and rural Tanzania17 where men with high risky sexual behavior were more likely to accept HIV VCT as compared to those without risky sexual behavior. This could be due to the reason that men who have risky sexual behavior are more apprehensive about their HIV test result than men without risky sexual behavior and are more curious to know their HIV status.
Religion was among the sociodemographic variables significantly associated with HIV VCT uptake. Male Protestant Christians were less likely to accept HIV VCT as compared to Orthodox Christians. The secondary data analysis of the DHS in Zimbabwe also showed that religion was associated with HIV VCT uptake.29 Another studies done in Ethiopia and in South Africa showed that the odds of opting for HIV VCT of male Muslims were 40% and 30% lower compared to Christians, respectively.27,30 But two different studies done in Tanzania showed that Muslims were more likely to opt for HIV VCT than Christians.17,31 The discrepancy could be due to the differences in dogmas of churches and mosques at different geographical locations and cultures.
It is undeniable that education plays a great role in gaining knowledge and has an unpresented contribution in the intention to accept VCT for HIV, and the results in the current study also confirm this idea. For males who attended primary school, the odds of getting tested for HIV/AIDS was higher than those with no education by more than 29.5%; whereas for both of those who attended secondary and higher institutions, the odd increases nearly by three-fold. The secondary data analysis from Zimbabwe showed that the odds of up taking HIV VCT increase as educational level increases.29 Many different studies10,15,16,32 also showed that people with higher educational level were more likely receive HIV VCT than those with lower educational status. Educated people might have better knowledge of HIV than those who are not educated and may better accept HIV VCT than their counterparts. On the other hand, people with higher educational status might not have a feeling of stigma toward PLWHIV and better accept HIV VCT. In contrary to this, the study done in South Africa showed that higher educational status was inversely associated with HIV VCT.30 The discrepancy might be described by differences in integration and mainstreaming of HIV-related education in academic curricula.
According to the results from this study, marital status is found to have a statistically significant association with the VCT for HIV uptake. Compared to those who have never been in union, the odds of uptaking HIV/AIDS VCT for married and other males was higher by more than two-fold for both categories of married status. This finding is concordant with the results of secondary DHS data analyses from Cambodia and Malawi where married men were more likely to opt into HIV VCT uptake as compared to those who were unmarried.10,15 Other studies done in rural Tanzania and South Africa also showed that married men were more likely to opt into HIV VCT as compared to their unmarried counterparts.17,30 This may be due to a feeling of family responsibility among married men compared with those who are unmarried. The other possible explanation for this could be inter-spousal discussion about HIV in order to safeguard their marriage and the health of their future children.
Occupational status of the male subjects was also found to be a statistically significant factor associated with the VCT for HIV uptake. Compared to males who were not working and did not work in last 12 months before the interview, the odds of getting tested for HIV/AIDS for professional workers surpasses by about two-fold; whereas the odds for the males engaged in trade/sales, elementary, and other types of work are on the upper hand by about 73.2%, 46.3%, and 83.6% respectively. The current finding is consistent with the results elicited by studies conducted in Burkina Faso and Soweto, South Africa.21,22 This is reasonably due to the exposure to different workplaces than agriculture being expected to give different level of access to information about VCT services and benefits.
Sex of the household head also matters when it comes to the likelihood of getting tested for HIV/AIDS. The odds of getting tested for HIV/AIDS for males residing in the households where females are the head is lower by about 17.6% compared to males residing in the male-headed households.
Nowadays, the government of Ethiopia is trying to implement health insurance in the country although its coverage is at its infant stage. This study identified that the health insurance coverage status for Ethiopian males was found statistically significant, in that males covered by health insurance were more likely to be tested than those who were not covered. This result is in line with the recent finding on the DHS from Malawi.10 The result seems to be reasonable as people with health insurance covered are very likely to visit health facilities to get health services, because they do not worry about the cost of the services as the insurance is expected to cover.
Contact with health workers, specifically discussion about family planning with health workers, was significantly associated with the chance of getting tested for HIV/AIDS. In addition, the odds of getting tested for HIV/AIDS for males who had the chance to discuss family planning with the health workers is higher by about 55%. This result supports the existing finding pointed out by the study conducted in rural Ethiopia.16 Contacting HWs and discussing about family planning usually paves the way to discuss HIV/AIDS VCT and that perhaps made a difference in uptaking of VCT.
It is not uncommon to see the effect of access to media on the likelihood of getting tested for HIV/AIDS and the current result reaffirms the same. More specifically, the effect of access to a mobile telephone is found to be statistically significant. For mobile telephone users, the odds of getting tested for HIV/AIDS was higher by 91% compared to the non-users. Moreover, the odds of getting tested for HIV/AIDS for males who were listening to the radio at least once a week, compared to non-listeners, is higher by about 23.2%. Whereas the odds of getting tested for HIV/AIDS for males who watch TV at least once a week surpasses that of males who do not watch TV at all by about 29%. This result is similar to the findings from Zimbabwe and Burkina Faso where exposure to media was positively associated with HIV VCT uptake.21,29 Evidence from analysis of the 2016 Uganda DHS showed that listening to the radio once a week and watching television more than once a week increases the odds of being tested for HIV by 4.57% and 8.57% respectively.33 Another study in SSA using three rounds of DHS also presented that there is a significant relationship between exposure to mass media and HIV VCT uptake.34 The same study also suggested that continuous and proactive media movements may lead to diffusion of ideas that may ultimately promote HIV testing. Evidence from analysis of the 2016 Uganda DHS and results from the longitudinal analysis conducted in India also showed that exposure to mass media was significantly associated with HIV-related knowledge,33,35 and, from the current study, it is evident that HIV-related knowledge is strongly associated with HIV VCT uptake.
Strength of the Study
The sampling methods used to reach the study participants, the methods of data collection, the interviewing techniques applied, the data processing, management, and organization are to the standard and the quality of DHS data is unquestionably the most reliable kind of data. The number of study participants was also sufficiently large and selected from every corner of the country to ensure national representation of the Ethiopian population. The authors have used both descriptive and inferential analyses by weighting the data prior to doing analyses of any kind to reduce the anticipated bias due to clustering. Moreover, multilevel modeling was also applied to account for the variation of VCT uptake across the regions in Ethiopia.
Limitation of the Study
Since the study used data from a single time survey, the temporality between HIV VCT uptake and aforementioned factors cannot be ascertained and the evidence should be utilized with care. Besides, because of the lack of qualitative data on the EDHS, the authors were unable to investigate the association between some qualitative variables like sociocultural factors and HIV VCT uptake. On the other hand, some pertinent variables like distance from the nearest health facility which were significantly associated with HIV VCT uptake from other literature and could have an effect in the current study are missing from the EDHS.
Conclusions
HIV VCT among sexually active men in Ethiopia is still unacceptably too low although it is higher than the uptake in some African countries. This study disclosed the presence of significant disparities in the uptake of HIV VCT among sexually active men residing in different regions of Ethiopia, with the lowest uptake of 14.45% in Somali region and the highest uptake of 73.30% in Addis Ababa. Ethiopia has committed to ending AIDS as a public health threat by 2030. But achieving this goal without scaling up the current HIV VCT uptake among sexually active men in the country is unlikely. Therefore, any stakeholder working on HIV/AIDS prevention and control should implement region-specific interventions to scale up HIV knowledge, which in turn helps to avoid risky sexual behavior, improving access to health insurance and media, and working on the significant modifiable sociodemographic determinants for better success of the uptake. Future researchers interested in the area should also address qualitative variables like sociocultural factors, which might have a tremendous effect on HIV VCT uptake among sexually active men in the country.
Abbreviations
AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; AIDS, acquired immuno-deficiency syndrome; aOR, adjusted odds ratio; ART, anti-retroviral therapy; CI, confidence interval; EA, enumeration area; EDHS, Ethiopian Demographic and Health Survey; FP, family planning; HAPCO, Federal HIV/AIDS Prevention and Control Office; HIV, human immuno-deficiency virus; HW, health worker; ICC, intraclass correlation; OR, odds ratio; PLWHIV, people living with HIV; PPS, probability proportionate to size; SD, standard deviation; TV, television; UNAIDS, United Nations Program on HIV/AIDS; VCT, voluntary counseling and testing; WHO, World Health Organization.
Acknowledgments
The authors would like to extend our gratitude to different workforces participated in the 2016 Ethiopian Demographic and Health Survey and who allowed us to access the datasets from the MEASURE DHS website.
Disclosure
The authors have declared that there is no competing interest.
References
1. UNAIDS I. Voluntary Confidential Counselling and HIV Testing for Workers. Geneva; 2016.
2. UNAIDS. 90-90-90an Ambitious Treatment Target to Help End the AIDS Epidemic. Geneva; 2014.
3. WHO. HIV Testing and Counselling; Consolidated ARV Guidelines, June2013. Geneva; 2013.
4. HAPCO. Guidelines for HIV Counselling and Testing in Ethiopia. Addis Ababa; 2007.
5. WHO. HIV Testing and Counselling: The Gateway to Treatment, Care and Support. Geneva; 2003.
6. WHO. HIV Testing and Counselling: Guiding Principles. Geneva; 2013.
7. UNAIDS. Global Hiv Statistics. Geneva; 2019.
8. Who. Fact Sheet to the Who Consolidated Guidelines on Hiv Testing Services. Geneva; 2015.
9. De Allegri M, Agier I, Tiendrebeogo J, Louis VR. Factors affecting the uptake of HIV testing among men: a mixed-methods study in rural Burkina Faso. PLoS One. 2015;10(7):1–15. doi:10.1371/journal.pone.0130216
10. Mandiwa C, Namondwe B. Uptake and correlates of HIV testing among men in Malawi: evidence from a national population – based household survey. BMC Health Serv Res. 2019;3:1–8.
11. Girum T, Wasie A, Worku A. Trend of HIV/AIDS for the last 26 years and predicting achievement of the 90 – 90-90 HIV prevention targets by 2020 in Ethiopia: a time series analysis. BMC Infect Dis. 2020;18(3):1–10.
12. ICF CSA (CSA) [Ethiopia] and. Ethiopia. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
13. Gebregziabher M, Dai L, Vrana-diaz C, Teklehaimanot A, Sweat M. Gender disparities in receipt of HIV testing results in six sub-saharan African countries. Heal Equity. 2018;2(1).
14. Ha JH, Van LLM, Mallalieu EC, et al. Gendered relationship between HIV stigma and HIV testing among men and women in Mozambique: a cross- sectional study to inform a stigma reduction and male-targeted HIV testing intervention. BMJ Open. 2020:1–10.
15. Narin P, Id EY, Saw YM, Net N, Inthaphatha S. Factors associated with HIV testing among the general male population in Cambodia: a secondary data analysis of the demographic health survey in 2005, 2010, and 2014. PloS One. 2019:1–16.
16. Teklehaimanot HD, Teklehaimanot A, Yohannes M, Biratu D. Factors influencing the uptake of voluntary HIV counseling and testing in rural Ethiopia: a cross sectional study. BMC Public Health. 2016;14:1–13. doi:10.1186/s12889-016-2918-z
17. Wringe A, Isingo R, Urassa M, et al. Uptake of HIV voluntary counselling and testing services in rural Tanzania: implications for effective HIV prevention and equitable access to treatment. Trop Med Int Health. 2008;13(3):319–327. doi:10.1111/j.1365-3156.2008.02005.x
18. GELMAN A JENNIFERHILL. Data Analysis Using Regression and Multilevel/Hierarchical Models.
19. Carle AC. Fitting multilevel models in complex survey data with design weights: recommendations. BMC Med Res Methodol. 2009;9(1):1–13. doi:10.1186/1471-2288-9-49
20. Gazimbi MM, Magadi MA. A multilevel analysis of the determinants of HIV testing in zimbabwe: evidence from the demographic and health surveys. J AIDS HIV Res Treat. 2015;4(1).
21. Kirakoya-samadoulougou F, Jean K, Maheu-giroux M. Uptake of HIV testing in Burkina Faso: an assessment of individual and community- level determinants. BMC Public Health. 2017:1–11.
22. Mhlongo S, Dietrich J, Otwombe KN, Robertson G, Coates TJ, Gray G. Factors associated with not testing for HIV and consistent condom use among men in Soweto, South Africa. PLoS One. 2013;8(5):e62637. doi:10.1371/journal.pone.0062637
23. Bwambale FM, Ssali SN, Byaruhanga S, Kalyango JN, Karamagi CAS. Voluntary HIV counselling and testing among men in rural western Uganda: implications for HIV prevention. BMC Public Health. 2008;8(1):1–12. doi:10.1186/1471-2458-8-263
24. Erena AN, Shen G, Lei P. Factors affecting HIV counselling and testing among Ethiopian women aged 15 –49. BMC Infect Dis. 2020;19(2019):1–12.
25. Fessler MB, Rudel LL, Brown M. Impact of small group size on neighborhood influences in multilevel models. J Epidemiol Community Health. 2008;23(1):1–7.
26. Godif M, Assefa H, Alemayehu M, Terefe W. Factors associated with HIV counseling and testing among males and females in Ethiopia: evidence from ethiopian demographic and health survey data. J AIDS Clin Res. 2015;6(3). doi:10.4172/2155-6113.1000429
27. Leta TH, Sandøy IF, Fylkesnes K. Factors affecting voluntary HIV counselling and testing among men in Ethiopia: a cross-sectional survey. BMC Public Health. 2012;12:1–12.
28. Jimoh AAG, Balogun OR. Factors hindering acceptance of HIV/AIDS voluntary counseling and testing (VCT) among youth in Kwara State, Nigeria. Afr J Reprod Health. 2010;14(3):159–164.
29. Sambisa W. DHS WORKING PAPERS AIDS Stigma and Uptake of HIV Testing in Zimbabwe. Geneva; 2008.
30. Baisley K, Doyle AM, Changalucha J, et al. Uptake of voluntary counselling and testing among young people participating in an HIV prevention trial: comparison of opt-out and opt-in strategies. PLoS One. 2012;7(7):1–10. doi:10.1371/journal.pone.0042108
31. Sanga Z, Kapanda G, Msuya S, Mwangi R. Factors influencing the uptake of voluntary HIV counseling and testing among secondary school students in Arusha City, Tanzania: a cross sectional study. BMC Public Health. 2015;15(452):1–9.
32. Conserve D, Sevilla L, Mbwambo J, King G. Determinants of previous HIV testing and knowledge of partner ’ s HIV status among men attending a voluntary counseling and testing clinic in Dar es Salaam, Tanzania. Am J Men’s Health. 2012;7(6):1–11.
33. Lompo ML, Bago J-L. How does exposure to mass media affect HIV testing and HIV-related knowledge among adolescents? Evidence from Uganda. Glob J Health Sci. 2018;10(9):1. doi:10.5539/gjhs.v10n9p1
34. Somefun OD, Wandera SO, Odimegwu C. Media exposure and HIV testing among youth in Sub-Saharan Africa: evidence from demographic and health surveys (DHS). Reprod Health Sub Sahara Afr. 2019;1–13.
35. Sood S, Shefner-Rogers CL, Sengupta M. The impact of a mass media campaign on HIV/AIDS knowledge and behavior change in north India: results from a longitudinal study. Asian J Commun. 2006;16(3):231–250. doi:10.1080/01292980600857740
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.