")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
HIV Positive Status Disclosure and Its Associated Factors Among Children on Antiretroviral Therapy in West Shoa Zone, Western Ethiopia, 2019: A Mixed Method Cross-Sectional Study
Received 19 April 2020
Accepted for publication 5 June 2020
Published 16 June 2020 Volume 2020:13 Pages 507—517
DOI https://doi.org/10.2147/JMDH.S258851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Seifadin Ahmed Shallo,1 Mesfin Tassew2
1Department of Public Health, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 2Department of Pediatrics and Child Health, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia
Correspondence: Seifadin Ahmed Shallo
Department of Public Health, College of Medicine and Health Sciences, Ambo University, P.o.box-19, Ambo, Ethiopia
Tel +251 910768226
Email [email protected]
Background: Evidence from previous studies supports the idea that informing children about their HIV status has long-term positive implications in HIV disease management, children’s quality of life, and ART drug adherence. However, in sub-Saharan African Countries, the HIV status disclosure among children ranges from 0% to 69.2%. So it is important to investigate the up to date evidence that will help in designing contextualized approaches for disclosure. Therefore, this study aimed to assess the HIV status disclosure and its associated factors among children on ART in West Shoa Zone, Ethiopia.
Materials and Methods: Institutional-based observational study was conducted from February to April 2019. Quantitative data were collected from a randomly selected sample of 247 HIV positive children on ART for the last six months, and the qualitative data were collected from caregivers and health care professionals.
Results: The mean age of the children was 11.11±SD2.8, and 43.6%, (95% CI: 37, 50.9) of the children were fully disclosed. The average age at disclosure was 11±SD2.12. The main reasons for the disclosure were for drug adherence and better self-care while being underage was the commonest reason for non-disclosure. Compared to the age 10– 15 years, the child in the age 6– 9 was 97% [AOR: 0.027, 95% CI: 0.003, 0.22, P< 0.001] less likely to be disclosed. Female children were 2.7 times more likely to be disclosed compared with male children [AOR: 2.73, 95% CI: 1.24, 6, P< 0.013].
Conclusion: This finding reveals that HIV status disclosure is generally low, and the decision to disclose or not is affected by factors like child-related, caregivers, and health institution-related factors. This may affect the child’s drug adherence, treatment outcome, and disease transmission. Updating health care providers’ knowledge and skills and working on caregivers’ attitude are needed to manage disclosure and challenges following it.
Keywords: disclosure, children, West Shoa
Introduction
Globally, it was estimated that 38.8 million (95% CI 36.7–40.4) people were living with HIV/AIDS by 2015. Of these, more than 66.2% (above 25.7 million) were from Africa, and Children of age less than 15 years contributed about 2.1 million out of the total HIV infected population.1,2
In Ethiopia, nearly 710, 000 people were living with HIV, of which 62,000 were children of less than 15 years of age. Of these, only 35% of them were on antiretroviral treatment (ART) by 2016.3
Notifying children about their HIV status is advantageous in the long-term management of HIV infection.4 Studies indicate that if children living with HIV know about their HIV status, they are more likely to adhere to ART and this has a positive influence on the children’s quality of life.5
It is also the children’s right to get information about their health status. Because of this, the World Health Organization (WHO) recommends that children of school age should be told their HIV positive status and their parents’ HIV positive status; younger children should be told their status and their parents’ status incrementally to accommodate their cognitive skills and emotional maturity, in preparation for full disclosure. Therefore, it is recommended to start HIV disclosure at the age of 6 and continued in incremental approach up to 12 years so that at the age of 12 the child should fully know his/her status.6,7 For instance, a case-control study conducted among 309 HIV positive children indicated that quality of life was comparatively high among children with HIV status disclosed compared to those without HIV status disclosure.5
Although studies claim that informing children about their HIV status has long-term positive implications in HIV disease management, children’s quality of life, and ART drug adherence. In many parts of the sub-Saharan African Countries, the HIV status disclosure reaches from 0 to 69.2%.8 For instance, the HIV status disclosure reaches 26% to 33% in Kenya,9 32.6% in Uganda,10 22.3% in Tanzania,11 40% in South Africa,12 with the age at disclose ranging from 5 to 15 years.13 In the Democratic Republic of Congo, nearly 50% of children did not know their status while 15% partially informed. The full disclosure only reached 3%.14 In a cross-sectional study among 149 caregivers of 4–17 years old children in South African indicated that only 39.6% with the median age of discloser of 9.3 years, in Ghana only 15 out of 71 of the caregivers disclosed the HIV status of their children to the child.15
One study conducted in North Gondar, Northern Ethiopia revealed that only 39.5% of the children were disclosed.16 In another study conducted among 177 participants in Hawassa, Southern Ethiopia, the prevalence of the disclosure was 33%.4 Most parents or caregivers of HIV positive children do agree that the status of the child should be disclosed to the child. However, evidence from different studies indicates that a minority of HIV-infected children in resource-limited settings knew his/her HIV status, reaching from 0–69%.17
This evidence supports the fact that a significant number of caregivers/parents lack skills or sufficient knowledge of when and how to disclose the child’s status.6 And most of the children’s parents prefer disclosure by a health professional than themselves. However, due to a lack of clear guidelines on the roles and responsibility of health care providers and standardized training in pediatric HIV disclosure, confusion was noted among health professionals in the process of disclosure.18 The inability of most caregivers to handle disclosure has demonstrated three main patterns of disclosure: complete parental; partial; and non-disclosure. In complete disclosure, the child is told that he/she has HIV and is given disease-specific information; while, in partial disclosure, the child may know that he/she has an illness but he/she has not told specifically that he/she has HIV infection.15 Evidence from a systematic review indicated that the prevalence of HIV status disclosure in resource-limited countries was generally low among both children and adolescents and for different reasons. The age of the child, fear of stigma in the community if disclosed, whether the child asks about his/her status, and caregivers’ perception about the child’s ability to understand about the meaning of HIV if disclosed were common reasons mentioned by parents or caregivers as a reason for not disclosing the status for their children. Additionally, the parents’/caregivers’ skill gap on how to disclose is also other factors for not disclosing.4,12 Many parents prefer the age at disclosure to be above 10 and if the child’s age is 10 and above he/she has 80% more likely to be informed about his/her status (AOR: 8.8, 95% (CI: 4.7, 16.5)4.5, 16.5).15,19 In the same study, the main reason for disclosing the child status was that the children were not adhering to the ART.12
Materials and Methods
Study Area
This study was conducted in Health Facilities found in West Shoa Zone, Oromia Regional State, Ethiopia. There were eight hospitals and 92 Health centers in west Shoa Zone. Out of these, 24 sites (health centers and Hospitals) were delivering ART services for patients with HIV. According to the data obtained from the CDC branch of the West Shoa Zone Health Department, there were 9156 HIV positive patients on ART. Out of these, children between 6–15 years numbered 556. The number of children who fulfilled the inclusion criteria in each ART site ranged from 1 to 218 (West Shoa Health Department, 2018).
Study Design and Period
The institutional-based cross-sectional study design was used. The study was conducted from February 15- April 15/2019. Study population
By considering the WHO recommendation for the lowest age at which disclosure should be initiated, all HIV positive children age between 6 and 15 on ART for the last six months at the selected hospital or Health centers (Ambo General Hospital, Incini Health Center, Ginchi H/C, Holota H/C) were included in the study.
Inclusion Criteria
All children aged between 6 and 15, and on ART for at least 6 months were included.
Sample Size Determination
To calculate the sample size for this study the following assumptions were considered: The sample size for the first objective was calculated using the prevalence of HIV status disclosure (P=33%) among children in southern Ethiopia,17 95% CI, and 0.05 degree of precision. Accordingly, the sample size was 339.
The Sample Size for the Second Objective
The sample size for the second objective was calculated as follows: for the power of the study to be 80%, the ratio of exposed to unexposed to be 1:1, 95% CI, % of outcome among exposed and unexposed were taken into account. Accordingly, the sample size was calculated using open Epi info version TM7 computer software as 442 (Table 1).
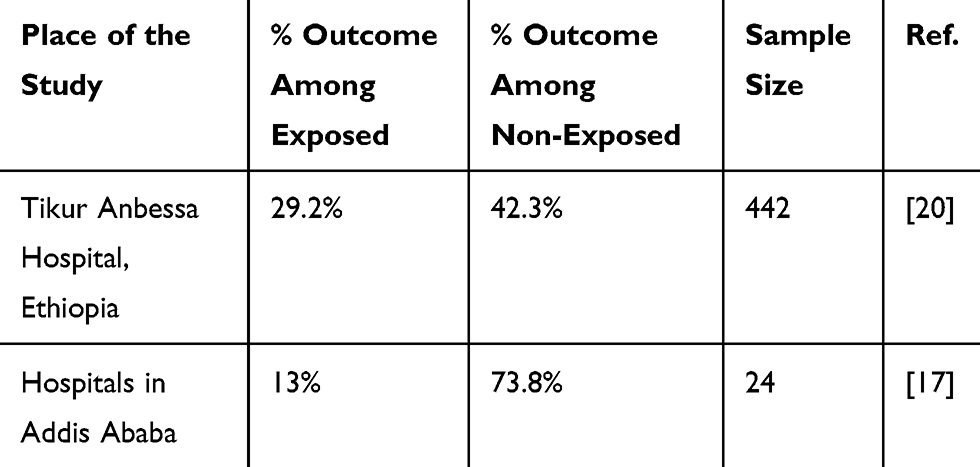 |
Table 1 Sample Size Calculation Using Different Works of Literature as a Baseline for Study on HIV Status Disclosure and Associated Factors Among Children on ART in West Shoa Zone, Ethiopia |
But, since the total study population was 556 (less than 10,000); the population correction formula was applied, and the final sample size was 247.
Sampling Procedure
Since some health centers had only one case who fulfilled the inclusion criteria, we decided to include all health centers with at least 20 and above cases. Accordingly, we selected four health institutions. The study participants who fulfilled the inclusion criteria were selected by simple random sampling technique. The sample for a qualitative study was selected purposively.
Data Collection Tools
Both open-ended and close-ended questionnaire was developed after reviewing related works of literature and some of the questionnaires were adopted from previous similar studies and contextualized accordingly. The questionnaire contains child socio-demographic characteristics and HIV related questions, caregivers’ sociodemographic characteristics and HIV related questions, and disclosure related issues. Some of the child HIV related data were extracted from the child’s card. For the qualitative data collection, open-ended questions grouped under different themes were developed.
Sampling Techniques and Data Collection Procedures
Quantitative data were collected through a face-to-face interview. Data were collected from the child’s caregivers, or the child alone or both. First, we asked the child’s caregiver whether the child knows his/her status. In case the caregiver reported the child knows his/her HIV status, we verified from the child based on the caregivers’ consent. Some of the children who knew their status came alone to the health institution. In such cases, the data were collected directly from the child themselves. For data collection, five-degree holder nurses (one for each health institution except for Ambo Hospital where it was two) were recruited, and trained for two days on the objectives of the study, how to conduct clients interview, and on how to take the consent from the caregivers or parents. Nine in-depth interviews (IDI) (four with health care providers and five with child caregivers) were conducted. The participants for IDI were purposively selected health care providers working on ART clinics from all health institutions and child caregivers, whose child’s HIV status had been disclosed.
Operational Definitions
Full disclosure: Disclosure was considered as “full disclosure” when it involved the caregiver or health care providers or anyone else having disclosed to the child that he or she has HIV specifically. This was determined if the caregivers claimed that he/she describes the term HIV in his/her explanation for the child during the disclosure process.
Partial disclosure: Disclosure is considered “partial” when the illness is described in a way that is consistent with HIV although the term “HIV” is avoided. For insistence: when the child is informed/knows that he/she has chronic health problems but not told specifically that the disease is HIV.
No disclosure: When the caregiver reported telling the child nothing about his or her illness.
Deflected disclosure: The strategy of deceptive disclosure that caregivers often use, frequently out of concern for the child’s psychological well-being, telling their children only about an unrelated condition (eg, asthma, cancer), and attributing all medical needs (eg, appointments, medication) to that less-stigmatized condition.21
Data Management and Analysis
The in-depth interview was tape-recorded and transcribed. The qualitative data were analyzed through a thematic analysis. The patterns of experiences were derived from the transcripts, either from direct quotes or through paraphrasing common ideas. Data from all the transcripts relating to the classified patterns were identified and placed under the relevant theme where it complemented the quantitative findings.
This study is reported in compliance with the STROBE guidelines.26
Ethical Considerations
The study was done in accordance with the Declaration of Helsinki, and ethical clearance was obtained from the ethical review committee of the College of Medicine and Health Sciences, Ambo University, Ethiopia. The supportive letter and clearance letter were communicated to each Hospital and Health Centers, where the study was conducted. Then, permission to proceed was assured by the hospitals’ and health centers’ managers. During the fieldwork, the objectives of the study were clearly explained for the study participants, the confidentiality of the data to be collected and the right not to participate was also assured. The written consent was taken from the caregivers after they read/the consent form was read for them. The participants were asked to confirm their participation in the study by signing the consent form.
Availability of Data and Supportive Materials
All data generated or analyzed during this study were included in this published article and its supplementary information files (data collection tools) are also included as Figure S1 with this submission. In addition, further data can also be obtained from the corresponding author on a formal request.
Results
Socio-Demographic Characteristics of the Children and Their Caregivers
A total of 236 participants were interviewed. Out of the interviewed participants, 129 (54.7%) were the child’s caregivers, 61 (25.8%) were both caregivers and children, and 46 (19.5%) were only children. One hundred thirty-five (57.2%) of the caregivers were biological mothers. More than half (53%) of the children were males, and most of the children (95%) had started their education which reaches from the level of the nursery to junior primary school. The mean age of the children was 11.11±SD2.8. Most (73.2%) of the children were aged between 10 and 15. Eighty-three (35.2%) of the children were the first child for the family. Nearly 2/3 of the children were from urban residency. Thirty-eight (10.2%) of the children were orphaned ie lost either their mothers or fathers or both. Out of them, 24 (10.2%) lost their fathers and mothers, 10 (4.2%) lost their mothers and 4 (1.7%) lost their fathers. One hundred twenty-five (53%) of the caregivers were in union (married), and 71 (30.1%) could not read and write. The caregivers’ mean age was 36.4±8.2 (Table 2).
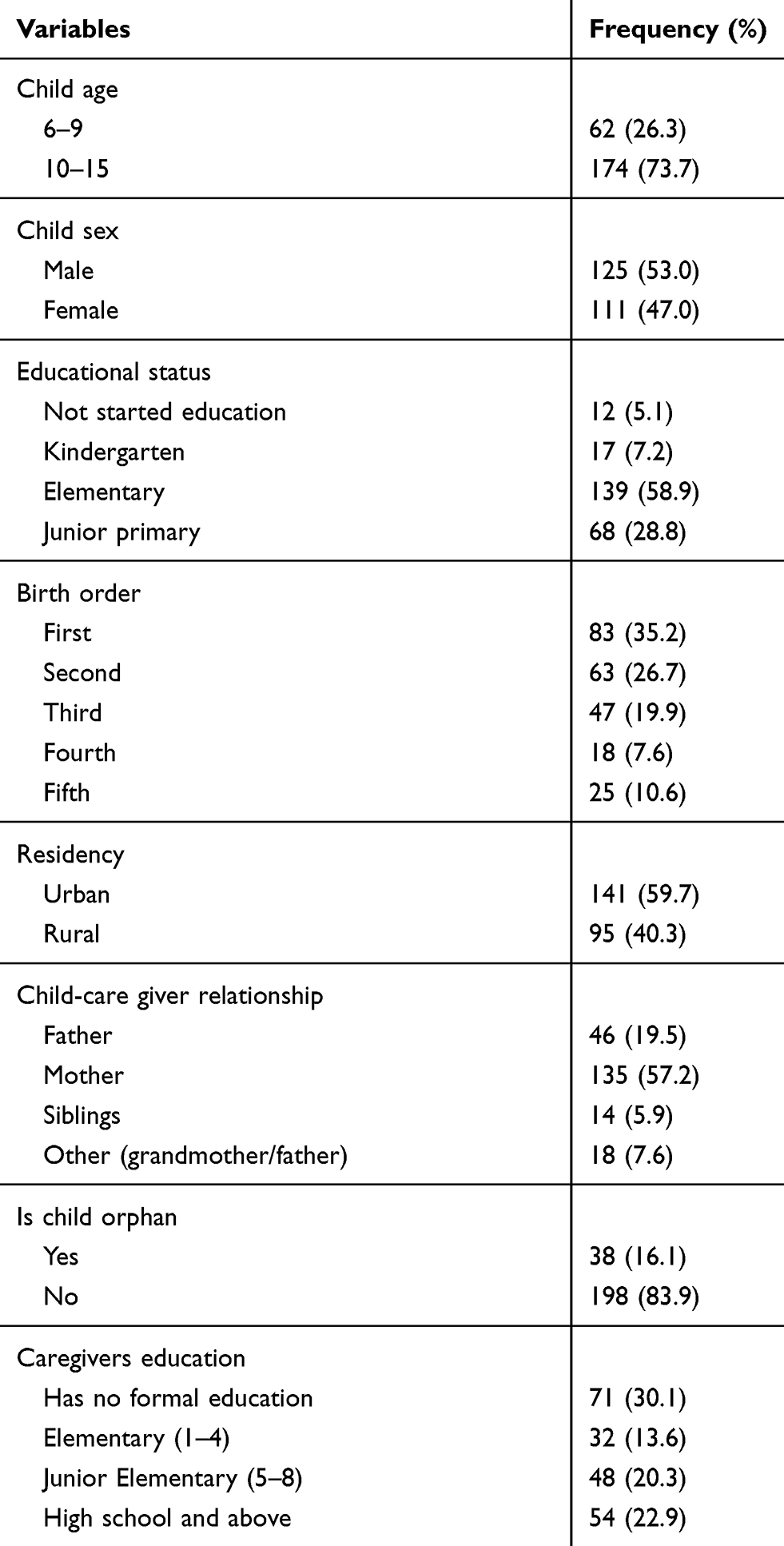 |
Table 2 The Socio-Demographic Characteristics of the Children on ART and Their Caregivers in West Shoa Zone, Ethiopia, 2019 |
HIV and ART Status of the Children and Caregivers
The caregivers were asked whether their child knows why he/she was taking the drug. If the caregivers said yes for this question, the question “what did you tell him/her?” followed with three options was asked. The options were: i) I told him that he has HIV in his blood; ii) I told him/her that he/she has a chronic disease in his body but did not mention the term HIV in explanation, or iii) the third option was open for the respondents. Accordingly, out of the total 236 participants interviewed, 103[43.6%, 95% CI: 37, 50.9] of the children were fully disclosed (told that they had HIV in their blood), 32 (13.5%) were partially disclosed (told that they had some germs in their blood which is not curable, but the term HIV was not mentioned).
The mean age at disclosure was 11±SD2.12. Only one child was fully disclosed at the age of less than 10 years. The caregivers’ preferred mean age to disclose was 12.26±SD2.3 (minimum=6 to maximum=18). The median age of children since they have started ART was 8.35 years. Ninety-four (92.15%) of the disclosure was done after the child had started ART, while the others were disclosed pre-ART drugs. One hundred three (43.5%) of the children were in the third stage, 82 (34.6%) were in the first stage and 42 (17.7%) of the children were in the second stage of WHO HIV classification Table 3. Most children (92%) took the TB prophylaxis drug. Of the caregivers, 170 were HIV positive and 167 of them were taking ART drugs. From the HIV positive caregivers, 164 disclosed their HIV status to either family members or someone else. Twenty-two (9.3%) of the caregivers reported that their child missed a drug in the last two weeks. Forgetfulness was the commonest reason for missing ART drugs followed by child refusal.
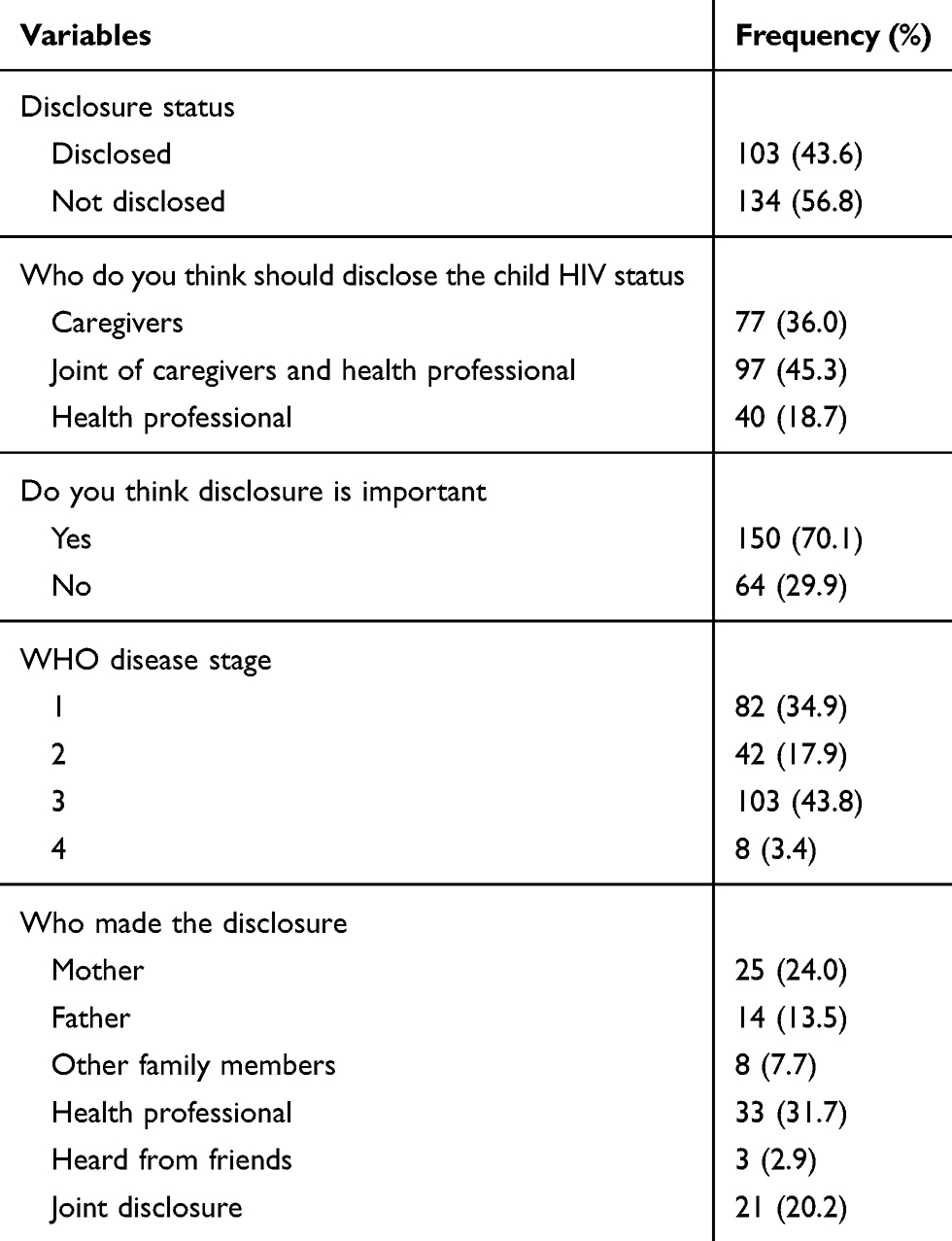 |
Table 3 Child and Caregivers’ HIV and ART Status and Related Matters in West Shoa Zone, Ethiopia, 2019 |
Reasons for Disclosing or Not Disclosing the Child Status
The commonest reasons explained for the children as to why they were taking the drug were: the child has a disease like TB, intestinal parasitosis, anemia among others was mentioned by most caregivers. Some of the caregivers also mentioned that they told their child that she/he was taking candy. The caregivers were asked why they decided to disclose the child’s status, and the commonest reason they mentioned were: if the child knows his/her status he/she will take her drug as ordered by the physician, and also he/she will take care of her/his health ie the child will take responsibility in caring for his/her self so that she/he will live better lives in the future. Some caregivers also mentioned that they disclosed the child’s status to ease the child’s confusion and tension since the child repeatedly asked them why she/he is taking the drug.
Those caregivers who did not disclose mentioned that since the child was not mature enough, she/he would not understand the discussion about HIV. Some of the caregivers mentioned that it is better not to disclose because not thinking about HIV will avoid child psychological disturbance and in turn avoid child death. Some others also reported the child could not keep a secret as a reason for not disclosing yet. Ninety-seven (41.1%), 77 (32.6%), and 40 (16.6%) of the caregivers reported that the disclosure should be done by joint caregivers and health professionals, only by caregivers and only by health professionals respectively (Table 3).
Factors Associated with the Child HIV Status Disclosure
To assess the factors associated with the child status disclosure, bivariate analysis was done first. Variables that were associated with the dependent variable at p-value ≤ 0.25 were selected and included in multiple logistic regressions analysis (Table 4). The model fit was checked by Hosmer and Lemeshow test (p-value=0.54) and it was fitted. Accordingly, three of the variables, child age, child sex, and caregivers’ level of education were significantly associated with the child status disclosure. Compared with the adolescents (10–15), children in the pre-adolescence age were 97% [AOR: 027, 95% CI: 0.003, 0.22, P<0.001] less likely to be disclosed. Females children were 2.7 times more likely to be disclosed compared with male children [AOR: 2.73, 95% CI: 1.24, 6, P<0.013] (Table 4).
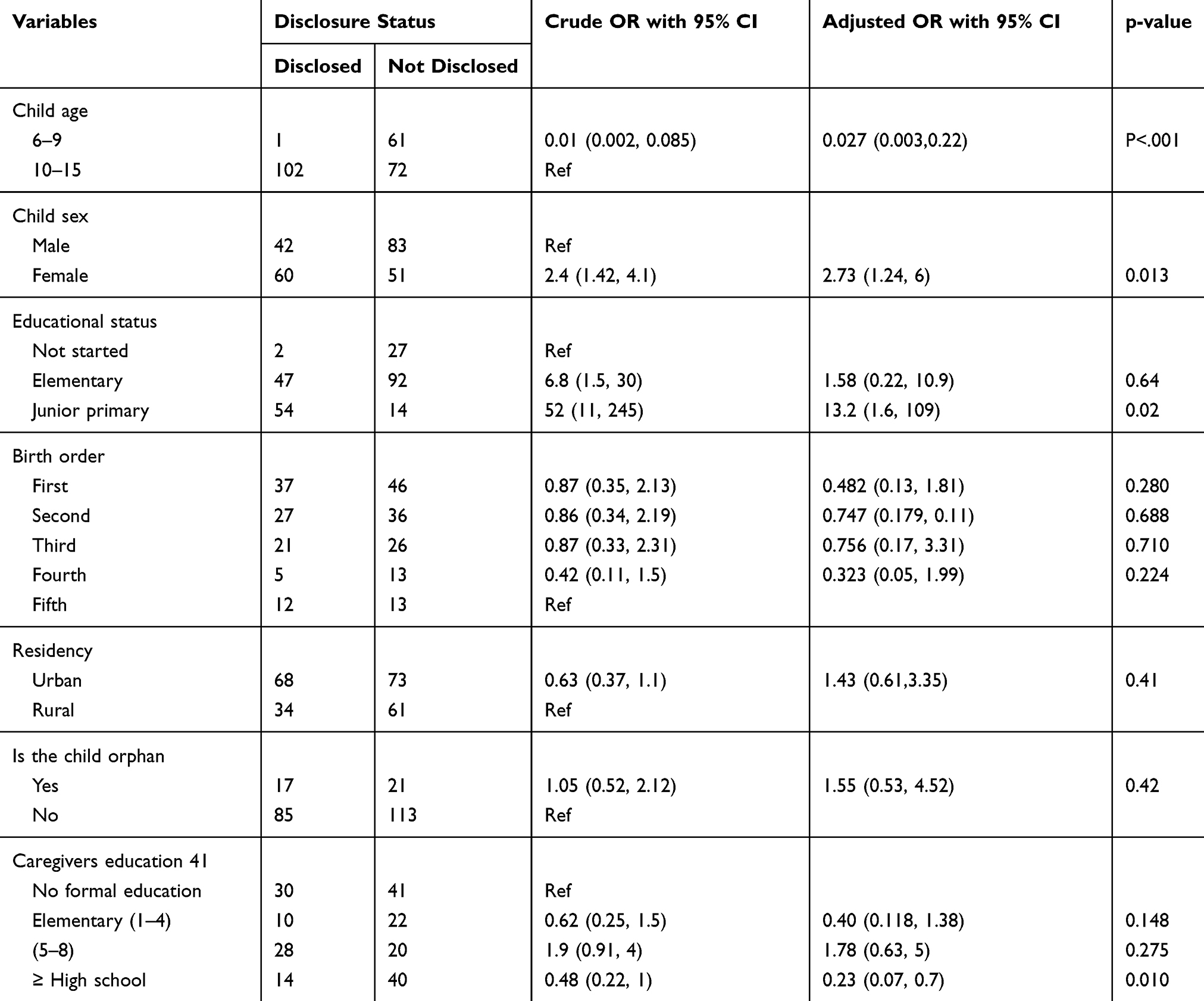 |
Table 4 Binary and Multiple Logistic Regression Analysis results on Factors Associated with HIV Status Disclosure Among 6–15 Years Old Children in West Shoa Zone, Oromia, 2019 |
Findings from the Qualitative Study
Four nurses (3 females and 1 male) working on ART at different health institutions and five child caregivers (3 mothers and 2 fathers) who had disclosed their child status were interviewed. All of them agree on the importance of HIV status disclosure and believe it should be done when the child is mature enough to understand the discussion about HIV. However, the age that the participants consider as maturing age varies. Some of the participants said maturity age is 10, others 12 and above:
Currently, we are facing many challenges concerning the child viral load. Children are discontinuing their drug and their viral load become higher when they come to the health center here. So, to overcome the challenges of drug adherence, I think disclosure is the solution if they are matured. Many children are entering into the fire age, and by this age, they will have opposite-sex friends. Knowing their status is better for them so that they will prevent themselves and others from disease transmission …. (Female ART Nurse from Holota Health Center)
In addition, if the child is disclosed at an early age they will more likely to refuse to take the drug and they become hopeless. One of the participants described the consequences of early disclosure as follows:
If the child disclosure is done before maturity, the child will discontinue the drug or not adhere to it. The child will disturb the family. Since she/he acquired the disease from his/her mother, he/she will angry with his/her mother saying I acquired this curse from you which I have not done. The child becomes hopeless, and he/she will discontinue the drug and then finally come to us by developing Opportunistic Infection.
Both health professionals and caregivers had a different perception of who should disclose child status. Some of the health professionals responded that it is better determined by caregivers as who should disclose it to the child.
Some caregivers say we will disclose it. But, for me, it is better if the disclosure is by joint caregiver and health professional. Because, it is difficult for the caregiver alone to disclose, and the health professional can use their scientific knowledge to make the children understand. (ART Nurse from Ambo Hospital)
One of the child caregiver also responded to the same idea with the above as follows:
For me, since the health professionals have more detailed knowledge about the disease and the drug, the issue about the disease is better told by the health profession. We, the caregivers will inform about our status, as we are taking the drug and sharing our life experience with the child. So, it is better if done jointly, and some part by a health professional and some part by the family/caregivers.
Both the caregivers and health professionals were asked about their experience of the disclosure process. Although the process of disclosure varies, the common sense was that all of them were trying to disclose the child with the best system of calming and stabilizing the child. One of the caregivers (father) portrayed his experience as follows:
… To disclose the child’s status, first I start from myself. I said, my daughter; I am a patient person, infected with HIV disease. Currently, as you are seeing me, I am taking this drug. I am doing my daily activities. Nothing is different for me from my pre-disease condition. You are also infected with this disease. The disease was transmitted to you from your mother while you were in the womb. Now, you can continue your education, you can live as any other healthy person can live, and when you success in your education, you will help me in the future.
Children experience different feelings during disclosure. The commonest experiences mentioned were described as follows:
They will anger to their mother, they will cry, some of the children will refuse to take their drug in the first week, and become depressed. But, if they get support from their caregivers, they become stable after a week. Even though it is rare, those children in the age of 15 and above may sometimes engage in revenging others. They will try to infect other people by concealing their status. Both male and female will engage in unsafe sex. (ART Nurse from Ambo Hospital)
The other disclosure process mentioned by the health profession was what he explained as peer disclosure, which they used rarely:
… … Rarely, we also use peer disclosure. In such type of disclosure, children/adolescents of nearly on same age are collected together …. Their numbers may reach up to forty. Then, the disclosure will be done at the collection moment. Those already disclosed children will introduce themselves as they are HIV positive … saying I am X, I am living with HIV for the last 15 years, now I am grade eight. So, being HIV positive does not prohibit you from your future goal … different individuals will share their experience there. Those not disclosed will know themselves there, and will develop hope. They will develop hope by seeing those people who were introducing themselves as a model … (Male ART Nurse from Ambo Hospital)
Discussion
We assessed the magnitude of HIV status disclosure, the process of disclosure, and what factors were influencing the disclosure. Accordingly, 43% of the children were fully disclosed. This relatively higher finding could be attributed to the fact that most (73%) of our study children were aged greater than 10 years. However, only 65% of those children aged at least 12 years were disclosed, which is lower than the ideal, which should be 100%, since most of the children were in the age considered to be a mature age for disclosure. This finding is like the finding from a study in South Africa (40%), in Eastern Ethiopia (49%), and in Gondar town (44%), North Gondar (39%) of Ethiopia.16,22-24 However, it is greater than the studies conducted in Hawassa, the southern part of Ethiopia, and in Tanzania.17,25 The difference could be due to the difference in sample size. The one study conducted in Hawassa was with 177 children while the current study was with 236. In addition, disclosure is a complex process that is influenced by socio-cultural factors like fear of stigma. So, the difference in the socio-cultural circumstances of the previous and current study could also the possible reason for this difference. In addition, the issue of drug non-adherence among children is gaining attention among the scientific community which in turn is influencing the disclosure process.
The mean age at disclosure was 11 years and this age was close to the age assumed to be maturity and preferred by most caregivers. The rate of disclosure increases with age. Only a single child of age less than 10 was disclosed. Approximately 40%, 35%, and 30% of the children age 10 and above, or 11 and above or 12 and above were not disclosed yet, respectively. The finding from the qualitative data also justifies this result:
“I think children should know their status. But, the disclosure should be based on their maturity and ability to understand what we are going to discuss with them. From my experience, it is better if fully disclosed at 12 or 13 years. But sometimes, some children are very active and fast even at 9 years. In such a case, the disclosure could possible.“ (ART nurse from Holota Health Center).
“The most challenging part in disclosure is convincing the family. They do not want their child to be disclosed. I do have an experience of 16 years old client. I have tried to convince the father to disclose. But, he refused … … Our culture is also difficult. Most of the time, our community does not want to share sensitive things with their children. Here, the family says, do not disclose my child’s status; I will do it at home. But, they do not do it at home. This means they want to hide it.” (ART nurse from Ambo Hospital)
The same finding was reported previously in a study in the Eastern and North-East part of Ethiopia.16,22
Almost all the caregivers agreed that child status disclosure is important. The commonly mentioned advantages of the disclosure were: drug adherence after disclosure, for better self-care and to ease child confusion and tension since the child repeatedly asks the caregivers why she/he is taking the drug. Being underage was the commonest reason for not disclosing the child. The result from the caregiver’s in-depth interview is also consistent with the above quantitative finding.
Similar findings were reported in many studies conducted in Africa and Asian Countries.17,18,20,22-24 This finding is different from the finding reported in one study conducted in Addis Ababa among orphanage and community children in which disclosure was mainly followed by family death and it was unplanned.9
Those undisclosed children were told deception by their caregivers about their status and why they were taking the drug. But partial disclosure is recommended when the child is not considered to be mature enough. Failure to do so during an early age will make disclosure difficult at a later age.
Female children were more likely to be disclosed than their male counterparts. Although we did not find another study supporting this finding, the following justification was forwarded in qualitative findings:
It is easy to tell the female children about their status than males. This is due to many reasons such as most of the time female children keep secret. A female child does not expose family’s mystery to other people if she is told the issue is secret and also females are eager to know things than males and ask repeatedly (mothers of 11 years old female child)
I think; female disclosure is also related to violence. I do have experience with this. One mother told me as she disclosed her daughter at 9 years. I asked her why she disclosed it at this age. She said, my daughter may experience sexual abuse, and for whatever she may face, she better knows and keeps herself. (ART nurse from Ambo Hospital)
Many challenges were hindering both caregivers and health care providers from disclosing the children’s HIV status. Factor such as the age of child ie not being mature enough, fear of stigma, and fear of psychological disturbance if disclosed were commonly mentioned. This finding is like many of the studies conducted previously. But what is unique in this study is the barriers claimed by the health professionals. Almost all the IDI participant health professionals raised the issue of family/caregivers’ resistance, lack of training on disclosure issues, shortage of time, and space:
… … If I plan to disclose a child status, first I will lock the door. You need to take time for and silent environment to discuss disclosure. But, here, we visit up to 40–50 clients per day. The environment is crowded; the patients will wait for us. And the number of professionals here is few and even out of the three ART professionals here, only me, who took the training. In addition to our daily duties, sometimes we are ordered to do some management activities. So, these factors are hindering us to fully practice the issue of disclosure in our hospital. (ART Nurses from Ambo Hospital)
Limitation of the Study
We did not include disclosed children as part of qualitative data collection for fear that discussing may cause psychological disturbance or unnecessary reaction. In addition, since these data were collected during service rendering for the clients in the ART clinic, there could be a probability of false reports in favor of what the health care providers were advising.
Conclusion and Recommendations
Although most of the children were aged at least 10 years, an age interval considered to be maturity by the caregivers, the prevalence of children’s HIV status disclosure was found to be low and it was affected by factors such as child age, child sex, fear of child psychological disturbance after disclosure, and fear of stigma. The child’s age was the most significant factor affecting the disclosure status. Accordingly, disclosure at the two extreme ages ie age less than 10 or age greater than 14 was perceived by both caregivers and health professionals to have a negative consequence on either the child or child’s family. In addition, lack of sufficient training about disclosure ie when, where, and how, by whom should it be done, shortage of time, inconvenience of place for discussion about the disclosure were factors identified affecting disclosure from the health care providers’ perspective.
The challenges from caregivers’ side, plus gaps from care providers’ side, in general, contributed to this low level of the disclosure. This will affect directly or indirectly the child’s drug adherence, treatment outcome, and also disease transmission. Since disclosure is a complex process, it needs the collaboration of caregivers and health care providers. There should be clear and contextualized guidelines on when to start, how, where, and who should do what in the disclosure process. The guideline should address issues like the culture of the society, means of managing the concern of family after disclosure which includes stigma, and child psychological disturbances.
Updating health care providers’ knowledge and skills and working on caregivers’ attitude is needed to manage disclosure and challenges following it. Health care providers are also strongly urged to emphasize discussing the issue of disclosure with caregivers. In addition, health institutions managers should consider facilitating space and other challenges hindering the disclosure process in their plan.
Abbreviations
AOR, adjusted odds ratio; ART, antiretroviral treatment; CDC, communicable disease control; CI, confidence interval; H/C, health center; in, depth interview; SD, standard deviation.
Acknowledgment
We would like to thank Ambo University for covering the data collectors’ costs and supervisors per diem. In addition, we would like to forward our heartfelt gratitude to our study participants, our data collectors, and ART nurses at Ambo Hospital, Ginchi Health Center, Inchini Health Center, and Holota health center for their valuable cooperation during the data collection process.
Lastly, our thank goes to professor Roger Watson for editing the manuscript.
Disclosure
The authors declare that they have no competing interests in this section.
References
1. UNAIDS. Global and Regional HIV Statistics; 2017.
2. Wang H. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: the Global Burden of Disease Study 2015. Lancet HIV. 2016;3:361–387. doi:10.1016/S2352-3018(16)30087-X
3. WHO. Ethiopia Country Profile; 2017:59
4. Vreeman RC, Gramelspacher AM, Gisore PO, et al. Disclosure of HIV status to children in resource-limited settings: a systematic review. J Int AIDS Soc. 2013;16:18466. doi:10.7448/IAS.16.1.18466
5. Regina EB, Stephen MK, Bonaventura CTM. Factors associated with HIV status disclosure and its effect on treatment adherence and quality of life among children 6–17 Years on antiretroviral therapy in southern highlands zone, Tanzania: unmatched Case-Control Study. Int J Pediatr. 2017;2018 ID 8058291:10.
6. WHO. Guideline on HIV Disclosure Counseling for Children Up to 12 Years of Age; 2011.
7. National Consolidated Guidelines For Comprehensive Hiv Prevention, Care, And Treatment. Available from: https://www.afro.who.int/sites/default/files/2019-04/NationalComprehensiveHIVCareGuideline2018.pdf.
8. Vreeman RC, Scanlon ML, Marete I, et al. Characteristics of HIV-infected adolescents enrolled in a disclosure intervention trial in western Kenya. AIDS Care Psychol Socio-Medical Asp AIDS/HIV. 2015;27(sup1):6–17. doi:10.1080/09540121.2015.1026307
9. Vreeman RC, Scanlon ML, Mwangi A, et al. A cross-sectional study of disclosure of HIV status to children and adolescents in Western Kenya. PLoS One. 2014;9(1):e86616. doi:10.1371/journal.pone.0086616
10. Bikaako-Kajura W, Luyirika E, Purcell DW, et al. Disclosure of HIV status and adherence to daily drug regimens among HIV-infected children in Uganda. AIDS Behav. 2006;10(S1):85–93. doi:10.1007/s10461-006-9141-3
11. Mumburi LP, Bernardus CH, Philemon RN, Kapanda GN, Levina JM. Factors associated with HIV-status disclosure to HIV-infected children receiving care at Kilimanjaro Christian Medical Centre in Moshi, Tanzania. Pan Afr Med J. 2014;10 18:50.
12. Mahloko JM, Madiba S. Disclosing HIV diagnosis to children in Odi district, South Africa: reasons for disclosure and non-disclosure. Afr J Prm Heal Care Fam Med. 2012;4(1):
13. Aderomilehin O, Hanciles-Amu A, Ozoya OO. Perspectives and practice of HIV disclosure to children and adolescents by health-care providers and caregivers in sub-Saharan Africa: a Systematic review. Front Public Heal. 2016;4. doi:10.3389/fpubh.2016.00166
14. Vaz LME, Maman S, Eng E, Barbarin OA, Tshikandu T, Behets F. Patterns of disclosure of HIV status to infected children in a Sub-Saharan African setting. J Dev Behav Pediatr. 2011;32(4):307–315. doi:10.1097/DBP.0b013e31820f7a47
15. Kallem S, Renner L, Ghebremichael M, Paintsil E. Prevalence and pattern of disclosure of HIV status in HIV-infected children in Ghana. AIDS Behav. 2011;15:1121–1127. doi:10.1007/s10461-010-9741-9
16. Negese D, Addis K, Awoke A, et al. HIV-positive status disclosure and associated factors among Children in North Gondar, Northwest Ethiopia. ISRN AIDS. 2012;2012:1–7. doi:10.5402/2012/485720
17. Tadesse BT, Foster BA, Berhan Y. Cross-sectional characterization of factors associated with pediatric HIV status disclosure in Southern Ethiopia. PLoS One. 2015;10(7):e0132691. doi:10.1371/journal.pone.0132691
18. Sariah A, Rugemalila J, Somba M, et al. Experiences with disclosure of HIV-positive status to the infected child”: perspectives of healthcare providers in Dar es Salaam, Tanzania. BMC Public Health. 2016;16:1083. doi:10.1186/s12889-016-3749-7
19. Nzota MS, Joseph KB, Matovu HR, Draper RKSNK. Determinants and processes of HIV status disclosure to HIV - infected children aged 4 to 17 years receiving HIV care services at Baylor College of Medicine Children’s Foundation Tanzania, Centre of Excellence (COE) in Mbeya: a cross-sectional study. BMC Paediatr. 2015;15:81. doi:10.1186/s12887-015-0399-3
20. Silenat B, Woldaregay EA, Markos A, Workeabeba AT, Mulugeta B. Adherence to Antiretroviral Therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatr. 2013;13:132. doi:10.1186/1471-2431-13-132
21. Britto C, Mehta K, Thomas R, Shet A. Prevalence and correlates of HIV disclosure among children and adolescents in low- and middle-income countries: a systematic review. J Dev Behav Pediatr. 2016;37(6):496–505. doi:10.1097/DBP.0000000000000303
22. Mengesha MM, Dessie Y, Roba AA. Perinatally acquired HIV-positive status disclosure and associated factors in Dire Dawa and Harar, Eastern Ethiopia: a health facility-based cross-sectional study. BMJ Open. 2018;8(8):e019554. doi:10.1136/bmjopen-2017-019554
23. Meena R, Hemal A, Arora SK. Pediatric HIV disclosure in northern india: evaluation of its prevalence, perceptions amongst caregivers, and its impact on CLHIV. AIDS Res Treat. 2018;2018:1–7. doi:10.1155/2018/2840467
24. Tilahunb AD. HIV positive status disclosure and associated factor among HIV infected children in pediatric ART clinics in Gondar town public health facilities, North West Ethiopia, 2018. J Infect Public Health. 2018;12(6):873–877.
25. Brown BJ, Oladokun RE, Osinusi K, Ochigbo S, Adewole IF, Kanki P. Disclosure of HIV status to infected children in a Nigerian HIV care program. AIDS Care Psychol Socio-Medical Asp AIDS/HIV. 2011;23(9):1053–1058. doi:10.1080/09540121.2011.554523
26. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573–577. doi:10.7326/0003-4819-147-8-200710160-00010
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.