Back to Journals » Cancer Management and Research » Volume 14
High Superior-Middle Pharyngeal Constrictor Muscle Mean Dose Correlates with Severe Late Lung Infection and Survival in Nasopharyngeal Cancer Patients
Authors Liu WS, Chien JC, Huang YH, Chen PC, Huang WL, Chiang SW, Lee CC, Kang BH ![]() , Hu YC
, Hu YC ![]()
Received 26 November 2021
Accepted for publication 28 February 2022
Published 8 March 2022 Volume 2022:14 Pages 1063—1073
DOI https://doi.org/10.2147/CMAR.S350714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Wen-Shan Liu,1– 3 Ju-Chun Chien,1 Yu-Hsien Huang,1 Po-Chun Chen,4,5 Wei-Lun Huang,1 Shao-Wei Chiang,1 Ching-Chih Lee,6 Bor-Hwang Kang,3,6 Yu-Chang Hu1
1Department of Radiation Oncology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 2Department of Nursing, Meiho University, Pingtung, Taiwan; 3School of Medicine, National Defense Medical Center, Taipei, Taiwan; 4Department of Radiation Oncology, Pingtung Christian Hospital, Pingtung, Taiwan; 5Graduate Institute of Bioresources, National Pingtung University of Science and Technology, Pingtung, Taiwan; 6Department of Otorhinolaryngology - Head and Neck Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
Correspondence: Wen-Shan Liu, Department of Radiation Oncology, Kaohsiung Veterans General Hospital, No. 386, Dazhong 1st Road, Zuoying Dist., Kaohsiung City, 813414, Taiwan, Tel +886934075313, Email [email protected]
Purpose: The study aimed to evaluate 1) the correlation of doses of swallowing-related organs at risk (OAR) with severe swallowing-related late adverse effects (AE) in nasopharyngeal carcinoma (NPC) patients and 2) the effect of high mean doses of OARs on overall survival (OS).
Patients and Methods: This retrospective cohort study enrolled non-metastatic Stage I–IV NPC patients from January 2012 to June 2017. OAR mean doses and severe (≥G3) swallowing-related late AE (xerostomia, dysphagia, and lung infection) were evaluated by t-test and validated using receiver operating characteristic curves. The risk factors of OS were calculated by Cox regression methods.
Results: This study enrolled 185 (43 female, 142 male) NPC patients, mean age 52.4 years, primarily with Stage III (93, 50.3%) or Stage IV (67, 36.2%) disease. The mean doses of pharyngeal constrictor muscle (PCM), superior-middle PCM (SMPCM), and superior PCM (SPCM) were significantly higher in those with severe (≥G3) lung infection than in those without (65.7 vs 62.2 Gy, p = 0.036; 68.1 vs 64.2 Gy, p = 0.015; and 70.0 vs 65.9 Gy, p = 0.012, respectively). Patients with severe (≥G3) dysphagia had significant higher mean doses of base of tongue (56.2 vs 50.2 Gy, p = 0.008), laryngeal box (50.6 vs 46.4 Gy, p = 0.036), PCM (65.4 vs 62.1 Gy, p = 0.008), SMPCM (67.1 vs 64.2 Gy, p = 0.014), and SPCM (69.3 vs 65.8 Gy, p = 0.004). Mean SMPCM dose > 64.9 Gy (adjusted hazard ratio [aHR] = 3.2, 95% confidence interval [CI] 1.2– 8.8, p = 0.021), age > 62 years (aHR = 2.7, 95% CI 1.1– 6.9, p = 0.032), N3 status (aHR = 4.0, 95% CI 1.8– 9.0, p = 001), and severe late AE of lung infection (aHR = 4.6, 95% CI 1.5– 14.0, p = 0.007) significantly affected OS.
Conclusion: Severe lung infection and dysphagia were associated with significantly higher mean doses of PCM, SMPCM, and SPCM. Among these OARs, only a high SMPCM mean dose was a risk factor for OS in NPC patients.
Keywords: nasopharyngeal carcinoma, late adverse effect, pneumonia, dysphagia, pharyngeal constrictor muscle, intensity-modulated radiotherapy
Introduction
The results for treatment of nasopharyngeal carcinoma (NPC) have improved in recent decades.1 In addition to systemic chemotherapy,2 numerous studies have confirmed the usefulness of intensity-modulated radiotherapy (IMRT).3–6 For example, the RTOG-0225 trial demonstrated that IMRT could be used in multi-institutional setting with 2-year progression-free and overall survival (OS) rates of 72.7% and 80.2%, respectively.3 Zhang et al5 in a meta-analysis, found that IMRT treatment significantly improved both 5-year OS (Odds Ratio [OR] = 1.51; 95% confidence interval [CI] 1.23–1.87; p<0.05) and local control (OR = 1.94; 95% CI 1.53–2.46; p < 0.05). Furthermore, IMRT could significantly reduce the incidence of the swallowing-related late adverse effects (AEs) of trismus and xerostomia, compared to 2D or 3D radiotherapy treatments (OR = 0.18; 95% CI 0.04–0.83; p<0.05; OR = 0.18; 95% CI 0.07–0.46; p<0.05, respectively). However, at long-term follow up, patients who received IMRT still suffer from many kinds of swallowing-related severe late AE such as malnutrition, dysphagia, xerostomia, trismus and aspiration pneumonia.7,8 Together with other late AEs, these conditions impair quality of life in such patients.7
A recent study found that the swallowing-related severe late AE of lung infection significantly reduced the OS in NPC patients (adjusted Hazard Ratio [aHR] 6.3, 95% CI 1.6–24.2, p=0.007).9 Aspiration pneumonia as a late AE after definitive radiotherapy with or without chemotherapy in head and neck cancer patients (especially NPC and hypopharyngeal cancer) were found using population database studies.10−11 Xu et al found that these patients had a significantly increased rate of aspiration pneumonia (5-year: 23.8% vs 8.7%, p<0.001) and, most importantly, risk of death (HR=1.42, p<0.001).10 In oropharyngeal cancer patients, it is well documented that these swallowing-related late AE (dysphagia and pneumonia) are significantly correlated with the dosages of swallowing-related OARs.12–14 However, such findings are lacking for NPC patients. Also unknown are the cut-off values for which swallowing-related OARs are correlated with AEs and OS in NPC patients. Therefore, the primary aim of this study was to evaluate whether severe swallowing-related late AE correlated with the doses of swallowing-related OARs in NPC patients. The secondary aim was to evaluate whether certain high mean doses of OARs were risk factors in the OS of NPC patients.
Patients and Methods
Ethics
This study was approved by the Institutional Review Board of the Kaohsiung Veterans General Hospital (KSVGH20-CT5-23) and conducted in accordance with the Declaration of Helsinki. The informed consent was waived by the Board due to its retrospective design and the use of de-identified data without patient’s personal information.
Patients
This retrospective cohort study included patients with pathologically-proven NPC from January 2012 to June 2017. The inclusion criteria were Stage I to IV NPC without any distant metastatic disease and total radiotherapy doses >66 Gy. The exclusion criteria were previous malignant disease or non-standard chemotherapy regimens. The studies used to determine clinical stage were magnetic resonance imaging (MRI) or computed tomography (CT) scan, physical examination, chest X-ray, bone scan and liver sonography. The stage group was that defined by American Joint Committee on Cancer’s (AJCC) Cancer Staging Manual, 7th Edition.15 The treatments consisted of radiotherapy, concurrent chemoradiotherapy (CCRT), neoadjuvant chemotherapy and/or adjuvant chemotherapy.
Radiotherapy
IMRT was performed for all patients. The immobilization device was a thermoplastic mask combined with localizer (U-Plast thermoplastic mask, Orfit Industries NV, Wijnegem, Belgium). Image acquisition was done by CT simulator with 3 mm slice thickness. All treatment plans were calculated using the Eclipse planning system (Varian Medical System, Palo Alto, CA). During this study period, two different clinical target volumes (CTVs) and CTV dosage protocols were defined as per those reported in a previous study.9 Subjects were divided into the simultaneously reduced volume and dose (SRVD) group and the conventional volume and dose (CVD) group. The principles of target delineation of CTV-1 and CTV-2 in SRVD group were similar to those of the study by Lin et al.16 The principle of target delineation of CTV-1 in the CVD group was similar to that of the RTOG 0225 study.3
Delineation of Swallowing-Related Structures
Many muscles and structures involved in the function of swallowing also correlate with the late AEs of dysphagia and aspiration pneumonia.12–14,17,18 This study retrospectively delineated swallowing-related muscles and structures for analysis. These structures included soft palate (SP), base of tongue (BOT), laryngeal box (LB), pharyngeal constrictor muscle (PCM), superior-middle PCM (SMPCM), superior PCM (SPCM), middle PCM (MPCM), inferior PCM (IPCM), and cricopharyngeal muscle (CPM). Except for the LB,18 the delineation principle of all above organs at risk (OARs) was based on the Danish Head and Neck Cancer Group consensus19 and the study of Christianen et al.20
Chemotherapy and Salvage Treatments
Chemotherapy was suggested for all patients except those with Stage I disease. For all Stage IV and some Stage III patients, chemotherapy with either neoadjuvant or adjuvant therapy were suggested as the standard of care. The regimens of CCRT were weekly cisplatin of 40 mg/m2 or 80 mg/m2 cisplatin every 3 weeks. The regimens of both neoadjuvant and adjuvant chemotherapy were 2–3 cycles of 80 mg/m2 cisplatin for one day and 800–1000 mg/m2 5-fluorouracil for 4–5 days every 3 weeks.
Salvage treatments were performed individually depended on the types of recurrence and the patient’s condition. These included radiotherapy with or without chemotherapy; surgical excision with or without adjuvant radiotherapy; and chemotherapy with or without target therapy, etc.
Evaluation of Severe Late Adverse Effects (AEs) and Clinical Response
All treatment-related late AEs were recorded using the Common Terminology Criteria for Adverse Events 4.0 system.21 The grading of late AEs was recorded thought-out the follow-up period to the end of study or death of patient. The late AEs were repeatedly recorded at every outpatient follow-up. In addition, the grading of severe late dysphagia and lung infection (pneumonia) were double checked with all admission medical records. The time definition of late AEs was the event happened six months after the completion of treatment.
Clinical response was evaluated by physical examination, nasopharyngeal fiberscope; MRI or CT scan; and Epstein-Barr virus test 3 months after the completion of radiotherapy or CCRT with or without adjuvant chemotherapy. Evaluation of disease status using a series of imaging studies was performed annually for five years at least and included MRI/CT scans, chest X-rays, upper abdominal sonography and whole body bone scan (optional) as well as other images as deemed appropriate. Nasopharyngeal biopsy was performed in cases with any suspicion of persistent or recurrent disease. The status of neck residual disease was evaluated by aspiration cytology or excisional biopsy if indicated. Survival time was defined as the time from the date of radiotherapy initiation to the date of death or last follow-up.
Statistical Analysis
First, this study used t-test to evaluate whether the mean doses of swallowing-related OARs significantly differed between T or N groups. Second, we used Friedman test to evaluate the differences in mean doses for different PCM sub-structures (SPCM, MPCM, IPCM and SMPCM). Third, we evaluated the relationship among mean doses of swallowing-related OARs and swallowing-related severe late AEs by t-test. Fourth, we used the receiver operating characteristic (ROC) curve method to validate the findings of the above results. Finally, we used Cox proportional hazard models to evaluate the risk factors for lower OS, including positive OARs correlated with severe late lung infection. A p value of less than 0.05 was considered as statistically significant. The statistical software used was IBM SPSS version 20 (IBM Corp., Armonk, NY, USA).
Results
Patient Characteristics
During the study period, 207 patients were diagnosed with NPC. After applying inclusion and exclusion criteria, we enrolled 185 patients for further analysis. There were 43 female and 142 male patients with a median age of 52.0 years (mean 52.4 ± 13.7 years, range 18–89 years). The Stage distribution was: 7 in Stage I, 18 in Stage II, 93 in Stage III and 67 in Stage IV. The patient and treatment characteristics are listed in Table 1. Patients with Stage I disease received radiotherapy treatment only. For Stage II to IV patients, 97.2% (173/178) received CCRT with or without induction and/or adjuvant chemotherapy. The mean doses of planning target volume (PTV) −1, PTV-2 and PTV-3 were 71.0 Gy, 58.2 Gy and 52.3 Gy, respectively (Table 1).
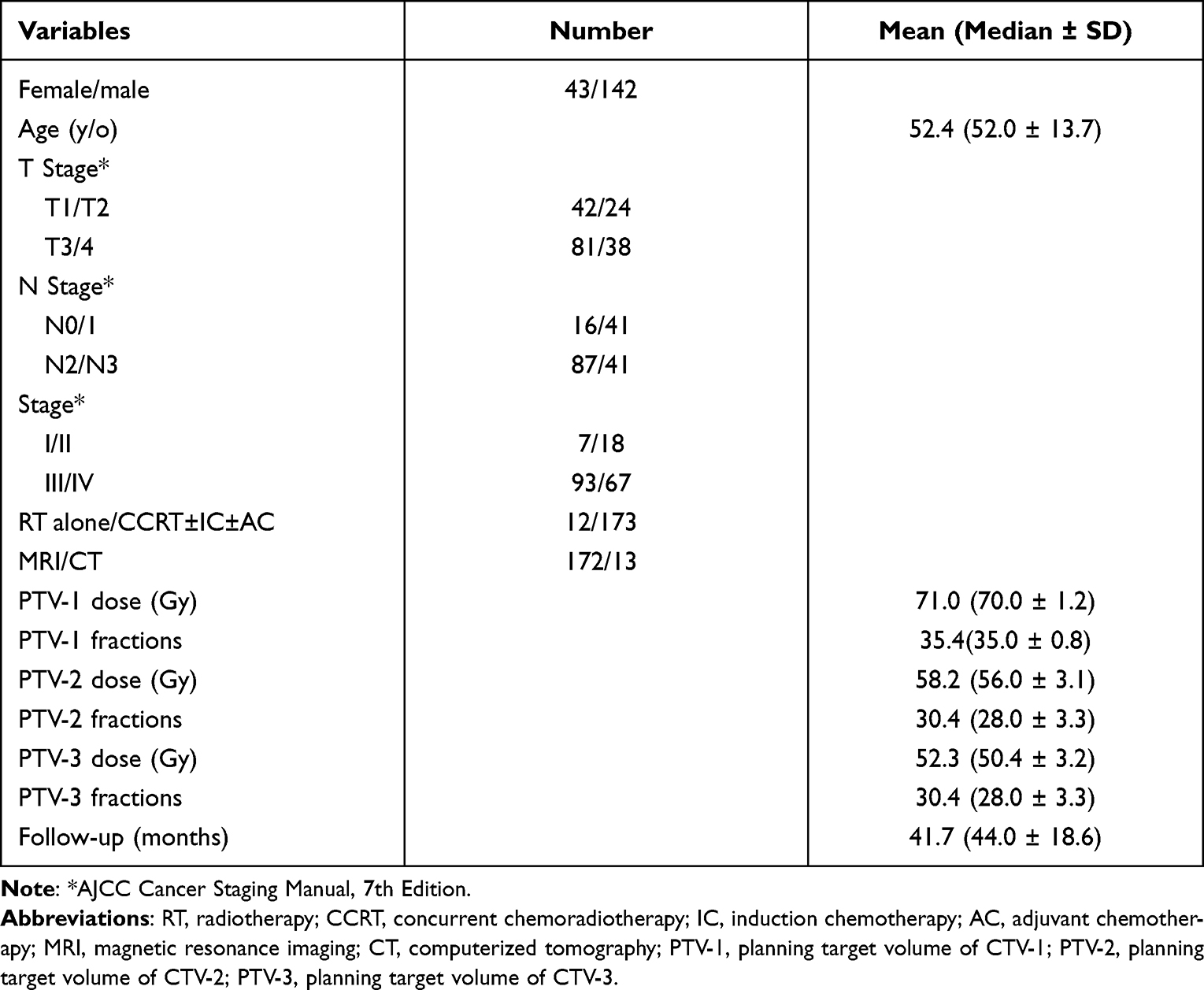 |
Table 1 Patient and Treatment Characteristics (n =185) |
The Doses of Various Swallowing-Related Muscles and Structures
The mean doses of SP, BOT, LB, PCM, SMPCM, SPCM, MPCM, IPCM and CPM were 65.3 Gy, 50.6 Gy, 46.7 Gy, 62.3 Gy, 64.4 Gy, 66.1 Gy, 58.6 Gy, 52.7 Gy and 48.8 Gy, respectively (Table 2). For the PCM sub-structures, the mean doses of SMPCM (64.4 Gy), SPCM (66.1 Gy), MPCM (58.6 Gy) and IPCM (52.7 Gy) were significantly different (p=0.000) from each other. The PCM sub-structures nearest the primary nasopharyngeal tumor received significantly higher doses than those distal to the primary tumor site.
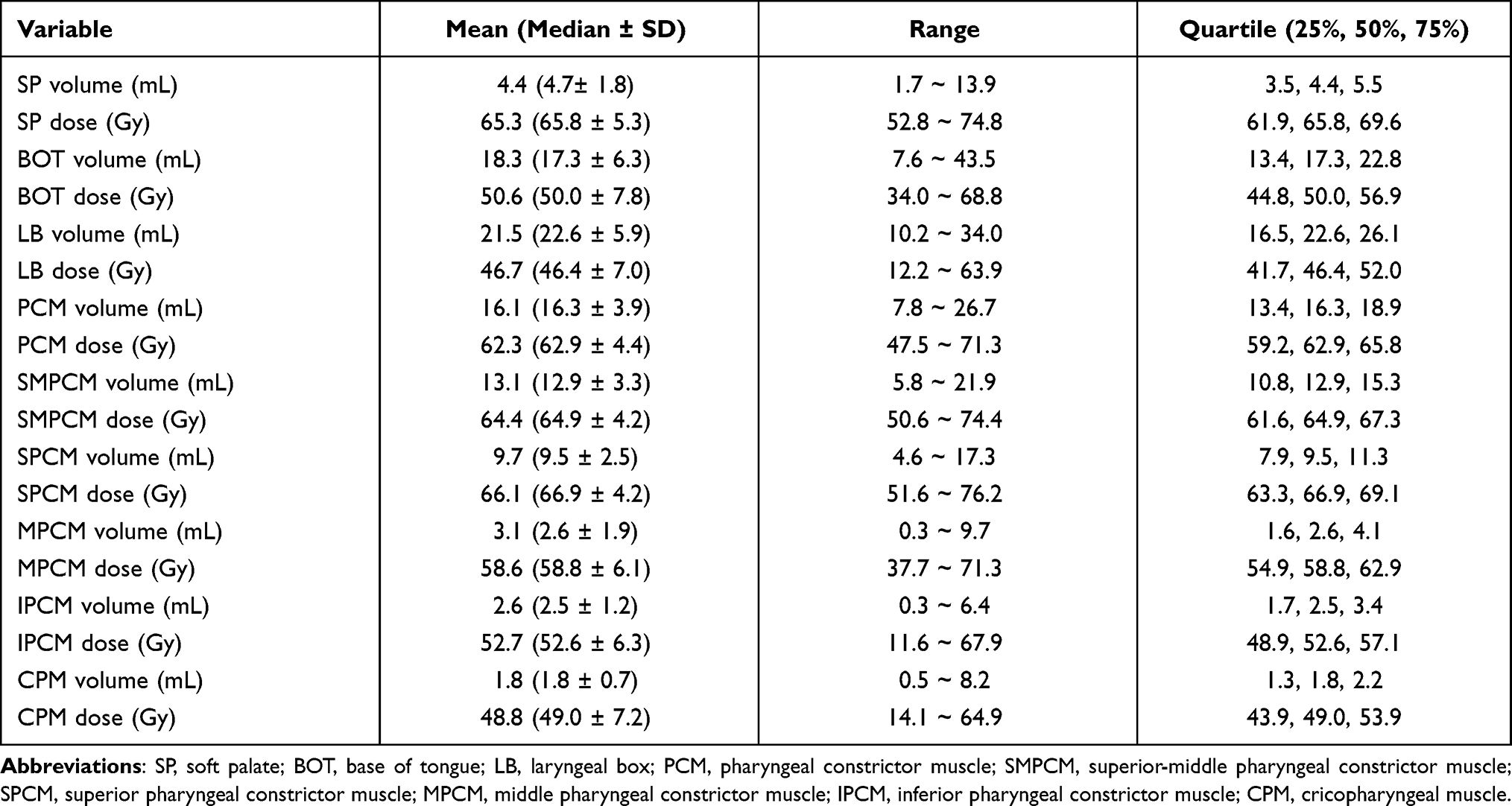 |
Table 2 The Volume and Mean Doses of Swallowing Related Structures (n =185) |
Among various swallowing-related OARs, only the SP mean dose differed significantly between T stage groups (63.8 Gy for T1-2 vs 66.1 Gy for T3-4, p=0.005). For all evaluated OARs, N2-3 patients had significantly higher mean doses of swallowing-related OARs than N0-1 patients (Table 3). The mean doses of all OARs did not differ significantly between Stage I–II patients and Stage III–IV patients.
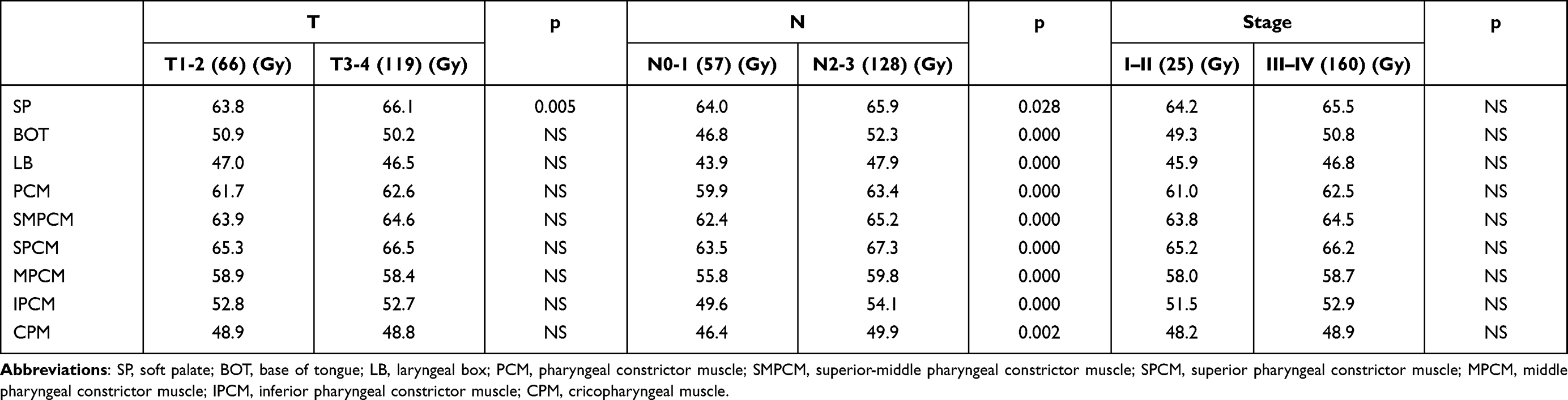 |
Table 3 The Correlation Between Disease Status and Mean Doses of Swallowing Related Structures (n =185) |
Severe Swallowing-Related Late AEs vs Mean Doses of Swallowing-Related Organs at Risk
Table 4 lists the correlations between different mean doses of OARs and the groups with or without severe swallowing-related late AEs. The mean doses of PCM, SMPCM and SPCM were significantly higher in patients with severe (≥ G3) lung infection than in those without lung infection (65.7 vs 62.2 Gy, p=0.036; 68.1 vs 64.2 Gy, p=0.015; 70.0 vs 65.9 Gy, p=0.012, respectively). Patients with severe (≥ G3) dysphagia had significant higher mean doses of BOT (56.2 vs 50.2 Gy, p=0.008), LB (50.6 vs 46.4 Gy, p=0.036), PCM (65.4 vs 62.1 Gy, p=0.008), SMPCM (67.1 vs 64.2 Gy, p=0.014) and SPCM (69.3 vs 65.8 Gy, p=0.004) than patients who did not have severe dysphagia. However, the mean doses of OARs did not differ significantly between those with or without severe (≥ G3) xerostomia. ROC curve analysis validated the above findings (Figure 1). For ≥ G3 lung infections, the area under the curve (AUC) of PCM, SMPCM and SPCM mean doses were 0.734 (95% CI 0.52–0.94, p=0.036), 0.741 (95% CI 0.54–0.94, p=0.031) and 0.763 (95% CI 0.56–0.96, p=0.018), respectively (Figure 1A). For ≥ G3 dysphagia, the AUC of the mean doses of PCM, SMPCM, SPCM, BOT and LB were 0.721 (95% CI 0.58–0.86, p=0.008), 0.685 (95% CI 0.54–0.83, p=0.026), 0.731 (95% CI 0.60–0.86, p=0.005), 0.725 (95% CI 0.59–0.86, p=0.007) and 0.686 (95% CI 0.56–0.82, p=0.025), respectively (Figure 1B).
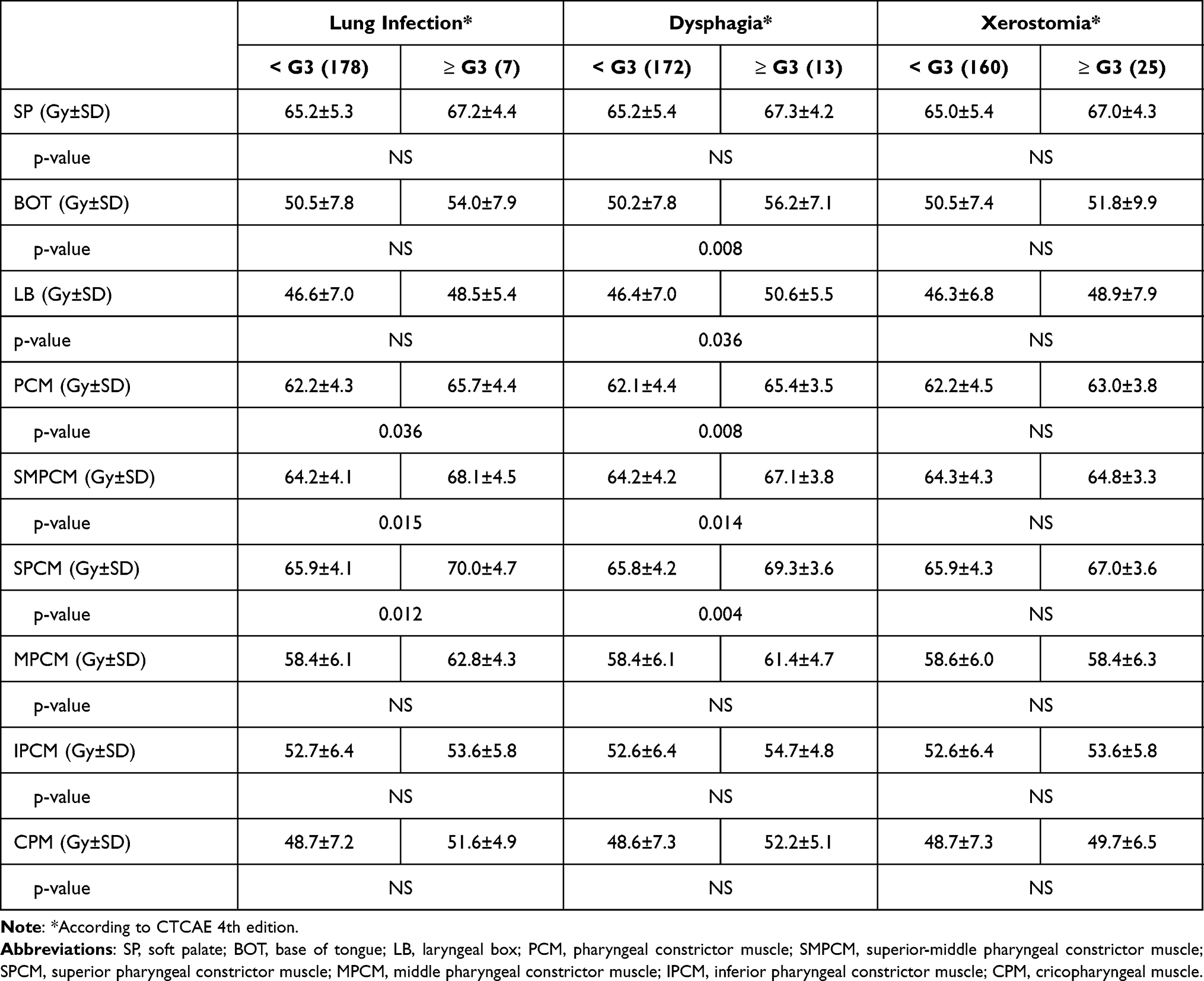 |
Table 4 The Correlation Between Severe Swallowing Related Adverse Effects and Mean Doses of Swallowing Related Structures (n=185) |
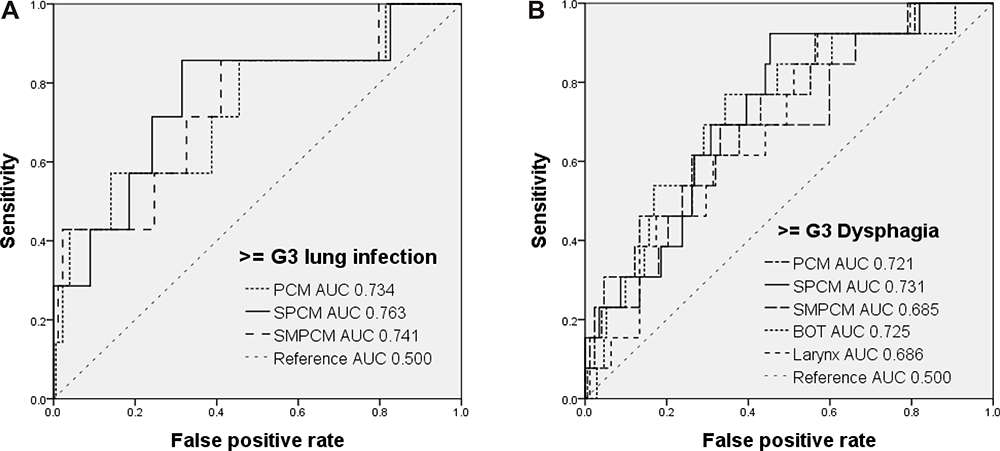 |
Figure 1 ROC curve analysis of correlations between severe late AEs and mean doses of OARs. (A) For severe late lung infection, the AUC of mean doses of PCM, SPCM and SMPCM were 0.734, 0.763 and 0.741, respectively. (B) For severe late dysphagia, the AUC of mean doses of PCM, SMPCM, SPCM, BOT and laryngeal box were 0.721, 0.685, 0.731, 0.725 and 0.686, respectively. |
Risk Factors Affecting Overall Survival
The median follow-up time for this study population was 44.0 months (mean 41.7 ± 18.6 months). The OS rate of the whole population was 83.5% (24 deaths within the follow-up period). Cox regression analysis showed that SMPCM mean dose higher than 64.9 Gy (aHR 3.2, 95% CI 1.2–8.8, p=0.021) was a predictor of low OS (Table 5). In addition, older age (>62 years, aHR 2.7, 95% CI 1.1–6.9, p=0.032), N3 status (aHR 4.0, 95% CI 1.8–9.0, p=0.001) and severe (≥ G3) lung infection (aHR 4.6, 95% CI 1.5–14.0, p=0.007) were also prognostic factors for poor OS (Table 5).
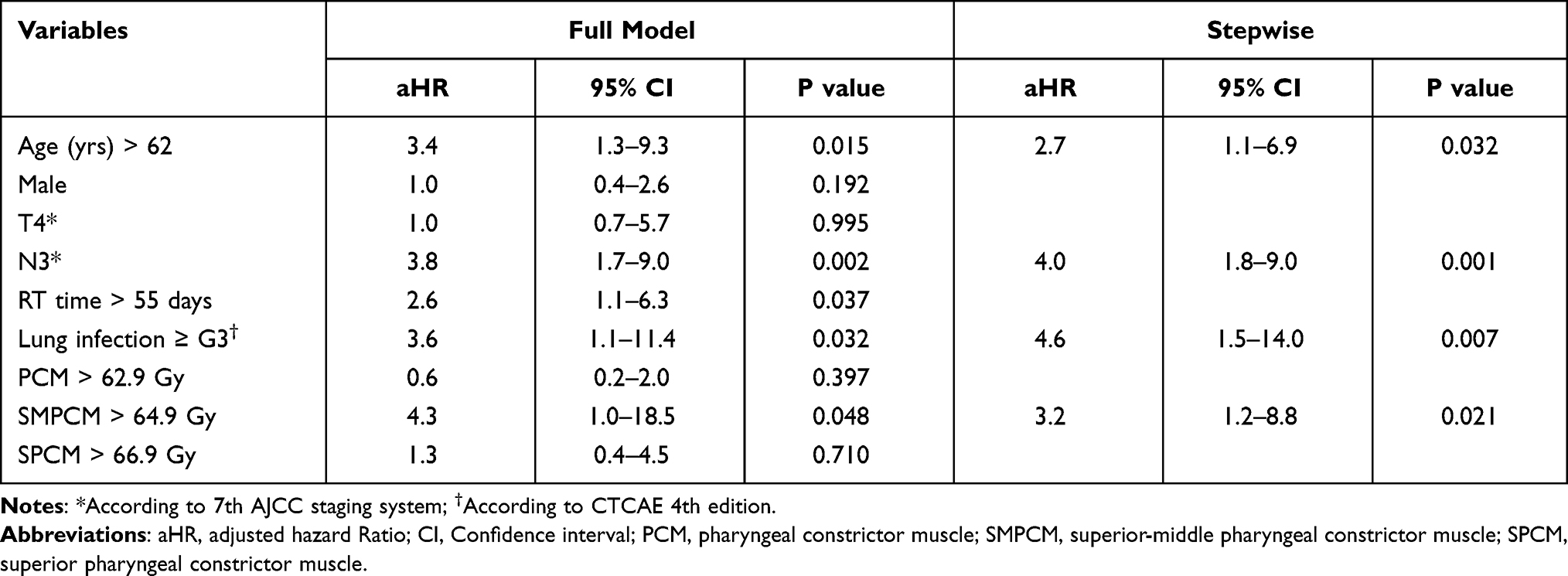 |
Table 5 Prognostic Factors of Overall Mortality Evaluated by Cox Regression (n=185) |
Discussion
IMRT with or without chemotherapy is the standard of care for patients with non-metastatic NPC.2,5,6 Compared to conventional (2D/3D) radiotherapy, IMRT can significantly improve survival1,4,5 and reduce the severity of late effects.4,5,22 However, long-term follow-up studies found that survivors treated with IMRT suffer from many late AEs.7,23 Addressing this issue, researchers have tried to decrease the elective CTV volume or dose to reduce the severity of AEs.9,16,24,25 A recent report on the results of SRVD compared to conventional CTV volume and dose found that SRVD treatment could significantly reduce the ratio of severe (≥ G3) late xerostomia, dysphagia and lung infection.9 Furthermore, it improved the OS by reducing the severe late AE of lung infection (aHR=6.3, 95% CI 1.6–24.2, p=0.007), although it did not improve disease control. Previous studies also found this negative impact on survival caused by severe lung infection after radiotherapy or CCRT.10,11 For example, Xu et al analyzed 3513 head and neck cancer patients who received CCRT, using the SEER-Medicare database. They reported a significantly higher incidence of aspiration pneumonia in these patients than in control populations (5-year rates 23.8% vs 8.7%, respectively, p<0.001).10 Among all head and neck malignant diseases, the diagnosis of NPC was one of the independent risk factors correlated with this event. Most importantly, this AE was associated with a significantly higher risk of death (42% increase, HR 1.42, p<0.001). Another population-based study documented a 5.5% incidence of late-onset pneumonia in NPC patients. After the diagnosis of late-onset pneumonia, 30% (64/210) died within 2 months.11 Hence, if we could identify which factor(s) cause this severe late AE of lung infection in NPC patients, we could devise a strategy to reduce its occurrence.
As early as 2004, Eisbruch et al found that the radiation damage to the pharyngeal constrictors, glottis and supraglottic larynx caused dysphagia and aspiration after radiotherapy combined with gemcitabine CRT in head and neck cancer patients (not including NPC patients).12 They suggested reducing the V50 of dysphagia and aspiration-related structures as a planning and evaluation goal. Levendag et al reviewed 81 patients receiving treatment for oropharyngeal cancer and concluded that every additional 10 Gy added to the mean dose of the superior constrictor muscle (51 Gy) and the middle constrictor muscle (48 Gy) increased the probability of dysphagia 19%.13 Hutchison et al analyzed 53 oropharyngeal cancer patients who received radiotherapy with or without chemotherapy.26 They found a significant correlation between moderate-severe physiological swallowing impairment and doses of > 40 Gy to the extended oral cavity, 50 Gy to the supraglottic/glottic larynx and 60 Gy to the pharyngeal constrictor muscle. As above, many studies have found a significant correlation between a higher dose of swallowing-related OARs and the incidence of post-irradiation dysphagia or aspiration pneumonia.12–14,17,18,25 Petkar et al conduct the first Phase III clinical trial (ISRCTN25458988) that included oropharyngeal and hypopharyngeal cancer patients to validate the role of dysphagia-optimized IMRT.27 However, these studies did not include patients with NPC. The treatment fields and high dose regions differ among NPC, oropharyngeal cancer and other head and neck malignant diseases.3,6 Hence, different conclusions may be drawn on the impact of OARs on the swallowing-related AEs from studies including NPC or oropharyngeal cancer patients. To our best knowledge, this study is the first designed to disclose whether swallowing-related OARs and their doses correlate with severe late dysphagia and pneumonia in NPC patients. Among various OARs, the mean doses of BOT, LB, PCM, SMPCM and SPCM were significantly higher in patients with ≥ G3 dysphagia than those patients without G3 dysphasia (56.2 vs 50.2 Gy, p=0.008; 50.6 vs 46.4 Gy, p=0.036; 65.4 vs 62.1 Gy, p=0.008; 67.1 vs 64.2 Gy, p=0.014; and 69.3 vs 65.8 Gy, p=0.004; respectively) (Table 4). As for patients with ≥ G3 lung infection, the mean doses of PCM, SMPCM and SPCM were significantly higher than in patients without this severe late AE (65.7 Gy vs 62.2 Gy, p=0.036; 68.1 Gy vs 64.2 Gy, p=0.015; 70.0 Gy vs 65.9 Gy, p=0.012; respectively) (Table 4). Not like severe dysphagia, the mean doses of BOT and LB did not reach significant differences between with or without severe late lung infection groups. The above findings were also confirmed by ROC analysis (Figure 1). When patient needed nutritional support and/or rehabilitation of swallow, our multidisciplinary team would take their professional action for them. As expected, the severity of xerostomia did not correlated with any mean doses of OARs. It is well documented that the incidence of xerostomia is correlated with the dosage of parotid glands.28,29 Although the dosage levels differed, our findings of a correlation of higher mean doses of PCM, SMPCM and SPCM with dysphagia and lung infection are compatible with those from studies analyzing patients with oropharyngeal cancer.12–14,17,26 However, we did not find that other OAR structures (such as soft palate, IPCM or CPM) were associated with severe late dysphagia or lung infection in NPC patients. Bhide et al demonstrated that the doses of sub-structures of the pharyngeal constrictor muscles differed significantly by different types of head and neck cancer.30 So, it is reasonable that our finding of significant structures and its dosages (Table 4) were different from previous studies contributed by diseases other than NPC. Among different groupings of patients by T-, N- and Stage, only higher N-status (N2-3 vs N0-1) was significantly correlated with all mean doses of OARs (Table 3). Hence, for NPC patients, we should pay attention to protect these OARs, especially PCM/SMPCM/SPCM in N2-3 patients.
A recent study found that severe dysphagia did not significantly impair survival, but severe late lung infection did.9 Hence, we included those OARs correlation with severe lung infection (PCM, SMPCM and SPCM, Table 4) for Cox regression model calculation. Among these three sub-structures of pharyngeal muscles, only SMPCM > 64.9 Gy (50% quartile) was a risk factor influencing OS (aHR 3.2, 95% CI 1.2–8.8, p=0.021, Table 5). The SMPCM mean dose was not just correlated with the incidence of severe late lung infection; it also affected OS. Besides SMPCM mean dose, the severe late AE of ≥ G3 lung infection (aHR 4.6, p=0.007), N3 status (aHR 4.0, p=0.001) and older age (> 62 years, 75% quartile) (aHR 2.7, p=0.032) significant impaired OS in NPC patients (Table 5). It is well documented that above three risk factors (≥ G3 lung infection, N3 and older age) significantly impair the survival of NPC patients.1,2,9–11,31–33 Clinically, we cannot alter the patient’s characteristics such as N status or age. However, if we could reduce the incidence of severe lung infection (pneumonia), it is highly possible that we could improve the survival of NPC patients. For this purpose, setting a dose constraint of SMPCM, such as less than 64.9 Gy (Table 5), is warranted.
The limitations of this study were stated as follows. The retrospective nature of the study may have introduced selection bias. Not routinely evaluated the status of dysphagia prior to treatment and during the follow-up period by video-fluoroscopy or other objective methods may underrate the incidence of dysphagia. Lastly, the median follow-up time of 44.0 months may have led us to underestimate the incidence of severe late AEs.
Conclusions
Among various swallowing-related OARs, higher mean doses of PCM, SMPCM and SPCM were significantly correlated with the incidence of the severe late AEs of lung infection and dysphagia in NPC patients treated by the IMRT. In addition to older age, N3 disease and severe late lung infection, higher SMPCM mean dose significantly impaired the survival of NPC patients. Limiting the mean dose of SMPCM is warranted, if possible, for reduction of the incidence of severe lung infections and potentially may increase survival in this population.
Abbreviations
NPC, nasopharyngeal carcinoma; IMRT, intensity-modulated radiotherapy; AE, adverse effect; OAR, organs at risk; OS, overall survival; aHR, adjusted Hazard Ratio; PCM, pharyngeal constrictor muscle; SPCM, superior pharyngeal constrictor muscle; MPCM, middle pharyngeal constrictor muscle; IPCM, inferior pharyngeal constrictor muscle; SMPCM, superior-middle pharyngeal constrictor muscle; CPCM, cricopharyngeal constrictor muscle; SP, soft palate; BOT, base of tongue; LB, laryngeal box; CCRT, Concurrent chemoradiotherapy.
Data Sharing Statement
All study data were repositioned at Zenodo (Available at: https://zenodo.org/).
Acknowledgments
The authors thank Miss Hsin-Hui Tseng, Miss Hui-Chi Lai and Miss Yu-Han Yen for their valuable support. The authors would like to thank Convergence CT for assistance with English editing during development of the manuscript. Part of this manuscript was presented at the 60th Annual Meeting of American Society for Radiation Oncology, San Antonio, October 2018. This study was partially supported by grant from Kaohsiung Veterans General Hospital Funding (KSC108-022).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Sun XS, Liu SL, Luo MJ, et al. The association between the development of radiation therapy, image technology, and chemotherapy, and the survival of patients with nasopharyngeal carcinoma: a cohort study from 1990 to 2012. Int J Radiat Oncol Biol Phys. 2019;105:581–590. doi:10.1016/j.ijrobp.2019.06.2549
2. Zhang B, Li MM, Chen WH, et al. Association of chemoradiotherapy regimens and survival among patients with nasopharyngeal carcinoma: a systematic review and meta-analysis. JAMA Netw Open. 2019;2:e1913619. doi:10.1001/jamanetworkopen.2019.13619
3. Lee N, Harris J, Garden AS, et al. Intensity-modulated radiation therapy with or without chemotherapy for nasopharyngeal carcinoma: radiation therapy Oncology group Phase II trial 0225. J Clin Oncol. 2009;27:3684–3690. doi:10.1200/JCO.2008.19.9109
4. Peng G, Wang T, Yang KY, et al. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother Oncol. 2012;104:286–293. doi:10.1016/j.radonc.2012.08.013
5. Zhang B, Mo Z, Du W, et al. Intensity-modulated radiation therapy versus 2D-RT or 3D-CRT for the treatment of nasopharyngeal carcinoma: a systematic review and meta-analysis. Oral Oncol. 2015;51:1041–1046. doi:10.1016/j.oraloncology.2015.08.005
6. Lee AW, Ma BB, Ng WT, Chan AT. Management of nasopharyngeal carcinoma: current practice and future perspective. J Clin Oncol. 2015;33:3356–3364. doi:10.1200/JCO.2015.60.9347
7. McDowell LJ, Rock K, Xu W, et al. Long-term late toxicity, quality of life, and emotional distress in patients with nasopharyngeal carcinoma treated with intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2018;102:340–352. doi:10.1016/j.ijrobp.2018.05.060
8. Wu CH, Hsiao TY, Ko JY, et al. Dysphagia after radiotherapy: endoscopic examination of swallowing in patients with nasopharyngeal carcinoma. Ann Otol Rhinol Laryngol. 2000;109:320–325. doi:10.1177/000348940010900315
9. Liu WS, Tsai KW, Kang BH, et al. Simultaneous reduction of volume and dose in clinical target volume for nasopharyngeal cancer patients. Int J Radiat Oncol Biol Phys. 2021;109:495–504. doi:10.1016/j.ijrobp.2020.09.034
10. Xu B, Boero IJ, Hwang L, et al. Aspiration pneumonia after concurrent chemoradiotherapy for head and neck cancer. Cancer. 2015;121:1303–1311. doi:10.1002/cncr.29207
11. Yen TT, Lin CH, Jiang RS, et al. Incidence of late-onset pneumonia in patients after treatment with radiotherapy for nasopharyngeal carcinoma: a nationwide population-based study. Head Neck. 2015;37:1756–1761. doi:10.1002/hed.23827
12. Eisbruch A, Schwartz M, Rasch C, et al. Dysphagia and aspiration after chemoradiotherapy for head-and-neck cancer: which anatomic structures are affected and can they be spared by IMRT? Int J Radiat Oncol Biol Phys. 2004;60:1425–1439. doi:10.1016/j.ijrobp.2004.05.050
13. Levendag PC, Teguh DN, Voet P, et al. Dysphagia disorders in patients with cancer of the oropharynx are significantly affected by the radiation therapy dose to the superior and middle constrictor muscle: a dose-effect relationship. Radiother Oncol. 2007;85(1):64–73. doi:10.1016/j.radonc.2007.07.009
14. Head MA, Hutcheson K, Mohamed ASR. Neck Cancer Symptom Working Group: beyond mean pharyngeal constrictor dose for beam path toxicity in non-target swallowing muscles: dose-volume correlates of chronic radiation-associated dysphagia (RAD) after oropharyngeal intensity modulated radiotherapy. Ra Oncol. 2016;118(2):304–314. doi:10.1016/j.radonc.2016.01.019
15. Edge SB, Byrd DR, Compton CC, et al. Editors. AJCC Cancer Staging Manual.
16. Lin S, Pan J, Han L, et al. Nasopharyngeal carcinoma treated with reduced-volume intensity-modulated radiation therapy: report on the 3-year outcome of a prospective series. Int J Radiat Oncol Biol Phys. 2009;75:1071–1078. doi:10.1016/j.ijrobp.2008.12.015
17. Mortensen HR, Jensen K, Aksglæde K, et al. Late dysphagia after IMRT for head and neck cancer and correlation with dose–volume parameters. Radiother Oncol. 2013;107(3):288–294. doi:10.1016/j.radonc.2013.06.001
18. Sanguineti G, Adapala P, Endres EJ, et al. Dosimetric predictors of laryngeal edema. Int J Radiat Oncol Biol Phys. 2007;68(3):741–749. doi:10.1016/j.ijrobp.2007.01.010
19. Brouwer CL, Steenbakkers RJ, Bourhis J, et al. CT-based delineation of organs at risk in the head and neck region: DAHANCA, EORTC, GORTEC, HKNPCSG, NCIC CTG, NCRI, NRG Oncology and TROG consensus guidelines. Radiother Oncol. 2015;117(1):83–90. doi:10.1016/j.radonc.2015.07.041
20. Christianen ME, Langendijk JA, Westerlaan HE, et al. Delineation of organs at risk involved in swallowing for radiotherapy treatment planning. Radiother Oncol. 2011;101(3):394–402. doi:10.1016/j.radonc.2011.05.015
21. National Cancer Institute. Common Terminology Criteria for Adverse Events v.4.0 (CTCAE); 2010. Available from: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
22. Chen YY, Zhao C, Wang J, et al. Intensity-modulated radiation therapy reduces radiation-induced trismus in patients with nasopharyngeal carcinoma: a prospective study with >5 years of follow-up. Cancer. 2011;117:2910–2916. doi:10.1002/cncr.25773
23. Wang JJ, Jiang RS, Yen TT, et al. Risk factors for recurrent pneumonia in post-irradiated patients with nasopharyngeal carcinoma. J Chin Med Assoc. 2017;80:558–562. doi:10.1016/j.jcma.2017.01.006
24. Li M, Huang XG, Yang ZN, et al. Effects of omitting elective neck irradiation to nodal level IB in nasopharyngeal carcinoma patients with negative level IB lymph nodes treated by intensity-modulated radiotherapy: a Phase 2 study. Br J Radiol. 2016;89:20150621. doi:10.1259/bjr.20150621
25. Cho WK, Oh D, Lee E, et al. Feasibility of selective neck irradiation with lower elective radiation dose in treating nasopharynx cancer patients. Cancer Res Treat. 2019;51:603–610. doi:10.4143/crt.2018.240
26. Hutchison AR, Wishart LR, Brown B, et al. Exploring the interplay between radiotherapy dose and physiological changes in the swallowing mechanism in patients undergoing (chemo) radiotherapy for oropharynx cancer. Dysphagia. 2021. doi:10.1007/s00455-021-10307-2
27. Petkar I, Rooney K, Roe JW, et al. DARS: a phase III randomised multicentre study of dysphagia- optimised intensity- modulated radiotherapy (Do-IMRT) versus standard intensity- modulated radiotherapy (S-IMRT) in head and neck cancer. BMC Cancer. 2016;16:770. doi:10.1186/s12885-016-2813-0
28. Liu WS, Kuo HC, Lin JC, et al. Assessment of salivary function change in nasopharyngeal carcinoma treated by parotid-sparing radiotherapy. Cancer J. 2006;12:494. doi:10.1097/00130404-200611000-00009
29. Lou J, Huang P, Ma C, et al. Parotid gland radiation dose-xerostomia relationships based on actual delivered dose for nasopharyngeal carcinoma. J Appl Clin Med Phys. 2018;19:251–260. doi:10.1002/acm2.12327
30. Bhide SA, Gulliford S, Kazi R, et al. Correlation between dose to the pharyngeal constrictors and patient quality of life and late dysphagia following chemo-IMRT for head and neck cancer. Radiother Oncol. 2009;93:539–544. doi:10.1016/j.radonc.2009.09.017
31. Au KH, Ngan RKC, Ng AWY, et al. Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in Hong Kong: a report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018;77:16–21. doi:10.1016/j.oraloncology.2017.12.004
32. Jiang Y, Qu S, Pan X, et al. Prognostic nomogram for locoregionally advanced nasopharyngeal carcinoma. Sci Rep. 2020;10:861. doi:10.1038/s41598-020-57968-x
33. Fei Z, Qiu X, Mengying L, et al. Prognosis viewing for nasopharyngeal carcinoma treated with intensity-modulated radiation therapy: application of nomogram and decision curve analysis. Jpn J Clin Oncol. 2020;50:159–168. doi:10.1093/jjco/hyz165
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.