Back to Journals » Infection and Drug Resistance » Volume 15
High Prevalence of Asymptomatic Nasopharyngeal Carriage Rate and Multidrug Resistance Pattern of Streptococcus pneumoniae Among Pre-School Children in North Showa Ethiopia
Authors Tilahun M ![]() , Fiseha M
, Fiseha M ![]() , Ebrahim E
, Ebrahim E ![]() , Ali S, Belete MA
, Ali S, Belete MA ![]() , Seid A, Demsiss W, Gedefie A
, Seid A, Demsiss W, Gedefie A ![]() , Tadesse S, Belayhun C
, Tadesse S, Belayhun C
Received 2 June 2022
Accepted for publication 1 August 2022
Published 5 August 2022 Volume 2022:15 Pages 4253—4268
DOI https://doi.org/10.2147/IDR.S377186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Mihret Tilahun,1 Mesfin Fiseha,1 Endris Ebrahim,1 Seada Ali,1 Melaku Ashagrie Belete,1 Abdurahaman Seid,1 Wondmagegn Demsiss,1 Alemu Gedefie,1 Selamyhun Tadesse,2 Chernet Belayhun3
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Medical Laboratory Science, College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia; 3Department of Medical Laboratory Science, Mehal Meda Hospital, Mehal Meda, North Showa, Ethiopia
Correspondence: Mihret Tilahun, Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, 1145, Ethiopia, Tel +251- 913867849, Email [email protected]
Background: Streptococcus pneumoniae infection is still the world’s most serious public health problem among children under the age of five. Nasopharyngeal carriage rate of Streptococcus pneumoniae has been identified as an important risk factor for the acquisition of community acquired respiratory tract infection. To date, little is known about the nasopharyngeal infection and antimicrobial susceptibility pattern of Streptococcus pneumoniae among preschool children in Ethiopia.
Objective: The aim of this study was to assess the prevalence of nasopharyngeal carriage and antimicrobial susceptibility pattern of Streptococcus pneumoniae among preschool children.
Methods: A cross-sectional study was conducted from September 2021 to April 2022. A total of 418 preschool children were enrolled using a multistage sampling technique. Nasopharyngeal swab was collected and transported to Medical Microbiology Laboratory at Debre Berhan comprehensive specialized hospital using skim-milk tryptone glucose glycerol transport media. The swab was inoculated on blood agar plates supplemented with 5μg/mL gentamycin and incubated at 37°C for 24– 48 hours under 5% CO2 using a candle jar. Identification of Streptococcus pneumoniae was performed using Gram stain, catalase test, optochin test and bile solubility test. Antimicrobial sensitivity tests were done using a modified Kirby-Bauer disk diffusion method. Data were entered into the statistical package Epi data 4.0.0.6 and transferred to and analyzed using SPSS software version-23. A P-value ≤ 0.05 with 95% CI was considered to be statistically significant.
Results: The prevalence of Streptococcus pneumoniae nasopharyngeal carriage was 29.9% (125/418). The overall rate of multidrug resistance was 86 (68.8%), with tetracycline (68.8%) and TMP-SMX (68%). Among risk factors, young age and passive smoking were associated with pneumococcal carriage.
Conclusion: The present study revealed a substantially lower prevalence of Streptococcus pneumoniae nasopharyngeal carriage. High antimicrobial resistance was observed for most antimicrobial drugs tested. Younger age groups and passive smokers were at risk of Streptococcus pneumoniae nasopharyngeal carriage.
Keywords: Streptococcus pneumoniae, nasopharyngeal carriage, antimicrobial susceptibility
Corrigendum for this paper has been published.
Introduction
Streptococcus pneumoniae (S. pneumoniae) is a gram-positive, facultative anaerobic bacteria that exists in 100 different serotypes. All serotypes of S. pneumoniae can cause disease, only a small number of serotypes cause the bulk of pneumococcal infections.1 S. pneumoniae is found in the upper respiratory tract as normal flora and colonizes the nasopharyngeal area.2 However, it can progress to respiratory or even systemic disease.3 S. pneumoniae (Pneumococcus) is a major pathogen that can cause mortality over one million children each year throughout the world. Pneumococcus pneumonia is a common and often severe illness in children.4 Nasopharyngeal carriage has a role in the development of invasive and non-invasive disease if pneumococci disseminate to other areas of the respiratory system. Because nasopharyngeal colonization often precedes invasive disease, it can act as a reservoir for disease spread in the host population. As a result, asymptomatic carriage is now thought to be a risk factor for S. pneumoniae disease.5 Air droplets disseminate S. pneumoniae from person to person through coughing, sneezing, and close contact with people who are carriers or sick.6
Nasopharynx is recognized to be S. pneumoniae primary environmental habitat, from which it can spread to other parts of the respiratory system or enter normally sterile bodily fluids to cause sickness.3 Nasopharyngeal colonization by antibiotic-resistant S. pneumoniae has steadily increased over the last few years in many countries, including Ethiopia.7–9 Resistance to common antibiotics, particularly penicillin, has been shown to be on the rise. A change in penicillin-binding proteins (PBPs) causes beta-lactam resistance in S. pneumoniae. The number of PBP alterations determines the level of resistance. The beta lactam agent’s binding affinity to S. pneumoniae is reduced as a result of the altered PBPs.10
S. pneumoniae is the most common cause of sickness and mortality worldwide. Mortality attributed to pneumococcal diseases is expected to kill at least one million children under the age of five every year. More than 70% of them are in developing countries.11 Invasive pneumococcal disease (IPD) is a major cause of morbidity and mortality around the world. Despite the availability of effective antibiotics and vaccines, around 14.5 million severe pneumococcal infections occur worldwide each year. Of these, 825,000 occur in children under the age of five, accounting for 11% of total infant mortality.12 In Ethiopia, the mortality rate from pneumococcal disease has been 21%13 because of their immature immune systems and frequent exposure to and colonization by pneumococcal strains, preschool children are the most vulnerable to invasive pneumococcal illness.14 S. pneumoniae infections cause pneumonia, meningitis, bacteremia, sinusitis, and otitis media, and their associated morbidity and mortality place a considerable financial burden on society.15
In industrialized countries and high-income populations, the prevalence of nasopharyngeal carriage of S. pneumoniae in preschool children is lower, and the average carriage prevalence usually settles at a lower level, about 20–50%. The turnover and acquisition of novel strains is rapid in high-risk populations with a high burden of pneumococcal illness, and pneumococcal carriage is common.16–20 Several factors, including environmental and socioeconomic factors, overcrowding circumstances, and antibiotic overuse, appear to influence the nasopharyngeal colonization of S. pneumoniae, according to several research.21–23
Antibiotic resistance in S. pneumoniae is gradually becoming a severe public health issue. Multidrug-resistant (MDR) S. pneumoniae isolates have been observed in 15–30% of S. pneumoniae isolates worldwide.24,25 Antimicrobial-resistant S. pneumoniae colonization of the nasopharynx has been rising in several parts of the world, including Ethiopia. S. pneumoniae resistance to penicillin (64.5%) and tetracycline (53.2%) was observed in Hawassa and Jimma, respectively, in Ethiopia.8,26 In Ethiopia, empirical therapy plays a big role in antibiotic selection. As a result, immunization is a viable option for preventing pneumococcal illness and lowering nasopharyngeal carriage. Despite the use of PCV in Ethiopia since 2011, hospital-based research has revealed that nasopharyngeal carriage is still a problem among youngsters.8,27 However, to date, there are little data conducted on S. pneumoniae prevalence of nasopharyngeal carriage, antimicrobial susceptibility pattern and associated risk factors in the community. Therefore, the aim of this study is to assess the prevalence of nasopharyngeal carriage, antimicrobial susceptibility pattern and associated risk factors of S. pneumoniae among preschool children attending nurseries and daycare centers at Debre Berhan North Showa Ethiopia.
Materials and Methods
Study Area and Period
A community-based cross-sectional study was conducted from September 2021 to April 2022 at selected kindergartens and day care centers in Debre Berhan town, North Shewa, Ethiopia. The town is located 130 km from the capital city of the country, Addis Ababa, and 587 km from Bahir Dar, which is the capital city of the Amhara regional state. The town has 18 kebeles (small administrative). According to the 2007 G.C population and housing census results in Ethiopia, the town had a total population of 155,987.36 In Debre Berhan town, there are 30 governmental and 15 private kindergartens with a total of 15,237 children; and 2 day-care centers, which had 33 (21 males and 12 females) children.
Source and Target Population
All children attending nurseries and daycare centers were the source population. Whereas the target population was all children attending selected nurseries and day care centers during the study period.
Inclusion Criteria and Exclusion Criteria
All children 1–6 years of age attending selected nurseries and daycare centers were included in the study. Whereas, children who had been on antibiotics for the previous two weeks, children with nasopharyngeal malformations or trauma, children with any signs or symptoms of respiratory disease, and children who were not brought to school by their parents or guardians were excluded from the study.
Study Variables
The dependent variables are the prevalence of S. pneumoniae and antimicrobial susceptibility pattern. Whereas, age, sex, income, parents’ educational background, occupation, bed sharing with parents, passive smoking, family size, sibling, PCV immunization, hospitalization history, waiting time in daycare center/kindergarten, number of students in one class room, and previous history of respiratory tract infection.
Sample Size Determination and Sampling Technique
The sample size was calculated using a single population proportion formula with the prevalence of nasopharyngeal S. pneumoniae carriage taken from previous study done in Bahir Dar town,28 which was 44.8%, a 5% margin of error, and a 95% confidence interval of 1.96 by using the sample size calculation formula below:

where n is the minimal sample size, Za/2 is the 95% of confidence interval significant value, p is the predicted frequency of S. pneumoniae, and d is the margin of error. A total sample size was 418 with considering a 10% non-response rate.
Sampling Technique
A multistage sampling technique was used to select nurseries and day care centers by using a simple random sampling technique (lottery method). Nine kindergartens were selected randomly with a 1:2 private to government kindergarten proportion, and the two-day care centers were included. We determine the sample size of each kindergarten and day-care center by allocating a sampling proportional to the total number of children of each kindergarten and day care center using the formula: ni =  . Stratifying the kindergartens into KGs and the numbers of study participants were allocated proportionally to each KG based on the kindergartens’ sampling frame (registration book or attendance list), and 418 study participants were selected by a simple random sampling technique (lottery method). However, stratification was unnecessary in daycare centers because all children were in nearly equal age groups (1–2 years of age).
. Stratifying the kindergartens into KGs and the numbers of study participants were allocated proportionally to each KG based on the kindergartens’ sampling frame (registration book or attendance list), and 418 study participants were selected by a simple random sampling technique (lottery method). However, stratification was unnecessary in daycare centers because all children were in nearly equal age groups (1–2 years of age).
Data Collection
Socio-demographic information and clinical data were collected by trained nurses and principal investigators using a pretested standardized questionnaire guided by interview. Demographic characteristics such as child age, gender, educational status of parents, occupation of parents, average monthly income, and associated factors such as grade level of students, occupation of parents, bed-sharing with parents, passive smoking, family size, food cooking tools in the house, previous history of hospitalization, and a single nasopharyngeal swab sample were collected from each study participant after appropriate instructions were given; The status of a PCV vaccinated child was from their vaccination card.
Nasopharyngeal Sample Collection, Transportation and Processing
A nasopharyngeal specimen was collected from each child using a sterile flexible flocked swab (Copan Italia s.p.a.). The swab was placed in a sterile tube containing skim-milk tryptone glucose glycerol transport medium and transmitted to the Medical Microbiology Laboratory at Debre Berhan comprehensive specialized hospital. The specimens were inoculated into blood agar base (HiMediaTM) supplemented with 5% sheep blood and 5g/mL gentamycin plates by rolling the swab over a small part of the plate and streaking the sample with a sterile loop. The medium was incubated in a 5% CO2-enriched environment in a candle jar at 37°C for 24–48 hours.29 Suspect colonies with a greenish colony (alpha hemolytic) were sub-cultured on blood agar with 5 g Optochin disks (Mumbai, India) and then incubated at 37°C in a 5% CO2 enriched atmosphere for 24 hours.30
Isolation and Identification of S. pneumoniae
The bacteria isolate was characterized using colony morphology, haemolysis pattern, Gram staining reaction, and a panel of biochemical tests following the standard microbiological procedure. Gram-positive cocci were distinguished and recognized based on Gram stain, blood agar haemolysis patterns, colonial characteristics, catalase test, coagulase test, mannitol fermentation test, and optochin (5μg) susceptibility. Optochin susceptible strains ≥14 mm in diameter of the zone of inhibition were identified as S. pneumoniae; strains with zones of inhibition <14 mm were subjected to a bile solubility test (tube method) using 2% sodium deoxycholate or bile salt (Oxoid Ltd.).31
Antimicrobial Susceptibility Testing
Briefly, 3–5 pure colonies were added to 5 mL of normal saline and compared with 0.5 McFarland turbidity standards. A sterile cotton swab was dipped into the adjusted suspension, and the excess was removed by gentle rotation of the swab against the inside wall of the tube. The swab was inoculated evenly over the entire surface of Mueller–Hinton agar (HiMediaTM) supplemented with 5% sheep blood, and then the inoculated plates were allowed to air dry for 15 minutes. The disks were placed aseptically on the plate using sterile forceps, and the plates were incubated at 37°C for 24 hours in a 5% CO2 atmosphere. All isolates of S. Pneumoniae were tested against penicillin (10 μg), tetracycline (30 μg), chloramphenicol (30 μg), clindamycin (30 μg), trimethoprim-sulfamethoxazole (1.25/23.75 μg), cefotaxime (30μg), ceftriaxone (30 μg), erythromycin (15μg), and oxacillin (30 μg) for antimicrobial agents.32 The antimicrobial agents were selected based on the Clinical and Laboratory Standard Institute (CLSI) 2021.33 Finally, the inhibition zone diameter was measured to the nearest millimetres using a ruler. The interpretation of the results of antimicrobial susceptibility tests was based on a standardized table supplied by CLSI 2021.33 The results were interpretive as sensitive, intermediate or resistant. Moreover, an isolate was considered MDR if it is resistant to at least one agent in three or more antimicrobial categories 2021.33
Operational Definitions
Nasopharyngeal colonization: the presence of bacteria in nasopharynx without causing disease.
MDR: bacteria being resistant to three or more classes (penicillin and two/more non-beta lactam antimicrobials).
Recent exposure to antibiotics: consumption of any antibiotic in the 3 months prior to the data collection.
Recent hospitalization: stay in hospital for 3 months prior to the data collection.
Previous respiratory tract infection: the presence of respiratory tract infections in the 3 months prior to the data collection.
Quality Assurance
Training was given for data collectors, and the completeness of the questionnaires was checked by the principal investigator. Cultural outcome reliability was ensured by the implementation of standard quality control measures across the entire process, and standard operating procedures (SOPs) were followed. Quality control of culture media was verified for sterility testing by overnight incubation of 5% of one uninoculated plate/tube of the prepared media from each batch. Positive and negative controls were used for biochemical media; and visual inspections of holes, uneven filling, and haemolysis, signs of freezing, bubbles, and corrosion in media or plastic Petri dishes were conducted to check the quality of all prepared culture media. Moreover, the standard reference strains of S. aaureus (ATCC-25923), E. coli (ATCC-25922), and P. aeruginosa (ATCC-27853) and for fastidious organisms, H. influenzae (ATCC 49247) and S. pneumoniae (ATCC 49619) were used as control strains.
Statistical Analysis
The data generated were entered every day into the epi-data version 4.6.0.4. The data was then exported and analysed using the Social Sciences Statistical Package (SPSS) version 25. The frequency and percentage descriptive statistics were calculated and presented using graphs and tables. A bivariable analysis was conducted in order to classify factors that separately affect the frequency of dependent variables. Variables with a P-value less than or equal to 0.25 in bivariable analysis were subjected to multi-variable analysis. Adjusted odds ratio with a p value of <0.05 and 95% CI taken as statistically significant. Finally, the results were presented in words, graphs, and tables.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the ethical review committee of the College of Medicine and Health Sciences, Wollo University, ethical clearance was obtained with approval number CMHS/MLS-24/018/2014. Prior to commencing the study, written informed consent was obtained from each study participant. Prior to commencing the study, an ascent was provided from each study participants; and informed consent was obtained from the parent’/guardians. Confidentiality and any special data security requirements were maintained and assured throughout the study. All data and samples collected from them were kept confidential and used only for the purpose of the study. The positives were communicated with their physicians so that study participants got the respective treatment and management accordingly.
Results
Sociodemographic and Clinical Characteristics of the Study Participants
A total of 418 children were enrolled with a 100% response in this study, of whom 220 (52.6%) were female. The median age was 5, with a range of 1–6 years. Two hundred twenty-four (53.6%) of the children lived in households with fewer than five people. The majority of the children 380 (90.9%) were fully vaccinated. One hundred and sixty-three (39%) children were taking antibiotics within the past 3 months of enrolment. The majority of fathers (35.9%) and mothers’ educational level (134, 32.1%) were from primary school. Of the total children enrolled, 116 (27.8%) were found to have respiratory illness (Table 1).
 |
Table 1 Socio-Demographic and Clinical Characteristics of Study Participants Among Preschool Children in Kindergartens and Day Care Centers in Gondar Town North West Ethiopia, 2022 |
Nasopharyngeal Carriage Rate of S. pneumoniae
The overall prevalence of nasopharyngeal carriage of S. pneumoniae was 29.9% (125/418) (95% CI: 22.3–32.4). Carriage was common at a younger age group of 1 to 4 years old with a prevalence of 29.8% (28 of 94). Streptococcus pneumoniae carriage was high in partially immunized (2/4) and passive smoking-exposed children (6/13). Streptococcus pneumoniae carriage in children having respiratory tract infections prior to 3 months from data collection was 14 (30.4%) (Table 1).
Antimicrobial Susceptibility Pattern of S. pneumoniae Isolated
The Streptococcus pneumoniae isolates showed a higher level of drug resistance to tetracycline (68.8%) and TMP-SMX (68%). While erythromycin oxacillin (40.8%), cefotaxime (39.2%), penicillin (36%), chloramphenicol (47.2%), and clindamycin (29.6%) showed low levels of resistance (Table 2).
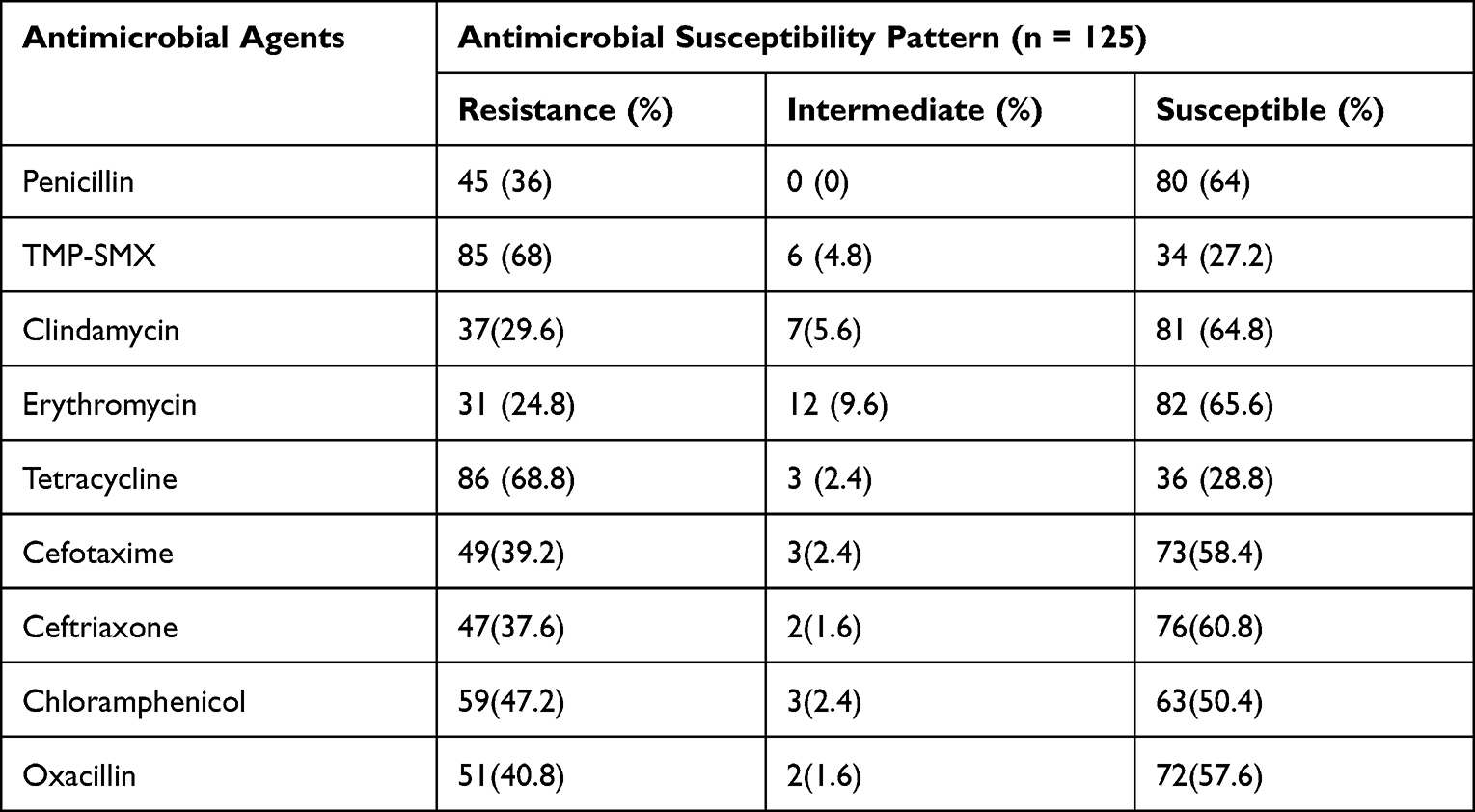 |
Table 2 Antimicrobial Susceptibility Pattern of S. pneumoniae Among Preschool Children in Kindergarten and Day Care Centers in Gondar Town, North West Ethiopia, 2022 |
Multiple Drug Resistance Pattern of the Isolates
Overall, 112 (89.6%) of streptococcus pneumoniae isolates were resistant to at least one antimicrobial agent, whereas 101 (80.8%) of isolates were resistant to ≥2 antimicrobials. Multidrug resistance (defined as resistance to at least one agent in three or more antimicrobial categories) was seen in 86 (68.8%) of the Streptococcus pneumoniae isolates and 31.2 of the isolates were non-multidrug resistance (Figure 1 and Table 3).
 |
Table 3 Multi Drug Resistance Pattern of S. pneumoniae Among Preschool Children in Kindergarten and Day Care Centers in Gondar Town, North West Ethiopia, 2022 |
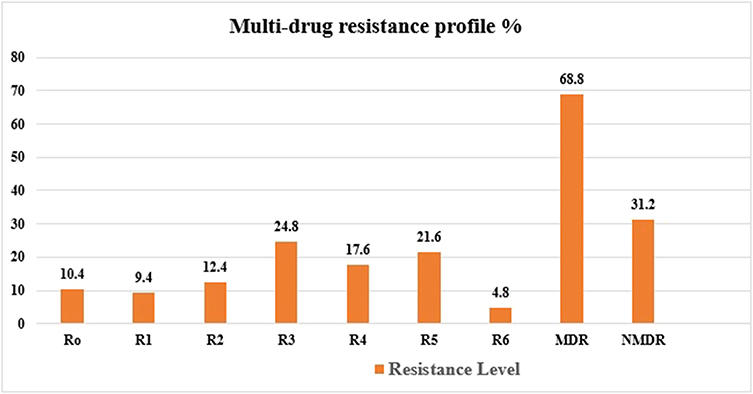 |
Figure 1 Multi-drug resistance pattern S. pneumoniae among preschool children in kindergartens and day care centers in Debre Berhan town North West Ethiopia, 2022. Abbreviations: MDR, multi-drug resistance; R0, no antibiotic resistance; R1 to R7, resistance to 1 antimicrobial class category to 6 antimicrobial categories. |
Risk Factors for Nasopharyngeal Carriage of S. pneumoniae
In the current study, bivariate analysis was performed and sociodemographic and facility characteristics such as sex, family size, siblings, bed sharing with parents, immunization status, food preparation tools in the house, education level of mother and father, average monthly income, and occupation were not significantly associated with nasopharyngeal bacteria carriage. However, age, grade level, number of rooms in the house, number of rooms in the house, respiratory tract infections in the past 3 months, passive smoking, number of children in one class, and mothers’ education level were associated with COR and subjected to multivariate analysis. Age 1–2 years [AOR = 4.87, 95% CI: 1.11–23.47, P = 0.021], numbers of rooms <2 per house [AOR = 3.45, 95% CI: 1.53–31.88, P = 0.012], having history of hospitalization [AOR = 3.5, 95% CI: 1.85–25.74, P = 0.002], having history of respiratory tract infection [AOR = 4.52, 95% CI: 1.78–24.65, P = 0.025], passive smoking [AOR = 4.75, 95% CI: 1.88–31.85, P = 0.031], and number of students >60 in the classroom [AOR = 5.78, 95% CI: 1.66–35.52, P = 0.001] and mothers who were Illiterate [AOR = 4.54, 95% CI: 1.22–32.67, P = 0.0012] were statistically significant associated risk factors for nasopharyngeal bacteria carriage (Table 4).
 | 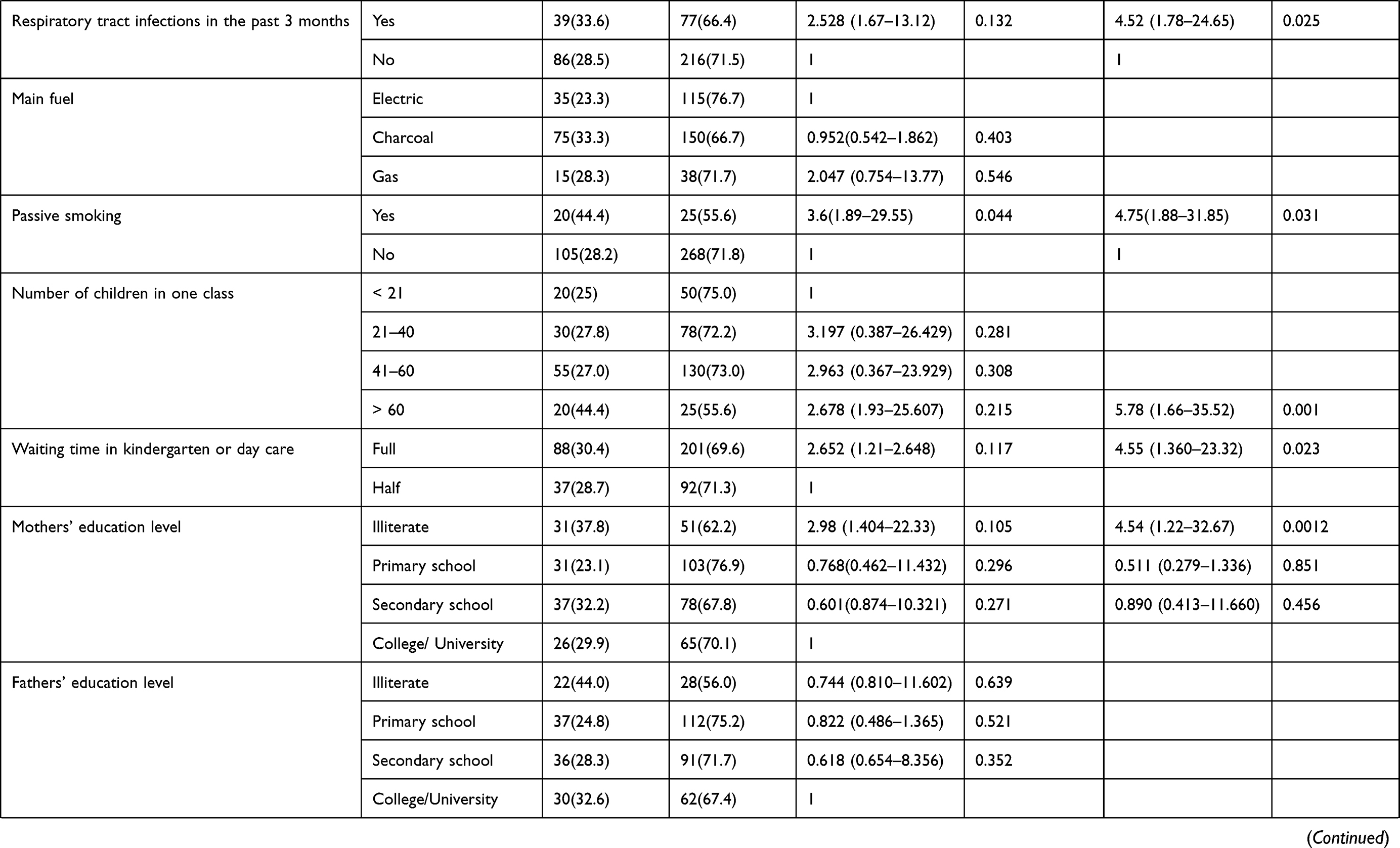 | 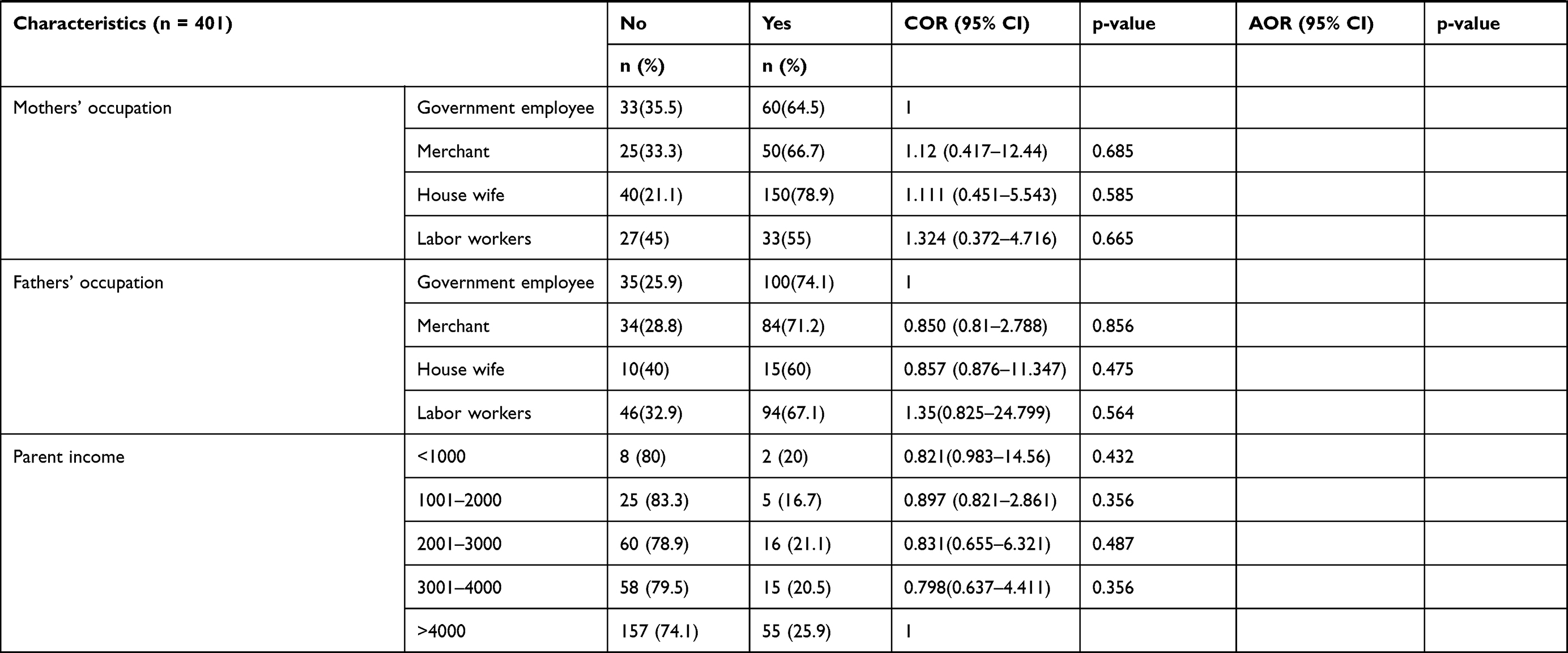 |
Table 4 Bivariate and Multivariate Analyses of Risk Factors Associated with S. pneumoniae Among Preschool Children in Kindergartens and Day Care Centers in Debre Berhan North West Ethiopia, 2022 |
Discussion
The asymptomatic nasopharyngeal carriage of S. pneumoniae is common in young children and has been linked to illness development and pathogen dissemination in the community. The prevalence of S. pneumoniae nasopharyngeal carriage varies with age, geographical area, crowding, concomitant respiratory tract illness, nutritional condition, and sample procedure. We assessed the prevalence of asymptomatic nasopharyngeal carriage and the multidrug resistance pattern of Streptococcus pneumoniae in pre-school children in North East Ethiopia. Several studies in various parts of the world have revealed a wide range of S. pneumoniae nasal carriage rates. In the present study, the overall prevalence of S. pneumoniae nasopharyngeal carriage was 29.9% (95% CI: 24.9–34.8), which lies between the low carriage rate of 2.8% and the high rate of 58.6% in different areas of the world.34,35 The carriage rate was comparable to the study done in India 27%36 and Tanzania 35.0%.37 However, the finding of the current study was lower than studies done in Brazil 43.4%,38 Indonesia 43%,39 Nigeria 42.2%,40 Uganda 58.6%,35 Jimma 43.8%8 and Gondar 41.0%27 and higher than studies done in Turkey 2.8%34 and Iran 15.7%.25 These differences might be related to sampling, characteristics of the population studied (the age, residence, having siblings, presence of respiratory tract infection, vaccination status) and laboratory methods. The children who visited the hospital may have had undetected underlying immunosuppressive problems in addition to hunger, which motivated them to seek medical assistance; these could be contributing factors to our finding of increased carriage.
In this study, a substantially lower prevalence was detected as compared to the previous studies. This might be because most of the 307 (76.6%) children recruited were 5 to 6 years old. The decrease in S. pneumoniae carriage rate associated with increasing age may reflect the gradual development of mucosal immunity and progressive increase in clearance rates. Moreover, 97.3% of the children included in the present study were fully vaccinated and apparently healthy.
Antimicrobial resistance has been recognized as an emerging worldwide problem both in developed and developing countries. The increased uses of antimicrobial agents are a significant factor in the emergence of antibiotic resistant bacteria.41 Treatment of S. pneumonia infections has become a complex global problem due to antibiotic resistance, and it is becoming more difficult to treat as the drugs used to treat them grow less effective. Antibiotic resistance results in longer hospital stays, higher medical expenses, and higher fatality rates.42 In this study, the majority 86/125 (68.8%) and 85/125 (68%) of the isolates tested were resistant to tetracycline and trimethoprim-sulfamethoxazole, respectively. However, the resistance level of tetracycline and trimethoprim-sulfamethoxazole were lower in developed countries as compared to the current study.34,36 This may be because tetracycline is one of the most widely used antimicrobials in most public and private health care settings. It has been used in the community to treat respiratory tract infections (symptoms) without a prescription (self-medication). Tetracycline, on the other hand, has been linked to tooth retardation in children under the age of eight, making it less suited for oral usage in children. In our study, excessive consumption, unsuitable use, and overuse of TMP-SMX may be contributing reasons for S. pneumoniae resistance to these antibiotics. TMP-SMX has been widely utilized to treat respiratory tract infections because of its broad antibacterial coverage, synergistic effects, and low cost. The pneumococcal nasopharyngeal isolates also demonstrated resistance to other antimicrobial agents like erythromycin, penicillin, tetracycline, and clindamycin. In this study, 27.9% of isolates were resistant to penicillin. This finding was in line with the study conducted in Brazil, which found 28.8%.38 However, higher proportions of S. pneumoniae were reported in Iran (73%25 and Jimma 36.1%).8 This difference might be due to methodology differences; most of the studies used dilution techniques, and the low resistance rates of isolated S. pneumoniae to clindamycin might be due to the restricted use of some antibiotics in the community.
Multi-drug and antibiotic resistance in Streptococcus pneumoniae is a growing public health concern around the world. Antimicrobial-resistant S. pneumoniae is becoming more common, and nasal colonization of S. pneumoniae in children increases the risk of pneumococcal illness. This has been reported in many parts of the globe.43,44 Penicillin susceptibility is an essential indicator of whether or not a multidrug resistant phenotype exists. Penicillin-resistant strains are typically cross-resistant to other antibiotics. Prolonged carriage and quick reacquisition increase the likelihood of antibiotic exposure and may thus be a major selection factor in predisposing to antibiotic resistance.45 In our study, 68.8% of the isolates were multi-drug resistance. The majority of MDR isolates consist of resistance to penicillin, TMP-SMX, and tetracycline. The occurrence of MDR was higher than the findings of other studies conducted in India 19%36 Jimma 17.7%27 and Gondar 6.3%.27 The high MDR observed in this study might be due to the administration of multiple antimicrobials for infections and indiscriminate use of antimicrobials. This might be due to S. pneumoniae developing a beta-lactam resistance pathway, which includes genetic changes that alter the structure of penicillin-binding proteins, resulting in a lower affinity for all beta-lactam medicines.
Various demographic characteristics in different studies have been described to be associated with an increase in S. Pneumoniae carriage, including, age 1–2 years [AOR = 4.87, 95% CI: 1.11–23.47, P = 0.021], having a history of hospitalization [AOR = 3.5, 95% CI: 1.85–25.74, P = 0.002], having a history of respiratory tract infection [AOR = 4.52, 95% CI: 1.78–24.65, P = 0.025], passive smoking [AOR = 4.75, 95% CI: 1.88–31.85, P = 0.031], and number of students >60 in the classroom [AOR = 5.78, 95% CI: 1.66–35.52, P=0.001], and mothers who were illiterate [AOR = 4.54, 95% CI: 1.22–32.67, P = 0.0012]. This finding was consistent with studies performed in Gondar, North West Ethiopia,27 India36 and Indonesia.39 This can be explained by the fact that younger children are immunologically immature and carry S. pneumoniae in their nasopharynx in high magnitude. We also found an increased carriage of S. pneumoniae in children who were exposed to passive smoking. This was also in agreement with reports in Indonesia.39 This might be due to the fact that smoke damages and inflames nasopharyngeal mucosa, increasing susceptibility to S. pneumoniae colonization. A previous study in Gondar town27 discovered that having 5 year old siblings and only one room in the house were risk factors for S. pneumoniae nasopharyngeal carriage in children. But in this study, none of them were associated with S. pneumoniae carriage. The differences observed in this study might be due to changes in the epidemiologic characteristics of pneumococcal carriage in Ethiopia.
Conclusions and Recommendations
Among a total of 418 samples collected from pre-school children, the asymptomatic S. pneumoniae carriage rate was 29.9% (125/418). The overall MDR rate of isolated bacteria was 86 (68.8%). The Streptococcus pneumoniae isolates showed a higher level of drug resistance to tetracycline (68.8%) and TMP-SMX (68%). However, the most effective drugs were penicillin and clindamycin. Nasopharyngeal bacteria carriage in asymptomatic children is alarming for community-acquired infection. Children who had a history of hospitalization, family size, passive smoking, greater than twenty-five students per classroom, and the number of rooms per house were identified as associated risk factors for nasopharyngeal bacteria carriage. Large-scale health education programs on the risk factors for nasopharyngeal infections should be implemented for lower-level education students. The number of students per classroom in each grade level should be minimized. The study was conducted among asymptomatic children of different levels (other than primary school kindergarten and day-care children) and different geographical locations to follow the carriage rate and species identification.
Limitation of the Study
Moreover, serotyping and molecular characterization of the isolated bacterial agents, detection of virulence and antimicrobial resistance genes was not performed. Similarly, the correlation between the phenotypic and genotypic MDR was not performed.
Abbreviations
AMR, Antimicrobial Resistance; AOR, Adjusted Odds Ratio; ATCC, American Type Cell Culture, Clinical and Laboratory Standard Institute; BAP, Blood Agar Plate; CAP, Chocolate Agar Plate; CI, Confidence Interval; COR, Crude Odds Ratio; IPD, Invasive Pneumococcal Disease; KGs, Kindergartens; MDR, multidrug resistance; MHA, Muller Hilton Agar; NP, nasopharyngeal; PBPs, penicillin-binding proteins; PCV, Pneumococcal Conjugate Vaccine; SOP, Standard Operating Procedure; SPSS, Statistical package for social sciences; STGG, Skim Milk Tryptone Glucose Glycerol; TMP-SMX, Trimethoprim Sulfamethoxazole; WHO, World Health Organization.
Data Sharing Statement
Data supporting the conclusions of this article are within the manuscript.
Acknowledgments
The authors would like to acknowledge the Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wollo University, for giving me the opportunity to conduct this thesis work, and all the study participants, APHI staff, especially the Microbiology Department and the staff of DRH for their participation and support during the sample collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funds were obtained, only institutional support from Wollo university.
Disclosure
The authors declare that they have no conflicts of interest in this research work.
References
1. Dion CF, Ashurst JV. Streptococcus pneumoniae. 2017.
2. Unger SA, Bogaert D. The respiratory microbiome and respiratory infections. J Infect. 2017;74:S84–S8. doi:10.1016/S0163-4453(17)30196-2
3. Bogaert D, de Groot R, Hermans P. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis. 2004;4(3):144–154. doi:10.1016/S1473-3099(04)00938-7
4. Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K, Campbell H. Epidemiology and etiology of childhood pneumonia. Bull World Health Organ. 2008;86(5):408–16B. doi:10.2471/BLT.07.048769
5. Chewapreecha K. Evolution of Streptococcus Pneumoniae During Carriage. University of Cambridge; 2015.
6. Usonis V, Stacevičienė I, Petraitienė S, Vaičiūnienė D, Alasevičius T, Kirslienė J. Streptococcus pneumoniae nasopharyngeal colonisation in children aged under six years with acute respiratory tract infection in Lithuania, February 2012 to March 2013. Euro Surveill. 2015;20(13):34–41. doi:10.2807/1560-7917.ES2015.20.13.21079
7. Bayer M, Aslan G, Emekdaş G, Kuyucu N, Kanik A. Nasopharyngeal carriage of Streptococcus pneumoniae in healthy children and multidrug resistance. Mikrobiyol Bul. 2008;42(2):223–230.
8. Gebre T, Tadesse M, Aragaw D, et al. Nasopharyngeal carriage and antimicrobial susceptibility patterns of Streptococcus pneumoniae among children under five in southwest Ethiopia. Children. 2017;4(4):27. doi:10.3390/children4040027
9. Neves FPG, Pinto TCA, Corrêa MA, et al. Nasopharyngeal carriage, serotype distribution and antimicrobial resistance of Streptococcus pneumoniae among children from Brazil before the introduction of the 10-valent conjugate vaccine. BMC Infect Dis. 2013;13(1):318. doi:10.1186/1471-2334-13-318
10. Bennett JE, Dolin R, Blaser MJ. Principles and Practice of Infectious Diseases. Elsevier Health Sciences; 2014.
11. Stamboulidis K, Chatzaki D, Poulakou G, et al. The impact of the heptavalent pneumococcal conjugate vaccine on the epidemiology of acute otitis media complicated by otorrhea. Pediatr Infect Dis J. 2011;30(7):551–555. doi:10.1097/INF.0b013e31821038d9
12. O’Brien KL, Wolfson LJ, Watt JP, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009;374(9693):893–902. doi:10.1016/S0140-6736(09)61204-6
13. Negera A, Abelti G. An Analysis of the Trends, Differentials and Key Proximate Determinants of Infant and Under-Five Mortality in Ethiopia: Further Analysis of the 2000, 2005, and 2011 Demographic and Health Surveys. ICF International; 2013.
14. Black RE, Cousens S, Johnson HL, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375(9730):1969–1987. doi:10.1016/S0140-6736(10)60549-1
15. Hofmann J, Cetron MS, Farley MM, et al. The prevalence of drug-resistant Streptococcus pneumoniae in Atlanta. N Engl J Med. 1995;333(8):481–486. doi:10.1056/NEJM199508243330803
16. Mameli C, Fabiano V, Daprai L, et al. A longitudinal study of streptococcus pneumoniae carriage in healthy children in the 13-valent pneumococcal conjugate vaccine era. Hum Vaccin Immunother. 2015;11(4):811–817. doi:10.1080/21645515.2015.1010945
17. Loughlin AM, Hsu K, Silverio AL, Marchant CD, Pelton SI. Direct and indirect effects of PCV13 on nasopharyngeal carriage of PCV13 unique pneumococcal serotypes in Massachusetts’ children. Pediatr Infect Dis J. 2014;33(5):504–510. doi:10.1097/INF.0000000000000279
18. Zuccotti G, Mameli C, Daprai L, et al. Serotype distribution and antimicrobial susceptibilities of nasopharyngeal isolates of Streptococcus pneumoniae from healthy children in the 13-valent pneumococcal conjugate vaccine era. Vaccine. 2014;32(5):527–534. doi:10.1016/j.vaccine.2013.12.003
19. Lee GM, Kleinman K, Pelton SI, et al. Impact of 13-valent pneumococcal conjugate vaccination on Streptococcus pneumoniae carriage in young children in Massachusetts. J Pediatric Infect Dis Soc. 2013;3(1):23–32. doi:10.1093/jpids/pit057
20. Camilli R, Daprai L, Cavrini F, et al. Pneumococcal carriage in young children one year after introduction of the 13-valent conjugate vaccine in Italy. PLoS One. 2013;8(10):e76309. doi:10.1371/journal.pone.0076309
21. Huang SS, Finkelstein JA, Rifas-Shiman SL, Kleinman K, Platt R. Community-level predictors of pneumococcal carriage and resistance in young children. Am J Epidemiol. 2004;159(7):645–654. doi:10.1093/aje/kwh088
22. Katsarolis I, Poulakou G, Analitis A, et al. Risk factors for nasopharyngeal carriage of drug-resistant Streptococcus pneumoniae: data from a nation-wide surveillance study in Greece. BMC Infect Dis. 2009;9(1):120. doi:10.1186/1471-2334-9-120
23. Tsai H-Y, Lauderdale T-L, Wang J-T, et al. Updated antibiotic resistance and clinical spectrum of infections caused by Streptococcus pneumoniae in Taiwan: emphasis on risk factors for penicillin nonsusceptibilities. J Microbiol Immunol Infect. 2013;46(5):345–351. doi:10.1016/j.jmii.2012.07.012
24. Song J-H, Yang J-W, Jin JH, et al. Molecular characterization of multidrug-resistant Streptococcus pneumoniae isolates in Korea. J Clin Microbiol. 2000;38(4):1641–1644. doi:10.1128/JCM.38.4.1641-1644.2000
25. Rahmati MB, Jalilinejad H, Mousavi A. Study of risk factors for nasopharyngeal carriage of penicillin-resistant Streptococcus pneumoniae and antibiotic sensitivity in preschool children. Am J Life Sci Res. 2015;3(3):1.
26. Daka D, Loha E, Giday A. Streptococcus pneumoniae and antimicrobial resistance, Hawassa Referral Hospital, South Ethiopia. J Med Lab Diagn. 2011;2(3):27–30.
27. Assefa A, Gelaw B, Shiferaw Y, Tigabu Z. Nasopharyngeal carriage and antimicrobial susceptibility pattern of Streptococcus pneumoniae among pediatric outpatients at Gondar University Hospital, North West Ethiopia. Pediatr Neonatol. 2013;54(5):315–321. doi:10.1016/j.pedneo.2013.03.017
28. Tefera FB. Sciences, School of Medicine Department of Microbiology, Immunology& Parasitology. Addis Ababa University; 2015.
29. Satzke C, Turner P, Virolainen-Julkunen A, et al. Standard method for detecting upper respiratory carriage of Streptococcus pneumoniae: updated recommendations from the World Health Organization Pneumococcal Carriage Working Group. Vaccine. 2013;32(1):165–179. doi:10.1016/j.vaccine.2013.08.062
30. Murray P, Rosenthal K, Pfaller M. Medical microbiology 8th edition. Elsevier; 2016. Available from: http://evolve.elsevier.com/Murray/microbiology.
31. Cheesbrough M. District Laboratory Practice in Tropical Countries. Cambridge university press; 2006.
32. Wayne P. Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute; 2007:17.
33. Humphries R, Bobenchik AM, Hindler JA, Schuetz AN. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100. J Clin Microbiol. 2021;2021:213–221.
34. Enginyurt Ö, Çetinkol Y, Korkmaz M, Yıldırım AA, Korkmaz H, Çankaya S. Nasopharyngeal carriage rates of streptococcus pneumoniae and changes after conjugate pneumococcal vaccine. Biomed Res. 2016;27(1):172–176.
35. Rutebemberwa E, Mpeka B, Pariyo G, et al. High prevalence of antibiotic resistance in nasopharyngeal bacterial isolates from healthy children in rural Uganda: a cross-sectional study. Ups J Med Sci. 2015;120(4):249–256. doi:10.3109/03009734.2015.1072606
36. Kumar KR, Ashok V, Ganaie F, Ramesh A. Nasopharyngeal carriage, antibiogram & serotype distribution of Streptococcus pneumoniae among healthy under five children. Indian J Med Res. 2014;140(2):216.
37. Moyo SJ, Steinbakk M, Aboud S, et al. Penicillin resistance and serotype distribution of Streptococcus pneumoniae in nasopharyngeal carrier children under 5 years of age in Dar es Salaam, Tanzania. J Med Microbiol. 2012;61(7):952–959. doi:10.1099/jmm.0.042598-0
38. Velasquez PA, Parussolo L, Cardoso CL, Tognim MCB, Garcia LB. High prevalence of children colonized with penicillin-resistant Streptococcus pneumoniae in public day-care centers. J Pediatr (Rio J). 2009;85(6):516–522. doi:10.2223/JPED.1949
39. Farida H, Severin JA, Gasem MH, et al. Nasopharyngeal carriage of Streptococcus pneumoniae in pneumonia-prone age groups in Semarang, Java Island, Indonesia. PLoS One. 2014;9(1):e87431. doi:10.1371/journal.pone.0087431
40. Iroha I, Chibuko N, Moses I, et al. Antibiotic susceptibility patterns of Streptococcus pneumoniae isolated from the nasopharyngeal mucosa of children in Enugu Metropolis, Nigeria. Int J Curr Microbiol App Sci. 2015;4(9):1–9.
41. Huttner A, Harbarth S, Carlet J, et al. Antimicrobial resistance: a global view from the 2013 World Healthcare-Associated Infections Forum. Antimicrob Resist Infect Control. 2013;2(1):31. doi:10.1186/2047-2994-2-31
42. Čižman M. The use and resistance to antibiotics in the community. Int J Antimicrob Agents. 2003;21(4):297–307. doi:10.1016/S0924-8579(02)00394-1
43. Soewignjo S, Gessner BD, Sutanto A, et al. Streptococcus pneumoniae nasopharyngeal carriage prevalence, serotype distribution, and resistance patterns among children on Lombok Island, Indonesia. Clin Infect Dis. 2001;32(7):1039–1043. doi:10.1086/319605
44. Thummeepak R, Leerach N, Kunthalert D, Tangchaisuriya U, Thanwisai A, Sitthisak S. High prevalence of multi-drug resistant Streptococcus pneumoniae among healthy children in Thailand. J Infect Public Health. 2015;8(3):274–281. doi:10.1016/j.jiph.2014.11.002
45. Çiftçi E, Doğru Ü, Aysev D, Ince E, Güriz H. Nasopharyngeal colonization with penicillin‐resistant Streptococcus pneumoniae in Turkish children. Pediatr Int. 2000;42(5):552–556. doi:10.1046/j.1442-200x.2000.01269.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.