Back to Journals » Journal of Inflammation Research » Volume 17
High Preoperative Systemic Immune-Inflammation Index Values Significantly Predicted Poor Outcomes After on-Pump Coronary Artery Bypass Surgery
Authors Parmana IMA ![]() , Boom CE, Poernomo H, Gani C, Nugroho B, Cintyandy R
, Boom CE, Poernomo H, Gani C, Nugroho B, Cintyandy R ![]() , Sanjaya L, Hadinata Y, Parna DR, Yulia M, Hanafy DA
, Sanjaya L, Hadinata Y, Parna DR, Yulia M, Hanafy DA ![]()
Received 27 November 2023
Accepted for publication 23 January 2024
Published 7 February 2024 Volume 2024:17 Pages 755—764
DOI https://doi.org/10.2147/JIR.S449795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
I Made Adi Parmana,1 Cindy Elfira Boom,1 Herdono Poernomo,1 Chairil Gani,1 Budi Nugroho,1 Riza Cintyandy,1 Lisa Sanjaya,1 Yudi Hadinata,1 Dian Raseka Parna,1 Mefri Yulia,1 Dudy Arman Hanafy2
1Department of Anesthesiology and Intensive Care, National Cardiovascular Center Harapan Kita, Jakarta, Indonesia; 2Department of Cardiothoracic and Vascular Surgery, National Cardiovascular Center Harapan Kita, Jakarta, Indonesia
Correspondence: I Made Adi Parmana, Department of Anesthesiology and Intensive Care, National Cardiovascular Center Harapan Kita, Jakarta, Indonesia, Email [email protected]
Purpose: On-pump coronary artery bypass grafting (CABG) is one of the most common revascularization surgical therapies for coronary artery disease (CAD). However, owing to the use of cardiopulmonary bypass (“on-pump”), the body develops systemic inflammatory response syndrome, which leads to the risk of morbidity and mortality. This study aimed to determine the perioperative outcomes of patients who underwent on-pump CABG surgery using the systemic immune-inflammation index (SII).
Patients and methods: This single-center retrospective study used secondary data from patients’ electronic medical records and medical records archives at the National Cardiovascular Center Harapan Kita, who underwent on-pump CABG from January 2019 to December 2022. A total of 1056 on-pump CABG procedures were performed after exclusion. Lymphocyte, segmental neutrophil, and platelet counts from the preoperative data were used to calculate the SII values. An SII cutoff value of 528.715 × 103/mm3 divided the patients into two groups.
Results: The SII value of 1056 patients were calculated, among which 490 (46%) patients had a preoperative SII value of ≥ 528.715 × 103/mm3. Multivariate analysis showed that a high SII significantly prolonged the duration of surgery (OR 1.005, 95% CI 1.003– 1.006) and cardiopulmonary bypass (CPB) time (OR 1.007, 95% CI 1.005– 1.009). High SII values significantly predicted prolonged mechanical ventilation (OR 6.154, 95% CL 3.938– 9.617), intensive care unit (ICU) stay (OR 6.332, 95% CL 4.232– 9.474), and hospital stay (OR 3.517, 95% CL 2.711– 4.562). Regarding other perioperative outcomes, a high SII significantly predicted the risk of postoperative atrial AF, cardiac arrest, acute myocardial infarction, and mortality.
Conclusion: A high preoperative SII value can predict morbidity and mortality in patients undergoing on-pump CABG surgery.
Keywords: systemic immune-inflammation index, on-pump coronary artery bypass graft, systemic inflammation, morbidity, mortality
Introduction
Reported that developing countries had an estimated 19 million deaths in 2010 by coronary artery disease (CAD), making it one of the leading causes of mortality.1 CAD is often associated with atherosclerosis, a form of lipid accumulation and inflammation in the artery that reduces the blood flow in the lumen.2 Once it forms, the lack of blood flow causes clinical complications such as myocardial infarction and stroke. CAD therapy involves lifestyle modifications, medications, and revascularization surgeries.
Coronary artery bypass grafting (CABG) is one of the most common revascularization surgeries for CAD patients. CABG is defined as a surgery in which autologous veins or arteries are used as grafts to bypass an obstructed coronary artery.3 During its development, CABG can be performed using either cardiopulmonary bypass (on-pump) or without (off-pump). On-pump CABG uses cardiopulmonary bypass (CPB) to maintain blood flow, but it is often associated with complications in the form of systemic inflammation.
The mechanism of acute inflammation involves many cytokines that promote the synthesis of tumor necrosis factor (TNF), a major contributor to the activation of polymorphonuclear neutrophils (PMNs).4 Due to blood exposure to artificial materials, the intrinsic coagulation factor initiates a cascade of factors that lead to a high platelet count in the blood.5 This may lead to severe complications, such as thrombus formation in the blood flow.6 During the use of CPB, using liquid to support the blood flow into the extracorporeal circuit causes a hemodilution effect that affects the lymphocyte count.7 This leads to a higher count of neutrophils and platelets, but a lower lymphocyte count.
Several examples of scores for assessing the inflammatory process based on neutrophil and lymphocyte values include the Naples score (NS) and systemic immune-inflammation index (SII). The Naples score (NS) has emerged as a valuable prognostic tool in cancer patients and can be used to assess both the inflammatory and nutritional status of patients. NS is a composite of serum albumin levels, total cholesterol levels, neutrophil/lymphocyte ratio (NLR), and lymphocyte/monocyte ratio (LMR). NS can be used for risk stratification for long-term mortality in patients with ST-elevation myocardial infarction (STEMI) undergoing percutaneous coronary intervention (PCI).8
The systemic immune-inflammation index (SII) was introduced by Hu in 2014 as a predictor of the prognosis of cancer and inflammation-related diseases. The SII is formulated by multiplying the platelet count and neutrophil count and then divided by the lymphocyte count.9 A previous study stated that high SII had a better prediction than traditional risk factors in determining the outcome of patients with CAD.10 Another study suggested that SII ≥1119 x 103/mm3 may be an independent predictive marker for both long-term mortality and appropriate intracardiac defibrillator (ICD) therapy in patients with heart failure with reduced ejection fraction (HFrEF).11
Longer use of ventilation machine and intensive care unit (ICU) stay were predicted by a high SII in patients after off-pump CABG.12 Low SII was associated with consuming an anti-inflammatory diet after on-pump CABG surgery.13 However, there is a lack of studies about the usage of SII in predicting morbidity and mortality in patients after on-pump CABG surgery. This study aimed to determine the role of SII in predicting the morbidity and mortality of patients after on-pump CABG surgery.
Methods
This single-center, retrospective study was conducted at the National Cardiovascular Center, Harapan Kita. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the National Cardiovascular Center Harapan Kita (DP.04.03/KEP137/EC072/2023). Due to electronic medical records, written informed consent was not required, and all patient data were anonymized and de-identified. This study included all patients who underwent on-pump CABG surgery at the National Cardiovascular Center Harapan Kita from January 2019 to December 2022. Patients with the following criteria were excluded: incomplete preoperative data, renal failure requiring hemodialysis, emergency status, laboratory results older than one week, and patients who underwent valve surgery. 1574 on-pump CABG procedures were performed, and 518 patients were excluded based on the exclusion criteria (Figure 1). Patient characteristics, such as age, sex, body mass index (BMI), history of hypertension, diabetes mellitus, dyslipidemia, chronic obstructive pulmonary disorder, smoking, recent myocardial infarction (MI), family history of CAD, preoperative ejection fraction, left main (LM) disease, and EuroSCORE II, were recorded.
 |
Figure 1 Flow chart of study population selection. |
Intraoperative data included the duration of surgery, cardiopulmonary bypass (CPB) time, aortic cross-clamp time, and the number of grafts. The recorded perioperative outcome data includes the vasoactive-inotropic score (VIS), intra-aortic balloon pump (IABP), perioperative atrial fibrillation (PoAF), stroke, heart failure, cardiac arrest, acute myocardial infarction (AMI), septic shock, cardiogenic shock, and mortality. The VIS was determined by adding dopamine (µg/kg/min), dobutamine (µg/kg/min), 10 × milrinone (µg/kg/min), 100 × epinephrine (µg/kg/min), 100 × norepinephrine (µg/kg/min), and 10000 × vasopressin (µg/kg/min).
The patients were observed and evaluated during their stay in the ICU. Patients were extubated after they were hemodynamically stable. The prolonged duration of mechanical ventilation was defined as >24 hours since all operations were performed (DO-MV > 24 h) by avoiding unnecessary use of anesthetic agents. Prolonged ICU stay was defined as >48 hours of ICU stay (LOS-ICU > 48 h). After the patients stabilized, they were transported to the surgery ward with a length of stay >7 days, defined as a prolonged hospital stay (LOS-H > 7 days). The poor outcomes comprise DO-MV > 24 h, LOS-ICU > 48 h, and LOS-H > 7 days. The mortality rate was evaluated 30 days after the postoperative day.
Statistical Analysis
All data were collected and analyzed using SPSS version 23.0 (SPSS Inc., Chicago, IL, USA). The normality test was performed using the Kolmogorov–Smirnov test. Normally distributed continuous variables are expressed as mean and standard deviation (SD) and analyzed using an unpaired t-test. In contrast, non-normally distributed data are expressed as medians and analyzed using the Mann–Whitney U-test. Categorical variables are expressed as numbers and analyzed using the chi-square test. Statistical significance was set at p <0.05. All significant variables were tested using Pearson’s and Spearman correlations with a significance level of p <0.05.
Results
The identified cut-off value of preoperative SII in patients with poor outcomes in this study, obtained from the largest Youden index and achieving an AUC of 0.669, was 528.715 × 103/mm3. This value demonstrated a sensitivity of 65% and a specificity of 67%. In the study, out of the 1056 patients present in the study, 490 (46%) had a preoperative SII of ≥528.715 × 103/mm3. Table 1 presents the demographic characteristics of patients with high SII values significantly correlated with LM disease and higher EuroSCORE scores, whereas Table 2 presents intraoperative data. Table 3 presents the univariate analysis, which showed that the presence of LM disease, longer duration of surgery, CPB time, aortic cross-clamp time, and the cutoff SII were significant predictors of poor perioperative outcomes. The multivariate analysis of preoperative variables in Table 4 shows that the duration of surgery (p=0.08) was insignificant and included as a confounding factor. The cut-off SII (p<0.001) was more significant than CPB time (p=0.020), although both were found to be independent factors in predicting poor perioperative outcomes. Table 5 shows that a high SII significantly prolonged the duration of mechanical ventilation, ICU stay, and hospital stay (p <0.05).
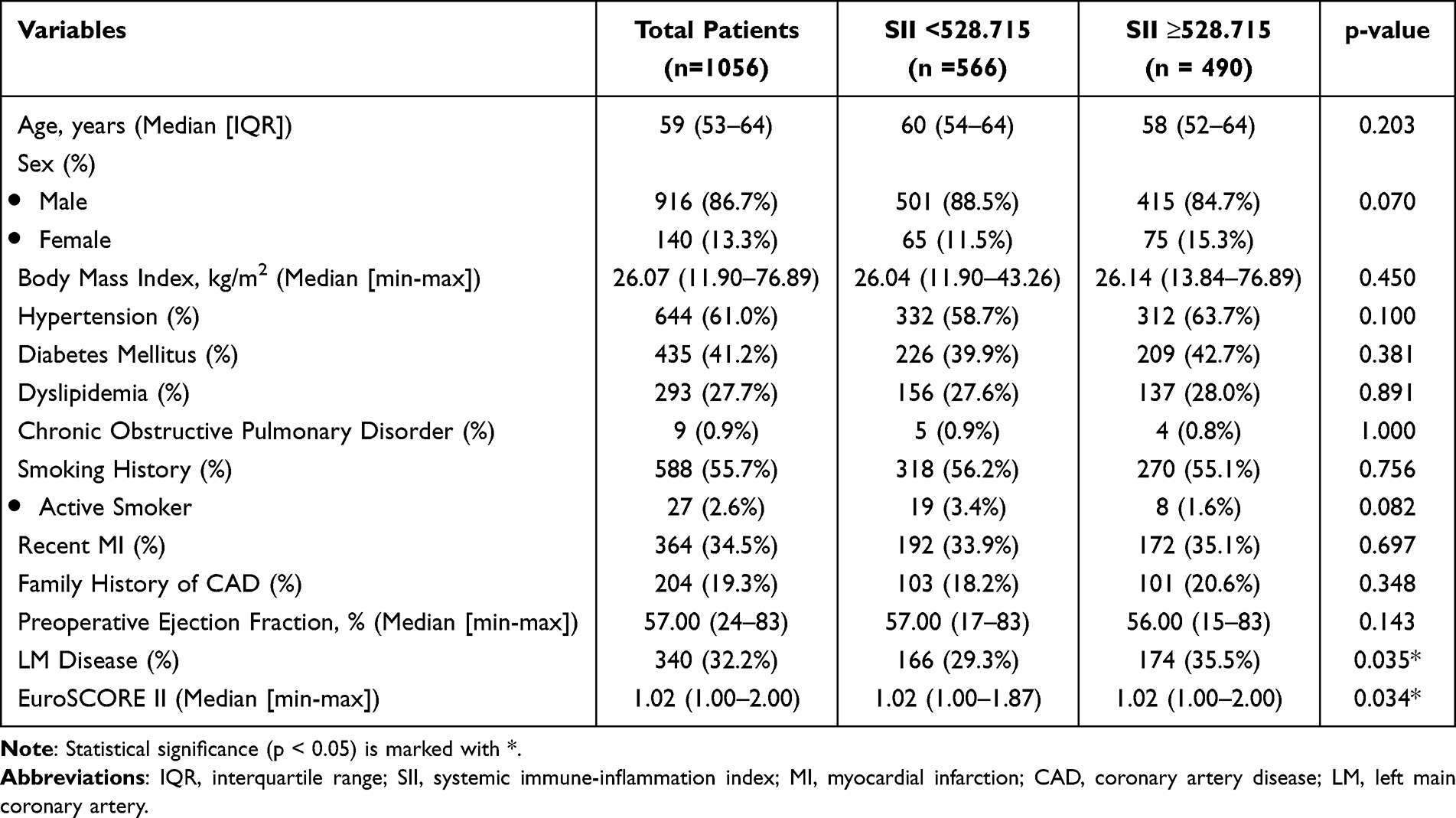 |
Table 1 Patients Characteristics |
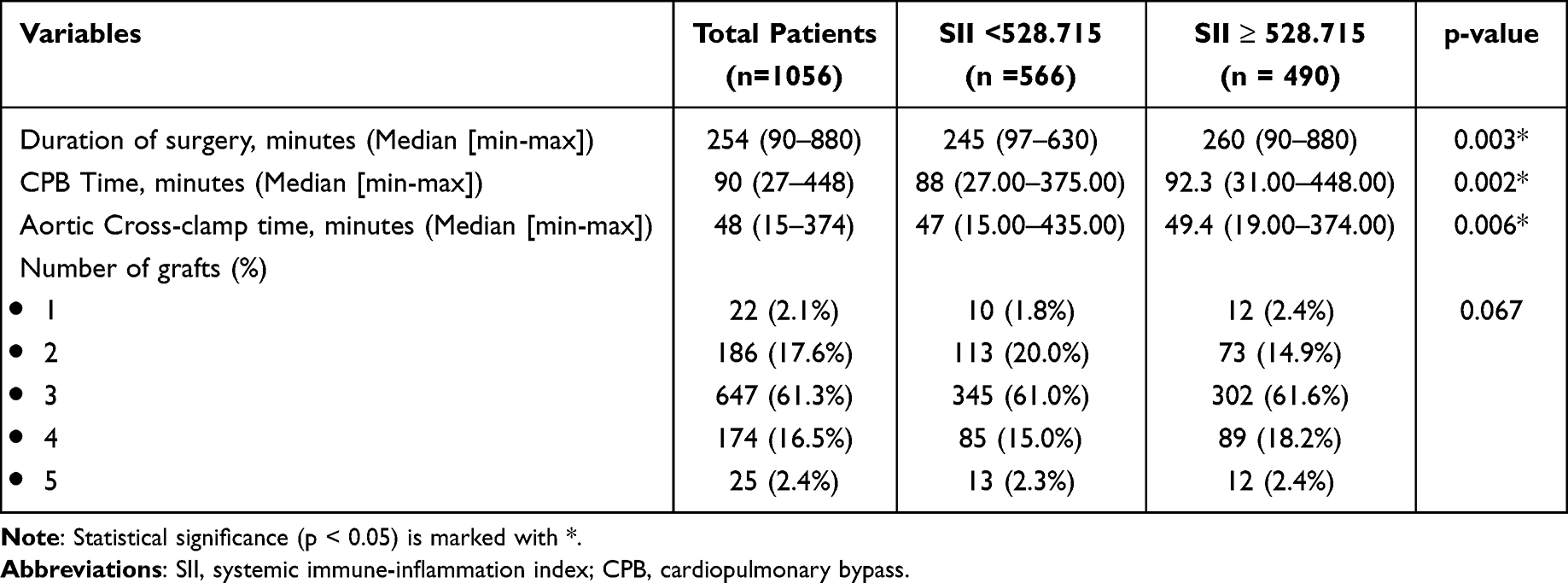 |
Table 2 Intraoperative Data |
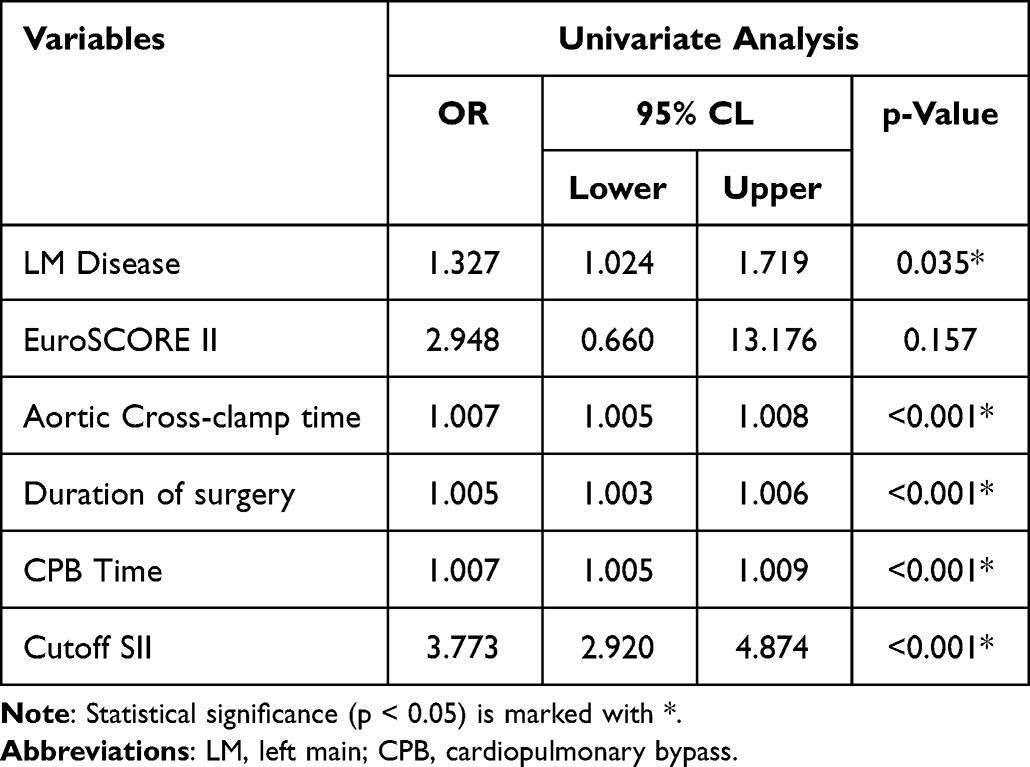 |
Table 3 Univariate Analysis on Preoperative Variables That Were Significant with Poor Perioperative Outcomes |
 |
Table 4 Multivariate Analysis on Preoperative Variables That Were Significant with Poor Perioperative Outcomes |
 |
Table 5 Analysis of High SII Values in Predicting Poor Perioperative Outcomes |
As shown in Table 6, a high SII value predicted other perioperative outcomes. Significant results were observed in higher-count VIS, use of IABP, PoAF, cardiac arrest, and acute myocardial infarct incidents. A strongly significant result was shown in the higher SII, predicting the mortality rate (95% CI 1.883–6.523, p ≤ 0.001).
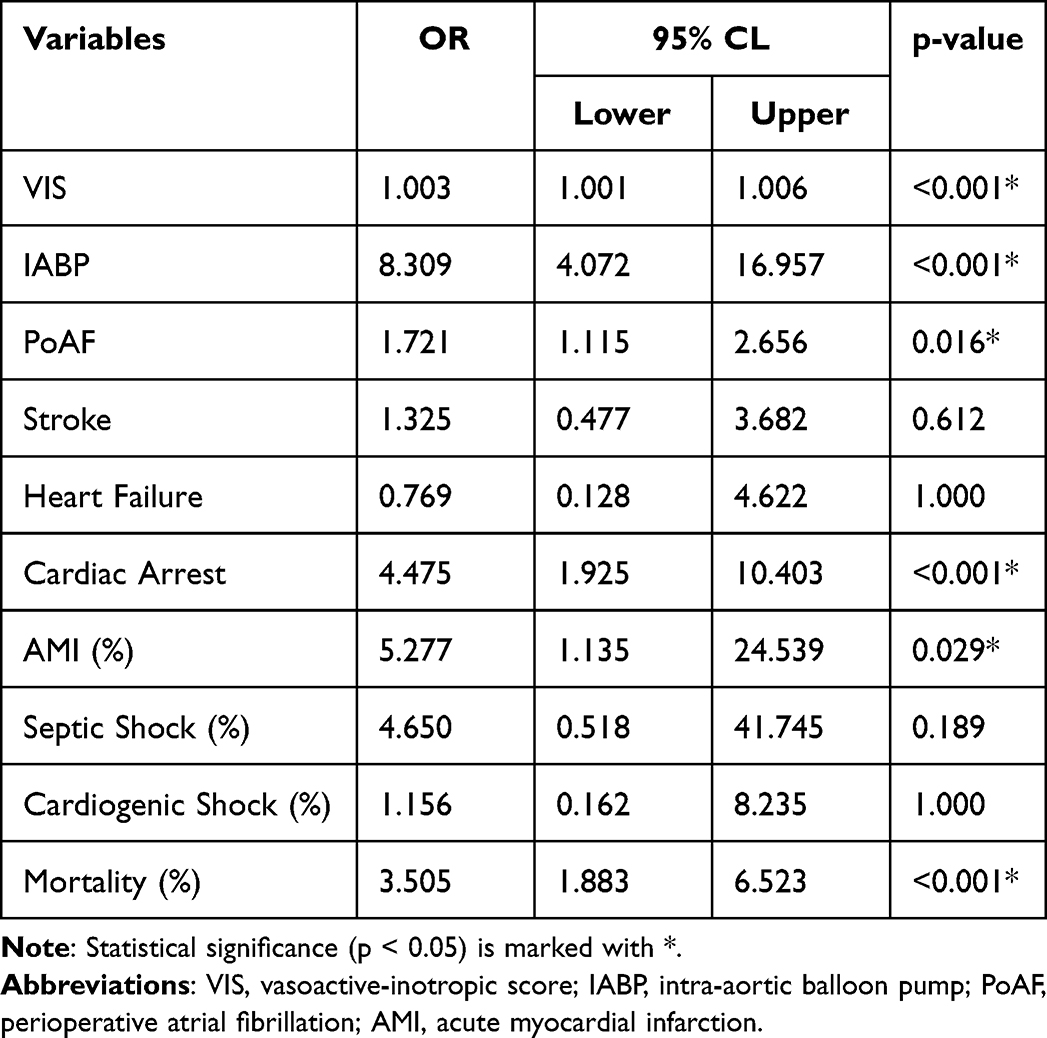 |
Table 6 Analysis of High SII Values in Predicting Poor Perioperative Outcomes |
Discussion
In this study, a high SII predicted poor perioperative outcomes after on-pump CABG. These outcomes included longer use of mechanical ventilation, intensive care unit stay, and stay in the surgical ward. The long-term use of mechanical ventilation is one of the most common complications in patients post-CABG surgery. It is related to the longer duration of CPB, which affects the hemodynamic status and the need for an inotropic agent.14,15 Rapid weaning of the ventilator is related to factors such as metabolic derangement in arterial bicarbonate levels and hemodynamic stability.16 The prolonged use of mechanical ventilation may lead to a longer stay in the ICU, due to a higher risk of complications.17 The length of ICU stay is correlated with patient characteristics such as diabetes mellitus, hyperlipidemia, and a history of hypertension.17 Another factor that causes the prolonged stay in the ICU is a possible sign of inflammation caused by exposure during open heart surgery, longer duration of surgery, and the use of cardiopulmonary bypass.18
During open heart surgery, the trauma to the body during the incision of the sternum, extraction of the internal mammary artery, and aortic manipulation leads to systemic inflammatory response syndrome (SIRS).6 IL-6 and C-reactive protein (CRP) are the main markers in determining the SIRS. The magnitude of the CRP level is associated with the level of tissue injury during surgery.19 Cardiopulmonary bypass initiates SIRS due to blood contact with the artificial surface that activates the inflammatory cascade at the humoral (coagulation system, pro-inflammatory cytokines) and cellular (leukocytes, platelets, vascular endothelial cells) levels.6 This cascade includes different and complex pathways that intersect with each other, which would later cause injury due to ischemia-reperfusion, leading to an increase in the inflammatory response.7
Although it remains unclear, there is a relationship between the inflammatory response and the occurrence of PoAF.20 The inflammation that persists post-open heart surgery could lead to a high level of CRP, which could predict PoAF.20,21 Since a higher SII reflects a higher level of inflammation, this study showed that SII also predicts a higher likelihood of PoAF (p=0.016). Although PoAF is related to the incidence of stroke (p=0.612) and heart failure (p=1.000), it is not statistically significant.21 However, regarding the same effect of systemic inflammation conditions, PoAF is interrelated to mortality due to heart failure and stroke.22
Over the past decade, artificial intelligence (AI) has demonstrated its efficacy, particularly in managing cardiovascular diseases, specifically AF and CAD. The potential and versatility of future AI applications in AF and CAD are promising, with the capability to revolutionize the diagnosis, risk classification, and optimization of therapies for these conditions. AI algorithms can integrate data from various sources, including wearable devices, imaging data, and electronic health records, providing a comprehensive overview of a patient’s health to improve risk categorization and diagnostic precision. Physicians should equip themselves for AI by acquiring the necessary skills to utilize AI models and adeptly interpret their findings.23
The SII can be integrated with other scores, such as the electrocardiography (ECG) score. Various ECG scores have been proposed to predict outcomes related to ECG, one of which is the morphology-voltage-p wave duration (MVP) ECG risk score. The MVP ECG risk score has been demonstrated to have predictive value for both in-hospital and long-term atrial fibrillation (AF) diagnosis in a substantial population of patients with acute ischemic stroke (AIS).24 Other scores, such as the electrocardiographic diastolic index (EDI), can also be employed. EDI plays a significant role in predicting diastolic dysfunction in adult patients undergoing transthoracic echocardiography.25
A higher VIS also corresponds to prolonged use of ventilation and ICU stays due to longer recovery time affected by inotropic support.26 In this study, high SII levels predicted a higher use of VIS (p <0.001), in accordance with a higher risk of mortality after on-pump CABG. The VIS is the numerical count of vasoactive and inotropic support after cardiac surgery. A previous study showed that VIS predicts morbidity and mortality after pediatric cardiac surgery.27 Yamazaki et al showed that VIS was a better model for predicting morbidity and mortality in adult cardiac surgery than EuroSCORE and Parsonnet scores.28
IABP has been acknowledged as one of the most effective ways to deal with low cardiac output after post-CABG.29 The analysis showed that the use of IABP in postoperative cardiac surgery is more common in the higher SII group (p<0.001). Although the findings suggest no significant difference in outcome when using IABP before and after surgery, the clinical use of IABP reduces the mortality rate.30
Since the introduction of SII, its use for assessing the prognosis of cancer and other inflammatory diseases has been rapidly updating.9 A higher SII, according to its formulation, is accepted as a marker for a higher state of inflammation, including chronic inflammation. Cardiovascular disease (CVD) is an important condition affected by chronic inflammation.
In several studies, MI has shown a connection between its initiation and progression with inflammation. Platelets, leukocytes, and neutrophils are also involved in disease development. Saylik et al reported that the SII was noted for predicting cardiac death in patients with ST-elevation myocardial infarction.31 This study acknowledges this report since the SII is statistically significant in predicting AMI (p=0.029).
Yang et al in their study proved that a higher SII is associated with a higher risk of death by cardiovascular means such as cardiac arrest and heart failure.10 As stated by the result of this study, a high SII can predict the occurrence of cardiac arrest (p<0,001). Although insignificant in predicting heart failure (p=1.000), heart failure is considered a prevalent cause of cardiac arrest.32
A high SII value can predict a higher probability of mortality based on patient characteristics. Table 1 shows that patient characteristics, including LM disease and EuroSCORE II, were significantly associated with high SII values. Both of these criteria are related to an increased risk of mortality in patients after on-pump CABG.33 The presence of LM disease is correlated with a higher risk of cardiac failure that leads to death in patients, as stated by a previous study.34 A higher EuroSCORE II also leads to a higher mortality risk.
Receiver operating characteristic (ROC) analysis for the SII resulted in a cutoff value of 528.715 × m3/mm3 with 65% sensitivity and 67% specificity (Figure 2). This result was consistent with a study by Candemir et al which produced an SII cutoff value at 750 × 103/mm3 (sensitivity 60% and specificity 70.11%) in patients with CAD.35 Another study by Zengin showed that an SII cutoff value of 651,7 × 103/mm3 (sensitivity 65% and specificity 64.9%), also predicted acute kidney injury (AKI) as a complication after patients undergo CABG.36 The difference in the cutoff values of SII may be due to the different sample sizes and population characteristics.
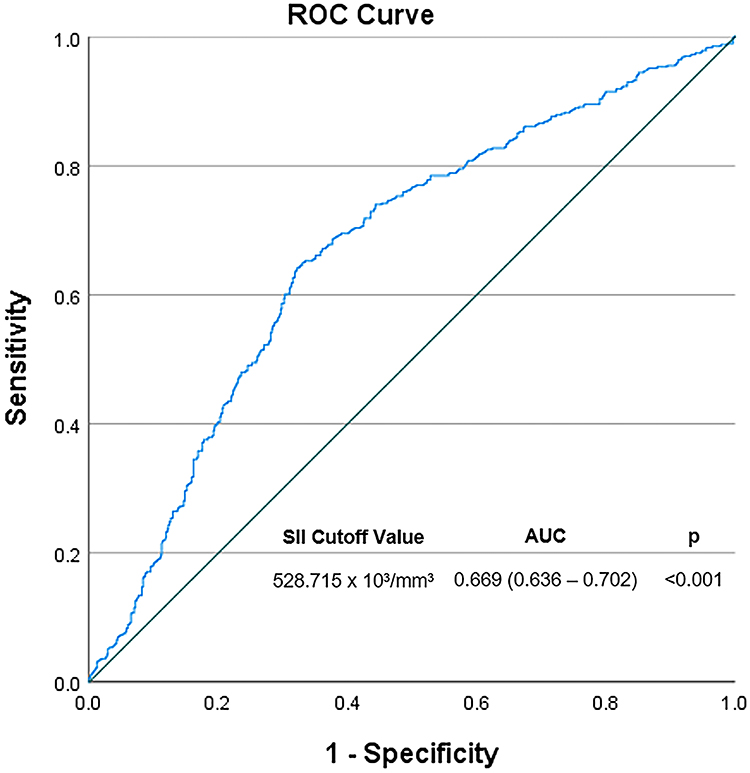 |
Figure 2 Receiver Operating Characteristic (ROC) curve for prediction of poor outcome based on SII. The highest area under the curve of 0.669 (p = <0.001*) for SII, with its respective cutoff value of 528.715×103 /mm3. Poor outcomes were defined as ≥ 1: duration of mechanical ventilation >24 hours (DO-MV > 24 h), length of intensive care unit stay >48 hours (LOS-ICU > 48 h), and length of hospital stay >7 days (LOS-H > 7 days). Abbreviations: AUC, area under the curve; SII, systemic immune-inflammation index. |
Limitations and Implications
The limitations of this study include the exclusion of patient counts owing to the exclusion criteria. This was because of the incomplete medical records available. The high number of excluded patients makes the data not attributable to the Indonesian population. Since this study was conducted in a single center at the National Cardiovascular Center Harapan Kita, another study involving multiple centers and numerous populations could be considered as studies on the SII are still limited.
Conclusion
In patients undergoing on-pump CABG surgery, high SII values significantly predict a higher morbidity rate in the form of longer ventilation duration, ICU stay, and hospital stay. This may lead to poor outcomes and complications such as higher VIS, the need to use IABP, PoAF, cardiac arrest, AMI, and even mortality. Since SII is more recognized and is defined as more reliable than traditional risk factors, it could be used to provide information regarding perioperative prognosis.
Data Sharing Statement
Individual de-identified participant data from this study will be made available upon request after publication and will be available for 36 months following article publication. Researchers must state the aims of their analysis and provide a methodologically sound proposal directed toward the corresponding author.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;11(2):169–177. doi:10.2991/JEGH.K.201217.001
2. Björkegren JLM, Lusis AJ. Atherosclerosis: recent developments. Cell. 2022;185(10):1630–1645. doi:10.1016/j.cell.2022.04.004
3. Alexander JH, Smith PK. Coronary-artery bypass grafting. N Engl J Med. 2016;374(20):1954–1964. doi:10.1056/NEJMra1406944
4. Squiccimarro E, Stasi A, Lorusso R, Paparella D. Narrative review of the systemic inflammatory reaction to cardiac surgery and cardiopulmonary bypass. Artif Organs. 2022;46(4):568–577. doi:10.1111/aor.14171
5. Stahl GL, Shernan SK, Smith PK, Levy JH. Complement activation and cardiac surgery: a novel target for improving outcomes. Anesth Analg. 2012;115(4):759–771. doi:10.1213/ANE.0b013e3182652b7d
6. Boehne M, Sasse M, Karch A, et al. Systemic inflammatory response syndrome after pediatric congenital heart surgery: incidence, risk factors, and clinical outcome. J Card Surg. 2017;32(2):116–125. doi:10.1111/jocs.12879
7. Warren OJ, Smith AJ, Alexiou C, et al. The inflammatory response to cardiopulmonary bypass: part 1-mechanisms of pathogenesis. J Cardiothorac Vasc Anesth. 2009;23(2):223–231. doi:10.1053/j.jvca.2008.08.007
8. Şaylık F, Çınar T, Selçuk M, et al. Evaluation of Naples score for long-term mortality in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Angiology. 2023;10(10). doi:10.1177/00033197231170982
9. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
10. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5). doi:10.1111/eci.13230
11. Hayıroğlu Mİ, Çınar T, Çinier G, et al. Evaluating systemic immune-inflammation index in patients with implantable cardioverter defibrillator for heart failure with reduced ejection fraction. Pacing Clin Electrophysiol. 2022;45(2):188–195. doi:10.1111/pace.14436
12. Dey S, Kashav R, Kohli JK, et al. Systemic immune-inflammation index predicts poor outcome after elective off-pump CABG: a retrospective, single-center study. J Cardiothorac Vasc Anesth. 2021;35(8):2397–2404. doi:10.1053/j.jvca.2020.09.092
13. Szymanska P, Rozalski M, Wilczynski M, Golanski J. Systemic immune-inflammation index (SII) and neutrophil to lymphocyte ratio (NLR) are useful markers for assessing effects of anti-inflammatory diet in patients before coronary artery bypass grafting. Rocz Panstw Zakl Hig. 2021;72(3):327–335. doi:10.32394/rpzh.2021.0170
14. Gumus F, Polat A, Yektas A, et al. Prolonged mechanical ventilation after CABG: risk factor analysis. J Cardiothorac Vasc Anesth. 2015;29(1):52–58. doi:10.1053/j.jvca.2014.09.002
15. Daza-Arana JE, Lozada-Ramos H, Ávila-Hernández DF, Ordoñez-Mora LT, Sánchez DP. Prolonged mechanical ventilation following coronary artery bypass graft in Santiago De Cali, Colombia. Vasc Health Risk Manag. 2022;18:767–781. doi:10.2147/VHRM.S367108
16. Trouillet JL, Combes A, Vaissier E, et al. Prolonged mechanical ventilation after cardiac surgery: outcome and predictors. J Thorac Cardiovasc Surg. 2009;138(4):948–953. doi:10.1016/j.jtcvs.2009.05.034
17. Tunç M, Şahutoğlu C, Karaca N, Kocabaş S, Aşkar FZ. Risk factors for prolonged intensive care unit stay after open heart surgery in adults. Turk J Anaesthesiol Reanim. 2018;46(4):283–291. doi:10.5152/TJAR.2018.92244
18. Di KK, Sykc L, Liu CY, Chou NK. Risk factors associated with longer stays in cardiovascular surgical intensive care unit after CABG. JFormos Med Assoc. 2022;121(1):304–313. doi:10.1016/j.jfma.2021.04.020
19. Watt DG, Horgan PG, McMillan DC. Routine clinical markers of the magnitude of the systemic inflammatory response after elective operation: a systematic review. Surgery. 2015;157(2):362–380. doi:10.1016/j.surg.2014.09.009
20. Jacob KA, Nathoe HM, Dieleman JM, Van Osch D, Kluin J, van Dijk D. Inflammation in new-onset atrial fibrillation after cardiac surgery: a systematic review. Eur J Clin Invest. 2014;44(4):402–428. doi:10.1111/eci.12237
21. Thorén E, Wernroth ML, Christersson C, Grinnemo KH, Jidéus L, Ståhle E. Compared with matched controls, patients with postoperative atrial fibrillation (POAF) have increased long-term AF after CABG, and POAF is further associated with increased ischemic stroke, heart failure and mortality even after adjustment for AF. Clin Res Cardiol. 2020;109(10):1232–1242. doi:10.1007/s00392-020-01614-z
22. Van Linthout S, Tschöpe C. Inflammation – cause or consequence of heart failure or both? Curr Heart Fail Rep. 2017;14(4):251–265. doi:10.1007/s11897-017-0337-9
23. Hayıroğlu Mİ, Altay S. The role of artificial intelligence in coronary artery disease and atrial fibrillation. Balkan Med J. 2023;40(3):151–152. doi:10.4274/balkanmedj.galenos.2023.06042023
24. Hayıroğlu Mİ, Çınar T, Selçuk M, et al. The significance of the morphology-voltage-P-wave duration (MVP) ECG score for prediction of in-hospital and long-term atrial fibrillation in ischemic stroke. J Electrocardiol. 2021;69:44–50. doi:10.1016/j.jelectrocard.2021.09.006
25. Hayıroğlu Mİ, Çınar T, Çiçek V, et al. A simple formula to predict echocardiographic diastolic dysfunction-electrocardiographic diastolic index. Herz. 2021;46(Suppl 2):159–165. doi:10.1007/s00059-020-04972-6
26. Gaies MG, Gurney JG, Yen AH, et al. Vasoactive-inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr Crit Care Med. 2010;11(2):234–238. doi:10.1097/PCC.0b013e3181b806fc
27. Koponen T, Karttunen J, Musialowicz T, Pietiläinen L, Uusaro A, Lahtinen P. Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br J Anaesth. 2019;122(4):428–436. doi:10.1016/j.bja.2018.12.019
28. Yamazaki Y, Oba K, Matsui Y, Morimoto Y. Vasoactive-inotropic score as a predictor of morbidity and mortality in adults after cardiac surgery with cardiopulmonary bypass. J Anesth. 2018;32(2):167–173. doi:10.1007/s00540-018-2447-2
29. Jannati M, Attar A. Intra-aortic balloon pump postcardiac surgery: a literature review. J Res Med Sci. 2019;24(1):6. doi:10.4103/jrms.JRMS_199_18
30. Gilotra NA, Stevens GR. Temporary mechanical circulatory support: a review of the options, indications, and outcomes. Clin Med Insights Cardiol. 2015;8(Suppl 1):75–85. doi:10.4137/CMC.S15718
31. Saylik F, Akbulut T. Systemic immune-inflammation index predicts major cardiovascular adverse events in patients with ST-segment elevated myocardial infarction. Arq Bras Cardiol. 2022;119(1):14–22. doi:10.36660/abc.20210412
32. Allencherril J, Lee PYK, Khan K, Loya A, Pally A. Etiologies of In-hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2022;175:88–95. doi:10.1016/j.resuscitation.2022.03.005
33. Sheikhy A, Fallahzadeh A, Sadeghian S, et al. Mid-term outcomes of off-pump versus on-pump coronary artery bypass graft surgery; statistical challenges in comparison. BMC Cardiovasc Dis. 2021;21(1). doi:10.1186/s12872-021-02213-0
34. Stone GW, Kappetein AP, Sabik JF, et al. Five-year outcomes after PCI or CABG for left main coronary disease. N Engl J Med. 2019;381(19):1820–1830. doi:10.1056/nejmoa1909406
35. Candemir M, Kiziltunç E, Nurkoç S, Şahinarslan A. Relationship between Systemic Immune-Inflammation Index (SII) and the severity of stable coronary artery Disease. Angiology. 2021;72(6):575–581. doi:10.1177/0003319720987743
36. Zengin EN. Systemic immune-inflammation index predicts acute kidney injury after cardiac surgery: a retrospective observational study. J Cardio-Vascular-Thoracic Anaesth Inten Care Soc. 2024;24:1. doi:10.14744/gkdad.2023.79664
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Short- and Mid-Term Survival Prediction in Patients with Acute Type A Aortic Dissection Undergoing Surgical Repair: Based on the Systemic Immune-Inflammation Index
Li Z, Zhang H, Baraghtha S, Mu J, Matniyaz Y, Jiang X, Wang K, Wang D, Xue YX
Journal of Inflammation Research 2022, 15:5785-5799
Published Date: 10 October 2022
Predictors of Cardiovascular Morbidity Among Adult Hypertensive Patients: A Cross-Sectional Study from the Kingdom of Saudi Arabia
Al-Ghamdi S, Aldosari KH, Hussain ABO
Patient Preference and Adherence 2023, 17:1361-1369
Published Date: 6 June 2023
Relationship Between Systemic Immune-Inflammation Index and Risk of Respiratory Failure and Death in COPD: A Retrospective Cohort Study Based on the MIMIC-IV Database
Zhang Y, Tan X, Hu S, Cui Z, Chen W
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:459-473
Published Date: 19 February 2024
Early Postoperative Complications in Colorectal Cancer Patients Following Colorectal Surgery Among Yemeni Patients: A Prospective Study
Al-Amry AL, Obadiel YA, Al-Shehari MM, Gailan WM, Bajubair MH, Jowah HM
Open Access Surgery 2024, 17:81-90
Published Date: 26 June 2024
Global Trends in Incidence and Mortality Rates of Endometrial Cancer Among Individuals Aged 55 years and Above From 1990 to 2021: An Analysis of the Global Burden of Disease
Gao S, Wang J, Li Z, Wang T, Wang J
International Journal of Women's Health 2025, 17:651-662
Published Date: 6 March 2025