Back to Journals » Journal of Pain Research » Volume 15
High Pain Intensity is a Risk Factor of Non-Resolving TMD: A Three-Year Follow-Up of a Patient Group in a Norwegian Interdisciplinary Evaluation Program
Authors Staniszewski K, Willassen L, Berge T, Johansson A ![]() , Schjødt B, Rosen A
, Schjødt B, Rosen A ![]()
Received 2 October 2021
Accepted for publication 10 March 2022
Published 2 May 2022 Volume 2022:15 Pages 1283—1296
DOI https://doi.org/10.2147/JPR.S341861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Keith
Kordian Staniszewski,1 Lisa Willassen,1 Trond Berge,1,2 Anders Johansson,1,2 Borrik Schjødt,3 Annika Rosen1,2
1Department of Clinical Dentistry, University of Bergen, Bergen, Norway; 2Department of Oral and Maxillofacial Surgery, Haukeland University Hospital, Bergen, Norway; 3Centre for Pain Management and Palliative Care, Haukeland University Hospital, Bergen, Norway
Correspondence: Kordian Staniszewski, Department of Clinical Dentistry University of Bergen, Årstadveien 19, Bergen, 5009, Norway, Tel +47 47602632, Email [email protected]
Purpose: To investigate the outcome of patients with long-term refractory temporomandibular disorders (TMD) three years after a Norwegian interdisciplinary evaluation program with attention to patient satisfaction, function, pain, and psychosocial variables.
Patients and Methods: The study population consisted of 60 long-term refractory TMD patients who were investigated by a Norwegian interdisciplinary team. A questionnaire that covered medical history, function, pain, lifestyle factors, TMD-status and follow-up from their general medical practitioner (GMP) was sent to the patients three years after the evaluation. Questionnaires that assessed function (Mandibular Functional Index Questionnaire [MFIQ] and Roland Morrison Scale [RMS]), pain intensity (General Pain Intensity questionnaire [GPI]) and psychosocial factors (Hospital Anxiety and Depression scale [HADS]); a 2-item version of the Coping Strategies Questionnaire [CSQ]) were included in the package.
Results: Thirty-nine out of 60 TMD patients completed the questionnaires. Improvements in TMD symptoms were reported in 10 patients (26%), were unchanged in 16 patients (41%) and worsened in 13 patients (33%). Only 8 patients (21%) were satisfied with the follow-up of the suggested treatments from their GMP. Significant improvements of symptoms were noted in MFIQ (jaw function), GPI (including pain intensity at maximum and suffering from pain), and CSQ (pain related catastrophizing), in all 39 TMD patients as one group. However, a subgroup analysis showed that the significant improvements were mostly within patients who reported improvement of TMD symptoms. A high pain intensity at baseline was a significant risk factor (OR = 5 .79, 95% CI: 1.34, 24.96) for patients who reported worsening of TMD symptoms at follow-up.
Conclusion: High pain intensity at baseline was a significant risk factor for poorer recovery three years after an interdisciplinary evaluation. Our data support the notion that improved coping with TMD pain includes both decreased pain intensity, CSQ and MFIQ scores.
Keywords: catastrophizing, interdisciplinary, orofacial pain, refractory pain, stress, evaluation
Introduction
Temporomandibular disorders (TMD) are characterized by pain and dysfunction of the temporomandibular joint (TMJ) and the masticatory apparatus.1,2 The prevalence of TMD related signs and symptoms has been estimated to be approximately 30% in the general population,3 predominantly in women.4 The Orofacial Pain Prospective Evaluation and Risk Assessment (OPPERA) study has reported a 4% incidence per year of first onset of TMD.1 TMD has been linked to many comorbidities including fibromyalgia, irritable bowel syndrome, and depression, additionally to trauma and stress symptoms.1,5–9 Significantly higher prevalence of psychosocial factors such as somatic awareness, distress, catastrophizing, pain amplification, and psychosocial stress in subjects with TMD symptoms compared to healthy individuals, was observed in the OPPERA study.1,10 Our group have previously reported increased saliva levels of stress hormones together with increased psychometric scoring, decreased pain thresholds and catastrophizing as predictors for TMD.11,12
Several systematic reviews of TMD highlight the lack of evidence on how to base management decisions.13–15 In 2013, the Norwegian Ministry of Health established a national interdisciplinary evaluation program for TMD patients at Haukeland University Hospital (HUH) in Bergen, Norway. The missions were to establish an assessment program consisting of several specialists who would characterize the patient group, and establish national guidelines for assessment and treatment of TMD.16 Chronic oral and facial pain, including TMD has been determined to be multifactorial and therefore should be investigated and treated by an interdisciplinary team in order to arrive at the correct diagnoses and provide appropriate and tailored treatments for the patients.17 It is preferable that medical specialists, psychologists, physiotherapists, and dental specialists are all included in the team and together assess and treat these patients18 to avoid patients being referred from one specialist to another and further subjected to treatment previously tried by other disciplines. The goal of our approach is to evaluate the patient’s condition from as many different perspectives as possible and come up with a treatment plan that can be followed up by the patient’s GMP. Further, it is important to exclude other diseases, give the patient an explanation of why they are in pain as well as give them different strategies for managing their pain and ensuring the best possible quality of life.16,18–20
There are no agreed, standardized guidelines for outcome measures of chronic pain management in clinical trials, but it has earlier been suggested that such measures should incorporate at least some of the 6 proposed core domains;1 pain;2 physical functioning;3 emotional functioning;4 participant ratings of improvement and satisfaction with treatment;5 symptoms and adverse events; and6 participant disposition.21,22
The present study was a follow up of patients with long-term refractory TMD who had been evaluated at the interdisciplinary clinic at HUH for a minimum of three years. The overall objective was to identify risk factors of non-resolving TMD, which may indicate the need for earlier treatment of these patients. Further objectives were to assess patients TMD symptoms, physical function, and psychosocial variables, and patients’ satisfaction with treatments proposed by the interdisciplinary team.
Materials and Methods
Study Design
The present study was a longitudinal self-assessed questionnaire-based study of a group of patients with long term refractory TMD symptoms who had been evaluated at the Haukeland University Hospital (HUS) in Bergen with a follow-up of 3 years.16 In addition, patients’ satisfaction with the suggested treatments and follow-up by their GMP was evaluated. Pain related symptoms and dysfunction (both general and TMD-related), general health status, psychosocial factors, previous treatment and medication, and the duration of pain and disease were included in the evaluation.
Ethics
Ethical approval was granted by the Regional Ethical Review Board Southeast (2015/930) for the first examination, and for the present study (2018/647), in accordance with the Helsinki Declaration (1964). A written informed consent was received from all subjects who participated in the study.
Participants
Our study population consisted of 60 TMD patients, all affected with long term refractory TMD symptoms. The patients were referred to the National TMD-project from all health regions in Norway, by their GMP during the years 2013–2015 for an assessment by the interdisciplinary team and were consecutively included in the study. The inclusion criteria were adults older than 18 years with long-term TMD-related pain assessed by their GMP. The study patients were diagnosed by the team in accordance with a beta version of the TMD guidelines from the Norwegian National Health Directorate that were published in 2016,23 which are comparable to the diagnoses included in the Diagnostic Criteria for TMD (DC/TMD).24 Exclusion criteria were non-TMD-related orofacial pain, drug dependency, psychiatric diagnoses, and unresolved economic disability claims.
Baseline Data (First Evaluation)
The first evaluation was performed by the interdisciplinary evaluation team at HUH. The patients had completed a comprehensive questionnaire about their symptoms prior to the clinical examination. The questionnaire covered pain and other symptoms, psychosocial factors, physical functioning, symptoms, and adverse events (eg, facial trauma). A four-item GPI was used to indicate the TMD patients’ subjective experience of pain and the degree of suffering from pain using the NRS. The patients reported their:1 pain intensity at its minimum,2 pain intensity when it was at its maximum,3 how much they suffered from the pain, and4 the lowest pain intensity they could accept to live with. A 0–10 NRS was used, where 0 represents no pain at all, and 10 represents the worst imaginable pain.25 Other questionnaires were the HADS,26 a 2-item version of the CSQ27 regarding pain catastrophizing, RMS28 and a shortened version of MFIQ. The RMS consisted of 24 claims regarding physical disability caused by general pain. The MFIQ is a tool for measuring mandibular function.29 The questionnaire was a shortened version and consisted of five claims regarding mandibular functional impairment related to speech, yawning, and chewing. Claims regarding work were excluded from the MFIQ due to possible bias, since a significant proportion of TMD patients were unemployed or disabled by chronic pain. The claims were rated from 0–4, where 0 was “no difficulties” and 4 “was impossible without help”.
Six different specialists examined the patients in the interdisciplinary team, an oral and maxillofacial surgeon, a dental specialist in orofacial pain, a pain physician, a physiotherapist, a clinical psychologist, and a medical radiologist. At the final consultation, the results of the assessment were presented to the patient along with an explanation of why they are in pain followed by treatment suggestions which were discussed with the patients and their relatives. A questionnaire with seven questions about how satisfied they were with the evaluation was given to the patients. The patients were informed that the rating of the evaluation was anonymous. The seven questions were: 1) Did you expect that the cause of pain could be detected? 2) Were you well received by the team? 3) Do you find the team to be skilled professionals? 4) Did the team show you respect? 5) Did you get proper information about the condition you have? 6) Did you get adequate information about the condition you have? 7) Was the investigation as expected? They were asked to fill it in at home and send it back by mail. All questions were rated from 1–10, where 1 was “totally satisfied” and 10 was “completely dissatisfied”.
The suggested treatment plan was reported to their GMP with a request of a follow up. A description of the interdisciplinary work up and a characterization of the patient group with severe TMD has previously been published.11,12,16,30,31
Three-Year Follow Up
Three years after the interdisciplinary evaluation, the patients received a comprehensive questionnaire by mail, similar to the questionnaire that they had filled in at the first evaluation with the addition of questions regarding their satisfaction with the follow-up by their GMP. Further, there were questions regarding the progression of their TMD symptoms (on a five-point scale, from much improved to much worse) and general health symptoms (on a three-point scale, from improved to worse), what kind of treatments they had received and the outcome of the treatments. If they did not answer the questionnaire, they were reminded by the first author via a telephone call.
Statistical Methods
All statistical analyses were performed in STATA version 16 (StataCorp, College Station, TX, USA). Data from the first evaluation, were considered as baseline values for comparison with follow up values in the statistical analyses. Mean, median, range, and standard deviation (SD) were calculated for continuous variables. A Wilcoxon matched test was performed for comparison of GPI, HADS, RMS, CSQ and MFIQ, between the first examination and the follow-up. For further statistical analyses, the patients were divided into three subgroups: 1 Improvement of TMD symptoms (Group 1), 2 No difference in TMD symptoms (Group 2), and 3 worsening of TMD symptoms (Group 3). A Kruskal Wallis test with a post hoc Dunn test was performed to calculate significant differences (alpha = 0.05) between the three subgroups at both baseline and follow-up. A Wilcoxon matched test was used to calculate the p-value of no difference within the three subgroups from baseline to follow-up. A logistic regression model with the two subgroups Group 1 (improvement of TMD symptoms) and Group 3 (worsening of TMD symptoms) as the dependent variable and multiple independent baseline variables was performed as well. Both the unadjusted model, and adjusted model with stepwise forward method were calculated. For the adjusted model, the probability of enter (pe) was set to p<0.2, and the probability of removal (pr) was set at p>0.4. A Chi-squared test was performed to measure association between TMD symptoms and general health in the 3×3 Table 1.
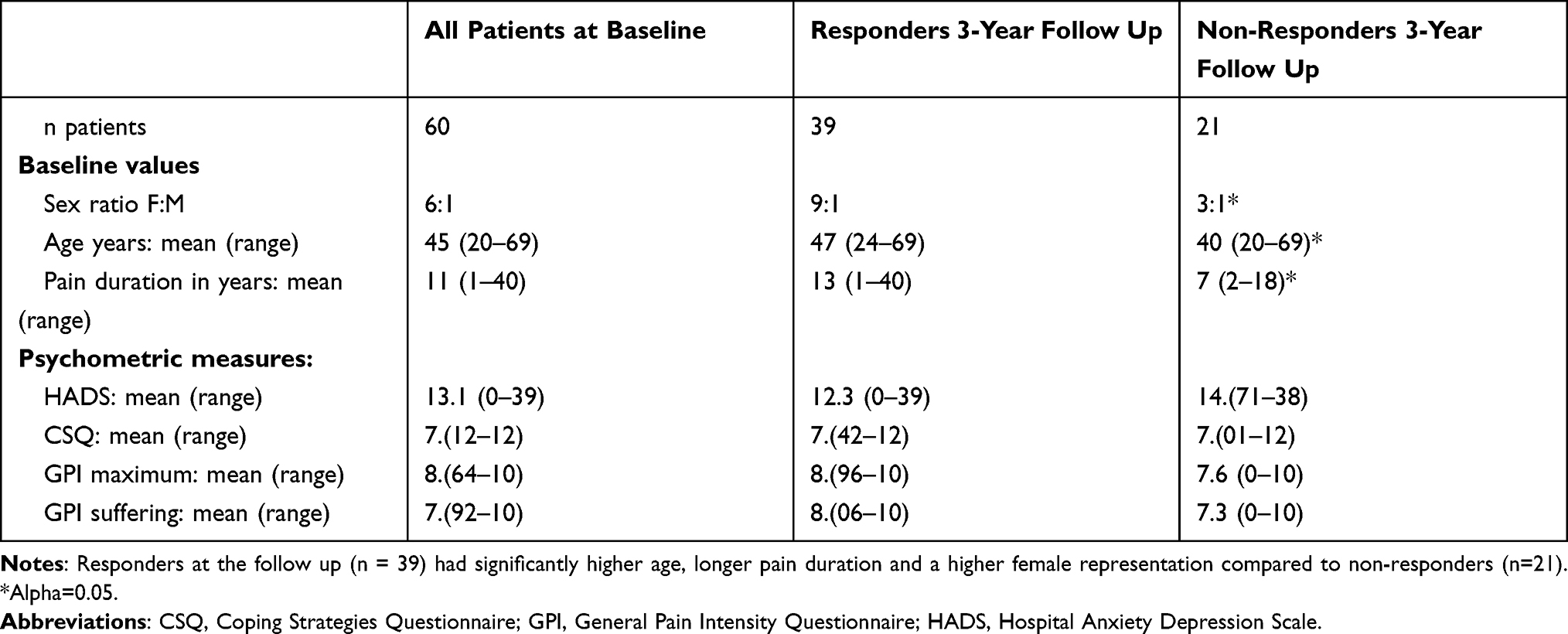 |
Table 1 Drop-Out Analysis Between Responders and Non-Responders at the 3-Year Follow Up Study |
Results
Baseline Registrations
Baseline characteristics of all patients (n=60), responders at the three year-follow up (n=39), and non-responders at follow-up (n=21) are presented in Table 2. The TMD diagnoses in the whole study group of 60 patients were myalgia (n = 22), arthralgia (n = 1), disc derangement (n = 2), and combinations (n = 35). All 60 patients completed the evaluation of the interdisciplinary investigation. In general, the patients were very satisfied with the evaluation. The distribution of data from the 60 TMD patients who responded at the follow up are presented in Figure 1.
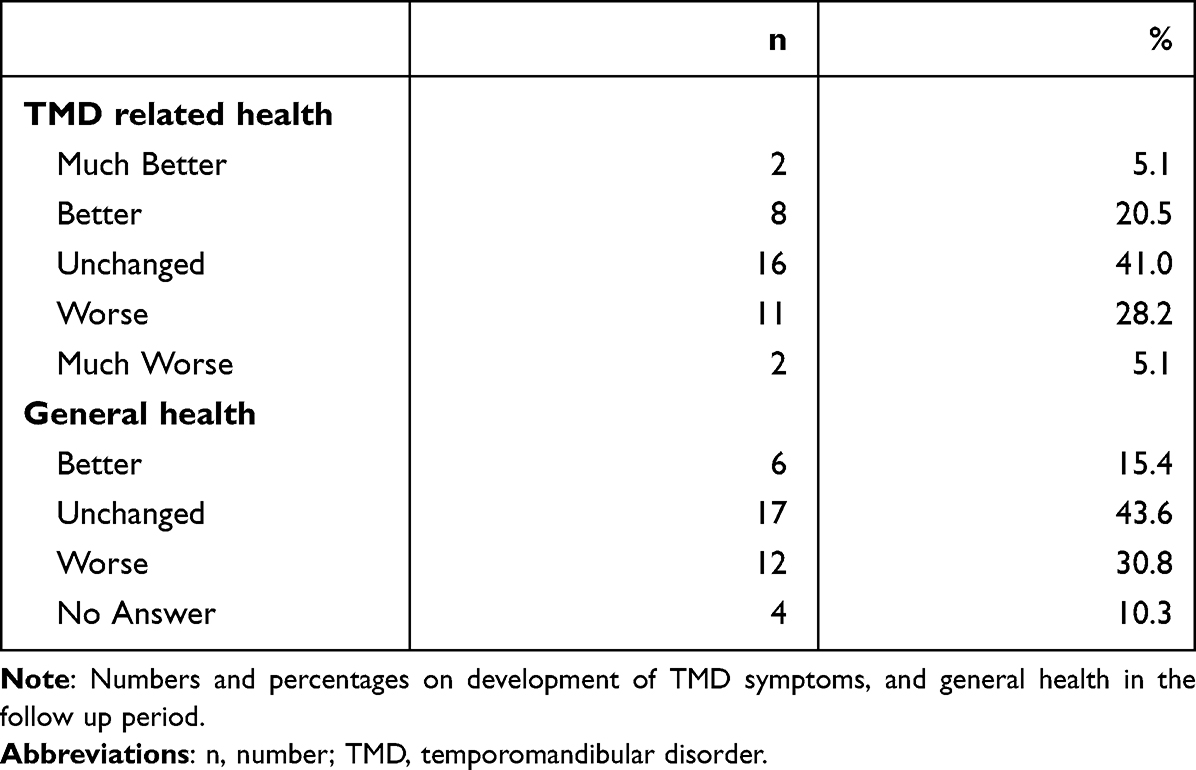 |
Table 2 Patient’s Health Development (n=39) |
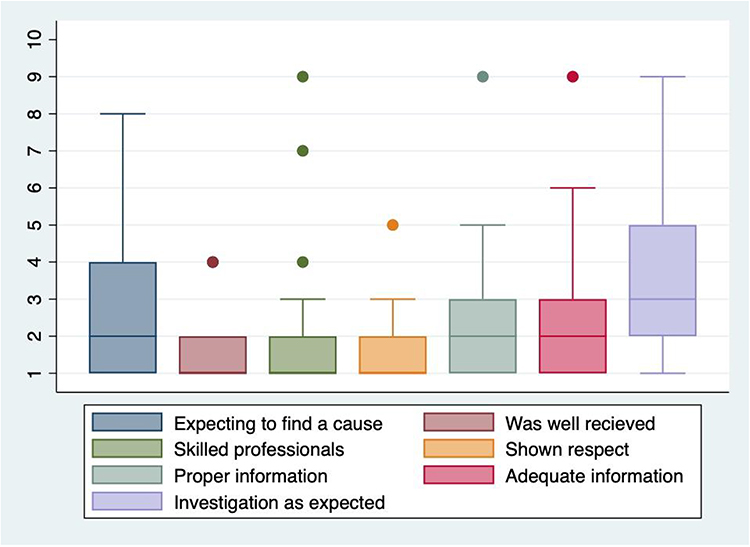 |
Figure 1 Rating of the interdisciplinary evaluation. Abbreviations: HUH, Haukeland University Hospital in Bergen, Norway; TMD, temporomandibular disorder. Notes: Results are from the patient’s own evaluation after the interdisciplinary investigation of TMD patients at HUH (n=60). The evaluation consisted of seven questions regarding the patients’ experience of the examination and evaluation process. Answers were rated from 1–10, where 1 was “totally satisfied” and 10 was “completely dissatisfied”. The ratings were anonymous and could not be linked to the patients who were informed of this. |
Follow-Up Registrations
Of the 60 TMD patients who participated in the interdisciplinary investigation program, 39 patients answered the follow-up questionnaires. The baseline characteristics of the 39 responders compared to the 21 non-responders are shown in Table 2. There were some missing answers in the 39 completed questionnaires. The number of patients who filled in the questionnaires is specified in each table of the 39 patients at follow up, the initial diagnoses included myalgia (n = 11), arthralgia (n = 1), disc derangement (n = 2), and combinations (n = 25).
TMD Related Health and General Health
TMD symptoms were improved in 10 patients (26%), unchanged in 16 patients (41%), and worsened in 13 patients (33%) (Table 3). General health symptoms were improved in 6 patients (15%), unchanged in 17 patients (44%) and worsened in 12 patients (31%) (Table 3). The coincidence between TMD symptoms and general health at follow up is presented in Table 1.
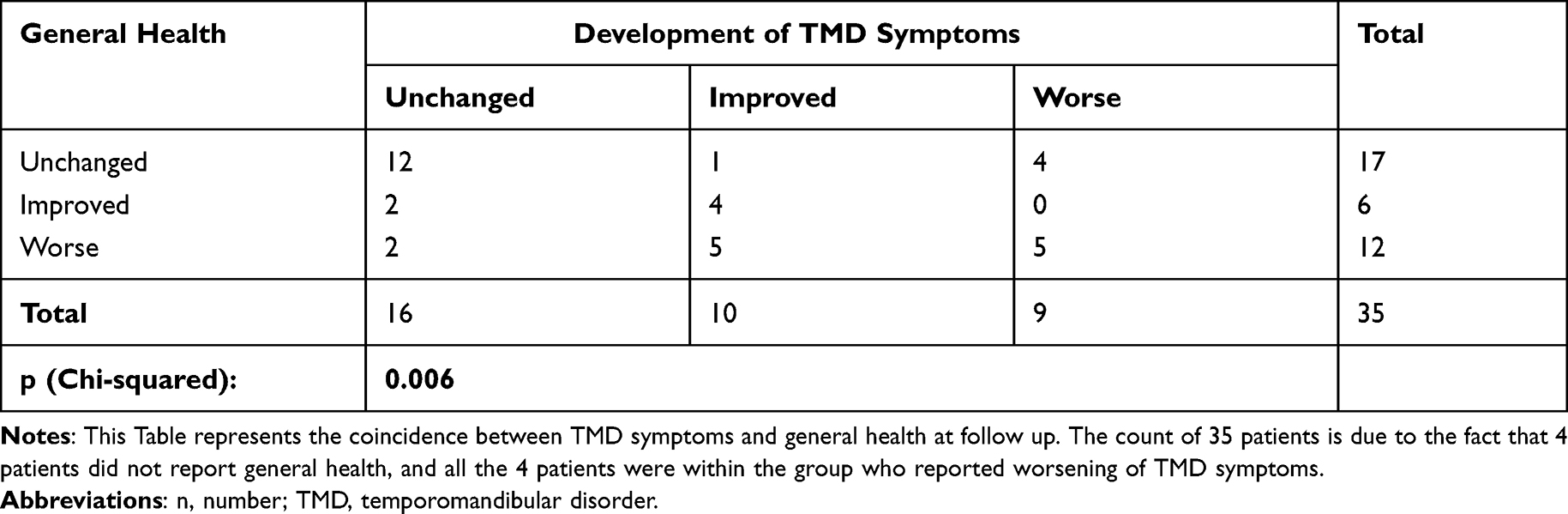 |
Table 3 Coincidence Between TMD Symptoms and General Health (n=35) |
Pain Intensity and Suffering from Pain
Improvements in the maximum pain intensity (NRS 0–10) was reported at the follow-up (from NRS 9.0 to 8.0; p<0.001), and the highest level of suffering from pain decreased (median value from 8.0 to 7.0; p<0.001). No statistical differences were reported in the minimum pain (p=0.38), nor in the option of the highest pain intensity that the patients would accept to live with (p=0.11) (Figure 2A–D).
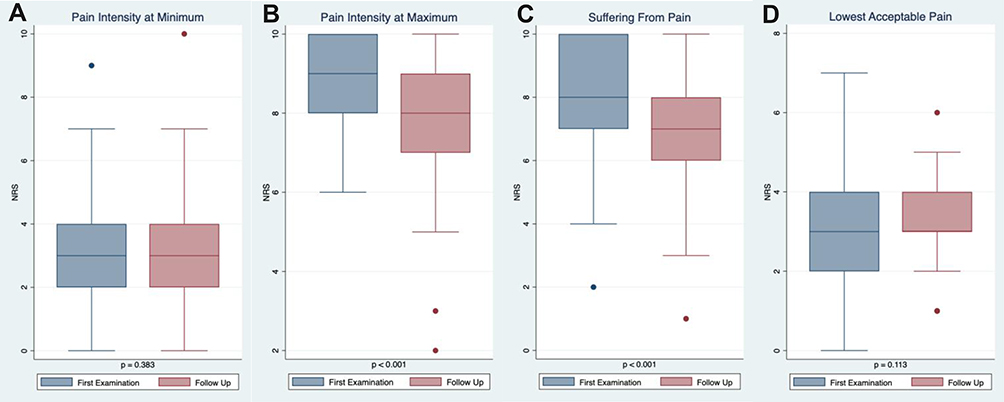 |
Figure 2 (A–D) General Pain Intensity and degree of suffering. Results from the GPI, using a NRS (0–10), where 0 refers to no pain, and 10 refers to the worst imaginable pain. Data are from the 39 patients who completed the questionnaire at the follow-up study. The results from the follow-up are compared to the first evaluation. Abbreviations: GPI, General Pain Intensity Questionnaire; NRS, Numeric Rating Scale. |
Functional Related Questionnaires
The MFIQ score was significantly lower at the follow-up compared to the baseline level (decrease in median value from 12.0 to 10.0; p<0.001). The RMS was not significantly changed (p=0.218) (Table 4).
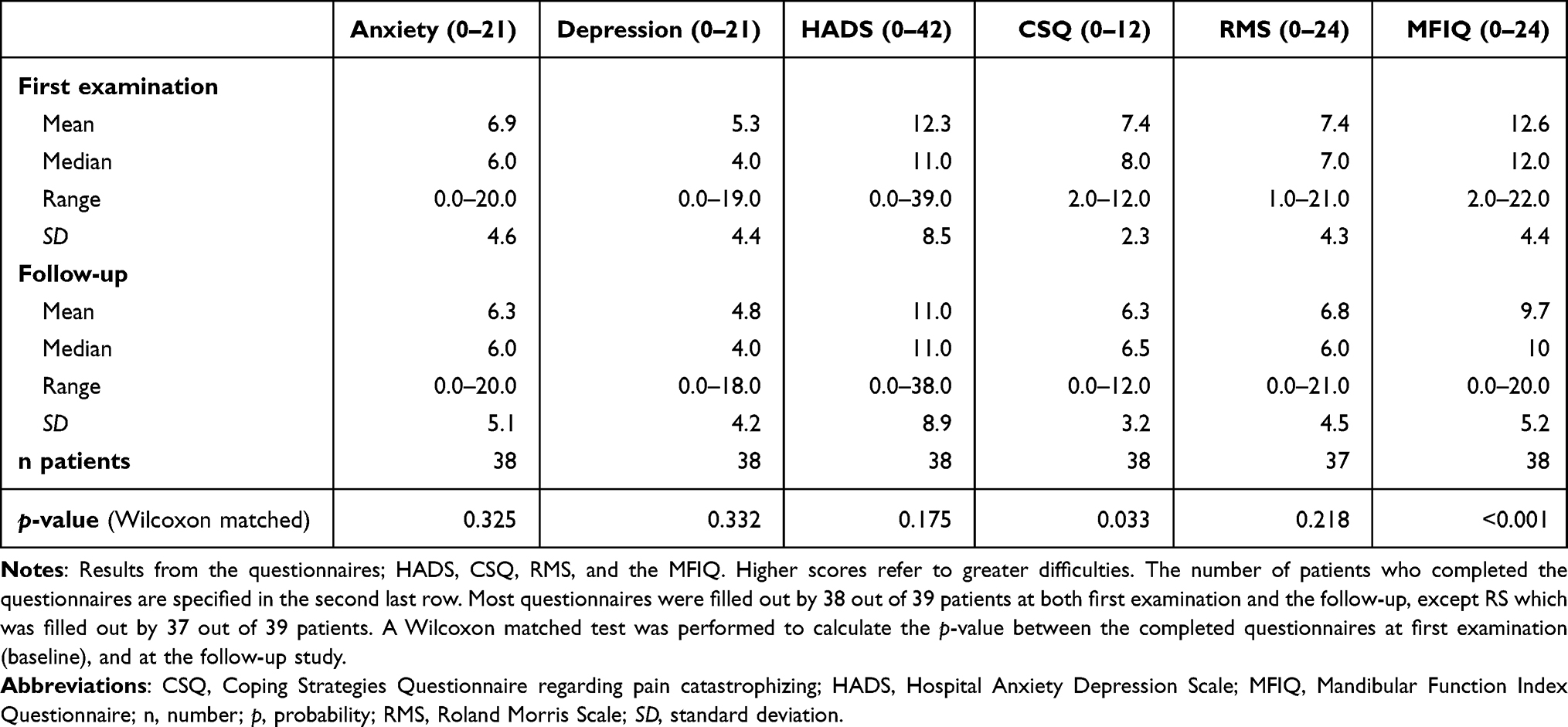 |
Table 4 Results from Psychosocial- and Functional Related Questionnaires |
Psychosocial-Related Questionnaires
The results from the CSQ significantly showed a lower score at the follow-up compared to the baseline level (decrease in median value from 8.0 to 6.5; p=0.03). No statistical differences were observed in HADS (p=0.175), anxiety (p=0.33), and depression (p=0.32) (Table 4).
Satisfaction of the Follow Up by Their GMP
Only 8 patients (21%) were satisfied with the follow-up by their GMP, while 15 patients (39%) were dissatisfied. Eleven patients (28%) were not sure, and three patients (8%) reported that their GMP did not follow-up at all. Two patients (5%) did not answer.
TMD Related Treatments and Outcome
Self-reported treatments of TMD are presented in Table 5 (n=39). The most frequently reported treatment was an occlusal splint (n=27, 69%). The second most frequent treatment was analgesics, reported by 24 patients (62%). The third most frequent treatments were physiotherapy and self-treatment/ exercises, both reported by 22 patients (56%). It should be noted that individual patients could have had several different treatments (Table 6).
 |
Table 5 Treatment of TMD in the Follow Up Period |
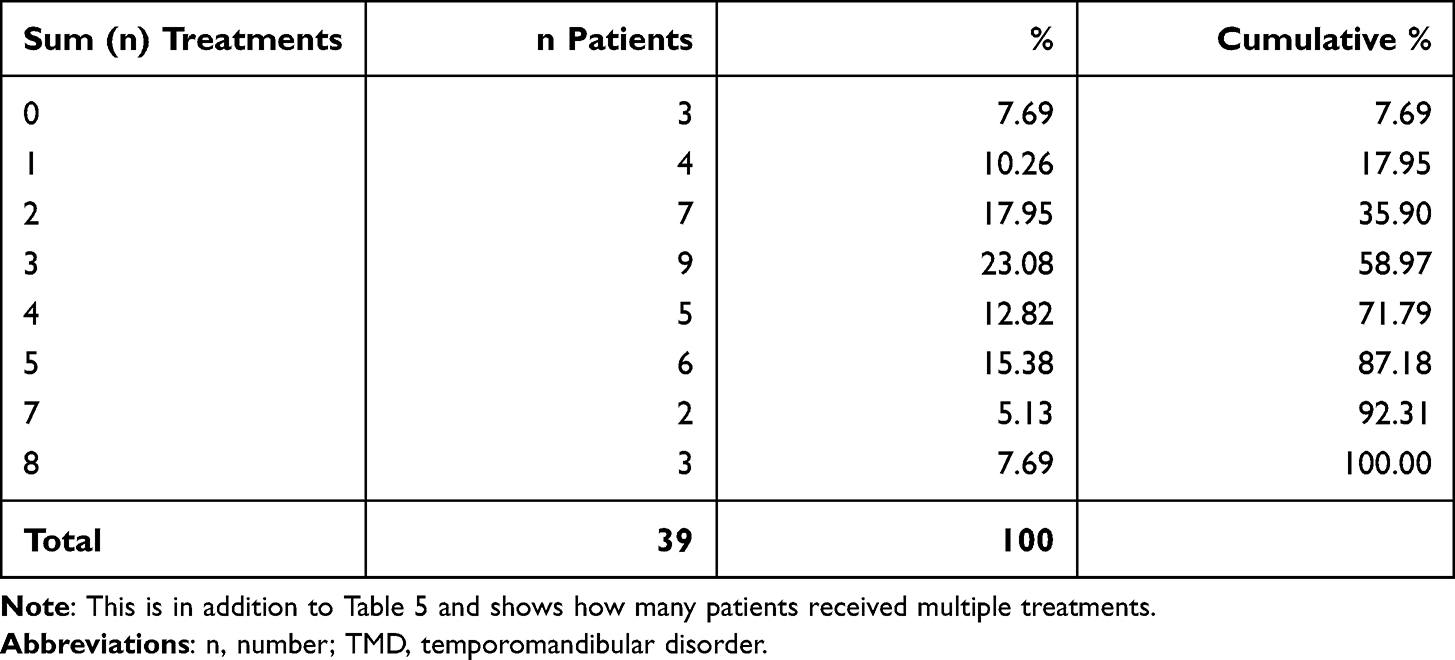 |
Table 6 Number of Several Different Treatments |
Subgroup Analysis
In the group that reported worsening of TMD symptoms (Group 3), the maximum pain intensity was significant higher at baseline compared to the other groups (Table 7, time a). Furthermore, Group 3 had significant higher minimum pain intensity, higher maximum pain intensity as well as higher level of suffering from pain, followed by Group 2>Group 1 (Table 7, time b). Further, Group 1 patients showed significantly lower minimum pain, maximum pain and suffering from pain at the follow up (Table 7).
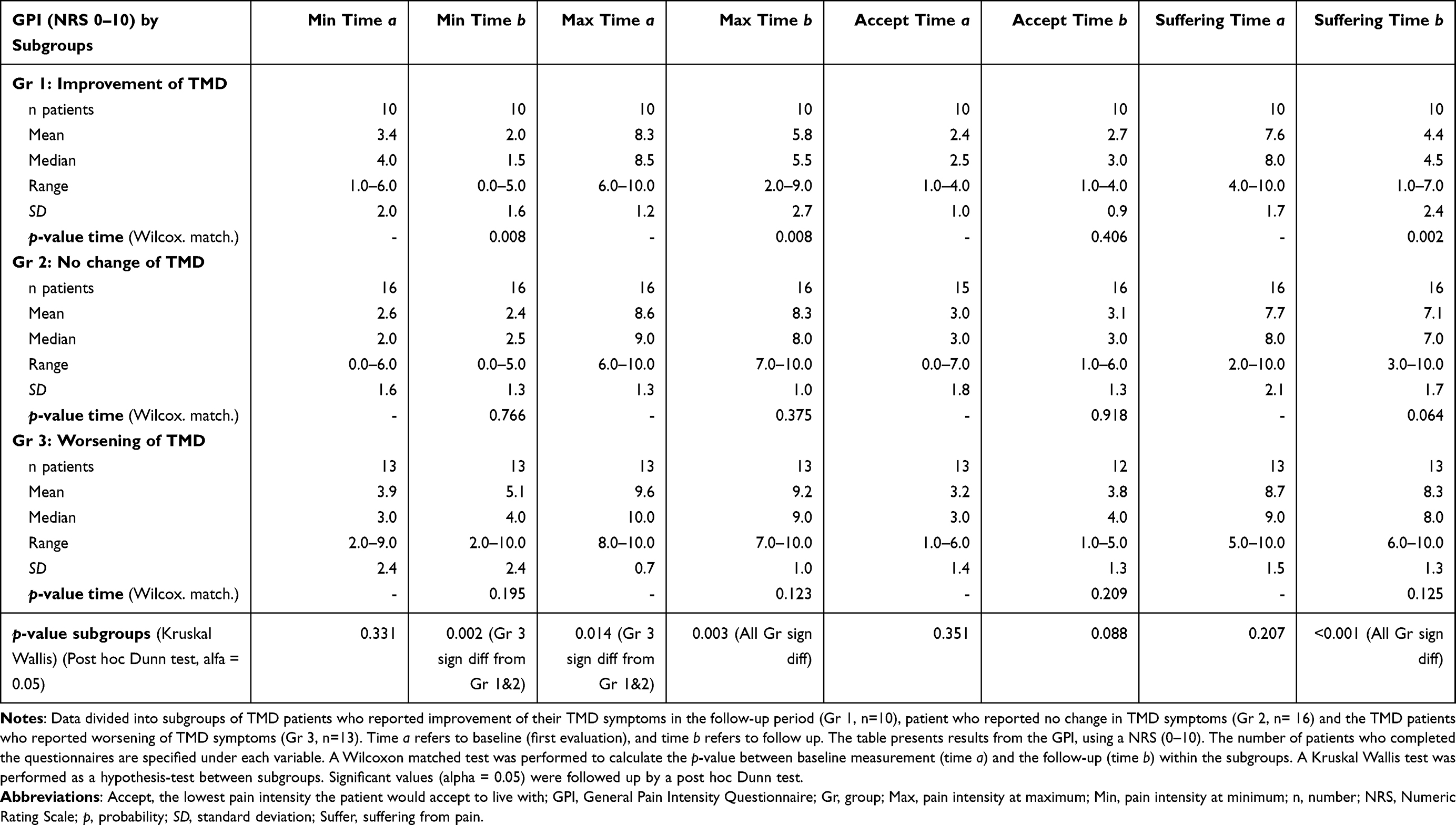 |
Table 7 Subgroup Analysis of General Pain Intensity Using a NRS (0–10) |
No statistical differences were seen between the three subgroups at baseline analyzing HADS, CSQ, RMS, and MFIQ (Table 8, time a). But at the follow up, significantly lower (positive outcome) CSQ score in Group 1, and significantly higher (negative outcome) MFIQ in Group 3 were seen (Table 8, time b). Improvement in MFIQ scores was observed within Group 1 and 2 from baseline (time a) to the follow up (time b), while only the patients in Group 1 had a significant decrease in CSQ score (Table 8). A logistic regression model showed that high maximum pain intensity at baseline was a significant risk factor to reported worsening of TMD symptoms at follow-up (Table 9).
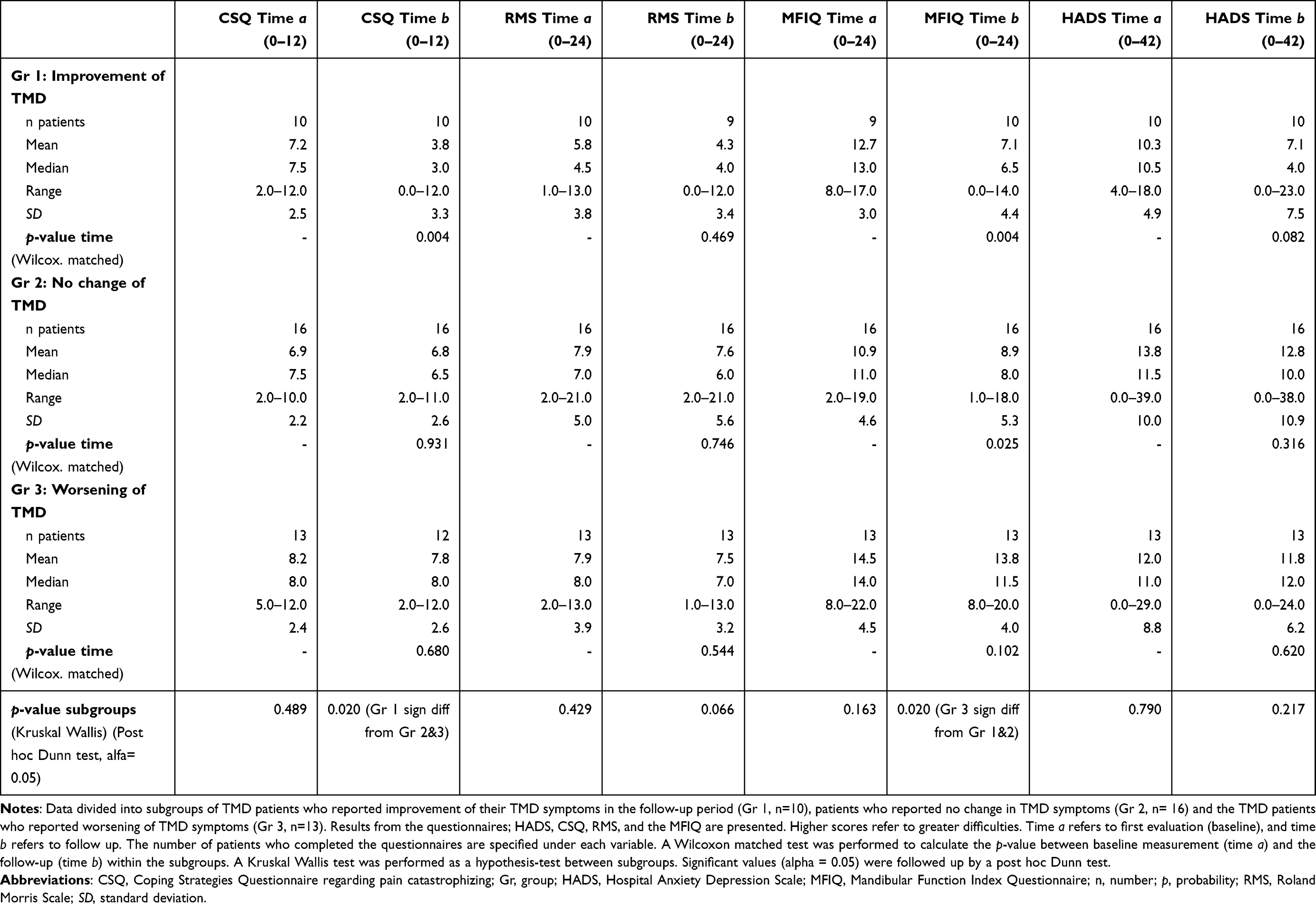 |
Table 8 Subgroup Analysis of Psychosocial- and Functional Related Questionnaires |
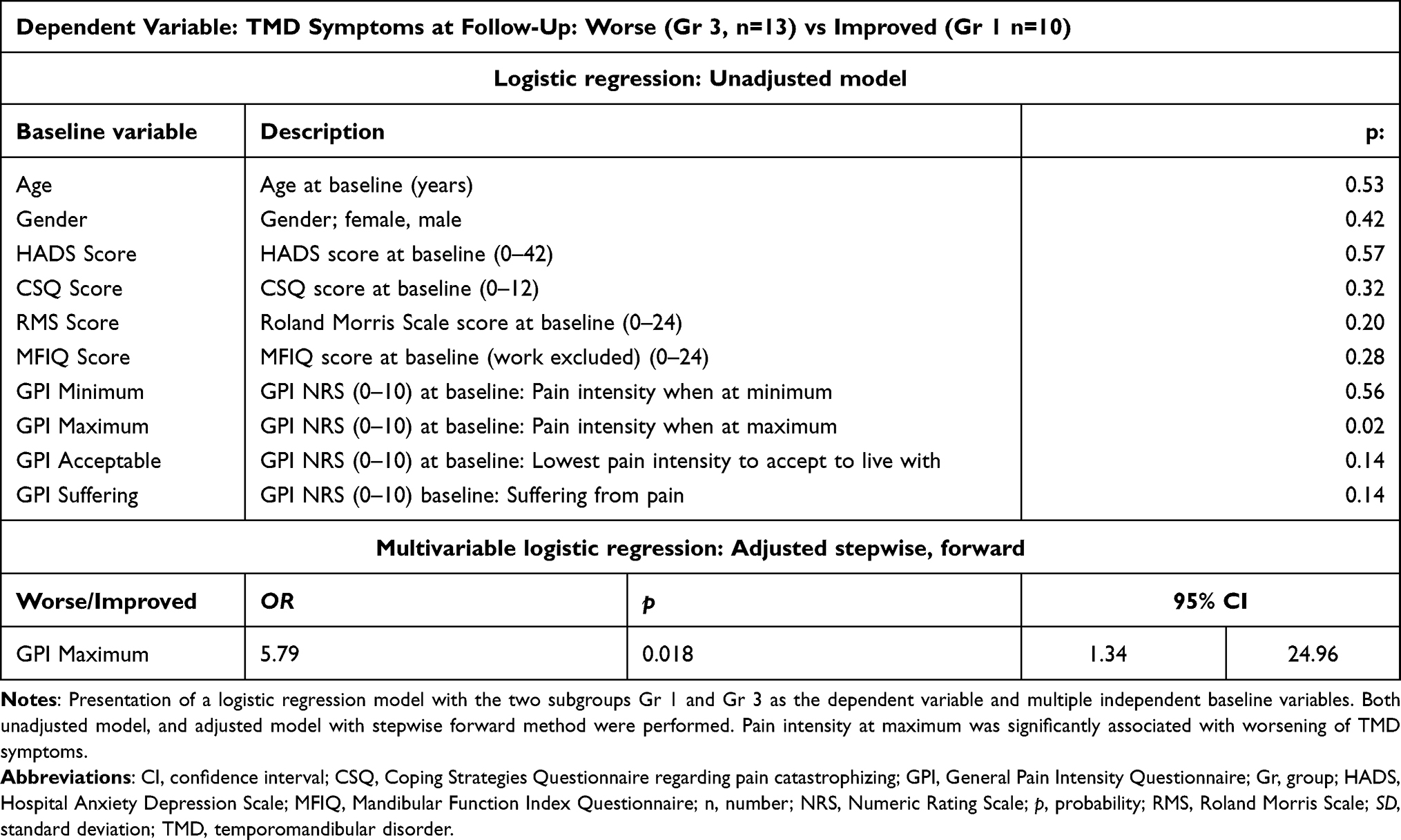 |
Table 9 Logistic Regression of Baseline Variables |
Discussion
This study presents a three-year follow-up of a group of patients with long term refractory TMD, with a mean of 13.4 years of pain, who were assessed by an interdisciplinary team in a National Norwegian program for TMD patients, on request from the Norwegian Health Directorate, a part of the Government. As a group, the TMD patients were satisfied with the interdisciplinary evaluation at baseline, but the majority of these patients were dissatisfied with the follow up by their GMP three years later, and only one third of the patients reported an improvement in their TMD symptoms at follow up. One third reported unchanged status and one third reported worsening of their TMD symptoms, where high pain intensity at baseline was considered as a risk factor. In those with a positive outcome, we observed statistically significant improvement in some measures, such as mandibular function, maximum pain intensity and pain related catastrophizing.
Long-term follow-up results of chronic TMD in the OPPERA study have been reported and an improvement of TMD was shown, including jaw function, pain pressure thresholds, psychosocial variables and somatic symptoms.32 In our study, we also observed some improvements in functioning and psychosocial factors, even in those patients who reported their TMD symptoms unchanged. However, it is important to note that the patients in our study were long term refractory TMD (13.4 years), and our results may therefore differ from other studies.
Other factors may influence outcomes as it has been shown that physical and emotional functioning might affect the pain intensity over time.21 The presence of several TMD-associated clinical findings, has been associated with a poorer treatment outcome compared to if there is only one finding.33 Also, the number of other comorbidities is associated with higher pain intensity and duration in TMD.34 Discrepancies between patient’s subjective feeling and the clinician’s objective evaluation are common and may explain differences between symptoms and clinical findings.35
There is evidence that interdisciplinary evaluations and treatments improve quality of life in chronic pain patients.18 Several studies suggest the need for improvement in the interdisciplinary approach with the development of individual/tailored pain treatments as well including both dental and medical specialists in the interdisciplinary team.17,18,36 Furthermore, the patients should not only be investigated by an interdisciplinary team, but they should also be treated by the disciplines recommended. It is also important to simultaneously manage psychological comorbidities to achieve the intended treatment outcome in patients with chronic orofacial pain.17
As shown in this study, the patients rated the interdisciplinary evaluation highly. Most of the patients resided in other parts of the country and were referred back to be treated at their place of residence. Since specialists are concentrated in cities in Norway there can be lack of specialist treatments and multidisciplinary teams in rural areas. It was assumed that the treatment suggestions from the interdisciplinary team would be followed up by the GMP but most of the patients were not satisfied with the follow up that they actually received, reflecting the situation that most patients did not get the opportunity to be treated in an interdisciplinary way. Other factors that may explain why most patients in the present study did not report improvement in their TMD symptoms might be that this patient group had long term refractory pain at their initial visit. A large longitudinal register study of chronic pain in Norway (HUNT Study) has shown that treatment of long-term chronic pain, especially in combination with psychosocial factors, has a poor prognosis.35
In this study the maximum pain or how much the patients suffered from pain was improved at follow-up, though the pain intensity was still high. In the subgroup analysis, among those who reported that the TMD symptoms had improved, lower pain intensities and less suffering from pain was reported. In the groups that reported that the TMD symptoms were unchanged or worse, pain intensities were not significantly different from baseline. Higher pain intensity has also been associated with poorer TMD prognosis in a previous longitudinal study,37 as well as patients who experience pain more frequently have a poorer prognosis.38 Adaptation to chronic pain has been supported by findings from long-term follow-up of TMD patients in the OPPERA study, where the pain intensity significantly decreased.32 It seems that adaptation to pain is more common among those with lower pain intensity compared to those with higher pain intensity as was the case in this study. This is further supported by the results from the present study that the best predictor for reporting worsened TMD symptoms at follow up, was high pain intensity at baseline.
In this study, the TMD patients still had high scorings in CSQ and HADS at the follow-up, though the CSQ was statistically decreased compared to baseline. While the CSQ score was statistically equal in all subgroups at baseline, there was a significantly lower CSQ score among those who reported improvement at the follow-up. Chronic stress in patients with TMD has been considered an important characteristic of TMD, as previously shown by high CSQ and HADS scores.11,12,39 Psychosocial factors, including stress, have also been considered as a major risk factor in TMD,1,10,40 in the development of chronic pain.41 Elevated CSQ may indicate poorer prognosis for pain relief in chronic pain in general.41 Results from the OPPERA study have shown that pain catastrophizing may decrease in long term (median 7.6 years) follow-up of chronic TMD,32 even without associations with subjective improvement of TMD. However, findings from the present study together with previous studies may indicate that improved coping with TMD includes both decreased pain intensity and CSQ scores.
In a large longitudinal study, longer duration of chronic pain and higher pain intensity were significantly associated with anxiety and depression disorders, suggesting that both pain and psychological disorders have a worsening impact on each other.42 Furthermore, psychosocial factors are considered important in the perception and tolerance of pain.43 The experience of fear related to pain is individual and may increase pain intensity and anxiety in two ways;44 where pain leads to avoidance of physical activity and the anxiety related to pain might increase the focus on pain and result in higher suffering.45 Chronic pain and psychological symptoms such as anxiety and depression are commonly observed together and may reinforce each other and impair the prognosis for the improvement of chronic pain.42,46 It has also been suggested that both pain and stress might modulate the same neurobiological pathways, which have a major effect on the outcome of their endocrinologic signals.47–49 Results from a Randomized Controlled Trial (RCT), with one-year follow up, showed that patients who had been educated to self-treatment of TMD, reported significantly greater decrease of pain intensity, and increase in coping with pain, compared to patients who received TMD treatment by health professionals.50 These results may indicate that it is important for the patient to take responsibility for their own recovery.
Recommended treatment of TMD includes jaw muscle exercises, relaxation exercises, and sometimes an occlusal splint or NSAIDs.2,23,51,52 The authors of a recent RCT study have concluded that jaw motion exercises are a cost-effective and pain reducing treatment.52 The most common treatments reported by patients in our study were conservative treatments, including jaw muscle exercises, occlusal splint, and physiotherapy. The fact that only 10 out of 39 patients reported improvement of TMD might be due to different circumstances including the fact that the GMP and not the general dentist had the responsibility for the follow up and treatment. The GMP does normally not treat TMD and the general dentist might lack knowledge of how to treat TMD. Treatment of severe TMD belongs to specialists, both within dentistry and medicine, who ideally should form interdisciplinary teams, however there is a shortage of specialists in rural parts of Norway.
Treatment of chronic pain is a challenge; available treatment options do not necessarily reduce pain intensity or improve psychological and functional variables in an effective manner.53 However, during the last few decades there has been a switch in the scientific approach to chronic pain, from a direct linear association with tissue damage, to a multifactorial etiology including several biopsychosocial factors.54 It has reasonably been suggested that psychosocial health care should be involved in treatment of chronic pain and the appropriate goal for the future should be individualized pain management program for each patient.17,55
Limitations to this study include the reliability and validity of the self-reported questionnaires. A previous study on the outcome of treatment for TMD reported a 44% discrepancy between the doctor’s evaluation and the patients’ answer to a TMJ symptom and function assessing questionnaire in which patients scored their symptoms both better and worse.35 The Authors had no control over whether the patients followed up with their GMP, in accordance with the suggested treatment plan. The relatively small study population and low response rate, and the fact that the patients were not clinically examined at follow up should also be considered as a limitation. In the drop-out analysis, patients who responded at the three-year follow-up had a longer pain duration and slightly higher age at baseline compared to the non-responders (Table 1) suggesting that a possible selection bias might be that responders were more severely affected than non-responders.
Conclusion
This study of patients with long-termed refractory TMD, evaluated by a Norwegian Government sponsored interdisciplinary team showed that high pain intensity at baseline was a significant risk factor for poorer recovery after three years. Findings from the present study together with previous studies may indicate that improved coping with TMD pain includes both decreased pain intensity, CSQ and MFIQ scores. The authors want to encourage further research on management of stress in the presence of chronic pain as an important factor for treatment outcome. Furthermore, it is important to improve access to trained care in rural areas and to maintain the interdisciplinary process. If the Interdisciplinary team were to follow up with the patients and the GMP/general dentist, the results of the treatment could be improved. To further increase the quality of care, a personalized, digital rehabilitation program with feedback could be established, which could give the patient the opportunity to take responsibility for their own recovery.
Acknowledgments
The authors of the present study want to thank all patients for participating. We also want to thank the Norwegian Directorate of Health for funding this study, and Professor Stein Atle Lie for his contribution to the statistical analyses.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Slade GD, Ohrbach R, Greenspan JD, et al. Painful temporomandibular disorder: decade of discovery from OPPERA studies. J Dent Res. 2016;95(10):1084–1092. doi:10.1177/0022034516653743
2. Scrivani SJ, Keith DA, Kaban LB. Temporomandibular disorders. New Engl J Med. 2008;359(25):2693–2705. doi:10.1056/NEJMra0802472
3. Valesan LF, Da-cas CD, Réus JC, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig. 2021;25(2):441–453. doi:10.1007/s00784-020-03710-w
4. Bueno CH, Pereira DD, Pattussi MP, Grossi PK, Grossi ML. Gender differences in temporomandibular disorders in adult populational studies: a systematic review and meta-analysis. J Oral Rehab. 2018;45(9):720–729. doi:10.1111/joor.12661
5. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley AW
6. De La Torre Canales G, Câmara-Souza MB, Muñoz Lora VRM, et al. Prevalence of psychosocial impairment in temporomandibular disorder patients: a systematic review. J Oral Rehab. 2018;45(11):881–889.
7. Ayouni I, Chebbi R, Hela Z, Dhidah M. Comorbidity between fibromyalgia and temporomandibular disorders: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019;128(1):33–42. doi:10.1016/j.oooo.2019.02.023
8. Mottaghi A, Menéndez-Díaz I, Cobo JL, González-Serrano J, Cobo T. Is there a higher prevalence of tinnitus in patients with temporomandibular disorders? A systematic review and meta-analysis. J Oral Rehab. 2019;46(1):76–86. doi:10.1111/joor.12706
9. Häggman-Henrikson B, Rezvani M, List T. Prevalence of whiplash trauma in TMD patients: a systematic review. J Oral Rehab. 2014;41(1):59–68. doi:10.1111/joor.12123
10. Fillingim RB, Slade GD, Diatchenko L, et al. Summary of findings from the OPPERA baseline case-control study: implications and future directions. J Pain Offic J Am Pain Soc. 2011;12(11 Suppl):T102–7. doi:10.1016/j.jpain.2011.08.009
11. Staniszewski K, Lygre H, Bifulco E, et al. Temporomandibular disorders related to stress and HPA-axis regulation. Pain Res Manage. 2018;2018:7020751. doi:10.1155/2018/7020751
12. Willassen L, Johansson AA, Kvinnsland S, Staniszewski K, Berge T, Rosén A. Catastrophizing has a better prediction for TMD than other psychometric and experimental pain variables. Pain Res Manag. 2020;2020:1–8. doi:10.1155/2020/7893023
13. Mujakperuo HR, Watson M, Morrison R, Macfarlane TV, Pharmacological interventions for pain in patients with temporomandibular disorders. Cochrane Database Syst Rev. 2010;10:Cd004715. doi:10.1002/14651858.CD004715.pub2
14. Fricton JR, Ouyang W, Nixdorf DR, Schiffman EL, Velly AM, Look JO. Critical appraisal of methods used in randomized controlled trials of treatments for temporomandibular disorders. J Orofac Pain. 2010;24(2):139–151.
15. Riley P, Glenny AM, Worthington HV, et al. Oral splints for patients with temporomandibular disorders or bruxism: a systematic review and economic evaluation. Health Technol Assess. 2020;24(7):1–224. doi:10.3310/hta24070
16. Berge T, Schjødt B, Bell RF, et al. Assessment of patients with severe temporomandibular disorder in Norway – a multidisciplinary approach. Den Nor Tann Tid. 2016;126:114–121.
17. Zakrzewska JM. Multi-dimensionality of chronic pain of the oral cavity and face. J Headache Pain. 2013;14(1):1–10. doi:10.1186/1129-2377-14-37
18. Ahmed N, Poate T, Nacher-Garcia C, et al. Temporomandibular joint multidisciplinary team clinic. Brit J Oral Maxillofac Surg. 2014;52(9):827–830. doi:10.1016/j.bjoms.2014.07.254
19. Nilsson H, Samuelsson M, Ekdahl S, Halling Y, Oster A, Perseius KI. Experiences by patients and health professionals of a multidisciplinary intervention for long-term orofacial pain. J Multidiscip Healthc. 2013;6:365–371. doi:10.2147/JMDH.S42488
20. Quirk M, Mazor K, Haley HL, et al. How patients perceive a doctor’s caring attitude. Patient Educ Couns. 2008;72(3):359–366. doi:10.1016/j.pec.2008.05.022
21. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1):9–19. doi:10.1016/j.pain.2004.09.012
22. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. doi:10.1016/j.pain.2003.08.001
23. Helsedirektoratet T. Nasjonal faglig retningslinje for utredning og behandling av TMD. (National guidelines in diagnostics and treatment of TMD. Available from: https://www.helsedirektoratet.no/retningslinjer/temporomandibulaer-dysfunksjon-tmd.
24. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
25. Lundeberg T, Lund I, Dahlin L, et al. Reliability and responsiveness of three different pain assessments. J Rehab Med. 2001;33(6):279–283. doi:10.1080/165019701753236473
26. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
27. Jensen MP, Keefe FJ, Lefebvre JC, Romano JM, Turner JA. One- and two-item measures of pain beliefs and coping strategies. Pain. 2003;104(3):453–469. doi:10.1016/S0304-3959(03)00076-9
28. Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;8(2):141–144. doi:10.1097/00007632-198303000-00004
29. Stegenga B, de Bont LG, de Leeuw R, Boering G. Assessment of mandibular function impairment associated with temporomandibular joint osteoarthrosis and internal derangement. J Orofac Pain. 1993;7(2):183–195.
30. Rosén ALB, Berge T. Addressing non-responding chronic TMD patients experiences from a multidisciplinary approach. J Otolaryng Res. 2017;1(2):116.
31. Staniszewski K, Lygre H, Berge T, Rosén A. Serum analysis in patients with temporomandibular disorders: a controlled cross-sectional study in Norway. Pain Res Manag. 2019;2019:1360725. doi:10.1155/2019/1360725
32. Fillingim RB, Slade GD, Greenspan JD, et al. Long-term changes in biopsychosocial characteristics related to temporomandibular disorder: findings from the OPPERA study. Pain. 2018;159(11):2403–2413. doi:10.1097/j.pain.0000000000001348
33. Sanders C, Dougall AL, Haggard R, et al. TMD diagnostic groups affect outcomes independently of treatment in patients at-risk for developing chronicity: a two-year follow-up study. J Oral Facial Pain Headache. 2016;30(3):187–202. doi:10.11607/ofph.1613
34. Dahan H, Shir Y, Velly A, Allison P. Specific and number of comorbidities are associated with increased levels of temporomandibular pain intensity and duration. J Headache Pain. 2015;16(1):1–10. doi:10.1186/s10194-015-0528-2
35. Ness GM, Laskin DM. Global doctor opinion versus a patient questionnaire for the outcome assessment of treated temporomandibular disorder patients. J Oral Maxillofac Surg. 2012;70(7):1531–1533. doi:10.1016/j.joms.2011.11.015
36. Garrigós-Pedrón M, Elizagaray-García I, Domínguez-Gordillo AA, Del-castillo-pardo-de-vera JL, Gil-Martínez A. Temporomandibular disorders: improving outcomes using a multidisciplinary approach. J Multidiscip Healthc. 2019;12:733–747. doi:10.2147/JMDH.S178507
37. Forssell H, Kauko T, Kotiranta U, Suvinen T. Predictors for future clinically significant pain in patients with temporomandibular disorder: a prospective cohort study. Eur J Pain. 2017;21(1):188–197. doi:10.1002/ejp.916
38. Rammelsberg P, LeResche L, Dworkin S, Mancl L. Longitudinal outcome of temporomandibular disorders: a 5-year epidemiologic study of muscle disorders defined by research diagnostic criteria for temporomandibular disorders. J Orofac Pain. 2003;17(1):9–20.
39. Welte-Jzyk C, Pfau DB, Hartmann A, Daubländer M. Somatosensory profiles of patients with chronic myogenic temporomandibular disorders in relation to their painDETECT score. BMC Oral Health. 2018;18(1):18. doi:10.1186/s12903-018-0482-x
40. Gameiro GH, da Silva Andrade A, Nouer DF, Ferraz de Arruda Veiga MC. How may stressful experiences contribute to the development of temporomandibular disorders? Clin Oral Investig. 2006;10(4):261–268. doi:10.1007/s00784-006-0064-1
41. Landmark T, Dale O, Romundstad P, Woodhouse A, Kaasa S, Borchgrevink PC. Development and course of chronic pain over 4 years in the general population: the HUNT pain study. Eur J Pain. 2018;22(9):1606–1616. doi:10.1002/ejp.1243
42. Gerrits MM, Vogelzangs N, van Oppen P, van Marwijk HW, van der Horst H, Penninx BW. Impact of pain on the course of depressive and anxiety disorders. Pain. 2012;153(2):429–436. doi:10.1016/j.pain.2011.11.001
43. Bélanger C, Blais Morin B, Brousseau A, et al. Unpredictable pain timings lead to greater pain when people are highly intolerant of uncertainty. Scand J Pain. 2017;17(1):367–372. doi:10.1016/j.sjpain.2017.09.013
44. Ochsner KN, Ludlow DH, Knierim K, et al. Neural correlates of individual differences in pain-related fear and anxiety. Pain. 2006;120(1–2):69–77. doi:10.1016/j.pain.2005.10.014
45. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
46. Stevans JM, Delitto A, Khoja SS, et al. Risk factors associated with transition from acute to chronic low back pain in US patients seeking primary care. JAMA Netw Open. 2021;4(2):e2037371. doi:10.1001/jamanetworkopen.2020.37371
47. Dutra Dias H, Botelho AL, Bortoloti R, Dos Reis AC. Neuroscience contributes to the understanding of the neurobiology of temporomandibular disorders associated with stress and anxiety. Cranio J Craniomandib Pract. 2021;1–6. doi:10.1080/08869634.2021.1977901
48. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
49. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
50. Dworkin SF, Huggins KH, Wilson L, et al. A randomized clinical trial using research diagnostic criteria for temporomandibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program. J Orofac Pain. 2002;16(1):48–63.
51. Dworkin SF, Turner JA, Wilson L, et al. Brief group cognitive-behavioral intervention for temporomandibular disorders. Pain. 1994;59(2):175–187. doi:10.1016/0304-3959(94)90070-1
52. Lindfors E, Magnusson T, Ernberg M. Effect of therapeutic jaw exercises in the treatment of masticatory myofascial pain: a randomized controlled study. J Oral Facial Pain Headache. 2020;34(4):364–373. doi:10.11607/ofph.2670
53. Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011;377(9784):2226–2235. doi:10.1016/S0140-6736(11)60402-9
54. Turk DC, Fillingim RB, Ohrbach R, Patel KV. Assessment of psychosocial and functional impact of chronic pain. J Pain Offic J Am Pain Soc. 2016;17(9 Suppl):T21–49. doi:10.1016/j.jpain.2016.02.006
55. Borisovskaya A, Chmelik E, Karnik A. Exercise and Chronic Pain. Adv Exp Med Biol. 2020;1228:233–253.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.