Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
High Expression of DNTTIP1 Predicts Poor Prognosis in Clear Cell Renal Cell Carcinoma
Authors Wang X, Li W ![]() , Lou N, Han W, Hai B, Xiao W
, Lou N, Han W, Hai B, Xiao W ![]() , Zhang X
, Zhang X
Received 18 July 2022
Accepted for publication 5 December 2022
Published 6 January 2023 Volume 2023:16 Pages 1—14
DOI https://doi.org/10.2147/PGPM.S382843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Xuegang Wang,1,* Weiquan Li,2,* Ning Lou,3,* Weiwei Han,3 Bo Hai,2 Wen Xiao,2 Xiaoping Zhang2
1Department of Urology, The First Affiliated Hospital, School of Medicine, Xiamen University, Xiamen, Fujian, People’s Republic of China; 2Department of Urology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 3Department of Urology, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Xiao; Bo, Hai, Department of Urology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1277 Jiefang Avenue, Wuhan, Hubei Province, 430022, People’s Republic of China, Tel +86-17088353610, Fax +86 85776343, Email [email protected]; [email protected]
Background: Invasion and metastasis led to poor prognosis and death of clear cell renal cell carcinoma (ccRCC) patients. The deoxynucleotidyl transferase terminal interacting protein 1 (DNTTIP1) was reported to promote multiple tumor progression. However, there is no research about DNTTIP1 in ccRCC.
Methods: Kaplan–Meier survival analysis, multivariate analysis demonstrated the prognostic indicator in overall survival (OS) and disease-free survival (DFS) of ccRCC with DNTTIP1 expression in the Cancer Genome Atlas Kidney Clear Cell Carcinoma (TCGA-KIRC). Receiver operator characteristic (ROC) curve analyzed diagnostic ability of DNTTIP1 in TCGA-KIRC and validation dataset. The quantitative real-time polymerase chain reaction (qRT-PCR) detected the DNTTIP1 expression in renal cancer tissues, and the Office of Cancer Clinical Proteomics Research (CPTAC) verified the protein expression of DNTTIP1. Moreover, nomogram predicted the role of DNTTIP1 in ccRCC patient. Single-sample Gene Set Enrichment Analysis (SsGSEA) and GSEA evaluated the pathogenesis role of DNTTIP1 in TCGA-KIRC.
Results: DNTTIP1 expression was higher in ccRCC tumor tissues. High expression of DNTTIP1 was associated with poor OS (HR = 1.618, P < 0.0001), and poor DFS (HR = 1.789, P < 0.0001). SsGSEA and GSEA showed DNTTIP1 was associated with hypoxia, epithelial-mesenchymal transition (EMT), angiogenesis, G2M checkpoint. DNTTIP1 had a positive correlation with EMT biomarkers in ccRCC, and might be an effective target for ccRCC.
Conclusion: This study provided that higher expression of DNTTIP1 predicted poor prognosis in ccRCC, and DNTTIP1 might be a novel detection biomarker and therapeutic target of tumor malignant in the future.
Keywords: DNTTIP1, ccRCC, gene therapy, prognostic indicator
Background
Renal cell cancer (RCC) was estimated about 79,000 new cases and 13,920 new deaths in 2022 in the United States,1 but estimated about 77,410 new cancer cases and 46,345 new deaths in 2022 in China.2 Histopathologic classifications identified three major subtypes: clear cell RCC (ccRCC; 70–75%), papillary RCC (pRCC; 10–16%), and chromophobe RCC (chRCC; 5%).3 pRCC occurs sporadically, with several agents including mTOR inhibitors could be used in the treatment of advanced and metastatic pRCC.4 ChRCCs originated from the intercalated cell of distal tubules, tumor protein P53 and phosphatase and tensin homolog deleted on chromosome ten (PTEN) were the two main frequently mutated genes.5 CcRCC was the main pathological types, and associated with von Hippel-Lindau (VHL) disease. Loss of function of the VHL tumor suppressor protein (pVHL).6 pVHL catalyzed the ubiquitination of hypoxia inducible factor (HIF), the degradation of HIFs was inhibited in renal cell carcinoma,7,8 then increases angiogenesis and tumor metabolism.9,10 It is of great significance to clarify the potential diagnostic markers and molecular roles in the occurrence and development of ccRCC.
Tumor recurrence is still one of the high risks affecting the survival of tumor patients after surgery.11 Epithelial-mesenchymal transition (EMT), is a characteristic of malignant tumor.12–14 Inhibition of tumor EMT can slow down tumor metastasis.15,16 Target of tyrosine kinase inhibitor (TKI) drugs had been discovered for treatment of metastatic ccRCC patients,17,18 but it still leads to poor progression and recurrence when incomplete reversal of tumor hypoxia and EMT in ccRCC.19,20 Urgent need to explore new biomarkers or drug targets for ccRCC.
The deoxynucleotidyl transferase terminal interacting protein (DNTTIP) plays multiple roles in gene transcription and cell proliferation. DNTTIP1 is a prognostic biomarker in hepatocellular carcinoma and correlated with immune infiltration.21 DNTTIP1 activated extracellular regulated protein kinases (ERK) signaling by recruiting histone deacetylase 1 (HDAC1) to facilitate nasopharyngeal carcinoma metastasis.22 DNTTIP2 is associated with malignant characteristics and macrophage infiltration in glioma.23 However, the role of DNTTIPs in ccRCC is unclear.
In this study, we investigated the role of DNTTIPs in ccRCC with patient survival in the Cancer Genome Atlas (TCGA) database, and the expression of DNTTIP1 in the Office of Cancer Clinical Proteomics Research (CPTAC), and clinical samples. Single-sample Gene Set Enrichment Analysis (ssGSEA) and GSEA evaluated the biological role of DNTTIP1 in ccRCC. Our study demonstrated that DNTTIP1 has a significant marker role for ccRCC.
Patients and Methods
Patient Samples from Public Database and Validation Dataset
Public database from TCGA-KIRC database contains a total of 533 patients with clinical information.24 Eighteen matched ccRCC tumor tissues and normal tissues were from the Department of Urology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology between 2020 and 2022. They were obtained from radical nephrectomy as the stage of cancer or endophytic location, and partial nephrectomy. The information of age stage, grade, tumor size (T stage) is shown in Supplementary Table 1. The patients/participants provided their written informed consent to participate in this study. The experimental and research procedures were approved by the institutional review committee of Huazhong University of Science and Technology (2017-S346).
RNA Extraction, RNA Reverse Transcription and qRT-PCR
TRizol reagent (Thermo, Massachusetts, USA), strand cDNA Synthesis (Vazyme, Nanjing, China.) and qPCR SYBR® Green Master Mix (Vazyme, Nanjing, China.) were used for RNA extraction, RNA reverse transcription, and qRT-PCR of tumor tissues.15 DNTTIP1 expression was calculated by: 2−ΔCt (ΔCt = Ct DNTTIP1–CtGAPDH).
DNTTIP1, (forward, 5′- GGGCAGCTGGTTCTTAC −3′,
reverse, 5′- GATCCATGGAGATGGCAGGA −3′)
GAPDH (forward, 5’-GAGTCAACGGATTTGGTCGT-3’;
reverse, 5’-GACAAGCTTCCCGTTCTCAG-3’).
Bioinformatics Analysis
Receiver operator characteristic (ROC) curve and area under the curve (AUC) were used to assess clinical diagnostic ability. The Kaplan–Meier (KM) curve, univariate and multivariate Cox proportional hazard regression evaluated survival rate of DNTTIP1 for ccRCC patients as previously described.25
Nomogram Analysis
Nomogram analysis with different parameters (DNTTIP1 expression, N stage, T stage, M stage) had been used for prognosis prediction.13 The c-index and probability of 1-, 3-, 5-year survival were calculated with R software.
Single-Sample Gene Set Enrichment Analysis
Ss-GSEA and GSEA were used to evaluate the possible pathogenesis of DNTTIP1 (http://www.broadinstitute.org/gsea). p < 0.05 and false discovery rate (FDR) of <25% were considered to have statistically significant difference as previously described.21,26
Statistical Analysis
RNA result was described with median and standard error of the mean (SEM). The paired samples were analyzed with paired sample t-test. The unpaired samples were analyzed with t-test.27 Data analyses were performed with SPSS Statistics 22.0 and p < 0.05 as previously described.28
Results
DNTTIP1 Was Highly Expressed in ccRCC
Firstly, we analyzed the expression of a tumor to determine the role of DNTTIP1 in ccRCC with t-test or paired sample t-test. The mRNA expression levels of the DNTTIP1 and DNTTIP2 were investigated in TCGA-KIRC database with heat map. The result is shown in Figure 1A. The expression of DNTTIP1 (N = 72, T = 72) was higher in paired ccRCC tissues (p < 0.0001, Figure 1B and D), but not DNTTIP1. Expression of DNTTIP1 was higher in total ccRCC tissues and corresponding normal tissues (N = 72, T = 533) (p < 0.0001, Figure 1C and D), but not DNTTIP1. QRT-PCR showed the mRNA expression of DNTTIP1 was higher in ccRCC cancer tissue (p < 0.001, Figure 1E). The protein expression of DNTTIP1 in ccRCC tumor tissues was significantly higher with CPTAC database (p < 0.001, Figure 1F).
 |
Figure 1 DNTTIP1 was highly expressed in ccRCC. (A) Heat map of DNTTIPs expression in TCGA-KIRC (n=605). (B) and (C) Relative DNTTIPs expression in TCGA-KIRC. (D) and (E) DNTTIP1 was highly expressed in TCGA-KIRC and clinical samples. (F) DNTTIP1 protein level was highly expressed in CPTAC data. Red indicates high expression; black indicates medium expression; green indicates low expression. CPTAC: Office of Cancer Clinical Proteomics Research. *P < 0.05, ***P < 0.001, and ****P < 0.0001. Abbreviations: DNTTIP, the deoxynucleotidyl transferase terminal interacting protein; TCGA-KIRC, The Cancer Genome Atlas kidney renal clear cell carcinoma. |
Clinical Characteristics of the Patients
The total patients were divided by DNTTIP1 median expression levels into two group respectively. DNTTIP1 had a significant association between high mRNA expression and sex, tumor stage (T stage), lymphatic metastasis (N stage), grade, distant metastasis (M stage), TNM stages, but not age with t-test. DNTTIP1 expression was significantly higher in dead patients (p < 0.0001, Figure 2A), recurred patients (p < 0.0001, Figure 2B), M1 patients (p < 0.0001, Figure 2C), N1 patients (p < 0.01, Figure 2D), female (p < 0.05, Figure 2E), older patients (NS, Figure 2F), T3+T4 patients (p < 0.0001, Figure 2G), G3+G4 patients (p < 0.0001, Figure 2H), and higher TNM patients (p < 0.0001, Figure 2I).
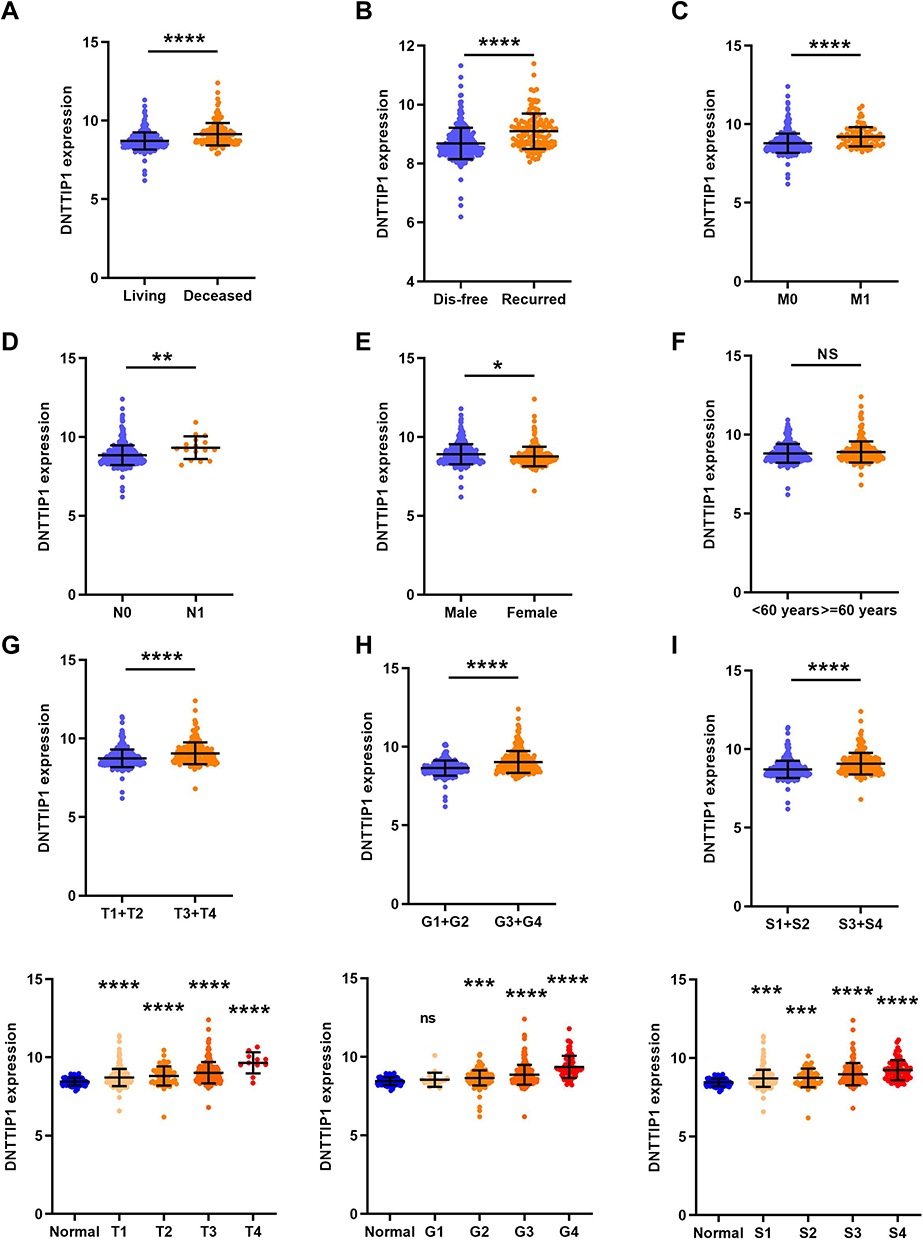 |
Figure 2 Clinical and molecular characteristics of the patients. (A) overall survival status, (B) disease free status, (C) M stage, (D) N stage, (E) sex, (F) age, (G) T stage, (H) grade, and (I) TNM stage. *P < 0.05, **P < 0.01, ***P < 0.001 and ****P < 0.0001. Abbreviation: DNTTIP, the deoxynucleotidyl transferase terminal interacting protein. |
The Association and Diagnostic Capability of DNTTIP1 in ccRCC
ROC curve and AUC were used to distinguish the diagnostic role of a biomarker in diseases. Then we investigated the diagnostic capability of DNTTIP1 in ccRCC. The results showed AUC of 0.7276 (95% CI: 0.6768–0.7784; p < 0.0001, Figure 3A) and 0.6887 (95% CI: 0.6022–0.7751; p < 0.0001, Figure 3B) with total patients and pair-para patient. Similar results were found in collected clinical samples in Figure 3C. High expression of DNTTIP1 had a diagnostic capability for ccRCC patients with living vs deceased (AUC = 0.7005, p < 0.0001, Figure 3D), recurred vs disease free (AUC = 7154, p < 0.0001, Figure 3E), (T3 + T4)/(T1 + T2) (AUC = 0.6530, p < 0.0001, Figure 3F), N1/N0 stage (AUC = 0.7064, p = 0.0049, Figure 3G), M1/M0 stage (AUC = 0.7114, p < 0.0001, Figure 3H), pathological stage (III + IV)/(I + II) (AUC = 0.6776, p < 0.0001, Figure 3I), grade (III + IV)/(I + II) (AUC = 0.6594, p < 0.0001, Figure 3J).
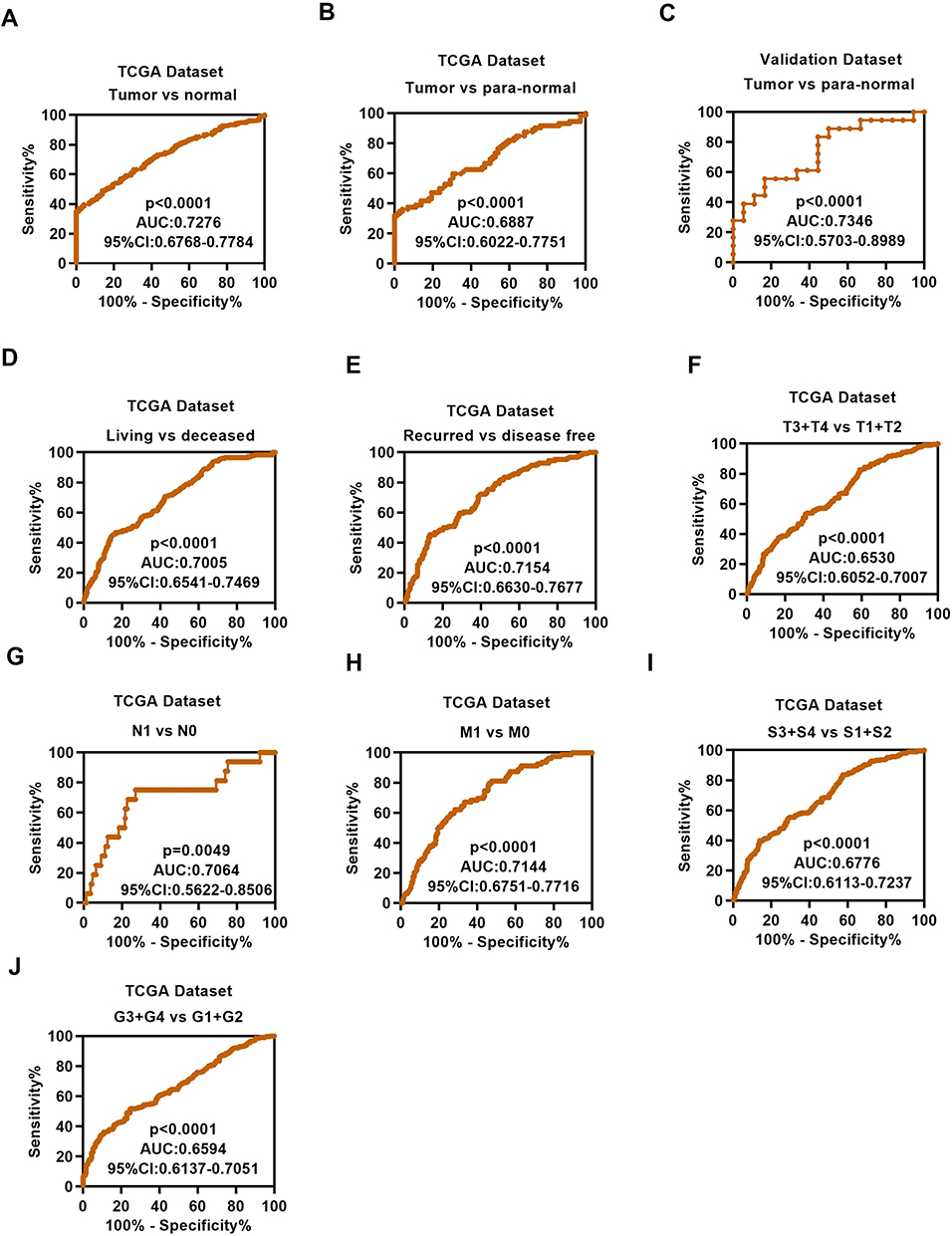 |
Figure 3 The diagnostic value of DNTTIP1 in ccRCC. (A) ROC curve of DNTTIP1 between tumor and non-cancerous normal tissues, the AUC: 0.7276 (p < 0.0001); (B) ROC curve of DNTTIP1 between tumor and paired non-cancerous normal tissues, the AUC: 0.6887 (p < 0.0001). (C) ROC curve of DNTTIP1 between tumor and non-cancerous normal tissues in clinical samples, the AUC: 0.7346 (p < 0.0001). (D–J) Subgroup ROC curve analysis implied that the high expression of DNTTIP1 might have diagnostic value for ccRCC patients with living vs deceased, recurred vs disease free, (T3 + T4) / (T1 + T2), N1 / N0 stage, M1 / M0 stage pathological stage, grade (III + IV)/ (I + II). Abbreviations: DNTTIP, the deoxynucleotidyl transferase terminal interacting protein; AUC, Area under the curve; ROC receiver operator characteristic. |
Prognostic Significance of DNTTIP1 in ccRCC
Kaplan – Meier curve was used to compare the survival time of two groups with Log Rank test. We defined high risk and low risk with high and low expression groups of DNTTIP1 (Figures 4A and 5A). Patient survival and recurrence data are shown in Figures 4B and 5B. Z-score is shown in Figures 4C and 5C. High DNTTIP1 expression had shorter OS (p < 0.0001, Figure 4D) and shorter DFS (p < 0.0001, Figure 5D). DNTTIP1 had a certain diagnostic capability with 1-, 3-, and 5-years’ OS (Figure 4E) and DFS (Figure 5E) in ccRCC.
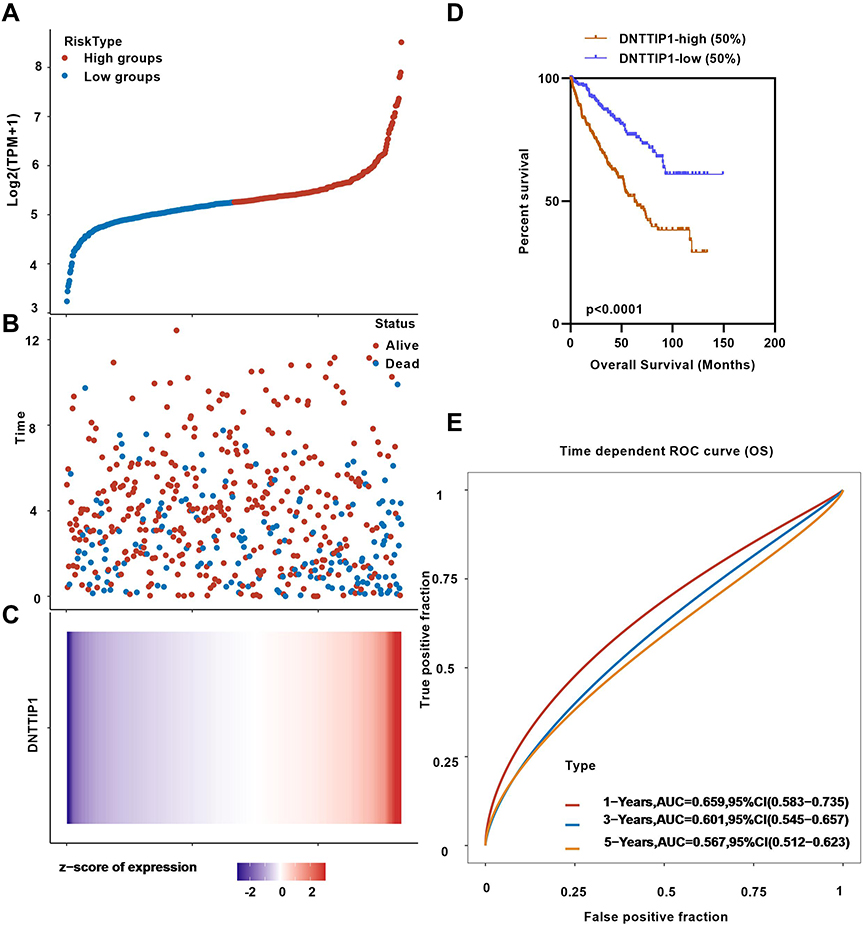 |
Figure 4 Kaplan–Meier curves of OS in different expression levels of DNTTIP1. (A) High risk and low risk by the median expression levels of DNTTIP1. (B) living or deceased patient distributed in ccRCC. (C) Z-score of total patients in ccRCC. (D) Higher DNTTIP1 expressers had shorter OS than the lower expressers. (E) DNTTIP1 had diagnostic capabilities in KIRC with 1-, 3-, and 5-years’ OS. Abbreviations: OS, overall survival; DNTTIP, the deoxynucleotidyl transferase terminal interacting protein. |
 |
Figure 5 Kaplan–Meier curves of DFS in different expression levels of DNTTIP1. (A) High risk and low risk by the median expression levels of DNTTIP1. (B) recurred or disease-free patient distributed in ccRCC. (C) Z-score of total patients in ccRCC. (D) Higher DNTTIP1 expressers had shorter DFS than the lower expressers. (E) DNTTIP1 had diagnostic capabilities in KIRC with 1-, 3-, and 5-years’ DFS. Abbreviations: DFS, disease-free survival; DNTTIP, the deoxynucleotidyl transferase terminal interacting protein. |
Univariate and Multivariate Analyses of OS and DFS
Univariate and multivariate analysis were used to evaluate the prognostic ability of DNTTIP1. The results showed that DNTTIP1 had a capacity of independent prognosis in ccRCC. The results of OS were shown as follows (Table 1 and Table 2): age (HR, 1.615; p = 0.003), T stage (HR, 1.653; p = 0.006), N stage (HR, 2.209; p = 0.03), M stage (HR, 2.495; p < 0.0001), Grade (HR, 1.608; p = 0.011), DNTTIP1 expression (HR, 1.618; p = 0.006), DFS: T stage (HR, 2.029; p = 0.001), N stage (HR, 3.313; p = 0.002), M stage (HR, 4.478; p < 0.0001), Grade (HR, 2.222; p < 0.0001), DNTTIP1 expression (HR, 1.789; p = 0.007).
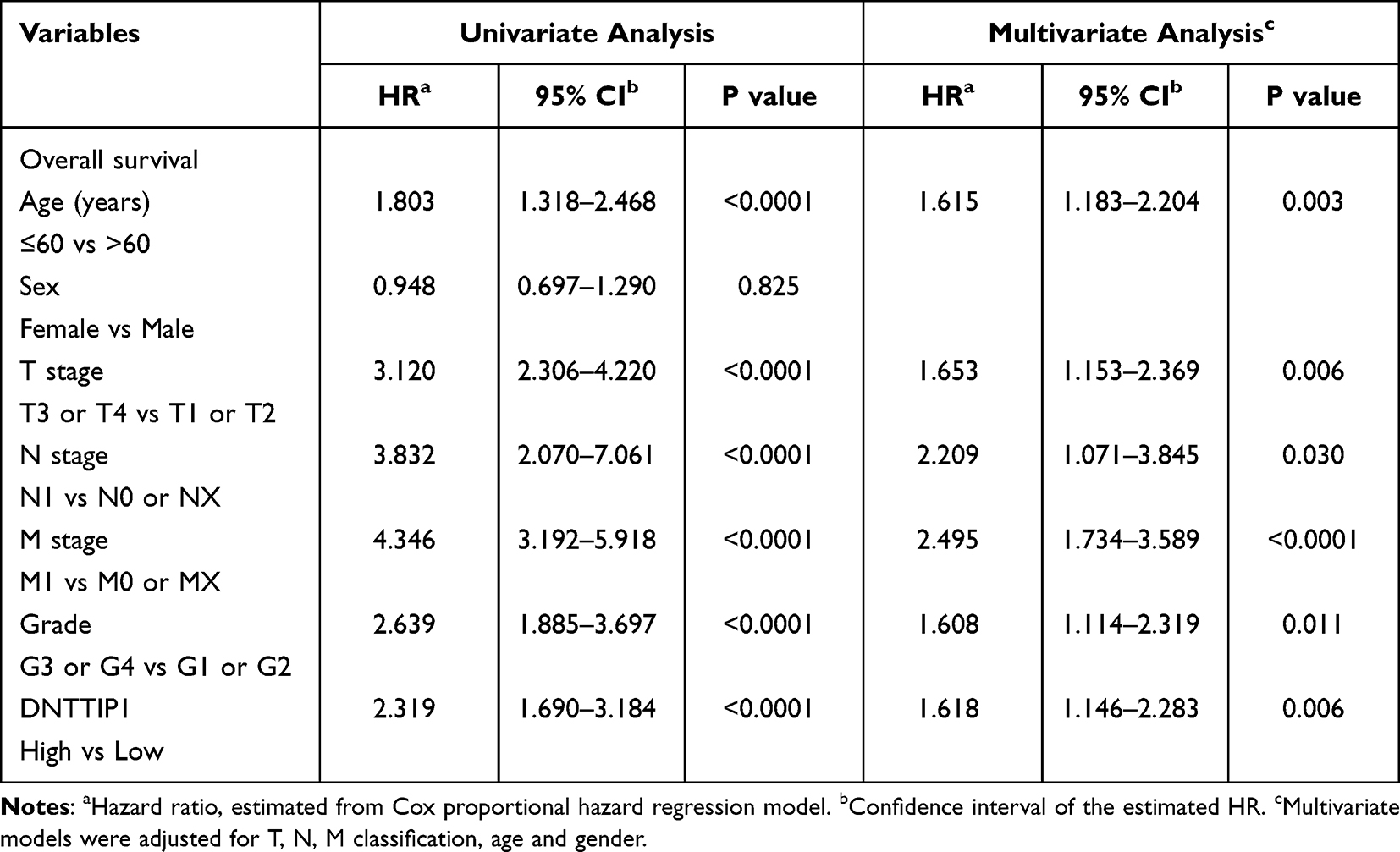 |
Table 1 Univariate and Multivariate Analyses of DNTTIP1 mRNA Level and Patient Overall Survival |
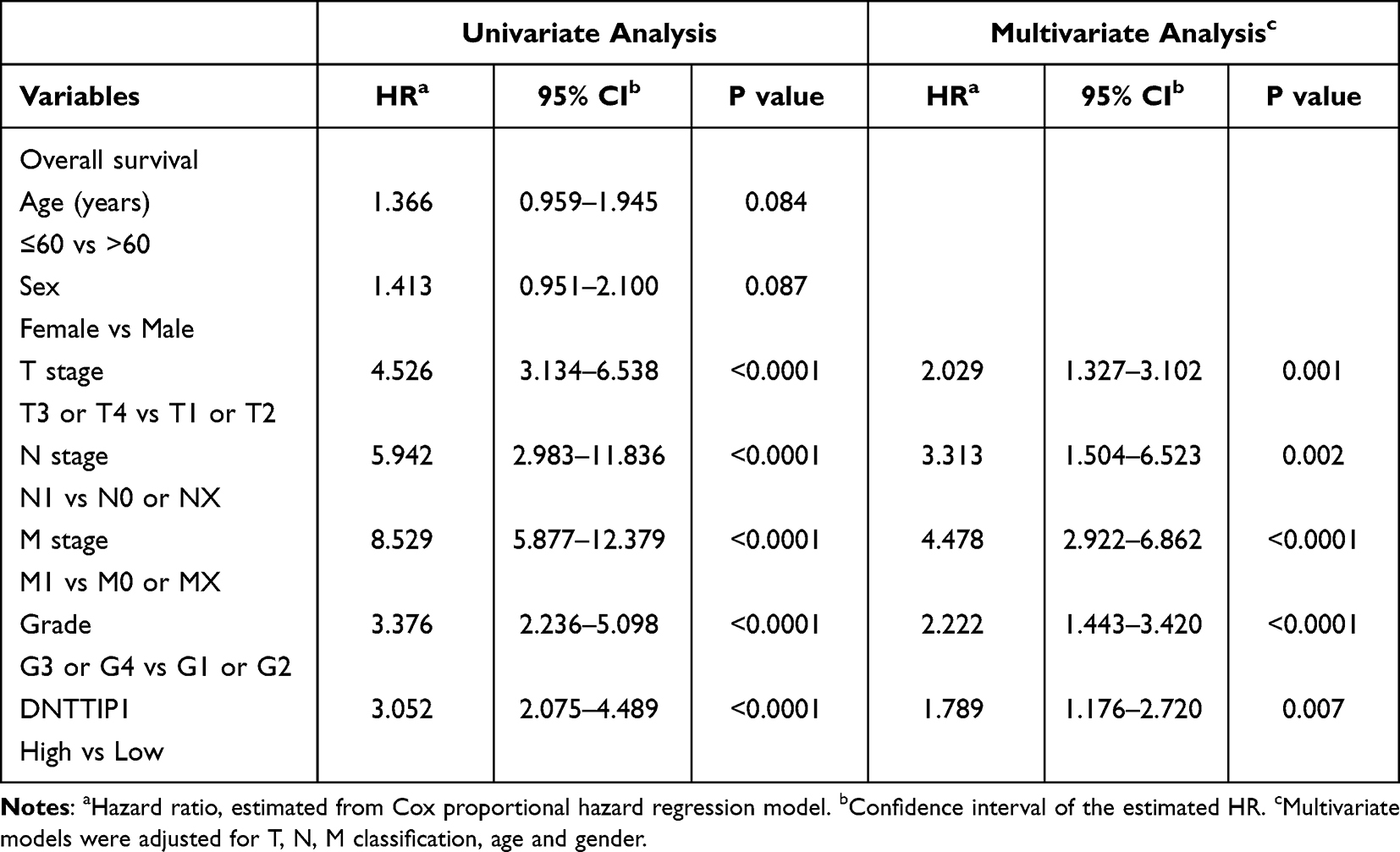 |
Table 2 Univariate and Multivariate Analyses of DNTTIP1 mRNA Level and Patient Disease-Free Survival |
Nomogram Models of DNTTIP1 in ccRCC
Nomogram models had been used as one of the most common prognostic models. We constructed nomogram of OS in ccRCC patients (Figure 6A). 1-year, 3-year, and 5-year calibration curves of OS are shown in Figure 6B–6D. The value of the c-index was 0.766, meaning that the result was relatively accurate and credible when it was larger than 0.71.
 |
Figure 6 Nomogram models of DNTTIP1 in ccRCC. (A) Nomogram of OS in ccRCC patients. (B–D) Calibration curves of 1-year, 3-year, and 5-year OS. Red line: actual calculation result; Grey line: the result of prediction. The fitting degree of red line and gray line indicates the success rate of the prediction model. Abbreviations: OS, overall survival; DNTTIP, the deoxynucleotidyl transferase terminal interacting protein. |
Functional Prediction of DNTTIP1 in ccRCC
Ss-GSEA and GSEA can be used to discover which gene sets with specific biological significance are significantly associated with two groups of samples from the expression. Ss-GSEA was used to explore the function of DNTTIP1 in ccRCC. DNTTIP1 had a positive correlation with hypoxia (p < 0.0001, Figure 7A), EMT (p < 0.0001, Figure 7B), extracellular matrix (ECM)-related gene (p < 0.0001, Figure 7C), DNA repair (p < 0.0001, Figure 7D), p53 pathway (p < 0.0001, Figure 7E), tumor growth signature (p < 0.0001, Figure 7F), G2M checkpoint (p < 0.0001, Figure 7G), DNA replication (p < 0.0001, Figure 7H), angiogenesis (p < 0.0001, Figure 7I). GSEA showed that DNTTIP1 was associated with EMT (p < 0.0001, Figure 8A), angiogenesis (p = 0.014, Figure 8B), G2M checkpoint (p = 0.002, Figure 8C), hypoxia (p = 0.025, Figure 8D), Kirsten rat sarcoma viral oncogene (KRAS) (p < 0.0001, Figure 8E). DNTTIP1 expression was positive correlation with oncogene of snail1 (p = 0.0002, Figure 8F), twist1 (p < 0.0001, Figure 8G), vim (p < 0.0001, Figure 8H), MKI67 (p < 0.0001, Figure 8I), matrix metalloproteinases2 (MMP2) (p < 0.0001, Figure 8J), but had a negative correlation with cdh1 (E-cadherin) (p < 0.0001, Figure 8K).
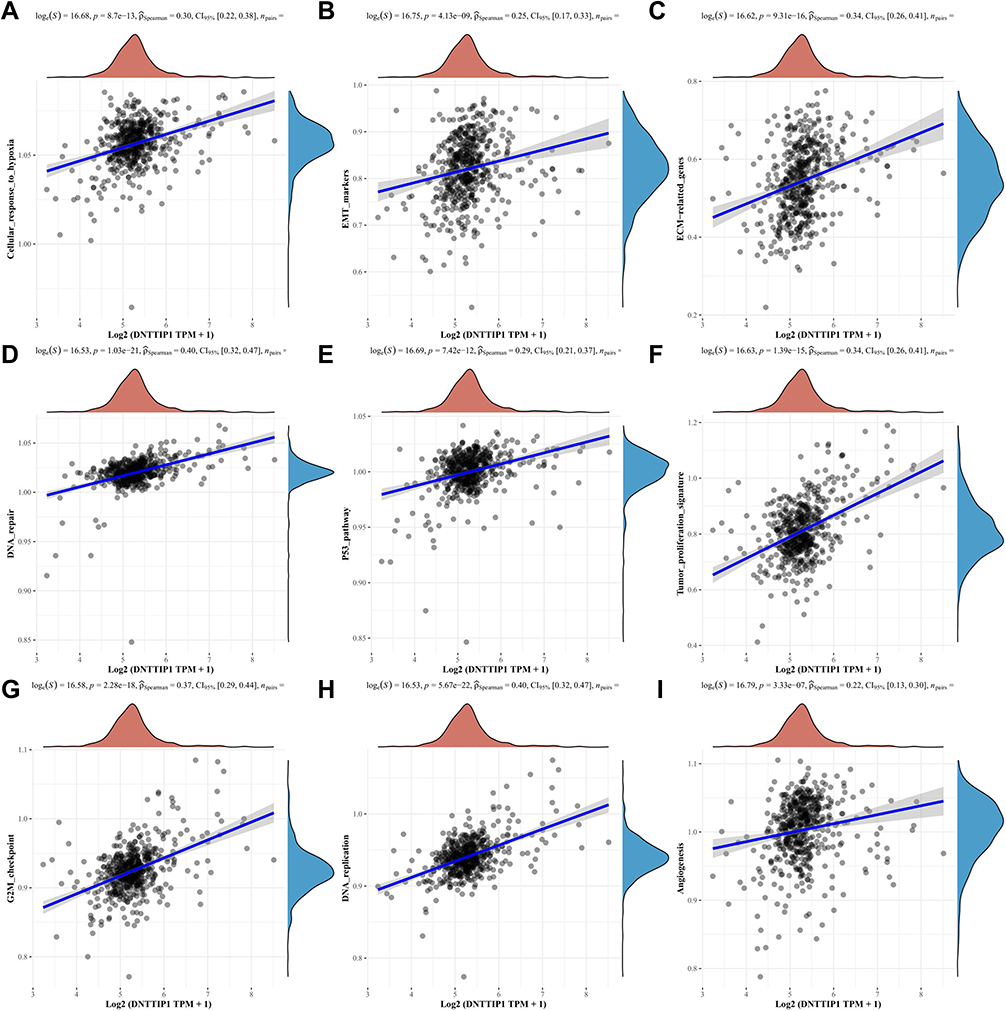 |
Figure 7 Pathway of DNTTIP1 in TCGA-KIRC with SsGSEA. (A) Cellular response to hypoxia; (B) EMT (C) ECM-related gene; (D) DNA repair; (E) p53 pathway; (F) Tumor growth signature; (G) G2M checkpoint; (H) DNA replication; (I) Angiogenesis. Round indicators represent the pathway scores of high and low DNTTIP1 groups. |
 |
Figure 8 GSEA and tumor malignancy characteristic genes correlation analysis of DNTTIP1 in TCGA-KIRC. (A) EMT; (B) Angiogenesis; (C) G2M checkpoint; (D) Hypoxia; (E) KRAS; (F–K) Tumor malignancy characteristic genes correlation analysis of DNTTIP1 with snal1, twist1, vim, MKI67, MMP2, cdh1 (E-cadherin). Abbreviations: EMT, Epithelial-mesenchymal transition; KRAS, Kirsten rat sarcoma viral oncogene. |
Discussion
Our study reported the expression of DNTTIPs and the prognostic role of DNTTIP1 in ccRCC for the first time. Previous research results confirmed that DNTTIP1 can interact with HDAC1/2 when acted as a scaffold with its amino-terminal region.29 The expression of DNTTIP1 was significantly up-regulated in oral cancer, and correlated with tumor growth.30 DNTTIP1 was a prognostic biomarker in hepatocellular carcinoma.21 Bioinformatics analysis shows that DNTTIP1 can predict patient survival in acute myeloid leukemia.31 Mechanically, DNTTIP1 could activate ERK signaling in metastasis of nasopharyngeal carcinoma.22 ERK signaling activation or KRAS mutation mediated TKI resistance in various tumors.32–36 DNTTIP2 was associated with malignant characteristics in glioma.15
Here, we explored the expression of DNTTIPs in ccRCC. DNTTIP1 was significantly escalated, but not DNTTIP2 in ccRCC. DNTTIP1 was positively correlated with disease progression and could be an independent predictor for ccRCC. High DNTTIP1 expression was related to poor OS and DFS with Kaplan–Meier survival curves, univariate and multivariate Cox proportional hazard regression, and nomogram analysis.
Ss-GSEA and Spearman correlation were employed to reveal the link between DNTTIP1 expression and tumor signaling pathways in ccRCC. Our results revealed that DNTTIP1 expression was significantly positively correlated with cellular response to hypoxia, EMT, ECM-related gene, DNA repair, p53 pathway, tumor growth signature, G2M checkpoint, DNA replication, angiogenesis. GSEA showed that DNTTIP1 was associated with EMT, angiogenesis, G2M checkpoint, hypoxia, KRAS. Hypoxia induced tumor-associated macrophages were related to poor prognosis of ccRCC.8 HIF degradation was inhibited and then promoted angiogenesis, increased tumor growth or metastasis in kidney cancer.9 HIF2α is believed to be the most important driver for the development of the ccRCC.27 HIF1α and HIF2α could induce angiogenesis37,38 and lipid accumulation in renal cancer tissues.27,39 DNTTIP1 was predicted to play a certain role in cellular response to hypoxia and angiogenesis. It indicated that DNTTIP1 may have an effect on the metabolism or malignant characteristics of renal cancers.
EMT was one of malignant characteristic and a key foundation of cancer progression.12,13,40 Twist1 signaling boosted tumor progression and promoted metastasis in ccRCC.41 G2M checkpoint had a significant effect on cell proliferation, especially tumors.42–44 Stabilizing Snail1 could regulate metastasis and chemoresistance of triple-negative breast cancer by.45 MKI67 and MMPs could promote the progress of tumor, were the potential biomarker for clinical examination of malignant characteristics in tumors.46–48
Here, we show that DNTTIP1 was associated with EMT in Ss-GSEA and GSEA. DNTTIP1 expression had a positive correlation with oncogene of snail1, twist1, vim, MKI67, and MMP2, but had a negative correlation with E-cadherin (E-cad). Homologous recombination DNA repair was one aspect of chemotherapy resistance.49 P53 was a tumor suppressor and mutated in more than 50% of cancers, transactivating p53 pathway could induce apoptosis and cell-cycle arrest.50 DNTTIP1 expression was significantly positively correlated with DNA repair, p53 pathway, tumor growth signature, G2M checkpoint, DNA replication, indicating that DNTTIP1 was related to cell cycle and cell repair.
However, the mechanism of pathway and DNTTIP1 was not investigated in the current research. However, it is worth for our further study as DNTTIP1 is one of the prognostic biomarkers in ccRCC. The increased expression of DNTTIP1 may be a potential biomarker of renal cell carcinoma and a therapeutic target of renal cell carcinoma. Direction on DNTTIP1, hypoxia and tumor metabolism may be the future research topics.
Conclusion
Our studies indicated that high DNTTIP1 was significantly correlated with disease progression and identified DNTTIP1 as an independent predictor for ccRCC with univariate and multivariate Cox proportional hazard regression, and Nomogram. DNTTIP1 had a positive correlation with malignant features of tumor. The results of all these studies suggest a potential role for DNTTIP1 in ccRCC, and downregulation of DNTTIP1 may provide a new therapeutic strategy for ccRCC patients.
Declaration of Helsinki
The written informed consent provided by the patient to participate in this study is consistent with the Helsinki Declaration.
Acknowledgments
This work was supported by grants from Fujian Provincial Department of Science and Technology (2020J011222), and Xiamen medical and health guidance project (3502Z20199123).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. doi:10.3322/caac.21708
2. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
3. Schodel J, Grampp S, Maher ER, et al. Hypoxia, hypoxia-inducible transcription factors, and renal cancer. Eur Urol. 2016;69:646–657. doi:10.1016/j.eururo.2015.08.007
4. Feng D, Zhang F, Liu L, et al. SKA3 serves as a biomarker for poor prognosis in kidney renal papillary cell carcinoma. Int J Gen Med. 2021;14:8591–8602. doi:10.2147/IJGM.S336799
5. Alaghehbandan R, Przybycin CG, Verkarre V, et al. Chromophobe renal cell carcinoma: novel molecular insights and clinicopathologic updates. Asian J Urol. 2022;9:1–11. doi:10.1016/j.ajur.2021.11.010
6. Hsieh JJ, Purdue MP, Signoretti S, et al. Renal cell carcinoma. Nat Rev Dis Primers. 2017;3:17009. doi:10.1038/nrdp.2017.9
7. Chappell JC, Payne LB, Rathmell WK. Hypoxia, angiogenesis, and metabolism in the hereditary kidney cancers. J Clin Invest. 2019;129:442–451. doi:10.1172/JCI120855
8. Gu W, Gong L, Wu X, et al. Hypoxic TAM-derived exosomal miR-155-5p promotes RCC progression through HuR-dependent IGF1R/AKT/PI3K pathway. Cell Death Discov. 2021;7:147. doi:10.1038/s41420-021-00525-w
9. Cuvillier O. The therapeutic potential of HIF-2 antagonism in renal cell carcinoma. Transl Androl Urol. 2017;6:131–133. doi:10.21037/tau.2017.01.12
10. Lainakis G, Bamias A. Targeting angiogenesis in renal cell carcinoma. Curr Cancer Drug Targets. 2008;8:349–358. doi:10.2174/156800908785133132
11. Ravaud A, Motzer RJ, Pandha HS, et al. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N Engl J Med. 2016;375:2246–2254. doi:10.1056/NEJMoa1611406
12. Chen B, Zhang G, Lai J, et al. Genetic and immune characteristics of sentinel lymph node metastases and multiple lymph node metastases compared to their matched primary breast tumours. EBioMedicine. 2021;71:103542. doi:10.1016/j.ebiom.2021.103542
13. Li Z, Wang Q, Peng S, et al. The metastatic promoter DEPDC1B induces epithelial-mesenchymal transition and promotes prostate cancer cell proliferation via Rac1-PAK1 signaling. Clin Transl Med. 2020;10:e191. doi:10.1002/ctm2.191
14. Wang H, Wang M, Wen Y, et al. Biphasic regulation of mesenchymal genes controls fate switches during hematopoietic differentiation of human pluripotent stem cells. Adv Sci. 2020;7:2001019. doi:10.1002/advs.202001019
15. Lv Q, Xiao W, Xiong Z, et al. Identification of candidate biomarker EMP3 and its prognostic potential in clear cell renal cell carcinoma. Front Biosci. 2021;26:1176–1190.
16. Shen S, Wang JW, Zheng BH, et al. The lnc-CITED2-2:1 inhibits metastasis via inhibiting CITED2 and epithelial-mesenchymal transition in gallbladder cancer. Clin Transl Med;2020. e116. doi:10.1002/ctm2.116
17. Chen W, Hill H, Christie A, et al. Targeting renal cell carcinoma with a HIF-2 antagonist. Nature. 2016;539(7627):112–117. doi:10.1038/nature19796
18. Cancer Genome Atlas Research N. Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature. 2013;499:43–49. doi:10.1038/nature12222
19. Bergers G, Hanahan D. Modes of resistance to anti-angiogenic therapy. Nat Rev Cancer. 2008;8:592–603. doi:10.1038/nrc2442
20. Nallandhighal S, Vince R, Karim R, et al. Molecular characterization of clear cell renal cell carcinoma reveals prognostic significance of epithelial-mesenchymal transition gene expression signature. Eur Urol Oncol. 2022;5:92–99. doi:10.1016/j.euo.2021.10.007
21. Zhu C, Tong R, Jiang X, et al. DNTTIP1 is a prognostic biomarker correlated with immune infiltrates in hepatocellular carcinoma: a study based on the cancer genome atlas data. Front Genet. 2021;12:767834. doi:10.3389/fgene.2021.767834
22. Ding S, Gao Y, Lv D, et al. DNTTIP1 promotes nasopharyngeal carcinoma metastasis via recruiting HDAC1 to DUSP2 promoter and activating ERK signaling pathway. EBioMedicine. 2022;81:104100. doi:10.1016/j.ebiom.2022.104100
23. Liu YJ, Zeng SH, Qian WH, et al. DNTTIP2 expression is associated with macrophage infiltration and malignant characteristics in low-grade glioma. Pharmgenomics Pers Med. 2022;15:261–275. doi:10.2147/PGPM.S356326
24. Goldman M, Craft B, Swatloski T, et al. The UCSC cancer genomics browser: update 2015. Nucleic Acids Res. 2015;43:D812–7. doi:10.1093/nar/gku1073
25. Xiao W, Chen K, Liang HG, et al. Identification of KIF20A as a tumor biomarker and forwarder of clear cell renal cell carcinoma. Chin Med J. 2021;134:2137–2139. doi:10.1097/CM9.0000000000001331
26. Meng X, Yuan H, Li W, et al. Solute carrier family 16 member 5 downregulation and its methylation might serve as a prognostic indicator of prostate cancer. IUBMB Life. 2021;73:1363–1377. doi:10.1002/iub.2560
27. Xiong Z, Xiong W, Xiao W, et al. NNT-induced tumor cell “slimming” reverses the pro-carcinogenesis effect of HIF2a in tumors. Clin Transl Med. 2021;11:e264. doi:10.1002/ctm2.264
28. Li W, Meng X, Yuan H, et al. M2-polarization-related CNTNAP1 gene might be a novel immunotherapeutic target and biomarker for clear cell renal cell carcinoma. IUBMB Life. 2022;74:391–407. doi:10.1002/iub.2596
29. Itoh T, Fairall L, Muskett FW, et al. Structural and functional characterization of a cell cycle associated HDAC1/2 complex reveals the structural basis for complex assembly and nucleosome targeting. Nucleic Acids Res. 2015;43:2033–2044. doi:10.1093/nar/gkv068
30. Sawai Y, Kasamatsu A, Nakashima D, et al. Critical role of deoxynucleotidyl transferase terminal interacting protein 1 in oral cancer. Lab Invest. 2018;98:980–988. doi:10.1038/s41374-018-0070-3
31. Zhuang H, Chen Y, Sheng X, et al. Searching for a signature involving 10 genes to predict the survival of patients with acute myelocytic leukemia through a combined multi-omics analysis. PeerJ. 2020;8:e9437. doi:10.7717/peerj.9437
32. Fenouille N, Puissant A, Dufies M, et al. Persistent activation of the Fyn/ERK kinase signaling axis mediates imatinib resistance in chronic myelogenous leukemia cells through upregulation of intracellular SPARC. Cancer Res. 2010;70:9659–9670. doi:10.1158/0008-5472.CAN-10-2034
33. Chorzalska A, Ahsan N, Rao RSP, et al. Overexpression of Tpl2 is linked to imatinib resistance and activation of MEK-ERK and NF-kappaB pathways in a model of chronic myeloid leukemia. Mol Oncol. 2018;12:630–647. doi:10.1002/1878-0261.12186
34. Wu DW, Wang YC, Wang L, et al. A low microRNA-630 expression confers resistance to tyrosine kinase inhibitors in EGFR-mutated lung adenocarcinomas via miR-630/YAP1/ERK feedback loop. Theranostics. 2018;8:1256–1269. doi:10.7150/thno.22048
35. Zhang P, Xing Z, Li X, et al. Tyrosine receptor kinase B silencing inhibits anoikisresistance and improves anticancer efficiency of sorafenib in human renal cancer cells. Int J Oncol. 2016;48:1417–1425. doi:10.3892/ijo.2016.3356
36. Fanini F, Bandini E, Plousiou M, et al. MicroRNA-16 restores sensitivity to tyrosine kinase inhibitors and outperforms MEK inhibitors in KRAS-mutated non-small cell lung cancer. Int J Mol Sci. 2021;23:22. doi:10.3390/ijms23010022
37. Swiatek M, Jancewicz I, Kluebsoongnoen J, et al. Various forms of HIF-1alpha protein characterize the clear cell renal cell carcinoma cell lines. IUBMB Life. 2020;72:1220–1232. doi:10.1002/iub.2281
38. Pajdzik K, Wilamowski M, Zurawek D, et al. Anterior gradient 2 promotes tumorigenesis through upregulation of CCAAT-enhancer binding protein beta and hypoxia-inducible factor-2 alpha and subsequent secretion of interleukin-6, interleukin-8, and vascular endothelial growth factor in the Caki-1 clear cell renal cell carcinoma cell line. IUBMB Life. 2020;72:1807–1818. doi:10.1002/iub.2331
39. Qiu B, Ackerman D, Sanchez DJ, et al. HIF2alpha-dependent lipid storage promotes endoplasmic reticulum homeostasis in clear-cell renal cell carcinoma. Cancer Discov. 2015;5:652–667. doi:10.1158/2159-8290.CD-14-1507
40. Wang W, Xie X, Zhou Z, et al. Expression analysis of MIST1 and EMT markers in primary tumor samples points to MIST1 as a biomarker of cervical cancer. Int J Gen Med. 2021;14:1293–1300. doi:10.2147/IJGM.S307367
41. Yin L, Li W, Xu A, et al. SH3BGRL2 inhibits growth and metastasis in clear cell renal cell carcinoma via activating hippo/TEAD1-Twist1 pathway. EBioMedicine. 2020;51:102596. doi:10.1016/j.ebiom.2019.12.005
42. Dong Z, Gao M, Li C, et al. LncRNA UCA1 antagonizes arsenic-induced cell cycle arrest through destabilizing EZH2 and facilitating NFATc2 expression. Adv Sci. 2020;7:1903630. doi:10.1002/advs.201903630
43. He K, Xie M, Li J, et al. CENPO is associated with immune cell infiltration and is a potential diagnostic and prognostic marker for hepatocellular carcinoma. Int J Gen Med. 2022;15:7493–7510. doi:10.2147/IJGM.S382234
44. Meng X, Yuan H, Li W, et al. Biomarker screening and prognostic significance analysis for renal cell carcinoma. Int J Gen Med. 2021;14:5255–5267. doi:10.2147/IJGM.S325347
45. Guan T, Yang X, Liang H, et al. Deubiquitinating enzyme USP9X regulates metastasis and chemoresistance in triple-negative breast cancer by stabilizing Snail1. J Cell Physiol. 2022;237:2992–3000. doi:10.1002/jcp.30763
46. Meng X, Li W, Yuan H, et al. KDELR2-KIF20A axis facilitates bladder cancer growth and metastasis by enhancing Golgi-mediated secretion. Biol Proced Online. 2022;24:12. doi:10.1186/s12575-022-00174-y
47. Lin Y, Gao X, Liu Z, et al. Effective treatment of low-grade myofibroblastic sarcoma with apatinib: a case report and literature review. Pharmgenomics Pers Med. 2022;15:573–582. doi:10.2147/PGPM.S359492
48. Bao Z, Cheng J, Zhu J, et al. Using weighted gene co-expression network analysis to identify increased MND1 expression as a predictor of poor breast cancer survival. Int J Gen Med. 2022;15:4959–4974. doi:10.2147/IJGM.S354826
49. Huang TT, Burkett SS, Tandon M, et al. Distinct roles of treatment schemes and BRCA2 on the restoration of homologous recombination DNA repair and PARP inhibitor resistance in ovarian cancer. Oncogene. 2022;41(46):5020–5031. doi:10.1038/s41388-022-02491-8
50. Li Y, Wu M, Zhang L, et al. Nonsense-mediated mRNA decay inhibition synergizes with MDM2 inhibition to suppress TP53 wild-type cancer cells in p53 isoform-dependent manner. Cell Death Discov. 2022;8:402. doi:10.1038/s41420-022-01190-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.