Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
High-Dose Baricitinib for Severe Alopecia Areata with Suboptimal Response to Conventional Therapy: A Real-World Assessment
Authors Liu Q, Sun M, Cao Y, Zhao H
Received 23 February 2026
Accepted for publication 19 June 2026
Published 30 June 2026 Volume 2026:19 604762
DOI https://doi.org/10.2147/CCID.S604762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Anne-Claire Fougerousse
Qinsi Liu, Mang Sun, Yuwei Cao, Hengguang Zhao
Department of Dermatology & Cosmetic Medicine Center, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
Correspondence: Hengguang Zhao, Department of Dermatology & Cosmetic Medicine Center, The Second Affiliated Hospital of Chongqing Medical University, 74 Linjiang Road, Yuzhong District, Chongqing, 400010, People’s Republic of China, Tel +86 139 8335 9539, Email [email protected]
Background: Severe alopecia areata (AA) causes substantial psychosocial burden, with suboptimal response rates to approved baricitinib 4 mg. Pharmacologic strategies for dose escalation, supported by inter-specialty evidence, may address this therapeutic gap.
Aim: To evaluate efficacy and safety of baricitinib 6 mg daily in severe, refractory AA patients who showed suboptimal response to conventional therapies.
Methods: In this retrospective study, four females (mean age 26.5 years) with severe AA (mean baseline Severity of Alopecia Tool, SALT 64.5) received baricitinib 6 mg between January 2023 and June 2025. Efficacy was assessed via serial SALT score changes; safety through standardized laboratory monitoring.
Results: Following escalation to baricitinib 6 mg daily, clinically meaningful SALT improvement was achieved in three patients (75%). Transient laboratory abnormalities occurred in 3 patients (75%), including asymptomatic mild platelet count elevation, self-resolving mild anemia (within normal ranges) and asymptomatic creatinine elevation. No severe adverse events occurred.
Conclusion: Baricitinib 6 mg daily demonstrated enhanced efficacy in 75% of patients with severe refractory AA and exhibited an acceptable short-term safety profile under close monitoring. These findings support further investigation of step-up dosing strategies in randomized controlled trials.
Keywords: alopecia areata, baricitinib, off-label use, dose–response relationship, treatment outcome, JAK inhibitors
Introduction
Alopecia areata (AA), a chronic immune-mediated non-scarring hair loss, imposes profound psychosocial burdens in severe cases (≥50% scalp involvement). Although JAK inhibitors (eg, baricitinib, ritlecitinib, and deuruxolitinib) are a therapeutic breakthrough, real-world efficacy remains suboptimal.1–4 Pivotal trials (BRAVE-AA1/AA2) showed only 35.9% to 40.9% of severe AA patients achieved clinically meaningful responses (Severity of Alopecia Tool, SALT ≤20) after 36–52 weeks of baricitinib 4 mg therapy, leaving approximately 60% of patients with suboptimal response.5–7 This gap is compounded by AA pathogenesis heterogeneity, where cytokine redundancy and chronicity drive JAK inhibitor resistance.8–10 Importantly, suboptimal response is particularly prevalent in specific, difficult-to-treat subgroups. Extended disease duration (eg, >10 years) and higher baseline severity (eg, SALT ≥ 95) have been identified as predictors of poorer response to JAK inhibitors.11 While the approved dose for AA is 2–4 mg daily, therapeutic strategies for such refractory cases remain an unmet need. However, dose optimization draws on rheumatology and psoriasis precedents showed baricitinib doses up to 8 mg/day in rheumatoid arthritis (RA) and 10 mg/day in psoriasis demonstrated dose-dependent efficacy, improving responses without a meaningful increase in adverse reactions.12–15 Furthermore, in the management of AA, dose escalation is recognized as one of the potential strategies when facing an inadequate response.11 Therefore, we hypothesize that increasing baricitinib may narrow the efficacy gap in severe AA while maintaining tolerability.12–14,16,17
In this retrospective assessment, we enrolled a series of patients with treatment-refractory AA characterized by extended disease duration and high baseline severity who received baricitinib at an increased daily dose of 6 mg to evaluate its efficacy and safety. Our aim is to reconsider the conventional dosing standard for this challenging subgroup, offering a pragmatic dose-optimization strategy for patients with limited therapeutic alternatives.
Methods
Medical records of four consecutive patients with severe AA (SALT ≥ 50) treated at our department between January 2023 and June 2025 were retrospectively reviewed. All patients met the following inclusion criteria: (1) primary diagnosis of severe AA (SALT ≥ 50), including alopecia totalis (AT) or alopecia universalis (AU); (2) previously received treatments of JAK inhibitors (baricitinib or ritlecitinib) or oral glucocorticoid (prednisone) for no less than 6 months, but without satisfied response or relapsed; (3) demonstrating an inadequate early response, defined as a reduction in SALT score of ≤20% from baseline after at least 6 months of standard-dose (2–4 mg) baricitinib therapy or an equivalent period of other systemic therapy; (4) patients had explicitly and in writing agreed to receive off-label high-dose baricitinib after thorough discussion of risks, benefits, and alternatives. Data extraction encompassed demographic characteristics, clinical subtypes, baseline SALT scores, treatment regimens (including dose adjustments), efficacy outcomes (absolute SALT scores and percentage improvement from baseline), adverse events, and monitoring tests. The study was approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (Approval No. 2025-LS-232). This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study for the use of their clinical data and images for research and publication purposes.
Results
In this study, four patients meeting all inclusion criteria (all female; mean age 26.5 years, range 22–33), who completed the full treatment protocol and underwent prospective safety and efficacy monitoring. All patients manifested severe hair loss (mean baseline SALT 64.5, range 50–100), with two cases (50%) classified as AU (Box 1). The cohort demonstrated heterogeneous clinical trajectories following individualized JAK inhibitor regimens, with systematic documentation of treatment modifications, efficacy outcomes, and safety parameters throughout the study period.
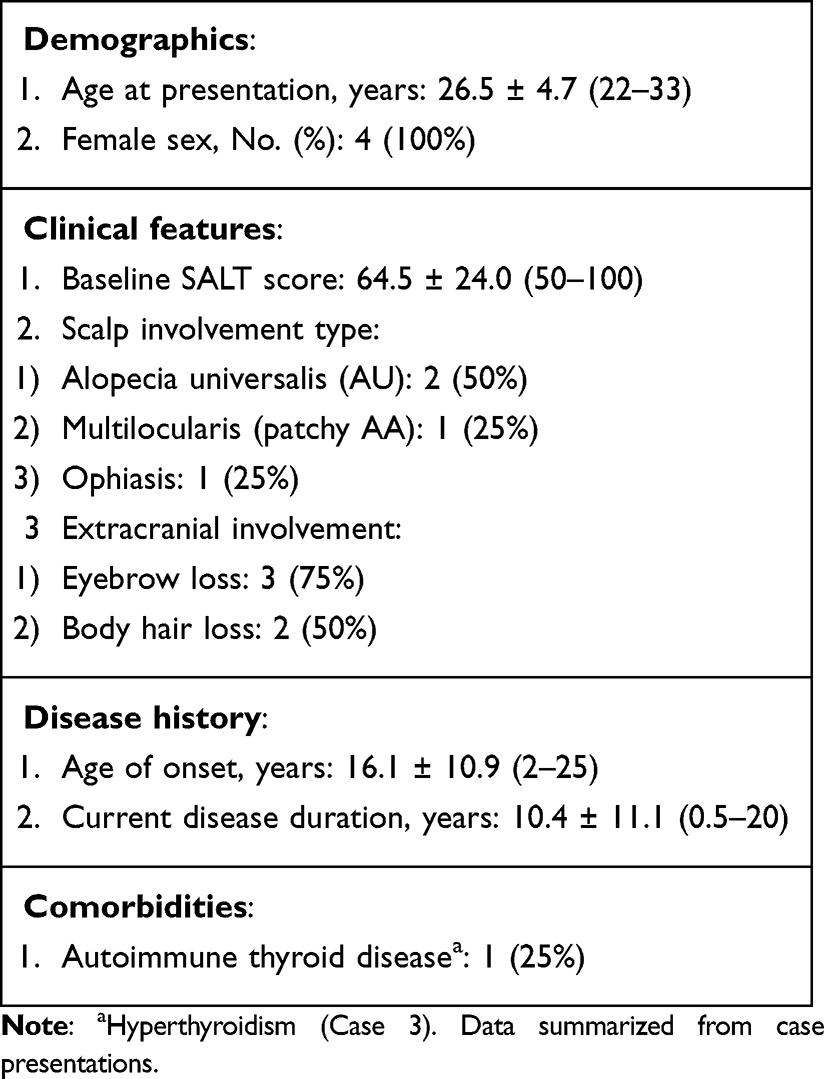 |
Box 1 Baseline Characteristics of Patients with Severe Alopecia Areata (N=4) |
Baseline Characteristics
The cohort exhibited diverse phenotypic manifestations, including one patient (25%) with multifocal patchy AA characterized by discrete bald patches (baseline SALT 50), and one patient (25%) presenting with ophiasis pattern involving band-like temporal-occipital hair loss (Box 1). Extracranial involvement was notable, with three patients (75%) demonstrating complete eyebrow alopecia and two patients (50%) manifesting total body hair loss. The mean age at disease onset was 16.1 years (range, 2–25 years), including 1 patient with onset at 2 years of age. The mean disease duration was 10.4 years (range: 0.5–20 years), including two patients with two-decade disease chronicity (Box 1). This extended disease duration aligns with the profile of patients predicted to have a higher likelihood of suboptimal response to standard JAK inhibitor therapy.11 Comorbid autoimmune conditions included one patient (Case 3) with documented hyperthyroidism requiring ongoing management, while no atopic disorders or other autoimmune comorbidities were reported. The diverse clinical presentations and chronic disease course posed significant challenges for treatment.
Individualized Therapeutic Regimens and Treatment Modifications
The therapeutic pathways for each patient, detailed in Table 1. Case 1 commenced with oral prednisone 20 mg/day tapered to 5 mg/day over eight months before transitioning to baricitinib, which underwent a stepwise escalation from 2 mg/day to 4 mg/day to address incomplete regrowth. After achieving SALT 17 on 4 mg, further escalation to 6 mg led to complete regrowth (SALT 0). Case 2 received ritlecitinib 50 mg/day for 11 months with suboptimal response (SALT 100 to 96) and recurrent upper respiratory tract infections. She was then switched directly to baricitinib 6 mg/day. The switch to a higher dose of a different JAK inhibitor aimed to overcome primary non-response and improve tolerability. Case 3 illustrates the challenge of dose reduction in severe AA. After an excellent initial response to baricitinib 4 mg/day for 6 months (SALT 58 to 2), the dose was reduced to 2 mg/day in an attempt to find the minimal effective maintenance dose. This reduction led to disease relapse, necessitating re-escalation first to 4 mg/day and ultimately to 6 mg/day to re-establish disease control. Case 4 required dose intensification from baricitinib 4 mg/day to 6 mg/day after seven months due to inadequate clinical response.
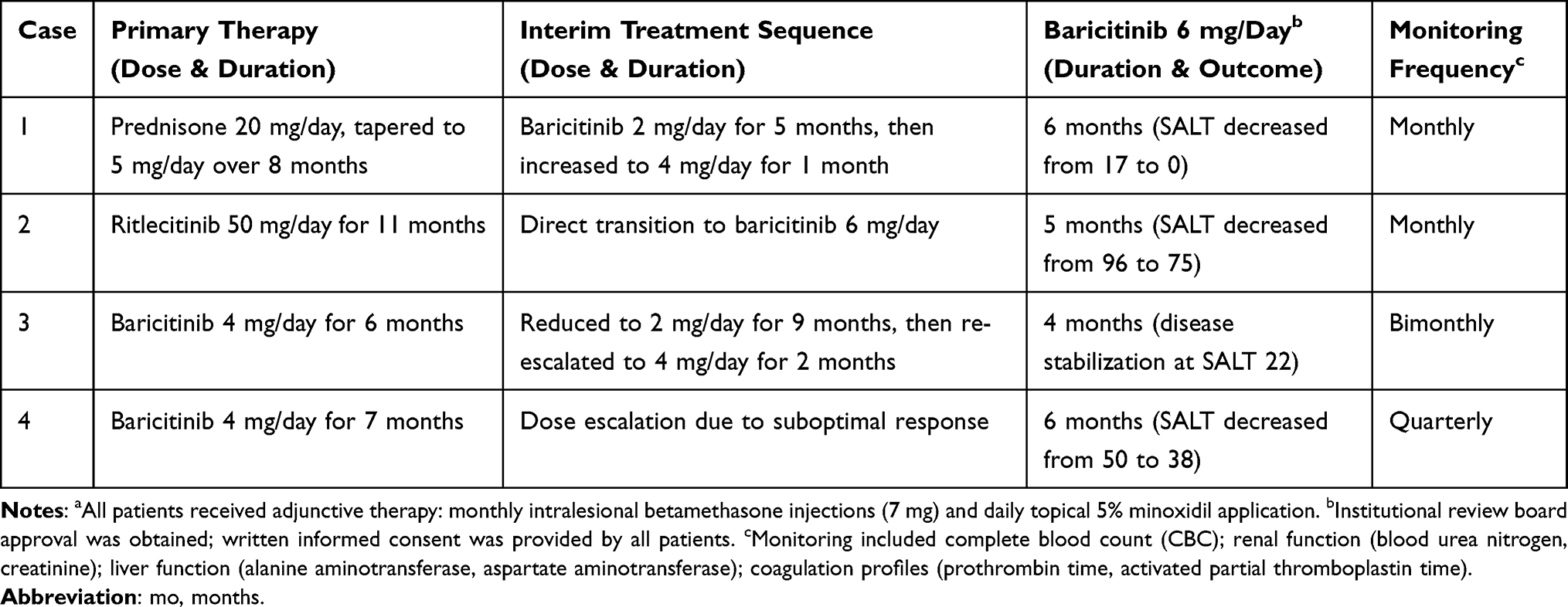 |
Table 1 Treatment Protocols and Safety Monitoring Schedule for Patientsa |
Efficacy Outcomes
Therapeutic escalation to baricitinib 6 mg/day demonstrated clinically meaningful improvements in three (75%) and stabilization in 1 of four patients (25%; Figure 1). Case 1 (Figure 2) demonstrated a robust satisfied dose-dependent response: sequential escalation from baricitinib 2 mg to 6 mg over 6 months resulted in progressive improvement, culminating in complete hair regrowth (SALT 0) at month 6 of 6 mg therapy. Case 2 (Figure 3) achieved a reduction in SALT score from 96 to 75 after 5 months of baricitinib 6 mg/day, contrasting with marginal improvement during prior ritlecitinib therapy (SALT 100 to 96 over 11 months). Although SALT did not reach ≤20, the patient reported modest visible regrowth. Case 3 (Figure 4) initially responded well to 4 mg/day (improvement from baseline SALT 58 to 2) but subsequently relapsed during dose reduction. Following disease progression despite re-challenge with 4 mg/day, escalation to 6 mg/day resulted in disease stabilization, underscoring that higher therapeutic intensity may be required to maintain control in severe AA. Case 4 (Figure 5) exhibited gradual improvement, achieving a SALT reduction from 50 to 38 after 6 months of sustained 6 mg therapy. The treatment outcomes across all cases revealed that 75% of patients (3/4) were dose-dependent responders, demonstrating that baricitinib 6 mg daily is clinically essential for refractory AA cases or inadequate response to lower doses (2–4 mg).
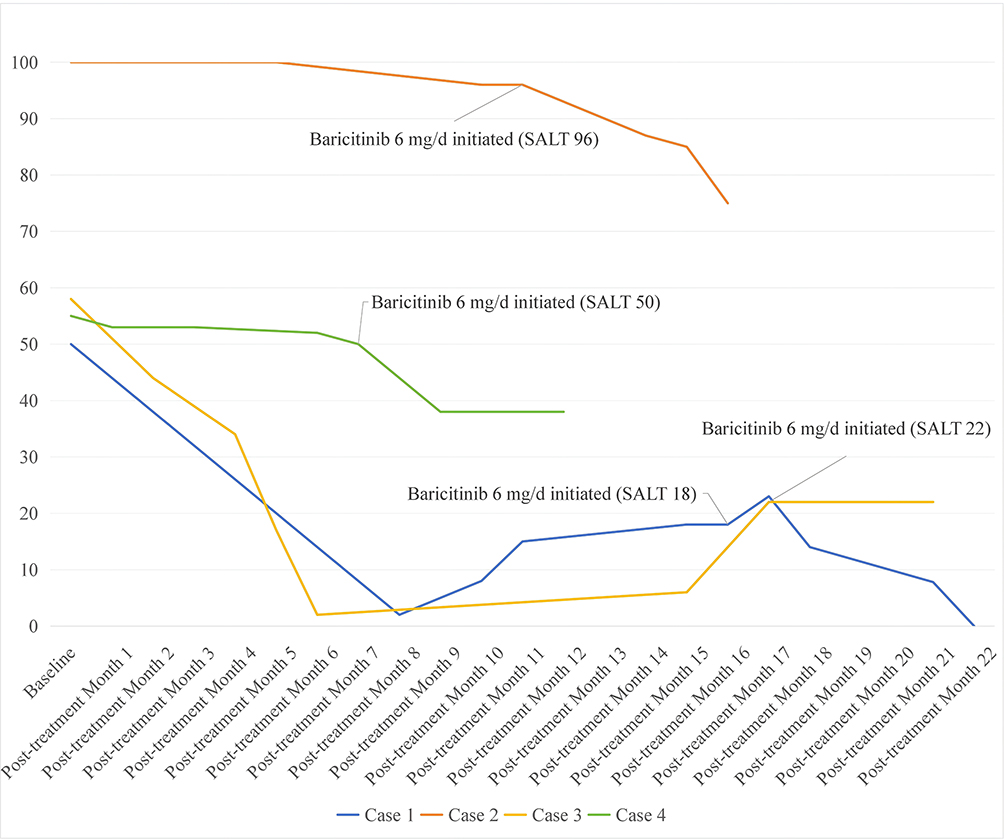 |
Figure 1 Longitudinal SALT (Severity of Alopecia Tool) score aggregation trends across all cases during therapy. |
 |
Figure 2 Clinical response of the patient to high-dose baricitinib (6 mg/day). (A–D) Baseline scalp appearance: (A) left temporal, (B) right temporal, (C) occipital, (D) vertex. (E–H) After 6 months of treatment: (E) left temporal, (F) right temporal, (G) occipital, (H) vertex. Progressive improvement in hair regrowth was observed. |
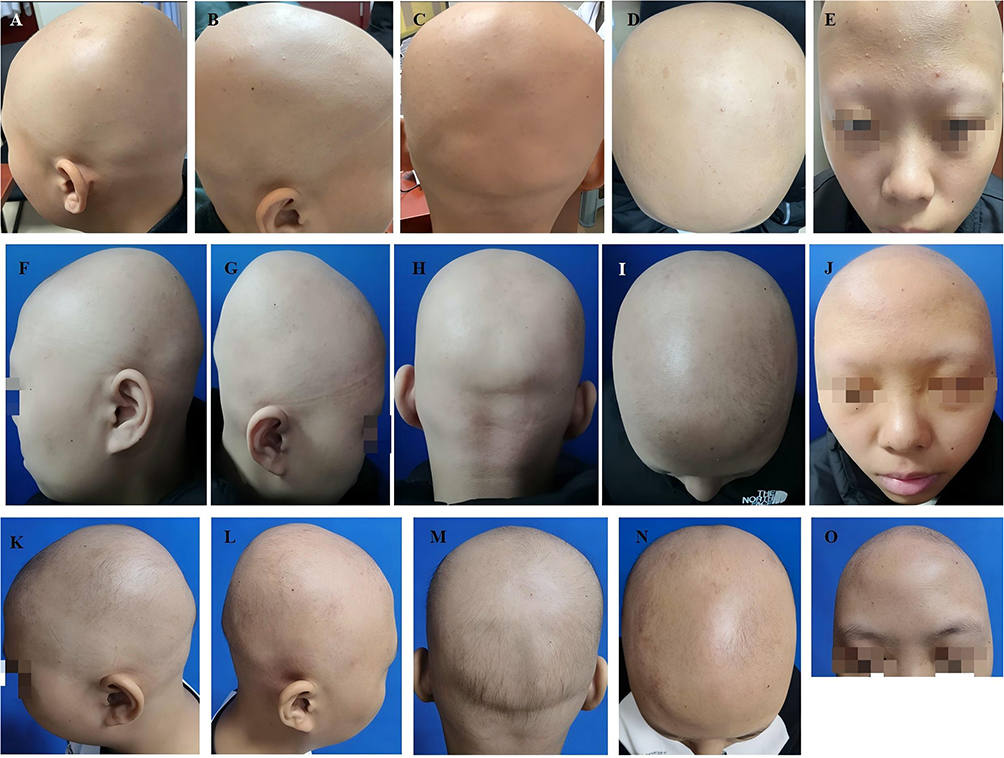 |
Figure 3 Clinical response of the patient to high-dose baricitinib (6 mg/day). (A–E) Pretreatment baseline: (A) left temporal, (B) right temporal, (C) occipital, (D) vertex, (E) eyebrows. (F–J) At initiation of baricitinib 6 mg/day: (F) left temporal, (G) right temporal, (H) occipital, (I) vertex, (J) eyebrows. (K–O) After 5 months of treatment: (K) left temporal, (L) right temporal, (M) occipital, (N) vertex, (O) eyebrows. Limited scalp and eyebrow hair regrowth was observed. |
 |
Figure 4 Clinical course of the patient on high-dose baricitinib (6 mg/day). (A–D) Baseline alopecia before therapy: (A) left temporal, (B) right temporal, (C) occipital, (D) vertex. (E–H) After 6 months of baricitinib 4 mg/day: (E) left temporal, (F) right temporal, (G) occipital, (H) vertex. (I–L) At commencement of baricitinib 6 mg/day: (I) right temporal, (J) occipital, (K) occipital (second view), (L) vertex. Left temporal view was not recorded at this time point. (M–P) Stabilization achieved after 4 months of treatment: (M) left temporal, (N) right temporal, (O) occipital, (P) vertex. Disease stabilization was achieved after dose escalation. |
 |
Figure 5 Clinical response of the patient (Case 4) to high-dose baricitinib (6 mg/day). (A–D) Pretreatment baseline: (A) left temporal, (B) right temporal, (C) occipital, (D) frontal hairline. (E–H) Clinical status at initiation of baricitinib 6 mg/day: (E) left temporal, (F) right temporal, (G) occipital, (H) vertex. (I–L) After 6 months of continuous treatment: (I) left temporal, (J) right temporal, (K) occipital, (L) vertex. Gradual improvement in scalp hair regrowth was observed. |
Safety Profile
The therapeutic regimens demonstrated acceptable safety profiles with predominantly mild laboratory abnormalities (Table 2). Asymptomatic platelet count elevations occurred in Case 1 (397 to 416 × 103/μL) and Case 2 (platelet count, 324 to 334 × 103/μL). These values remained within normal ranges and did not require intervention. Case 3 developed mild anemia (hemoglobin, 10.7 g/dL vs normal range of 11.5–15.0 g/dL) that resolved spontaneously within 5 months without dose adjustment. Metabolic alterations manifested as elevated serum creatinine in Case 2 (0.85 mg/dL vs normal of 0.46–0.82 mg/dL), which remained stable during continued therapy. Case 2 experienced recurrent upper respiratory tract infections (approximately twice monthly) during ritlecitinib therapy, while resolved upon switching to baricitinib 6 mg/d. No patient developed hepatic transaminitis, lipid abnormalities, or coagulation disorders during monitoring.
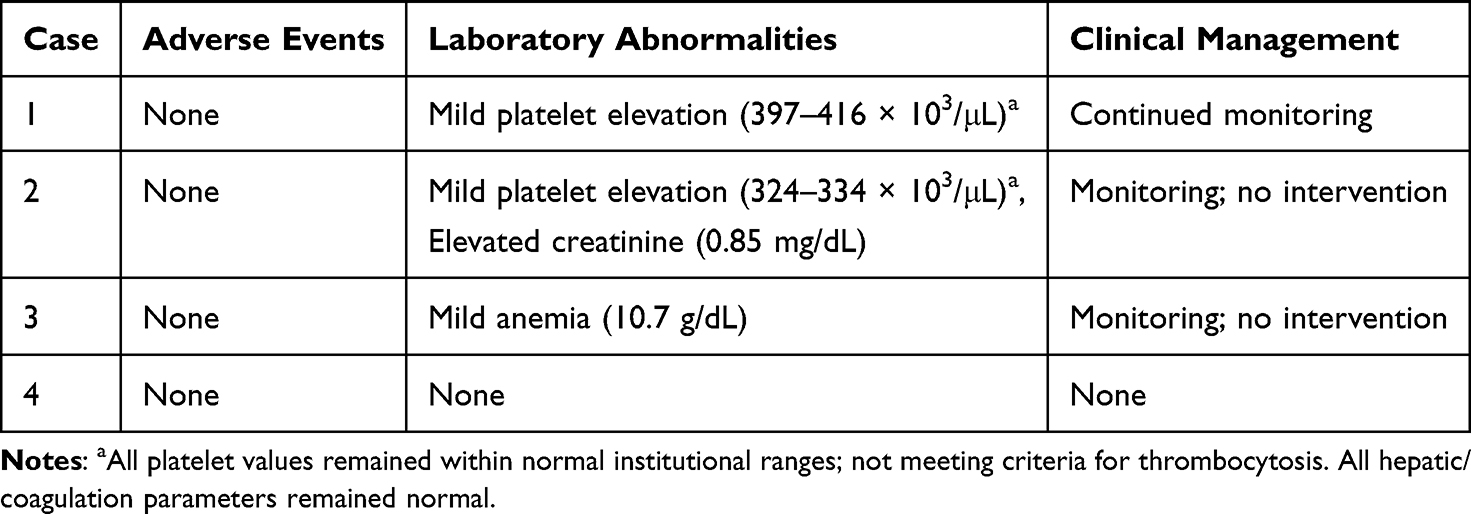 |
Table 2 Safety and Laboratory Abnormalities |
Discussion
While oral JAK inhibitors like baricitinib have recently transformed the landscape for AA, pivotal Phase III studies have consistently shown that, even at the currently approved maximal dose (4 mg), a significant proportion, more than half of patients with severe disease fail to achieve substantial regrowth.5–7 This is especially true for patients with predictive factors for poorer outcomes, such as long disease duration and very high baseline SALT scores, a profile that matches our cohort (mean duration 10.4 years; two patients with AU).11
We acknowledge the standard 12-month efficacy assessment timeline. However, our treatment decisions were informed by emerging evidence that early incomplete response may predict poor long-term outcomes, combined with patient preferences for more aggressive management.18–20 For patients with minimal early improvement (≤20% SALT reduction at 6 months), particularly those with poor prognostic features, persisting with a suboptimal regimen for an additional 6 months may prolong psychosocial distress. Regarding the initiation of 6 mg baricitinib in patients with SALT <50 (Cases 1 and 3), recent international consensus statements indicate that AA severity can be upgraded beyond scalp SALT scores based on additional factors such as long disease duration, prior treatment failures, rapid relapse upon dose reduction, and significant psychosocial impact. Our patients exhibited multiple such factors, justifying escalation despite moderate SALT scores.18–20
Importantly, we do not advocate for routine early-dose escalation. Rather, we propose that in a well-defined, refractory subgroup (characterized by long disease duration, high baseline severity, and ≤20% SALT improvement at 6 months), as well as a carefully monitored trial of dose intensification represents a rational and personalized treatment strategy.
Our data indicate baricitinib 6 mg/day induces further regrowth in patients suboptimal to 2–4 mg/day. Following therapeutic dose escalation, 100% of the cohort achieved either hair regrowth or disease stabilization, suggesting higher dosing may overcome the 4 mg efficacy “ceiling” in select refractory AA patients. To our knowledge, this is the first systematic evaluation of baricitinib 6 mg for AA, innovatively applying rheumatology and psoriasis paradigms to dermatology.12–15,21 In our cohort, only mild transient platelet count elevations occurred, with no severe adverse events, supporting an acceptable short-term risk profile under vigilant monitoring.
Our study is limited by its small sample size and retrospective design, as well as variability in baseline SALT scores at the time of 6 mg initiation (not all patients had SALT ≥50 at that point, reflecting real-world disease fluctuation). Future randomized controlled trials are warranted to validate the efficacy and long-term safety of baricitinib dose escalation and to better define the characteristics of patients who would benefit most from this approach.
Conclusions
This study provides novel preliminary evidence supporting the therapeutic potential of baricitinib 6 mg daily as an optimized-dose strategy for a well-defined subgroup of patients with severe, long-standing, treatment-refractory AA who show an inadequate early response to standard dosing. Our findings suggest that dose escalation beyond the currently approved 4 mg can enhance clinical efficacy by overcoming resistance mechanisms, while maintaining a manageable safety profile under vigilant monitoring, which lays the groundwork for individualized, stepwise treatment paradigms in AA. Future prospective studies are needed to confirm these findings and to establish standardized criteria for early treatment intensification in refractory disease.
Data Sharing Statement
The anonymized individual patient data supporting the findings of this study have been deposited in the Mendeley Data repository and are publicly available. Liu, Qinsi. (2025). Excessive-Dose Baricitinib for Severe Alopecia Areata Unresponsive to Conventional Therapy: A Real-World Assessment Dataset. Mendeley Data. https://doi.org/10.17632/wgb2kxd2nc.1. The data are also available from the corresponding author upon reasonable request.
Author Contributions
Qinsi Liu contributed to the study conception and design, data collection, analysis and interpretation, visualization, and drafted the original manuscript. Mang Sun assisted in data validation, formal analysis, and literature review. Yuwei Cao contributed to clinical data extraction and safety data verification. Hengguang Zhao (corresponding author) was responsible for overall study design, supervision, methodology, critical revision of the manuscript for important intellectual content, and final approval. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Natural Science Foundation of China (no.82473555, 82173440, and 82304058), Natural Science Foundation of Chongqing (cstc2021jcyj-msxmX0955), and Chongqing Postdoctoral Science Foundation (CSTB2023NSCQ-BHX0049). The National Natural Science Foundation of China, Natural Science Foundation of Chongqing, and Chongqing Postdoctoral Science Foundation had no role in the preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors report there are no competing interests to declare for this work.
References
1. King B, Shapiro J, Ohyama M, et al. When to expect scalp hair regrowth during treatment of severe alopecia areata with baricitinib: insights from trajectories analyses of patients enrolled in two phase III trials. Br J Dermatol. 2023;189(6):666–10. doi:10.1093/bjd/ljad253
2. Apalla Z, Zafiriou E, Zagkliverinou E, et al. Real-world experience of tofacitinib and baricitinib use in alopecia areata in Greek population: a retrospective analysis with focus on safety. Dermatol Pract Concept. 2024;14(2):e2024073. doi:10.5826/dpc.1402a73
3. Mesinkovska N, King B, Zhang X, et al. Efficacy and safety of ritlecitinib, an oral JAK3/TEC family kinase inhibitor, in adolescent and adult patients with alopecia totalis and alopecia universalis. J Dermatol. 2024;51(11):1414–1424. doi:10.1111/1346-8138.17442
4. Tsianakas A, Passeron T, Magnolo N, et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase 1/2 inhibitor, in adults with alopecia areata: results from the THRIVE-AA2 Phase 3, randomized, double-blind, controlled trial. J Am Acad Dermatol. 2026;94(4):1134–1143. doi:10.1016/j.jaad.2025.11.070
5. Kwon O, Senna MM, Sinclair R, et al. Efficacy and safety of baricitinib in patients with severe alopecia areata over 52 weeks of continuous therapy in two phase III trials (BRAVE-AA1 and BRAVE-AA2). Am J Clin Dermatol. 2023;24(3):443–451. doi:10.1007/s40257-023-00764-w
6. King B, Ko J, Kwon O, et al. Baricitinib withdrawal and retreatment in patients with severe alopecia areata: the BRAVE-AA1 randomized clinical trial. JAMA Dermatol. 2024;160(10):1075–1081. doi:10.1001/jamadermatol.2024.2734
7. Ko JM, Mayo TT, Bergfeld WF, et al. Clinical outcomes for uptitration of baricitinib therapy in patients with severe alopecia areata: a pooled analysis of the BRAVE-AA1 and BRAVE-AA2 Trials. JAMA Dermatol. 2023;159(9):970–976. doi:10.1001/jamadermatol.2023.2581
8. Barati Sedeh F, Michaelsdóttir TE, Henning MAS, Jemec GBE, Ibler KS. Comparative efficacy and safety of janus kinase inhibitors used in alopecia areata: a systematic review and meta-analysis. Acta Derm Venereol. 2023;103:adv00855. doi:10.2340/actadv.v103.4536
9. Lensing M, Jabbari A. An overview of JAK/STAT pathways and JAK inhibition in alopecia areata. Front Immunol. 2022;13:955035. doi:10.3389/fimmu.2022.955035
10. Damsky W, King BA. JAK inhibitors in dermatology: the promise of a new drug class. J Am Acad Dermatol. 2017;76(4):736–744. doi:10.1016/j.jaad.2016.12.005
11. Zhang X, Jiang Y. Predictors and management of inadequate response to JAK inhibitors in alopecia areata. Am J Clin Dermatol. 2024;25(6):975–986. doi:10.1007/s40257-024-00884-x
12. Keystone EC, Genovese MC, Schlichting DE, et al. Safety and efficacy of baricitinib through 128 weeks in an open-label, longterm extension study in patients with rheumatoid arthritis. J Rheumatol. 2018;45(1):14–21. doi:10.3899/jrheum.161161
13. Papp KA, Menter MA, Raman M, et al. A randomized phase 2b trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br J Dermatol. 2016;174(6):1266–1276. doi:10.1111/bjd.14403
14. Tanaka Y, Ishii T, Cai Z, Schlichting D, Rooney T, Macias W. Efficacy and safety of baricitinib in Japanese patients with active rheumatoid arthritis: a 52-week, randomized, single-blind, extension study. Mod Rheumatol. 2018;28(1):20–29. doi:10.1080/14397595.2017.1307899
15. Kremer JM, Genovese MC, Keystone E, et al. Effects of baricitinib on lipid, apolipoprotein, and lipoprotein particle profiles in a Phase IIb Study of patients with active rheumatoid arthritis. Arthritis Rheumatol. 2017;69(5):943–952. doi:10.1002/art.40036
16. Samuel C, Cornman H, Kambala A, Kwatra SG. A review on the safety of using JAK inhibitors in dermatology: clinical and laboratory monitoring. Dermatol Ther. 2023;13(3):729–749. doi:10.1007/s13555-023-00892-5
17. Wang Y, Liu T, Li S, et al. Efficacy and safety of baricitinib in patients with refractory alopecia areata. Dermatol Ther. 2022;35(12):e15845. doi:10.1111/dth.15845
18. Moussa A, Bennett M, Wall D, et al. The Alopecia Areata Severity and Morbidity Index (ASAMI) study: results from a global expert consensus exercise on determinants of alopecia areata severity. JAMA Dermatol. 2024;160(3):341–350. doi:10.1001/jamadermatol.2023.5869
19. Harries MJ, Ascott A, Asfour L, et al. British Association of Dermatologists living guideline for managing people with alopecia areata 2024. Br J Dermatol. 2025;192(2):190–205. doi:10.1093/bjd/ljae385
20. Zhou C, Du X, Fan W, et al. Expert consensus on systemic treatment activation and grading evaluation for alopecia areata. Chin Med J. 2025. doi:10.1097/cm9.0000000000003870
21. Taylor PC, Takeuchi T, Burmester GR, et al. Safety of baricitinib for the treatment of rheumatoid arthritis over a median of 4.6 and up to 9.3 years of treatment: final results from long-term extension study and integrated database. Ann Rheumatic Dis. 2022;81(3):335–343. doi:10.1136/annrheumdis-2021-221276
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Potential Mechanism of Fatigue Induction and Its Management by JAK Inhibitors in Inflammatory Rheumatic Diseases
Felis-Giemza A, Massalska M, Roszkowski L, Romanowska-Próchnicka K, Ciechomska M
Journal of Inflammation Research 2023, 16:3949-3965
Published Date: 8 September 2023