Back to Journals » Psychology Research and Behavior Management » Volume 19
Hidden Shields: How Parental Resilience and Social Intelligence Shape Behavioral Profiles in Children with Autism Spectrum Disorder
Authors Alqarawi N, Hamzaa HG, El-Sayed MM, Khedr MA ![]() , Hendy A
, Hendy A ![]() , Amin SM, Klila ZEK
, Amin SM, Klila ZEK
Received 24 January 2026
Accepted for publication 28 March 2026
Published 9 April 2026 Volume 2026:19 598638
DOI https://doi.org/10.2147/PRBM.S598638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Nada Alqarawi,1 Huda Gaber Hamzaa,2,3 Mona Metwally El-Sayed,1 Mahmoud Abdelwahab Khedr,4 Abdelaziz Hendy,5 Shaimaa Mohamed Amin,1 Zainab Eid Kamal Klila3
1Department of Community, Psychiatric, and Mental Health Nursing, College of Nursing, Qassim University, Buraydah, 52571, Saudi Arabia; 2Psychiatric and Mental Health Nursing, Department of Nursing, College of Applied Medical Sciences, King Faisal University, Al-Ahsa, 31982, Saudi Arabia; 3Psychiatric and Mental Health Nursing Department, College of Nursing, Port Said University, Port Said, Egypt; 4Department of Psychiatric and Mental Health Nursing, Faculty of Nursing, Alexandria University, Alexandria, Egypt; 5Department of Maternal and Child Health Nursing, College of Nursing, Qassim University, Buraydah, 52571, Saudi Arabia
Correspondence: Mona Metwally El-Sayed, Department of Community, Psychiatric, and Mental Health Nursing, College of Nursing, Qassim University, Buraydah, 52571, Saudi Arabia, Email [email protected]
Background: Parents of autistic children face significant stress, which can impact their child’s behavioral outcomes. Parental psychological resources, specifically resilience and social intelligence, are theorized to be protective factors, yet their combined influence and interplay require further investigation.
Objective: This study aimed to examine the relationships between parental resilience, parental social intelligence, and concerning behaviors in autistic children, and to test whether social intelligence mediates the link between parental resilience and child behavior.
Methods: A cross-sectional study was conducted with 300 parents of children diagnosed with ASD at a mental health outpatient clinic. Participants completed the Arabic versions of the Brief Resilience Scale, the Tromsø Social Intelligence Scale, and the Assessment of Concerning Behavior scale. Data were analyzed using descriptive statistics, Pearson’s correlations, multiple linear regression (controlling for child age, level of needs, parental income, and rehabilitation participation), and mediation analysis with the PROCESS macro.
Results: Both parental resilience and social intelligence were negatively correlated with children’s internalizing problems (r = − 0.38 and − 0.33), externalizing problems (r = − 0.23 and − 0.27), and total concerning behavior (r = − 0.36 and − 0.36; all p< 0.001). After controlling for covariates, regression analysis indicated both factors remained significant predictors, explaining 25.8% of the variance in concerning behavior (R2 =0.258, p < 0.001). Mediation analysis confirmed a significant partial mediation, where social intelligence accounted for 17.1% of the association between resilience and child behavior (Sobel z = − 3.08, p =0.002).
Conclusion: Parental resilience and social intelligence are significant, interrelated protective factors associated with reduced behavioral problems in children with ASD. Interventions that simultaneously enhance both parental resources may be most effective in improving family well-being and child outcomes.
Keywords: child, autism spectrum disorder, resilience, psychological, emotional intelligence, parents
Introduction
Autism Spectrum Disorder (ASD), as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is a group of neurodevelopmental disorders characterized by early onset and persistent challenges in social interaction, communication, and the presence of restricted or repetitive behaviors and interests.1 Over the past two decades, the prevalence of ASD has increased significantly, with improved recognition and awareness contributing to its identification in approximately 1–2% of the global population.2,3 A global meta-analysis estimated the prevalence of ASD to be 0.6% worldwide.3 In the United States, data from the Centers for Disease Control and Prevention (CDC) showed that the prevalence of ASD among 8-year-old children was 1 in 59 in 2014, increased to 1 in 54 in 2016, and was 1 in 36 in 2020.4,5 In Egypt, studies on the prevalence of ASD are more limited, and estimates vary considerably depending on methodology and population sampled. Research conducted in the Sharkia Governorate reported a community-based prevalence rate of 5.4 per 1,000 children (95% CI: 3.8–7.5), or approximately 0.54%, among preschool children.6 A more recent study utilizing a nationally representative sample of Egyptian children aged 1 to 12 years estimated the prevalence of ASD at 0.91% (95% CI: 0.68–1.19), with higher rates observed among boys and urban residents.7
Although reported prevalence rates in Egypt appear lower than estimates from high-income countries, this likely reflects contextual factors rather than true differences in underlying risk. In many low- and middle-income settings, limited specialist services, delayed referral pathways, and insufficient training among primary care providers contribute to under-recognition and underdiagnosis of ASD. Additionally, societal stigma and misconceptions about developmental and behavioral difficulties may lead families to avoid or postpone seeking formal assessment, further suppressing officially documented prevalence. Therefore, existing Egyptian figures should be interpreted cautiously, as they may underestimate the true burden of ASD in the community.6,8
Families of children with ASD face substantial challenges that span physical, emotional, and financial domains.7 Due to the lifelong nature of support, many children with ASD require families to often experience heightened stress. Parents frequently report that their children struggle with basic daily tasks. Social difficulties are also common, as children with ASD usually find it challenging to form friendships and maintain social relationships, which can further strain family dynamics.9 Behavioral problems are also highly prevalent among children with ASD, further intensifying the challenges for families. Over 90% of children with ASD exhibit at least one co-occurring behavioral issue, including inattention, hyperactivity, oppositional behaviors, temper tantrums, aggression, abnormal fear responses, disrupted eating and sleeping patterns, or self-injurious behaviors.10 These behavioral difficulties increase the complexity of caregiving and treatment approaches, heightening parental stress. Factors such as the child’s behavioral phenotype, severity of impairment, age, and gender have also been associated with parental stress and overall emotional well-being.11
Studies suggest that parental resilience and social support are crucial in mitigating these challenges and fostering a stable family environment.12,13 Resilience, conceptualized as a “positive adaptation within the context of significant adversity”,14 is a dynamic process involving the presence of risk, positive adaptation outcomes, and protective factors.15,16 Protective factors, such as social support, cognitive appraisals, and religiosity, enhance coping capacity and psychological well-being, enabling parents to manage the demands of parenting a child with ASD.12,17 Several resilience models describe how protective factors function. In the compensatory model, protective factors (eg., social support or spirituality) directly counterbalance stress, helping parents achieve better outcomes despite challenges.18 In the protective model, protective factors interact with adversity to lessen its impact. For instance, parents with strong social support may report higher life satisfaction, even when facing severe behavioral challenges in their child.19,20
Parents of children with ASD require not only resilience but also external support due to the significant challenges they face.21,22 Social intelligence (SI) is crucial in helping them build supportive relationships and advocate for their children’s needs. Silberman and Hansburg (2000) outlined several characteristics of SI, which include understanding others, expressing feelings and personal ideas, articulating personal needs, providing and receiving feedback from others, motivating and inspiring those around them, offering innovative solutions to complex problems, and valuing teamwork over individual work while being a good team member. Individuals with high levels of social intelligence are often better equipped to solve everyday problems and cope with challenging situations using effective strategies.23
Studies have shown that the ability of parents of children with ASD to make supportive social relationships was linked to improved parental mood, reduced psychological distress, and enhanced parenting efficacy.24–26 Research showed that family support increases optimism and positive maternal well-being, while emotional support can lessen negative feelings. However, persistent stress often leads to lower perceptions of available support, indicating that parents may be unaware of resources.22,27
SI can be broadly categorized into two key domains: social awareness and social facility.25,26 Social awareness involves perceiving and understanding social cues, emotions, and dynamics, enabling parents to recognize and respond to their child’s unique behavioral triggers. On the other hand, social facility encompasses managing interactions effectively, fostering collaboration, and navigating social relationships. This is especially important for advocating for their child’s needs in educational and healthcare systems and building a strong social support network.27
Research indicated that parents with higher levels of SI are more likely to use effective strategies to manage behavioral challenges in children with ASD.18 SI improves communication, helping parents connect empathetically with their children, which fosters emotional security and reduces behavioral outbursts.12 Additionally, socially intelligent parents better establish support networks, demonstrating empathy and problem-solving skills that enable their children to improve social skills and reduce maladaptive behaviors.12,13,25 In Egypt, cultural factors may uniquely influence both parental resilience and SI. Strong family bonds, religious coping mechanisms, and community support networks, particularly in rural areas, may serve as important resources that enhance parents’ capacity to manage the challenges of raising a child with ASD.7 Religious faith often provides meaning-making frameworks that help parents reframe their experiences and maintain hope.28 Understanding how these cultural dynamics shape parental psychological resources is essential for developing culturally appropriate interventions in the Egyptian context.
Most research on parental resilience, social intelligence, and child behavior in ASD has been conducted in high-income countries, with relatively little evidence from Arab or North African contexts. In Egypt, families of children with ASD navigate unique combinations of limited formal services, financial constraints, and stigma, which may shape how parental psychological resources translate into child behavioral outcomes.9 Understanding these processes in the Egyptian setting is crucial for designing culturally sensitive interventions that strengthen parental resilience and social resources while addressing children’s internalizing and externalizing difficulties. Thus, this paper aimed to provide a comprehensive analysis of the role of parental resilience and social intelligence in shaping behavioral issues among children with ASD. By determining these factors, it seeks to highlight their importance in addressing the challenges of ASD and informing future intervention strategies.
Study Objectives
Primary Objective
To examine the relationships between parental resilience, parental social intelligence, and concerning behaviors in autistic children.
Secondary Objective
To test whether parental social intelligence mediates the relationship between parental resilience and concerning behaviors in autistic children.
Research Hypotheses
H1: Parental social intelligence will be positively correlated with parental resilience in autistic children. H2: Parental resilience will be negatively correlated with behavior problems in autistic children. H3: Parental social intelligence will be negatively correlated with behavior problems in autistic children. H4: Parental social intelligence will mediate the relationship between parental resilience and behavior problems in autistic children (Figure 1).
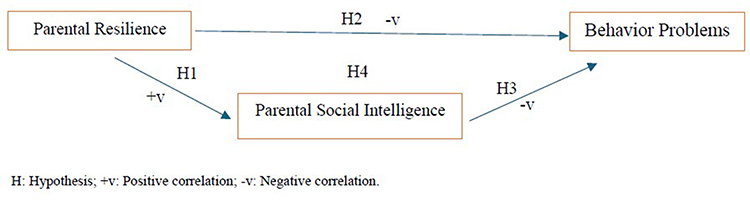 |
Figure 1 Conceptual model illustrating the hypothesized mediating role of parental social intelligence in the relationship between parental resilience and concerning behaviors in autistic children. |
Methods
Study Design and Setting
A cross-sectional descriptive research design was utilized to conduct the study, following the STROBE checklist for accurate and transparent reporting. The research took place at the Mental Health Hospital, Child Clinic, located in Port Said’, Egypt. This specialized governmental institution operates under the Ministry of Health and Population, offering a wide range of mental health services to individuals of all ages. The Child Clinic serves as a dedicated outpatient department within the hospital, specializing in the evaluation, diagnosis, and treatment of diverse childhood psychiatric and developmental conditions, with a particular focus on ASD.
Sample Size and Study Population
The sample size of the study was based on the feasibility of the research as well as statistical considerations. The sample of 300 parents of children with ASD was used, which was higher than the recommended number of participants for multiple regression with two predictor variables. The sample size of 300 was sufficient to detect a medium effect size with adequate statistical power, according to the guidelines of Cohen (2017).29 A post hoc power analysis was conducted using GPower 3.1. With an alpha of 0.05 and an observed effect size (f2 = 0.272), the statistical power exceeded 0.99, indicating that the study was adequately powered to detect the reported associations.
The inclusion criteria consisted of parents of children who had received a formal diagnosis of ASD from a certified healthcare professional and who expressed a willingness to participate in the study. Conversely, the exclusion criteria ruled out parents with known cognitive or psychological impairments that could impede their ability to fully understand and accurately respond to the study instruments. This exclusion was applied to ensure the validity of self-report responses; however, it may have limited the generalizability of findings to parents with such conditions.
Participants
A total of 300 parents of children diagnosed with autism spectrum disorder (ASD) were included in the study. The mean age of parents was 34.41 years (SD = 5.41). The sample was predominantly female (95.7%), and over half of the participants held a bachelor’s degree (58.3%). The majority were not employed or were housewives (84.7%), and most reported insufficient monthly income (95.3%). Most participants resided in rural areas (67.3%), and a substantial proportion reported participation in counseling or psychotherapy programs (79.0%), see Table 1.
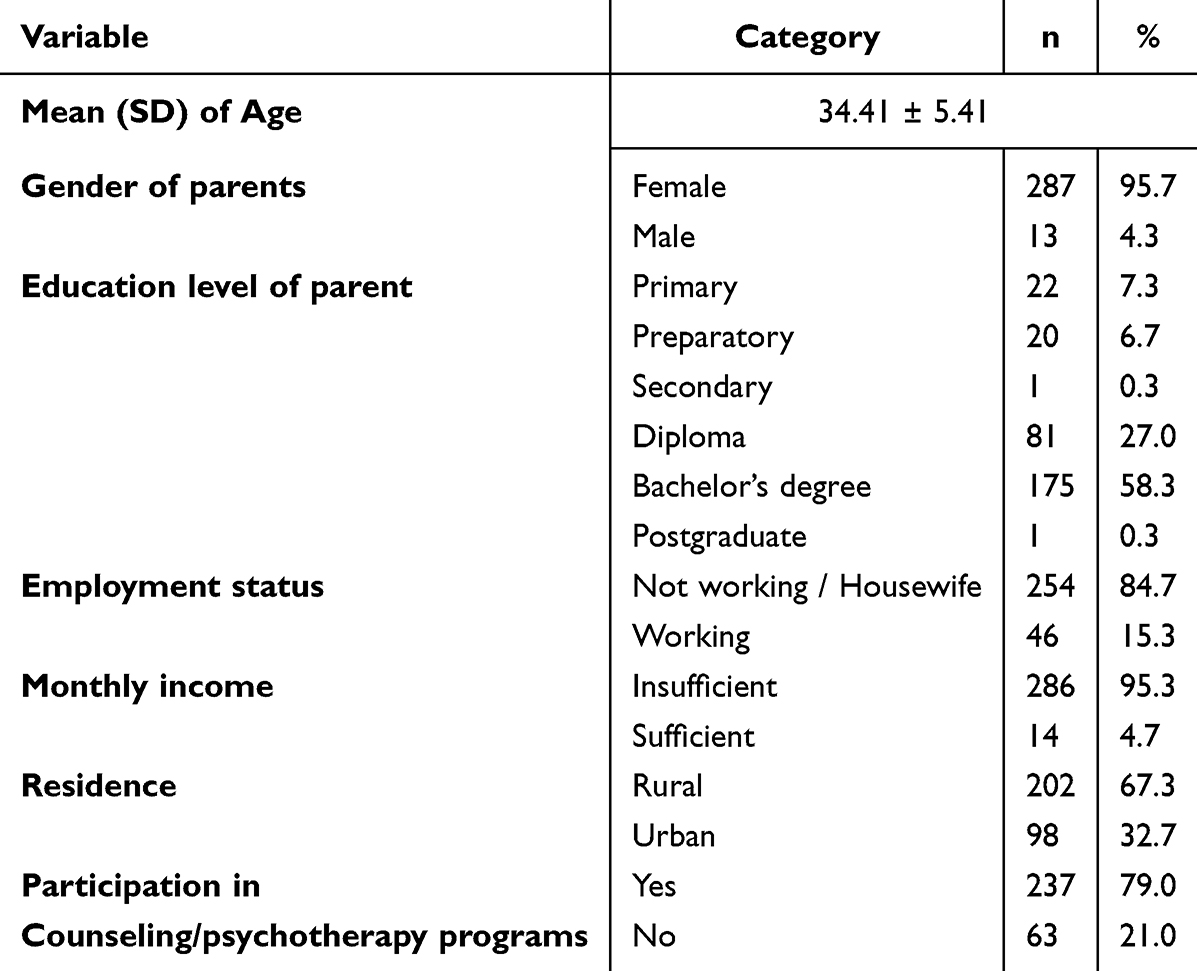 |
Table 1 Sociodemographic and Background Characteristics of Parents (n=300) |
The children had a mean age of 8.46 years (SD = 2.52), with the largest proportion aged between 6 and 8 years (46.3%). Most children were male (74.7%) and enrolled in primary school (67.3%). More than half had been diagnosed with ASD for four years or more (55.3%), and the majority were classified as having moderate support needs (86.3%). Nearly all children were non-fluent speakers (99.7%), and most were engaged in rehabilitation programs (96.7%), see Table 2.
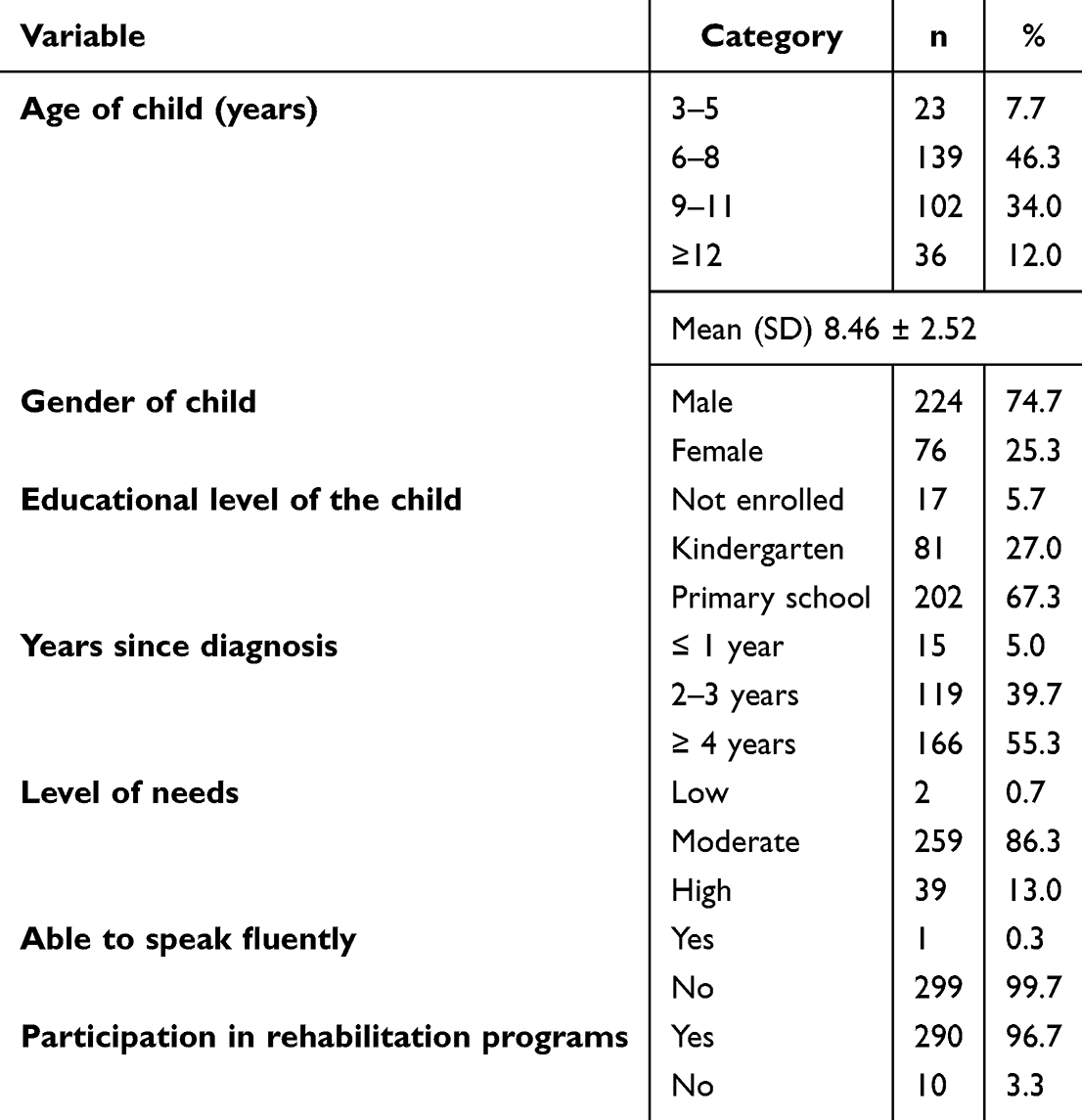 |
Table 2 Characteristics of Children with Autism Spectrum Disorder (n=300) |
Measurement of Interests
Demographic Form
The demographic form collected detailed information about both the parents and the child. For parents, it captured data on age, gender, marital status, place of residence, occupation, and family income. For the child, the form included details on age, gender, educational status, and the duration since receiving an autism diagnosis.
Brief Resilience Scale (BRS)
The Brief Resilience Scale (BRS) is a self-reported instrument designed to assess an individual’s capacity to recover or “bounce back” from adversity and stress. Originally developed by Smith et al in 2008, the BRS has been widely validated across diverse populations and cultural settings.30 The Arabic version, adapted by Baattaiah et al in 2023, comprises 6 items rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).31 Three of the items are reverse-scored, and a higher overall score indicates greater resilience. The Arabic BRS demonstrated strong psychometric properties, including excellent internal consistency (α = 0.98) and test–retest reliability (ICC = 0.88, 95% CI: 0.82–0.92, p ≤ 0.0001). Factor analysis revealed a two-factor structure with satisfactory fit indices (CMIN/DF = 9.105, GFI = 0.97, CFI = 0.99, RMSEA = 0.09). The scale also showed negative correlations with anxiety (r = −0.61), depression (r = −0.60), and stress (r = −0.53). In the current study, the Arabic BRS demonstrated additional evidence of reliability, with Cronbach’s alpha of 0.91, indicating excellent internal consistency.
Arabic Version of the Tromso Social Intelligence Scale (TSIS)
The Tromso Social Intelligence Scale (TSIS) is a self-report measure created by Silvera et al in 2001 to assess social intelligence.32 The Arabic version was developed by Chater et al in 2022, consisting of 21 items distributed across three subscales, each containing 7 items.33 These subscales evaluate Social Information Processing (the ability to interpret social cues), Social Skills (effectiveness in social interactions), and Social Awareness (understanding others’ emotions and perspectives). The items are rated on a 5-point Likert scale (from “Doesn’t describe me at all” to “Describes me very well”), with higher scores indicating greater social intelligence. 10 items are reverse-scored. The Arabic version demonstrated strong internal consistency, with Cronbach’s alpha ranging from 0.86 to 0.90 across the subscales. It also exhibited good test-retest reliability, with Intraclass Correlation Coefficients (ICC) between 0.84 and 0.91, and the factor analysis confirmed the scale’s validity with good model fit (CFI = 0.96, RMSEA = 0.08). Additionally, the overall Cronbach’s alpha of 0.89 in this study further supports the tool’s excellent reliability, confirming its consistency across different samples and contexts.
Assessment of Concerning Behavior Scale (ACB)
The Assessment of Concerning Behavior (ACB) is a tool used to assess mental health challenges and problematic behaviors in children and adolescents with ASD. Initially developed by Tarver et al (2021),34 the ACB was later validated for use in Iran by Mohammadi et al (2023).35 The scale includes 35 items divided into two subscales: Internalizing Problems (19 items) and Externalizing Problems (16 items). Internalizing problems involve inward-directed behaviors like anxiety, depression, withdrawal, and emotional distress. In contrast, externalizing problems relate to outward-directed behaviors, such as aggression, hyperactivity, impulsivity, and defiance, which are more evident in social interactions. Each item is rated on a five-point Likert scale ranging from 1 (never true) to 5 (always true), with higher scores reflecting a higher level of concerning behaviors. The psychometric analysis by Mohammadi et al (2023) confirmed the scale’s strong validity and reliability.35 Confirmatory factor analysis supported a two-factor structure with significant factor loadings (p < 0.05), and positive correlations with the Aberrant Behavior Checklist established its concurrent validity. The scale’s internal consistency was confirmed with Cronbach’s alpha coefficients exceeding 0.70 for the subscales, while the overall Cronbach’s alpha was reported as 0.88, indicating high reliability.
Additionally, the test-retest reliability was reported as 0.91, demonstrating the stability of the scale over time. In the present study, the Arabic version demonstrated strong internal consistency, with a Cronbach’s alpha of 0.91. Factor loadings ranged from 0.58 to 0.85, increasing to 0.70 to 0.90 following varimax rotation, which explained 74.2% of the total variance. The Kaiser-Meyer-Olkin (KMO) value was 0.926, and Bartlett’s test of sphericity yielded significant results (p ≤ 0.001), indicating the adequacy of the data for factor analysis. All items were preserved.
Study Procedures
Tool Preparation & Pilot Study
The research instruments, including the Assessment of Concerning Behavior (ACB) scale, were translated into Arabic by bilingual professionals fluent in both English and Arabic. The translation process prioritized both linguistic accuracy and cultural relevance. To verify that the translated version retained the intended meaning, a separate group of bilingual experts conducted a back-translation into English. This step enabled the identification of discrepancies and ensured conceptual equivalence with the original version. Face validity was subsequently evaluated by a panel of six specialists, three in Community Health Nursing and three in Psychiatric and Mental Health Nursing, who reviewed the translated tools for accuracy, conceptual alignment, and suitability for the target population. Feedback was also obtained from a small group of potential participants to further assess clarity, relevance, and cultural appropriateness, ensuring the instrument’s applicability within the Arabic-speaking context.
Reliability testing was performed using Cronbach’s alpha to determine internal consistency. A pilot study was conducted with 30 parents of children with autism to evaluate the clarity, relevance, reliability, and practicality of the instruments. The pilot was carried out in a setting similar to that of the main study, with the research team monitoring completion times, participant engagement, and potential signs of fatigue or confusion. After completing the instruments, participants took part in structured interviews to provide feedback on language clarity, cultural suitability, and comprehensibility. Data from the pilot were analyzed to examine item performance and internal consistency, with results showing high reliability. As no changes were required, the instruments were finalized for the main study. To avoid duplication and bias, pilot participants were excluded from subsequent data collection. Overall, the pilot study confirmed that the translated tools were linguistically accurate, culturally appropriate, and methodologically sound for full-scale use.
Data Collection
Data for this study were collected from March to May 2025 using a convenience sampling method, in which parents of children with autism attending the outpatient clinic were invited to participate based on their availability and willingness. The researchers clearly explained the purpose and objectives of the study to all participants, ensuring they fully understood their role and the aims of the research. Both oral and written informed consent were obtained prior to participation, confirming that parents voluntarily agreed to take part and were aware of their rights and the study procedures. Participation was strictly voluntary and anonymous, with strong assurances of confidentiality to protect participants’ personal information and responses, which were used solely for research purposes.
Structured interviews with parents of autistic children were conducted in the outpatient clinic waiting area, during which the study questionnaires were administered. Each interview lasted about 25 to 35 minutes. These interviews were scheduled on Monday and Thursday between 9:00 AM and 2:00 PM to fit parents’ schedules and minimize disruption to their daily routines. This consistent scheduling helped ensure reliability in data collection and enabled more accurate comparisons across participants.
Ethical Considerations
Ethical approval for this study was obtained from the Research Ethics Committee of the Faculty of Nursing, Port Said University, Egypt (IRB: NUR (2/3/2025 (45)). The study complied with all relevant local laws and regulations, as well as the ethical principles set forth in the Declaration of Helsinki (DoH, Oct, 2008), to ensure full protection of participants’ rights and well-being. All participants received clear and detailed information about the study’s purpose and were informed that their participation was entirely voluntary and anonymous. They were assured that the information collected would remain strictly confidential and accessible only to the authorized research team. Prior to data collection, written informed consent was secured from each participant, and they were made aware of their right to withdraw from the study at any point without any negative consequences.
Statistical Analysis
The data analysis for this study was conducted using the Statistical Package for the Social Sciences (SPSS) version 25. Prior to conducting the main analyses, the normality of the distribution for all continuous variables (parental resilience, social intelligence, and child behavioral outcomes) was assessed using the Shapiro–Wilk test. The results indicated that the data for these variables did not significantly deviate from a normal distribution (p >0.05), supporting the use of parametric statistical tests. Descriptive statistics, including means, standard deviations, frequencies, and percentages, were calculated to summarize the demographic characteristics of the participants and the primary study variables. To examine the relationships between parental psychological resources (resilience and social intelligence) and child behavioral outcomes (internalizing problems, externalizing problems, and total concerning behavior), Pearson’s correlation coefficients were computed. A multiple linear regression analysis was performed to determine the extent to which parental resilience and social intelligence predict total concerning behavior in children, with model assumptions checked. Finally, a mediation analysis was conducted using the PROCESS macro (Model 4) to test whether social intelligence mediates the relationship between parental resilience and child concerning behavior. The significance of the indirect effect was assessed using the Sobel test. For all inferential tests, the threshold for statistical significance was set at p <0.05.
Results
The mean score for Concerning Behavior was 119.01 (SD = 7.33), while Internalizing Problems averaged 60.37 (SD = 4.01) and Externalizing Problems averaged 58.64 (SD = 4.91). Social Intelligence had a mean of 43.33 (SD = 16.35), and Resilience averaged 17.72 (SD = 2.91), as shown in Table 3.
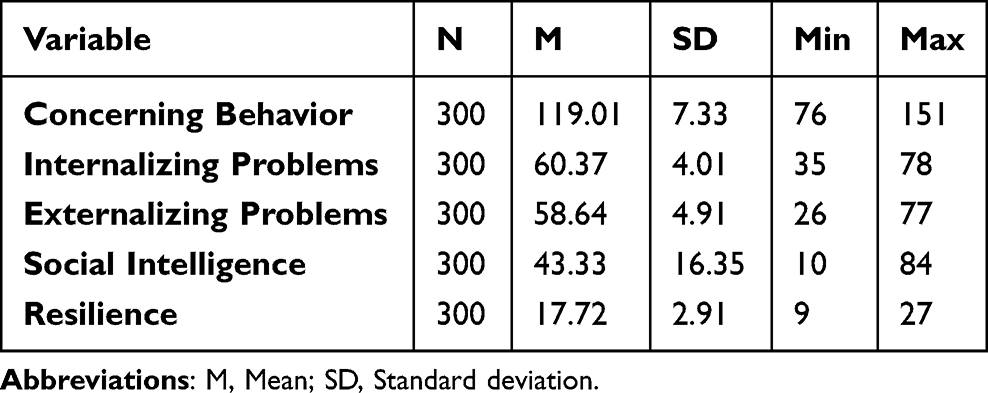 |
Table 3 Means and Standard Deviations of Study Variables (N = 300) |
Parental resilience was significantly negatively correlated with children’s internalizing problems (r = −0.38, p <0.001), externalizing problems (r = −0.23, p <0.001), and total concerning behavior (r = −0.36, p <0.001). Similarly, parental social intelligence showed significant negative associations with internalizing problems (r = −0.33, p <0.001), externalizing problems (r = −0.27, p <0.001), and total concerning behavior (r = −0.36, p <0.001), indicating protective effects of parental psychological resources, as shown in Table 4.
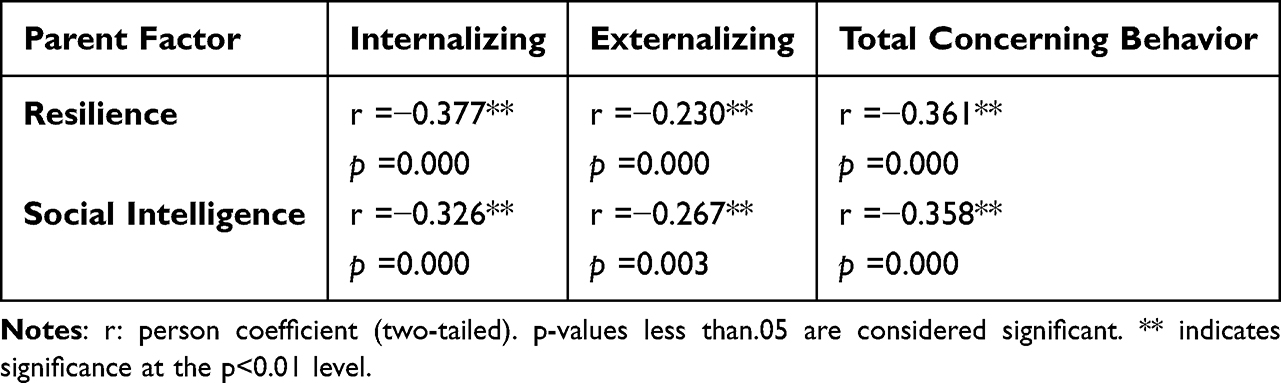 |
Table 4 Pearson Correlations Between Parental Psychological Resources and Child Behavioral Outcomes (n = 300) |
A multiple linear regression analysis was conducted to examine whether parental resilience and social intelligence predict total concerning behavior while controlling for child age, level of needs, parental income, and participation in rehabilitation programs (N = 300). The overall model was statistically significant and explained 25.8% of the variance in concerning behavior (R2 =0.258, F (6, 293) = 16.98, p <0.001, Cohen’s f2 =0.35. Parental resilience (B = −0.74, β = −0.29, t = −5.62, p <0.001, partial R2 =0.097) and social intelligence (B = −0.13, β = −0.29, t = −5.55, p <0.001, partial R2 =0.095) remained significant negative predictors of concerning behavior. Among the control variables, parental income was also a significant predictor (B = −6.42, β = −0.21, t = −4.06, p <0.001, partial R2 =0.053), whereas child age, level of needs, and participation in rehabilitation programs were not statistically significant. Variance inflation factor (VIF) values ranged from 1.02 to 1.07, indicating no evidence of multicollinearity, as shown in Table 5.
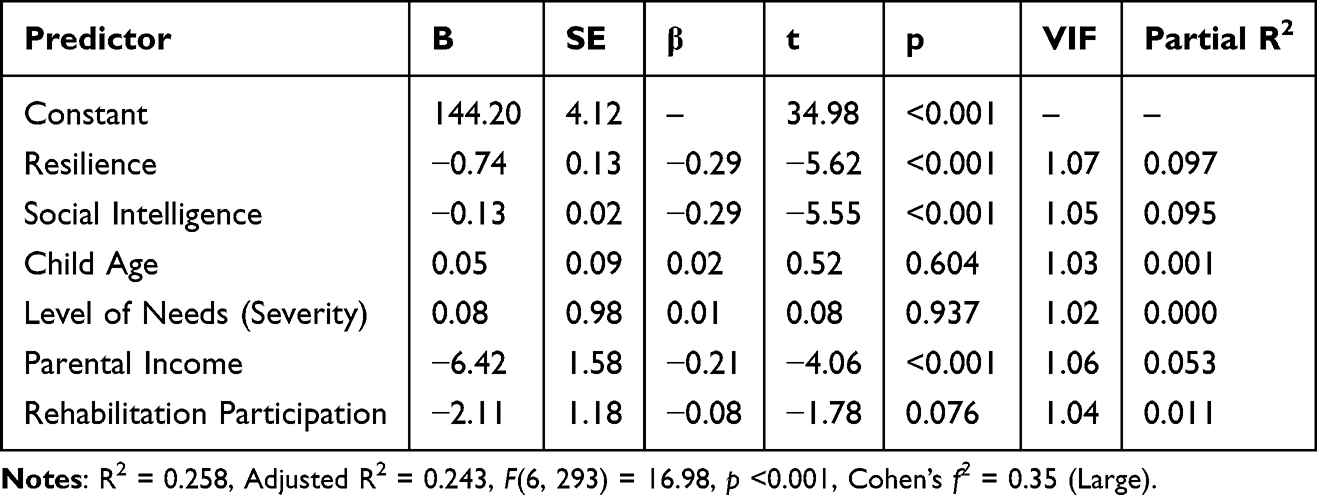 |
Table 5 Linear Regression Analysis Predicting Child Concerning Behavior from Parental Resources |
A mediation analysis tested whether parental social intelligence mediates the relationship between resilience and children’s total concerning behavior. The total effect of resilience on behavior was significant (B = −0.91, p <0.001). Resilience significantly predicted social intelligence (path a: B = 1.17, p <0.001), and social intelligence significantly predicted behavior, controlling for resilience (path b: B = −0.13, p <0.001). The direct effect remained significant (B = −0.75, p <0.001), but the indirect effect was also significant (a×b = −0.16, Sobel z = −3.08, p =0.002). Social intelligence partially mediates 17.1% of resilience’s protective effect on child behavior, as presented in Table 6 and Figure 2.
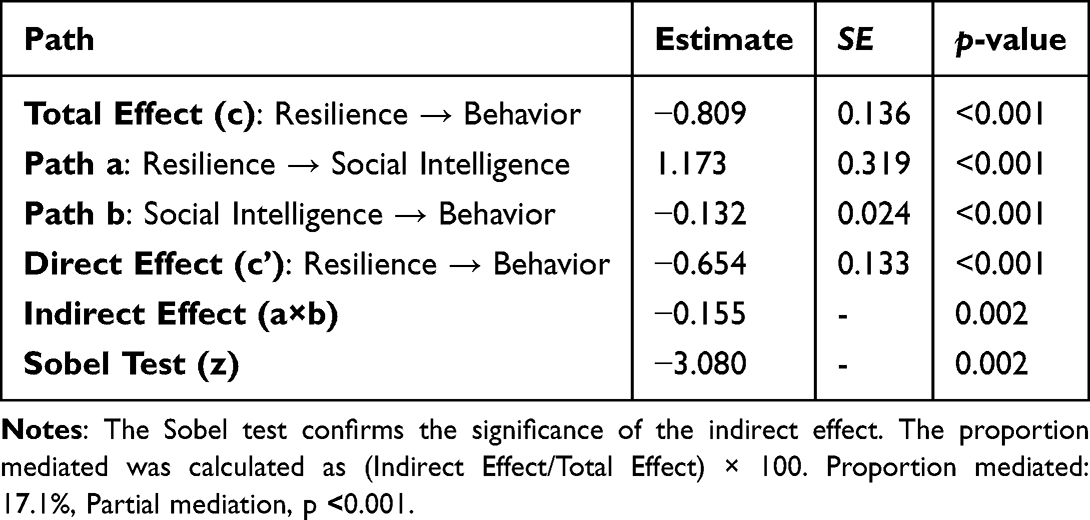 |
Table 6 Mediation Analysis of Social Intelligence in the Relationship Between Parental Resilience and Child Concerning Behavior (n=300) |
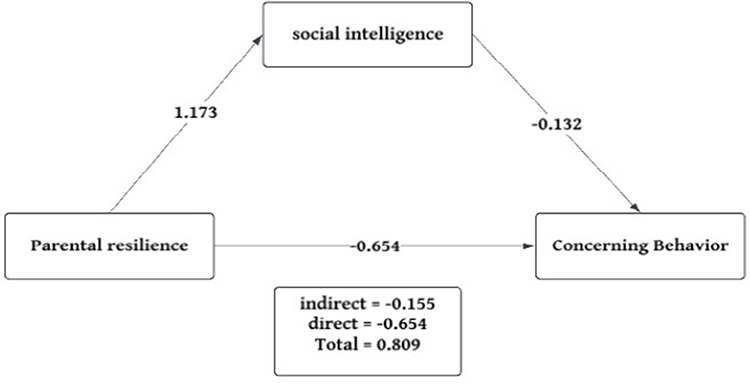 |
Figure 2 Mediation model showing the direct and indirect effects of parental resilience on children’s concerning behaviors through social intelligence. Values represent unstandardized regression coefficients (B). p <0.001. |
Discussion
Understanding the influence of parental factors is vital for effectively managing behavioral challenges in autistic children. This study aims to explore the roles of parental resilience and social intelligence in shaping concerning behaviors among autistic children. By analyzing the interaction between these two factors, the research aims to shed light on their effects on child behavior, ultimately informing strategies to enhance parental skills and improve outcomes for children on the autism spectrum.
The current findings provide an overview of children’s worrisome behaviors as well as the psychological resources (resilience) and social skills-related capacity (social intelligence) of parents. Overall, children’s scores show that concerning behaviors are present at a substantive level, with both internalizing and externalizing dimensions represented in the sample. This is consistent with previous research demonstrating that emotional and behavioral difficulties, rather than just social-communication difficulties, are frequently associated with autism.36 At the same time, the parent-level measures suggest meaningful variability in resilience and social intelligence across participants, supporting the idea that parental psychological resources and social competence are not uniform and may therefore account for differences in child outcomes in a way that is consistent with protective-factor models used in autism research.37
Importantly, the particular cultural and socioeconomic background of the sample should be taken into consideration when interpreting these results. Mothers who lived in rural Egypt and were mostly unemployed or homemakers with low incomes made up the bulk of participants. Parental resilience and social intelligence may be actively shaped by these contextual elements, which go beyond simple background traits. The difficulty of providing care may be increased in rural Egyptian settings due to limited access to specialist services, transportation issues, and financial limitations. This can lead to increased stress and the need to build adaptive coping mechanisms (resilience).6 At the same time, strong kinship networks and extended family systems common in these communities may provide informal social support, which can enhance aspects of social intelligence such as interpersonal awareness and relationship management.37 However, traditional gender roles that position mothers as primary caregivers may also increase psychological pressure and limit opportunities for broader social engagement, potentially constraining the development or expression of social intelligence in formal systems such as healthcare and education.38
From a clinical standpoint, these descriptive patterns offer a justification for examining the direct and indirect relationships between children’s worrisome behaviors and parental resilience/social intelligence. Parental resources may help buffer stress and support more adaptive family functioning if children exhibit elevated internalizing and externalizing difficulties while parents differ in resilience and social intelligence, mechanisms that have been highlighted across multiple strands of autism research.24,39 For example, studies have linked parental resilience and related protective variables with improved child or family outcomes in autism,40,41 and other research has reported that socially intelligent and resourceful caregivers are more likely to manage complex situations and advocate effectively, which can reduce the likelihood or severity of concerning behaviors.42
Importantly, the results also suggest that interventions aimed at improving parental resilience and social intelligence should be translated into concrete, accessible caregiver supports. In practical terms, resilience-focused components may include structured coaching in coping, emotion regulation, problem-solving, and stress-management strategies, while social intelligence-focused components may include skill-building for interpreting social cues, improving communication with professionals and schools, and using collaborative strategies for managing day-to-day interaction demands.43 To maximize caregiver benefit, delivery should consider barriers to access (eg., time constraints, transportation, cost, and competing caregiving demands), using flexible formats such as hybrid or virtual sessions, brief modular content, and culturally responsive materials.44
In the Egyptian context, such interventions should be particularly sensitive to socioeconomic constraints and cultural norms. For example, low-income rural mothers may have limited time, mobility, or financial resources to attend in-person programs, highlighting the importance of community-based or home-delivered interventions. Additionally, leveraging existing informal support systems, such as extended family networks or community groups, may enhance intervention uptake and sustainability.38 Cultural expectations regarding motherhood and caregiving should also be considered when designing programs, ensuring that interventions empower mothers without increasing perceived burden or stigma.
Given that autism has a genetic component, some parents may themselves experience social-communication differences that influence how they interpret social information, communicate needs, and navigate support systems.45 Therefore, interventions should not assume uniform baseline social competence; instead, social intelligence training may need to be individualized, more explicit, and practice-based (eg., using concrete communication scripts, role-play, and structured feedback).
The findings show that fewer concerning child behaviors, including internalizing difficulties, externalizing problems, and overall concerning behavior, are substantially correlated with stronger parental resilience and social intelligence. The protective role of parents’ psychological and interpersonal resources in families affected by ASD is supported by these inverse relationships, which imply that children may experience a more supportive and responsive environment that lessens emotional distress and disruptive behavioral patterns when caregivers are better able to manage social demands (social intelligence) and adapt to adversity (resilience). This pattern aligns with more general findings in the literature on autism.43,44
Notably, within this socioeconomically disadvantaged sample, the protective effects of resilience and social intelligence may be particularly salient. In contexts where formal resources are limited, internal psychological strengths and interpersonal competencies may compensate for structural deficits, allowing parents to better navigate challenges and support their children despite environmental constraints.46 The current results also reveal that, after controlling for child age, severity/level of needs, parental income, and participation in rehabilitation, both parental resilience and parental social intelligence remain significant predictors of children’s total concerning behavior. The negative standardized coefficients indicate that higher caregiver resources are associated with lower levels of child difficulties, suggesting that protective parental factors operate even when relevant contextual and clinical variables are held constant.47
Regarding the covariates, only parental income shows a significant association in the regression model, while child age, level of needs (severity), and rehabilitation participation do not reach statistical significance. This finding further underscores the role of socioeconomic conditions, suggesting that financial strain may directly or indirectly exacerbate caregiving stress and limit access to supportive resources, thereby influencing child behavioral outcomes.36 Overall, the results support a dual-focus framework for intervention: programs that build resilience and social intelligence may be especially valuable for reducing child concerning behaviors in ASD. This aligns with prior research linking parental protective resources to improved outcomes.46,48–52
The findings of the study show that the relationship between parental resilience and children’s worrisome behaviors is partially mediated by parental social intelligence. In particular, resilience is linked to greater social intelligence, which is linked to fewer problematic behaviors. This implies that social intelligence converts resilience’s psychological ability to manage stress into efficient social functioning. This mediation pathway may show how resilient parents use the social institutions that are available to them, including community networks or extended family support, to better handle the demands of caring within the cultural setting of this study.43,53–55 Thus, social intelligence may represent the mechanism through which resilience is operationalized in real-world, culturally embedded interactions. The mediation model also highlights that resilience-based interventions alone may be insufficient without strengthening social intelligence. A dual-focus approach is therefore recommended.
Future research should investigate whether parental resilience and social intelligence differentially relate to internalizing versus externalizing behaviors. Additionally, future studies should explicitly examine how cultural norms, gender roles, and socioeconomic inequalities interact with parental psychological resources to influence child outcomes, particularly in low- and middle-income countries.
Limitations
Several methodological limitations should be considered when interpreting the findings of this study, though each suggests clear directions for future research. The cross-sectional design precludes causal inference, as all variables were measured at a single time point, making it impossible to establish temporal precedence or rule out bidirectional relationships, such as the possibility that severe child behavioral problems erode parental resilience over time, yet this limitation can be addressed in future studies through longitudinal designs that track parents and children over multiple time points to clarify directionality. Convenience sampling from a single outpatient clinic in Egypt limits generalizability and introduces selection bias, but subsequent research should employ probability sampling across multiple sites, including both urban and rural settings, to enhance representativeness. The sample was demographically homogeneous, predominantly comprising low-income, rural, unemployed mothers, which underrepresented fathers, urban residents, and higher-income families; therefore, future investigations should intentionally recruit diverse participant groups to examine whether findings hold across different familial structures and socioeconomic strata. The reliance on single-informant self-report measures for all constructs introduced shared method variance and susceptibility to social desirability bias, potentially inflating observed correlations, a limitation that can be mitigated in future studies by incorporating multi-informant approaches, such as partner reports, teacher evaluations, and direct observational measures of child behavior. Additionally, while a formal ASD diagnosis was required for inclusion, the study did not independently verify diagnostic accuracy or severity using standardized instruments such as the Autism Diagnostic Observation Schedule, highlighting the need for future research to employ objective diagnostic tools to ensure clinical homogeneity. Data collection in a semi-public outpatient waiting area may have compromised privacy and encouraged underreporting of sensitive information, suggesting that future studies should prioritize private, confidential settings to foster honest disclosure. Although key covariates, child age, level of needs, parental income, and rehabilitation participation, were controlled in the regression analysis, other potentially important confounders, including ASD symptom severity, co-occurring medical or psychiatric conditions, marital dynamics, quality of rehabilitation services, and informal social support, were not measured, underscoring the value of comprehensive covariate assessment in future investigations.
Conclusion
This study examined the associations between parental resilience, social intelligence, and behavioral outcomes in autistic children within an Egyptian context. The findings indicate that higher levels of parental resilience and social intelligence are each associated with fewer internalizing and externalizing behaviors in children. Mediation analysis revealed that social intelligence partially accounted for the association between resilience and child behavior, suggesting that these two parental resources are interrelated in ways that may influence caregiving outcomes. Interventions designed to strengthen these capacities, for example, through coping skills training, emotion regulation strategies, and communication skill development, may offer complementary pathways for supporting families.
Clinical Implications
Nurses are often at the forefront of supporting families of autistic children, and this research provides a clear framework for enhancing that support. First, nurses should integrate the assessment of parental resilience and social intelligence into routine family-centered care, moving beyond a sole focus on the child’s symptoms to evaluate the psychological resources of the primary caregivers. This holistic assessment allows for the early identification of parents who may be experiencing significant stress or feeling ill-equipped to navigate complex systems, enabling timely and targeted intervention. Based on this assessment, nurses can develop and implement psychoeducational interventions and skill-building workshops designed to bolster these specific parental resources. For instance, nurses can lead support groups that teach resilience-building strategies, such as cognitive reframing, stress management techniques, and self-care practices, while concurrently fostering social intelligence through role-playing, communication skills training, and guidance on how to effectively advocate within educational and healthcare systems.
Furthermore, nurses are uniquely positioned to act as case managers and system navigators, actively connecting families to essential resources, facilitating support networks with other parents, and modelling socially intelligent behaviours during interactions. By adopting this dual-focused approach that empowers parents both internally (through resilience) and externally (through social intelligence), nurses can help create more stable, supportive, and effective caregiving environments. This, in turn, can mitigate child behavioural challenges, reduce overall family stress, and promote better long-term outcomes for both the autistic child and their parents, ultimately translating research into tangible, compassionate, and effective clinical practice.
Data Sharing Statement
Data can be obtained from the corresponding author upon a reasonable request.
Ethical Approval
Ethical approval for this study was received from the Research Ethics Committee of the Faculty of Nursing at Port Said University, Egypt (IRB: NUR (2/3/2025 (45)). The study adhered to all applicable local laws and regulations, as well as the ethical principles outlined in the Declaration of Helsinki (DoH, Oct, 2008), to ensure the full protection of participants’ rights and well-being.
Informed Consent Statement
Each participant gave their informed written consent. They were assured that their participation was completely voluntary and that they could withdraw at any point without any negative consequences. The privacy of the information gathered was rigorously upheld.
Acknowledgments
The authors express their gratitude to all the parents who consented to participate in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (APC-QU-2026).
Disclosure
The authors declare no conflict of interest.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Solmi M, Firth J, Miola A, et al. The prevalence of autism spectrum disorder in global populations: a comprehensive review. Psychol Med. 2022;52(3):1–15. doi:10.1038/s41380-022-01630-7
3. Salari N, Rasoulpoor S, Shohaimi S, et al. The global prevalence of autism spectrum disorder: a comprehensive meta-analysis. Iran J Psychiatry Behav Sci. 2022;16(2):1–12. doi:10.1186/s13052-022-01310-w
4. Baio J, Wiggins L, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill Summ. 2018;67(6):1–23. doi:10.15585/mmwr.ss6706a1
5. Maenner MJ, Warren Z, Williams AR, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveill Summ. 2023;72(2):1–14. doi:10.15585/mmwr.ss7202a1
6. Yousef AM, Roshdy EH, Abdel Fattah NR, Said RM. Prevalence and risk factors of autism spectrum disorders in preschool children in Sharkia, Egypt: a community-based study. Middle East Curr Psychiatry. 2021;28(1):1–9. doi:10.1186/s43045-021-00114-8
7. Metwally AM, Helmy MA, Salah El-Din EM, et al. National screening for Egyptian children aged 1 year up to 12 years at high risk of Autism and its determinants: a step for determining what ASD surveillance needs. BMC Psychiatry. 2023;23(1):471. doi:10.1186/s12888-023-04977-5
8. Meguid NA, Mohamed M, Shawky RM. Autism spectrum disorder in Egyptian children: prevalence and associated factors. Egypt J Otolaryngol. 2023;39(1):1–7.
9. Ibrahim N, El-abdeen AMZ, Ng F, Zoromba M, Haikal A. Socio-economic and demographic factors associated with adaptive behavior among children diagnosed with an autism spectrum disorder in Egypt. Middle East Curr Psychiatry. 2020;27.
10. Kurzius-Spencer M, Pettygrove S, Christensen D, et al. Behavioral problems in children with autism spectrum disorder with and without co-occurring intellectual disability. Res Autism Spectr Disord. 2018;56:61–71. doi:10.1016/j.rasd.2018.09.002
11. Alhuzimi T. Stress and emotional wellbeing of parents due to change in routine for children with autism spectrum disorder (ASD) at home during COVID-19 pandemic in Saudi Arabia. Res Develop Disabilities. 2021;108:103822. doi:10.1016/j.ridd.2020.103822
12. Ilias K, Cornish K, Park MS-A, Toran H, Golden KJ. Risk and resilience among mothers and fathers of primary school age children with ASD in Malaysia: a qualitative constructive grounded theory approach. Front Psychol. 2019;9:2275. doi:10.3389/fpsyg.2018.02275
13. Pepperell TA, Paynter J, Gilmore L. Social support and coping strategies of parents raising a child with autism spectrum disorder. Early Child Dev Care. 2018;188(10):1392–1404. doi:10.1080/03004430.2016.1261338
14. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/1467-8624.00164
15. Abate BB, Sendekie AK, Tadesse AW, et al. Resilience after adversity: an umbrella review of adversity protective factors and resilience-promoting interventions. Front Psychiatry. 2024;15:1391312. doi:10.3389/fpsyt.2024.1391312
16. Kuldas S, Foody M. Neither resiliency-trait nor resilience-state: transactional resiliency/e. Youth Society. 2022;54(8):1352–1376. doi:10.1177/0044118X211029309
17. Fullerton DJ, Zhang LM, Kleitman S, Sudzina F. An integrative process model of resilience in an academic context: resilience resources, coping strategies, and positive adaptation. PLoS One. 2021;16(2):e0246000. doi:10.1371/journal.pone.0246000
18. McDorman SA, Taylor-Robinette EK, Romeo RR. Risk and resilience models in child development. Adv Child Dev Behav. 2024;67:133.
19. Powell KM, Rahm-Knigge RL, Conner BT. Resilience protective factors checklist (RPFC): buffering childhood adversity and promoting positive outcomes. Psychol Rep. 2021;124(4):1437–1461. doi:10.1177/0033294120950288
20. Zhao M, Fu W. The resilience of parents who have children with autism spectrum disorder in China: a social culture perspective. Int J Develop Disabilities. 2022;68(2):207–218. doi:10.1080/20473869.2020.1747761
21. Dey NEY, Amponsah B. Sources of perceived social support on resilience amongst parents raising children with special needs in Ghana. Heliyon. 2020;6(11):e05569. doi:10.1016/j.heliyon.2020.e05569
22. Fong V, Gardiner E, Iarocci G. Satisfaction with informal supports predicts resilience in families of children with autism spectrum disorder. Autism. 2021;25(2):452–463. doi:10.1177/1362361320962677
23. Silberman ML, Hansburg F. PeopleSmart: Developing Your Interpersonal Intelligence. San Francisco, CA: Berrett-Koehler Publishers; 2000.
24. Bhagat V, Joash J, Haque M. Parents’ self-efficacy, emotionality, and intellectual ability impacting the intervention of autism spectrum disorders: a review proposed model for appraisal of intervention. Int J Pharm Pharm Sci. 2015;7(11):7–12.
25. Mihus I, Nakonechna N. The role of communicative competence in the structure of social intelligence of teachers of higher education institutions. Public Adm Law Rev. 2022;(4):75–86.
26. Nazemi M, Niazazari K, Jabari N. Modeling the impact of social intelligence on teachers’ quality of life by explaining the role of risk management. Iranian J Educ Sociolog. 2019;2(3):158–166. doi:10.29252/ijes.2.3.158
27. Anchesi SD, Corallo F, Di Cara M, et al. Autism and ADHD: a literature review regarding their impacts on parental divorce. Children. 2023;10(3):438. doi:10.3390/children10030438
28. Gabra RH, Hashem DF, Ahmed GK. The possible relation between stigma, parent psychiatric symptoms, quality of life and the disease burden in families of children with autism spectrum disorder in Egypt: a multicentre study. Egyptian J Neurol Psychiatry Neurosurg. 2021;57(1):170. doi:10.1186/s41983-021-00426-w
29. Cohen L, Manion L, Morrison K. Statistical significance, effect size and statistical power. In: Research Methods in Education.
30. Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. doi:10.1080/10705500802222972
31. Baattaiah BA, Alharbi MD, Khan F, Aldhahi MI. Translation and population-based validation of the Arabic version of the brief resilience scale. Ann Med. 2023;55(1):2230887. doi:10.1080/07853890.2023.2230887
32. Silvera D, Martinussen M, Dahl TI. The Tromsø social intelligence scale, a self-report measure of social intelligence. Scand J Psychol. 2001;42(4):313–319. doi:10.1111/1467-9450.00242
33. Chater W, Rebhi M, Saidane M, Guelmami N, Bouassida A. Reliability and validity of the Tromso social intelligence scale (TSIS). Adv Phys Educ. 2023;13(1):53–65. doi:10.4236/ape.2023.131006
34. Tarver J, Vitoratou S, Mastroianni M, et al. Development and psychometric properties of a new questionnaire to assess mental health and concerning behaviors in children and young people with autism spectrum disorder (ASD): the assessment of concerning behavior (ACB) scale. J Autism Dev Disord. 2021;51(8):2812–2828. doi:10.1007/s10803-020-04748-1
35. Mohammadi K, Samavi A, Mehdiabadi FZ, Samavi SA. Psychometric validation of concerning behavior scale in Iranian children and young people with autism spectrum disorder. Front Psychiatry. 2023;14:1153112. doi:10.3389/fpsyt.2023.1153112
36. Restoy D, Oriol-Escudé M, Alonzo-Castillo T, et al. Emotion regulation and emotion dysregulation in children and adolescents with autism spectrum disorder: a meta-analysis of evaluation and intervention studies. Clin Psychol Rev. 2024;109:102410. doi:10.1016/j.cpr.2024.102410
37. Nguyen TMH, Khuu DT, Nguyen TAN, Nguyen TP. Understanding the link between parental stress and child autism spectrum disorder symptoms: insights from Vietnam. Research in Autism. 2025;125:202627. doi:10.1016/j.reia.2025.202627
38. Mohammed AA, Abd El-Naser AE, Hashem MM. The impact and relation of different socio-demographic variables on social support among parents of children with autism spectrum disorder. Assiut Sci Nurs J. 2025;13(49):91–99. doi:10.21608/asnj.2025.347363.1976
39. El-Monshed AH, Amr M. Perceived stress among mothers of children with autism spectrum disorder in Egypt. Adv Autism. 2021;7(4):335–344. doi:10.1108/AIA-02-2020-0014
40. Gharaibeh M, Ayasrah MN, Al-Rousan AH, Khasawneh YJA, Khasawneh MAS. Parental stress and coping in autism spectrum disorder: a network analysis of internalizing and externalizing symptoms in children with autism spectrum disorder. Clin Psychol Psychother. 2025;32(3):e70100. doi:10.1002/cpp.70100
41. Flores-Buils R, Andrés-Roqueta C. Factors influencing resilience of parents with children with neurodevelopmental disorders: the role of structural language, social cognition, and social support. Front Psychiatry. 2022;13:886590. doi:10.3389/fpsyt.2022.886590
42. Papadopoulos D. Mothers’ experiences and challenges raising a child with autism spectrum disorder: a qualitative study. Brain Sci. 2021;11(3):309. doi:10.3390/brainsci11030309
43. Carlier S, Van der Paelt S, Ongenae F, De Backere F, De Turck F. Empowering children with ASD and their parents: design of a serious game for anxiety and stress reduction. Sensors. 2020;20(4):966. doi:10.3390/s20040966
44. Ghanouni P, Eves L. Resilience among parents and children with autism spectrum disorder. Ment Illn. 2023;2023(1):2925530. doi:10.1155/2023/2925530
45. Nagy SS, Sayied NE, Saber EH, Kotb FN. Impact of strengthening resilience training program on parents and communication skills of their children with autism spectrum disorder. Minia Sci Nurs J. 2024;16(2):114–132.
46. Klitzman R, Bezborodko E, Chung WK, Appelbaum PS. Impact of receiving genetic diagnoses on parents’ perceptions of their children with autism and intellectual disability. J Autism Dev Disord. 2025;55(1):284–296. doi:10.1007/s10803-023-06195-0
47. Vess SF, Campbell JM. Parent–child interaction therapy (PCIT) with families of children with autism spectrum disorder. Autism Develop Language Impairm. 2022;7:23969415221140707. doi:10.1177/23969415221140707
48. Higgins L, Mannion A, Chen JL, Leader G. Adaptation of parents raising a child with ASD: the role of positive perceptions, coping, self-efficacy, and social support. J Autism Dev Disord. 2023;53(3):1224–1242. doi:10.1007/s10803-022-05537-8
49. Smith-Young J, Chafe R, Audas R, Gustafson DL. I know how to advocate: parents’ experiences in advocating for children and youth diagnosed with autism spectrum disorder. Health Services Insights. 2022;15:11786329221078803. doi:10.1177/11786329221078803
50. Buchholz AA. Correlation between resilience and social support in mothers of young children with autism. Polish perspective. Health Psychology Report. 2023;11(1):10. doi:10.5114/hpr/151607
51. Galán-Vera IZ, Robles-Bello MA, Sarhani-Robles A, Valencia-Naranjo N. Experiences and coping strategies of parents with children diagnosed with autism spectrum disorder in early care with emphasis on social skills and family cultural values: a qualitative study. Arch Psychiatric Nurs. 2025;56:151864. doi:10.1016/j.apnu.2025.151864
52. García-García L, Martí-Vilar M, Hidalgo-Fuentes S, Cabedo-Peris J. Enhancing emotional intelligence in autism spectrum disorder through intervention: a systematic review. Eur J Investig Health Psychol Educ. 2025;15(3):33. doi:10.3390/ejihpe15030033
53. Hsiao Y-J. Parental stress, family resilience, and health-related quality of life: parents of children with autism spectrum disorder. Curr Psychol. 2024;43(39):31019–31026. doi:10.1007/s12144-024-06687-x
54. Ramadan Ragab Ahmed N, Haggag Soleiman M, Ahmed AbuElEla L, Abo Elsoud Ahmed H. Burden on caregivers of children with autism spectrum disorder in El-Beheira governorate. Egypt J Health Care. 2023;14(4):724–740. doi:10.21608/ejhc.2023.331413
55. Schwartzman JM, Millan ME, Uljarevic M, et al. Resilience intervention for parents of children with autism: findings from a randomized controlled trial of the AMOR Method. J Autism Dev Disord. 2022;52(2):738–757. doi:10.1007/s10803-021-04977-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Explorative Study of Affiliate Stigma, Resilience, and Quality of Life Among Parents of Children with Autism Spectrum Disorder (ASD)

Salleh NS, Tang LY, Jayanath S, Lim Abdullah K
Journal of Multidisciplinary Healthcare 2022, 15:2053-2066
Published Date: 13 September 2022
Emotional Intelligence and Resilience Outcomes in Adolescent Period, is Knowledge Really Strength?
Collado-Soler R, Trigueros R, Aguilar-Parra JM, Navarro N
Psychology Research and Behavior Management 2023, 16:1365-1378
Published Date: 22 April 2023
Mediating Role of Emotional Intelligence in the Relationship Between Resilience and Academic Engagement in Adolescents: Differences Between Men and Women
Tortosa Martínez BM, Pérez-Fuentes MDC, Molero Jurado MDM
Psychology Research and Behavior Management 2023, 16:2721-2733
Published Date: 18 July 2023
Evaluating Parents’ Concerns, Needs, and Levels of Satisfaction with the Services Provided for ASD Children in Saudi Arabia
Al Awaji NN, Al-Taleb SM, Albagawi TO, Alshammari MT, Sharar FA, Mortada EM
Journal of Multidisciplinary Healthcare 2024, 17:123-146
Published Date: 8 January 2024
Seeking Care for Children with Intellectual and/or Developmental Disabilities in the Emergency Department: A Mixed Methods Systematic Review of Parents’ Experiences and Information Needs
Elliott SA, Rahman S, Scott SD, Craig WR, Knisley L, Shearer K, Hartling L
Open Access Emergency Medicine 2024, 16:117-131
Published Date: 19 June 2024