")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
An Explorative Study of Affiliate Stigma, Resilience, and Quality of Life Among Parents of Children with Autism Spectrum Disorder (ASD)
Authors Salleh NS , Tang LY, Jayanath S , Lim Abdullah K
Received 7 June 2022
Accepted for publication 30 August 2022
Published 13 September 2022 Volume 2022:15 Pages 2053—2066
DOI https://doi.org/10.2147/JMDH.S376869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of "Affiliate stigma, resilience and QoL among parents of children with ASD" [ID 376869].
Views: 194
Noor Shuhada Salleh,1 Li Yoong Tang,1 Subhashini Jayanath,2 Khatijah Lim Abdullah3
1Department of Nursing Science, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 2Developmental Pediatrics Unit, Department of Pediatrics, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 3Department of Nursing, School of Medical and Life Sciences, Sunway University, Petaling Jaya, Malaysia
Correspondence: Li Yoong Tang, Department of Nursing Science, Faculty of Medicine, University of Malaya, Kuala Lumpur, 50603, Malaysia, Tel +6012 9762363, Email [email protected]
Purpose: Children diagnosed with ASD usually have impaired social functions, exhibit repetitive, stereotyped and self-stimulatory behaviors, which make them prone to be stigmatized by the public. However, stigma not only affects those with stigmatization characteristics such as children with ASD but also tends to include other people related to them including parents. This is called affiliate stigma. However, affiliate stigma is unlikely to occur if public awareness is high. Considering that awareness of ASD is still comparatively low in this region and that, as a review of the literature showed, there have been limited studies on stigma and ASD conducted in South-East Asia, particularly in Malaysia, this study is of great significance, especially in the context of the East and other developing countries. The aim of this study was to explore parents’ experiences of caring and perceptions of affiliate stigma, resilience and quality of life (QoL) when caring for a child with ASD.
Methods: This paper is part of the sequential explanatory mixed-methods study in which, after a cross-sectional study of 144 parents, a qualitative approach was used to explore parents’ experiences of caring and their perceptions of affiliate stigma, resilience, and QoL. Participants were recruited when they were accompanying their children to therapy at two tertiary public hospitals in one of the north-eastern states of Malaysia. Eleven parents of children with ASD aged 2– 12 years participated. Qualitative data analysis followed Braun and Clarke’s methodology of thematic analysis.
Results: Four themes were identified: the meaning of QoL, ASD and life adjustment, perceived stigma, and resilience.
Conclusion: This is the first Southeast Asian study on parent-perceived affiliate stigma, resilience, and QoL in the context of ASD. These findings can inform healthcare personnel and policymakers into day-to-day parenting realities and therefore an effort to coordinate support services across all disciplines could be made to improve outcomes for both parents and children.
Keywords: autistic disorder, child, parents, social stigma, quality of life
Introduction
Children diagnosed with autism spectrum disorder (ASD) usually have impaired social functions, exhibit repetitive, stereotyped, and self-stimulatory behavior, and often exhibit a significant delay in the development of verbal interactions.1 Hence, it is estimated that many parents of children with ASD have to face additional issues such as stigma and psychological problems of stress and depression due to their child’s behavior.2,3 This is due to the fact that stigma not only affects those with stigmatization characteristics such as children with ASD, but also tends to include other people related to them including parents and family. These close persons are subject to courtesy stigma, which refers to negative attitudes towards individuals, not due to their own characteristics, but their connections or relationships with other stigmatized individuals.4 Eventually, parents of children with ASD may be affected by the second type of stigma; self-stigma which refers to individuals’ acceptance of social stereotype evaluations and incorporating these ideas into their own value systems.5 Recently, researchers have distinguished between courtesy stigma and the internalization of stigma (self-stigma) by these family members, which is called affiliate stigma.6 Previous studies have found that the impact of affiliate stigma on parents of children with ASD is extreme and relatively more prevalent in an Asian background.2,7,8
In Malaysia, the issue of affiliate stigma should be highlighted for many reasons. Firstly, ASD is not widely known within our society and the stigma of this disorder is widespread.9 Secondly, parents of children with ASD are more likely to internalize stigma. This is because the experience of affiliate stigma is more group attention rather than personal attention, and parents are often stigmatized due to the behavior of the their child or associates rather than themselves.10 Thirdly, culture affects people’s knowledge of and attitude towards ASD.11 Stigma in collectivist cultures, like the one in Malaysia, seems to be more prevalent compared to individualist cultures, like those in many Western countries.12 Finally, awareness of ASD is still comparatively low in the former region and a review of literature has shown that there have been limited studies on stigma and ASD conducted in South-East Asia, particularly in Malaysia.13 Therefore, this study is of great significance, especially in the context of the East and other developing countries.
Although most studies assess the disorder from the perspective of health-related stigma, research also needs to focus on parental adjustment to their parenting situation, especially in the process of internalizing stigma. Nonetheless, research in recent years has not allowed the establishment of a broad theoretical framework concerning the relationship of affiliate stigma, resilience and QoL among parents during the upbringing of a child with ASD. Another reason in support of increased research is that resilience may also represent an important factor in the intervention paradigms for parents of children diagnosed with ASD and their families.14 From the same study, it was found that parents reported a higher level of stress secondary to their child’s difficult behavior, which often led to stigma. However, a lower score of parental distress is related to high resilience.14 This study showed that ASD needs special attention from our society and more research as well as guidance are required to educate the Malaysian society on how this issue of parenting with ASD can be managed by parents.
Moreover, since ASD is a lifelong condition, the negative impact of ASD on parental QoL is undeniable. Measurability of QoL is vital because treatment includes not only reducing ASD symptoms but also improving QoL, in this case of the parents. Since parenting a child with ASD can be a lifelong endeavor, these parents have reported encountering various problems which can lead to poorer QoL.7 Correspondingly, given that it is recognized that parents and families are essential to the well-being of children with ASD, researchers, policymakers, and service providers need to recognize the importance of supporting them and allowing for their involvement in the intervention for their children. This may be one way to improve parents’ QoL,15 especially in Malaysia where currently there is limited support from the public and private sectors in providing more suitable centers and facilities to assist them in their difficult situation.9
As there has been relatively little investigation on the impact of internal parental issues (given that affiliate stigma, resilience, and QoL can affect parents’ personalities or behavior patterns) and the references of the relationships between these three variables are scarce, this study is designed to fill the gap. This study addresses the knowledge gap in parental thoughts on affiliate stigma, resilience, and QoL in the context of ASD. The aim of this study was to explore parental experiences of caring and perceptions of affiliate stigma, resilience, and QoL when caring for a child with ASD. Understanding parental experiences is vital as it can inform healthcare personnel and policymakers and lead to improved outcomes for both parents and children. Thus, open-ended interviews in this study were adopted that allowed researchers to assess parents’ viewpoints which gave rich insights into the upbringing of their children.
Materials and Methods
Study Design
This paper is part of a mixed methods study in which, after a cross-sectional study of 144 parents, a qualitative approach was used to explore parental experiences of caring and perceptions of affiliate stigma, resilience, and QoL. Parents were purposefully selected to be involved in the interviews based on their lower QoL ratings and the study utilized data from these semi-structured interviews which focused on experiences of caring and perceptions of affiliate stigma, resilience, and QoL from a parental perspective.
Recruitment of Participants
This study included 11 parents of children with ASD residing in a north eastern state in Malaysia (Table 1). Participants were recruited using convenience sampling when they accompanied their children for therapy at two of the largest, tertiary public hospitals, namely Hospital Universiti Sains Malaysia (HUSM) and Hospital Raja Perempuan Zainab II (HRPZ II). The selected hospitals were ideal for conducting this study as one is a major teaching hospital (HUSM) and the other is the largest tertiary referral hospital (HRPZ II) in the state, which deals with the highest total of referral cases from the providers of primary and secondary care. Also, both hospitals are located in the central district of the state where the highest population is recorded, which ensured the study would be logistically feasible.
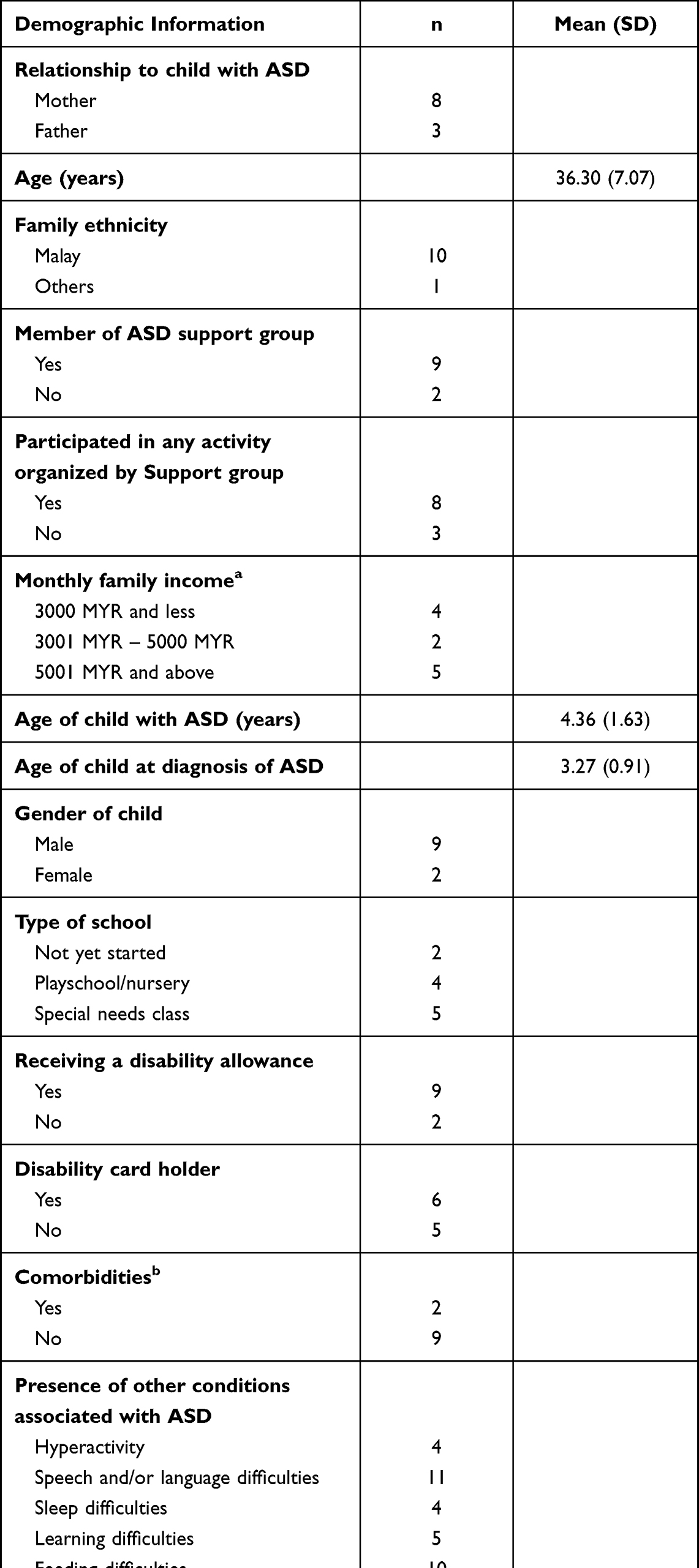 |
Table 1 Parents’ and Child’s Demographic Characteristics (n = 11) |
After the cross-sectional study of 144 parents, a qualitative approach was used to explore parents with a lower QoL based on their QoL ratings on the Quality of Life in Autism-Parent version QoLA-P.16 Higher scores indicate higher perceived QoL, with possible total scores of between 28 and 140. Median scores of ≤ 85 are considered as low QoL and so participants who scored in this range were then purposefully selected to be involved in the interviews. It was appropriate to only include parents with a lower QoL as discovering the reasons for their lower QoL could lead to understanding the issues underpinning the problem and thus provide a basis for further intervention.17,18 In addition, purposive sampling with maximum variability was used to obtain a comprehensive overview of those who had experienced the situation of looking after a child with ASD since it provides a detailed account of their unique experiences, thereby uncovering its core elements.
A sample of parents were recruited who: (a) were primary caregivers for at least one child with a confirmed ASD diagnosis determined by a clinician (psychiatrist or pediatrician), in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria;1 (b) had a major caregiving responsibility and lived in the same residence as the child; (c) had a child with ASD of between two and 12 years old; and (d) were able to read, understand, and communicate in either Malay or English, or both. Exclusionary criteria consisted of parents of children whose ASD diagnosis was not yet confirmed at the time of the study.
Finally, the recruitment was discontinued with the 11th parent when data saturation was reached in the qualitative interviews. This study was conducted in compliance with the Declaration of Helsinki – Version 2000. Written, informed consent for voluntary participation was obtained from each parent, which included publication of anonymized responses. Also, ethical approvals were obtained from the Medical Research Ethics Committee (MREC) University of Malaya Medical Centre (UMMC) (MRECID. No: 2019426–7360), the Human Research Ethics Committee of USM (JEPeM) (USM/JEPeM/19050281), and the National Medical Research Register of Malaysia (NMRR) (NMRR-19-928-47338 (IIR)) prior to study commencement.
The Interviews
Eleven interviews were conducted in total. The researcher developed an interview guide based on a previous literature review, comments of the expert panel, and feedback from the pilot test (Table 2). A pilot study with two face-to-face interviews was conducted to test the interview guide prior to the main study. The first author conducted all interviews and each interview lasted about 60–90 minutes. The study was complicated by the fact that it was conducted during the 2019 novel coronavirus (COVID-19) pandemic which restricted the movement of people around the world to break the chain of infection. Also, all hospital visits were restricted unless for emergencies. In this study, six participants were located within a reasonable geographical distance and suitable for face-to-face contact; however, due to the movement control order (MCO) during the COVID-19 pandemic, these individuals were offered alternative options of interview, over the telephone or via video conference.
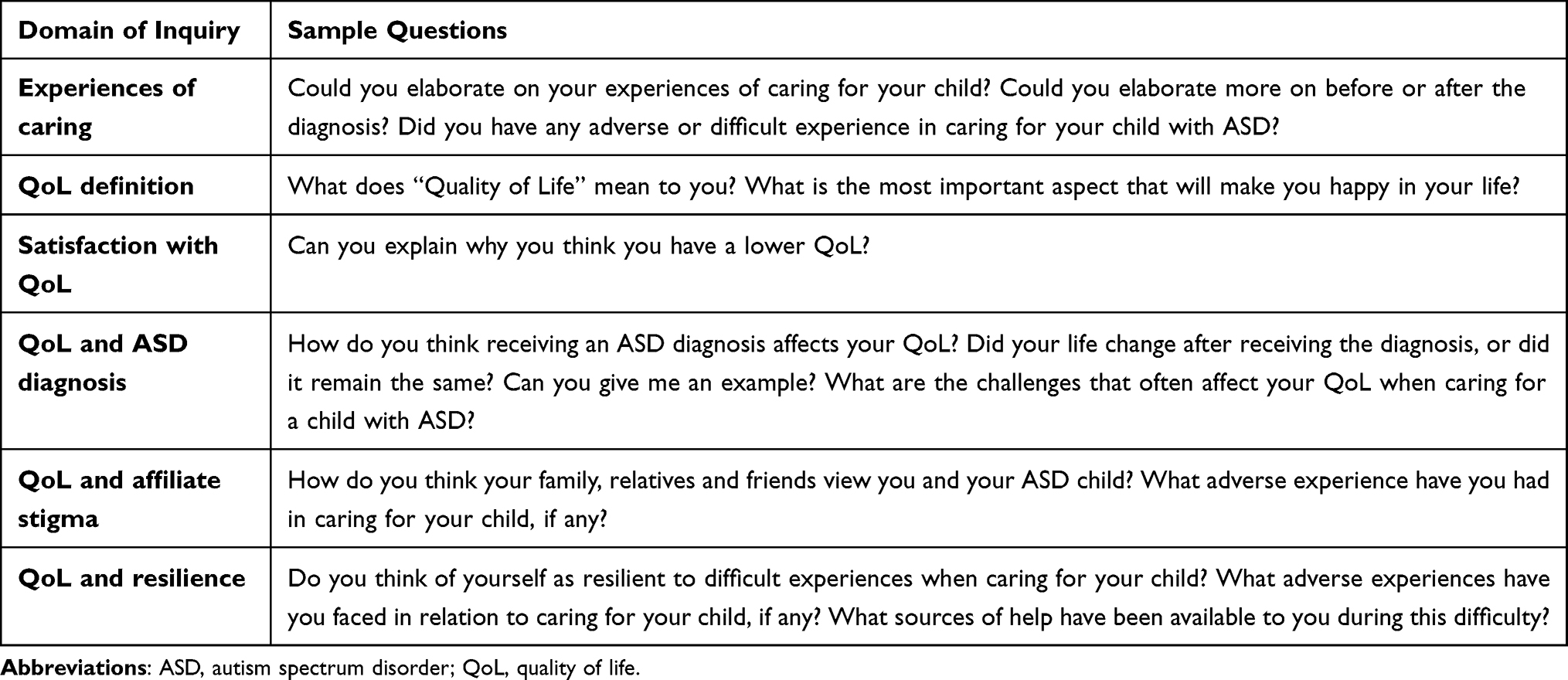 |
Table 2 The Interview Guides |
To compensate for the lack of face-to-face contact, the first author followed the guidelines proposed by Rubin and Rubin,19 which included contacting interviewees several times prior to the interview session to establish rapport. Since the researcher had an average of 11 interactions with each participant before the scheduled interview (range = 7–15), this was easy to achieve. To build trust, interactions included text messages and telephone calls, face-to-face meetings at an autism symposium and ASD support groups’ events, and during the child’s therapy at the hospital. Therefore, the participants and interviewer were reasonably familiar with each other by the time the interviews were conducted.
Moreover, in order to compensate for the lack or inability to read nonverbal prompts or cues (for instance, prompts demonstrating when a particular issue was sensitive), the interviewer paid meticulous attention to changes in voice and pauses to determine whether the participants were comfortable enough to continue. When there were instances where parents became emotional or showed signs of psychological distress during the interview (for example, crying), a discussion concerning the continuation of the interview was instigated and the option to discontinue involvement in the study was offered. The interview continued as and when the parents were ready. The interviewer also used silent probes to gain more information and ensure the participants had enough opportunity to share their viewpoints. This eventually yielded a great depth to, and the utmost variation in the responses. The use of the techniques above was calculated to compensate adequately for the limitations associated with telephone interviews.
There was one participant who chose a video conference interview. The advantage of using video over just voice in telephone interviews is the ability to analyze verbal and visual information such as body movement, facial expression, and hand gestures.20 In summary, five interviews were conducted in-person, five took place via telephone, and one occurred via video conference (WhatsApp video call) at the request of each participant. Open-ended interviews provided parents with an opportunity to describe their concerns in their own words and for the researcher to seek clarification. After the participants had provided consent, they were reminded that their participation was voluntary, that it was possible to withdraw at any time and their confidentiality was guaranteed. They were contacted by phone for the interview at a date, time, and place convenient for them. All interviews were digitally recorded and transcribed verbatim.
Data Analysis
Qualitative data were manually analyzed using the six phases of Braun and Clarke’s thematic analysis21 to elicit and understand the experiences and perceptions of parents when caring for a child with ASD. Transcripts were read several times by NSS to reflect on the overall meaning of what was said and to get familiar with the qualitative data prior to the analysis. After an initial reading to get the general sense of the content, a thorough review of the data was initiated by generating initial codes, led by NSS and reviewed independently by TLY, and KLA. Different coding labels were grouped and organized according to the common ideas that appeared in the answers to the research questions, to develop themes. Themes were identified and discussed among the authors (NSS, TLY, SJ, KLA) to rationalize theme. Where any discrepancies in the data interpretation occurred, it was resolved by consensus and discussion by referring back to the transcripts or judgement by an additional researcher, as appropriate. The following measures were taken to obtain trustworthiness.22 For example, credibility was ensured by having two of the researchers independently analyze and code the transcript. Quotations from parents are presented in the Table S1 to illustrate the inductive analysis and to enhance the confirmability of the results as well as to strengthen credibility.
Results
Based on the 11 interviews that corresponded to the aim of the study, the thematic analysis resulted in four main themes: (a) the meaning of QoL, (b) ASD and life adjustment, (c) perceived stigma, and (d) resilience.
Theme 1: Meaning of Quality of Life
Parents were first asked to think broadly about what the term “QoL” meant to them. Most parents expressed their own general definitions of QoL and described QoL as what it takes to make their life better. In this study, responses from parents fell into four out of eight domains of the QoL construct as proposed by Schalock et al,23 (personal development, self-determination, interpersonal relationships, social inclusion, rights, emotional well-being, physical well-being and material well-being). The four domains were: 1) self-determination, 2) emotional well-being, 3) physical well-being, and 4) material well-being. Thematic analysis showed that parents in this study viewed QoL as a term that included one or more of these subthemes.
Subtheme 1.1: Self-Determination
Most participants (6 out of 11) described QoL as the ability to apply their personal goals/values to raise their child with ASD as “normal” and to guide them to be independent in the future, much like other typically developing children. One parent said:
I want my son to get into normal school, like other kids. [P1]
Subtheme 1.2: Emotional Well-Being
Within this domain, several parents (4 out of 11) described the meaning of QoL as the state of being happy as one of the fundamental aspects of life. A mother said:
It’s all about happiness. Happy family, happy marriage, that’s all what I want in life. As long as I’m happy, so life is better. [P2]
Subtheme 1.3: Physical Well-Being
Additionally, there were three mothers who equated QoL to a restful life. For example, a mother said:
For me, if I have enough rest, then I’m more than a happy person. At least I can relax a bit. [P3]
Subtheme 1.4: Material Well-Being
When relating to material well-being, a few parents (4 out of 11) mentioned that in order to achieve a better QoL, material needs like money must be met. They highlighted the importance of financial stability for hospital treatment and to deal with possible challenges that may arise during the upbringing of their child. One parent said:
QoL is about money. If you have enough money, your life will be better. But you’re always short of money when you have a child with autism. [P4]
Theme 2: ASD and Life Adjustment
This theme reflected the continuous challenges associated with ASD faced by parents which have led to adjustments in their daily and social life. This theme consists of four subthemes: 1) impact on parents (themselves), 2) impact on spouse, 3) impact on the child’s siblings, and 4) impact on family.
Subtheme 2.1: Impact on Parents
A number of parents (4 out of 11) reported that they were overwhelmed by the child’s demands and eventually felt stressed, exhausted, and drained from the effort of caring for their child. A mother described it thus:
I am stressed by his behavior. If I have time, it must spend only on him. But I have so many other things to do. [P5]
Parents’ careers were also affected in terms of taking leave, as mentioned by one working mother.
I have to take leave very often. She has a list of appointments which affects my work schedule. [P2]
In the extreme, a number of mothers (4 mothers) had to quit their jobs because of the demands of caregiving. One mother said:
I had to resign because I need to take care of him. [P10]
In comparison to mothers, fathers mentioned having made fewer adjustments to their careers following their child’s diagnosis. In fact, there was no interruption of employment for any of the fathers in this study, and they remained as the financial provider of the household.
Subtheme 2.2: Impact on Spouse
Parents indicated that raising a child with ASD had both positive and negative effects on their relationship with their spouse. A number of parents (3 out of 11) reported that in the process of caring for their child with ASD, they had grown closer to their spouse. A mother testified:
My husband understands me very well. Even when he is busy, he will help me do the housework. [P11]
However, in some cases, it pushed couples apart, with mothers and fathers playing different roles in the family. Fulfilling these different roles sometimes resulted in resentment, especially among mothers (two mothers in this study) who believed they received insufficient support from their husbands. One mother stated as follows:
I don’t get support from him. He doesn’t care. He just doesn’t understand. [P7]
One mother was worried that the constant stress she endured while caring for her child could put her marriage at risk of divorce.
We’ve had fights because I’m so stressed with my son misbehavior. Sometimes, we talk about divorce … [P6]
Subtheme 2.3: Impact on the Child’s Siblings
Caring for a child with ASD also affected the relationship between parents and other children. Parents (3 out of 11) described their other children feeling that they had not been treated like their brother or sister with ASD, and they rebelled because of this.
Everything focuses on her. My eldest child gets jealous as she needs to learn everything by herself because I focus too much on her sister. [P2]
In other cases, older siblings assisted parents (3 out of 11) to take care of their autistic sibling and sometimes showed greater patience and maturity, which may be due to their relationship with their sibling with ASD. One mother mentioned:
He is used to helping me care for his brother. He’s done it since he was little. [P7]
Subtheme 2.4: Impact on Family
Parents also explained that there had been changes in the family’s financial situation due to raising a child with ASD. A few parents (3 out of 11) reported that therapy and treatment burdened them financially. For example:
It is a burden for us. We can’t afford this in the long run. [P9]
On another level, the family’s social life had also been affected, which may have led to isolation as a result of having to spend time and energy to raise a child with ASD. Six out of 11 of them reported a sense of disconnection from society and described struggling to maintain flexibility in their lives.
Autism not only affects my life; it controls it as well … You are cut off from everyone, from everything! [P6]
Theme 3: Perceived Stigma
Within this theme, parents stated that they often perceived stigma from others due to their relationship with their child with ASD, and this affiliate stigma further affected their lives. It included: 1) guilt and embarrassment and 2) negative attitudes from others.
Subtheme 3.1: Guilt and Embarrassment
Parents perceived being stigmatized as they felt blamed, judged by others, and embarrassed by their child’s disorder. Three of the mothers admitted that they felt guilty about the child’s disorder as they linked the causes of ASD to their experience during and after pregnancy. One mother mentioned this as follows:
I think it started when I was pregnant. I breathed in some chemical smoke which came from an accidental fire. So, I think that was the cause. [P1]
Two fathers also felt they should be blamed, because they had not noticed the disorder earlier. This perceived blame led to stigma. One father testified:
They said he has autism; I felt like I had done something wrong. I hadn’t picked it up. [P8]
They also reported that they felt blamed and judged for their child’s misbehavior. All parents indicated that they felt their parenting skills had been questioned by others who perceived them as lacking in parenting skills, for not appropriately disciplining their child. One father said:
I’m judged on my parenting as my son doesn’t listen to me. [P9]
Furthermore, the majority of parents (5 out of 11) echoed that shame was another manifestation due to the child’s publicly inappropriate behavior. A mother reported:
Sometimes, she will act up. I feel ashamed of bringing her out. I feel like people will stare at us. [P3]
Subtheme 4.2: Negative Attitudes from Others
Parents also perceived that they faced negative reactions from others. Rejection was reported to be directed at parents and their child alike. A mother said:
I sent my son to the mainstream classes. On day 5, the teachers didn’t let him in because he had made trouble. They rejected him straight away! [P1]
Rude comments expressed by others were frequently experienced and much harder to ignore by 3 out of 11 parents in this study. For instance:
‘Serves you right for having this kind of son!’ That’s what she told me. [P1]
Another manifestation of stigma was inappropriate staring by others. This usually happened in public places such as shopping complexes when the child displayed socially inappropriate behavior. Overt staring also made parents feel uncomfortable, which has led to social isolation. For example:
People don’t understand. They will look at you badly [by staring]. So, I rather stay at home. [P6]
Theme 4: Resilience
This theme describes the process of successful adaptation and perseverance by parents who have faced, and for the most part, overcome great challenges and adversities in their lives. This theme is characterized by three subthemes: 1) acceptance of the diagnosis, 2) feelings of normalcy, and 3) appreciation.
Subtheme 4.1: Acceptance of the Diagnosis
Within this subtheme, all parents reported that they had grown to accept their child’s diagnosis. One mother said:
Just accept it and move on. You cannot deal with it until you accept it. [P2]
Subtheme 4.2: Feelings of Normalcy
Several parents found a new normal for their family. They established a caregiving routine and stopped trying to “fix” their child. Resilience emerged when they persevered to a point in which they experienced normalcy. For instance:
Sometimes, he behaves like a normal kid. That’s when we can go out together. [P6]
Subtheme 4.3: Appreciation
A few parents (5 out of 11) also described their appreciation of having and caring for their child with ASD. A mother said that ASD had brought her closer to her spouse and her child.
Only now, starting this year, I can see [my husband’s] changes towards my son. [P7]
Some parents believed that they had personally changed, for example, by acquiring greater patience, love and tolerance, and enhanced coping ability. A father added:
He challenges us but he has taught us so many things, like patience, tolerance and love. [P8]
Discussion
We aimed to explore parental experiences and their perceptions of affiliate stigma, resilience, and QoL when caring for a child with ASD. The results of this study generated four themes, namely the meaning of QoL, ASD and life adjustment, perceived stigma and resilience.
With regard to parents’ experiences of caring, the first theme identified was ASD and life adjustment. Given the nature of this disorder, raising a child with ASD was a continuous endeavor that had led to adjustments in parents’ daily and social lives. Also, under this theme, it is suggested that there were impacts of ASD on the parent’s spouse, child’s siblings and family (for example, financial). It was revealed that parents felt overwhelmed by family demands and eventually felt stressed and exhausted which later impacted their health, much like findings in previous studies.24,25 Also, daily parenting responsibilities including interaction with the physician, interventions and therapies were often tiring and time-consuming, reducing the opportunities of parents to engage in social communication with family and friends, thus leading to a sense of isolation.26
This finding suggests that healthcare professionals should be aware of the signs of health deterioration and the need to educate parents on adaptive coping styles. Research has shown that parents of children with disabilities who used problem-focused coping strategies such as seeking social support and going on outings showed more psychological adaptation compared to those who used emotion-focused coping strategies (for instance, ignorance or detachment).27 Also, healthcare professionals should assist parents to develop strategies and good parenting skills to manage their child at home.
Another subtheme captured the impact on spousal relationships when caring for children with ASD in which a few parents grew closer while others grew apart. The finding of potential marital problems is consistent with previous studies, which reported marital problems and higher divorce rates among parents of children with ASD.28–30 Hence, healthcare providers need to be aware of this increased risk of divorce among parents. Additionally, the findings in the current study indicated that caring for a child with ASD influenced the relationship between parents and other children, as was also found in past research.31 However, older siblings in this study reported positive feelings in helping parents care for their autistic sibling, which is consistent with a previous study that showed that some siblings expressed a sense of responsibility towards their autistic brother or sister.32 Lastly, parents reported that they faced an additional financial burden, which included substantial healthcare costs and non-medical expenses, such as therapies and school services.33,34 Again, healthcare professionals need to be fully aware and on the lookout for these lifelong risks and impacts which affect the physical, emotional, social, and financial well-being of family members living with individuals with ASD.
Another three themes emerged from the interviews pertaining to parental perceptions of affiliate stigma, resilience, and QoL. With regard to the theme of perceived stigma, parents often blamed themselves for their child’s disorder; a finding similar to past research.29,35 For example, parents felt guilt and blame when they started to wonder about the suspected causes of their child’s behavior.35 Also, they felt that they were blamed and criticized as “bad parents” by others who misjudged their child’s misbehavior.36 In addition, parents in this study reported that they endured criticism or negative attitudes from others as their child did not “act normal”. This perception showed the manifestations of enacted stigmatization, which is defined as occurrences of obvious rejection, discrimination or prejudice faced by the stigmatized person.37 As the public does not notice a physical manifestation of ASD, they believe that the bad behavior is due to poor parenting.38 For instance, one study explored the perceptions of stigma among mothers of children with Asperger syndrome who indicated that their child usually “behaves very well”, but when they did not meet the expectations of society, they and their families were stigmatized.39 Therefore, it is suggested that the invisible nature of ASD makes it particularly challenging for families with ASD to be out in public. However, affiliate stigma is unlikely to occur if courtesy stigma from the public lessens.12 Hence, collaboration with local authorities may be beneficial to enhance public awareness and foster a more positive attitude within the community towards ASD which may alleviate affiliate stigma.40
The theme of resilience described the process of successful adaptation and perseverance when faced with major life challenges, consistent with a few studies which reported that some families are considered resilient and have a more positive outlook.28,41 It is suggested that families demonstrate resilience when, despite adversity, they are competent in performing core family functions including family bonding; economic support; nurturance, education and socialization; and protection of vulnerable members.42 Hence, it can be concluded that their resilience is shown when they persevere to a point in which they experience normalcy and have established a caregiving routine, as well as having stopped trying to “fix” their child, as reported in one of the subthemes under this theme.
The last theme was the meaning of QoL. QoL is a complex construct with various definitions. Within this theme, parents shared their views on what QoL meant to them and their responses fell into four out of eight of Schalock’s domains;23 self-determination, emotional well-being, physical well-being, and material well-being.
With regard to self-determination, this finding is consistent with past research which showed optimism about their children’s future.7,41,43 Many wanted their child to achieve typical milestones, such as living on their own.35 Moreover, this theme highlighted the importance of emotional, physical, and material well-being in achieving better QoL as perceived by parents in this study, which is also supported by previous literature.43
With regard to emotional well-being, four participants alluded to this aspect of well-being, and much discussion centered around personal fulfilment. Within this subtheme, parents equated QoL with being happy and with the absence of stress and problems. For example, one parent said, “It’s all about happiness. Happy family, happy marriage, that’s all what I want in life. As long as I’m happy, life is better.” This response may reflect how this happiness is related to having a purpose or meaning in life.
Pertaining to physical well-being, there were three mothers who mentioned the lack of physical well-being when discussing QoL when they complained that they were more often than not physically exhausted. As one of the mothers reported; “For me, if I have enough rest, then I’m more than a happy person. At least I can relax a bit.” Previous studies have shown that QoL has a consistently low rating in the physical domain, compared to the other domains (for example social, emotional), thus indicating a more direct effect of ASD on parental physical well-being.44,45 A possible explanation may lie in the positive aspects adopted by parents in raising a child with ASD. Parental benefits of caring for an individual with ASD as reported in this current study include heightened spirituality and personal growth, which could potentially protect parents from emotional distress but not against the more physical aspects of caregiving, for example, lack of sleep and physical exhaustion.6,29,46 In this case, the availability of parent support groups is critical for boosting parents’ sense of control over their well-being and for offering techniques for parenting children with ASD to prevent further issues which may impair their physical and mental health. Above all, providing more support, such as home services for parents, will allow for their improved health.
Lastly, with regard to the financial burden, healthcare professionals should engage parents in a discussion related to financial resources and address the unmet needs of lower socio-economic families, as well as referring them to the relevant authority that can provide appropriate assistance.
Methodological Considerations and Limitations
While this study supports previous research and provides additional insights regarding parental experiences of caring and perception of affiliate stigma, resilience, and QoL, methodological considerations and limitations have to be taken into account.
A qualitative approach was chosen in order to provide parents with an adequate opportunity to describe their experiences and perceptions, as well as to explore new themes. By using semi-structured interviews, in-depth information was obtained. In order to minimize inconsistency during data collection and to strengthen trustworthiness, each decision made during every step of the research process was logged. Measures taken to increase trustworthiness, especially the credibility criteria included prolonged engagement, triangulation, member checking, and peer debriefing. Transferability was addressed by providing a detailed description of the study background, themes, and participants so that readers can determine the generalizability of findings within the context. Furthermore, field notes were used during data collection to increase the richness of the data. Participants’ socio-demographic characteristics were outlined so readers can identify sample attributions and determine comparability to existing research. Themes were presented in detail and as mentioned earlier, evidence in both positive and negatives cases were emphasized. Lastly, to enhance confirmability, reflexivity was implemented.
However, one limitation of this study is that only three of the 11 parents were fathers. This echoes most studies examining parental outcomes among children with ASD and is representative of the distribution of parental responsibilities within many families. Since mothers were mostly the primary caregivers, this added to the gender disparity of participants. Thus, the results may not fully reflect fathers’ experiences and perceptions to the same extent as the mothers’.
Also, the research methodology utilized provided invaluable insights into the experiences of families of children with ASD, but parents had to speculate on the opinions of other members, including the child’s siblings, parent’s spouse, and other members of the extended family. Hence, the data were limited as it represented the views of only one family member (for instance, parents). In addition, this study only represents the experiences of parents of children of a certain age and a certain gender. The age group under study here was from two to 12 years old, and the majority of parents who participated were caring for a son with ASD (81.8%). In conjunction, these might limit the generalizability of the findings.
Conclusion
Parents have first-hand expert knowledge that can inform ASD family-centered models of care and help researchers identify gaps in programs and available services. Therefore, the study findings can be used to develop educational and support plans for parents and to recommend appropriate mental health services for families in need. In addition, healthcare administration should act strategically to modify treatment and service provision for parents according to socio-demographic backgrounds. Taking it a step further, the establishment of family centers where parents can receive advice on strategies or measures to cope with their child’s behavior are warranted. These could also serve as centers for advocacy for parents to raise societal awareness of ASD. Establishing a support group may also enhance their sense of control and support. The study also reveals a need for increased collaborative support between policymakers and healthcare professionals who are directly or indirectly involved in provision of care.
We also suggest that future research should involve parents of children with ASD from more diverse backgrounds and whose children include adolescents and adults to determine whether their experiences are similar. Also, due to the limited number of fathers involved in this study, future studies should explore paternal experiences in more depth and in comparison to mothers. Moreover, further research should recruit a range of individuals in the family system, such as caregivers, siblings, and extended family members as well as parents of more gender-diverse individuals with ASD. This is important as all these factors may affect parenting behaviors and experiences.
Acknowledgments
Special thanks to all the parents who participated and shared their experiences in this study. We wish to thank the top management of Hospital Universiti Sains Malaysia and Hospital Raja Perempuan Zainab II for permitting us to conduct the study.
Funding
NSS is supported by the Ministry of Higher Education Malaysia and Universiti Sains Malaysia through the Academic Staff Training Scheme (ASTS).
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. DSM-5: diagnostic and statistical manual of mental disorders, (5th ed.); 2013. Available from: https://www.psychiatry.org/psychiatrists/practice/dsm/educational-resources/dsm-5-fact-sheets.
2. Chan KKS, Lam CB. Self-stigma among parents of children with autism spectrum disorder. Res Autism Spectr Disord. 2018;48:44–52. doi:10.1016/j.rasd.2018.01.001
3. Kartini I, Cornish K, Kummar AS, et al. Parenting stress and resilience in parents of children with autism spectrum disorder (ASD) in Southeast Asia: a systematic review. Front Psychol. 2018;9:280. doi:10.3109/13668250.2016.1196657
4. Goffman E. Stigma: Notes on the Management of Spoiled Identity. New York, NY: Simon and Schuster Inc; 2009.
5. Corrigan PW, Watson AC. The paradox of self-stigma and mental illness. Clin Psychol. 2002;9(1):35–53. doi:10.1093/clipsy.9.1.35
6. Mak WWS, Kwok YTY. Internalization of stigma for parents of children with autism spectrum disorder in Hong Kong. Soc Sci Med. 2010;70:2045–2051. doi:10.1016/j.socscimed.2010.02.023
7. Fairuz Nazri Abd R, Wan Salwina Wan I, Nik Ruzyanei Nik J, et al. Reducing the isolation: a Malaysian family in need. Int J Case Rep Imag. 2012;6:46. doi:10.5348/ijcri-2012-06-138-CR-11
8. Illias K, Hui JJL, Cornish K, et al. Wellbeing of mothers of children with “A-U-T-I-S-M” in Malaysia: an interpretative phenomenological analysis study. J Intellect Dev Disabil. 2016;42:74–89. doi:10.3109/13668250.2016.1196657
9. Dolah J, Yahaya WAJW, Chong TS, Mohamed AR. Identifying autism symptoms using Autism Spectrum Quotient (ASQ). Procedia Soc Behav Sci. 2012;64:618–625. doi:10.1016/j.sbspro.2012.11.072
10. Chiu MYL, Yang X, Wong FHT, Li JH, Li J. Caregiving of children with intellectual disabilities in China - An examination of affiliate stigma and the cultural thesis. J Intellect Disabil Res. 2013;57(12):1117–1129. doi:10.1111/j.1365-2788.2012.01624.x
11. de Vries M, Cader S, Colleer L, et al. University student’s notion of autism spectrum conditions: a cross-cultural study. J Autism Dev Disord. 2020;50:1281–1294. doi:10.1007/s10803-019-04343-z
12. Papadopoulos C, Foster J, Caldwell K. ‘Individualism-collectivism’ as an explanatory device for mental illness stigma. Community Ment Health J. 2013;49:270–280. doi:10.1007/s10597-012-9534-x
13. Shin YC, Park H, Lee J, Shaharuddin KK, Chun HG. Self-stigma and its associations with stress and quality of life among Malaysian parents of children with autism. Child Care Health Dev. 2020;46:485–494. doi:10.1111/cch.12771
14. Duca DS. Family resilience and parental stress: the effects on marital relationship in the context of a child diagnosed with an autism spectrum disorder. Sci Ann Al I Cuza Univ Psychol Ser. 2015;24(1):71–90.
15. Musetti A, Manari T, Dioni B, et al. Parental quality of life and involvement in intervention for children or adolescents with autism spectrum disorders: a systematic review. J Pers Med. 2021;11(9):894. doi:10.3390/jpm11090894
16. Eapen V, Crncec R, Walter A, et al. Conceptualization and development of a quality of life measure for parents of children with autism spectrum disorder. Autism Res Treat. 2014;3:1–11. doi:10.1155/2014/160783
17. Alhazmi A, Petersen R, Donald KA. Quality of life among parents of South African children with autism spectrum disorder. Acta Neuropsychiatr. 2018;30:226–231. doi:10.1017/neu.2018.5
18. Kheir N, Ghoneim O, Sandridge A, et al. Quality of life of caregivers of children with autism in Qatar. Autism. 2012;2012:1–6. doi:10.1177/1362361311433648
19. Rubin HJ, Rubin IS. Listening, hearing, and sharing social experiences. Qual Interview. 2005;2:1–4.
20. Meirsschaut M, Roeyers H, Warreyn P. The social interactive behavior of young children with autism spectrum disorder and their mothers: is there an effect of familiarity of the interaction partner? Autism. 2011;15:43–64. doi:10.1177/1362361309353911
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
22. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
23. Schalock RL, Bonham GS, Verdugo MA. The conceptualization and measurement of quality of life: implications for program planning and evaluation in the field of intellectual disabilities. Eval Program Plann. 2008;30(2):181–190. doi:10.1016/j.evalprogplan.2008.02.001
24. Fletcher PC, Markoulakis R, Bryden PJ. The costs of caring for a child with autism spectrum disorder. Issues Compr Pediatr Nurs. 2012;35(1):45–69. doi:10.3109/01460862.2012.645407
25. Lai WW, Goh TJ, Oei TPS, et al. Coping and well-being in parents of children with autism spectrum disorders (ASD). J Autism Dev Disord. 2015;45(8):2582–2593. doi:10.1007/s10803-015-2430-9
26. Zablotsky B, Anderson C, Law P. The association between child autism symptomatology, maternal quality of life, and risk for depression. J Autism Dev Disord. 2013;43(8):1946–1955. doi:10.1007/s10803-012-1745-z
27. Bos AER, Pryor JB, Reeder GD, et al. Stigma: advances in theory and research. Basic Appl Soc Psych. 2013;35(1):1–9. doi:10.1080/01973533.2012.746147
28. Chong WH, Kua SM. Parenting self-efficacy beliefs in parents of children with autism: perspectives from Singapore. Am J Orthopsychiatry. 2016;87:365–375. doi:10.1037/ort0000169
29. Ha VS, Whittaker A, Whittaker M, et al. Living with autism spectrum disorder in Hanoi, Vietnam. Soc Sci Med. 2014;120:278–285. doi:10.1016/j.socscimed.2014.09.038
30. Manor-Binyamini I, Shoshana A. Listening to Bedouin mothers of children with autism. Cult Med Psychiatry. 2018;42(3):401–418. doi:10.1007/s11013-018-9567-x
31. Ayalz R, Yilmaz U, Polat S. Effect of difficulties experienced by parents of autistic children on their sexual life: a qualitative study. Sex Disabil. 2012;30(4):395–406. doi:10.1007/s11195-011-9251-3
32. Corsano P, Musetti A, Guidotti L, Capelli F. Typically developing adolescents’ experience of growing up with a brother with an autism spectrum disorder. J Intellect Dev Disabil. 2017;42(2):151–161. doi:10.3109/13668250.2016.1226277
33. Daniels AM, Mandell DS. Explaining differences in age at autism spectrum disorder diagnosis: a critical review. Autism. 2014;18:583–597. doi:10.1177/1362361313480277
34. Nik Aida Nik A, Mohd Ismail I, Azriani Ab R, et al. Predictors of caregivers’ satisfaction with the management of children with autism spectrum disorder: a study of multiple level of health care. Int J Environ Res Public Health. 2019;16:1684–1701. doi:10.3390/ijerph16101684
35. DePape AM, Lindsay S. Parents’ experience of caring a child with autism spectrum disorder. Qual Health Res. 2014;1–15. doi:10.1177/1049732314552455
36. Byrne G, Sarma KM, Hendler J, et al. On the spectrum, off the beaten path. A qualitative study of Irish parents’ experiences if raising a child with autism spectrum conditions. Br J Learn Disabil. 2018;46(3):1–11. doi:10.1111/bld.12227
37. Gray DE. ‘Everybody just freezes, everybody is just embarrassed’: felt and enacted stigma among parents of children with high functioning autism. Sociol Health Illn. 2002;24(6):734–749. doi:10.1111/1467-9566.00316
38. Neely-Barnes SL, Hall HP, Roberts RJ, et al. Parenting a child with an autism spectrum disorder: public perceptions and parental conceptualizations. J Fam Soc Work. 2011;14(3):208–225. doi:10.1080/10522158.2011.571539
39. Gill J, Liamputtong P. Being the mother of a child with Asperger’s syndrome: women’s experiences of stigma. Health Care Women Int. 2011;32(8):708–722. doi:10.1080/07399332.2011.555830
40. Salleh NS, Abdullah KL, Tang LY, Jayanath S, Husain M. Parents’ experiences of affiliate stigma when caring for a child with autism spectrum disorder (ASD): a meta-synthesis of qualitative studies. J Pediatr Nurs. 2020;55:174–183. doi:10.1016/j.pedn.2020.09.002
41. Santoso TB, Ito Y, Oshima N, Hidaka M, Bontje P. Resilience in daily occupations of Indonesian mothers of children with autism spectrum disorder. Am J Occup Ther. 2015;69:6905185020p1–6905185020p8. doi:10.5014/ajot.2015.017566
42. Patterson JM. Integrating family resilience and family stress theory. J Marriage Fam. 2002;64(2):349–360. doi:10.1111/j.1741-3737.2002.00349.x
43. Gardiner E Quality of life in families of children with autism spectrum disorder: considerations of risk and resilience [doctoral thesis]. Simon Fraser University; 2014.
44. Allik H, Larsson J, Smedje H. Health-related quality of life in parents of school-age children with Asperger syndrome or high-functioning autism. Health Qual Life Outcomes. 2006;4(1). doi:10.1186/1477-7525-4-1
45. Vasilopoulou E, Nisbet J. The quality of life of parents of children with autism spectrum disorder: a systematic review. Res Autism Spectr Disord. 2016;23:36–49. doi:10.1016/j.rasd.2015.11.008
46. Quilendrino MIO, Castor MAR, Mendoza NRNP, et al. Parents’ perceptions of autism and their health-seeking behaviors. Clin Epidemiol Glob Health. 2015;3:10–15. doi:10.1016/.j.cegh.2015.11.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.