Back to Journals » Infection and Drug Resistance » Volume 16
Heterogeneous Vancomycin Intermediate Staphylococcus aureus Infections in Diabetic and Non-Diabetic Patients – A Hospital-Based Comparative Study
Authors M S ![]() , Mulki SS
, Mulki SS ![]() , Shenoy S
, Shenoy S ![]() , Dhanashree B
, Dhanashree B ![]() , M C
, M C ![]() , Bhat G
, Bhat G
Received 19 October 2022
Accepted for publication 23 December 2022
Published 5 January 2023 Volume 2023:16 Pages 9—17
DOI https://doi.org/10.2147/IDR.S393415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Sreejisha M,1 Shalini Shenoy Mulki,1 Suchitra Shenoy,1 Biranthabail Dhanashree,1 Chakrapani M,2 Gopalakrishna Bhat1
1Department of Microbiology, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education (MAHE), Manipal, Karnataka, 575001, India; 2Department of Medicine, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education (MAHE), Manipal, Karnataka, 575001, India
Correspondence: Gopalakrishna Bhat, Department of Microbiology, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education (MAHE), Manipal, Karnataka, India, Tel +91 9480424729, Email [email protected]
Purpose: To study the infections caused by methicillin resistant Staphylococcus aureus (MRSA) with emphasis on heterogeneous vancomycin intermediate S. aureus (hVISA) in diabetic and non-diabetic patients and their comparison.
Patients and Methods: S. aureus strains isolated from diabetic and non-diabetic patients admitted in four tertiary care hospitals in Coastal Karnataka, South India, were tested for methicillin resistance and included in the present study. Demographic and clinical data of the patients were collected using structured proforma. Antimicrobial susceptibility testing was done using the Kirby-Bauer disc diffusion method, and MLSB phenotypes were identified using the D-test. The minimum inhibitory concentration (MIC) of vancomycin was determined using agar dilution. MRSA isolates were tested for hVISA using vancomycin screen agar and population analysis profile – area under the curve (PAP-AUC) test. Statistical analysis of the results was done using the chi-square test. SPSS version 29.0 was used for this purpose.
Results: Out of 665 strains of S. aureus isolated, 220 (33.1%) were MRSA. Of these 220 MRSA strains, 122 (55.5%) and 98 (44.5%) were isolated from diabetic and non-diabetic patients, respectively. There was no significant difference in the antimicrobial resistance patterns of MRSA strains isolated from diabetic and non-diabetic patients. Foot infections and osteomyelitis caused by MRSA were significantly more among diabetic patients. Out of 220 strains of MRSA, 14 (6.4%) were hVISA. The rates of hVISA among MRSA isolated from diabetic and non-diabetic were 9.0% and 3.1%, respectively. This difference was statistically not significant.
Conclusion: The rate of hVISA among all MRSA isolates was 6.4%. The risk of hVISA infection was three times more in diabetic patients. The results emphasize the importance of the detection of hVISA among MRSA isolates especially from diabetic patients.
Keywords: methicillin-resistant S. aureus, diabetes mellitus, antimicrobial resistance, heterogeneous vancomycin intermediate S. aureus
Introduction
Methicillin resistant Staphylococcus aureus (MRSA) is one of the most common pathogens causing healthcare-associated infections (HAIs).1 Since MRSA is multidrug resistant (MDR), treatment of infections caused by this organism is a challenge.2 Vancomycin is being used for the treatment of serious invasive infections caused by MRSA.3 However, there has been a rise in the rate of MRSA with reduced susceptibility to vancomycin in recent years.4,5 Vancomycin intermediate S. aureus (VISA) and heterogeneous vancomycin intermediate S. aureus (hVISA) were described in 1997.6 The minimum inhibitory concentration (MIC) of vancomycin to VISA is 4–8 µg/mL.7 Therefore, VISA can be detected by dilution methods.7 hVISA is a type of S. aureus that contains one vancomycin intermediate cell per 105 to 106 vancomycin-susceptible cells.5 Vancomycin MIC for hVISA remains in the susceptible range (≤2 µg/mL).5,8
Antimicrobial susceptibility tests conducted routine in clinical microbiology laboratories fail to detect hVISA.5,8 Special screening methods and confirmatory population analysis-area under the curve (PAP-AUC) test are required to identify hVISA.8–10 Vancomycin treatment may not be effective for hVISA infections.11 Therefore, it is essential to detect hVISA before starting vancomycin treatment. The first case of vancomycin resistant S. aureus (VRSA) was reported in a diabetic patient in 2002.12 Although VRSA infections are uncommon, infections caused by hVISA and VISA are being reported from different parts of the world.4
Diabetic patients are more susceptible for infectious diseases because of the increase in blood glucose level, impaired phagocytosis, impaired immunity, peripheral neuropathy and peripheral vascular disease.13 Further, diabetic patients are predisposed to infections with multidrug resistant bacteria due to frequent hospitalizations and long-term use of antimicrobial agents.14 According to previous research, MRSA is the most common pathogen isolated from diabetic foot infections and ulcers.13 Further, a recent study from South India reported MRSA as an important pathogen to cause bone infection and the rate of methicillin resistance among S. aureus was 37.0%.15
hVISA is emerging as an important healthcare-associated pathogen.4,16 A meta-analysis described the prevalence of VRSA, VISA and hVISA across the globe, 1.5%, 1.7% and 4.6%, respectively.4 In India, the prevalence of VRSA, VISA and hVISA is 1.6%, 4.6% and 2.5%, respectively.4 A previous study from India has shown that among MRSA isolates with vancomycin MIC of ≥1 μg/mL, 12.0% were hVISA.17 Previous MRSA infection, hospitalization and previous vancomycin treatment are common risk factors for hVISA infection.5
There is paucity of literature on hVISA infections among diabetic patients in South India. The purpose of the current investigation was to study infections caused by MRSA with emphasis on hVISA in diabetic and non-diabetic patients and their comparison.
Materials and Methods
Study Setting and Design
The present hospital-based cross-sectional study was conducted on MRSA isolated from diabetic and non-diabetic patients admitted in four tertiary care hospitals (2 public and 2 private hospitals) attached to a private medical college in Coastal Karnataka, India. Public tertiary care hospital 1 and 2 have 1000 and 260 beds, respectively. Private tertiary care hospital 1 and 2 have bed strength of 350 and 600, respectively. The present investigation was conducted in the Department of Microbiology between February 2019 and March 2020. Healthcare-associated infections (HAIs) were identified based on Centers for Disease Control and Prevention (CDC) guidelines.18
The study had approval of the Institutional Ethics Committee, Kasturba Medical College, Mangalore. The bacterial strains included in the present study were isolated from the clinical specimens received at the laboratory for investigation, and the samples were anonymized. Therefore, informed consent was not required.
Isolation and Identification of Bacteria
Isolation and identification of S. aureus was done using the standard bacteriological methods including gram stain, colony morphology, beta hemolysis, pigmentation, catalase test, coagulase test, DNase test, and mannitol fermentation.19
Methicillin resistance was detected using the cefoxitin disk (30 µg) diffusion method as suggested by CLSI.7 A diameter of zone of inhibition ≤ 21mm was considered methicillin resistance. S. aureus ATCC 43300 and S. aureus ATCC 25923 were used as positive and negative controls, respectively. Methicillin resistance was confirmed by the detection of mecA gene using PCR.20
Antimicrobial Susceptibility Testing
Antimicrobial Susceptibility Testing Using Kirby-Bauer Disk Diffusion Method
Antimicrobial susceptibility testing was done using the Kirby-Bauer disk diffusion method.7 The following antibiotics (BD BBL™ Sensi-Disc™ antimicrobial susceptibility test disks) were used: ciprofloxacin (5 µg), clindamycin (2 µg), erythromycin (15 µg), gentamicin (10 µg), linezolid (30 µg), rifampicin (5 µg), teicoplanin (30 µg) tetracycline (30 µg) and trimethoprim-sulphamethoxazole (1.25 µg/23.75 µg). The results were interpreted as per CLSI guidelines.7 S. aureus ATCC 25923 was used as control strain.
Detection of Macrolide, Lincosamide and Streptogramin B (MLSB) Phenotypes
MRSA strains were tested for MLSB phenotypes using D test.7 Mueller–Hinton agar (MHA) plates were inoculated with the test bacterial inoculum having turbidity matching with McFarland 0.5 standard (bacterial count 1.5 × 108 CFU/mL). Clindamycin (2 µg) and erythromycin (15 µg) (BD BBL™ Sensi-Disc™ antimicrobial susceptibility test disks) disks were placed on the inoculated plate at a distance of 15 mm edge to edge. The plates were incubated at 35°C for 16–18 h, and the results were interpreted as per CLSI guidelines.7
- Flattening of the zone of inhibition around the clindamycin disk facing erythromycin disk, producing D-shaped zone of inhibition was considered inducible clindamycin resistance (iMLSB phenotype).
- No zone of inhibition around erythromycin and clindamycin disk was considered constitutive MLSB (cMLSB).
- No zone of inhibition around erythromycin disk but susceptible circular zone around clindamycin disk without flattening was considered MSB phenotype.
Determination of Minimum Inhibitory Concentration (MIC) of Vancomycin
The MIC of vancomycin to the test organism was determined using agar dilution.7 MHA plates containing different concentrations (32, 16, 8, 4, 2, 1, 0.5, 0.25 and 0.125 µg/mL) of vancomycin (Sigma chemical) were prepared. Two to three colonies of the test organism grown on blood agar plate were inoculated into Mueller–Hinton broth and incubated at 37°C for 4 to 6 h till the turbidity was matched with McFarland 0.5 standard (1.5 × 108 CFU/mL). The broth culture was diluted 10 folds to prepare the working inoculum (1.5 × 107 CFU/mL). Two microliters of the working inoculum was spot inoculated on the plates. The plates were incubated at 35°C for 24 h. The minimum concentration of vancomycin that inhibited the bacterial growth was considered the MIC and the results were interpreted as per CLSI guidelines.7 Isolates with vancomycin MIC ≤ 2 µg/mL, 4 to 8 µg/mL and ≥16 µg/mL were considered VSSA, VISA and VRSA, respectively.7 Enterococcus faecalis ATCC 29212 and S. aureus ATCC 29213 were used as vancomycin-susceptible controls. E. faecalis ATCC 51299 was used as vancomycin resistant control.
Identification of hVISA
Screening for hVISA
Brain heart infusion agar (BHI, HiMedia, Mumbai) with 16 g/L pancreatic digest of casein (Sigma Chemical) and 4 µg/mL vancomycin (Sigma Chemical) (BHI screen agar) was used for screening of hVISA.8 Two bacterial inocula matching with McFarland 2.0 and 0.5 standard were used. Four 10 µL drops from each inoculum were placed on the BHI screen agar plate and allowed to dry for 10 minutes. The plates were incubated at 35°C for 48 h and observed for bacterial growth. If at least one drop had two or more colonies, the isolate was considered hVISA.8 S. aureus ATCC 25923 and S. aureus ATCC 700698 (Mu3 strain of hVISA) were used as negative and positive controls, respectively.
Confirmation of hVISA
Modified population analysis profile-area under the curve (PAP-AUC) test described previously by Wootton et al was used for the confirmation of hVISA.9 Briefly, the test organism was grown in brain heart infusion broth at 35°C for 6 h and the turbidity was matched with McFarland 0.5 standard (1.5 × 108 CFU/mL). The broth culture was further diluted 10−2 to 10−5. One bacterial dilution with bacterial count 104 CFU/mL was used for inoculation.10 Ten microliters bacterial inoculum was spread on BHI agar with a range of vancomycin concentrations (16, 8, 4, 2, 1, 0.5, 0.25 and 0.125 µg/mL). Reference strain Mu3, hVISA (S. aureus ATCC 700698) was used as positive control. The plates were incubated at 35°C for 48 h and observed for bacterial growth. The PAP-AUC ratio was determined using GraphPad Prism software version 9.0 (GraphPad Software, USA). The test isolate with AUC ratio 0.9 to 1.3 was reported as hVISA. Strains with AUC ratio >1.3 considered as VISA.10
Statistical Analysis of Results
The rates of MRSA among S. aureus and hVISA among MRSA were expressed in percentage. Statistical analysis of the results was done using chi-square test (Statistical Analysis-Supplementary File). P value of ≤0.05 was considered statistically significant. Statistical Package for the Social Sciences (SPSS), Version 29.0 (IBM Corp., Chicago, Illinois, USA) was used for this purpose.
Results
Out of 665 non-repetitive strains of S. aureus isolated from hospitalized patients, 357 (53.7%) were from diabetic patients and 308 (46.3%) were from non-diabetic patients. Out of 665 S. aureus strains, 220 (33.1%) were methicillin resistant. Of these 220 MRSA strains, 122 (55.5%) were isolated from diabetic patients and 98 (44.5%) were isolated from non-diabetic patients. The mean and median age of diabetic patients were 58 and 57 years, respectively. The mean and median age of non-diabetic patients were 27 and 28 years, respectively. MRSA was isolated from pus, tissue, blood and IV catheter tip.
The rate of methicillin resistance among S. aureus strains isolated from the two public and two private tertiary care hospitals was 33.1% (93/281), 31.0% (9/29), 32.7% (54/165) and 33.7% (64/190), respectively. Of the 220 clinical isolates of MRSA, 143 (65.0%) were from male and 75 (35.0%) were from female patients.
Gender distribution and types of MRSA infections in diabetic and non-diabetic patients are presented in Table 1. Compared with non-diabetic male patients, MRSA infections were significantly more in diabetic male patients. Foot infection and osteomyelitis caused by MRSA were significantly more among the diabetic patients.
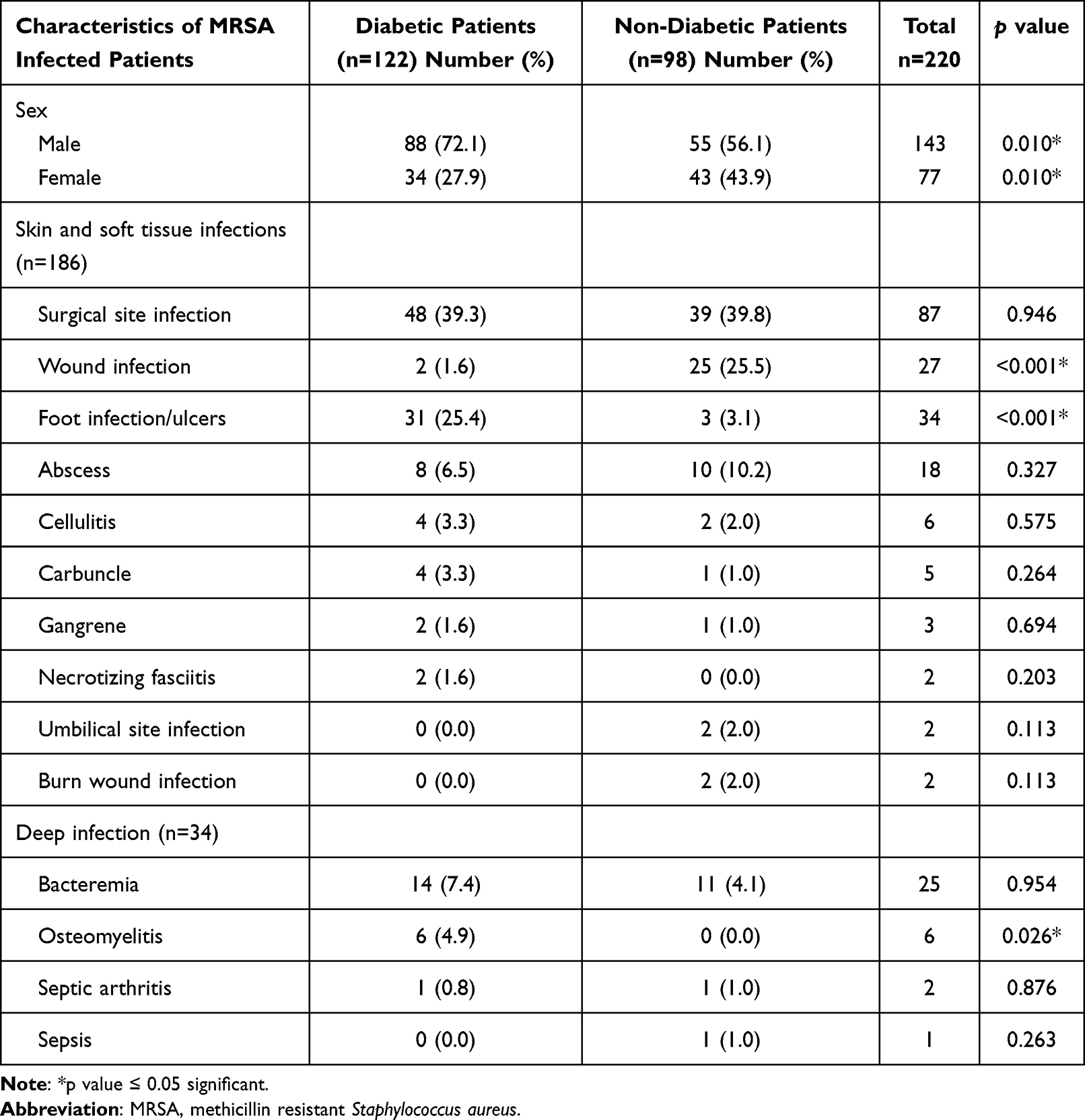 |
Table 1 Gender Distribution and Clinical Characteristics of Diabetic and Non-Diabetic Patients with MRSA Infection |
The antimicrobial resistance pattern of MRSA isolates is shown in Table 2. There was no significant difference in antimicrobial resistance of MRSA strains isolated from diabetic and non-diabetic patients. Over 80.0% of MRSA were resistant to ciprofloxacin and erythromycin. Multidrug resistance was detected among 72.3% of MRSA strains. All the isolates were susceptible to linezolid and teicoplanin. All 220 strains of MRSA were susceptible to vancomycin (MIC ≤ 2 µg/mL) by agar dilution. MIC90 and MIC50 of vancomycin were 2 µg/mL and 1 µg/mL, respectively.
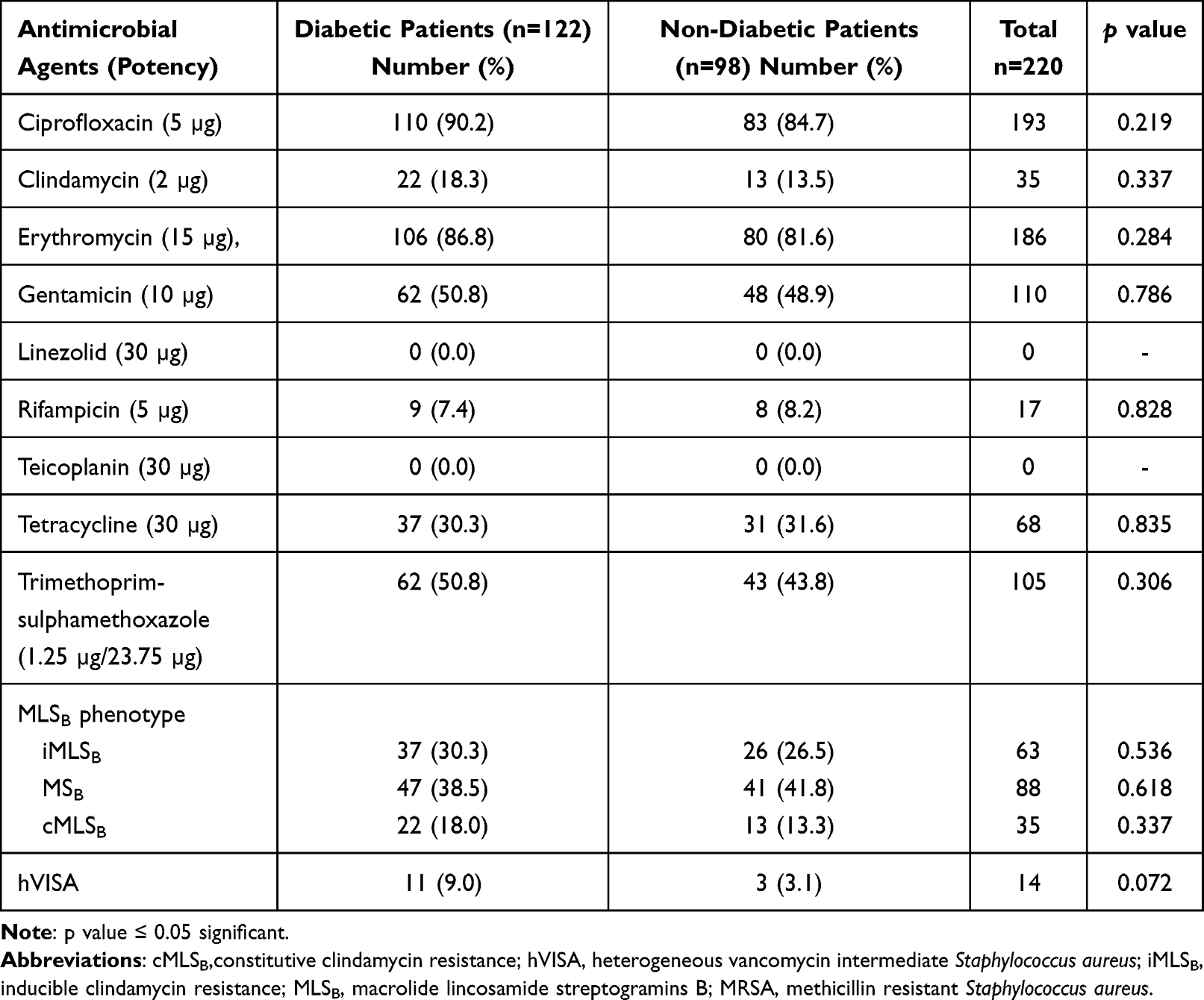 |
Table 2 Antimicrobial Resistance Profile of MRSA Strains Isolated from Diabetic and Non-Diabetic Patients |
Out of 220 strains of MRSA, 14 (6.4%) were confirmed hVISA by modified PAP-AUC method. None of the isolate was VISA. No statistically significant difference was observed in the rate of hVISA isolated from diabetic and non-diabetic patients (p = 0.072) (Table 2).
Although skin and soft tissue infection was most commonly caused by hVISA in diabetic patients, there were two cases of bacteremia also. Further, 10 out of 11 hVISA isolated from diabetic patients had MIC of vancomycin in the range 1–2 µg/mL (Table 3).
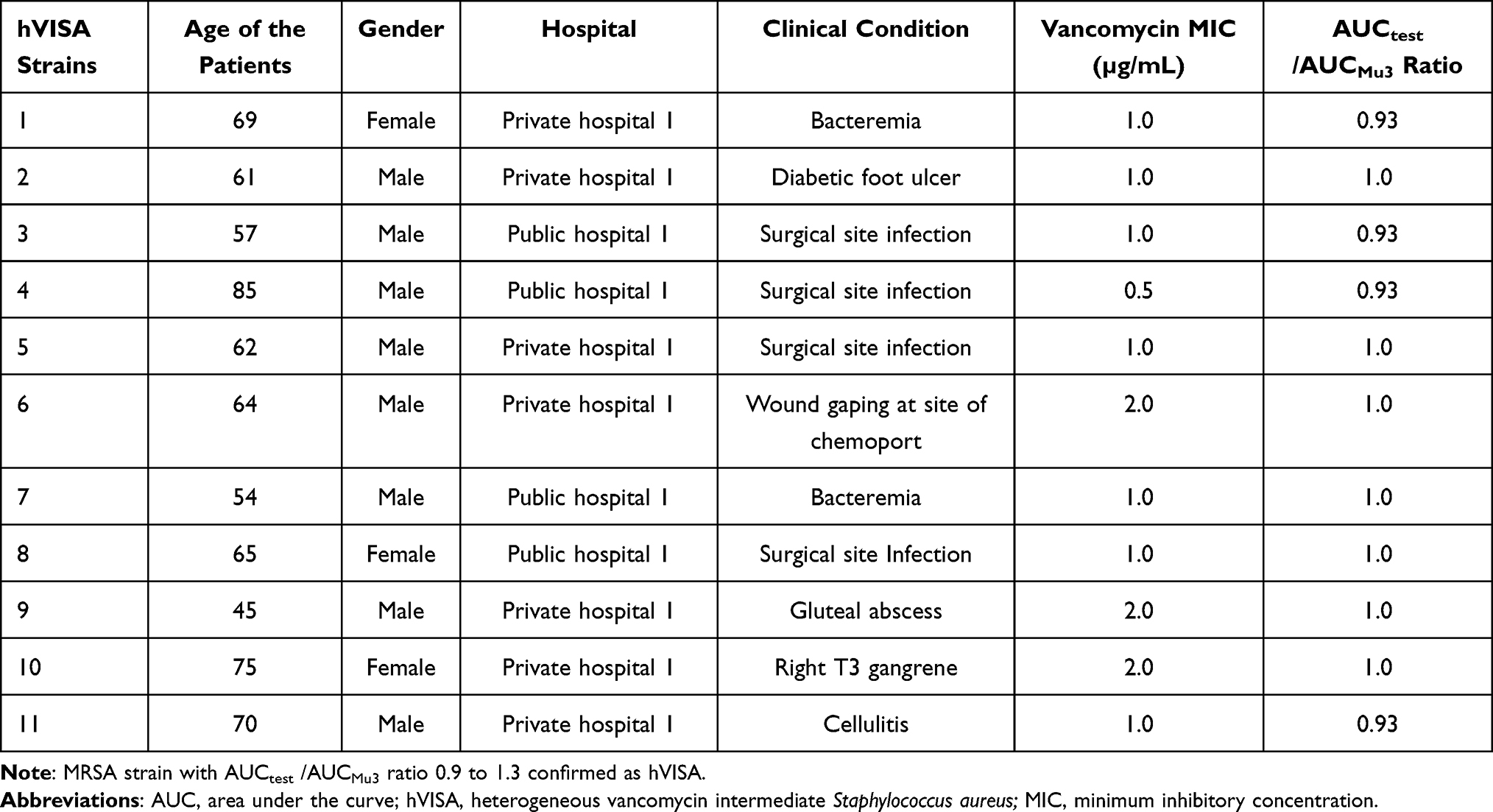 |
Table 3 Demographic and Clinical Details of Diabetic Patients Infected with hVISA |
Discussion
The rate of methicillin resistance among S. aureus isolated from HAIs was 33.1% in our study. The rate of MRSA infections varies widely across the country.17,21,22 A previous study conducted in 2016, in the same study setting, showed methicillin resistance at a rate of 30.2%.23 This shows that the rate of MRSA has increased in the study area. Further, a higher rate of HA-MRSA (38.6%) was reported in a study from Mangalore, India.21 Another study has reported an increase in the prevalence of MRSA from 28.0% in 2017 to 35.1% in 2019.24 The prevalence of MRSA infection is often high among diabetics than non-diabetics.14,25 The results of the present study are consistent with this observation. Patient population, geographical area, previous use of antibiotics, sample size, and testing methods may affect the reported rate of MRSA.26
We compared the type of infections caused by MRSA among diabetic and non-diabetic patients. Skin and soft tissue infections were more than deep infections. Diabetic patients, had significantly higher rates of foot infections and osteomyelitis than non-diabetic patients. Our results are consistent with those of Shah and Hux, who reported four-fold higher rate of osteomyelitis among diabetic patients.27 Furthermore, in a recent investigation from South India, MRSA was a significant pathogen in bone infection.15 S. aureus is the most common pathogen isolated from diabetic foot infections, primarily in Western countries.28,29
In the present study, all MRSA isolates were susceptible to linezolid, and teicoplanin, which is in agreement with observations of previous studies.23,30 Over 80.0% of MRSA isolates were resistant to ciprofloxacin and erythromycin in our study. This is consistent with results of a previous study.25 No statistically significant difference was observed in antimicrobial resistance profile of MRSA strains isolated from diabetic and non-diabetic patients. About 72.3% of MRSA were multidrug resistant, leaving limited options for treatment.
Macrolide, lincosamide and streptogramin B (MLSB) are distinct family of antibiotics.31,32 Clindamycin, a member of the MLSB family, is effective in the treatment of MRSA skin and soft tissue infections.32,33 Inducible clindamycin resistance (iMLSB) limits the use of clindamycin as a therapeutic agent.31,33 These strains appear resistant to erythromycin but susceptible to clindamycin in disk diffusion test and are unnoticed;31 therefore, MRSA strains resistant to erythromycin but susceptible to clindamycin should be tested by D-test to detect any inducible clindamycin resistance. In our study, 30.0% of MRSA isolated from diabetic and 26.5% MRSA isolated from non-diabetic patients were D-test positive (Inducible clindamycin resistance detected).
The rate of hVISA among MRSA was 6.4% in our study. Further, the rate of hVISA was three times higher in diabetic patients. The majority of hVISA infections among diabetic patients in our study were related to skin and soft tissue. However, there were two cases of bacteremia. There are reports of vancomycin treatment failure in hVISA infection.4,5,11,34 Therefore, it is essential to detect hVISA among MRSA isolated from diabetic patients before starting vancomycin treatment.
Although the current study did not reveal the presence of VISA and VRSA, the presence of hVISA among MRSA is a matter of concern. hVISA is considered the precursor of VISA.5,6 Therefore, we may expect the emergence of VISA in the future. Implementation of antimicrobial stewardship programme and infection control in the hospitals may help prevent rise in the rate of hVISA and its transmission.
Conclusion
The rate of hVISA among all MRSA strains isolated from healthcare-associated infections was 6.4%. The risk of hVISA infection was three times more in diabetic patients. The results emphasize the importance of the detection of hVISA among MRSA isolates especially from diabetic patients.
Abbreviations
ATCC, American Type Culture Collection; CDC, Centers for Disease Control and Prevention; CLSI, Clinical Laboratory Standard Institute; DFI, diabetic foot infection; DFU, diabetic foot ulcer; DM, Diabetes mellitus; HA, Healthcare associated; HAI, Healthcare-associated infection; hVISA, heterogeneous vancomycin intermediate Staphylococcus aureus; MDR, Multidrug resistance; MIC, minimum inhibitory concentration; MLSB, Macrolide lincosamide streptogramins B; MRSA, Methicillin resistant Staphylococcus aureus; PAP-AUC, Population analysis profile-area under the curve; VRSA, Vancomycin resistant Staphylococcus aureus; VISA, Vancomycin intermediate Staphylococcus aureus.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Statement
The study had approval of the Institutional Ethics Committee, Kasturba Medical College, Mangalore, India [Reference No: IEC KMC MLR 03-19/75 Dated 20-03-2019].
Acknowledgments
The authors gratefully acknowledge Department of Science and Technology, INSPIRE fellowship, Ministry of Science and Technology, Government of India for providing INSPIRE Fellowship to Sreejisha M. The authors are thankful to Department of Microbiology, Manipal Academy of Higher Education (MAHE), Manipal, India and to the Head of the Institution for providing the financial assistance, materials and infrastructure to conduct the study.
Funding
This project was funded by the Department of Science and Technology, INSPIRE fellowship, Government of India, Ministry of Science and Technology (Order No. DST/INSPIRE fellowship/2018/1F180903, date December 11, 2019) and Manipal Academy of Higher Education (MAHE), Manipal, India.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lakhundi S, Zhang K. Methicillin-resistant Staphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev. 2018;31(4):e00020–18. doi:10.1128/CMR.00020-18
2. Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Guo Y, Song G, Sun M, Wang J, Wang Y. Prevalence and therapies of antibiotic-resistance in Staphylococcus aureus. Front Cell Infect Microbiol. 2020;10:1–11. doi:10.3389/fcimb.2020.00107
4. Shariati A, Dadashi M, Moghadam MT, van Belkum A, Yaslianifard S, Darban-Sarokhalil D. Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis. Sci Rep. 2020;10(12689). doi:10.1038/s41598-020-69058-z
5. Howden BP, Davies JK, Johnson PDR, Stinear TP, Grayson ML. Reduced vancomycin susceptibility in Staphylococcus aureus, including vancomycin-intermediate and heterogeneous vancomycin-intermediate strains: resistance mechanisms, laboratory detection, and clinical implications. Clin Microbiol Rev. 2010;23(1):99–139. doi:10.1128/CMR.00042-09
6. Hiramatsu K, Kayayama Y, Matsuo M, et al. Vancomycin-intermediate resistance in Staphylococcus aureus. J Glob Antimicrob Resist. 2014;2(4):213–224. doi:10.1016/j.jgar.2014.04.006
7. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; 30th informational supplement M100, antimicrobial testing standards, M02, M07 and M 11. Wayne, PA; 2020.
8. Satola SW, Farley MM, Anderson KF, Patel JB. Comparison of detection methods for heteroresistant vancomycin-intermediate Staphylococcus aureus, with the population analysis profile method as the reference method. J Clin Microbiol. 2011;49(1):177–183. doi:10.1128/JCM.01128-10
9. Wootton M, Howe RA, Hillman R, Walsh TR, Bennett PM, MacGowan AP. A modified population analysis profile (PAP) method to detect hetero-resistance to vancomycin in Staphylococcus aureus in a UK hospital. J Antimicrob Chemother. 2001;47(4):399–403. doi:10.1093/jac/47.4.399
10. Charlton CL. Detection of VRSA, VISA and vancomycin-heteroresistant Staphylococcus aureus (hVISA)
11. Van Hal SJ, Paterson DL. Systematic review and meta-analysis of the significance of heterogeneous vancomycin-intermediate Staphylococcus aureus isolates. Antimicrob Agents Chemother. 2011;55(1):405–410. doi:10.1128/AAC.01133-10
12. Goldrick B. First reported case of VRSA in the United States. Am J Nurs. 2002;102(11):17. doi:10.1097/00000446-200211000-00015
13. Macdonald KE, Boeckh S, Stacey HJ, Jones JD. The microbiology of diabetic foot infections: a meta-analysis. BMC Infect Dis. 2021;21(1):770. doi:10.1186/s12879-021-06516-7
14. Stacey HJ, Clements CS, Welburn SC, Jones JD. The prevalence of methicillin-resistant Staphylococcus aureus among diabetic patients: a meta-analysis. Acta Diabetol. 2019;56(8):907–921. doi:10.1007/s00592-019-01301-0
15. Karthik S, Babu L, Joseph M, Bhatt A, Babu T. Microbiology of diabetic foot osteomyelitis - Is it geographically variable? Foot. 2021;52:101878. doi:10.1016/j.foot.2021.101878
16. Kang YR, Kim SH, Chung DR, et al. Impact of vancomycin use trend change due to the availability of alternative antibiotics on the prevalence of Staphylococcus aureus with reduced vancomycin susceptibility: a 14-year retrospective study. Antimicrob Resist Infect Control. 2022;11(1):1–10. doi:10.1186/s13756-022-01140-9
17. Bakthavatchalam YD, Babu P, Munusamy E, et al. Genomic insights on heterogeneous resistance to vancomycin and teicoplanin in methicillin-resistant Staphylococcus aureus: a first report from South India. PLoS One. 2019;14(12):e0227009. doi:10.1371/journal.pone.0227009
18. Centers for Disease Control and Prevention. CDC/NHSN surveillance definition for specific types of infection. Available From: www.cdc.gov/nhsn/PDFs/Manual/17pscNosInfDef_current.pdf.
19. Baird D. Staphylococcus. In: Collee JG, Fraser AG, Marmion BP, Simmons A, editors. Cluster-Forming Gram-Positive Cocci. Mackie & McCartney Practical Medical Microbiology.
20. Zhang K, McClure JA, Elsayed S, Louie T, Conly JM. Novel multiplex PCR assay for characterization and concomitant subtyping of staphylococcal cassette chromosome mec types I to V in methicillin-resistant Staphylococcus aureus. J Clin Microbiol. 2005;43(10):5026–5033. doi:10.1128/JCM.43.10.5026-5033.2005
21. Preeja PP, Kumar SH, Shetty V. Prevalence and characterization of methicillin-resistant Staphylococcus aureus from community-and hospital-associated infections: a tertiary care center study. Antibiotics. 2021;10(2):197. doi:10.3390/antibiotics10020197
22. Archana G, Sinha A, Annamanedi M, et al. Molecular characterisation of methicillin-resistant Staphylococcus aureus isolated from patients at a tertiary care hospital in Hyderabad, South India. Indian J Med Microbiol. 2020;38(2):183–191. doi:10.4103/ijmm.IJMM_20_151
23. Kumari J, Shenoy SM, Baliga S, Chakrapani M, Bhat GK. Healthcare-associated methicillin-resistant Staphylococcus aureus: clinical characteristics and antibiotic resistance profile with emphasis on macrolide-lincosamide-streptogramin B resistance. Sultan Qaboos Univ Med J. 2016;16(2):175–181. doi:10.18295/squmj.2016.16.02.007
24. Lohan K, Sangwan J, Mane P, Lathwal S. Prevalence pattern of MRSA from a rural medical college of North India: a cause of concern. J Fam Med Prim Care. 2021;10:752–757. doi:10.4103/jfmpc.jfmpc_1527_20
25. Anwar K, Hussein D, Salih J. Antimicrobial susceptibility testing and phenotypic detection of MRSA isolated from diabetic foot infection. Int J of Gen Med. 2020;13:1349–1357. doi:10.2147/IJGM.S278574
26. Lee AS, Hermínia DL, Javier Garau JK, Malhotra-Kumar S, Peschel A. Methicillin-resistant Staphylococcus aureus. Nat Rev Dis Prim. 2018;4:18033. doi:10.1038/nrdp.2018.33
27. Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care. 2003;26(2):510–513. doi:10.2337/diacare.26.2.510
28. Dunyach-Remy C, Essebe CN, Sotto A, Lavigne JP. Staphylococcus aureus toxins and diabetic foot ulcers: role in pathogenesis and interest in diagnosis. Toxins. 2016;8(7):1–20. doi:10.3390/toxins8070209
29. Hosny M, Dunyach-Remy C, Dunyach-Remy C, et al.; Lavigne JPTIE of S aureus ADPWFI. Long-term intrahost evolution of Staphylococcus aureus among diabetic patients with foot infections. Front Microbiol. 2021;12:741406. doi:10.3389/fmicb.2021.741406
30. Kot B, Wierzchowska K, Piechota M, Gruzewska A. Antimicrobial resistance patterns in methicillin-resistant Staphylococcus aureus from patients hospitalized during 2015–2017 in hospitals in Poland. Med Princ Pract. 2020;29(1):61–68. doi:10.1159/000501788
31. Goudarzi M, Kobayashi N, Dadashi M, et al. Prevalence, genetic diversity, and temporary shifts of inducible clindamycin resistance Staphylococcus aureus clones in Tehran, Iran: a molecular–epidemiological analysis from 2013 to 2018. Front Microbiol. 2020;11:663. doi:10.3389/fmicb.2020.00663
32. Wang W, Chen W, Liu Y, et al. Antibiotics for uncomplicated skin abscesses: systematic review and network meta-analysis. BMJ. 2018;8(2):5–7. doi:10.1136/bmjopen-2017-020991
33. Thapa D, Pyakurel S, Thapa S, et al. Staphylococcus aureus with inducible clindamycin resistance and methicillin resistance in a tertiary hospital in Nepal. Trop Med Health. 2021;49(1). doi:10.1186/s41182-021-00392-2
34. Holmes NE, Johnson PDR, Howden BP. Relationship between vancomycin-resistant Staphylococcus aureus, vancomycin-intermediate S. aureus, high vancomycin MIC, and outcome in serious S. aureus infections. J Clin Microbiol. 2012;50(8):2548–2552. doi:10.1128/JCM.00775-12
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.