Back to Journals » Psychology Research and Behavior Management » Volume 16
Heterogeneity in Adolescents’ Non-Suicidal Self-Injury Behaviour Trajectories Based on the Group-Based Trajectory Model and a Decision Tree Analysis of Family-Related Determinants
Received 12 July 2023
Accepted for publication 19 August 2023
Published 25 August 2023 Volume 2023:16 Pages 3359—3371
DOI https://doi.org/10.2147/PRBM.S427090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Linbo Li, Hui Yang
College of Nursing, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Hui Yang, College of Nursing, Shanxi Medical University, No. 56, Xinjian South Road, Yingze District, Taiyuan, Shanxi, 030001, People’s Republic of China, Tel +86 13834668531, Email [email protected]
Background: Non-suicidal self-injury (NSSI) is a global public health problem. While some studies have noted the importance of behavioural development patterns in NSSI, most NSSI research is based on cross-sectional survey data. Few studies explore the time-series heterogeneity of trajectories of NSSI symptoms and family-related influencing factors of NSSI.
Aim: The purpose of the study was to identify the heterogeneity in trajectories of adolescents’ NSSI behaviour and their family-related influencing factors.
Methods: The group-based trajectory model (GBTM) was used to identify the heterogeneity in the NSSI behaviour trajectories of 208 adolescents in China. Next, the decision tree model (DTM) was used to analyse which family related factors influence the trajectory type.
Results: The GBTM revealed two heterogeneous trajectories of NSSI behaviour: the high–risk and low-risk NSSI behaviour groups. Next, DTM’s average accuracy was 83.2%. A total of seven independent variables were used for the DTM: gender, number of NSSIs in the past month, and family economic, family structure, family conflict, parental psychological control, parental behavior control and family intimacy risks. Family conflict risk was located at the root node and was the most important factor.
Conclusion: Heterogeneity within the population should be considered in the management of adolescents’ NSSI behaviours. Further, from the perspective of family system theory and cumulative risk, focusing on the adverse effect of multiple risk factors on adolescents’ NSSI addiction is more meaningful rather than the impact of single risk factors. Studies that use time series data should focus on the trend of dynamic changes in NSSI addiction characteristics over time.
Keywords: non-suicidal self-injury, group-based, heterogeneity, trajectory, decision tree, influencing factor
Introduction
Non-suicidal self-injury (NSSI) is most commonly defined as deliberate and intentional damage to one’s body without suicidal intent;1,2 the methods include cutting, hitting, scratching, and burning oneself.3 Crucially, it has become a global public health problem.4,5 Adolescence is a critical period for children to transition to adulthood. During this period, their mental health education is mainly provided by the school, family, and society. However, due to immature cognitive behaviour patterns and emotional management skills, adolescents are more likely to turn to NSSI to vent their emotions when they encounter stressful events.6 NSSI reporting or detection in adolescents in different countries varies greatly due to differences in the definition of NSSI behaviour, measurement methods, and sample representation.7 For instance, the NSSI detection rate among adolescents in the US is 17.2%.8
A longitudinal study of NSSI by Plener et al showed that self-injurious behaviour typically occurs in early to middle adolescence, with an increasing incidence of self-injury throughout adolescence.9 NSSI can not only cause significant physical and psychological pain to middle school students but also raise the chance of self-injury in the future, thereby increasing the burden on society and families. Furthermore, NSSI has been linked to a variety of psychiatric issues, including depression, anxiety, and post-traumatic stress disorder.10 In 2018, 48,344 people died by suicide just in the US.11 Furthermore, suicide rates in the country have increased by 30% since 1999,11,12 indicating that NSSI has become a serious global public health concern, particularly among adolescents.13–16 Moreover, NSSI recurrence in adolescents is extremely high today and can even become an addiction. Some studies have defined NSSI recurrence of more than five times as severe relapse and addiction. Systematic reviews have also shown that NSSI can be conceptualised as addiction.17 As such, corresponding intervention strategies have been formulated and scientific interventions have been implemented to reduce its recurrence.17,18 In summary, NSSI has serious adverse effects on adolescents themselves, their parents, and even the entire family.19,20 Meanwhile, it also causes serious resource wastage for the clinic as well.21
Interestingly, research indicates that NSSI behaviour constantly changes22 with time, disease status, and family factors. Changes or heterogeneity in NSSI behaviour over the course of adolescents’ illness can be important indicators of further suicide.23 For instance, certain individual exhibit increasingly worsening NSSI behaviour, especially those who require emergency services.24 Latent growth curve modelling reveals three self-injury trajectories: stable-low, low-increasing, and increasing-decreasing trajectories. Thus, self-injury may have multiple directions of development during adolescence.25 Other studies have divided NSSI behaviour into two distinct trajectories of suicidal behaviours: low-decreasing and high-increasing NSSI groups26 High-increasing groups showed higher NSSI behavior, feelings of helplessness, and depressive symptoms compared to low-decreasing groups. Reasons for living served as protective factors in high-increasing group. Psychological interventions aimed at reducing the influence of risk factors and bolstering reasons to live may help to decrease the risk of suicide and NSSI behaviors. NSSI behaviour can also differ between sexes, age groups, geographic regions, and sociopolitical settings. Further, its relationship varies with different risk factors, suggesting the presence of heterogeneity in NSSI behaviours.27 Some studies have identified two NSSI subgroups and the factors associated with each subgroup.28 Crucially, identifying factors correlated with NSSI can help in the early identification of high-risk NSSI groups in adolescents diagnosed with depression. Overall, while exploring the heterogeneity in NSSI trajectories is vital, the corresponding studies have some inconsistencies, suggesting the need for future research.
Furthermore, a history of NSSI may result in increased pain tolerance and decreased fear of death, leading to recurrent NSSI behaviours.29 According to the ecosystem theory, individuals do not exist and develop in isolation. Their physical and mental development is not affected by a single factor, but by multiple environmental or personal factors, such as family, school, and peers. The family is the first school in life. As an important microsystem that affects an individual’s physical and mental development, the family plays an important role in the mental health development of adolescents. Drawing on family system theory, extensive evidence shows that the family is a dynamic and interactive system with interdependent factors at multiple levels. Factors at the family level as a whole and at the individual level play an important role in shaping and influencing children’s development. However, risks in the family environment can impair the academic, mental, and physical health of individuals.30–32
While the impact of individual household risk factors on problem behaviour is important, people are often affected by multiple risk sources. According to the cumulative risk model, these risk factors work together to cumulatively affect individuals.33 When a person is exposed to multiple risk factors, multiple risks create complex interactions and additive effects. In addition, the more risk factors interact, the stronger their negative impact on people, thereby contributing to problem behaviours.34 In our context, the various risk sources in the family can also have a cumulative effect.
We focused on three categories of core family-related influencing factors based on the family ecosystem theory and cumulative risk model: family structure, insufficient household resources, and family atmosphere. Family structure risk was measured by parents’ marital status. The risk of insufficient household resources was measured by parents’ education level and family financial difficulties. Finally, family atmosphere risk was measured using family intimacy, family conflict, parental behaviour control, and parental psychological control.
In summary, although NSSI is a public health concern, there is little information about its progression, and consequently, the risk factors for adolescents’ NSSI behaviours. As a finite hybrid model, the group-based trajectory model (GBTM) is often used to identify heterogeneous populations in development trajectories. Here, using longitudinal tracking data, we drew on the GBTM to explore the change in trajectory of adolescents’ NSSI behaviours and used DTM analysis to analyse the family-related factors influencing the trajectory type. The GBTM can also help us describe the overall longitudinal course and latent trajectory classes of NSSI in a population-based sample of adolescents using multi-wave data. We hope that this study’s insights can provide ideas for the prevention of and, if needed, interventions in NSSI behaviours.
Materials and Methods
Research Design
This study adopted a prospective longitudinal study design. NSSI behavioural addiction among adolescents was evaluated at discharge at baseline (patient admission, T0), when discharged (T1) and 1 (T2), 3 (T3), and 6 months (T4) after baseline assessment. The independent variables were assessed at admission.
Participants
According to the sample size estimation method of multivariate analysis, the total sample size should be at least 5–10 times the number of independent variables. As the number of independent variables in this study is 16, at least 160 cases are needed. Considering a 20% loss to follow-up, the final sample size was determined to be 208 cases. From September 2022 to May 2023, data were collected from NSSI adolescents hospitalised in the psychiatry department of a Chinese tertiary general hospital using purposeful sampling. Participants had to meet the following inclusion criteria: (a) fulfilled the Part III of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) for NSSI; (b) between 13–18 years; (c) no gender restriction; (d) were hospitalised patients who can be followed up on; and (e) provided informed consent on their voluntary participation. This research adheres to the voluntariness principle, respecting and safeguarding the privacy of research participants. Participants were excluded if they: (a) had strong suicidal ideation; (b) had concomitant schizophrenia, delusional illness, anxiety disorder, mental retardation, and autism now or before; (c) were psychoactive substance abusers; and (d) had serious physical diseases.
Ethical Considerations
This study did not use data from experimental animals and human tissues. All researchers agreed that the study was complied with the Declaration of Helsinki and general principles of research involving human subjects. It did not involve any physical and psychological harm to the researcher or research subjects. An informed consent form, which included the risks and benefits explanation, study purpose, study significance, interview duration, methods of data collection, disposal of the research results, and publication of anonymised responses, was provided to the participants and their parents. While asking participants and parents/guardians for consent, they were assured that the while individual demographic details would be published, their names would be not be disclosed. Participants could backout of the research at any point of time. This ethical attitude informed the entire research process to ensure that respect and tact were demonstrated toward participants. Only those provided consent participated. The study was approved by the Ethics Committee of the First Hospital of Shanxi Medical University (approval number: NO.KYLL-2023-015).
Data Collection
Clinical Observation Index Collection Questionnaire
Following extant research, consultations with psychiatric professionals, and the hospital’s real circumstances, the clinical observation index collection questionnaire collected the following information from participants: (a) gender; (b) age; (c) education degree; (d) NSSI history; (e) whether they were the only child; (f) whether they take medication regularly; (g) any NSSI recurrence; (h) parents’ marital status; and (i) whether participants live with parents.
The Family Adaptability and Cohesion Evaluation Scale
The Family Adaptability and Cohesion Evaluation Scale (FACES II) was developed by Olson et al.35 Fei et al revised this scale and added cohesion, which measures the emotional connection between family members.36 The scale contains 16 questions, which can be answered on a five-point scoring from “not” to “always”; the higher the questionnaire score, the higher the family intimacy. Here, FACES II’s internal consistency coefficient is 0.896, indicating good reliability.
Family Environment Scale-Contradiction Subscale
The Chinese version of the Family Environment Scale (FES-CV) was revised by Fei et al based on the “Family Environment Scale (FES)” compiled by American psychologist R. H. Moss. We focus on conflict in the family environment, so we used this subscale. Its Contradiction Subscale was used to assess the degree of family conflict using nine items: 0–1 are for low conflict, 2–5 are for medium conflict, and 6–9 are for high conflict. The retest reliability of the contradiction subscale is 0.73, and the Cronbach’s α is 0.67.36
Parental Control Scale
This study used the Chinese version of the Parental Control Scale revised by Wang et al.37 This scale retrospectively measures the degree of control in parenting using two dimensions: psychological and behavioural control. Psychological control is measured using 18 questions on three factors: insisting on authority, triggering feelings of guilt, and withdrawing love. There are 16 questions on behavioural control on two factors: questioning and limiting. Responses are measured on a five-point Likert scale (1 for never and 5 for always); the higher the score, the more control parents have over their children. Here, the Cronbach’s α of the psychological and behavioural control scales were 0.93 and 0.87, respectively, indicating good consistency.
NSSI Behavior Scale
The NSSI Behavior Scale was revised by Chen based on the Ottawa Selfinjury Inventory.38 The scale consists of three subscales: NSSI Thought and Behaviour Frequency, Addiction Characteristics, and Function Scale. Addiction scores range from 0–28 points, with higher scores indicating greater addiction. The Cronbach’s α of the NSSI Thought and Behavior Frequency Subscale was 0.799, and its fractional confidence coefficient was 0.714. The Cronbach’s α on the Addiction Characteristics Scale was 0.798, with a fractional confidence factor of 0.727 and retest confidence factor of 0.466. These results show that the scale has good reliability, content validity, and structural validity.
Data Collection Procedure
Prior to data collection, the patients and their primary caregivers were told of the study’s goal and relevance in detail; thankfully, they willingly provided informed consent. When a patient was discharged from the psychiatry ward, all scales were appraised according to the doctor’s order. The data collection was conducted by two graduate students with the assistance of two certified head nurses. All data collection staff in the psychiatry unit were registered nurses.
The goal and methodology of the study, time and manner of data collection, and quality control points of each connection were covered in investigator training. Data from the hospital’s medical record information system were collected in strict conformity with the operational criteria. The staff reminded each other whether mutual supervision was completed within the allotted time in accordance with ethical standards and quality control requirements. The instructor conducted the final quality assurance. Every Friday afternoon, members of the research team provided active comments on issues that surfaced during data collecting and discussed recurring issues.
The patients in the psychiatry unit completed the surveys in accordance with a unified set of instructions. Those who were unfamiliar with the surveys or had trouble writing were provided with detailed explanations of the questions and appropriate assistance. The questionnaires were gathered promptly after completion, and the acquired data were stored by a project manager and not altered arbitrarily. After a patient was discharged, we mostly followed up with them by telephone and inquired whether they had NSSI. After the data were gathered, two data entry operators inputted and double-checked the data.
Data Analysis
We constructed a GBTM and DTM for our analyses. All statistical analyses were conducted using SPSS 25.0 and Stata 17.0. Data conforming to the normal distribution were described as  , where
, where  is the mean and s is the standard deviation, and t-tests were used for comparison between groups. Next, count data were described as rates (percentages), and χ2, or the Fisher exact test, was used for comparisons between groups. Note that variables that were meaningful to one factor were included in the decision tree analysis.
is the mean and s is the standard deviation, and t-tests were used for comparison between groups. Next, count data were described as rates (percentages), and χ2, or the Fisher exact test, was used for comparisons between groups. Note that variables that were meaningful to one factor were included in the decision tree analysis.
We used the GBTM to explore the heterogeneity of total scores of NSSI addiction trends. GBTM identifies individual classes with similar trajectories by maximum likelihood estimation. Meanwhile, DTM was used to examine which family related factors determine the trajectory type. DTM identifies several subgroups with different trajectory types. Since the total score of NSSI addiction is continuous and can be regarded as an approximate normal distribution, the censored normal model was chosen for fitting. Fitting began with a small number of subgroups. Each subgroup had a higher-order function; the subgroup was removed if the higher-order function was meaningless and remained if it could fit a low-order function. The optimal model was selected according to Bayesian information criterion (BIC) and average posterior probability (AvePP). The closer the BIC is to zero, the better the model fit. Meanwhile, AvePP>0.7 indicates that the model is acceptable. The entropy range of 0–1 was used to evaluate the classification accuracy of the category; the closer the value is to 1, the higher the classification accuracy. The test direction was bilateral, and the difference was considered statistically significant at P<0.05.
The growth process of the decision tree was based on the growth method. The decision tree was constructed by a difference criterion with a maximum of 1 standard error to avoid overfitting. The parent and child nodes were 10 and 5, respectively, when the minimum number of cases was set. The CRT method was used for growing the decision tree.
Findings
Participant Characteristics
In total, 208 adolescents participated, including 144 females (69.23%) and 64 males (30.77%). The mean age of the low-risk and high-risk NSSI groups were 15.83±2.002 and 15.51±1.718, respectively. Education levels included junior high school to high school, and junior college, among others. 81 adolescents performed NSSI behavior again, while 127 had experienced it for the first time. 50 patients were the only child for their parents. The general information of the participants is shown in Table 1.
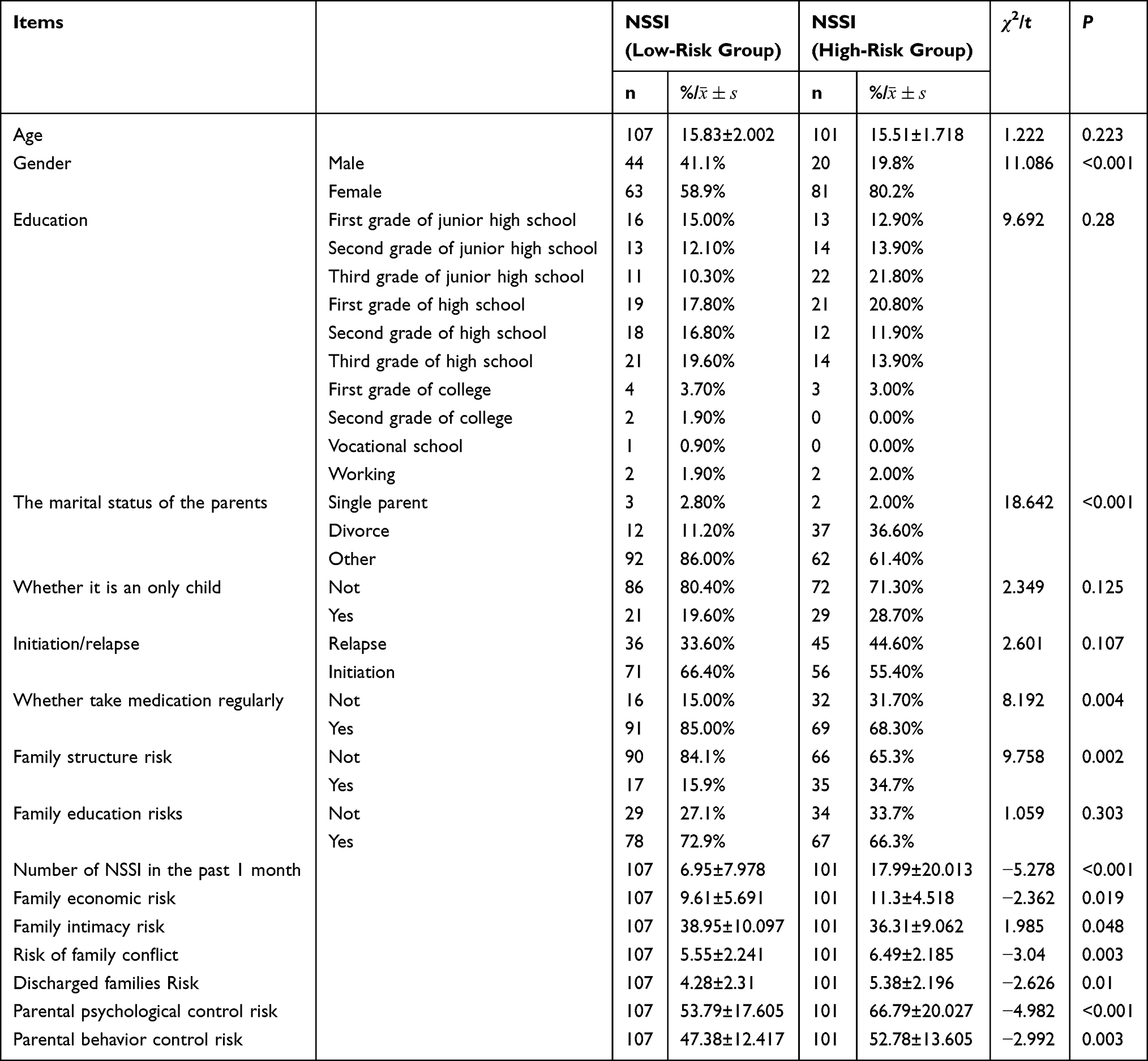 |
Table 1 Basic Characteristics and Univariate Analysis of Grouping of Heterogeneity of Trajectories |
Grouping of Heterogeneity of Trajectories
We fit the development trajectories of NSSI addiction scores according to different groups (1–5 groups) and functional forms (intercept, linear, square, cubic). By comparing BIC and AvePP, the optimal number of trajectory types was set to two groups. As the entropy was 0.46, the model was the most stable and accurate, and AvePP was greater than 0.98 with BIC = −3083.34. The comparison of the results of fitting evaluation indicators between different models of generalised method of moments (GMM) is shown in Table 2. The identification grouping of heterogeneity of trajectories by GMM (n = 208) is shown in Figure 1. The NISS trajectories of patients with different trajectory groups did not significantly differ. Therefore, the trajectories were grouped according to the entropy scores. The grouping of heterogeneity of trajectories is shown in Figure 2.
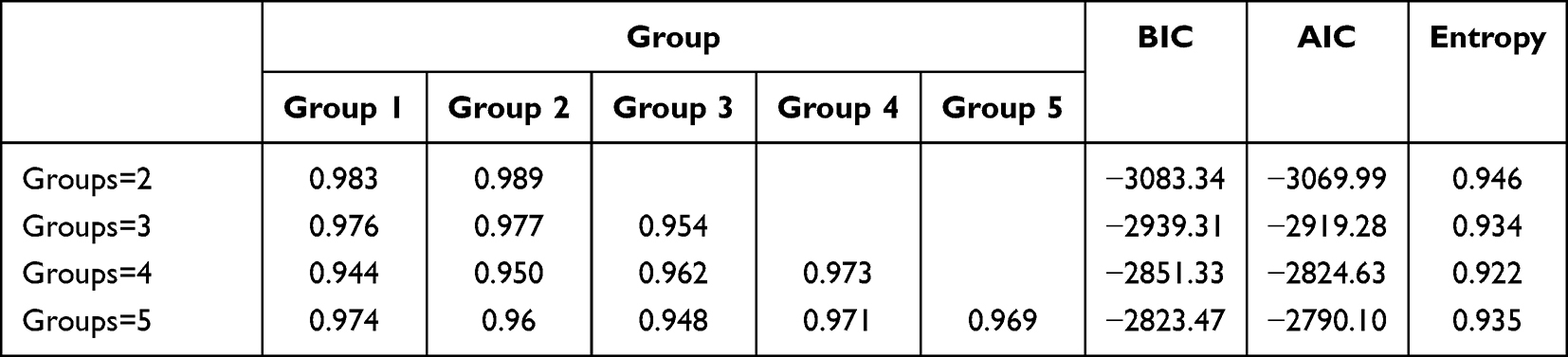 |
Table 2 The Comparison of the Results of Fitting Evaluation Indicators Between Different Models of GMM |
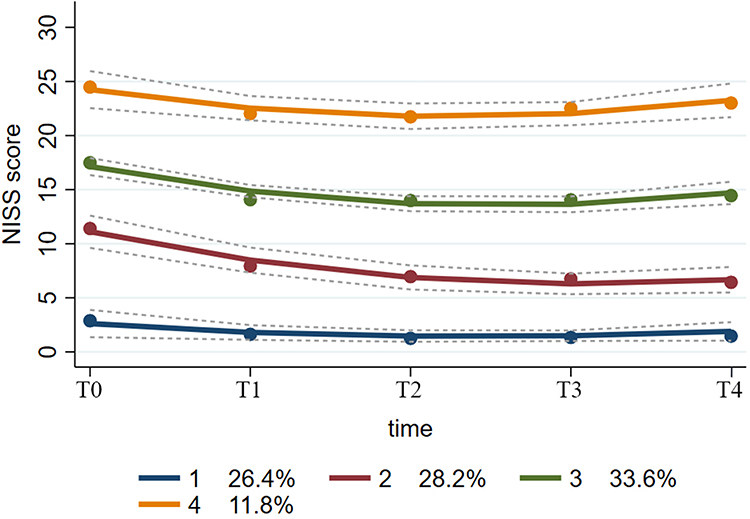 |
Figure 1 Identification grouping of heterogeneity of trajectories by GMM. |
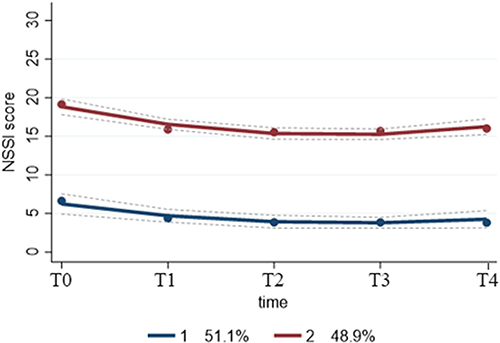 |
Figure 2 Grouping of heterogeneity of trajectories. |
Trajectory type 1, defined as the low-risk NSSI group, had 107 patients (51.4%), while trajectory type 2, defined as the high-risk NSSI group, had the remaining 101 patients (48.6%). The basic characteristics and univariate analysis of grouping of heterogeneity of trajectories is shown in Table 1.
Univariate Analysis
Univariate analysis showed that gender, parents’ marital status, regularly taking medicine (0: irregular; 1: regular), family structure risk, number of NSSI in the past month, family economic risk, family intimacy risk, family conflict risk, discharged family conflict risk, parental psychological control risk, and parental behaviour control risk were all associated with the patient’s NSSI addiction score (all P < 0.05).
Construction of a Decision Tree Model of Subgroup of Heterogeneity of Trajectories’ Influencing Factors
In total, 11 variables were significant in the univariate analysis. The significant independent variables were incorporated into the DTM shown in Figure 3.
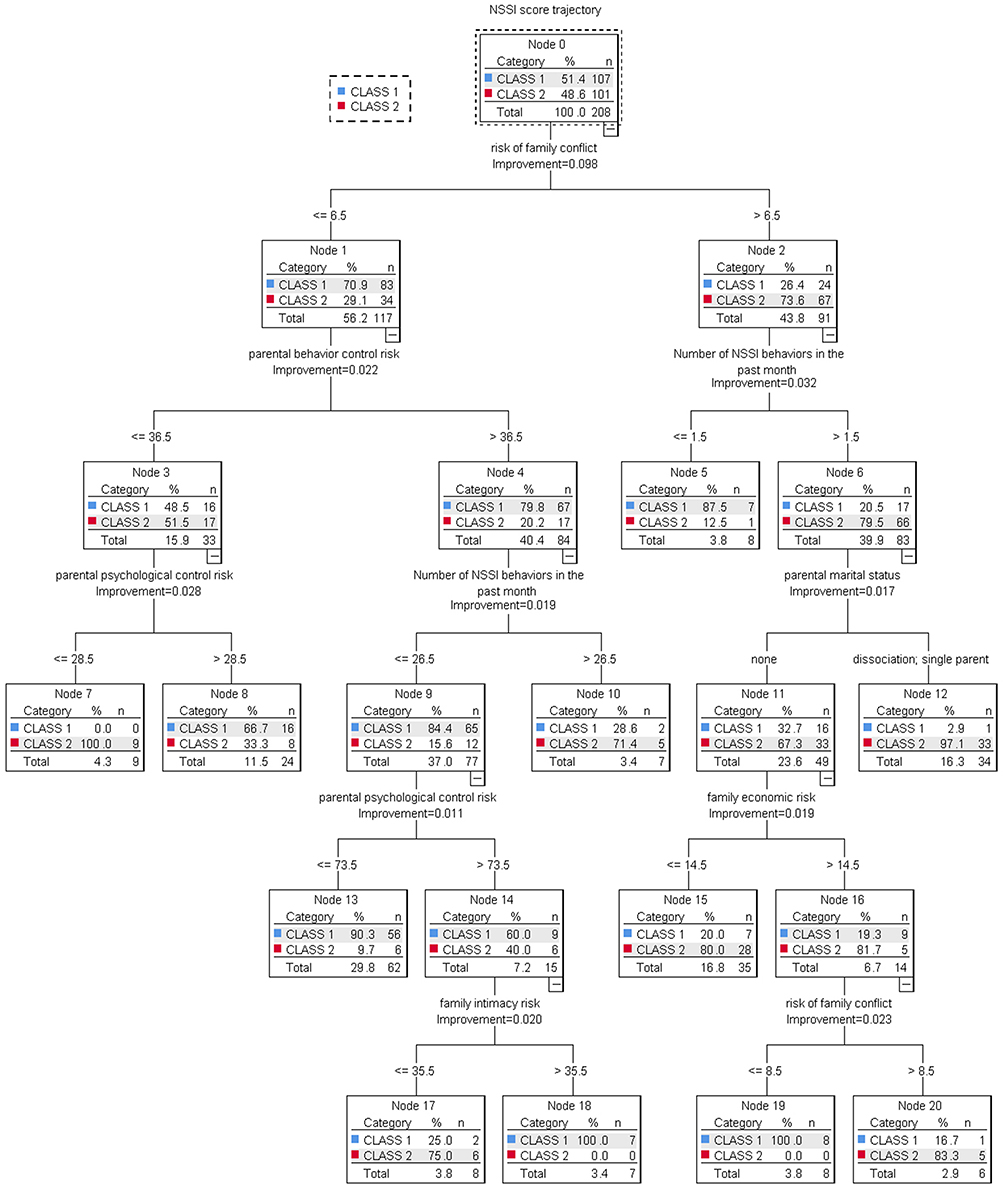 |
Figure 3 A decision tree prediction model for the NSSI behavior Heterogeneity of trajectories. |
This DTM’s average accuracy was 83.2%. Seven family related independent variables were used in the DTM: risk of family conflict, number of NSSI in the past month, family economic risk, marital status of parents, risk of parental psychological control, risk of parental behavior control and risk of family intimacy. Risk of family conflict was located at the root node and was the most important factor. Adolescents with a risk of family conflict exceeding 6.5 had higher probabilities of developing high-risk NSSI behaviours than those with a lower risk of family conflict (73.6% versus 29.1%). When adolescents at greater risk of family conflict (>6.5 points) and had higher number of NSSI behaviours in the past month (>1.5 times), the probability of high-risk NSSI behaviours significantly increased from 12.5% to 79.5%. If this population is further classified, compared with non-divorced or non-single-parent families, the probability of developing NSSI behavior was 97.1% versus 67.3%. Parental behavior control exceeding 24.5 points are more likely to develop NSSI behaviours. Further categorizing the population with a parental control score of >38.5, if the number of NSSI behaviors in the past month > 26.5, the probability of subsequent NSSI behaviors increased from 15.6 to 71.4%. Adolescents with a family economic risk than 14.5 points were more likely to develop NSSI behavior, and further classified it, the probability of adolescents developing NSSI behavior increased significantly if there was a risk of family conflict. If parents’ psychological control scores greater than 73.5 points were further classified, adolescents with a score of than 73.5 were more likely to develop NSSI behaviours (40% versus 9.7%). But if the closeness of the parents is high, even in the presence of psychological control, the probability of NSSI in adolescents can be reduced. Economically at-risk households have a significantly increased probability of NSSI if they combine family conflicts at the same time.
Discussion
Heterogeneity in the Trajectories of NSSI Behaviours in Adolescents
The self-regulation common sense model39 shows that with the progress of disease and treatment, the individual’s disease manifests itself as a dynamic change process of continuous correction and adjustment. From admission to 6 months after discharge, the high-risk group is the focus of our clinical staff. Measurements at different time points can more comprehensively determine the persistent high-risk group and the trend of their NSSI behavior. Consistent with previous findings,40 we found two heterogeneous trajectories of NSSI behaviour: high- and low-risk NSSI behaviour groups. The growing literature on the heterogeneity of NSSI behavioural trajectories typically identifies two to four developmental trajectories that reflect the severity and stability of NSSI behaviour.40,41 The heterogeneity of NSSI behavioural addiction trajectories suggests the importance of developing policies and interventions specific to each trajectory to reduce NSSI behaviour more effectively. However, we need to define these different subgroups of NSSI behaviour trajectories, understand their characteristics, and explore the risk factors influencing NSSI behaviour in each trajectory. For instance, some of the heterogeneity may be better represented by the underlying biological processes, perhaps even representing subgroups that can benefit from different types of interventions.42 Therefore, further subgroup analyses based on microscopic indicators will have important clinical value.
NSSI has obvious characteristics of behavioural addiction, which is a way to vent emotions.18 If an individual’s negative emotions decrease immediately after the occurrence of NSSI, their tendency to implement this behaviour will strengthen when they have negative emotions in the future. Moreover, as a repetitive and fixed behaviour, NSSI’s self-reinforcing nature can easily manifest as an avoidance strategy with the passage of time,43 thus exhibiting addictive characteristics. This can make it more difficult to mitigate NSSI behaviours.
While NSSI and patients’ suicidal impulse are not directly related, after NSSI behaviour loses its function of regulating emotions, the risk of adolescent suicidal behaviour may greatly increase.44,45 Hence, high-risk NSSI adolescents may be at greater risk of suicide, with irreversible consequences for their families and themselves. This group of adolescents should be the focus of clinical attention. Healthcare professionals should further identify their subgroup characteristics and develop targeted interventions to reduce the addictiveness of their NSSI behaviours.
In addition, we found that NSSI behaviour in adolescents increases three months after discharge.Thus, for both high-risk and low-risk NSSI groups, three months of intensive intervention and early recognition of the prodromal symptoms of NSSI behaviour may be life-critical in clinical work.
The Family Core Risk Factors on Adolescents’ NSSI Behaviour are Cumulative
The DTM showed that the risk of family conflict was an important predictor of NSSI addiction. Studies have found similar risk factors, including major family conflict and poor relationships with caregivers.46 Adolescents at high risk of family conflict have fewer opportunities to feel the warm love and understanding of their parents, and are more likely to vent their negative emotions through hurtful behaviour or seek the attention of those around them.47,48
A history of NSSI may result in increased pain tolerance and decreased fear of death, leading to recurrent self-harming behaviours.29,49 Patients with a history of NSSI are more likely to struggle with emotional management and self-efficacy resistance.50 This can influence the associations between outcome expectations and NSSI history.29 Moreover, if parents are divorced and family intimacy is low, NSSI behaviours are more likely. Meanwhile, even if there are fewer NSSI episodes in the past month, the probability of developing NSSI addiction may increase significantly if the family is at higher financial risk and there is conflict in the family. A family’s financial crisis may also increase adolescent’s coping with life stress, who may forcibly release their anger and depression by adopting NSSI behaviour.51 Further, the DTM showed that the probability of NSSI behaviour in adolescents increases sharply under parental psychological control.
Family intimacy is a reflection of family affinity. Close relationships and family atmosphere can promote communication between family members and help form a good parent-child relationship. Family intimacy is positively correlated with psychological resilience and negatively correlated with adolescent NSSI behaviour.52 High-intimacy families create a good living environment for adolescents, and are crucial for their physical and mental health development. Consequently, interventions can prevent or reduce the occurrence of NSSI behaviours in adolescents by improving family intimacy and improving parent-child relationships.
Next, while parents see increased control over teens as a sign of affection, teens may feel that their parents’ behaviour toward them is an invasion of privacy, a threat to autonomy, and a greater distrust of parents.53 This, in turn, may increase the frequency and severity of NSSI behaviour in adolescents. Parental psychological control makes it difficult for adolescents to develop effective cognitive and emotional regulation strategies, decreasing their ability to cope with emotional crises. Then, they are more likely to adopt NSSI, which is a rapid and effective compensatory response.54
Children of divorced families need stronger psychological resilience to cope with changes in family structure, and even endure loneliness for a long time. Furthermore, their home education system is usually in an incomplete state. Hence, they are more likely to adopt harmful behaviours than children with complete family structures.55 The family’s financial crisis may increase the adolescent coping with life stress, forced to release his anger and depression by adopting NSSI behaviour. Parents with psychological control can deprive adolescents of their autonomy in thoughts, emotions, and other inner activities, impose their own wishes and requirements on adolescents.56 Consequently, adolescents, in the process of “separation-individualisation”, may feel strong pressure.57 This may easily produce depression, anxiety, and other negative emotions. Then, adolescents may turn to NSSI to quickly alleviate these negative emotions. NSSI also has the function of interpersonal influence. Adolescents may adopt NSSI to attract the attention of their parents, express dissatisfaction with their parents’ psychological control, and hope to get parental responses to their emotional and psychological needs. Therefore, parental psychological control can significantly positively predict adolescent NSSI behaviour.54 However, not all teens with NSSI behaviours have a negative view of their relationship with their parents. For example, perfectionists who have a good parent-child relationship with their parents tend to experience more pressure to meet their parents’ expectations, which may lead them to NSSI behaviour.58 Parent-child relationship is multifaceted; future research should explore whether individuals with different views on parent-child relationship have different NSSI behaviours, as well as the relationship between the various combinations of this characteristic relationship, and different cognitive and behavioural aspects displayer by adolescents with NSSI.
Therefore, the decision tree analysis of influencing factors shows that focusing on the adverse effect of multiple risk factors on adolescent mental health is more meaningful rather than the impact of an individual risk factor. An individual’s physical and mental development is less sensitive to single or a few risk factors; rather, individuals exposed to more risk factors are more likely to have more serious problematic behaviours. Hence, a composite index of multiple risk factors can be helpful for objectively examining the impact of risk factors on the behaviour of adolescents with NSSI.
Conclusions
Based on the GBTM, this study found two heterogeneous trajectories of NSSI behaviours: high–risk and low-risk NSSI behaviour groups. Thus, research involving time series data should pay attention to the trend of dynamic changes in NSSI addiction characteristics over time. Furthermore, the potential heterogeneity within the population should be considered in the management of NSSI behaviour in adolescents. The decision tree analysis of family-related risk factors influencing the trajectories showed that gender, number of NSSI in the past month, family economic risk, marital status of parents, risk of family conflict, risk of parental psychological control, and risk of family intimacy were all influential. Notably, family conflict risk was located at the root node and was the most important factor. Overall, our findings show that focusing on the adverse effect of cumulative risk factors on adolescents’ NSSI addiction is more meaningful rather than that of single risk factors from the family system theory and cumulative risk perspectives.
Implications for Health Professionals, Policymakers, and Parents
We help identify the high–risk and low-risk NSSI behaviour groups, which have different trajectories of behaviours with different associated factors. Thus, targeted prevention and treatment interventions need to be tailored to the trajectory characteristics of different subgroups. For the low-risk NSSI behavioural group, interventions should pay more attention to medication adherence, regular follow-up, consolidation of emotional regulation strategies. In addition, healthcare professionals should strengthen the detection of precursor indicators of NSSI behavior to prevent their further transformation into high-risk groups. Naturally addressing the behaviours of adolescents with high NSSI addiction is difficult. Hence, besides active comprehensive treatment, early identification of risk factors and intervention are crucial. For high-risk groups, we should provide symptomatic interventions based on high-risk factors. For example, dialectical behavior therapy, family cumulative risk intervention strategies(DBT), nonviolent communication education, emotion regulation strategies, and dangerous goods management are used to reduce the addiction of NSSI behavior and help high-risk adolescents transform into low-risk groups.
Next, focusing on the decision tree model of family core risk factors, researchers and health professionals should examine the influence of family structure, resources, and atmosphere on NSSI behavioural addiction from the perspectives of family system theory and cumulative risk. Thus, even on admission in a treatment facility, the focus should be on identifying the adolescent’s NSSI behaviour history as well as assessing family intimacy, family conflict, and parental control over the child. Meanwhile, while parenting, parents should create a harmonious and warm family atmosphere for children, reducing psychological control over adolescents, increasing tolerance of adolescents’ individual independence and personality, and giving adolescents appropriate autonomy in personal issues for development attempts. This study advocates family therapy for parents rather than just for adolescents. This can help reduce the occurrence, development, and addiction of NSSI behaviours among adolescents by increasing parent classes, restoring autonomy, and reducing domestic violence language and conflict.
Limitations
Based on GBTM, this study explored two heterogeneous trajectories of NSSI behaviour. Further, drawing on family system theory and cumulative risk model, a DTM was constructed to analyse the core family factors affecting NSSI behavioural addiction. Nonetheless, it would have been preferable to explore more detailed subgroups based on microscopic indicators with larger sample sizes from multiple centres. Second, the follow-up period of patients with NSSI behaviour was relatively short; increasing the follow-up time point and extending the follow-up period can help us to better understand the long-term change characteristics of NSSI behaviour. Third, while the influence of family on NSSI behaviour is almost universally recognised, we did not explore the intrinsic mechanisms within the family through which the cumulative risks influence NSSI behaviour.
Future Research Avenues
These issues call for continuing our efforts, to see if our trajectories can be replicated and if they can conduct further subgroup analyses. Subgroup analyses based on microscopic indicators can have important clinical value. For example, functional near-infrared spectroscopy(fNIRS), genetic testing, etc. The study has founded that adolescents with NSSI showed significantly decreased PFC oxygenation compared to HC, as indexed by oxygenated hemoglobin.59 Second, NSSI behaviour is the result of the interaction of multiple factors; studies should explore the intrinsic mechanisms between different factors. Third, additional large-scale longitudinal studies are necessary to assess the different development trajectories associated with family cumulative risk, such as the relationships between the different development periods of family cumulative risk and NSSI. Such studies can provide crucial evidence, based on which evidence-based prevention and intervention strategies can be further strengthened and adopted.
Acknowledgment
Thanks to all the psychiatrists and nurses who supported this study, as well as all participants who were interviewed in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded by funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Klonsky ED. Non-suicidal self-injury: an introduction. J Clin Psychol. 2007;63(11):1039–1043. doi:10.1002/jclp.20411
2. International Society for the Study of Self-Injury. About Self-Injury; 2020. Available from: https://itriples.org/category/about-self-injury/.
3. Muehlenkamp JJ, Gutierrez PM. An investigation of differences between self-injurious behavior and suicide attempts in a sample of adolescents. Suicide Life Threat Behav. 2004;34(1):12–23. doi:10.1521/suli.34.1.12.27769
4. Lim KS, Wong CH, McIntyre RS, et al. Global Lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. 2019;16(22):4581. doi:10.3390/ijerph16224581
5. Mannekote Thippaiah S, Shankarapura Nanjappa M, Gude JG, et al. Non-suicidal self-injury in developing countries: a review. Int J Soc Psychiatry. 2021;67(5):472–482. doi:10.1177/0020764020943627
6. Koposov R, Stickley A, Ruchkin V. Non-suicidal self-injury among incarcerated adolescents: prevalence, personality, and psychiatric comorbidity. Front Psychiatry. 2021;12:652004. doi:10.3389/fpsyt.2021.652004
7. Chávez-Flores YV, Hidalgo-Rasmussen CA, Yanez-Peñúñuri LY. Instrumentos de evaluación de la autolesión no suicida en adolescentes 1990–2016: una revisión sistemática [Assessment tools of non-suicidal self-injury in adolescents 1990–2016: a systematic review]. Cien Saude Colet. 2019;24(8):2871–2882. Spanish. doi:10.1590/1413-81232018248.18502017
8. Thai TT, Jones MK, Nguyen TP, et al. The prevalence, correlates and functions of non-suicidal self-injury in Vietnamese adolescents. Psychol Res Behav Manag. 2021;14:1915–1927. doi:10.2147/PRBM.S339168
9. Plener PL, Kaess M, Schmahl C, Pollak S, Fegert JM, Brown RC. Nonsuicidal self-injury in adolescents. Dtsch Arztebl Int. 2018;115(3):23–30. doi:10.3238/arztebl.2018.0023
10. Bentley KH, Nock MK, Barlow DH. The four-function model of nonsuicidal self-injury: key directions for future research. Clin Psychol Sci. 2014;2(5):638–656. doi:10.1177/2167702613514563
11. Centers for Disease Control and Prevention [CDC]. WISQARS: web-based inquiry statistics query and reporting system; 2019. Available from: http://www.cdc.gov/ncipc/wisqars/default.htm.
12. Hedegaard H, Curtin SC, Warner M. Increase in Suicide Mortality in the United States, 1999–2018. NCHS Data Brief; 2020:1–8.
13. Kiekens G, Hasking P, Bruffaerts R, et al. Non-suicidal self-injury among first-year college students and its association with mental disorders: results from the World Mental Health International College Student (WMH-ICS) initiative. Psychol Med. 2021:1–12. doi:10.1017/S0033291721002245
14. Muehlenkamp JJ. Distinguishing between suicidal and nonsuicidal self-injury. In: Nock MK, editor. The Oxford Handbook of Suicide and Self-Injury. New York: Oxford University Press; 2014:23–46.
15. Muehlenkamp JJ, Claes L, Havertape L, Plener PL. International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Child Adolesc Psychiatry Ment Health. 2012;6(1):10. doi:10.1186/1753-2000-6-10
16. Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6(1):339–363. doi:10.1146/annurev.clinpsy.121208.131258
17. Blasco-Fontecilla H, Fernández-Fernández R, Colino L, Fajardo L, Perteguer-Barrio R, de Leon J. The addictive model of self-harming (Non-suicidal and suicidal) behavior. Front Psychiatry. 2016;7:8. doi:10.3389/fpsyt.2016.00008
18. Tang J, Ma Y, Lewis SP, et al. Association of internet addiction with nonsuicidal self-injury among adolescents in China. JAMA Netw Open. 2020;3(6):e206863. doi:10.1001/jamanetworkopen.2020.6863
19. Depestele L, Lemmens GM, Dierckx E, Baetens I, Schoevaerts K, Claes L. The role of non-suicidal self-injury and binge-eating/purging behaviours in the caregiving experience among mothers and fathers of adolescents with eating disorders. Eur Eat Disord Rev. 2016;24(3):257–260. doi:10.1002/erv.2428
20. Hasking P, Rees CS, Martin G, Quigley J. What happens when you tell someone you self-injure? The effects of disclosing NSSI to adults and peers. BMC Public Health. 2015;15:1039. doi:10.1186/s12889-015-2383-0
21. Benedict MA, Mofolo N, Adefuye AO. The economic burden of deliberate self-poisoning: insight from a tertiary hospital in the Free State Province, South Africa. Pan Afr Med J. 2020;36:35. doi:10.11604/pamj.2020.36.35.22346
22. Adrian M, Zeman J, Erdley C, Whitlock K, Sim L. Trajectories of non-suicidal self-injury in adolescent girls following inpatient hospitalization. Clin Child Psychol Psychiatry. 2019;24(4):831–846. doi:10.1177/1359104519839732
23. Hepp J, Carpenter RW, Störkel LM, Schmitz SE, Schmahl C, Niedtfeld I. A systematic review of daily life studies on non-suicidal self-injury based on the four-function model. Clin Psychol Rev. 2020;82:101888. doi:10.1016/j.cpr.2020.101888
24. Chartrand H, Tefft B, Sareen J, et al. A longitudinal study of correlates, discharge disposition, and rate of re-presentation to emergency services of adults who engage in non-suicidal self-injury. Arch Suicide Res. 2022;26(3):1141–1158. doi:10.1080/13811118.2020.1856259
25. Tilton-Weaver L, Latina D, Marshall SK. Trajectories of nonsuicidal self-injury during adolescence. J Adolesc. 2023;95(3):437–453. doi:10.1002/jad.12126
26. Shi X, Jiang L, Chen X, Zhu Y. Distinct trajectories of suicidal behaviors throughout the university stage and associated risk and protective factors: a large-scale prospective study. J Affect Disord. 2022;319:407–415. doi:10.1016/j.jad.2022.09.107
27. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227–1239. doi:10.1016/S0140-6736(15)00234-2
28. He H, Hong L, Jin W, et al. Heterogeneity of non-suicidal self-injury behavior in adolescents with depression: latent class analysis. BMC Psychiatry. 2023;23(1):301. doi:10.1186/s12888-023-04808-7
29. Carpenter RW, Trull TJ. The pain paradox: borderline personality disorder features, self-harm history, and the experience of pain. Personal Disord. 2015;6(2):141–151. doi:10.1037/per0000112
30. Davis E, Sawyer MG, Lo SK, Priest N, Wake M. Socioeconomic risk factors for mental health problems in 4–5-year-old children: Australian population study. Acad Pediatr. 2010;10(1):41–47. doi:10.1016/j.acap.2009.08.007
31. Lucio R, Hunt E, Bornovalova M. Identifying the necessary and sufficient number of risk factors for predicting academic failure. Dev Psychol. 2012;48(2):422–428. doi:10.1037/a0025939
32. Buehler C, Gerard JM. Cumulative family risk predicts increases in adjustment difficulties across early adolescence. J Youth Adolesc. 2013;42(6):905–920. doi:10.1007/s10964-012-9806-3
33. Tømmerås T, Kjøbli J. Family resources and effects on child behavior problem interventions: a cumulative risk approach. J Child Fam Stud. 2017;26(10):2936–2947. doi:10.1007/s10826-017-0777-6
34. Shen Y, Seo E, Walt DC, Kim SY. Stress of language brokering and Mexican American adolescents’ adjustment: the role of cumulative risk. J Early Adolesc. 2020;40(3):400–425. doi:10.1177/0272431619847526
35. Olson D. FACES IV and the Circumplex Model: validation study. J Marital Fam Ther. 2011;37(1):64–80. doi:10.1111/j.1752-0606.2009.00175.x
36. Fei LP, Shen QJ, Zhen YP, et al. “Preliminary evaluation of the Family Intimacy and Fitness Scale” and the “Family Environment Scale”: a controlled study of normal families and family members with schizophrenia. Chin Ment Health J. 1991;05:
37. Wang Q, Pomerantz EM, Chen H. The role of parents’ control in early adolescents’ psychological functioning: a longitudinal investigation in the United States and China. Child Dev. 2007;78(5):1592–1610. doi:10.1111/j.1467-8624.2007.01085.x
38. Chen H, Pan B, Zhang C, et al. Revision of the non-suicidal self-injury behavior scale for adolescents with mental disorder. J Cent South Univ. 2022;47(03):301–308. doi:10.11817/j.issn.1672-7347.2022.210549
39. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143(11):1117–1154. doi:10.1037/bul0000118
40. Reinhardt M, Rice KG, Durán BS, Kökönyei G. A person-centered approach to adolescent nonsuicidal self-injury: predictors and correlates in a community sample. J Youth Adolesc. 2022;51(9):1760–1773. doi:10.1007/s10964-022-01628-y
41. Wang B, You J, Lin MP, Xu S, Leung F. Developmental trajectories of nonsuicidal self-injury in adolescence and intrapersonal/interpersonal risk factors. J Res Adolesc. 2017;27(2):392–406. doi:10.1111/jora.12273
42. Klimes-Dougan B, Begnel E, Almy B, Thai M, Schreiner MW, Cullen KR. Hypothalamic-pituitary-adrenal axis dysregulation in depressed adolescents with non-suicidal self-injury. Psychoneuroendocrinology. 2019;102:216–224. doi:10.1016/j.psyneuen.2018.11.004
43. Hui C, Zhou JS. Research progress on addiction characteristics of non-suicidal self-injury behaviors. Chin J Psychiatry. 2022;55(1):64–68.
44. Brausch AM, Clapham RB, Littlefield AK. Identifying specific emotion regulation deficits that associate with nonsuicidal self-injury and suicide ideation in adolescents. J Youth Adolesc. 2022;51(3):556–569. doi:10.1007/s10964-021-01525-w
45. Gulbas LE, Hausmann-Stabile C, De Luca SM, Tyler TR, Zayas LH. An exploratory study of nonsuicidal self-injury and suicidal behaviors in adolescent Latinas. Am J Orthopsychiatry. 2015;85(4):302–314. doi:10.1037/ort0000073
46. Liang K, Zhao L, Lei Y, et al. Nonsuicidal self-injury behaviour in a city of China and its association with family environment, media use and psychopathology. Compr Psychiatry. 2022;115:152311. doi:10.1016/j.comppsych.2022.152311
47. Zhou HY, Luo YH, Shi LJ, Gong J. Exploring psychological and psychosocial correlates of non-suicidal self-injury and suicide in college students using network analysis [published online ahead of print, 2023 May 29]. J Affect Disord. 2023;23:S0165–S0327. doi:10.1016/j.jad.2023.05.089
48. Huang X, Liu H, Lan Z, Deng F. The effect of loneliness on non-suicidal self-injury behavior in Chinese Junior High School adolescents: a moderated mediation model. Psychol Res Behav Manag. 2023;16:1831–1843. doi:10.2147/PRBM.S410535
49. Hird K, Hasking P, Boyes M. Relationships between outcome expectancies and non-suicidal self-injury: moderating roles of emotion regulation difficulties and self-efficacy to resist self-injury. Arch Suicide Res. 2022;26(4):1688–1701. doi:10.1080/13811118.2021.1983492
50. Gratz KL, Spitzen TL, Tull MT. Expanding our understanding of the relationship between nonsuicidal self-injury and suicide attempts: the roles of emotion regulation self-efficacy and the acquired capability for suicide. J Clin Psychol. 2020;76(9):1653–1667. doi:10.1002/jclp.22950
51. Ferrey AE, Hughes ND, Simkin S, et al. The impact of self-harm by young people on parents and families: a qualitative study. BMJ Open. 2016;6(1):e009631. doi:10.1136/bmjopen-2015-009631
52. Teng C, Zhou WL, Song HD. Research progress on the relationship between family factors and adolescent non-suicidal self-injury.Chinese. J Child Health Care. 2022;30(05):535–539.
53. Zhang XM, Han L, Zhang H, et al. Experience of non-suicidal self-injury among adolescent mental disorder patients: a qualitative study. J Nurs Sci. 2022;37(2):71–74. doi:10.3870/j.issn.1001-4152.2022.02071
54. Guo J, Gao Q, Wu R, Ying J, You J. Parental psychological control, parent-related loneliness, depressive symptoms, and regulatory emotional self-efficacy: a moderated serial mediation model of nonsuicidal self-injury. Arch Suicide Res. 2022;26(3):1462–1477. doi:10.1080/13811118.2021.1922109
55. Wang L, Zou HO, Liu J, Hong JF. Prevalence of adverse childhood experiences and their associations with non-suicidal self-injury among Chinese Adolescents with Depression [published online ahead of print, 2023 Feb 22]. Child Psychiatry Hum Dev. 2023. doi:10.1007/s10578-023-01508-x
56. Chen QQ. The relationship between parenting style and non-suicidal self-injury of middle school students: the role of psychological need satisfaction and self-control [MA thesis]. Guangzhou University; 2023. doi:10.27040/d.cnki.ggzdu.2023.001447.
57. Donath C, Graessel E, Baier D, Bleich S, Hillemacher T. Is parenting style a predictor of suicide attempts in a representative sample of adolescents? BMC Pediatr. 2014;14:113. doi:10.1186/1471-2431-14-113
58. Claes L, Soenens B, Vansteenkiste M, Vandereycken W. The scars of the inner critic: perfectionism and nonsuicidal self-injury in eating disorders. Eur Eat Disord Rev. 2012;20(3):196–202. doi:10.1002/erv.1158
59. Koenig J, Höper S, van der Venne P, Mürner-Lavanchy I, Resch F, Kaess M. Resting state prefrontal cortex oxygenation in adolescent non-suicidal self-injury - A near-infrared spectroscopy study. Neuroimage Clin. 2021;31:102704. doi:10.1016/j.nicl.2021.102704
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.