Back to Journals » Infection and Drug Resistance » Volume 15
Herpes Zoster Duplex Bilateralis After Trauma Induced Emotional Dysregulation: A Case Report and Literature Review
Authors Yu T ![]() , Song J
, Song J ![]() , Chen X, Li J, Yang S, Yang J
, Chen X, Li J, Yang S, Yang J ![]()
Received 8 March 2022
Accepted for publication 12 May 2022
Published 24 May 2022 Volume 2022:15 Pages 2657—2660
DOI https://doi.org/10.2147/IDR.S364156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Tianhang Yu,1 Jikai Song,2 Xin Chen,1 Jin Li,1 Shuang Yang,1 Jie Yang1
1Department of Dermatology, Affiliated Hospital of North China University of Science and Technology, Tangshan, Hebei Province, People’s Republic of China; 2Zhejiang Provincial People’s Hospital, Qingdao University, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Jie Yang, Tel +8618832506999, Email [email protected]
Abstract: Herpes zoster (HZ) is usually distributed on one side of the body; HZ duplex bilateralis is very rare with only 0.1% of all HZ cases. The occurrence of HZ duplex bilateralis is associated with abnormal immune function. In this report, we present a case of a 47-year-old woman who had no major health issues developed HZ duplex bilateralis after an adverse life event and extreme depression one month ago. HZ related symptoms were controlled after patient received antiviral, analgesic, and nerve-nourishing treatment in our hospital.
Keywords: viral infections, duplex bilateralis, herpes zoster, immunological tests, bad mood
Introduction
Herpes zoster (HZ) is a disease caused by reactivation of latent varicella zoster virus (VZV) in sensory ganglia and almost always involves a single dermal area. HZ duplex bilateralis is rare,1 with an incidence of less than 0.1%,2 and usually occurs in individuals with comorbid chronic diseases or in the elderly.3 In this report, we present a case of an adult with no previous underlying disease who developed HZ duplex bilateralis after a serious negative mood caused by anger. After consulting domestic and foreign literature in the past ten years, this is the first reported case of HZ duplex bilateralis post trauma induced emotional dysregulation to the best of our knowledge. We analyzed the causes of HZ duplex bilateralis in healthy patients.
Case Report
A 44-year-old female farmer presented with erythematous blisters with paroxysmal tingling on the left side of the lower back and abdomen for 8 days and the same rash with pain on the right side of the chest, armpit and back for 7 days. After the onset of the disease, the patient was diagnosed with a “snake pan sore” by a local village doctor. The patient refused the treatment of Western Medicine and believed in alternative methods. In brief, patient used the “circling method” handed down by folklore, asking a so-called experienced person to dip a brush in ink and make circles around the skin lesions in an attempt to stop the rash from progressing. The lesions did not improve but continued to develop, and the pain became significantly worse, so she came to our department.
Before the acute episode of HZ, the individual was in good health and denied any history of chronic illnesses, such as hepatitis, tuberculosis, diabetes, tumors, or connective tissue disease, or hormone or immunosuppressant medications. Further inquiry into the medical history revealed that the patient had become angry with her husband for some reason one month before the onset and that both parties were noisy and intended to divorce. Since then, she had been feeling depressed, desperate, and fatigued all over her body.
The patient’s physical examination showed no systemic abnormalities. Dermatological conditions included the following: lesions on the left side of the waist and abdomen (Figure 1A) and posterior back (Figure 1B), on the right side of the chest (Figure 1C), axillae (Figure 1D), and posterior back, with clusters of red papules and small blisters the size of small rice grain on a base of flaky erythema, with the rash distributed in strips along the intercostal nerves. Part of the blisters burst, and there were small decayed surfaces and black scabs stained with the exudate of ink.
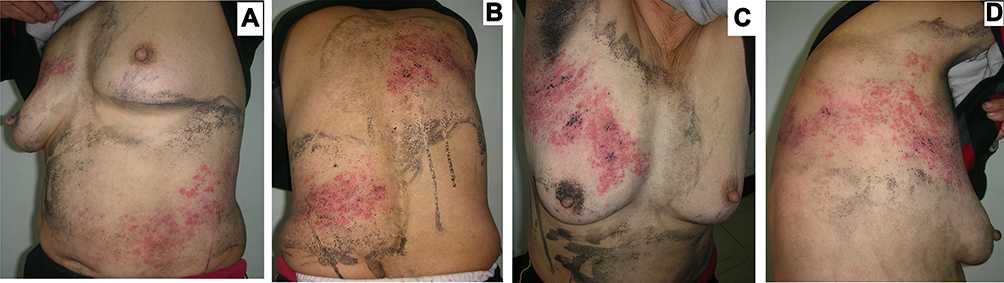 |
Figure 1 Painful papules and small blisters are distributed in clusters on the basis of flaky erythema, arranged in a band from the left abdomen (A) to the back (B), and on the right from the chest (C) extending in a band to the axillae (D) and back. Black dotted crusts of ink are scattered on the erythema, and black ink spots are painted around the rash (folklore “circling method”, using ink circles around the lesions). |
After further discussion, the patient stated that she had chickenpox caused by a primary VZV infection in childhood. The patient denies close contact with someone who had chickenpox or shingles before suffering from HZ and has not received the varicella zoster vaccine. Lab results (Supplementary Tables 1–3) showed an abnormal count of lymphocytes at 0.94*109/L, and other values in the complete blood count test are normal. Routine urinalysis (-), liver and kidney function tests (-), blood glucose (-), human immunodeficiency virus (HIV) (-), hepatitis (-), and tuberculosis antibodies (-), normal chest X-rays, ECG, and abdominal ultrasound. Thus, we diagnosed the patient as HZ duplex bilateralis. (References: 1. Chinese diagnostic standard4) Similar diagnostic procedures were also reported by other studies. (References: 2. Other papers used the same protocols.5 (may be more than one paper)) 5 papers published in good journals.
Acyclovir 0.25g q8h IV, gabapentin capsules 10 mg/day orally, vitamin B1 10 mg/day orally, and mecobalamin tablets 0.5 mg/day orally were prescribed for treatment. After 10 days of treatment, the original erythema and rash basically disappeared. All the papules and blisters dried up and crusted over, with a small amount of hyperpigmentation in some of the rash areas. Patients still had paroxysmal pain and we prescribed mecobalamin tablets, vitamin B1, and gabapentin capsules orally for maintenance treatment, and the pain disappeared after three weeks.
Discussion
HZ is a common skin disease caused by VZV that is mostly distributed along the peripheral nerves in a banded shape on one side of the body, and the lesions usually do not exceed the midline.6 In this case, skin lesions (Figure 2A and B) occurred on the left waist and abdomen (Lt. T7-9) and the right chest, axilla, and back (Rt. T2-3), which was consistent with the diagnosis of HZ duplex bilateralis.7 HZ duplex bilateralis is very rare, and its pathophysiologic mechanism is not clear.8 In the past, it has been reported that cases of HZ duplex bilateralis are more common in elderly individuals, people with various chronic diseases, cancers, or long-term immunosuppressants.9,10 This patient was in her prime and generally in good health. It is noteworthy that this patient was angry and depressed in the month prior to the onset of her illness, and it is considered that her onset of illness was closely related to her reduced immunity due to negative emotions such as depression and despair prior to her illness. In a cohort study, Sigrun A. J. Schmidt et al followed 77,310 individuals aged 40 years or older who participated in the 2010 Danish National Health Survey. The final conclusion was that high levels of psychological stress were associated with an increased risk of HZ.11 We believe that mood changes can weaken the body’s defenses against VZV, even leading to the development of more severe cases, such as HZ duplex bilateralis, or accelerate the progression of HZ disease. We speculate that severe depressed mood due to anger may be one of the risk factors for reactivation of the VZV in multiple independent ganglia. From the result of the low lymphocyte count, we can conclude the abnormal immune status of the patient, which also proves our speculation.12 Reviewing previous reports, there are reported cases of “healthy” patients, even children and adolescents, with unexplained sudden severe HZ duplex bilateralis. Dai, S summarized 40 cases of HZ duplex bilateralis that had been reported before 2020,2 including 10 in patients aged 20–49 years old in the prime of life and previously in good health. We know that HZ duplex is a rare event and is almost exclusively confined to immunocompromised patients.7 Is there also an underlying psycho-emotional cause for this unusual presentation, which leads to a low stage of immune function? It thus seems essential to understand and study in detail the psychological conditions and mood swings that precede the onset of these somatic health cases. Previous literature suggests an increase in widespread transmission and multisite incidence of HZ as cellular immunity declines.10 A reported case of HZ duplex bilateralis in a previously healthy 14-year-old boy with an abnormal natural killer (NK) cell test at the onset of the disease was found to be normal in subsequent follow-up repeat tests.13 In a 50-year-old female with HZ duplex, her cellular immune function CD4 count was 920/mm3, which was within the normal range.5 Can the inconsistency of these test results indicate that HZ duplex bilateralis has nothing to do with the patient’s immune status? The answer is definitely no. The reason for these inconsistent test results is related to a number of factors, including individual differences in immune response to various psychological and somatic disease stimuli. Therefore, attention should be given to the timing of the laboratory tests. We believe that it is more meaningful to test patients regularly at multiple stages, before and during the onset of the disease, to dynamically observe changes in their immune parameters. The lack of cellular immune assessment is the limitation of this case report. Future procedure at our institute may consider these assessments and tests to accelerate the judgment.
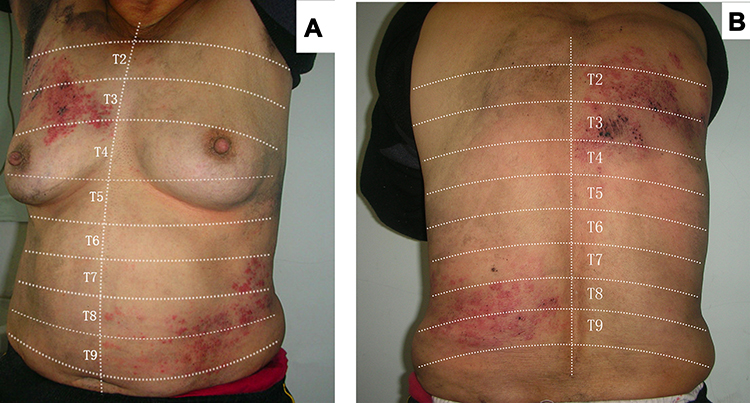 |
Figure 2 The left abdomen (Lt. T7-9) and the right thorax (Rt. T2-3) demonstrated clusters of papules and blisters on the basis of flaky erythema in a band-like distribution (A). The left lumbar region (Lt. T7-9) and the right dorsal region (Rt. T2-3) showed clusters of blisters on the basis of erythema distributed in bands (B). (Skin lesions after removing ink). |
Folk and alternative medicine may provide HZ patients some relief at certain levels.14 However, medical providers should pay attention to the development of new interventions and offer patients effective treatments as early as possible to improve their symptoms. For people who are in the midst of adverse life events (which may include stressful or sudden changes in life, work, or school) that potentially lead to low mood, despair, and depression, in addition to mental health management, it is worth exploring other treatment options. Further studies may explore the impact of preventive treatments such as varicella-zoster vaccination in the high-risk HZ patient population.15
Conclusion
We reported a case of a 44-year-old woman who developed Herpes Zoster duplex bilateralis after trauma induced emotional dysregulation. The symptoms were successfully controlled after the patient received anti-viral drug management and supportive treatment. To the best of our knowledge, this is the first case of its kind reported in the literate.
Data Sharing Statement
All the data are fully available without restriction.
Ethics Approval and Patient Consent
No ethical committee approval was required for this study as the data had been analyzed in a retrospective manner. Written informed consent was obtained from the patient for the publication of clinical results.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data (imaging features), or analysis and interpretation of results; took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Le P, Rothberg M. Herpes zoster infection. BMJ. 2019;364:k5095. doi:10.1136/bmj.k5095
2. Dai S, Huang X, Chen Y, et al. Bilateral asymmetrical herpes-zoster with Ramsay hunt syndrome in an immunocompetent adult. Virol J. 2020;17(1):123. doi:10.1186/s12985-020-01392-0
3. Yoo KH, Park JH, Kim BJ, Kim MN, Song KY. Herpes zoster duplex bilateralis in a patient with breast cancer. Cancer Res Treat. 2009;41(1):50–52. doi:10.4143/crt.2009.41.1.50
4. Herpes zoster expert consensus working group of Chinese Medical Doctor Association Dermatologist Branch. Chinese expert consensus on herpes zoster. Chin J Dermatol. 2018;51(6):403–408.
5. Agrawal S, Aara N, Bumb R. Herpes zoster duplex bilateralis symmetricus in an immunocompetent subject. Int J Dermatol. 2014;53(4):e281–e282. doi:10.1111/ijd.12235
6. Dayan RR, Peleg R. Herpes zoster - typical and atypical presentations. Postgrad Med. 2017;129(6):567–571. doi:10.1080/00325481.2017.1335574
7. Castronovo C, Nikkels AF. Chronic herpes zoster duplex bilateralis. Acta Derm Venereol. 2012;92(2):148–151. doi:10.2340/00015555-1206
8. Akimoto T, Muto S, Nagata D. Bilateral herpes zoster in a patient with end-stage kidney disease. Int Med Case Rep J. 2017;10:209–212. doi:10.2147/IMCRJ.S138398
9. Di Meo N, Bergamo S, Dondas A, Trevisan G. Bortezomib and bilateral herpes zoster. Acta Dermatovenerol Alp Pannonica Adriat. 2012;21(1):21–22.
10. Shin JW, Kim DH, Whang KU, et al. A case of zoster duplex bilateralis. Ann Dermatol. 2009;21(4):423–425. doi:10.5021/ad.2009.21.4.423
11. Schmidt S, Sørensen HT, Langan SM, Vestergaard M. Perceived psychological stress and risk of herpes zoster: a nationwide population-based cohort study. Br J Dermatol. 2021;185(1):130–138. doi:10.1111/bjd.19832
12. Tecoma ES, Huey LY. Psychic distress and the immune response. Life Sci. 1985;36(19):1799–1812. doi:10.1016/0024-3205(85)90152-3
13. Yan C, Laguna BA, Marlowe LE, Keller MD, Treat JR. Herpes zoster duplex bilateralis in an immunocompetent adolescent boy: a case report and literature review. Pediatr Dermatol. 2014;31(3):341–344. doi:10.1111/pde.12302
14. Sheu SY, Yao CH, Lei YC, Kuo TF. Recent progress in Glinus oppositifolius research. Pharm Biol. 2014;52(8):1079–1084. doi:10.3109/13880209.2013.876653
15. Keating GM. Shingles (herpes zoster) vaccine (zostavax(®)): a review in the prevention of herpes zoster and postherpetic neuralgia. Biodrugs. 2016;30(3):243–254. doi:10.1007/s40259-016-0180-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.