Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
HER2 Heterogeneity in Breast Cancer: Biological Basis, Clinical Implications, and Therapeutic Strategies
Authors Shi H ![]() , Feng Y, Guo T, Shou W, Li Y
, Feng Y, Guo T, Shou W, Li Y
Received 31 March 2026
Accepted for publication 3 June 2026
Published 12 June 2026 Volume 2026:18 612951
DOI https://doi.org/10.2147/BCTT.S612951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Hanxiao Shi,1 Yiqian Feng,1 Tao Guo,1 Wenjun Shou,2 Yuandong Li3
1Department of the First Clinical Medicine, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2Department of Occupational Health, School of Public Health, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 3Department of Breast Surgery, The First Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Yuandong Li, Department of Breast Surgery, The First Hospital of Shanxi Medical University, No. 85, Jiefang South Road, Yingze District, Taiyuan City, Shanxi Province, People’s Republic of China, Email [email protected]
Abstract: Human epidermal growth factor receptor 2 (HER2) is a key driver of breast cancer and exhibits significant heterogeneity at the temporal, spatial, and molecular levels. This heterogeneity not only complicates HER2 assessment but also significantly impacts the efficacy of targeted therapies, ultimately contributing to drug resistance. This review summarizes current standards for HER2 testing and highlights their inherent limitations. It outlines the multidimensional manifestations of HER2 heterogeneity and examines the underlying biological mechanisms driving this phenomenon. In addition, emerging diagnostic strategies and therapeutic approaches are being developed specifically to address HER2 heterogeneity. The review aims to provide insights for optimizing patient stratification and advancing precision treatment in breast cancer.
Keywords: breast carcinoma, human epidermal growth factor receptor 2 heterogeneity, targeted therapy, drug resistance
Introduction
Worldwide, breast cancer represents the most frequently diagnosed cancer in women and a leading cause of cancer-related mortality.1 Human epidermal growth factor receptor 2 (HER2) is an important driver gene in breast cancer initiation and progression. HER2 amplification or protein overexpression is closely associated with enhanced tumor invasiveness, increased metastatic risk, and poor prognosis.2 The application of HER2-targeted agents has substantially prolonged survival among patients with HER2-positive breast cancer. Furthermore, antibody-drug conjugate (ADC) trastuzumab deruxtecan (T-DXd) has expanded the population benefiting from treatment to include patients with HER2-low tumors.3
However, HER2 exhibits complex heterogeneity within tumors and across different lesions, including uneven gene amplification, differential protein expression, and dynamic evolution induced by treatment.4 HER2 intratumoral heterogeneity (HER2-ITH) refers to the presence of tumor cell subpopulations exhibiting heterogeneous HER2 gene or protein expression within the same tumor. It can be classified into genetic ITH, caused by differences in ERBB2 gene copy number, and non-genetic ITH, which occurs on a background of uniform gene amplification.4–6 A significant association has been demonstrated between HER2 heterogeneity and both diminished therapeutic response and poorer long-term survival following targeted therapy.7–9
In the era of ADC therapy, HER2 is increasingly regarded as a biomarker with a continuous distribution and dynamic variability.10 Changes in HER2 expression between primary and metastatic or recurrent lesions, as well as before and after neoadjuvant therapy, further exacerbate its spatiotemporal heterogeneity. This complexity poses new challenges for HER2 testing, patient stratification, and treatment decisions. Accordingly, this review summarizes the manifestations and underlying mechanisms of HER2 heterogeneity and further discusses its clinical implications and potential management strategies.
Clinical Standards and Current Practices of HER2 Testing
Early clinical trials of anti-HER2 targeted therapies revealed substantial inter-laboratory variability in HER2 test results. To address this issue, the American Society of Clinical Oncology (ASCO) and the College of American Pathologists (CAP) issued the first standardized guidelines for HER2 testing and interpretation in 2007. Immunohistochemistry (IHC) is used to assess protein expression levels, while in situ hybridization (ISH) is employed to evaluate ERBB2 gene amplification in cases with IHC 2+.11 The 2013 update further refined the interpretation criteria for IHC and ISH, providing a clearer definition for IHC 2+ cases and standardizing the classification of ISH results.12 This revision improved the accuracy of HER2 testing. The 2018 update focused on rare scenarios and challenging borderline results encountered in clinical practice.13
In recent years, the DESTINY-Breast04 and DESTINY-Breast06 trials have demonstrated clinically meaningful treatment benefits in patients with HER2-low and HER2-ultralow expression, respectively. The traditional binary classification of HER2 as positive or negative may no longer fully meet the needs of precise patient stratification in the era of ADCs. Consequently, the 2023 ASCO/CAP guidelines emphasized the importance of distinguishing IHC 0 from IHC 1+. However, HER2-null, HER2-ultralow, and HER2-low have not yet been recognized as distinct biological subtypes.14 (Figure 1 and Table 1). According to these criteria, tumors with IHC 3+ or IHC 2+/ISH amplified results are defined as HER2-positive, whereas IHC 0 or 1+ is considered HER2-negative.12,13
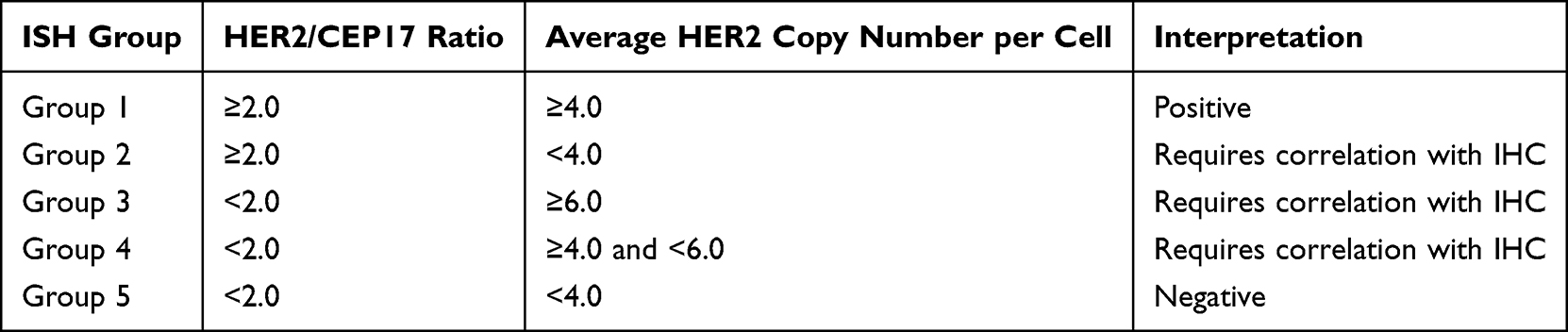 |
Table 1 HER2 ISH Interpretation Based on the 2018 ASCO/CAP Updated Guidelines |
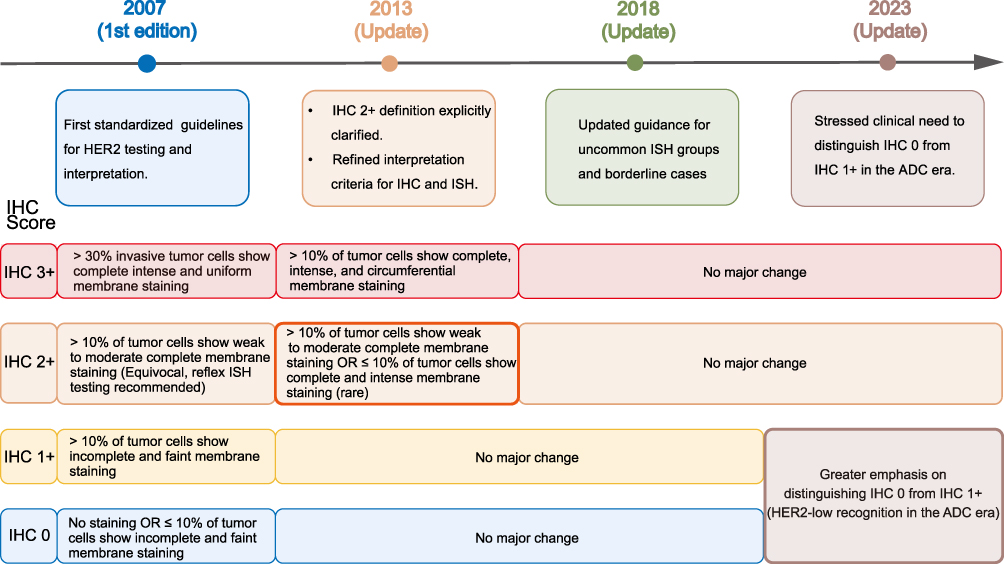 |
Figure 1 Evolution of ASCO/CAP HER2 IHC interpretation guidelines from 2007 to 2023. The figure highlights major updates in HER2 IHC interpretation. Bold borders indicate the two most significant changes in guideline evolution: refinement of the IHC 2+ category in the 2013 update and increased clinical emphasis on distinguishing IHC 0 from IHC 1+ in the ADC era (2023 update). Overall, the evolution reflects a shift from traditional binary HER2 classification toward a continuous HER2 expression spectrum. |
Despite continuous refinement of current testing standards, determination of HER2 status remains subject to inter-observer variability and sampling bias. Pre-analytical variables, such as tissue fixation, antigen retrieval, antibody clone, and assay conditions, can influence HER2 staining intensity and ISH sensitivity.15,16 Prolonged cold ischemia time can attenuate the signal intensity of HER2 IHC staining,17 while storing paraffin-embedded sections for excessive periods may lead to a decline in the HER2 positivity detection rate.18 Insufficient (< 6 hours) or excessive (> 72 hours) fixation increases the risk of errors in interpretation.12 Furthermore, detection antibodies differ in specificity and sensitivity, with HercepTest and PATHWAY 4B5 representing two commonly used assays.19,20
Multiple real-world studies have indicated considerable variability in the assessment of HER2-zero, HER2-ultralow, and HER2-low expression. A multicenter study reported that among 170 breast cancer samples interpreted by 18 pathologists, the concordance rate for IHC 1+ interpretations was less than 1%. The overall concordance rate for IHC 0 cases was only 25%.21 When IHC 0 was further subdivided into null and ultralow expression, agreement declined further (Fleiss κ = 0.230), markedly lower than that observed when classified simply as IHC 0 (Fleiss κ = 0.344).22 Additionally, the proportion of HER2-low cases reported by different pathology departments varied substantially, ranging from 46.3% to 71.8% (P < 0.0001).23 This variability is partly attributable to the continuous biological spectrum of HER2 expression, with most tumors exhibiting HER2/CEP17 ratios between 1 and 2, where conventional methods are limited in distinguishing extremely low expression levels.24 Although overall ISH concordance is generally high, it decreases significantly in cases with signals near the cutoff or in tumors exhibiting genetic heterogeneity.25
Multidimensional Manifestations of HER2 Heterogeneity
Spatial Heterogeneity of HER2
HER2 expression in breast cancer exhibits substantial variability across different spatial levels. Such heterogeneity may arise within distinct regions of the primary tumor, between primary and metastatic lesions, and among different metastatic sites.26–28 In a large paired sample analysis, comparison of 1299 matched primary and metastatic tumors revealed that 28.5% of patients experienced a change in HER2 status upon disease recurrence or metastasis, with the most common transition being from HER2-zero to HER2-low expression.29 Collectively, these results indicate that HER2 expression undergoes dynamic changes over the course of disease progression. In addition to tissue biopsy, liquid biopsy has also provided evidence from a dynamic perspective supporting the presence of spatial heterogeneity.30
Spatial discordance is more pronounced in the HER2-low population. Wu re-stratified HER2-negative cases based on HER2-zero, HER2-ultralow, and HER2-low expression. They found that 23.7% of cases exhibited discordant HER2 status across different lesions. In 12.0% of cases, the index lesion was not the site with the highest HER2 expression.31 Under current guidelines, HER2 testing is typically performed on the primary or a representative lesion. However, this approach may lead to underestimation of HER2 expression in some patients, potentially depriving them of the opportunity to receive ADC therapy. Furthermore, an autopsy study provided the first systematic evidence of marked spatial heterogeneity in HER2-low expression. The results showed that 80% of patients harbored both HER2-low and HER2-zero metastatic lesions. The proportion of HER2-low lesions varied widely among individuals, ranging from 5% to 89%.32
These findings challenge the conventional paradigm of relying on a single metastatic biopsy to guide treatment decisions. They support repeat biopsies at recurrence or metastasis, and integrating multi-regional sampling or liquid biopsy may further improve the accuracy of HER2 assessment and optimize therapeutic decision-making.
Dynamic Evolution Under Therapeutic Selection Pressure
In the context of neoadjuvant therapy for breast cancer, HER2 expression is not stable before and after treatment. Following neoadjuvant chemotherapy (NAC), 23.7% of cases exhibited discordant HER2 status between core needle biopsy (CNB) and surgical specimens. By comparison, patients who did not receive NAC showed a lower rate of discordance (12.5%, P = 0.023). Among the NAC cohort, approximately 3.4% of HER2-positive patients converted to HER2-negative status after receiving trastuzumab.33 Several studies have consistently demonstrated the loss of HER2 gene amplification following anti-HER2 targeted therapy.34–36 Therapeutic pressure may select for HER2-negative clones, leading to the loss of high HER2 expression and subsequently influencing treatment response.37 In patients with HER2-low tumors without a pathological complete response (PFS) after neoadjuvant therapy, a discordance rate of 26.4% was observed between pre- and post-treatment evaluations. Bidirectional conversion occurred in 33.8% of patients with baseline HER2-zero expression and in 37.7% of those with baseline HER2-low expression.38 A study by Kang reported an overall discordance rate as high as 36.5% in a larger cohort, further emphasizing the marked instability of HER2-low expression during treatment.
This instability varies across different molecular subtypes. In HER2-negative patients, the hormone receptor (HR)-positive subgroup shows a significantly higher proportion of HER2-low expression compared with the HR-negative subgroup (68.6% vs 46.8%, P = 0.001).37 HR-positive patients are also more likely to acquire HER2-low expression after treatment (OR = 2.48, P < 0.001).39 The study by Lian reinforced this association. Among patients with baseline HER2-low expression, the HR-positive subgroup exhibited the highest phenotypic stability (80.82% remained stable), while HR-negative patients were more likely to undergo expression conversion.40 These results suggest that HER2-low expression has a relatively high conversion rate across patients. However, in the presence of active HR signaling, the regulation of HR-related transcriptional networks may promote the maintenance or acquisition of the HER2-low expression phenotype.
Molecular Heterogeneity of HER2
Current understanding of HER2 molecular heterogeneity has become increasingly well characterized, and its underlying biological mechanisms are being elucidated. Multi-omics analyses have classified HER2-positive breast cancer into subtypes with distinct biological features and therapeutic sensitivities, including the classical target-responsive subtype, immune-modulatory subtype, luminal-like subtype, and basal/mesenchymal-like subtype.41,42 Similarly, based on the expression patterns of genes related to histone modifications, HER2-low breast cancer exhibits three distinct subtypes that differ in prognosis and pathway activation.43 These classifications indicate that significant molecular heterogeneity exists between tumors, even within the same HER2 expression category.
HER2-ITH manifests as multidimensional differences at the genomic, protein expression, and cellular state levels. When HER2 expression approaches the diagnostic threshold or the HER2/CEP17 ratio is elevated, heterogeneity in HER2 gene amplification becomes more readily detectable.44 This genomic heterogeneity provides a foundation for differences in protein expression. At the protein spatial level, HER2-ITH exhibits three histological patterns. (Figure 2) The clustered pattern is characterized by the simultaneous presence of HER2-high (IHC 3+) and HER2-negative/low (IHC 0/1+) tumor cells, with a distinct boundary between them. The mosaic pattern manifests as a diffuse intermingling of cells with differing HER2 expression levels, whereas the scattered pattern consists of a tumor cell population predominantly composed of HER2-negative/low cells, interspersed with isolated HER2-high cells.45,46 Moreover, in some HER2-positive tumors, HER2 protein expression does not occur in isolation but varies coordinately with markers such as estrogen receptor (ER), forming a continuous expression spectrum at the single-cell level.47,48 The heterogeneity across genomic, protein, and cellular states underlies dynamic changes in HER2 expression and differential responses to therapy.
 |
Figure 2 Schematic diagram of HER2 intratumoral heterogeneity patterns by immunohistochemistry. This schematic illustrates HER2-ITH in breast cancer, showing three distribution patterns of tumor cells. Clustered pattern (A): HER2-high cells form contiguous clusters. Mosaic pattern (B): HER2-high and HER2-low/negative cells are intermixed without clear boundaries. Scattered pattern (C): Rare HER2-high cells are dispersed in predominantly HER2-low/negative regions. |
Clinical Cost of Heterogeneity: Variations in Treatment Efficacy and Origins of Drug Resistance
Heterogeneity in Therapeutic Response Caused by HER2 Heterogeneity
Previous studies have indicated that the HER2-enriched subtype is associated with higher pCR rates and better long-term survival outcomes in patients receiving neoadjuvant HER2-targeted therapy.49,50 In contrast, tumor heterogeneity is linked to reduced therapeutic benefit and is a major driver of resistance to targeted therapy.7,51,52 Multiple studies have demonstrated that a high level of HER2-ITH is an independent factor associated with lower pCR rates after NAC combined with anti-HER2 therapy.8,52 A prospective Phase II trial of neoadjuvant trastuzumab emtansine (T-DM1) plus pertuzumab revealed a marked disparity in pCR rates according to HER2-ITH status, with 0% in patients with HER2-ITH compared with 55% in those without (P < 0.0001).53 Evidence from mouse models and single-cell analyses also associates high heterogeneity with shorter disease-free survival (DFS) and a higher risk of disease progression.9,54
Within the traditional binary HER2 classification framework, differences in HER2 expression levels influence treatment response. Pooled analyses from multiple studies and prospective trials have shown that HER2‑low breast cancer has an inferior pCR rate compared with HER2-zero disease following NAC.55–58 Direct prospective clinical evidence comparing long-term survival outcomes among these groups remains limited, while retrospective studies have yielded inconsistent results. Although HER2-low serves as a therapeutic target for ADC, its independent prognostic value is yet to be established. In HER2-positive patients, tumors with IHC 2+/ISH-amplified status exhibit lower pCR rates than those with IHC 3+ tumors. These tumors also contain a smaller proportion of the HER2-enriched subtype, potentially limiting the efficacy of targeted therapy in this subgroup.59,60
Dynamic changes in HER2 expression further impact clinical outcomes. Patients with loss of HER2 expression following neoadjuvant therapy had a significantly increased risk of recurrence (HR 1.85, 95% CI: 1.31–2.61, P = 0.0005) and poorer overall survival (OS) (HR 2.37, 95% CI: 1.27–4.41, P = 0.0065) relative to those with stable HER2 status.61 Spatiotemporal heterogeneity between primary and metastatic lesions also predicts treatment response. Patients with consistently HER2-positive disease achieved a median progression-free survival (PFS) of 16.8 months, significantly longer than the 13.7 months observed in those with acquired HER2 positivity or the 3.6 months in those who converted to HER2-negative (P < 0.0001).62
The Root Causes of Drug Resistance Induced by HER2 Heterogeneity
Anti-HER2 monoclonal antibodies (mAbs) and ADCs are the standard treatments for HER2-positive breast cancer in both neoadjuvant and adjuvant settings.63,64 Although these therapies improve survival outcomes for most patients, resistance related to HER2 heterogeneity remains a major challenge.
Compared with tumors exhibiting homogeneous HER2 overexpression, tumors with HER2 heterogeneity typically display lower ERBB2 mRNA and HER2 protein levels, resulting in a “target dilution” effect that reduces the binding and internalization of antibodies or ADCs.34 Although HER2 expression or dependency may be decreased, certain tumors retain active downstream signaling pathways, including PI3K/AKT/mTOR, thereby offering alternative means of survival.65,66 In parallel, compensatory activation of bypass pathways, including Insulin-like Growth Factor 1 Receptor (IGF-1R), Fibroblast Growth Factor Receptor (FGFR), and integrins, may further enhance tumor adaptability to targeted therapy.67–69 Additionally, HER2 molecular variants contribute to therapeutic resistance. For instance, the extracellular domain-truncated form p95HER2 lacks the trastuzumab-binding epitope and can mediate resistance to specific anti-HER2 therapies.70
Evidence suggests that treatment itself can drive clonal selection based on HER2 status.37 Following therapy with T-DM1 plus pertuzumab, a subset of HER2-positive tumor cells is selectively eliminated, whereas less sensitive HER2-negative cells persist and expand, thereby increasing intratumoral heterogeneity.53 Tumors with HER2 heterogeneity show limited overall transcriptomic changes after treatment, suggesting an intrinsic adaptive equilibrium state.34
The immunosuppressive tumor microenvironment (TME) is a major driver of resistance to HER2-targeted therapy. Multiple immune cell populations, including exhausted T cells, myeloid-derived suppressor cells (MDSCs), and tumor-associated macrophages (TAMs), cooperatively impair antitumor immunity and limit treatment efficacy.71 Tumor-infiltrating lymphocytes (TILs) in HER2-positive breast cancer frequently display an exhausted phenotype. In early-stage disease, multiple checkpoint receptors, including PD-1, CTLA-4, LAG-3, TIM-3, and TIGIT, are co-expressed on CD8+cytotoxic T cells and CD16+CD56bright natural killer (NK) cells. This coordinated checkpoint activation suppresses cytotoxic antitumor responses and facilitates immune evasion.72
MDSCs are central mediators of immune suppression within the TME. Pro-inflammatory cytokines such as IL-6 and IL-8 activate NF-κB and IL-6/STAT3 signaling, thereby promoting MDSC expansion and activation.73,74 IL-6 derived from tumor-infiltrating NK cells correlates with Arg1 expression in MDSCs. Inhibition of the IL-6/STAT3 axis alleviates T-cell suppression and reduces tumor growth.75 MDSCs further suppress T-cell function through Arg1 secretion and PD-L1 upregulation, ultimately compromising antibody-dependent cellular cytotoxicity (ADCC).74 Collectively, these findings highlight the critical role of myeloid-mediated immune suppression in resistance to HER2-targeted therapy.
TAMs are another major immunosuppressive component of the TME. They are generally classified into the tumoricidal M1 subtype and the immunosuppressive M2 subtype, the latter representing the dominant phenotype associated with tumor-promoting and immunosuppressive functions.76 TAM-derived IL-10 activates STAT3/Bcl-2 signaling and promotes chemoresistance in breast cancer cells.77 In parallel, TAM-derived IL-8 enhances EGFR-related signaling and contributes to lapatinib resistance.78 TAMs additionally suppress CD8+T-cell activity through PD-L1 upregulation and subsequent interaction with PD-1. Sustained PD-1/PD-L1 signaling may eventually result in T-cell exhaustion.79 TAMs also participate in antibody-dependent cellular phagocytosis (ADCP), thereby modulating trastuzumab efficacy. Although ADCP mediates antibody-dependent phagocytosis of tumor cells and exerts antitumor effects, it may also attenuate this response by promoting PD-L1 upregulation on TAMs.80,81 Furthermore, TAMs regulate stromal cell function through signaling pathways such as STAT3/NF-κB, indirectly promoting M2 macrophage-mediated chemoresistance.82
Diagnostic Upgrades and Therapeutic Strategies for HER2 Heterogeneity
Diagnostic Upgrades
Given the dynamic nature of HER2 expression, serial tumor biopsies are recommended at baseline, after treatment, as well as at recurrence and in the metastatic setting, to assess changes in molecular characteristics.83 As an invasive procedure, CNB reflects only the molecular state of a localized tumor region and may not fully capture the biological features of the overall tumor burden. In contrast, as a non-invasive imaging technique, positron emission tomography/computed tomography (PET/CT) enables the assessment of HER2 expression throughout the body, providing valuable information for clinical treatment decisions and patient management.84
In patients with advanced HER2-positive breast cancer, 89Zr-trastuzumab PET effectively identifies lesions unresponsive to T-DM1 therapy, demonstrating a negative predictive value (NPV) of 81%. When combined with early metabolic imaging via FDG PET/CT, the NPV for non-response to treatment increases to 100%. Moreover, the median time to treatment failure in patients with negative HER2 PET findings is significantly shorter (2.8 vs 9.9 months; HR = 3.7; 95% CI: 2.19–6.35; P < 0.0001).85 The IMPACT-MBC study, which enrolled patients with all subtypes of metastatic breast cancer, revealed significant systemic heterogeneity in HER2 expression. From the data obtained, an algorithm was developed to predict IHC positivity, achieving an area under the curve (AUC) of 0.86 (95% CI: 0.79–0.93).86 This whole-body visualization of HER2 expression challenges the representativeness of conventional single-site CNB in capturing tumor heterogeneity. Preliminary investigations using novel molecular tracers like 68Ga-ABY-025 have demonstrated that HER2 PET imaging is both feasible and safe, and can also uncover inter-lesion heterogeneity in tracer uptake.87
Artificial intelligence (AI) technologies are being applied in pathological image analysis. By leveraging image recognition algorithms, AI enables the quantitative analysis of HER2 membrane staining, thereby yielding more objective, accurate, and reproducible diagnostic results. This technology holds significant potential for aiding pathological diagnosis.88,89 Deep learning-based algorithms can automatically detect and classify interphase nuclei and HER2/CEP17 signals in ISH images. Their diagnostic accuracy is comparable to that of a team of pathologists, with an overall concordance of 96%. At the single-nucleus level, the Cohen’s κ coefficient for classification approaches the level observed between pathologists.90 Wu and colleagues provided direct evidence for the application of AI in standardizing HER2-low and heterogeneous IHC scoring. By integrating AI-assisted interpretation with an augmented reality microscope system, overall scoring accuracy improved from 0.80 to 0.93, and inter-observer agreement increased from 0.542 (95% CI: 0.496–0.592) to 0.812 (95% CI: 0.783–0.840).91 In the future, AI is expected to serve as a valuable adjunct to pathologists, ultimately improving patient stratification for HER2-targeted therapies and enhancing treatment outcomes.
Beyond improving diagnostic accuracy, AI-assisted HER2 scoring has the potential to directly inform personalized treatment strategies. A systematic review and meta-analysis evaluated the ability of AI to distinguish HER2 IHC scores, using IHC 1+/2+/3+ as the positive threshold for T-DXd eligibility. The results demonstrated a pooled sensitivity of 0.97 (95% CI, 0.96–0.98), a pooled specificity of 0.82 (95% CI, 0.73–0.88), and an area under the curve of 0.98 (95% CI, 0.96–0.99).92 This indicates that among 100 patients with metastatic breast cancer, AI would miss only three patients who could potentially benefit from T-DXd therapy, while eighteen patients might be overtreated.
Unlike diagnostic models that rely solely on IHC scoring, deep learning-based models can integrate multimodal imaging data to overcome sampling bias caused by intratumoral heterogeneity in CNB specimens, thereby enabling noninvasive prediction of neoadjuvant treatment response. Zhang developed a multimodal alignment and prediction (MAP) model using multicenter datasets that integrate imaging and clinical information. The model achieved 79% concordance between predicted HER2 status and surgical specimens, substantially exceeding the approximately 41% concordance observed between CNB and surgical specimens. These findings demonstrate that AI can effectively address HER2 spatial heterogeneity by capturing the whole-tumor field rather than a localized biopsy sample.93 Furthermore, the MAP model was also applied to predict pCR following neoadjuvant therapy. In the internal test cohort, the AUC for treatment response prediction based on AI-predicted HER2 status reached 0.858, significantly outperforming the AUC of 0.826 derived from biopsy-based HER2 assessment (P < 0.05).93 Similarly, another study developed an AI-based efficacy prediction model for SHR-A1811, which also demonstrated robust performance in a real-world multi-ADC cohort including T-DXd, SHR-A1811, and TQB2102 (AUC = 0.83, 95% CI: 0.68–1.00). This multi-modal learning framework generalizes across next-generation ADCs, providing predictive capability for both single and multiple agents.94 Although AI-assisted HER2 assessment requires further validation in larger prospective studies, its preliminary success in improving diagnostic consistency, predicting treatment response, and guiding individualized ADC therapy has substantially advanced the clinical translation of precision medicine.
Therapeutic Strategies for HER2 Heterogeneity
The dual HER2-targeted regimen combining trastuzumab and pertuzumab has become a cornerstone in the treatment of HER2-positive breast cancer based on evidence from multiple pivotal clinical trials. In the phase II NeoSphere study, the addition of pertuzumab to standard neoadjuvant chemotherapy plus trastuzumab increased the pCR rate to 45.8% (95% CI: 36.1–55.7), outperforming trastuzumab plus chemotherapy alone.95 Long-term follow-up of the APHINITY trial in patients with early HER2-positive breast cancer receiving adjuvant chemotherapy plus dual HER2 blockade demonstrated a significant improvement in invasive disease-free survival (iDFS) in the overall population. In the pertuzumab group, the 6-year iDFS rate was 91%, compared with 88% in the control group (HR 0.76; 95% CI: 0.64–0.91).96 The CLEOPATRA study established dual HER2 blockade combined with chemotherapy as the standard of care for metastatic disease, with a median OS of 57.1 months (95% CI: 50–72).97 This therapeutic advantage is primarily attributed to the complementary mechanisms of the two antibodies, which bind to distinct extracellular domains of the HER2. Such dual blockade achieves more potent inhibition of HER2 dimerization and downstream signaling.98,99 Multi-epitope strategy confers the potential to overcome the heterogeneity of HER2 expression.
In recent years, the emergence of ADCs has provided a novel therapeutic strategy to overcome HER2 heterogeneity. ADCs deliver cytotoxic agents into tumor cells through monoclonal antibody-mediated specific binding. Following internalization and lysosomal degradation, the cytotoxic payload is released to exert antitumor effects.100,101 Notably, some payload molecules can diffuse into adjacent cells and induce cell death, which is known as the bystander effect.102 This characteristic enables ADCs to exert a relatively broad antitumor effect even in the tumor microenvironments with heterogeneous HER2 expression.
T-DXd is one of the most representative HER2-targeted ADCs. Compared with T-DM1, T-DXd achieved significantly longer PFS in patients with HER2-positive metastatic breast cancer previously treated with trastuzumab and taxanes. Median PFS was 29.0 months in the T-DXd group versus 7.2 months in the T-DM1 group (HR = 0.30; 95% CI: 0.24–0.38). Median OS also favored T-DXd (52.6 vs 42.7 months; HR = 0.73; 95% CI: 0.56–0.94). Both the objective response rate (ORR) and PFS were markedly superior with T-DXd compared to T-DM1.103 The DESTINY-Breast04 trial was the first to demonstrate that HER2-low metastatic breast cancer represents a distinct population that can derive significant benefit from ADC therapy. This Phase III study showed that, compared with conventional chemotherapy, T-DXd significantly prolonged both PFS (median PFS: 9.9 vs 5.1 months; HR = 0.50; P < 0.001) and OS (median OS: 23.4 vs 16.8 months; HR = 0.64; P = 0.001).3 The efficacy of T-DXd in HER2-low tumors is thought to be attributable to its unique ADC design. A high-affinity antibody ensures effective targeting even at low antigen density, while the combination of a cleavable linker and a membrane-permeable cytotoxic payload enhances the bystander effect. Together, these features expand the cytotoxic range and overcome intratumoral HER2 heterogeneity.3,104
Subsequently, the DESTINY-Breast06 trial further extended the clinical application of T-DXd to patients with HER2-ultralow tumors. HER2-ultralow is defined as a subset of IHC 0 tumors showing faint but detectable membranous staining (>0%).105 In this subgroup, T-DXd treatment continued to provide clinically meaningful benefit, with a PFS of approximately 13.2 months (95% CI, 9.8–17.3) and an ORR of 61.8% (95% CI, 50.0–72.8).106 Although DESTINY-Breast06 independently confirmed that HER2-ultralow patients may benefit from ADC therapy, the trial did not include HER2-null patients as a separate analysis cohort. Recently, CAP issued reporting templates recommending further subdivision of conventional IHC 0 tumors into HER2-null and HER2-ultralow. This approach is expected to more precisely identify patients most likely to benefit from ADC treatment.105 Furthermore, the enrollment periods of these key clinical trials spanned several years. During this time, multiple updates to the ASCO/CAP guidelines were issued, and HER2 scoring criteria continued to evolve. This evolution may, to some extent, affect the comparability of patient populations across studies, a factor that should be considered when integrating and analyzing relevant data.
Beyond optimizing HER2-targeted therapies, developing treatment strategies independent of HER2 expression represents an important approach to addressing HER2 heterogeneity. Regardless of HER2 expression, ADCs targeting Trop-2, such as sacituzumab govitecan (SG) and datopotamab deruxtecan (Dato-DXd), are representative agents. By binding to the widely expressed Trop-2 protein on tumor cells and delivering cytotoxic payloads, these agents exert potent antitumor effects.107,108 Such ADCs may eliminate both HER2-positive and HER2-negative clones simultaneously, offering a potential alternative for tumors that are resistant to HER2-targeted therapies due to intratumoral heterogeneity.
Faced with the complex drug-resistance landscape posed by HER2 heterogeneity, traditional single-target strategies often prove inadequate. Multi-targeted approaches have increasingly become a focus of research. Zanidatamab is a HER2-directed IgG1 bispecific antibody that simultaneously binds to two distinct domains, ECD4 and ECD2, on the HER2 receptor.109 This dual-epitope targeting not only more effectively inhibits HER2 signaling but also induces HER2 receptor clustering and internalization, while enhancing ADCC and ADCP.110 In clinical studies targeting unresectable, locally advanced, recurrent, or metastatic HER2-positive breast cancer, zanidatamab and docetaxel demonstrated substantial antitumor activity. The combination yielded an ORR of 90.9% (95% CI: 75.7–98.1%) and a disease control rate (DCR) of 97.0% (95% CI: 84.2–99.9%), with a median duration of response of 23.5 months (95% CI: 11.3–NE). Median PFS reached 22.1 months (95% CI: 12.7–NE), while median OS was 36.9 months (95% CI: 36.9–NE).111 Another randomized clinical trial (NCT04224272) investigated zanidatamab combined with pembrolizumab and fulvestrant in patients with HR-positive/HER2-positive breast cancer, achieving a 6-month PFS rate of 66.7% (95% CI: 52.1–79.2%).112 These observations support multi-epitope HER2 targeting as a promising strategy to circumvent HER2 signaling heterogeneity.
By binding to the ATP-binding site of the HER2 intracellular tyrosine kinase domain, small-molecule tyrosine kinase inhibitors (TKIs) block receptor autophosphorylation and disrupt downstream signaling pathways, including PI3K/AKT and MAPK.113 Their antitumor activity is not fully dependent on HER2 membrane expression levels, suggesting that TKIs may provide more consistent inhibition in tumors with heterogeneous HER2 expression.113,114 Lapatinib, a first-generation reversible dual HER1/HER2 TKI, was the first agent to demonstrate the clinical feasibility of targeting the intracellular HER2 kinase domain. However, its reversible binding properties result in limited durability of HER signaling inhibition, which may partially restrict its therapeutic activity in tumors with heterogeneous HER2 expression.115 In contrast, the irreversible pan-HER TKIs neratinib and pyrotinib achieve more sustained blockade of HER signaling through covalent binding while simultaneously expanding the spectrum of HER family receptor inhibition.116 The phase III NALA trial demonstrated that neratinib plus capecitabine significantly reduced the risk of disease progression or death in patients with metastatic breast cancer who had received at least two prior lines of anti-HER2 therapy (HR = 0.76, 95% CI: 0.63–0.93; P = 0.0059).117 Similarly, the PHOEBE trial showed that pyrotinib combined with capecitabine significantly improved PFS in patients previously treated with trastuzumab (median PFS: 12.5 vs 6.8 months; HR = 0.39; P < 0.0001).118 These findings suggest that irreversible pan-HER inhibition may provide more durable pathway blockade in tumors with heterogeneous HER2 expression.
In the HER2CLIMB trial, the addition of tucatinib to trastuzumab and capecitabine yielded significantly improved outcomes for patients with previously treated HER2-positive metastatic breast cancer.119 Both OS and PFS were significantly prolonged compared with the control group (trastuzumab plus capecitabine alone). The HER2CLIMB-02 study further evaluated tucatinib combined with T-DM1 in the population with locally advanced or metastatic HER2-positive disease.120 Median PFS was superior in the tucatinib arm relative to the control arm (9.5 vs 7.4 months; HR = 0.76; 95% CI: 0.61–0.95; P = 0.0163). Integration of clinical findings with preclinical studies suggests that HER2 TKIs combined with trastuzumab or ADCs enhance antitumor activity through simultaneous blockade of both extracellular and intracellular HER2 signaling, resulting in a synergistic effect.114,121,122 In tumors with heterogeneous HER2 expression, the drug combination may offer advantages in overcoming HER2 heterogeneity.
BL-B01D1 is a bispecific ADC targeting EGFR and HER3. Upon binding to EGFR or HER3 receptors on tumor cells, the ADC undergoes internalization and releases its cytotoxic payload, Ed-04, within lysosomes, where the released payload induces tumor cell death by inhibiting DNA replication and RNA synthesis.123 Phase I clinical studies have demonstrated preliminary antitumor activity of BL-B01D1 in multiple solid tumor types.124 Ongoing clinical trials are evaluating BL-B01D1 in patients with unresectable locally advanced or metastatic triple-negative breast cancer, and for HR-positive/HER2-negative breast cancer, with its efficacy yet to be established.
Significant progress has been made in the treatment of HER2-positive and HER2-low breast cancer over the past decade. However, high-quality clinical evidence directly supporting the efficacy of these therapeutic strategies in tumors with confirmed HER2 heterogeneity remains limited (Table 2). Most existing clinical studies have not incorporated HER2 heterogeneity as a stratification or selection criterion at enrollment, making it difficult to determine which strategy is most effective for heterogeneous tumors. At present, the efficacy of these treatments in HER2-heterogeneous tumors is largely derived from mechanistic speculation or indirect evidence observed in unselected populations without heterogeneity screening. A fundamental challenge is the lack of a unified pathological definition and standardized detection system for HER2 heterogeneity. This lack of standardization hinders accurate patient identification and complicates comparisons across studies. Future efforts should aim to establish standardized diagnostic and grading systems for HER2 heterogeneity. Incorporating these parameters as key stratification factors in prospective clinical trials will be essential to optimize patient selection and move toward truly precise, individualized treatment.
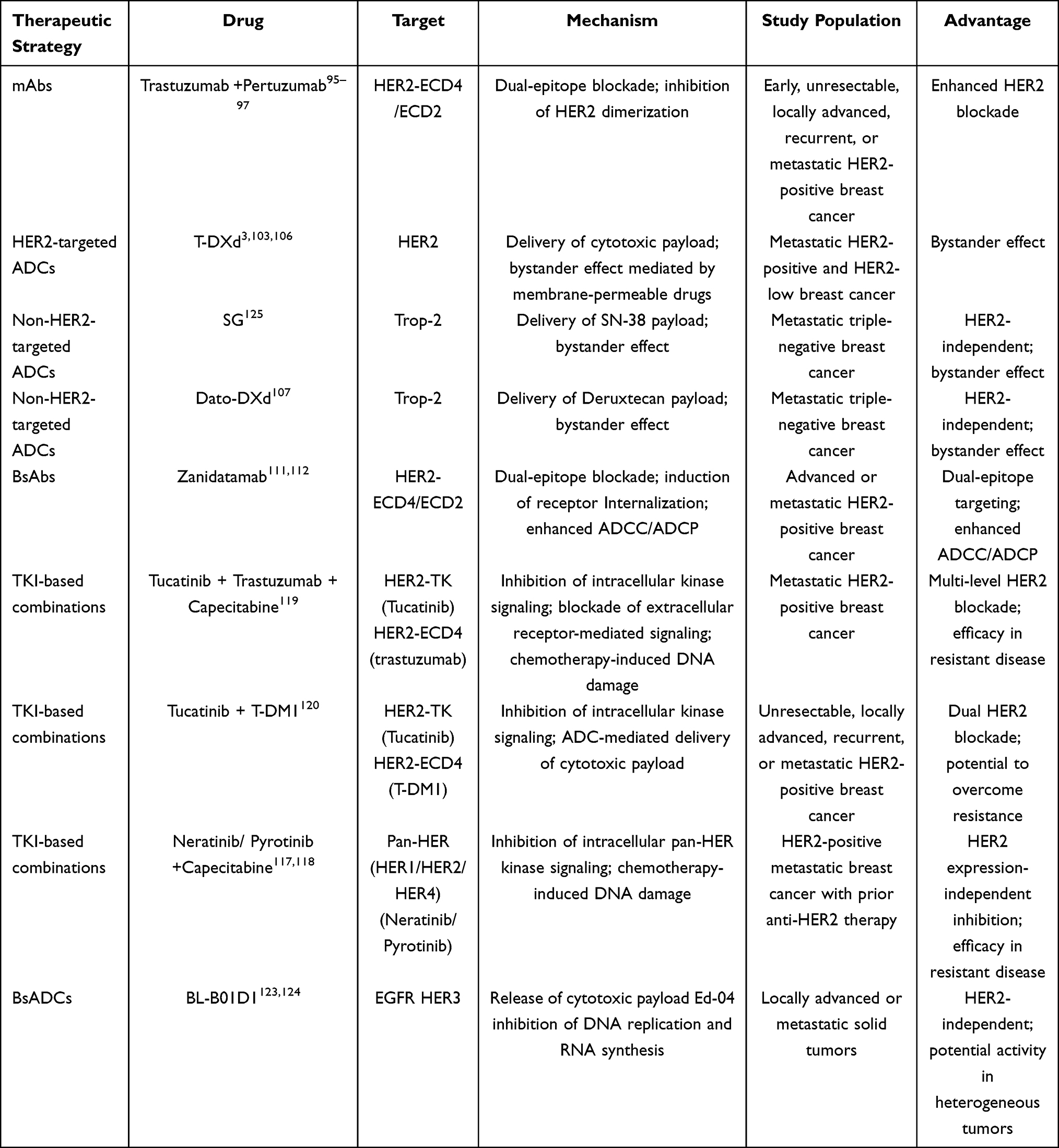 |
Table 2 Therapeutic Strategies to Overcome HER2 Heterogeneity in Breast Cancer |
Conclusion
As a critical driver molecule in breast cancer, the expression status of HER2 has long served as a key determinant for patient classification and for guiding anti-HER2 therapy. Numerous studies indicate that HER2 expression exhibits complex spatiotemporal and molecular heterogeneity in breast cancer. HER2 heterogeneity not only complicates accurate HER2 assessment but also contributes to substantial variability in treatment response and promotes therapeutic resistance. Further studies have revealed that HER2 heterogeneity affects the efficacy of anti-HER2 therapies through multiple mechanisms, including the target dilution effect, activation of bypass signaling pathways, and clonal selection.
A more comprehensive understanding of HER2 expression in tumors may be achieved by optimizing testing strategies, strengthening dynamic assessment at recurrence and metastasis, and incorporating emerging approaches such as liquid biopsy and molecular imaging. Meanwhile, the development of next-generation ADCs and multi-targeted combination strategies offers new avenues to overcome resistance associated with HER2 heterogeneity. Integrating multidimensional molecular information and refining patient stratification systems will be critical to advancing precision medicine in breast cancer.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–15. doi:10.3322/caac.21660
2. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. doi:10.1126/science.3798106
3. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
4. Hou Y, Nitta H, Li Z. HER2 intratumoral heterogeneity in breast cancer, an evolving Concept. Cancers. 2023;15(10). doi:10.3390/cancers15102664
5. Beca F, Polyak K. Intratumor heterogeneity in breast cancer. Adv Exp Med Biol. 2016;882:169–189. doi:10.1007/978-3-319-22909-6_7
6. Ng CK, Martelotto LG, Gauthier A, et al. Intra-tumor genetic heterogeneity and alternative driver genetic alterations in breast cancers with heterogeneous HER2 gene amplification. Genome Biol. 2015;16(1):107. doi:10.1186/s13059-015-0657-6
7. Hou Y, Nitta H, Wei L, et al. HER2 intratumoral heterogeneity is independently associated with incomplete response to anti-HER2 neoadjuvant chemotherapy in HER2-positive breast carcinoma. Breast Cancer Res Treat. 2017;166(2):447–457. doi:10.1007/s10549-017-4453-8
8. Santoro A, Vegni F, d’Amati A, et al. HER2 intratumoral heterogeneity predicts response to neoadjuvant therapy in HER2-positive breast cancer: impact and interplay with HER3 expression. Virchows Arch. 2025. doi:10.1007/s00428-025-04310-3
9. Hosonaga M, Arima Y, Sampetrean O, et al. HER2 heterogeneity is associated with poor survival in HER2-positive breast cancer. Int J Mol Sci. 2018;19(8). doi:10.3390/ijms19082158
10. Tarantino P, Hamilton E, Tolaney SM, et al. HER2-Low Breast Cancer: pathological and Clinical Landscape. J Clin Oncol. 2020;38(17):1951–1962. doi:10.1200/jco.19.02488
11. Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25(1):118–145. doi:10.1200/jco.2006.09.2775
12. Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997–4013. doi:10.1200/jco.2013.50.9984
13. Wolff AC, Hammond MEH, Allison KH, et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol. 2018;36(20):2105–2122. doi:10.1200/jco.2018.77.8738
14. Wolff AC, Somerfield MR, Dowsett M, et al. Human epidermal growth factor receptor 2 testing in breast cancer: ASCO-College of American Pathologists Guideline Update. J Clin Oncol. 2023;41(22):3867–3872. doi:10.1200/jco.22.02864
15. Sapino A, Goia M, Recupero D, Marchiò C. Current challenges for HER2 testing in diagnostic pathology: state of the art and controversial issues. Front Oncol. 2013;3:129. doi:10.3389/fonc.2013.00129
16. Zhang H, Katerji H, Turner BM, Hicks DG. HER2-low breast cancers. Am J Clin Pathol. 2022;157(3):328–336. doi:10.1093/ajcp/aqab117
17. Yildiz-Aktas IZ, Dabbs DJ, Bhargava R. The effect of cold ischemic time on the immunohistochemical evaluation of estrogen receptor, progesterone receptor, and HER2 expression in invasive breast carcinoma. Mod Pathol. 2012;25(8):1098–1105. doi:10.1038/modpathol.2012.59
18. Mirlacher M, Kasper M, Storz M, et al. Influence of slide aging on results of translational research studies using immunohistochemistry. Mod Pathol. 2004;17(11):1414–1420. doi:10.1038/modpathol.3800208
19. Rüschoff J, Friedrich M, Nagelmeier I, et al. Comparison of HercepTest™ mAb pharmDx (Dako Omnis, GE001) with Ventana PATHWAY anti-HER-2/neu (4B5) in breast cancer: correlation with HER2 amplification and HER2 low status. Virchows Arch. 2022;481(5):685–694. doi:10.1007/s00428-022-03378-5
20. Dabbs DJ, Torlakovic E, Nielsen S, et al. New standards in HER2-low testing: the CASI-01 comparative methods study. EBioMedicine. 2025;120:105919. doi:10.1016/j.ebiom.2025.105919
21. Robbins CJ, Fernandez AI, Han G, et al. Multi-institutional Assessment of Pathologist Scoring HER2 Immunohistochemistry. Mod Pathol. 2023;36(1):100032. doi:10.1016/j.modpat.2022.100032
22. Wu S, Shang J, Li Z, et al. Interobserver consistency and diagnostic challenges in HER2-ultralow breast cancer: a multicenter study. ESMO Open. 2025;10(2):104127. doi:10.1016/j.esmoop.2024.104127
23. Nielsen K, Sode M, Jensen MB, et al. High inter-laboratory variability in the assessment of HER2-low breast cancer: a national registry study on 50,714 Danish patients. Breast Cancer Res. 2023;25(1):139. doi:10.1186/s13058-023-01739-9
24. Zhong J, Gao B, Wang Q, et al. Exploring the heterogeneity of HER2 gene status and expression in non-positive breast cancer patients: insights from immunohistochemistry and fluorescence in situ hybridization. Diagn Pathol. 2025;20(1):4. doi:10.1186/s13000-024-01594-y
25. Peng R, Zhang K, Lin G, Li J. Interlaboratory variability of HER2 fluorescence in situ hybridization testing in breast cancer: results of a multicenter proficiency-testing ring study in China. Diagn Pathol. 2024;19(1):161. doi:10.1186/s13000-024-01588-w
26. Liwski CR, Castonguay MC, Barnes PJ, Rayson D, Bethune GC. HER2 testing in metastatic breast cancer - Is reflex ISH testing necessary on HER2 IHC-equivocal (2+) cases? Ann Diagn Pathol. 2022;59:151953. doi:10.1016/j.anndiagpath.2022.151953
27. Pellas U, Bauer A, Baroš IV, Fattorini C, Tot T. HER2-low metastases of HER2-negative primary tumors: a single institution analysis of intertumoral and internodal heterogeneity in node-positive breast cancer. Front Oncol. 2023;13:1167567. doi:10.3389/fonc.2023.1167567
28. Hu X, Chen W, Li F, et al. Expression changes of ER, PR, HER2, and Ki-67 in primary and metastatic breast cancer and its clinical significance. Front Oncol. 2023;13:1053125. doi:10.3389/fonc.2023.1053125
29. Lin M, Luo T, Jin Y, et al. HER2-low heterogeneity between primary and paired recurrent/metastatic breast cancer: implications in treatment and prognosis. Cancer. 2024;130(6):851–862. doi:10.1002/cncr.35101
30. Tretschock LM, Clemente H, Smetanay K, et al. HER2(-Low) expression on circulating tumor cells and corresponding metastatic tissue in metastatic breast cancer. Oncol Res Treat. 2025;48(4):161–173. doi:10.1159/000542830
31. Wu S, Liu H, Wang T, et al. HER2 testing in multifocal/multicentric breast cancer: should all foci be tested in the context of HER2-low and HER2-ultralow? Breast. 2025;84:104572. doi:10.1016/j.breast.2025.104572
32. Geukens T, De Schepper M, Richard F, et al. Intra-patient and inter-metastasis heterogeneity of HER2-low status in metastatic breast cancer. Eur J Cancer. 2023;188:152–160. doi:10.1016/j.ejca.2023.04.026
33. Jeong YH, Hong SA, Ahn HS, Ahn SK, Kim MK. Clinicopathologic factors affecting discrepancies in HER2 overexpression between core needle biopsy and surgical biopsy in breast cancer patients according to neoadjuvant treatment or not. J Cancer. 2021;12(15):4722–4728. doi:10.7150/jca.59419
34. Li Z, Metzger Filho O, Viale G, et al. HER2 heterogeneity and treatment response-associated profiles in HER2-positive breast cancer in the NCT02326974 clinical trial. J Clin Invest. 2024;134(7). doi:10.1172/jci176454
35. Guarneri V, Dieci MV, Barbieri E, et al. Loss of HER2 positivity and prognosis after neoadjuvant therapy in HER2-positive breast cancer patients. Ann Oncol. 2013;24(12):2990–2994. doi:10.1093/annonc/mdt364
36. Mittendorf EA, Wu Y, Scaltriti M, et al. Loss of HER2 amplification following trastuzumab-based neoadjuvant systemic therapy and survival outcomes. Clin Cancer Res. 2009;15(23):7381–7388. doi:10.1158/1078-0432.Ccr-09-1735
37. Loganzo F, Tan X, Sung M, et al. Tumor cells chronically treated with a trastuzumab-maytansinoid antibody-drug conjugate develop varied resistance mechanisms but respond to alternate treatments. Mol Cancer Ther. 2015;14(4):952–963. doi:10.1158/1535-7163.Mct-14-0862
38. Miglietta F, Griguolo G, Bottosso M, et al. HER2-low-positive breast cancer: evolution from primary tumor to residual disease after neoadjuvant treatment. NPJ Breast Cancer. 2022;8(1):66. doi:10.1038/s41523-022-00434-w
39. Kang S, Lee SH, Lee HJ, et al. Prognostic implications of HER2 changes after neoadjuvant chemotherapy in patients with HER2-zero and HER2-low breast cancer. Eur J Cancer. 2023;191:112956. doi:10.1016/j.ejca.2023.112956
40. Lian J, Yao R, Pang S, Ren X, Pan B, Zhou Y. Comprehensive analysis of HER2 low breast cancer response to neoadjuvant chemotherapy, a retrospective cohort study. Clin Breast Cancer. 2025;25(6):e801–e817e3. doi:10.1016/j.clbc.2025.03.013
41. Li YW, Dai LJ, Wu XR, et al. Molecular characterization and classification of HER2-positive breast cancer inform tailored therapeutic strategies. Cancer Res. 2024;84(21):3669–3683. doi:10.1158/0008-5472.Can-23-4066
42. Ferrari A, Vincent-Salomon A, Pivot X, et al. A whole-genome sequence and transcriptome perspective on HER2-positive breast cancers. Nat Commun. 2016;7:12222. doi:10.1038/ncomms12222
43. Li J, Yao J, Qi L. HER2 low expression breast cancer subtyping and their correlation with prognosis and immune landscape based on the histone modification related genes. Sci Rep. 2023;13(1):21753. doi:10.1038/s41598-023-49010-7
44. Buckley NE, Forde C, McArt DG, et al. Quantification of HER2 heterogeneity in breast cancer-implications for identification of sub-dominant clones for personalised treatment. Sci Rep. 2016;6:23383. doi:10.1038/srep23383
45. Hanna WM, Rüschoff J, Bilous M, et al. HER2 in situ hybridization in breast cancer: clinical implications of polysomy 17 and genetic heterogeneity. Mod Pathol. 2014;27(1):4–18. doi:10.1038/modpathol.2013.103
46. Marchiò C, Annaratone L, Marques A, Casorzo L, Berrino E, Sapino A. Evolving concepts in HER2 evaluation in breast cancer: heterogeneity, HER2-low carcinomas and beyond. Semin Cancer Biol. 2021;72:123–135. doi:10.1016/j.semcancer.2020.02.016
47. Ju J, Du F, Gao SL, et al. Combined analysis of receptor expression reflects inter-and intra-tumor heterogeneity in HR+/HER2+ breast cancer. Breast Cancer Res Treat. 2022;194(2):221–230. doi:10.1007/s10549-022-06629-w
48. Guerriero JL, Lin JR, Pastorello RG, et al. Qualification of a multiplexed tissue imaging assay and detection of novel patterns of HER2 heterogeneity in breast cancer. NPJ Breast Cancer. 2024;10(1):2. doi:10.1038/s41523-023-00605-3
49. Prat A, Pascual T, De Angelis C, et al. HER2-enriched subtype and ERBB2 expression in HER2-positive breast cancer treated with dual HER2 blockade. J Natl Cancer Inst. 2020;112(1):46–54. doi:10.1093/jnci/djz042
50. Schettini F, Pascual T, Conte B, et al. HER2-enriched subtype and pathological complete response in HER2-positive breast cancer: a systematic review and meta-analysis. Cancer Treat Rev. 2020;84:101965. doi:10.1016/j.ctrv.2020.101965
51. Carey LA, Berry DA, Cirrincione CT, et al. Molecular heterogeneity and response to neoadjuvant human epidermal growth factor receptor 2 targeting in CALGB 40601, a randomized phase III trial of paclitaxel plus trastuzumab with or without lapatinib. J Clin Oncol. 2016;34(6):542–549. doi:10.1200/jco.2015.62.1268
52. Tanei T, Seno S, Sota Y, et al. High HER2 intratumoral heterogeneity is a predictive factor for poor prognosis in early-stage and locally advanced HER2-positive breast cancer. Cancers. 2024;16(5). doi:10.3390/cancers16051062
53. Filho OM, Viale G, Stein S, et al. Impact of HER2 heterogeneity on treatment response of early-stage HER2-positive breast cancer: phase ii neoadjuvant clinical trial of T-DM1 combined with pertuzumab. Cancer Discov. 2021;11(10):2474–2487. doi:10.1158/2159-8290.Cd-20-1557
54. Rye IH, Trinh A, Saetersdal AB, et al. Intratumor heterogeneity defines treatment-resistant HER2+ breast tumors. Mol Oncol. 2018;12(11):1838–1855. doi:10.1002/1878-0261.12375
55. de Moraes FCA, de Castro Ribeiro CHD, Pessôa F, et al. Pathologic response rates in HER2-low versus HER2-zero early breast cancer patients receiving neoadjuvant therapy: a systematic review and meta-analysis. Breast Cancer Res. 2025;27(1):39. doi:10.1186/s13058-025-01989-9
56. Liu JJ, Zhang Y, Zhang SC, et al. Analysis of factors influencing the efficacy of NAC and prognosis between HER2-zero and HER2-low HR negative breast cancer. Front Cell Dev Biol. 2024;12:1417271. doi:10.3389/fcell.2024.1417271
57. Baez-Navarro X, van Bockstal MR, Jager A, van Deurzen CHM. HER2-low breast cancer and response to neoadjuvant chemotherapy: a population-based cohort study. Pathology. 2024;56(3):334–342. doi:10.1016/j.pathol.2023.10.022
58. Denkert C, Seither F, Schneeweiss A, et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol. 2021;22(8):1151–1161. doi:10.1016/s1470-2045(21)00301-6
59. Jiao D, Li G, Dai H, et al. Comparison of the response to neoadjuvant therapy between immunohistochemistry HER2 (3+) and HER2 (2+)/ISH+ early-stage breast cancer: a retrospective multicenter cohort study. Oncologist. 2024;29(7):e877–e886. doi:10.1093/oncolo/oyae047
60. Wang Y, Singh K, Dizon D, Graves T, Amin A, Yakirevich E. Immunohistochemical HER2 score correlates with response to neoadjuvant chemotherapy in HER2-positive primary breast cancer. Breast Cancer Res Treat. 2021;186(3):667–676. doi:10.1007/s10549-021-06124-8
61. Nakatani S, Hayashi T, Yamamoto K, Maeda H. Impact of loss of HER2 positivity following neoadjuvant therapy in HER2-positive breast cancer patients on long-term prognosis: a systematic review and meta-analysis. Cancer Treat Rev. 2025;135:102923. doi:10.1016/j.ctrv.2025.102923
62. Gong C, Liu C, Tao Z, et al. Temporal heterogeneity of HER2 expression and spatial heterogeneity of (18)F-FDG uptake predicts treatment outcome of pyrotinib in patients with HER2-Positive metastatic breast cancer. Cancers. 2022;14(16). doi:10.3390/cancers14163973
63. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(10):1674. doi:10.1093/annonc/mdz189
64. von Minckwitz G, Procter M, de Azambuja E, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N Engl J Med. 2017;377(2):122–131. doi:10.1056/NEJMoa1703643
65. Rexer BN, Chanthaphaychith S, Dahlman K, Arteaga CL. Direct inhibition of PI3K in combination with dual HER2 inhibitors is required for optimal antitumor activity in HER2+ breast cancer cells. Breast Cancer Res. 2014;16(1):R9. doi:10.1186/bcr3601
66. Li X, Xu Y, Ding Y, et al. Posttranscriptional upregulation of HER3 by HER2 mRNA induces trastuzumab resistance in breast cancer. Mol Cancer. 2018;17(1):113. doi:10.1186/s12943-018-0862-5
67. Nahta R, Yuan LX, Zhang B, Kobayashi R, Esteva FJ. Insulin-like growth factor-I receptor/human epidermal growth factor receptor 2 heterodimerization contributes to trastuzumab resistance of breast cancer cells. Cancer Res. 2005;65(23):11118–11128. doi:10.1158/0008-5472.Can-04-3841
68. Hanker AB, Garrett JT, Estrada MV, et al. HER2-overexpressing breast cancers amplify FGFR signaling upon acquisition of resistance to dual therapeutic blockade of HER2. Clin Cancer Res. 2017;23(15):4323–4334. doi:10.1158/1078-0432.Ccr-16-2287
69. Hanker AB, Estrada MV, Bianchini G, et al. Extracellular matrix/integrin signaling promotes resistance to combined inhibition of HER2 and PI3K in HER2(+) breast cancer. Cancer Res. 2017;77(12):3280–3292. doi:10.1158/0008-5472.Can-16-2808
70. Scaltriti M, Rojo F, Ocaña A, et al. Expression of p95HER2, a truncated form of the HER2 receptor, and response to anti-HER2 therapies in breast cancer. J Natl Cancer Inst. 2007;99(8):628–638. doi:10.1093/jnci/djk134
71. Ruocco MR, Gisonna A, Acampora V, et al. Guardians and mediators of metastasis: exploring T Lymphocytes, myeloid-derived suppressor cells, and tumor-associated macrophages in the breast cancer microenvironment. Int J Mol Sci. 2024;25(11). doi:10.3390/ijms25116224
72. Mollavelioglu B, Cetin Aktas E, Cabioglu N, et al. High co-expression of immune checkpoint receptors PD-1, CTLA-4, LAG-3, TIM-3, and TIGIT on tumor-infiltrating lymphocytes in early-stage breast cancer. World J Surg Oncol. 2022;20(1):349. doi:10.1186/s12957-022-02810-z
73. Peng D, Tanikawa T, Li W, et al. Myeloid-derived suppressor cells endow stem-like qualities to breast cancer cells through IL6/STAT3 and NO/NOTCH cross-talk signaling. Cancer Res. 2016;76(11):3156–3165. doi:10.1158/0008-5472.Can-15-2528
74. Gong B, Zheng L. Subtype-specific heterogeneity of myeloid-derived suppressor cells in breast cancer: current insights and future directions. PeerJ. 2026;14:e20937. doi:10.7717/peerj.20937
75. Neo SY, Tong L, Chong J, et al. Tumor-associated NK cells drive MDSC-mediated tumor immune tolerance through the IL-6/STAT3 axis. Sci Transl Med. 2024;16(747):eadi2952. doi:10.1126/scitranslmed.adi2952
76. Mantovani A, Allavena P, Marchesi F, Garlanda C. Macrophages as tools and targets in cancer therapy. Nat Rev Drug Discov. 2022;21(11):799–820. doi:10.1038/s41573-022-00520-5
77. Yang C, He L, He P, et al. Increased drug resistance in breast cancer by tumor-associated macrophages through IL-10/STAT3/bcl-2 signaling pathway. Med Oncol. 2015;32(2):352. doi:10.1007/s12032-014-0352-6
78. Ahmed S, Mohamed HT, El-Husseiny N, et al. IL-8 secreted by tumor associated macrophages contribute to lapatinib resistance in HER2-positive locally advanced breast cancer via activation of Src/STAT3/ERK1/2-mediated EGFR signaling. Biochim Biophys Acta Mol Cell Res. 2021;1868(6):118995. doi:10.1016/j.bbamcr.2021.118995
79. Petty AJ, Dai R, Lapalombella R, et al. Hedgehog-induced PD-L1 on tumor-associated macrophages is critical for suppression of tumor-infiltrating CD8+ T cell function. JCI Insight. 2021;6(6). doi:10.1172/jci.insight.146707
80. Tsao LC, Crosby EJ, Trotter TN, et al. CD47 blockade augmentation of trastuzumab antitumor efficacy dependent on antibody-dependent cellular phagocytosis. JCI Insight. 2019;4(24). doi:10.1172/jci.insight.131882
81. Su S, Zhao J, Xing Y, et al. Immune checkpoint inhibition overcomes ADCP-induced immunosuppression by macrophages. Cell. 2018;175(2):442–457.e23. doi:10.1016/j.cell.2018.09.007
82. Chen JS, Teng YN, Chen CY, Chen JY. A novel STAT3/ NFκB p50 axis regulates stromal-KDM2A to promote M2 macrophage-mediated chemoresistance in breast cancer. Cancer Cell Int. 2023;23(1):237. doi:10.1186/s12935-023-03088-1
83. Gennari A, André F, Barrios CH, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. doi:10.1016/j.annonc.2021.09.019
84. Bensch F, Brouwers AH, Lub-de Hooge MN, et al. (89)Zr-trastuzumab PET supports clinical decision making in breast cancer patients, when HER2 status cannot be determined by standard work up. Eur J Nucl Med Mol Imaging. 2018;45(13):2300–2306. doi:10.1007/s00259-018-4099-8
85. Mileva M, de Vries EGE, Guiot T, et al. Molecular imaging predicts lack of T-DM1 response in advanced HER2-positive breast cancer (final results of ZEPHIR trial). NPJ Breast Cancer. 2024;10(1):4. doi:10.1038/s41523-023-00610-6
86. Eisses B, van Geel JJL, Brouwers AH, et al. Whole-body HER2 heterogeneity identified on HER2 PET in HER2-negative, -low, and -positive metastatic breast cancer. J Nucl Med. 2024;65(10):1540–1547. doi:10.2967/jnumed.124.267636
87. Altena R, Burén SA, Blomgren A, et al. Human epidermal growth factor receptor 2 (HER2) PET imaging of HER2-low breast cancer with [(68)Ga]Ga-ABY-025: results from a pilot study. J Nucl Med. 2024;65(5):700–707. doi:10.2967/jnumed.123.266847
88. Qaiser T, Mukherjee A, Reddy Pb C, et al. HER2 challenge contest: a detailed assessment of automated HER2 scoring algorithms in whole slide images of breast cancer tissues. Histopathology. 2018;72(2):227–238. doi:10.1111/his.13333
89. Farahmand S, Fernandez AI, Ahmed FS, et al. Deep learning trained on hematoxylin and eosin tumor region of Interest predicts HER2 status and trastuzumab treatment response in HER2+ breast cancer. Mod Pathol. 2022;35(1):44–51. doi:10.1038/s41379-021-00911-w
90. Zakrzewski F, de Back W, Weigert M, et al. Automated detection of the HER2 gene amplification status in Fluorescence in situ hybridization images for the diagnostics of cancer tissues. Sci Rep. 2019;9(1):8231. doi:10.1038/s41598-019-44643-z
91. Wu S, Yue M, Zhang J, et al. The role of artificial intelligence in accurate interpretation of HER2 immunohistochemical scores 0 and 1+ in breast cancer. Mod Pathol. 2023;36(3):100054. doi:10.1016/j.modpat.2022.100054
92. Albuquerque DAN, Vianna MT, Sampaio LAF, Vasiliu A, Neves Filho EHC. Systematic review and meta-analysis of artificial intelligence in classifying HER2 status in breast cancer immunohistochemistry. NPJ Digit Med. 2025;8(1):144. doi:10.1038/s41746-025-01483-8
93. Zhang J, Li Y, Li Z, et al. Deep-learning-based HER2 status assessment from multimodal breast cancer data predicts neoadjuvant therapy response. Nat Biomed Eng. 2025. doi:10.1038/s41551-025-01495-5
94. Ma D, Dai LJ, Wu XR, et al. Spatial determinants of antibody-drug conjugate SHR-A1811 efficacy in neoadjuvant treatment for HER2-positive breast cancer. Cancer Cell. 2025;43(6):1061–1075.e7. doi:10.1016/j.ccell.2025.03.017
95. Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, Phase 2 trial. Lancet Oncol. 2012;13(1):25–32. doi:10.1016/s1470-2045(11)70336-9
96. Piccart M, Procter M, Fumagalli D, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer in the APHINITY trial: 6 years’ follow-up. J Clin Oncol. 2021;39(13):1448–1457. doi:10.1200/jco.20.01204
97. Swain SM, Miles D, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, Phase 3 study. Lancet Oncol. 2020;21(4):519–530. doi:10.1016/s1470-2045(19)30863-0
98. Franklin MC, Carey KD, Vajdos FF, Leahy DJ, de Vos AM, Sliwkowski MX. Insights into ErbB signaling from the structure of the ErbB2-pertuzumab complex. Cancer Cell. 2004;5(4):317–328. doi:10.1016/s1535-6108(04)00083-2
99. Molina MA, Codony-Servat J, Albanell J, Rojo F, Arribas J, Baselga J. Trastuzumab (herceptin), a humanized anti-Her2 receptor monoclonal antibody, inhibits basal and activated Her2 ectodomain cleavage in breast cancer cells. Cancer Res. 2001;61(12):4744–4749.
100. Staudacher AH, Brown MP. Antibody drug conjugates and bystander killing: is antigen-dependent internalisation required? Br J Cancer. 2017;117(12):1736–1742. doi:10.1038/bjc.2017.367
101. Drago JZ, Modi S, Chandarlapaty S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat Rev Clin Oncol. 2021;18(6):327–344. doi:10.1038/s41571-021-00470-8
102. Tarantino P, Carmagnani Pestana R, Corti C, et al. Antibody-drug conjugates: smart chemotherapy delivery across tumor histologies. CA Cancer J Clin. 2022;72(2):165–182. doi:10.3322/caac.21705
103. Cortés J, Hurvitz SA, Im SA, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in HER2-positive metastatic breast cancer: long-term survival analysis of the DESTINY-Breast03 trial. Nat Med. 2024;30(8):2208–2215. doi:10.1038/s41591-024-03021-7
104. Ogitani Y, Hagihara K, Oitate M, Naito H, Agatsuma T. Bystander killing effect of DS-8201a, a novel anti-human epidermal growth factor receptor 2 antibody-drug conjugate, in tumors with human epidermal growth factor receptor 2 heterogeneity. Cancer Sci. 2016;107(7):1039–1046. doi:10.1111/cas.12966
105. Rakha EA, Tan PH, Van Bockstal MR, et al. International expert consensus recommendations for HER2 reporting in breast cancer: focus on HER2-low and ultralow categories. Mod Pathol. 2026;39(1):100925. doi:10.1016/j.modpat.2025.100925
106. Bardia A, Hu X, Dent R, et al. Trastuzumab deruxtecan after endocrine therapy in metastatic breast cancer. N Engl J Med. 2024;391(22):2110–2122. doi:10.1056/NEJMoa2407086
107. Bardia A, Jhaveri K, Im SA, et al. Datopotamab deruxtecan versus chemotherapy in previously treated inoperable/metastatic hormone receptor-positive human epidermal growth factor receptor 2-negative breast cancer: primary results from TROPION-Breast01. J Clin Oncol. 2025;43(3):285–296. doi:10.1200/jco.24.00920
108. Nelson BE, Meric-Bernstam F. Leveraging TROP2 antibody-drug conjugates in solid tumors. Annu Rev Med. 2024;75:31–48. doi:10.1146/annurev-med-071322-065903
109. Tarantino P, Morganti S, Curigliano G. Targeting HER2 in breast cancer: new drugs and paradigms on the horizon. Explor Target Antitumor Ther. 2021;2(2):139–155. doi:10.37349/etat.2021.00037
110. Weisser NE, Sanches M, Escobar-Cabrera E, et al. An anti-HER2 biparatopic antibody that induces unique HER2 clustering and complement-dependent cytotoxicity. Nat Commun. 2023;14(1):1394. doi:10.1038/s41467-023-37029-3
111. Wang X, Lee KS, Zeng X, et al. Zanidatamab in combination with docetaxel in first-line HER2-positive breast cancer: results from an open-label, multicenter, phase Ib/II study. ESMO Open. 2025;10(11):105852. doi:10.1016/j.esmoop.2025.105852
112. Escrivá-de-Romani S, Cejalvo JM, Alba E, et al. Zanidatamab plus palbociclib and fulvestrant in previously treated patients with hormone receptor-positive, HER2-positive metastatic breast cancer: primary results from a two-part, multicentre, single-arm, phase 2a study. Lancet Oncol. 2025;26(6):745–758. doi:10.1016/s1470-2045(25)00140-8
113. Scaltriti M, Baselga J. The epidermal growth factor receptor pathway: a model for targeted therapy. Clin Cancer Res. 2006;12(18):5268–5272. doi:10.1158/1078-0432.Ccr-05-1554
114. Arshad M, Azad A, Chan PYK, et al. Neratinib could be effective as monotherapy or in combination with trastuzumab in HER2-low breast cancer cells and organoid models. Br J Cancer. 2024;130(12):1990–2002. doi:10.1038/s41416-024-02665-z
115. Frampton JE. Lapatinib: a review of its use in the treatment of HER2-overexpressing, trastuzumab-refractory, advanced or metastatic breast cancer. Drugs. 2009;69(15):2125–2148. doi:10.2165/11203240-000000000-00000
116. Xuhong JC, Qi XW, Zhang Y, Jiang J. Mechanism, safety and efficacy of three tyrosine kinase inhibitors lapatinib, neratinib and pyrotinib in HER2-positive breast cancer. Am J Cancer Res. 2019;9(10):2103–2119.
117. Saura C, Oliveira M, Feng YH, et al. Neratinib plus capecitabine versus lapatinib plus capecitabine in HER2-positive metastatic breast cancer previously treated with ≥ 2 HER2-directed regimens: phase III NALA trial. J Clin Oncol. 2020;38(27):3138–3149. doi:10.1200/jco.20.00147
118. Xu B, Yan M, Ma F, et al. Pyrotinib plus capecitabine versus lapatinib plus capecitabine for the treatment of HER2-positive metastatic breast cancer (PHOEBE): a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol Mar. 2021;22(3):351–360. doi:10.1016/s1470-2045(20)30702-6
119. Curigliano G, Mueller V, Borges V, et al. Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2+ metastatic breast cancer with and without brain metastases (HER2CLIMB): final overall survival analysis. Ann Oncol. 2022;33(3):321–329. doi:10.1016/j.annonc.2021.12.005
120. Hurvitz SA, Loi S, O’Shaughnessy J, et al. Tucatinib and trastuzumab emtansine for patients with previously treated HER2-positive locally advanced and metastatic breast cancer: primary analysis of the randomized phase III trial HER2CLIMB-02. Ann Oncol. 2026;37(3):341–352. doi:10.1016/j.annonc.2025.11.005
121. Kulukian A, Lee P, Taylor J, et al. Preclinical activity of HER2-selective tyrosine kinase inhibitor tucatinib as a single agent or in combination with trastuzumab or docetaxel in solid tumor models. Mol Cancer Ther. 2020;19(4):976–987. doi:10.1158/1535-7163.Mct-19-0873
122. Olson D, Taylor J, Willis K, et al. HER2-selective and reversible tyrosine kinase inhibitor tucatinib potentiates the activity of T-DM1 in preclinical models of HER2-positive breast cancer. Cancer Res Commun. 2023;3(9):1927–1939. doi:10.1158/2767-9764.Crc-23-0302
123. Liu C, Liu D, Ji Y, et al. A bispecific antibody-drug conjugate targeting EGFR and HER3 in metastatic esophageal squamous cell carcinoma: a Phase 1b trial. Nat Med. 2025;31(10):3485–3491. doi:10.1038/s41591-025-03792-7
124. Ma Y, Huang Y, Zhao Y, et al. BL-B01D1, a first-in-class EGFR-HER3 bispecific antibody-drug conjugate, in patients with locally advanced or metastatic solid tumours: a first-in-human, open-label, multicentre, phase 1 study. Lancet Oncol. 2024;25(7):901–911. doi:10.1016/s1470-2045(24)00159-1
125. Bardia A, Mayer IA, Diamond JR, et al. Efficacy and safety of anti-trop-2 antibody drug conjugate sacituzumab govitecan (IMMU-132) in heavily pretreated patients with metastatic triple-negative breast cancer. J Clin Oncol. 2017;35(19):2141–2148. doi:10.1200/jco.2016.70.8297
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.