Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
HER2 Expression and Axillary Metastasis in Treatment-Naïve Early Breast Cancer
Authors Aydin F, Yuksel C ![]() , Akyuz C, Pulat H, Tunc E, Sağdıç MF
, Akyuz C, Pulat H, Tunc E, Sağdıç MF ![]() , Aksel B, Dogan L
, Aksel B, Dogan L
Received 21 April 2026
Accepted for publication 1 July 2026
Published 9 July 2026 Volume 2026:18 618927
DOI https://doi.org/10.2147/BCTT.S618927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Robert Clarke
Ferit Aydin,1 Cemil Yuksel,2 Cuneyt Akyuz,2 Huseyin Pulat,2 Emre Tunc,3 Mehmet Furkan Sağdıç,1 Bulent Aksel,1 Lutfi Dogan1
1Department of Surgical Oncology, Ankara Etlik City Hospital, Yenimahalle, Ankara, Turkey; 2Department of Surgical Oncology, Mersin City Hospital, Mersin, Turkey; 3Department of Surgical Oncology, Sanliurfa Mehmet Akif Inan Training and Research Hospital, Sanliurfa, Turkey
Correspondence: Mehmet Furkan Sağdıç, Department of Surgical Oncology, Ankara Etlik City Hospital, Varlik Neighborhood, Halil Sezai Erkut Avenue, Yenimahalle, Ankara, 06100, Turkey, Tel +905542680141, Email [email protected]
Purpose: The clinical significance of human epidermal growth factor receptor 2 (HER2)–low breast cancer remains controversial, particularly in early-stage, treatment-naïve patients. Because neoadjuvant therapy may alter tumor biology and nodal status, we specifically evaluated patients who underwent upfront surgery without prior systemic treatment. We also investigated whether the recently recognized HER2-ultralow subgroup exhibited differences in axillary metastatic involvement.
Patients and Methods: In this multicenter observational study, we retrospectively analyzed 407 patients with hormone receptor–positive early-stage breast cancer who underwent upfront surgery between 2017 and 2023 without neoadjuvant therapy. Patients were categorized as HER2-ultralow (immuno-histochemistry [IHC] 0), HER2-low (IHC 1+ or 2+ with fluorescence in situ hybridization [FISH] negative), or HER2-positive (IHC 3+ or 2+ with FISH positive). Groups were compared for sentinel lymph node (SLN) positivity. Multivariable logistic regression and receiver operating characteristic (ROC) analyses were used to identify predictors of axillary metastasis.
Results: SLN positivity rates were similar across the HER2-ultralow (29.0%, n = 288), HER2-low (30.6%, n = 80), and HER2-positive groups (31.3%, n = 39) (p = 0.941). HER2 expression was not an independent predictor of SLN positivity. Lymphovascular invasion (LVI) was the strongest determinant (odds ratio = 5.42; 95% confidence interval: 3.13– 9.39; p < 0.001). Larger tumor size and higher proliferative activity were independently associated with increased axillary involvement. ROC analysis showed higher discrimination for LVI (AUC = 0.68) than Ki-67 (AUC = 0.53) and tumor size (AUC = 0.61). Exploratory survival analyses demonstrated no statistically significant differences among groups; however, these findings should be interpreted cautiously because of the limited follow-up duration and low number of events.
Conclusion: In hormone receptor–positive early-stage breast cancer treated with upfront surgery, HER2 expression was not independently associated with axillary metastasis risk in this treatment-naïve cohort. Classical pathological factors, particularly lymphovascular invasion, larger tumor size, and higher proliferative activity, remained the principal determinants of axillary involvement.
Keywords: breast neoplasms, receptor, Her-2, sentinel lymph node biopsy, lymphatic metastasis
Introduction
Breast cancer is the most frequently diagnosed malignancy among women worldwide and remains one of the leading causes of cancer-related mortality, particularly among middle-aged and older women.1–5 Owing to its diverse biological subtypes, this cancer demonstrates significantly heterogeneous clinical behavior in terms of diagnosis, treatment response, and prognosis. Following extensive research, hormone receptor status and the expression of the human epidermal growth factor receptor 2 (HER2) protein have been identified as the principal determinants influencing this heterogeneity.6,7 HER2-positive breast cancers are generally associated with increased proliferative activity and an aggressive clinical course; however, the recent development of targeted anti-HER2 therapies has led to a marked improvement in survival outcomes.8
While patients classified as HER2-negative have long been considered a biologically homogeneous group, recent clinical studies have demonstrated that a substantial proportion of HER2-negative tumors exhibit low-level HER2 protein expression on their cell surfaces.9–11 Furthermore, the introduction of antibody–drug conjugates into clinical practice has led to the emergence of the concept of “HER2-low breast cancer.”.12 Likewise, tumors lacking detectable HER2 expression (HER2-zero/ultralow), as well as those demonstrating HER2 amplification and classified as HER2-positive, are considered biologically and clinically distinct entities.11,13 HER2 expression categories were defined according to contemporary ASCO/CAP criteria and were used to stratify the study population for the present analyses. Recently, the term “HER2-ultralow” has been introduced to describe tumors with faint, incomplete membranous staining in ≤10% of tumor cells that do not meet the criteria for IHC 1+. Historically, these tumors were frequently categorized as HER2-zero. In the present study, this subgroup was classified as HER2-ultralow (IHC 0) for terminology consistency throughout the manuscript.
While some studies suggest that HER2-low tumors exhibit lower proliferative activity and distinct immune microenvironment characteristics compared to HER2-zero cases, there is a lack of substantial evidence demonstrating significant differences in survival or recurrence outcomes between the two subtypes.14 Because of this inconsistency, it remains unclear whether HER2-low breast cancer represents an independent biological subtype. Clarifying this distinction may have important implications for both the development of HER2-targeted therapies and the surgical management of early-stage breast cancer. Therefore, clarifying this relationship is particularly important in treatment-naïve patients, defined as individuals who have not received any prior systemic therapy, including neoadjuvant chemotherapy, endocrine therapy, or anti-HER2–targeted therapy, before surgical intervention.15
The increasing interest in HER2-low breast cancer has largely emerged from its therapeutic relevance, particularly with the development of novel HER2-targeted agents. However, whether HER2-low disease constitutes a biologically distinct subtype remains uncertain. Interpretation of HER2 expression may also be complicated by intratumoral heterogeneity and variability in assessment, especially in tumors with very low levels of HER2 staining. As a result, the boundaries between HER2-zero, HER2-ultralow, and HER2-low categories are not always clearly defined. Therefore, although HER2-low classification has clear clinical relevance, its biological significance continues to be investigated.
Neoadjuvant therapies for breast cancer may alter tumor biology, especially axillary lymph node (ALN) status. In particular, treatment related selection pressure, pathological response, and increased heterogeneity can confound true biological associations.16 Therefore, to understand the real untreated biological state, it is imperative to evaluate the relationship between HER2 expression levels and the risk of axillary metastasis and other prognostic factors in HER2-positive patients who have not received neoadjuvant therapy and undergo primary surgical treatment.
Sentinel lymph node (SLN) biopsy (SLNB) is currently the standard approach for axillary metastasis staging; this approach allows for diagnosis without unnecessary axillary dissection.17 Additionally, sensitivity analyses using different cut-off values for hormone receptor positivity may contribute to a more accurate interpretation of HER2-low biology.18 Previous studies have explored the relationship between HER2 expression levels and nodal involvement in breast cancer; however, available data remain heterogeneous with respect to receptor subgroups, treatment setting, and the inclusion of patients receiving neoadjuvant therapy. In this context, we aimed to evaluate the surgical relevance of HER2 expression levels in a homogeneous cohort of hormone receptor–positive, treatment-naïve early-stage breast cancer patients undergoing upfront surgery.
In this study, we comprehensively investigated the relationship between HER2 expression levels (ultralow, low, and HER2-positive) and ALN metastasis, SLN positivity, clinicopathological characteristics, and survival out-comes in patients with early-stage, hormone receptor–positive breast cancer who did not receive neoadjuvant therapy and underwent upfront surgery. In addition, we evaluated the relationships between established prognostic factors, such as lymphovascular invasion (LVI), tumor size, and proliferative activity, and HER2 expression levels to identify independent predictors for axillary metastasis.
Materials and Methods
In this multicenter, observational, retrospective study, we included female patients (aged ≥18 years) who underwent upfront surgical treatment for histologically confirmed breast cancer between 2017 and 2023. Eligible patients had no evidence of distant metastasis at diagnosis (M0), had not received neoadjuvant systemic therapy, and were hormone receptor–positive, defined as estrogen receptor (ER) and/or progesterone receptor (PR) positivity.
Patients were stratified into three groups according to HER2 status determined by immunohistochemistry (IHC), with in situ hybridization testing performed when indicated according to contemporary ASCO/CAP criteria. HER2-positive tumors were defined as IHC 3+ or IHC 2+ with confirmed HER2 gene amplification. HER2-low tumors were defined as IHC 1+ or IHC 2+ without gene amplification. HER2-ultralow/zero tumors were classified as IHC 0. All patients underwent primary breast surgery with sentinel lymph node biopsy (SLNB) performed according to standard institutional protocols. Axillary lymph node dissection was carried out in patients who were clinically node-positive at presentation or in those with positive SLNs not meeting the ACOSOG Z0011 criteria.
HER2 immunohistochemical evaluation was performed by experienced breast pathologists at each participating institution according to contemporary ASCO/CAP guidelines. Because of the retrospective multicenter design, central pathological review was not performed. Nevertheless, standardized institutional pathology protocols and routine quality-control procedures were applied across participating centers. The potential interobserver variability associated with HER2-low assessment was acknowledged as a limitation during interpretation of the findings.
For all patients, data regarding demographic characteristics, tumor size, clinical and pathological charac-teristics, Ki-67 proliferation index, ER and PR expression percentages, type of surgical procedure, number and status of SLNs, outcomes of axillary surgery, recurrence, mortality, and survival data were recorded. Lymphovascular invasion (LVI) status was determined from the final pathology reports issued after surgical specimen evaluation and was recorded as a binary variable (present/absent). In the primary analyses, a cut-off value of ≥1% was used to define hormone receptor (ER or PR) positivity. In addition, to evaluate the impact of alternative threshold values frequently used in the literature, supplementary sensitivity analyses were performed using the ER ≥10% and PR ≥10% criteria.
The primary outcome of interest was the association between HER2 expression levels and SLN positivity. Secondary outcomes included ALN metastasis, overall survival (OS), disease-free survival (DFS), and the associations between HER2 expression levels and clinicopathological characteristics. For subgroup analyses, Ki-67 was dichotomized using a 20% threshold, as this cut-off is commonly used in clinical practice and prior breast cancer studies to distinguish low from high proliferative activity.
The study was approved by the Non-Interventional Clinical Research Ethics Committee of Mersin City Training and Research Hospital (Approval No: 2025/57, Date: 24 December 2025). Given the retrospective design, the requirement for informed consent was waived in accordance with institutional regulations. Patient confidentiality was strictly maintained throughout the study, and all data were anonymized prior to statistical analysis.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 29.0; IBM Corp., Armonk, NY, USA). The distribution of continuous variables was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests; accordingly, non-normally distributed continuous variables were presented as median and interquartile ranges. Categorical variables were expressed using frequency and percentage.
For between-group comparisons, continuous variables were analyzed using the Kruskal–Wallis test. When a statistically significant difference was observed, pairwise comparisons were performed using the Mann–Whitney U-test with Bonferroni correction. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate.
To identify independent predictors of SLN positivity, a multivariable logistic regression analysis was per-formed using clinically relevant variables and those with a p-value < 0.10 in univariable analyses. Given the relatively limited number of events, the multivariable model was constructed using clinically relevant variables and those with p < 0.10 in univariable analyses to avoid overfitting and maintain model stability. The results were reported as odds ratios (ORs) with 95% confidence intervals (CIs) and corresponding p-values. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test. Additionally, a receiver operating characteristic (ROC) analysis was performed to assess the discriminative ability of variables in predicting SLN positivity by calculating the area under the curve (AUC); 95% CIs were obtained using the bootstrap method.
OS and DFS were estimated using the Kaplan–Meier method, and between-group comparisons were per-formed using the Log rank test. Given the limited number of events and the relatively short follow-up duration, the survival analyses were considered exploratory. A two-sided p-value <0.05 was accepted as statistically significant for all analyses.
Results
During the study period, 1500 patients underwent surgery for breast cancer. The patient selection process, including inclusion and exclusion criteria, is summarized in Figure 1. Of these, 407 patients met the predefined inclusion criteria and were included in the final analysis; of these, 288 (70.8%) were classified as ultralow, 80 (19.7%) as low, and 39 (9.6%) as HER2-positive. This distribution reflects the fact that a substantial proportion of patients in the HER2-positive group received neoadjuvant therapy and were therefore not eligible for inclusion in the present analysis. The three groups demonstrated no statistically significant differences in terms of age distribution (median age [IQR]: 56 [48–65] years, 56.5 [47.8–65.2] years, and 55 [50–63.5] years for the ultralow, low, and HER2-positive groups, respectively; p = 0.816), menopausal status, tumor laterality, surgical approach, multifocality, or multicentricity (Table 1).
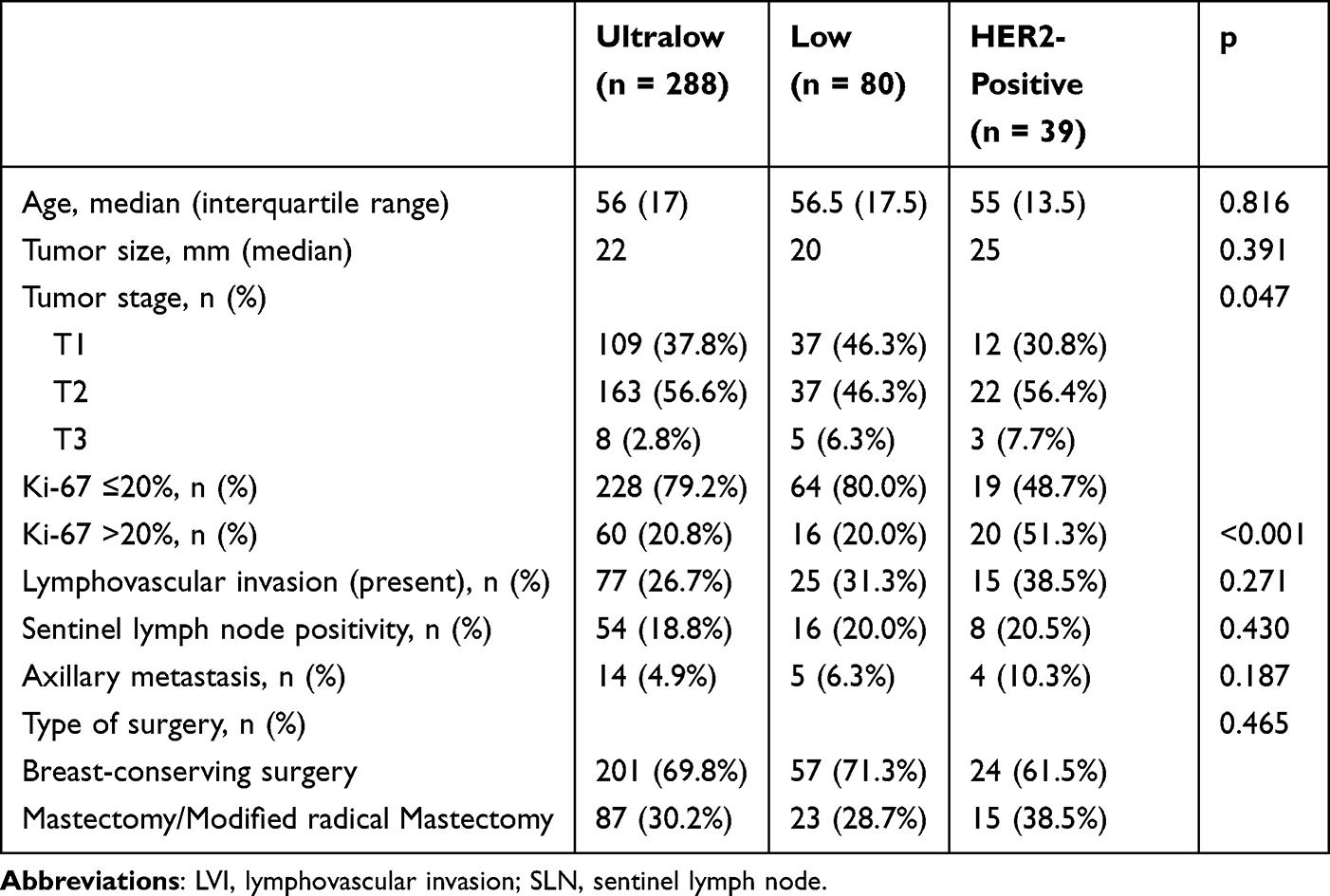 |
Table 1 Demographic and Clinicopathologic Characteristics of the Study Patients Stratified According to HER2 Status (N = 407) |
 |
Figure 1 Study flow chart showing patient selection, inclusion and exclusion criteria, and final study population. |
Primary tumor sizes were comparable across the ultralow, low, and HER2-positive groups (median: 22 mm, 20 mm, and 25 mm, respectively; p = 0.391). In contrast, significant between-group differences were identified regarding biological tumor parameters and clinicopathological characteristics. When the Ki-67 proliferation index was categorized as ≤20% and >20%, the proportion of tumors with Ki-67 >20% was significantly higher in the HER2-positive group (p < 0.001) (Table 1).
To assess the robustness of our hormone receptor–based inclusion criteria, we performed sensitivity analyses using alternative thresholds for hormone receptor positivity (ER ≥10% and PR ≥10%). The overall pattern of findings remained unchanged across HER2 groups. Specifically, the proportion of ER ≥10% positivity was 82.6% in the ultralow group, 70.0% in the low group, and 61.5% in the HER2-positive group (p = 0.002). Similarly, PR ≥10% positivity rates were 72.9%, 60.0%, and 46.2%, respectively (p < 0.001).
SLNB was performed in 89.2% of patients. When calculated among all included patients, SLN positivity rates were 18.8%, 20.0%, and 20.5% in the HER2-ultralow, HER2-low, and HER2-positive groups, respectively (Table 1). When the analysis was restricted to patients who underwent SLNB, the corresponding SLN positivity rates were 20.5%, 22.2%, and 25.0%, respectively, with no statistically significant difference between the groups (p = 0.941). Although the rate of ALN dissection was numerically higher in the HER2-positive group (30.8%) compared with the ultralow (22.6%) and low (20.0%) groups, this difference was not statistically significant. However, among the patients who underwent ALN dissection, the proportion of positive lymph nodes was comparable across the groups. ALN dissection was performed either in patients who were clinically node-positive at presentation or in those who underwent SLNB but did not meet the criteria of the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial. (ACOSOG Z0011). At no level of analysis was HER2 status significantly associated with SLN positivity.
In the multivariable logistic regression analysis, HER2 status was not identified as an independent predictor of SLN positivity (OR: low versus ultralow = 1.01; HER2-positive versus ultralow = 1.00). In contrast, LVI emerged as the strongest independent predictor for SLN node positivity (OR = 5.42; 95% CI: 3.13–9.39; p < 0.001) (Table 2). Findings from the ROC analysis were consistent with the multivariable logistic regression results. In the ROC analysis, LVI demonstrated the highest discriminative ability for predicting SLN positivity (AUC = 0.68; 95% CI: 0.62–0.73; p < 0.001).
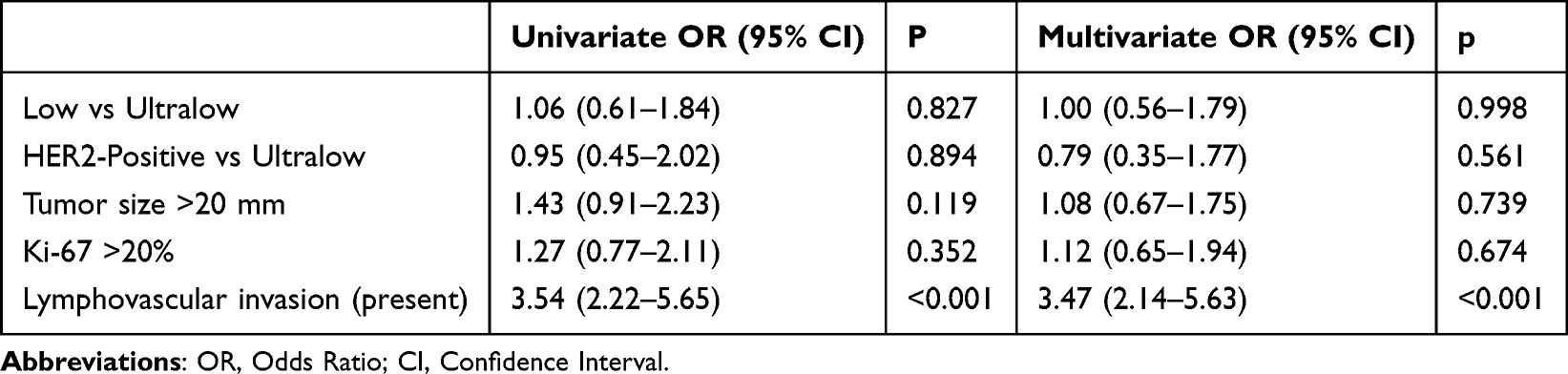 |
Table 2 Results of the Univariable and Multivariable Logistic Regression Analyses for Sentinel Lymph Node Positivity (Reference Category: Ultralow) |
While the Ki-67 proliferation index showed no significant discriminative value (AUC = 0.50), tumor size demonstrated moderate predictive performance (AUC = 0.61). No significant discriminative power was observed for ER and PR expression percentages or HER2 status (Figure 2).
 |
Figure 2 Receiver operating characteristic (ROC) curves for variables associated with sentinel lymph node positivity. The area under the curve (AUC) was 0.68 for lymphovascular invasion, 0.61 for tumor size, and 0.53 for Ki-67. These values are presented descriptively because the evaluated variables differ in their measurement characteristics. The red dashed diagonal line represents the line of no discrimination (AUC = 0.50). |
During a median follow-up period of 23 months, a total of three deaths and five recurrences were observed. Kaplan–Meier analyses did not identify statistically significant differences among the HER2 groups with respect to overall survival or disease-free survival. However, given the limited number of events observed during follow-up, these findings should not be interpreted as evidence of equivalent survival outcomes between HER2 expression categories. These negative findings are consistent with previous reports showing that HER2-low status does not confer a clear short-term survival disadvantage in early-stage hormone receptor–positive disease.19
In subgroup analyses stratified by proliferative activity, lymphovascular invasion (LVI), and tumor size, HER2 status was not significantly associated with SLN positivity, indicating that HER2 expression did not independently influence axillary metastatic risk. In contrast, LVI, proliferative activity, and tumor size were significantly associated with SLN positivity. Although SLN positivity rates increased markedly in the presence of LVI, this increase was observed across all HER2 expression subgroups, suggesting that LVI is a strong independent predictor of SLN metastasis irrespective of HER2 status.
Using a cut-off value of 20% for Ki-67, patients were categorized into low (≤ 20%) and high (> 20%) proliferative subgroups. In the high proliferative subgroup, the SLN positivity rates were 44.4% in the ultralow group, 23.1% in the low group, and 13.3% in the HER2-positive group. In the low proliferative subgroup, the SLN positivity rates were 24.9%, 32.2%, and 47.1% in the ultralow, low, and HER2-positive groups, respectively. While the SLN positivity rates were generally higher in the high proliferative subgroup, no statistically significant differences in SLN positivity were observed between the two proliferative subgroups in terms of HER2 status. These findings suggest that increased proliferative activity may contribute to a higher risk of axillary metastasis; however, this effect appears to be independent of HER2 status.
Subgroup analyses according to Ki-67 category, lymphovascular invasion (LVI) status, and tumor size are summarized in Table 3. Across all subgroup strata, HER2 status was not significantly associated with sentinel lymph node positivity. In contrast, SLN positivity rates were consistently higher in the presence of LVI and in tumors with larger size, supporting the dominant role of classical pathological risk factors. Among patients with LVI, SLN positivity rates were markedly higher across all HER2 groups compared with LVI-negative patients.
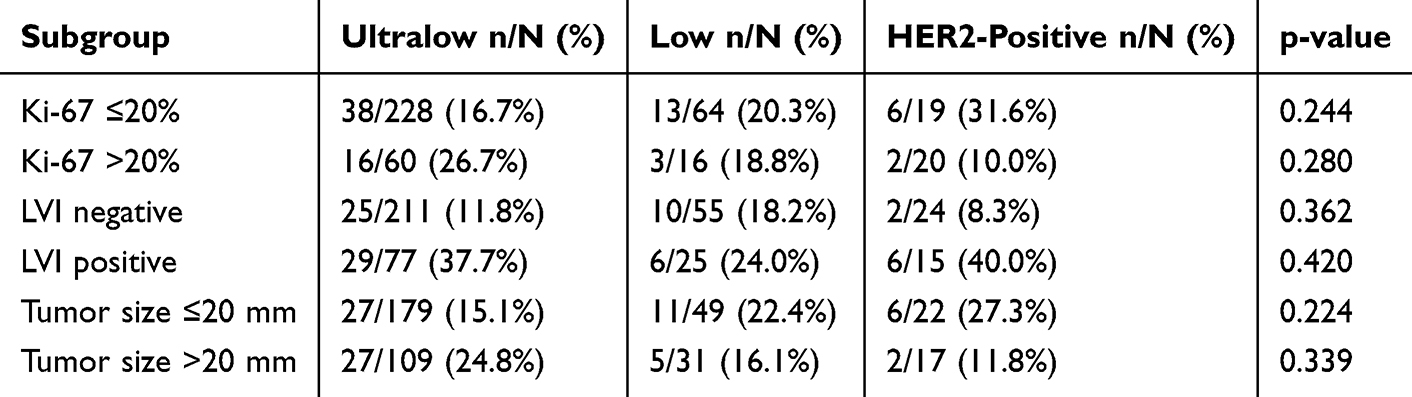 |
Table 3 Subgroup Analyses of SLN Positivity According to HER2 Status |
Tumor size was dichotomized using a cut-off value of 20 mm (≤ 20 mm versus >20 mm). Among patients with tumors > 20 mm, the SLN positivity rates were 38.2%, 29.0%, and 33.3% in the ultralow, low, and HER2-positive groups, respectively, whereas, among patients with tumors ≤ 20 mm, these rates were 19.5%, 31.7%, and 33.3% in the ultralow, low, and HER2-positive groups, respectively. In tumors >20 mm HER2 status was not significantly associated with SLN positivity (p = 0.196). Similarly, in tumors ≤20 mm, no significant association was observed (p = 0.219). However, SLN positivity rates were generally higher in patients with tumors > 20 mm. This finding indicates that tumor size plays a role in the risk of axillary metastasis, whereas HER2 status does not appear to modify this relationship. These findings further support that HER2 expression does not act as an effect modifier in the relationship between established pathological factors and SLN positivity.
Discussion
In this study, we comprehensively evaluated the impact of HER2 expression levels (ultralow, low, and HER2-positive) on axillary lymph node involvement, OS, and DFS in patients with hormone receptor–positive early-stage breast cancer who did not receive neoadjuvant therapy and underwent upfront surgery. The main finding of our study was that HER2 expression levels were not an independent predictor of SLN positivity at any level of analysis; in contrast, classical pathological factors, such as LVI, tumor size, and proliferative activity, maintained a strong and consistent association with axillary metastasis.
Although the concept of HER2-low breast cancer has gained significant attention in recent years, whether this subgroup truly represents a biologically and clinically distinct entity from HER2-zero or HER2-positive tumors remains controversial.20 A substantial proportion of conflicting data regarding the prognostic significance of HER2-low tumors originates from studies conducted in metastatic settings or with patients who have received neoadjuvant therapy.21, Considering the potential of neoadjuvant treatments to modify tumor biology, particularly ALN status, extrapolating these findings directly to early-stage, treatment-naïve populations may be challenging. By examining the association between HER2 expression levels and axillary metastasis in a cohort treated with upfront surgery, our study provides a distinct contribution to the existing literature by reflecting the untreated biological state.
The absence of a significant association between HER2 expression levels and SLN positivity in our cohort suggests that HER2-low tumors do not clinically differ from HER2-zero or HER2-positive tumors in terms of axillary dissemination potential. These findings do not support the hypothesis that HER2-low tumors are an intermediate biological phenotype in the context of axillary metastasis. Notably, in the multivariable logistic regression anal-ysis, neither the HER2-low nor the HER2-positive group demonstrated an additional risk for axillary metastasis compared with the ultralow group, indicating that this relationship lacks clinical relevance. This observation may partly be explained by the predominance of early-stage, clinically node-negative (cN0) tumors in our study cohort, which may have limited the variability in axillary metastatic burden.
Our findings support the interpretation that HER2-low disease may currently represent a therapeutically relevant classification rather than a biologically distinct axillary metastatic phenotype. Although HER2-low tumors may demonstrate differential sensitivity to antibody–drug conjugates, this therapeutic responsiveness does not necessarily imply distinct invasive or lymphatic dissemination behavior. Therefore, the clinical implications of the HER2-low concept in early-stage breast cancer may be more closely related to systemic treatment selection than to surgical decision-making or nodal metastatic biology. Our findings should also be considered in light of prior studies examining HER2 expression and nodal involvement. Shi et al evaluated treatment-naïve breast cancer patients according to HER2 expression levels and reported no consistent evidence that HER2-low status was associated with increased nodal metastatic burden compared with other HER2-defined subgroups.22 Likewise, Lu et al compared lymph node metastasis rates across HER2 expression categories and found no clear indication that HER2-low disease represents a distinct nodal metastatic phenotype. In contrast to these studies, our analysis was specifically restricted to a homogeneous cohort of hormone receptor–positive early-stage patients undergoing upfront surgery without neoadjuvant treatment, thereby offering a more focused surgical perspective on sentinel lymph node positivity.23
Conversely, LVI emerged as the strongest independent predictor of SLN positivity in the multivariable analysis. Importantly, this should not be interpreted as a novel observation, as LVI is already a well-established predictor of nodal involvement and adverse prognosis in invasive breast cancer. Rather, our results confirm its dominant role within this specific cohort of hormone receptor–positive, treatment-naïve patients undergoing upfront surgery.24 The observed AUC values (0.68 for LVI, 0.61 for tumor size, and 0.53 for Ki-67) indicated only modest discriminatory performance and should be interpreted descriptively, given the binary nature of LVI and the different measurement characteristics of the evaluated variables. Findings from the ROC analysis were consistent with those of the multivariable model, with LVI demonstrating the highest discriminative ability among the evaluated variables. However, the discriminatory performance of these variables was modest (AUC=0.68 for LVI, AUC=0.61 for tumor size, and AUC=0.53 for Ki-67) and does not support their use as clinically actionable predictive tools. Rather, these findings should be interpreted as supportive evidence reinforcing the predominant role of established pathological factors in axillary metastatic risk assessment.
The subgroup analyses further reinforced that even within clinically and pathologically relevant subgroups (defined by proliferative activity, LVI, and tumor size), HER2 expression levels did not exert a significant modifying effect on SLN positivity. Although subgroup analyses suggested potential variation across HER2 strata for both Ki-67 and lymphovascular invasion (LVI), formal interaction analyses were not performed due to the limited sample size and number of events, which may lead to unstable estimates. Therefore, these findings should be interpreted with caution. Although higher SLN positivity rates were generally observed in tumors with high proliferative activity, defined as Ki-67 >15% in the referenced study and >20% in our cohort, suggesting a potential role of proliferation in axillary metastatic risk, this effect was independent of HER2 expression status.25 Similarly, an increase in SLN positivity rates was observed with increasing tumor size; however, HER2 expression did not significantly affect this association, highlighting the dominant role of classical prognostic factors in axillary metastasis biology.26
The higher prevalence of HER2-low tumors among patients with hormone receptor–positive breast cancers further complicates the interpretation of their biological characteristics. This is because of the variability in the cut-off values used to define hormone receptor positivity in the literature, which represents a significant factor limiting comparability across studies involving HER2-low tumors.27 In our study, the consistency of findings in sensitivity analyses performed using both ≥1% and ≥10% thresholds for ER and PR positivity demonstrates that the lack of association between HER2 expression levels and axillary metastasis is independent of the receptor cut-off applied. This methodological robustness strengthens the validity of our findings.
The survival analyses conducted in our study did not demonstrate statistically significant differences in OS or DFS according to HER2 expression levels. However, only three deaths and five recurrences occurred during follow-up, and the median follow-up duration was relatively short. Therefore, the absence of statistically significant differences should not be interpreted as evidence of equivalent prognosis among HER2 expression groups. Rather, these analyses should be considered exploratory and hypothesis-generating, and larger studies with longer follow-up are needed to better define potential prognostic differences.
Although these results should be interpreted cautiously due to the limited number of events and relatively short follow-up, they are in line with previous reports suggesting that HER2-low status does not consistently confer distinct short-term survival outcomes in early-stage hormone receptor–positive breast cancer.28 Given the limited number of survival events and relatively short median follow-up duration, the present survival analyses should be considered exploratory and hypothesis-generating rather than definitive.
Several limitations of this study should be acknowledged. The retrospective design may have introduced potential selection biases. Furthermore, because HER2 assessment was performed across multiple institutions without central pathological review, some degree of interobserver variability in distinguishing HER2-ultralow and HER2-low categories cannot be excluded. A further limitation concerns the terminology used for HER2 expression categories. In this study, tumors with an IHC score of 0 were referred to as HER2-ultralow to maintain consistency throughout the manuscript. However, recent studies have suggested that HER2-ultralow tumors, defined by faint incomplete membranous staining in ≤10% of tumor cells, may represent a subgroup distinct from true HER2-zero disease. Because this was a retrospective multicenter study and no central pathological review was performed, such a distinction could not be reliably assessed. Therefore, our classification of IHC 0 tumors as HER2-ultralow should be interpreted in this context. The limited number of events restricted the statistical power of the survival analyses. In addition, the relatively small number of patients in the HER2-positive subgroup may have limited the statistical power of subgroup comparisons and increased the risk of type II error. Nonetheless, the inclusion of a homogeneous cohort of hormone receptor–positive treatment-naïve sample who underwent upfront surgery, standardized pathological assessment, and the use of multivariable analyses to support the findings represent important strengths of the study. The main contribution of the present study lies not in proposing HER2-low disease as a new determinant of nodal spread, but in testing this question within a narrowly defined and clinically relevant surgical cohort. By restricting the analysis to hormone receptor–positive, treatment-naïve early-stage patients treated with upfront surgery, we aimed to minimize confounding related to neoadjuvant treatment effects and receptor heterogeneity across broader breast cancer populations.
Overall, our findings indicate that HER2 expression levels are not independent determinants of axillary metastasis or SLN positivity in hormone receptor–positive early and locally advanced breast cancer patients who have not yet received neoadjuvant therapy. In assessing the risk of axillary metastasis, classical pathological factors, including LVI, tumor size, and proliferative activity, should remain the primary considerations. These results suggest that the clinical impact of the HER2-low concept on axillary biology and surgical decision-making is limited, and that management of axillary metastasis in early-stage breast cancer should be guided by biologically meaningful parameters. (Lymphovascular invasion, tumor size, histological grade, and Ki-67 proliferative index).
More importantly, the lack of a statistically significant relationship between HER2 expression and axillary metastasis risk suggests that HER2-low tumors do not exhibit an invasive or lymphatic dissemination pattern that is characteristic of HER2-positive tumors. Nevertheless, the clinical relevance of the HER2-low concept extends beyond prognostic and surgical contexts. In cases demonstrating borderline or heterogeneous HER2 expression on IHC evaluation, current testing methods may not fully capture tumor biology.29 In this regard, it is conceivable that some tumors classified as HER2-low or ultralow may harbor functionally relevant HER2 proteins on the cell surface, representing a potential area for future research on targeted therapeutic strategies. However, this hypothesis requires validation through prospective and biologically driven studies in treatment-naïve patients with early stage breast cancer.
Conclusions
In this retrospective multicenter cohort of hormone receptor–positive treatment-naïve early breast cancer patients undergoing upfront surgery, HER2 expression status was not independently associated with axillary metastasis or sentinel lymph node positivity. In contrast, the risk of axillary metastasis appears to be primarily determined by classical pathological factors, particularly LVI, larger tumor size, and higher proliferative activity, rather than by HER2 expression status. These findings suggest that the HER2-low concept has limited influence on axillary metastatic behavior and should not substantially impact surgical decision-making in early-stage breast cancer. However, given the retrospective design and limited number of events, these observations should be interpreted cautiously. Importantly, the present study primarily addresses surgical and nodal metastatic behavior and was not designed to evaluate the broader biological or therapeutic implications of HER2-low disease.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Mersin City Hospital (protocol code 2025/57).
Abbreviations
ALN, axillary lymph node; AUC, area under the curve; CI, confidence interval; DFS, disease-free survival; ER, estrogen receptor; FISH, fluorescence in situ hybridization; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; IQR, interquartile range; ISH, in situ hybridization; LVI, lymphovascular invasion; M0, no distant metastasis; OR, odds ratio; OS, overall survival; PR, progesterone receptor; ROC, receiver operating characteristic; SLN, sentinel lymph node; SLNB, sentinel lymph node biopsy.
Data Sharing Statement
The data in this study were obtained from Mersin City Hospital database where restrictions may apply as information could compromise the privacy of research participants. Datasets may be requested from the corresponding author (M.F.S).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study in accordance with institutional regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Giaquinto AN, Sung H, Newman LA, et al. Breast cancer statistics 2024. Ca a Cancer J Clinicians. 2024;74(6):477–11. doi:10.3322/caac.21863
2. Kim J, Harper A, McCormack V, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nature Med. 2025;31(4):1154–1162. doi:10.1038/s41591-025-03502-3
3. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
4. Zhang Y, Ji Y, Liu S, et al. Global burden of female breast cancer: new estimates in 2022, temporal trend and future projections up to 2050 based on the latest release from GLOBOCAN. Journal of the National Cancer Center. 2025;5(3):287–296. doi:10.1016/j.jncc.2025.02.002
5. Schonberg MA, Wolfson EA, Eliassen AH, et al. Population attributable risk of a competing-risk model for breast cancer and non-breast cancer death among women≥ 65 years. Breast Cancer Res Treat. 2025;211(3):687–698. doi:10.1007/s10549-025-07683-w
6. Shaaban AM, Kaur T, Provenzano E. HER2-low breast cancer—current knowledge and future directions. Medicina. 2025;61(4):644. doi:10.3390/medicina61040644
7. Ju J, Du F, Gao S-L, et al. Combined analysis of receptor expression reflects inter-and intra-tumor heterogeneity in HR+/HER2+ breast cancer. Breast Cancer Res Treat. 2022;194(2):221–230. doi:10.1007/s10549-022-06629-w
8. El Haddad G, Diab E, Hajjar M, et al. Insights into the emerging entity of HER2-low breast cancer. Int J Breast Cancer. 2024;2024(1):2853007. doi:10.1155/2024/2853007
9. Popović M, Silovski T, Križić M, Dedić Plavetić N. HER2 low breast cancer: a new subtype or a trojan for cytotoxic drug delivery? Int J Mol Sci. 2023;24(9):8206. doi:10.3390/ijms24098206
10. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
11. Modi S. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer: a plain language summary of the DESTINY-breast04 study. Future Oncol. 2025;21(4):367–380. doi:10.1080/14796694.2024.2434388
12. Tarantino P, Viale G, Press M, et al. ESMO expert consensus statements (ECS) on the definition, diagnosis, and management of HER2-low breast cancer. Ann Oncol. 2023;34(8):645–659. doi:10.1016/j.annonc.2023.05.008
13. Schettini F, Blondeaux E, Molinelli C, et al. Characterization of HER2-low breast cancer in young women with germline BRCA1/2 pathogenetic variants: results of a large international retrospective cohort study. Cancer. 2024;130(16):2746–2762. doi:10.1002/cncr.35323
14. Schmidt M, Lehr H-A, Almstedt K. HER2-low and HER2-zero in breast cancer between prognosis, prediction and entity. Oncotarget. 2024;15:418. doi:10.18632/oncotarget.28598
15. Shekari F, Bayat Mokhtari R, Salahandish R, et al. HER2-low breast cancer at the interface of pathology and technology: toward precision management. Biomedicines. 2025;14(1):49. doi:10.3390/biomedicines14010049
16. Kang S, Kim S-B. HER2-low breast cancer: now and in the future. Cancer Res Treat. 2024;56(3):700–720. doi:10.4143/crt.2023.1138
17. Veronesi U, Paganelli G, Viale G, et al. Sentinel-lymph-node biopsy as a staging procedure in breast cancer: update of a randomised controlled study. Lancet Oncol. 2006;7(12):983–990. doi:10.1016/S1470-2045(06)70947-0
18. Allison KH, Hammond MEH, Dowsett M, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J clin oncol. 2020;38(12):1346–1366. doi:10.1200/JCO.19.02309
19. Zeng Y, Qian P, Li G, Sun Y. Differences in survival outcomes between HER2-low and HER2-zero breast cancer across heterogeneous HR expression patterns: a real-world study. World J Surg Oncol. 2025;23(1):331. doi:10.1186/s12957-025-03962-4
20. Tarantino P, Hamilton E, Tolaney SM, et al. HER2-low breast cancer: pathological and clinical landscape. J clin oncol. 2020;38(17):1951–1962. doi:10.1200/JCO.19.02488
21. Agostinetto E, Rediti M, Fimereli D, et al. HER2-low breast cancer: molecular characteristics and prognosis. Cancers. 2021;13(11):2824. doi:10.3390/cancers13112824
22. Shi J, Zhang L, Geng C. HER-2 ultra-low breast cancer: exploring the clinicopathological features and prognosis in a retrospective study. Front Oncol. 2023;13:1210314. doi:10.3389/fonc.2023.1210314
23. Lu Y, Tong Y, Fei X, Chen X, Shen K. Clinical characteristics, tumor-infiltrating lymphocytes, and prognosis in HER2-low breast cancer: a comparison study with HER2-zero and HER2-positive disease. Cancer Med. 2023;12(15):16264–16278. doi:10.1002/cam4.6290
24. Rakha EA, Martin S, Lee AH, et al. The prognostic significance of lymphovascular invasion in invasive breast carcinoma. Cancer. 2012;118(15):3670–3680. doi:10.1002/cncr.26711
25. Inwald E, Klinkhammer-Schalke M, Hofstädter F, et al. Ki-67 is a prognostic parameter in breast cancer patients: results of a large population-based cohort of a cancer registry. Breast Cancer Res Treat. 2013;139(2):539–552. doi:10.1007/s10549-013-2560-8
26. Sopik V, Narod SA. The relationship between tumour size, nodal status and distant metastases: on the origins of breast cancer. Breast Cancer Res Treat. 2018;170(3):647–656. doi:10.1007/s10549-018-4796-9
27. Fei F, Siegal GP, Wei S. Characterization of estrogen receptor-low-positive breast cancer. Breast Cancer Res Treat. 2021;188(1):225–235. doi:10.1007/s10549-021-06148-0
28. Chen E, Chen C, Chen Y, et al. Investigating HER2-low in early breast cancer: prognostic implications and age-related prognostic stratification. Cancer Med. 2025;14(4):e70637. doi:10.1002/cam4.70637
29. Wolff AC, Hammond MEH, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of American pathologists clinical practice guideline focused update. Arch Pathol Lab Med. 2018;142(11):1364–1382. doi:10.5858/arpa.2018-0902-SA
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Predicting Positive Sentinel Lymph Node Biopsy in Clinically Node-Negative Breast Cancer
Alsumai TS, Alhazzaa N, Alshamrani A, Assiri S, Alhefdhi A
Breast Cancer: Targets and Therapy 2022, 14:323-334
Published Date: 11 October 2022