Back to Journals » Lung Cancer: Targets and Therapy » Volume 17
HER2-ADC and HER2-TKI Overcomes HER2 Amplification as an Acquired Resistance to Zongertinib – A Case Report
Authors Nagasaka M ![]() , Arter ZL
, Arter ZL ![]() , Park CJ
, Park CJ ![]() , Sarkari A, Ou SI
, Sarkari A, Ou SI
Received 9 February 2026
Accepted for publication 5 May 2026
Published 14 May 2026 Volume 2026:17 600499
DOI https://doi.org/10.2147/LCTT.S600499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fengying Wu
Misako Nagasaka,1,2 Zhaohui L Arter,1 Cathleen J Park,1 Akshat Sarkari,1 Sai-Hong Ignatius Ou1
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Department of Medicine, St Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, University of California Irvine School of Medicine, 101 The City Drive, Orange, CA, 92868, USA, Email [email protected]
Abstract: Trastuzumab deruxtecan, zongertinib and sevabertinib have been approved in the United States for the treatment of patients with advanced metastatic HER2 mutated non–small-cell lung cancer (NSCLC). Unfortunately, tumor progression is inevitable in many cases. In this case report, we share our experience with a patient with HER2 mutated NSCLC who responded to the combination of trastuzumab deruxtecan and zongertinib after progressing on each agent when given alone, highlighting the potential for such combinations.
Keywords: trastuzumab deruxtecan, T-Dxd, combination therapy, HER2 mutation, mechanism of resistance
Introduction
Targeted therapy is the standard of care treatment for advanced metastatic NSCLC when driver alterations exist. Specifically, for HER2 mutated NSCLC, trastuzumab deruxtecan (T-Dxd) was the first agent to be approved.1 Since then, zongertinib2 and sevabertinib3 have both been approved in HER2 mutated NSCLC. Unfortunately, tumor progression is inevitable in many cases. In this case report, we share our experience of a case of a patient with HER2 mutated NSCLC who responded to the combination of trastuzumab deruxtecan and zongertinib after progressing on each agent when given alone, highlighting the potential for such combinations.
Institutional approval for publication of case details was waived for this manuscript. The patient presented in this case report gave their informed consent authorizing publication of the case details and images.
Case Report
A 66-year-old man with no history of smoking presented to primary care for unintentional weight loss and was found to have multiple liver and spinal vertebrae lesions. He required decompression surgery for the C5 pathological fracture, and the final pathology report showed adenocarcinoma favoring a primary lung origin. Computed tomography (CT) chest also confirmed a 1.7 cm right lower lobe (RLL) mass. HER2 mutation (ERBB2 A775 G776insYVMA %CFDNA 1.7%) and TP53 I162N %CFDNA 1.2% were found on liquid (Table 1) and tissue next-generation sequencing (NGS), and he was started on cisplatin pemetrexed and pembrolizumab. Liquid NGS was performed through Guardant360®4 and tissue based NGS was performed through FoundationOne®CDx.5 Initial positron emission tomography (PET) scans after 4 cycles showed a response in the lung, liver and bone lesions. However, he experienced progression in the bone and liver 4 months into maintenance pemetrexed and pembrolizumab. For second line therapy, he was given trastuzumab deruxtecan with initial stability of disease. After 8 months, his cancer eventually progressed in his lung, liver and bones.
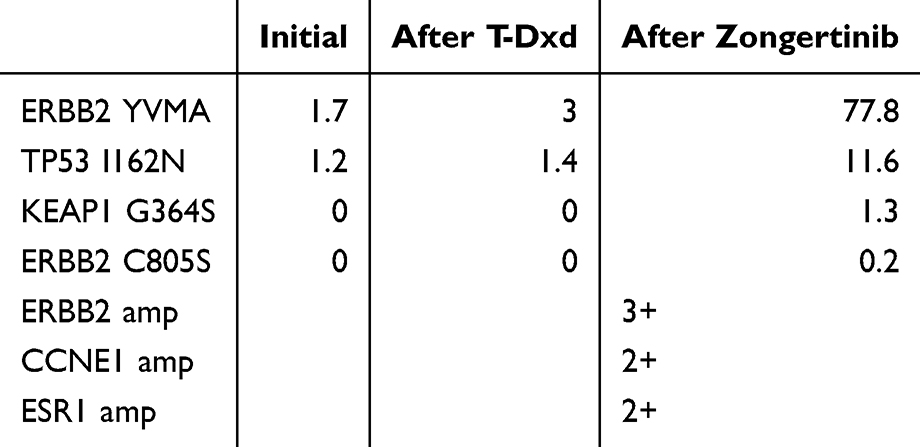 |
Table 1 % CFDNA on Liquid Biopsy at Different Time Points |
For third line therapy, he started zongertinib as part of a clinical trial (8/2024). While an initial response was seen in his RLL lung and liver lesions, he eventually progressed in the liver after 10 months (Figure 1). At this time, liquid NGS showed ERBB2 A775 G776insYVMA %CFDNA 77.8%, ERBB2 amp high (3+), TP53 I162N %CFDNA 11.6%, KEAP1 G364S %CFDNA 1.3%, CCNE1 amp medium (2+), ESR1 amp medium (2+) and ERBB2 C805S %CFDNA 0.2% (Table 1). He was switched back to trastuzumab deruxtecan (6/2025) with the addition of afatinib 30 mg for 1.5 months, followed by a switch from afatinib to zongertinib with its accelerated approval (8/2025). CT scans (10/2025), 2 months post trastuzumab deruxtecan and zongertinib, showed response in the liver lesions (Figure 1).
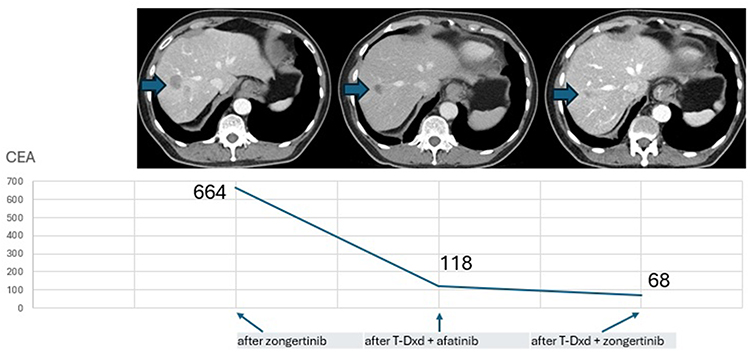 |
Figure 1 Liver lesions post zongertinib (left), post trastuzumab deruxtecan and afatinib (center) and post trastuzumab deruxtecan and zongertinib (right). |
Discussion
To the best of our knowledge, this is the first report of a patient with HER2 mutated NSCLC who progressed on trastuzumab deruxtecan as well as zongertinib when they were given as single agents, and who subsequently responded to the therapy when both were given together. The patient had liquid biopsy done at three different time points (Table 1). The significant increase in %CFDNA of ERBB2 YVMA from 3 after trastuzumab deruxtecan to 77.8 after zongertinib which was accompanied by ERBB2 amplification at 3+ is likely at least partially, a mechanism of resistance to zongertinib as a single agent. As the patient had responded previously to trastuzumab deruxtecan, the combination of trastuzumab deruxtecan with (initially afatinib followed by quick switch to) zongertinib (once it became available) was implemented and we were able to obtain another response to therapy.
Afatinib was selected as a “bridge” therapy awaiting approval of zongertinib given its activity against HER2 mutated NSCLC.6 While it is possible that afatinib also contributed to the patient’s response to therapy, the lack of selectivity against HER2 mutations over wild type EGFR makes it challenging to continue therapy. Indeed, the patient did suffer from grade 2 diarrhea from afatinib which resolved when switched to zongertinib.
Recently, Nilsson et al reported that loss of payload sensitivity and other mechanisms of resistance such as secondary HER2 extracellular mutations in domain IV, the trastuzumab binding site, could cause resistance to trastuzumab deruxtecan.7 Interestingly, HER2 tyrosine kinase inhibitors (TKIs) maintained sensitivity even in tumor cells with acquired payload resistance of domain IV mutations, implicating HER2 TKI as a salvage for post trastuzumab deruxtecan progression.7
This sequence was also seen in our patient, who had disease control with zongertinib alone for 10 months post progression on trastuzumab deruxtecan. However, just like in our patient case, the tumor tends to ultimately progress, thus, the need for further strategies to overcome such situations.
Interestingly, the successful switch to trastuzumab deruxtecan from zongertinib in a patient with HER2 mutated NSCLC who developed HER2 amplification has been previously reported8 and may be related to the TKI increasing the internalization of the antibody drug conjugate,9 but in our case, the patient’s tumor progressed on both drugs when given as a single agent and responded when given in combination, which may be related to synergy between the bystander effect of trastuzumab deruxtecan and signaling pathway inhibition from the TKI.9,10 It is also important to note that the doublet of trastuzumab deruxtecan and zongertinib was well tolerated in our patient. The fact that there are little overlapping toxicities and with the interstitial lung disease rates being exceedingly low with zongertinib also supports the combination strategy.
This case highlights the potential of this combination being able to overcome the resistance mechanism of each agent and complement each other. Further prospective studies are warranted incorporating multi-omic integration11 to explore further the efficacy and safety of combination therapy of trastuzumab deruxtecan and zongertinib.
Conclusion
We experienced a case of a patient with HER2 mutated NSCLC who responded to the combination of trastuzumab deruxtecan and zongertinib after progressing on each agent when given alone. This case highlights the potential for combination therapy to overcome resistance, and we believe that further prospective studies are warranted to document the efficacy and safety of this combination.
Acknowledgment
Institutional approval was waived for this manuscript. The patient presented in this case report gave their informed consent authorizing use and disclosure of de-identified health information.
Disclosure
M.N. is on the advisory board for AstraZeneca, Daiichi Sankyo, Takeda, Johnson and Johnson, Eli Lilly and Company, Bayer, Regeneron, BMS, Boehringer Ingelheim and Genentech; consultant for Caris Life Sciences (virtual tumor board); speaker for Johnson and Johnson, Pfizer, Mirati/BMS and Takeda; reports travel support from AnHeart/Nuvation Bio Therapeutics and has stock/stock options in MBrace Therapeutics. Z.A. has received honoraria from Johnson and Johnson, Catalyst, Boehringer Ingelheim, EMD Serono, Taiho, and Rigel. C.P. has received honoraria from Johnson and Johnson, BioImmunity and MJH LifeSciences. S.I.O. reports honorarium from Abbvie, AnHeart Therapeutics, BMS, Pfizer, Bayer, Daiichi Sankyo, Avistone Biotechnology, Fortvital and having stock/stock options in MBrace Therapeutics, BlossomHill Therapeutics, Lilly, Nuvalent, and Nuvation Bio. The authors report no other conflicts of interest in this work.
References
1. Li BT, Smit EF, Goto Y. et al. Trastuzumab Deruxtecan in HER2-Mutant Non-Small-Cell Lung Cancer. N Engl J Med. 2022;386(3):241–4. doi:10.1056/NEJMoa2112431. PMID: 34534430.
2. Heymach JV, Ruiter G, Ahn MJ, et al. Zongertinib in Previously Treated HER2-Mutant Non-Small-Cell Lung Cancer. N Engl J Med. 2025;392(23):2321–2333. doi:10.1056/NEJMoa2503704. PMID: 40293180.
3. Le X, Kim TM, Loong HH, et al. Sevabertinib in Advanced HER2-Mutant Non-Small-Cell Lung Cancer. N Engl J Med. 2025;393(18):1819–1832. doi:10.1056/NEJMoa2511065. PMID: 41104928.
4. Guardant Health. Guardant360® Liquid Assay Specification Sheet. Redwood City (CA): Guardant Health; 2025. Available from: https://www.guardantcomplete.com/assets/pdf/Guardant360-Liquid-Specification-Sheet.pdf.
5. Foundation Medicine. CDx Label. Boston (MA): Foundation Medicine; 2025. Available from: http://www.f1cdxlabel.com/.
6. Dziadziuskzo R, Smit EF, Dafni U, et al. Afatinib in NSCLC with HER2 Mutations: results of the Prospective, Open-Label Phase II NICHE Trial of European Thoracic Oncology Platform (ETOP). J Thorac Oncol. 2019;14(6):1086–1094. doi:10.1016/j.jtho.2019.02.017. PMID: 30825613
7. Nilsson MB, Le X, Poteete A, et al. Loss of payload sensitivity and other mechanisms of resistance to T-DXd in HER2-mutant NSCLC: implications for subsequent responsiveness to HER2 TKIs. J Thorac Oncol. 2026;16:S1556. doi:10.1016/j.jtho.2026.01.007. PMID: 41548807
8. McMahon DJ, John A, Kalofonou F, et al. Acquired ERBB2 amplification and overexpression as on-target resistance mechanisms to zongertinib with subsequent response to trastuzumab deruxtecan; a case report. JTO Clin Res Rep. 2026;2026:100960. doi:10.1016/j.jtocrr.2026.100960
9. Liu J, Zhu T, Zhao R, Ren W, Zhao F, Liu J. Elucidating molecular mechanisms and therapeutic synergy: irreversible HER2-TKI plus T-Dxd for enhanced anti-HER2 treatment of gastric cancer. Gastric Cancer. 2024;27(3):495–505. doi:10.1007/s10120-024-01478-6. PMID: 38386239
10. Wang Y, Cheng X, Li X, Chen W, Zhang X, Liu Y. Bystander effect in anitobody-drug conjugates: navigating the fine line in tumor heterogeneity. Crit Rev Oncol Hematol. 2025;216:104979. doi:10.1016/j.critrevonc.2025.104979. PMID: 41061840
11. Mersich I, Blagg BSJ, Ali A. Multi-omic integration identifies broad drug resistance mechanisms and strategies to therapeutically reprogram cancer cells. iScience. 2025;29(1):114293. doi:10.1016/j.isci.2025.114293. PMID: 41492468
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Advances in Immunotherapy for HER2 Low-Expressing Triple-Negative Breast Cancer
Zhang X, Yang D, Lin X, Hu X, Li J, Deng S, Chen Q, Chen X
Cancer Management and Research 2025, 17:2985-2995
Published Date: 1 December 2025