Back to Journals » International Journal of Women's Health » Volume 18
Hemoglobin Trajectory During Pregnancy and Postpartum Hemorrhage: A Retrospective Cohort Study
Authors Mu G ![]() , Li H, Du J, Jian Y, Shen X
, Li H, Du J, Jian Y, Shen X ![]() , Su Y
, Su Y
Received 7 February 2026
Accepted for publication 11 April 2026
Published 21 April 2026 Volume 2026:18 601942
DOI https://doi.org/10.2147/IJWH.S601942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Ge Mu,1 Hong Li,2 Jiang Du,2 Yingying Jian,2 Xin Shen,3,* Yani Su1,*
1Big Data Center, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, 710068, People’s Republic of China; 2Obstetrics Department, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, 710068, People’s Republic of China; 3Medical Record Center, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, 710068, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Shen, Medical Record Center, Shaanxi Provincial People’s Hospital, No. 256 Youyixi Road, Xi’an, Shaanxi, 710068, People’s Republic of China, Email [email protected]
Background: Studies on the association between anemia and postpartum hemorrhage (PPH) mostly use the hemoglobin (Hb) levels in a single trimester, thereby failing to capture the dynamic changes of Hb levels during pregnancy. This study aims to assess the trajectories of Hb during pregnancy and evaluate their association with PPH.
Methods: The study population consisted of 4296 women who gave birth in a tertiary hospital after 28 weeks of gestation between January 2024 and February 2025. Group-based trajectory modelling was used to identify hemoglobin trajectories. Logistic regression models were applied for evaluating the associations between hemoglobin trajectories and PPH.
Results: Three trajectories of maternal Hb were identified. In trajectory 1 (decline-stable, 20.41%), maternal Hb levels were higher than those in trajectory 2 in the first trimester, and rapidly declined across pregnancy with the lowest point at 35 weeks. In trajectory 2 (decline-rise, 73.16%), maternal Hb decreased during the first and second trimesters, and slightly increased during the third trimester. In trajectory 3 (stable-rise, 6.42%), maternal Hb remained stable in early and mid-pregnancy and increased in late pregnancy. Compared with trajectory 2, trajectory 1 was associated with a 2.36-fold higher risk of PPH (95% CI: 1.59– 3.47), while trajectory 3 showed no significant association (OR: 0.79, 95% CI: 0.27– 1.81), after adjustment. The area under the receiver operating characteristic curve was 0.74 (95% CI: 0.70– 0.79). Compared with women with Hb ≥ 116 g/L at 28– 32 weeks, women with Hb < 116 g/L had a 1.64-fold higher risk of PPH (95% CI: 1.08– 2.52).
Conclusion: Women who are not anemic in early pregnancy but experience a rapid decline in Hb during pregnancy, especially those with Hb < 116 g/L in the early third trimester, are at high risk for PPH.
Plain Language Summary: Based on the trajectory of hemoglobin levels during pregnancy, we divided the population into three groups. A total of 73.16% of women had a pattern where their hemoglobin (Hb) levels decreased during the first and second trimesters and then increased during the third trimester (trajectory 2). And 20.41% of women followed a pattern where Hb decreased more rapidly in the first and second trimester and remained lower in the third trimester (trajectory 1). Another 6.42% of women had a lower Hb in early and mid-pregnancy and an increased Hb in late pregnancy (trajectory 3). Women in trajectory 1 were 2.36 times more likely to experience postpartum hemorrhage than those in trajectory 2. Even if a woman is not anemic early in pregnancy, a rapid drop in hemoglobin later, especially Hb below 116 g/L in the early third trimester, may be a warning sign that deserves closer attention.
Keywords: hemoglobin, postpartum hemorrhage, pregnancy, trajectory, group-based trajectory modelling
Introduction
Postpartum hemorrhage (PPH) is a life-threatening obstetric complication. Although many countries have been improving maternal health care in recent years, the incidence of PPH remains relatively high.1–4 And PPH has become the leading cause of maternal deaths. Globally, up to 26.7% of maternal deaths can be attributed to obstetric hemorrhage and 14.8% can be attributed to PPH.5 In China, obstetric hemorrhage accounted for 17.8% of maternal deaths in 2023.6 Therefore, preventing PPH is critically important. The current challenge lies in the difficulty of predicting and identifying PPH, as existing risk assessment tools are often complex, costly, or require highly skilled personnel.7
Anemia is a well-established risk factor for PPH. Women with prepartum anemia have a 1.69- to 3.66-fold higher risk for PPH8–10 and a 1.45- to15.65-fold higher risk for severe PPH.11,12 Hemoglobin (Hb) is the primary indicator of anemia. According to the WHO guideline, anemia was defined as Hb<110 g/L during the first or third trimester, and Hb<105 g/L during the second trimester.13 While the Hb cutoff used in published literature varies, leading to the inconsistent findings that anemia defined with a lower cutoff is often associated with a higher risk of PPH.14 In addition to anemia, high maternal Hb is also associated with adverse health outcomes, although data on the association between high Hb and PPH are still insufficient.15 Given the inconsistency in Hb cutoffs for PPH risk assessment, exploring the direct use of hemoglobin as a predictive biomarker is necessary.
Hemoglobin concentration constantly changes during pregnancy. During pregnancy, Hb concentrations decrease due to physiological hemodilution.16 Therefore, the timing of maternal Hb measurement is crucial, and identifying dynamic changes in Hb is beneficial for assessing potential health risks. However, current evidence is limited to the trimester-specific association between Hb and PPH, with most studies focusing on the pre-delivery Hb.12,17,18 The longitudinal trajectory of hemoglobin data measured serially during routine prenatal checkups has yet to be explored. Therefore, the present study evaluates the trajectories of Hb during pregnancy and their associations with PPH, to facilitate earlier identification of high-risk group.
Methods
Study Population and Data Collection
This retrospective cohort study included 5975 pregnant women who gave birth in a tertiary hospital in Shaanxi, China after 28 weeks of gestation between January 2024 and February 2025. Among them, 4296 pregnant women underwent more than 3 hemoglobin tests at this hospital from 12 weeks before pregnancy to the period before delivery and were included in the final analyses.
Basic characteristics including age, height, weight, obstetric history and delivery-related information were collected according to the outpatient medical records and inpatient medical records. Body mass index (BMI) was calculated by dividing the weight by the square of the height. Macrosomia was identified as a birthweight exceeding 4000 grams.
Hemoglobin Tests
Hemoglobin tests were conducted using hematology analyzer (Sysmex XN-9100) by professional laboratory technicians. The results of hemoglobin were extracted through the hospital information system.
Postpartum Hemorrhage
Postpartum hemorrhage was diagnosed as the amount of blood loss ≥500 mL in vaginal delivery or ≥1000 mL in cesarean delivery within 24 hours after the delivery. The amount of blood loss was assessed jointly by one doctor and two midwives. In the present study, postpartum hemorrhage meeting this definition was identified using the International Classification of Diseases 10th Revision (ICD-10) code (O72) from the inpatient medical record.
Statistical Analyses
Group-based trajectory modelling (GBTM) was used to identify potential hemoglobin trajectories in pregnant women according to the “lcmm” package in R.19 GBTM divides pregnant women into different classes based on their hemoglobin change patterns, to reveal the different trajectories of change. Individuals assigned to the same class share the same trajectory. GBTM is being increasingly applied in the field of medicine.20,21 In this study, one to seven latent classes were fitted in the models; linear functions, quadratic functions and cubic functions were all taken into consideration. The optimal model was selected according to Bayesian information criterion (BIC), Akaike information criterion (AIC), average posterior probability (AvePP) and percentage of each class. Lower AIC and BIC values, the percentage of each class >5% and AvePP >0.7 indicate that the model is acceptable.
Analysis of variance and chi-square tests were applied to compare the basic characteristics among different trajectories. Association between hemoglobin trajectories and PPH was evaluated using logistic regression model, with adjustment for age, pre-delivery BMI, gestational age, primiparity, gravidity, caesarean section, history of caesarean section, and placenta previa. Receiver operating characteristic curve (ROC) was fitted to evaluate the final model. Furthermore, we applied logistic regression to evaluate the association between various hemoglobin cutoffs at the trajectory’s inflection point and PPH among women who had Hb measurements at the inflection point (N=3562). Sensitivity analysis was conducted among participants without hepatic diseases and metabolic diseases including hypertension, diabetes mellitus and thyroid diseases to avoid their effects on PPH. All analyses were performed using R software (version 4.3.1, R Core Team) and a two-sided P <0.05 was considered statistically significant.
Results
Basic Characteristics
Basic characteristics were shown in Table 1. The average age of the 4296 pregnant women was 31.04 years. The average pre-pregnancy BMI and pre-delivery BMI was 22.15 kg/cm2 and 26.84 kg/cm2, respectively. The average gestational age was 38.67 weeks. A total of 52.42% of the pregnant women were having their first pregnancy and 68.11% were primiparas. More than half (54.12%) of the participants delivered by caesarean section. And 12.78% of the pregnant women had a history of caesarean section. The proportions of assisted reproduction, multiple pregnancy, hypertensive disorders in pregnancy (HDP) were 1.89%, 0.91% and 10.94%, respectively. A total of 127 (2.96%) of the participants experienced PPH. The average hemoglobin concentration during the pregnancy was 119.48 g/L.
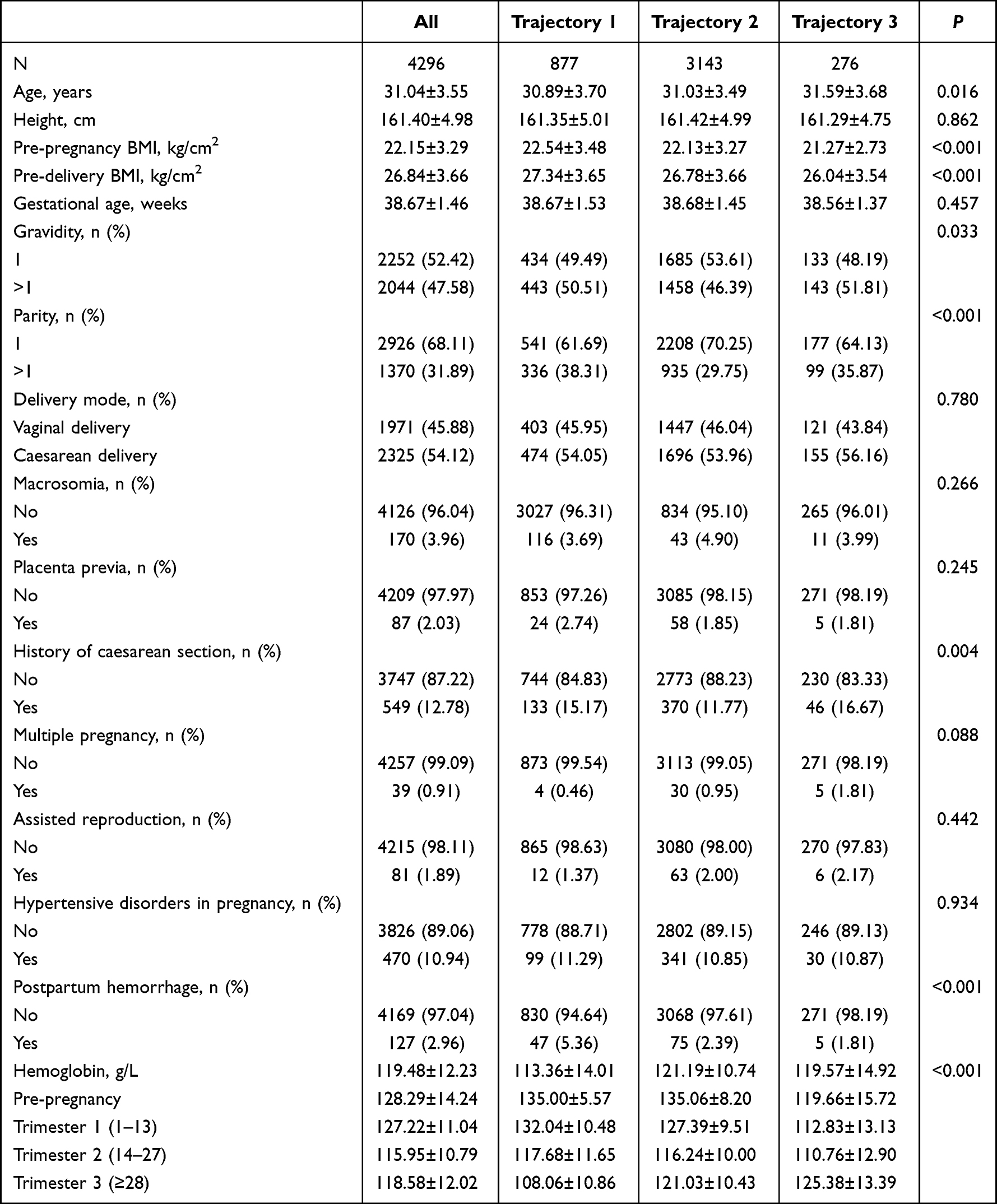 |
Table 1 Baseline Characteristics Comparison Among the Three Hemoglobin Trajectories |
Hemoglobin Trajectories
According to the AIC, BIC, AvePP and the percentage of each class, the 3-class model with cubic function was chosen as the optimal model (Figure 1). Three trajectories were identified. In trajectory 1 (decline-stable, N= 877, 20.41%), Hb levels were higher than those in trajectory 2 in the first trimester, and declined across pregnancy with no significant increase before delivery. In trajectory 2 (decline-rise, N=3143, 73.16%), maternal Hb decreased during the first and second trimesters (1–27 weeks), and increased during the third trimester (≥28 weeks). In trajectory 3 (stable-rise, N=276, 6.42%), Hb levels were stable and lower than those in trajectory 2 in early and mid-pregnancy and increased in late pregnancy. The AvePPs were 0.81, 0.82, 0.81 for trajectory 1, 2, 3, respectively, implying this model is acceptable.
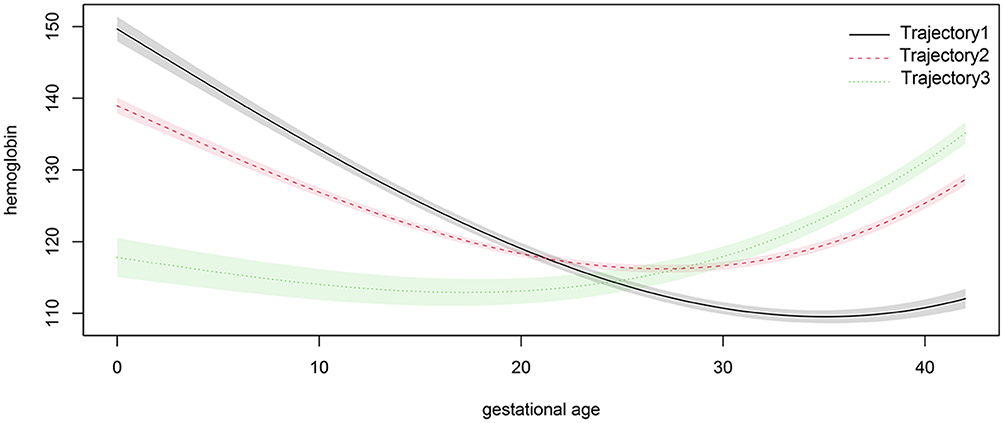 |
Figure 1 Hemoglobin trajectories over the gestational age (weeks). |
The mean predicted values of Hb trajectories were shown in Table S1. The lowest points of trajectory 1 and trajectory 2 were 109.53 g/L at 35 weeks and 116.21 g/L at 27 weeks, respectively. Between 28 and 35 weeks, Hb values in trajectory 1 continued to decline while Hb values in trajectory 2 had already started to rise.
The differences of basic characteristics among 3 trajectories were shown in Table 1. Pregnant women in trajectory 1 were younger, had higher pre-pregnancy BMI, higher pre-delivery BMI and less primiparas (P<0.05). The mean hemoglobin of trajectory 1 was the highest in the first trimester (1–13 weeks) and the second trimester 2 (14–27 weeks), and the lowest in the third trimester (≥28 weeks) among three trajectories. The proportion of PPH of participants in trajectory 1 was higher than that in trajectory 2 or 3 (P<0.05).
Hemoglobin Trajectories and Postpartum Hemorrhage
The association between hemoglobin trajectories and PPH was presented in Table 2. Compared with trajectory 2, trajectory 1 had a 2.36-fold higher risk (95% confident interval (CI): 1.59–3.47) for PPH, after adjusting for age, pre-delivery BMI, gestational age, primiparity, gravidity, caesarean section, history of caesarean section, and placenta previa. The association between trajectory 3 and PPH was not statistically significant with an OR of 0.79 (95% CI: 0.27–1.81). The area under the ROC curve (AUC) was 0.74 (95% CI: 0.70–0.79, Figure 2).
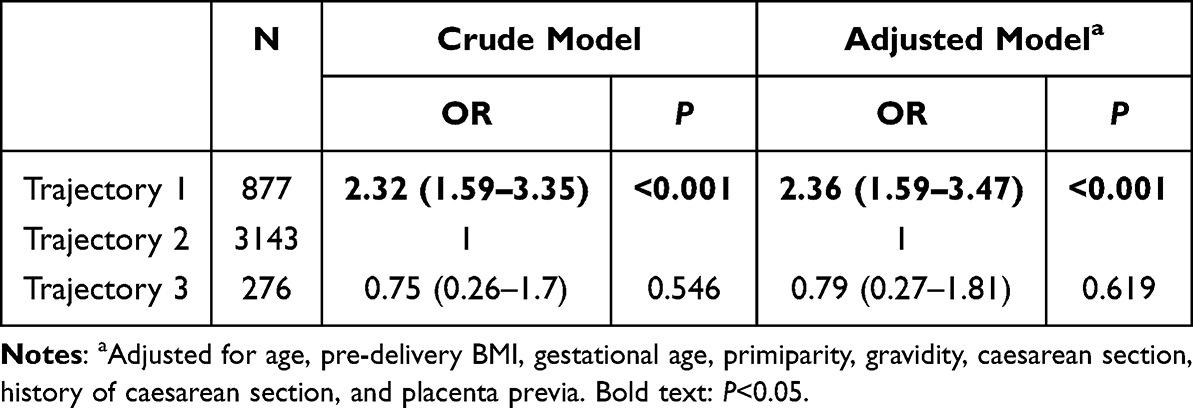 |
Table 2 Association Between Hemoglobin Trajectories and Postpartum Hemorrhage |
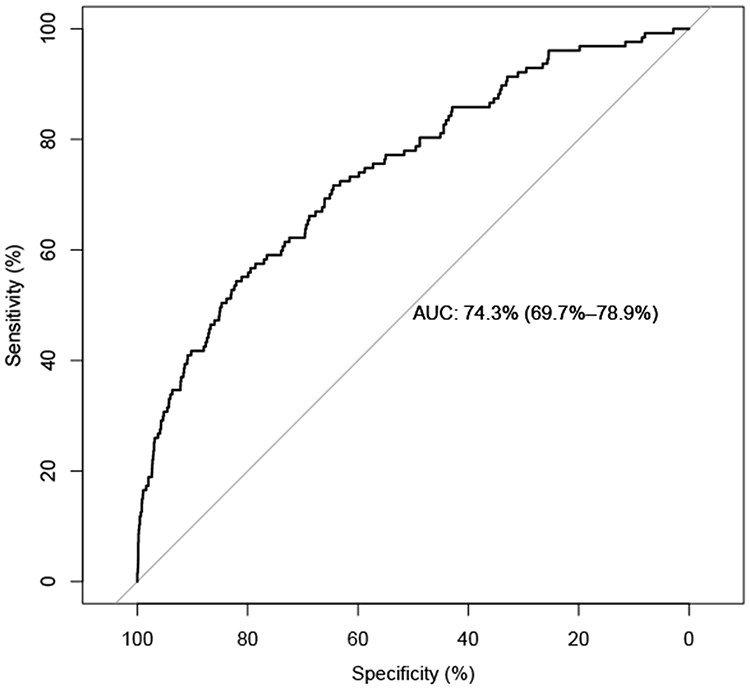 |
Figure 2 ROC curve. Abbreviation: ROC, receiver operating characteristic curve; AUC, area under the ROC curve. |
Table 3 showed the subgroup analyses of association between the hemoglobin trajectories and PPH. Among participants with vaginal delivery, trajectory 1 had a 2.90-fold increased risk for PPH (95% CI: 1.75–4.76), compared with trajectory 2. While the association was not statistically significant among participants with caesarean delivery (P for interaction =0.024). Interaction effects of age, pre-pregnancy BMI, gravidity, parity, gestational age, history of caesarean section and HDP with hemoglobin trajectories on PPH were not significant in the present study.
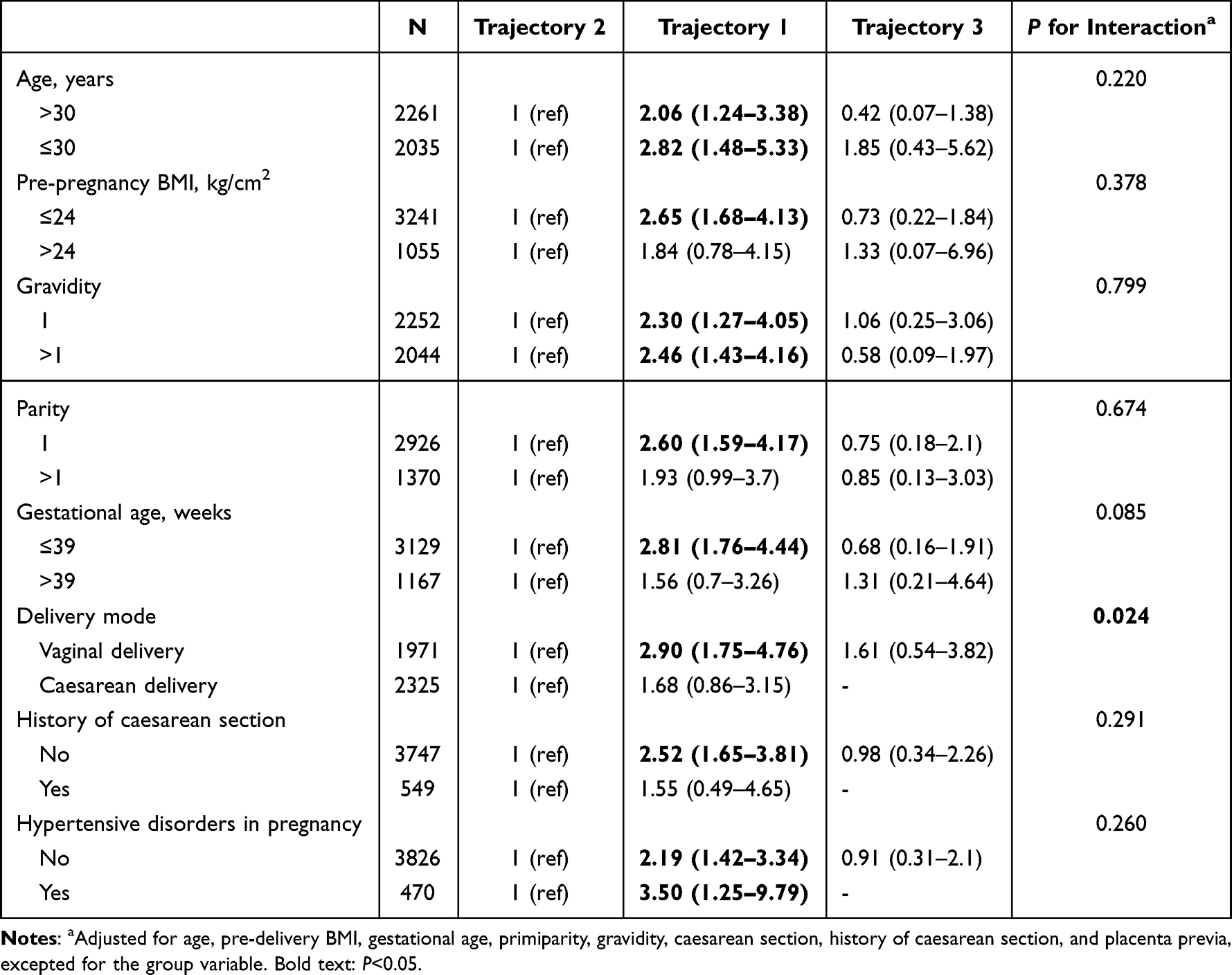 |
Table 3 Subgroup Analyses |
Given the divergent trends between trajectory 1 and trajectory 2 from 28 to 35 weeks, coupled with the timing of Hb tests in clinical practice (routine hemoglobin test at 28–32 weeks), we evaluated the association between various hemoglobin cutoffs at 28–32 weeks and PPH (Table S2). Odds ratios for PPH were statistically significant when Hb cutoffs were below 116 g/L, with adjustment for age, pre-delivery BMI, gestational age, primiparity, gravidity, caesarean section, history of caesarean section, and placenta previa. Compared with women with Hb ≥116 g/L at 28–32 weeks, women with Hb <116 g/L had a 1.64-fold higher risk of PPH (95% CI: 1.08–2.52).
Sensitivity Analysis
After excluding participants with hepatic diseases, hypertension, diabetes mellitus and thyroid disease, the results were robust and consistent with the main findings (Table 4). Compared with trajectory 2, trajectory 1 had a 3.02-fold higher risk (95% CI: 1.70–5.28), and trajectory 3 had a 0.69-fold higher risk of PPH (95% CI: 0.11–2.35), after adjustment for age, pre-delivery BMI, gestational age, primiparity, gravidity, caesarean section, history of caesarean section, and placenta previa.
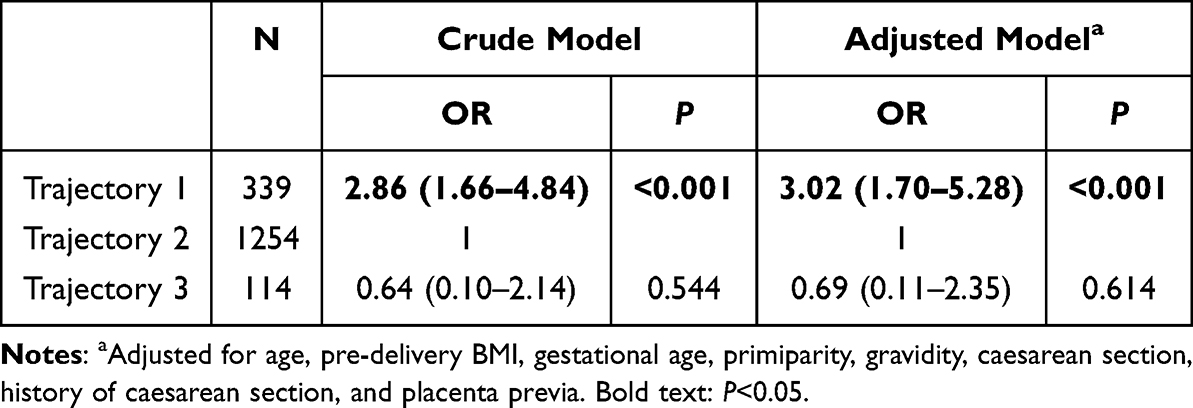 |
Table 4 Sensitivity Analysis Among Participants Without Hepatic Diseases, Hypertension, Diabetes Mellitus and Thyroid Disease |
Discussion
The present study identified three trajectories of maternal Hb concentration during pregnancy, and demonstrated that the Hb trajectory 1 (decline-stable) had a higher risk of PPH. Women who experience a rapid drop in hemoglobin during pregnancy, without a significant increase in late pregnancy, are at increased risk of PPH and should receive more attention. This study suggests that it is necessary to strengthen maternal health care and increase the frequency of Hb measurements during pregnancy, especially between 28 and 35 weeks.
In the current study, 73.16% of women were classified into trajectory 2, with Hb decreasing during the first and second trimesters, and increasing during the third trimester. The trend of trajectory 2 is consistent with previous studies on hematological changes in pregnancy.22 In early pregnancy, the renin-angiotensin-aldosterone system is substantially activated with expansion in plasma volume starting at 6 to 8 weeks and rising progressively until the beginning of the third trimester.16,23,24 Maternal Hb levels decrease because of the expansion in plasma volume being greater than the growth in red blood cell mass.25 During the third trimester, hemoglobin levels rise slightly from the lowest point in the second trimester, as red blood cell mass continues to grow while plasma volume expansion stabilizes.26
A total of 20.41% of the participants were classified into trajectory 1 and had a higher risk of PPH compared with those in trajectory 2, indicating that a higher drop of Hb during pregnancy, with no significant rise in late pregnancy, might be related to a higher risk of PPH. Published literature reported the association between the Hb drop during pregnancy and neonatal outcomes, such as small for gestational age, low birthweight, etc.27–29 However, the evidence for maternal outcomes is limited. Furthermore, most published literature only focuses on the trimester-specific Hb level. The protective effect of pre-delivery hemoglobin on PPH has been confirmed.12,14,30 However, the association between hemoglobin during the first or second trimester and PPH is inconsistent. A cohort study of 4082 births in Switzerland found that high Hb value in the second trimester increased PPH.17 A meta-analysis found that low maternal Hb (<110 g/L) during the second trimester could increase the risk of PPH (OR: 1.43, 1.01–2.03).9 The difference may be accounted for the timing of Hb measurement, because Hb levels are dynamic during pregnancy. Therefore, tracking these changes is important to better identify women at increased risk of PPH.
Only 6.42% of women were classified into trajectory 3 with a lower Hb in early pregnancy and an increased Hb in late pregnancy. No significant association was observed between trajectory 3 and PPH, which might be related to interventions in the low Hb concentration. For women diagnosed with anemia or iron deficiency, prompt treatment will be taken such as iron supplementation.31,32 Iron supplementation can effectively improve Hb levels.33 This might explain the increase of Hb in late pregnancy in trajectory 3.
Interestingly, the hemoglobin value continued to decline in trajectory 1 while the hemoglobin level in trajectory 2 had already started to rise at 28–35 weeks. Neither the women in trajectory 1 (111.80 g/L) nor that in trajectory 2 (116.26 g/L) met the criteria for anemia diagnosis at 28 weeks (<110 g/L, WHO guideline13). However, a Hb level below 116 g/L and a downward trend observed after 28 weeks showed a higher risk of PPH. In clinical practice, more attention and more active intervention should be provided for this group of women, even in the absence of an anemia diagnosis.
The subgroup analysis showed a strong association between Hb trajectory and PPH in vaginal deliveries, but no association in cesarean deliveries. Uterine atony is the most important cause of postpartum hemorrhage. Effective uterine contraction is an active and energy-consuming process that requires adequate oxygen. Moderate to severe anemia or low Hb level can lead to tissue hypoxia, thereby weakening the strength and endurance of uterine muscle fiber contractions. In cesarean delivery, as the uterine incision has been sutured and the major bleeding vessels can be managed under direct visualization, surgical measures largely compensate for the potential deficiency in uterine contractility caused by anemia or low Hb.34
There are several advantages in the present study. Firstly, to our best knowledge, this study is the first to evaluate the dynamic trajectories of maternal hemoglobin levels and their impact on PPH. The classification of Hb trajectories is beneficial for identifying women at high risk of PPH. A major advantage of this method is its low cost, as it utilizes existing prenatal data, eliminating the need for additional tests. Secondly, the application of group-based trajectory modelling identifies subgroups with the same Hb change patterns, revealing the differences in Hb trajectories among different pregnant groups and their clinical significance. Also, several limitations should be further improved. Firstly, this study is a single-center study. Although the present study was conducted in a provincial general hospital (Critical Maternal Care Center) where some women were from other regions, the extrapolation of the results still should be cautious. Secondly, some variables such as iron supplementation during pregnancy were not obtained in this study, so we cannot explore the underlying causes of different trajectories, which may be addressed in further studies.
Conclusions
In conclusion, the present study identified three trajectories of maternal hemoglobin. The hemoglobin levels of most maternal women decreased during the first and second trimesters and slightly increased during the third trimester. Women who are not anemic in early pregnancy but experience a rapid decline in Hb during pregnancy, especially women with Hb <116 g/L in the early third trimester, are at high risk of PPH and should receive more attention. Integrating the analysis of Hb trajectory into antenatal care provides a low-cost strategy for early risk stratification and proactive management of PPH.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. This study was approved by the Ethics and Human Subject Committee of Shaanxi Provincial People’s Hospital (Approval number: 2024-R146, 2024/6/13). All data used were de-identified and the need for consent was waived.
Funding
This study was supported by Natural Science Basic Research Program of Shaanxi (Program No. 2024JC-YBQN-0913) and Scientific and technological personnel support program of Shaanxi Provincial People’s Hospital (Program No. 2022JY-40).
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Corbetta-Rastelli CM, Friedman AM, Sobhani NC, Arditi B, Goffman D, Wen T. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstetrics Gynecol. 2023;141(1):152–10. doi:10.1097/aog.0000000000004972
2. Shi HF, Chen L, Wang XX, et al. Incidence and trend of severe postpartum hemorrhage between 2016 and 2019 in China. Zhonghua fu chan ke za zhi. 2021;56(7):451–457. DOI:10.3760/cma.j.cn112141-20210209-00070
3. Thams AB, Larsen MH, Rasmussen SC, Jeppegaard M, Krebs L. Incidence of postpartum hemorrhage and risk factors for recurrence in the subsequent pregnancy. Arch Gynecol Obstet. 2023;307(4):1217–1224. doi:10.1007/s00404-022-06591-4
4. Tolossa T, Fetensa G, Zewde EA, Besho M, Jidha TD. Magnitude of postpartum hemorrhage and associated factors among women who gave birth in Ethiopia: a systematic review and meta-analysis. Reproductive Health. 2022;19(1):194. doi:10.1186/s12978-022-01498-4
5. Cresswell JA, Alexander M, Chong MYC, et al. Global and regional causes of maternal deaths 2009-20: a WHO systematic analysis. Lancet Global Health. 2025;13(4):e626–e634. doi:10.1016/s2214-109x(24)00560-6
6. The China health statistics yearbooks 2024. The National Health Commission of China. 2025.
7. Neary C, Naheed S, McLernon DJ, Black M. Predicting risk of postpartum haemorrhage: a systematic review. BJOG. 2021;128(1):46–53. doi:10.1111/1471-0528.16379
8. Yunas I, Islam MA, Sindhu KN, et al. Causes of and risk factors for postpartum haemorrhage: a systematic review and meta-analysis. Lancet. 2025;405(10488):1468–1480. doi:10.1016/s0140-6736(25)00448-9
9. Young MF, Oaks BM, Rogers HP, et al. Maternal low and high hemoglobin concentrations and associations with adverse maternal and infant health outcomes: an updated global systematic review and meta-analysis. BMC Pregnancy Childbirth. 2023;23(1):264. doi:10.1186/s12884-023-05489-6
10. Cheng TS, Zahir F, Solomi C, et al. Does induction or augmentation of labor increase the risk of postpartum hemorrhage in pregnant women with anemia? A multicenter prospective cohort study in India. Int J Gynaecol Obstet. 2025;169(1):299–309. doi:10.1002/ijgo.16008
11. Shi H, Chen L, Wang Y, et al. Severity of anemia during pregnancy and adverse maternal and fetal outcomes. JAMA Network Open. 2022;5(2):e2147046. DOI:10.1001/jamanetworkopen.2021.47046
12. Liu CN, Yu FB, Xu YZ, et al. Prevalence and risk factors of severe postpartum hemorrhage: a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21(1):332. doi:10.1186/s12884-021-03818-1
13. World Health Organization. Guideline on Haemoglobin Cutoffs to Define Anaemia in Individuals and Populations. Geneva: World Health Organization; 2024.
14. Glonnegger H, Glenzer MM, Lancaster L, Barnes RFW, von Drygalski A. Prepartum anemia and risk of postpartum hemorrhage: a meta-analysis and brief review. Clin Appl Thromb Hemost. 2023;29:10760296231214536. doi:10.1177/10760296231214536
15. Young MF, Oaks BM, Tandon S, Martorell R, Dewey KG, Wendt AS. Maternal hemoglobin concentrations across pregnancy and maternal and child health: a systematic review and meta-analysis. Ann N Y Acad Sci. 2019;1450(1):47–68. doi:10.1111/nyas.14093
16. Ouzounian JG, Elkayam U. Physiologic changes during normal pregnancy and delivery. Cardiol Clin. 2012;30(3):317–329. doi:10.1016/j.ccl.2012.05.004
17. Robinson MR, Patxot M, Stojanov M, Blum S, Baud D. Postpartum hemorrhage risk is driven by changes in blood composition through pregnancy. Sci Rep. 2021;11(1):19238. doi:10.1038/s41598-021-98411-z
18. Mansukhani R, Shakur-Still H, Chaudhri R, et al. Maternal anaemia and the risk of postpartum haemorrhage: a cohort analysis of data from the WOMAN-2 trial. Lancet Global Health. 2023;11(8):e1249–e1259. doi:10.1016/s2214-109x(23)00245-0
19. Proust-Lima C, Philipps V, Liquet B. Estimation of extended mixed models using latent classes and latent processes: the R package lcmm. J Statistical Software. 2017;78(2):1–56. doi:10.18637/jss.v078.i02
20. Yang J, Ma B, Tong H. Lymphocyte count trajectories are associated with the prognosis of sepsis patients. Crit Care. 2024;28(1):399. doi:10.1186/s13054-024-05186-6
21. Dalrymple KV, Tydeman F, Bone JN, et al. The relationship between virtual antenatal care and pregnancy outcomes in a diverse UK inner-city population: a group-based trajectory modeling approach using routine health records. LID. 2025;S0002–9378(25)00538–1. (1097-6868 (Electronic)
22. Patxot M, Stojanov M, Ojavee SE, et al. Haematological changes from conception to childbirth: an indicator of major pregnancy complications. Eur J Haematol. 2022;109(5):566–575. doi:10.1111/ejh.13844
23. Tkachenko O, Shchekochikhin D, Schrier RW. Hormones and hemodynamics in pregnancy. Int J Endocrinol Metabol. 2014;12(2):e14098. doi:10.5812/ijem.14098
24. Sanghavi M, Rutherford JD. Cardiovascular Physiology of Pregnancy. Circulation. 2014;130(12):1003–1008. doi:10.1161/CIRCULATIONAHA.114.009029
25. Chandra M, Paray AA. Natural physiological changes during pregnancy. Yale J Biol Med. 2024;97(1):85–92. doi:10.59249/jtiv4138
26. De Haas S, Ghossein-Doha C, Van Kuijk SMJ, Van Drongelen J, Spaanderman MEA. Physiological adaptation of maternal plasma volume during pregnancy: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2017;49(2):177–187. doi:10.1002/uog.17360
27. Townsend K, Maric T, Steer PJ, Savvidou MD. Maternal hemoglobin drop in multiple pregnancy is associated with higher gestational age at birth and birthweight. Acta Obstet Gynecol Scand. 2024;103(10):2002–2012. doi:10.1111/aogs.14907
28. Jwa SC, Fujiwara T, Yamanobe Y, Kozuka K, Sago H. Changes in maternal hemoglobin during pregnancy and birth outcomes. BMC Pregnancy Childbirth. 2015;15(1):80. doi:10.1186/s12884-015-0516-1
29. Xu S, Wang W, Li Q, et al. Association of maternal longitudinal hemoglobin with small for gestational age during pregnancy: a prospective cohort study. Nutrients. 2022;14(7). doi:10.3390/nu14071403
30. Glenzer MM, Correia M, Nhantumbo V, et al. Postpartum hemorrhage in sub-saharan africa-a prospective study in metropolitan mozambique. J Thromb Haemost. 2023;21(12):3463–3476. doi:10.1016/j.jtha.2023.09.002
31. Benson AE, Shatzel JJ, Ryan KS, et al. The incidence, complications, and treatment of iron deficiency in pregnancy. Eur J Haematol. 2022;109(6):633–642. doi:10.1111/ejh.13870
32. Goonewardene M, Shehata M, Hamad A. Anaemia in pregnancy. Best Pract Res Clin Obstetrics Gynaecol. 2012;26(1):3–24. doi:10.1016/j.bpobgyn.2011.10.010
33. Finkelstein JL, Cuthbert A, Weeks J, et al. Daily oral iron supplementation during pregnancy. Cochrane Database Syst Rev. 2024;8(8):Cd004736. doi:10.1002/14651858.CD004736.pub6
34. Ashwal E, Bergel Bson R, Aviram A, Hadar E, Yogev Y, Hiersch L. Risk factors for postpartum hemorrhage following cesarean delivery. J Matern Fetal Neonatal Med. 2022;35(18):3626–3630. doi:10.1080/14767058.2020.1834533
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Pre-Pregnancy Hemoglobin Level on the Association Between Pre-Pregnancy Body Mass Index and Gestational Diabetes Mellitus: A Retrospective Cohort Study in a Single Center in China
Wu K, Ke HH, Gong W, Hu H, Chen L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3767-3775
Published Date: 8 December 2022