Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Hemoglobin as a Treatable Trait in COPD: A Retrospective Observational Cohort Study on Hemoglobin Levels and All-Cause Mortality from NHANES Data
Received 1 May 2025
Accepted for publication 11 October 2025
Published 25 October 2025 Volume 2025:20 Pages 3473—3481
DOI https://doi.org/10.2147/COPD.S537888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Dongxiang Ji,1 Hewei Yu2
1Department of Respiratory Medicine, Huzhou Central Hospital, Affiliated Central Hospital of Huzhou University, Huzhou, People’s Republic of China; 2Department of Otorhinolaryngology, Huzhou Central Hospital, Affiliated Central Hospital of Huzhou University, Huzhou, People’s Republic of China
Correspondence: Hewei Yu, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the third leading cause of death globally. Hemoglobin (HGB) abnormalities, including anemia and secondary polycythemia, are common comorbidities in COPD patients, yet their association with mortality remains less clear. This study aimed to investigate the relationship between HGB levels and all-cause mortality in COPD patients and to evaluate whether HGB could serve as a treatable trait in COPD.
Methods: We conducted a retrospective observational cohort study using data from the National Health and Nutrition Examination Survey (NHANES, 2013– 2018). A total of 544 COPD patients were included. Multivariable Cox regression was conducted to assess HGB-mortality associations, adjusting for age, sex, BMI, smoking status, and comorbidities. Nonlinear relationships were examined using generalized additive models with threshold effect analysis. Stratified analyses were performed by sex, age, and comorbidity status.
Results: Among 544 COPD patients, HGB levels demonstrated a significant nonlinear association with all-cause mortality, with a critical inflection point identified at 14.2 g/dL. Below this threshold, each 1g/dL in HGB was associated with reduced mortality (adjusted HR=0.73, 95% CI: 0.61– 0.79, P< 0.0001). Above 14.2g/dL, however, no significant association was observed (HR=1.24, 95% CI: 0.98– 1.55, P=0.0775). Although stratified analyses suggested variation in HR across subgroups (including males, elderly > 65 years, smokers, and those with cardiovascular disease), interaction tests did not reach statistical significance (all P-interaction > 0.05), indicating no evidence of effect modification. Smoothing curves supported this nonlinear relationship, showing decreasing mortality risk with rising HGB until the threshold, beyond which risk stabilized with a slight non-significant upward trend.
Conclusion: This study identifies a nonlinear relationship between HGB levels and mortality in COPD, establishing 14.2 g/dL as a critical threshold that supports anemia’s inclusion in the COPD “treatable traits” framework. Below this value, increasing HGB is associated with reduced mortality, whereas above it no further benefit is observed. Clinicians should prioritize HGB monitoring in high-risk subgroups (elderly males, smokers, and cardiac comorbidities).
Keywords: COPD, all-cause mortality, anemia, treatable traits
Introduction
Chronic obstructive pulmonary disease (COPD) ranks as the third leading cause of death globally, accounting for 3.23 million fatalities in 2019, surpassed only by ischemic heart disease and stroke.1 Projections from the Global Burden of Disease (GBD) database indicate a 23% increase in COPD prevalence among adults aged ≥25 years by 2050.2 Without effective interventions, annual deaths attributable to COPD and related complications are expected to exceed 5.4 million by 2060.1
The diagnosis of COPD is typically confirmed by post-bronchodilator spirometry, with a forced expiratory volume in 1 second to forced vital capacity ratio (FEV₁/FVC) <0.70 serving as the key diagnostic criterion. While the present study relies on self-reported physician diagnosis due to data availability, this approach is widely used in large epidemiological surveys and has been validated in prior research.3,4
The emerging concept of “treatable traits” in COPD encompasses pulmonary (eg, airflow limitation, eosinophilic inflammation), extrapulmonary (eg, cardiovascular comorbidities, metabolic dysfunction), and behavioral/lifestyle factors (eg, smoking cessation).5 Current clinical guidelines recognize the importance of managing comorbidities in COPD, though specific recommendations for routine hemoglobin monitoring remain limited. This evidence gap highlights the novelty of investigating HGB abnormalities-which may arise from chronic hypoxemia, systemic inflammation, erythropoietin resistance, or altered blood viscosity6,7-as a potential treatable trait.
In COPD, chronic hypoxemia may induce secondary polycythemia, with elevated HGB levels associated with pulmonary hypertension,8 venous thromboembolism,9 and increased mortality.10 Conversely, anemia—frequently observed in older COPD patients with multimorbidity—correlates with poorer quality of life,11 higher exacerbation risk,11 and elevated mortality.12 Despite HGB dysregulation being a prevalent comorbidity, the optimal HGB range for COPD patients remains undefined. This retrospective observational cohort study utilizes the NHANES database to examine HGB’s association with all-cause mortality in COPD, assesses its potential as a treatable trait, and determines an optimal threshold for personalized prognosis management.
Methods
Study Design and Population
This retrospective observational cohort study utilized data from the NHANES. COPD diagnosis was based on affirmative responses to the survey question: “Has a doctor ever told you that you have COPD?”—an established method validated in prior publications.3,4 We included participants aged >25 years with COPD enrolled between 2013 and 2018, excluding those with missing data on HGB, body mass index (BMI), waist circumference, or mortality outcomes (see Figure 1). Ninety-nine all-cause deaths were recorded.
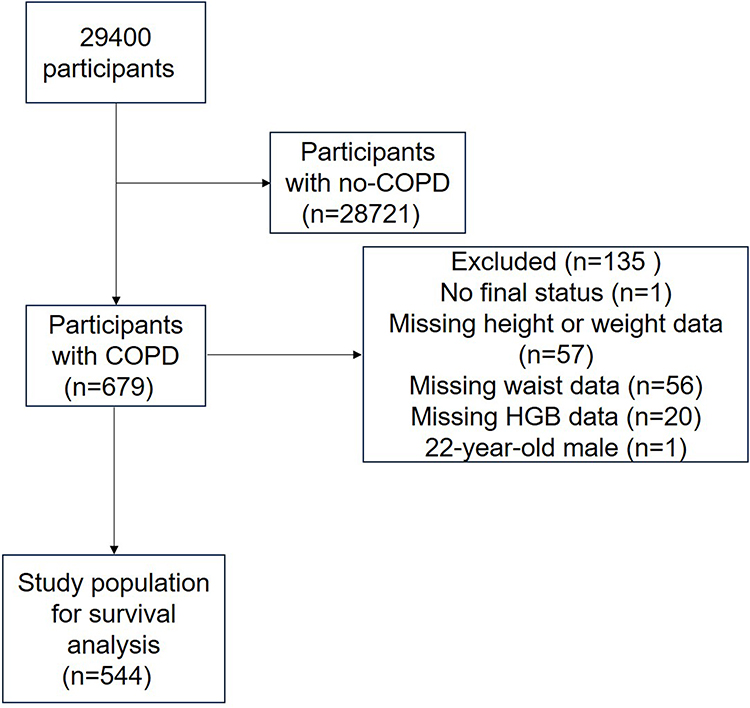 |
Figure 1 Flowchart of participant selection from the NHANES 2013–2018 cohort. Flowchart of participant selection. Of the 29,400 initial participants, 679 reported a physician’s diagnosis of COPD. After excluding participants with missing data on mortality outcome, body mass index, waist circumference, or hemoglobin levels, as well as one outlier due to age, a final cohort of 544 COPD patients was included in the survival analysis. |
Variables
Exposure: HGB (g/dL) was measured using the Beckman Coulter method at NHANES Mobile Examination Centers (MEC).
Outcome: All-cause mortality (through April 2022) was determined via linkage to the National Death Index (NDI), recorded as binary (alive/dead) and survival time (months).
Covariates: Sex, age, smoking status, BMI (kg/m²), waist circumference (cm), diabetes, and cardiovascular disease (coronary artery disease or heart failure).
Ethical Considerations
This study utilized de-identified, publicly available data from the NHANES database. According to Article 32, Items 1 and 2 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (issued by the National Health Commission of the People’s Republic of China on February 18, 2023; available at: https://www.nhc.gov.cn/qjjys/c100016/202302/6b6e447b3edc4338856c9a652a85f44b.shtml), this research qualifies for exemption from ethics approval as it involves the analysis of existing public domain data where individuals cannot be identified. Therefore, no additional informed consent or institutional review board approval was required. The study was conducted in accordance with the ethical standards laid down in the Declaration of Helsinki for retrospective research.
Statistical Analysis
Continuous variables with normal distribution were presented as mean ± standard deviation, while categorical variables were expressed as frequencies (percentages). Group comparisons across the four hemoglobin quartiles were performed using one-way ANOVA for normally distributed continuous variables, Kruskal–Wallis tests for non-normally distributed continuous variables, and chi-square tests for categorical variables.
Multivariable Cox proportional hazards models were constructed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality. Covariates were selected based on clinical relevance and data availability, including age, sex, BMI, waist circumference, and smoking status. HGB concentrations were analyzed both as continuous variables and quartile-based ordinal variables. To assess dose-response relationships, trend tests were performed by assigning median values to each quartile and treating this as a continuous variable in the Cox models.
Nonlinear associations were examined using generalized additive models (GAM) with smoothing splines. When nonlinearity was detected, inflection points were identified through recursive algorithms, and piecewise linear models were subsequently developed. The log-likelihood ratio test was used to compare the goodness-of-fit between linear and nonlinear models.
Stratified analyses were conducted by sex (male/female), age (≤65/>65 years), smoking status (ever/never), cardiovascular disease (yes/no), and diabetes (yes/no). Interaction effects were evaluated using likelihood ratio tests. All analyses were performed using EmpowerStats software (version 6.0), with two-tailed P-values<0.05 considered statistically significant.
Results
Baseline Characteristics
This study enrolled a total of 544 participants, who were stratified into four groups based on HGB levels (quartiles Q1-Q4). Baseline characteristic analysis revealed: The high HGB group (Q4) had a significantly higher proportion of males compared to other groups (Q4: 77.78% vs Q1: 41.35%, P<0.001). Post-hoc pairwise comparisons for gender, performed using chi-square tests with Bonferroni correction, indicated that the proportion of males in Q4 was significantly higher than in Q1 (P<0.001), Q2 (P<0.001), and Q3 (P<0.001). No significant differences were observed among groups for age (P=0.119), BMI (P=0.655), or waist circumference (P=0.365). Smoking prevalence showed an increasing trend with higher HGB levels (Q1: 81.95% vs Q4: 93.06%, P=0.003). Diabetes prevalence was highest in the low HGB group (Q1) (41.35% vs Q4: 28.47%, P=0.033), with post-hoc analysis indicating a significant difference between Q1 and Q2 (P=0.019). Heart disease prevalence followed a similar pattern (Q1: 41.35% vs Q4: 25.69%, P=0.031), with a significant difference between Q1 and Q4 (P=0.008) in post-hoc testing. Details are presented in Table 1.
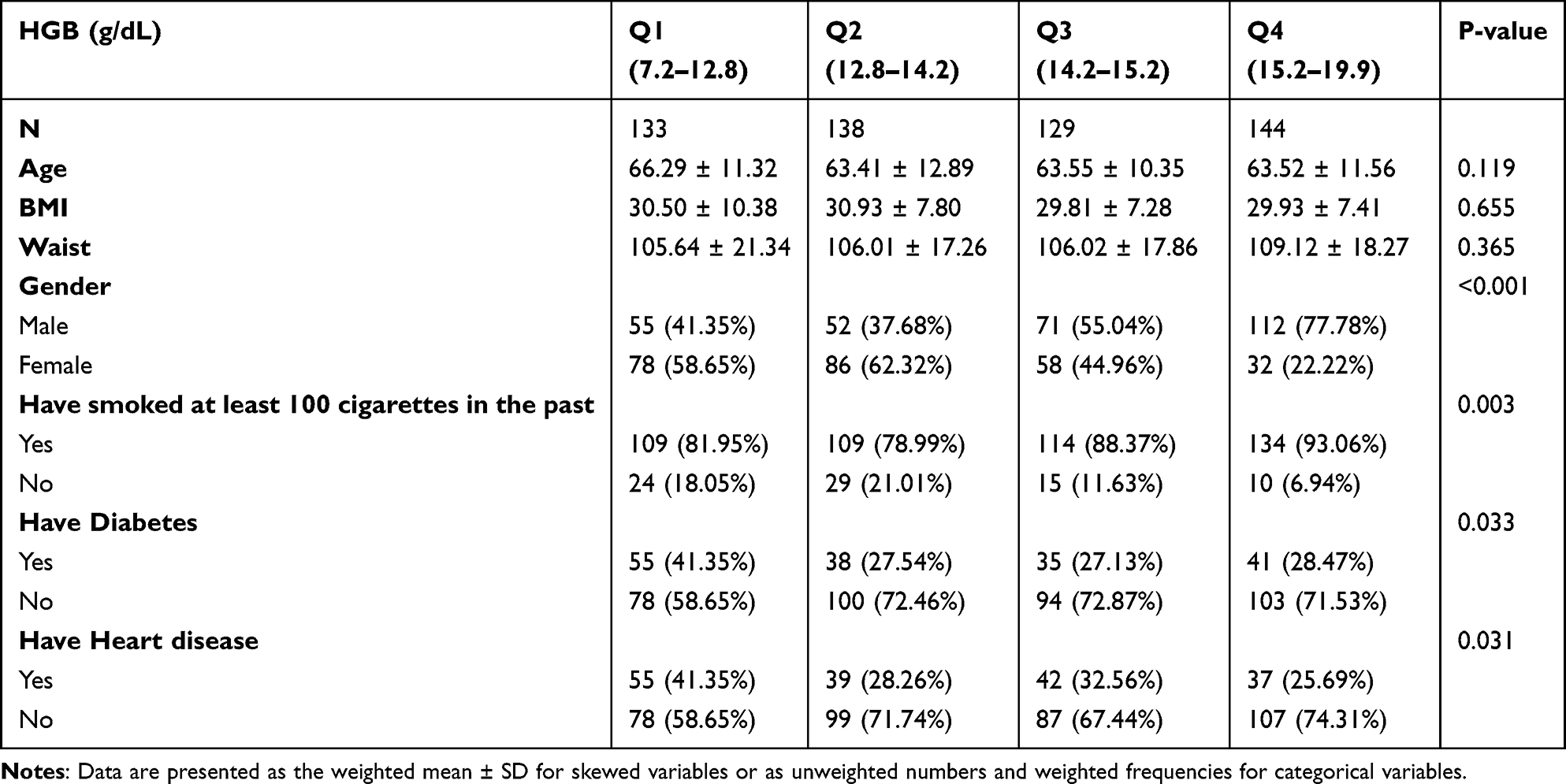 |
Table 1 Baseline Characteristics of COPD Participants |
Association Between Hemoglobin and All-Cause Mortality
We employed Cox proportional hazards models for analysis, constructing three sequential models: an unadjusted model, Model I (adjusted for sex and age), and Model II (further adjusted for smoking history, BMI, waist circumference, diabetes, heart disease, and other health-related factors). The results demonstrated a significant inverse association between HGB levels and mortality risk. In the unadjusted model, the hazard ratio for HGB was 0.79 (95% CI: 0.71–0.88, P<0.0001), indicating a strong association between higher HGB levels and lower mortality risk. This association remained significant after adjusting for sex and age (HR=0.81, 95% CI: 0.73–0.90, P<0.0001). Further adjustment for additional potential confounders yielded a slightly attenuated but still significant hazard ratio (HR=0.82, 95% CI: 0.74–0.91, P<0.0001).
In quartile analysis, the following trends emerged: The second quartile (Q2) showed an HR of 0.39 (95% CI: 0.22–0.68, P = 0.0009), suggesting significantly reduced mortality risk compared to the first quartile. The third quartile (Q3) demonstrated an HR of 0.37 (95% CI: 0.21–0.65, P = 0.0005), further validating this trend. The fourth quartile (Q4) exhibited an HR of 0.47 (95% CI: 0.28–0.79, P = 0.0045), indicating significantly lower mortality risk compared to Q1. When analyzing HGB quartiles as a continuous variable, the results showed an HR of 0.75 (95% CI: 0.63–0.90, P = 0.0023), providing additional support for the inverse relationship between HGB levels and mortality. A significant trend across quartiles was observed (P for trend <0.001). Detailed results are presented in Table 2.
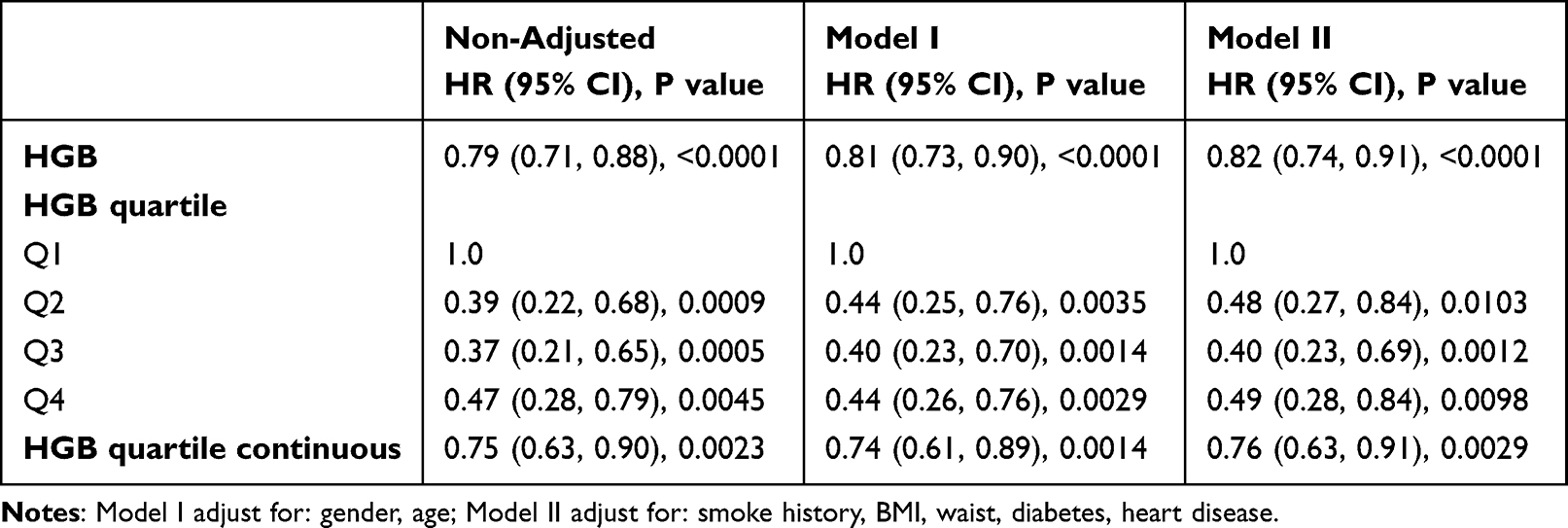 |
Table 2 Multivariate Cox Regression Analysis on Associations Between HGB and All-Cause Mortality |
Nonlinear Relationship and Threshold Effect Analysis
Generalized additive models revealed a nonlinear relationship between HGB levels and mortality risk. Smooth curve fitting in the figure illustrates that mortality risk initially decreases with increasing HGB values before plateauing (Figure 2). This pattern suggests that lower HGB levels are associated with higher mortality risk, while progressive HGB elevation correlates with gradually decreasing mortality risk that eventually stabilizes. See Figure 2 for details.
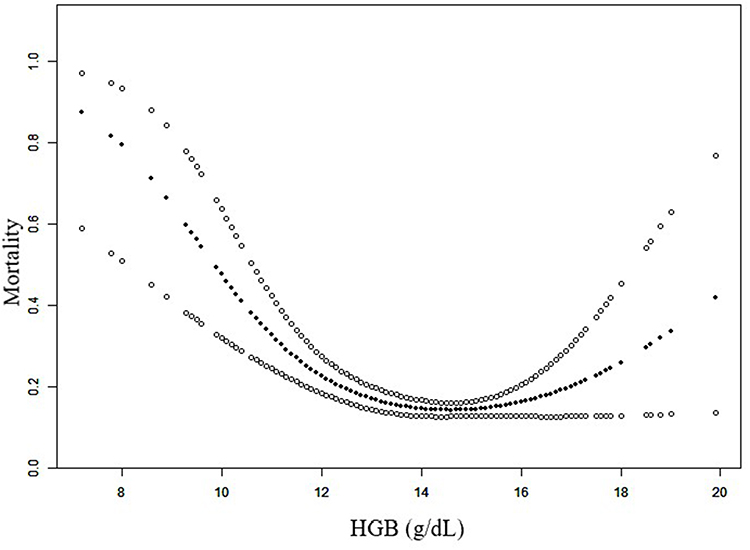 |
Figure 2 The nonlinear relationship between HGB levels and all-cause mortality risk in COPD patients. Smoothing curve fit with 95% confidence intervals from the generalized additive model, showing the nonlinear association between baseline HGB levels (g/dL) and the risk of all-cause mortality. The model is adjusted for sex, age, smoking history, body mass index, waist circumference, diabetes, and heart disease. A critical inflection point at 14.2 g/dL was identified through threshold effect analysis. |
Based on this nonlinear pattern, we conducted a piecewise linear regression to identify an inflection point. Threshold effect analysis identified a critical inflection point at 14.2 g/dL (Table 3). Below this threshold, each 1 g/dL increase in HGB was associated with a significant reduction in mortality risk (adjusted HR=0.73, 95% CI: 0.61–0.79, P<0.0001). Above this threshold, however, no significant association was observed (HR=1.24, 95% CI: 0.98–1.55, P=0.0775). The log-likelihood ratio test comparing the linear model with the piecewise linear model was statistically significant (P=0.003), confirming the superior fit of the nonlinear threshold model.
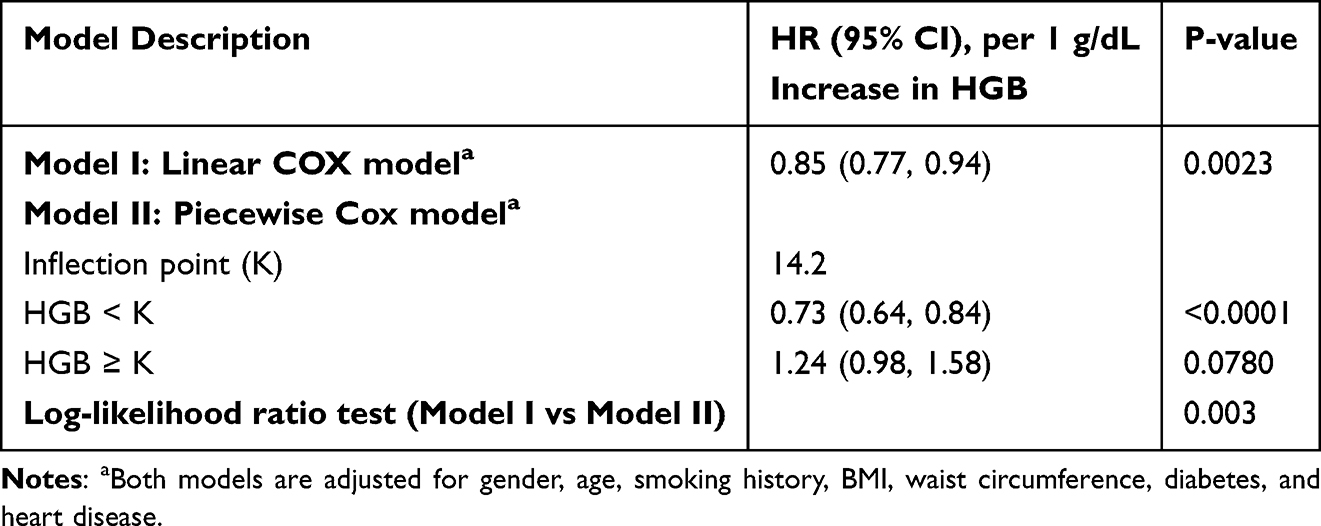 |
Table 3 Comparison of Linear and Piecewise Linear Cox Regression Models for the Association Between HGB (g/dL) and All-Cause Mortality |
In the linear regression model (Model I), which assumed a linear relationship across the entire HGB range, a significant inverse correlation existed between HGB and mortality probability was observed (HR=0.85, 95% CI: 0.77–0.94, P=0.0023). Both the linear and piecewise linear models were adjusted for the same set of covariates (sex, age, smoking history, BMI, waist circumference, diabetes, and heart disease).
Subgroup Analyses
Stratified analyses were performed by sex, age, smoking status, diabetes, and heart disease status (Table 4). Although point estimates suggested variation in HR across subgroups, likelihood ratio tests for interaction did not reveal any statistically significant effect modification by these covariates (all P-interaction >0.05).
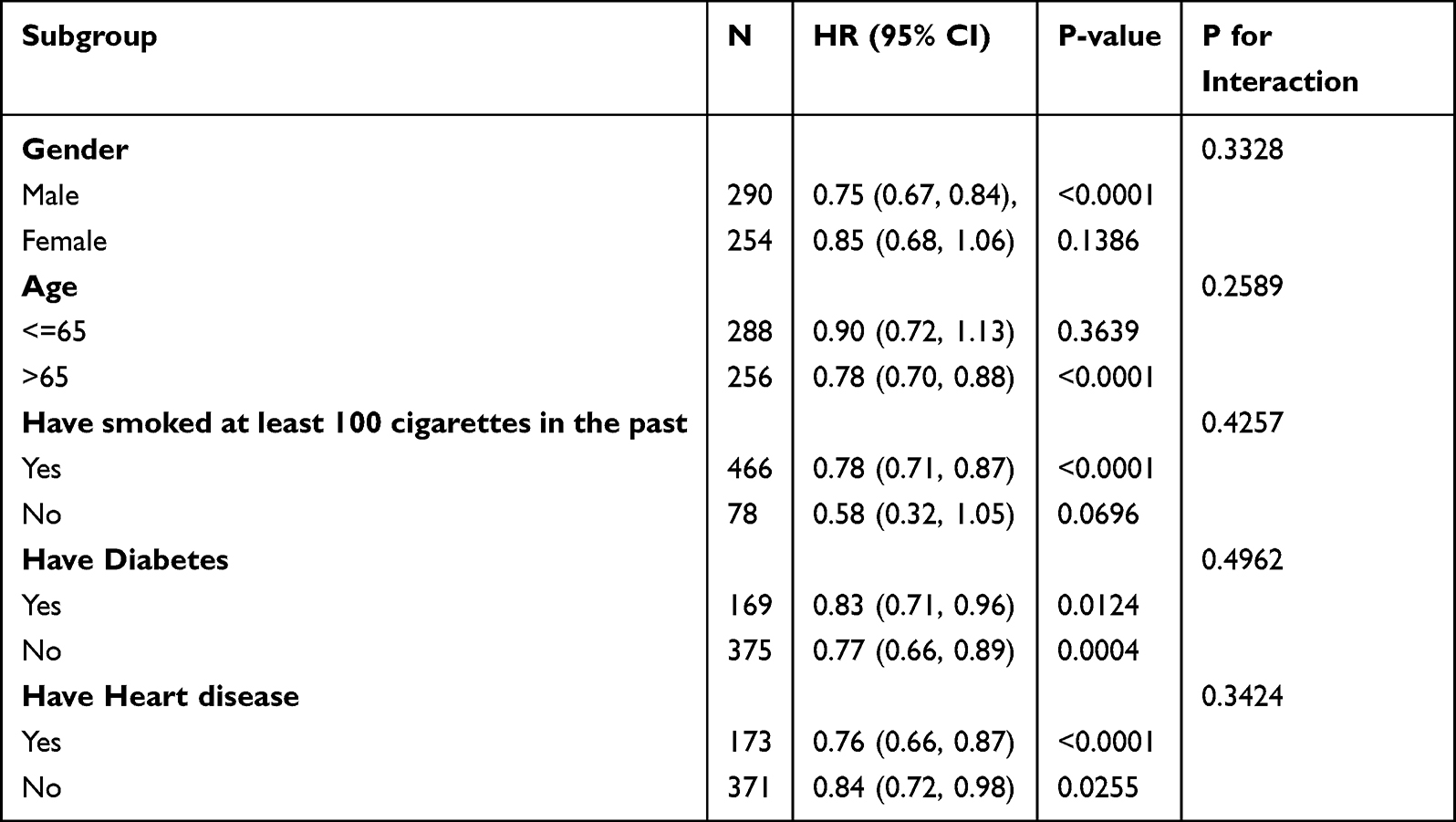 |
Table 4 Subgroups Analysis of HGB with All-Cause Mortality |
Discussion
This study, based on the NHANES database, employed a retrospective observational cohort design to investigate the association between baseline HGB levels and all-cause mortality in COPD patients. Our analysis demonstrated that lower HGB levels were significantly associated with an increased risk of all-cause mortality. Although stratified analyses suggested variation in the magnitude of association across subgroups—such as males, older patients (>65 years), those with a history of smoking, and those with comorbid cardiovascular disease—formal interaction tests did not reveal statistically significant effect modification (all P-interaction >0.05). Meanwhile, it should be noted that some subgroup analyses, particularly those with smaller sample sizes such as non-smokers (n=78), may have limited statistical power to detect significant associations. Therefore, these subgroup findings should be interpreted with caution and require further validation in larger cohorts.
Chronic obstructive pulmonary disease (COPD) presents multiple treatable traits, which can be categorized into: 1. Pulmonary treatable traits, including airflow limitation,13 airway mucosal edema, eosinophilic airway inflammation,14 cough hypersensitivity,15 bronchiectasis, pulmonary hypertension, and chronic respiratory failure. 2. Extrapulmonary treatable traits, such as physical functional decline, obesity, cachexia, obstructive sleep apnea syndrome, cardiovascular disease, gastroesophageal reflux,16 psychological disorders (eg, depression, anxiety, and other behavioral issues), and persistent systemic inflammation.17 3. Behavioral/lifestyle treatable traits, including smoking and other exposures (eg, biomass fuel, occupational hazards), allergen/pollutant exposure, polypharmacy of inhaler devices, poor treatment adherence, incorrect inhalation techniques, and inadequate family and social support. Our findings suggest that anemia may represent an additional treatable trait in COPD, and its intervention could play a crucial role in improving patient prognosis.
Several previous studies support the notion that anemia may be a treatable trait in COPD. Garcia-Pachon et al18 investigated 125 hospitalized patients with acute exacerbations of COPD (AECOPD) and found that anemic patients had significantly higher mortality risks at 1-year, 3-year, and study termination compared to non-anemic patients, with adjusted hazard ratios (HRs) of 5.20, 4.30, and 3.80, respectively. Their study identified anemia as an independent predictor of mortality in COPD patients, though further stratified analyses were not conducted. Liu et al3 reported that the HGB-to-red cell distribution width ratio (HRR) was inversely associated with mortality (HR = 0.14). In a single-center retrospective study of severe COPD patients with chronic respiratory failure requiring home noninvasive positive-pressure ventilation and long-term oxygen therapy, higher HGB levels were associated with better survival, with optimal cutoff values identified as 14.3 g/dL for women and 15.1 g/dL for men.19 Chambellan et al,20 in a large cohort of severe COPD patients receiving long-term oxygen therapy, observed that low hematocrit was not uncommon and was associated with higher mortality and morbidity. Among COPD patients treated for acute respiratory failure, 18% had anemia, which was linked to increased 90-day mortality.21 A prospective cohort study22 involving 683 stable COPD outpatients from US Veterans Affairs pulmonary clinics found that anemic patients had significantly worse dyspnea scores, 6-minute walk distances, and survival times compared to non-anemic patients, though anemia was not an independent predictor of mortality. Balasubramanian et al,23 in a cross-sectional study of 2539 COPD patients from the COPDGene project, reported that anemia was associated with worsened symptoms, reduced quality of life, decreased exercise tolerance, and increased exacerbation risk, though no significant association was found between HGB levels and clinical outcomes, and mortality was not assessed. If future research confirms a causal relationship, several therapeutic strategies could be considered: iron supplementation, erythropoiesis-stimulating agents, and multimodal interventions encompassing nutritional support, treatment of systemic inflammation, and management of comorbidities, which may synergistically improve anemia and overall outcomes.
The reported prevalence of anemia in COPD patients ranges from 7.5% to 34%.24 Anemia of chronic disease is the most common type in COPD, followed by iron-deficiency anemia, both of which are linked to chronic systemic inflammation and impaired iron utilization.25 Elevated inflammatory cytokines (eg, TNF-α, IL-6, IL-8) contribute to erythropoietin (EPO) resistance, leading to insufficient erythropoiesis despite elevated EPO levels.26 Iron, a cofactor for many immune-related enzymes, plays a critical role in immune function; iron deficiency may impair immune responses and increase infection risk in COPD patients. Anemia may contribute to impaired oxygen delivery and an earlier onset of anaerobic metabolism, increasing ventilatory drive. Additionally, hemic hypoxia exacerbates oxidative stress.27 Since COPD patients already exhibit reduced exercise tolerance, anemia further compromises systemic oxygen supply,28 impairing organ function—particularly in the heart and muscles. Increased cardiac workload may lead to complications such as heart failure, further elevating mortality risk. Respiratory muscle fatigue may also worsen respiratory failure. These mechanisms may explain the association between anemia and increased mortality in COPD patients.
Secondary polycythemia (defined as HGB ≥17 g/dL in men and ≥15 g/dL in women) is another common complication in COPD. Elevated blood viscosity in these patients may contribute to pulmonary hypertension, increased right heart strain, and higher thromboembolic risk,29 potentially worsening prognosis. In the COPDGene cohort, 9.2% of men and 3.5% of women had secondary polycythemia.30 Our study included a few such patients, precluding survival comparisons.
This study leverages the NHANES database, ensuring representative sampling and reliable longitudinal follow-up (mean follow-up ~10 years), providing high-quality evidence for the long-term association between HGB and mortality risk. We employed a multidimensional modeling approach: after initial trend identification via quartile stratification, we used generalized additive models (GAMs) to validate nonlinear associations and applied recursive algorithms to precisely identify an inflection point (14.2 g/dL), overcoming limitations of traditional linear assumptions. Furthermore, progressive adjustment for confounders (demographics, smoking history, metabolic diseases) and stratified interaction analyses minimized bias while revealing heterogeneity in risk associations. Strict exclusion of individuals with missing key variables ensured data integrity.
Several limitations warrant careful consideration in interpreting our findings. First, the exclusion of participants with missing data on HGB, BMI, waist circumference, or mortality outcomes may introduce selection bias. The inherent constraints of NHANES data precluded incorporation of pulmonary function measures, thereby limiting our ability to adjust for COPD severity. While self-reported COPD diagnosis is a well-established method in large population-based studies, it may introduce potential misclassification bias compared to spirometry-confirmed diagnoses. This approach could lead to inclusion of some non-COPD individuals or exclusion of undiagnosed cases, potentially attenuating the observed associations toward the null. Secondly, while our large sample size enhances internal validity, the exclusively US-derived population raises questions about generalizability to other ethnic groups (particularly Asian or African populations) and healthcare systems. Moreover, although we implemented rigorous multivariable adjustment for demographic and clinical confounders, residual confounding from unmeasured variables (such as medication use patterns or undocumented comorbidities) remains possible. Finally, the single-timepoint HGB measurement at baseline inherently restricts our capacity to evaluate the prognostic significance of temporal HGB fluctuations. The absence of detailed anemia subclassification data (eg, iron deficiency versus anemia of chronic disease) represents a missed opportunity to explore potentially differential mortality associations across anemia etiologies.
This observed trajectory supports the potential clinical utility of monitoring and managing HGB levels within the identified optimal range for improving outcomes in real-world COPD patient care. However, the translation of these findings into practice must be preceded by robust interventional trials to establish efficacy and safety. Future studies should also explore interactions between HGB and other treatable traits and examine the generalizability of these results across diverse populations and healthcare systems.
Conclusion
This study reveals a nonlinear association between hemoglobin levels and all-cause mortality in COPD patients, identifying 14.2 g/dL as a critical threshold. These findings support the inclusion of anemia within the “treatable traits” framework for COPD management. While subgroup trends were observed, interaction tests did not show significant effect modification. Future intervention studies are needed to confirm whether hemoglobin correction improves survival. Clinically, particular attention should be given to patients with hemoglobin levels below 14.2 g/dL, especially older males, smokers, and those with comorbid cardiovascular disease. Generalizability may be limited by the U.S.-based cohort, and further validation in diverse populations is recommended.
Funding
This study was funded by the Zhejiang Small yet Strong Unit for COPD Respiratory Failure, China.
Disclosure
The authors declare that they have no competing interests.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 report) 2024-11-12 2024. Available from: https://goldcopd.org/2025-gold-report/.
2. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
3. Liu S, Zhang H, Zhu P, Chen S, Lan Z. Predictive role of red blood cell distribution width and hemoglobin-to-red blood cell distribution width ratio for mortality in patients with COPD: evidence from NHANES 1999-2018. BMC Pulm Med. 2024;24(1):413. doi:10.1186/s12890-024-03229-w
4. Lan CC, Su WL, Yang MC, Chen SY, Wu YK. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011-2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
5. Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
6. Hasegawa T, Zhao J, Fuller DS, et al. Erythropoietin hyporesponsiveness in dialysis patients: possible role of statins. Am J Nephrol. 2017;46(1):11–17. doi:10.1159/000477217
7. Razi O, Mohammadi M, Zamani N, et al. Walking exercise and lower-body blood flow restriction: effects on systemic inflammation, lipid profiles and hematological indices in overweight middle-aged males. Res Sports Med. 2022;30(1):41–49. doi:10.1080/15438627.2021.1888100
8. Nakamura A, Kasamatsu N, Hashizume I, et al. Effects of hemoglobin on pulmonary arterial pressure and pulmonary vascular resistance in patients with chronic emphysema. Respiration. 2000;67(5):502–506. doi:10.1159/000067463
9. Samareh Fekri M, Torabi M, Azizi Shoul S, Mirzaee M. Prevalence and predictors associated with severe pulmonary hypertension in COPD. Am J Emerg Med. 2018;36(2):277–280. doi:10.1016/j.ajem.2017.08.014
10. Xu L, Chen Y, Xie Z, et al. High hemoglobin is associated with increased in-hospital death in patients with chronic obstructive pulmonary disease and chronic kidney disease: a retrospective multicenter population-based study. BMC Pulm Med. 2019;19(1):174. doi:10.1186/s12890-019-0933-4
11. Takizawa A, Shimada T, Chubachi S, et al. Exploring the pathophysiology of anemia in COPD: insights from chest CT and longitudinal clinical data. Respir Med. 2025;240:108046. doi:10.1016/j.rmed.2025.108046
12. Park SC, Kim YS, Kang YA, et al. Hemoglobin and mortality in patients with COPD: a nationwide population-based cohort study. Int J Chron Obstruct Pulmon Dis. 2018;13:1599–1605. doi:10.2147/COPD.S159249
13. Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
14. Wagener AH, de Nijs SB, Lutter R, et al. External validation of blood eosinophils, FE(NO) and serum periostin as surrogates for sputum eosinophils in asthma. Thorax. 2015;70(2):115–120. doi:10.1136/thoraxjnl-2014-205634
15. Morice AH, Millqvist E, Belvisi MG, et al. Expert opinion on the cough hypersensitivity syndrome in respiratory medicine. Eur Respir J. 2014;44(5):1132–1148. doi:10.1183/09031936.00218613
16. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
17. McDonald VM, Higgins I, Wood LG, Gibson PG. Multidimensional assessment and tailored interventions for COPD: respiratory utopia or common sense? Thorax. 2013;68(7):691–694. doi:10.1136/thoraxjnl-2012-202646
18. Garcia-Pachon E, Padilla-Navas I. The impact of anemia on long-term mortality in hospitalized patients with exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:2229–2237. doi:10.2147/COPD.S469627
19. Kollert F, Tippelt A, Müller C, et al. Hemoglobin levels above anemia thresholds are maximally predictive for long-term survival in COPD with chronic respiratory failure. Respir Care. 2013;58(7):1204–1212. doi:10.4187/respcare.01961
20. Chambellan A, Chailleux E, Similowski T. Prognostic value of the hematocrit in patients with severe COPD receiving long-term oxygen therapy. Chest. 2005;128(3):1201–1208. doi:10.1378/chest.128.3.1201
21. Rasmussen L, Christensen S, Lenler-Petersen P, Johnsen SP. Anemia and 90-day mortality in COPD patients requiring invasive mechanical ventilation. Clin Epidemiol. 2010;3:1–5. doi:10.2147/CLEP.S12885
22. Cote C, Zilberberg MD, Mody SH, Dordelly LJ, Celli B. Haemoglobin level and its clinical impact in a cohort of patients with COPD. Eur Respir J. 2007;29(5):923–929. doi:10.1183/09031936.00137106
23. Balasubramanian A, Henderson RJ, Putcha N, et al. Haemoglobin as a biomarker for clinical outcomes in chronic obstructive pulmonary disease. ERJ Open Res. 2021;7(3). doi:10.1183/23120541.00068-2021
24. Yohannes AM, Ershler WB. Anemia in COPD: a systematic review of the prevalence, quality of life, and mortality. Respir Care. 2011;56(5):644–652. doi:10.4187/respcare.01002
25. Vasquez A, Logomarsino JV. Anemia in chronic obstructive pulmonary disease and the potential role of iron deficiency. COPD. 2016;13(1):100–109. doi:10.3109/15412555.2015.1043519
26. Tsantes A, Tassiopoulos S, Papadhimitriou SI, et al. Suboptimal erythropoietic response to hypoxemia in idiopathic pulmonary fibrosis. Chest. 2003;124(2):548–553. doi:10.1378/chest.124.2.548
27. Similowski T, Agustí A, MacNee W, Schönhofer B. The potential impact of anaemia of chronic disease in COPD. Eur Respir J. 2006;27(2):390–396. doi:10.1183/09031936.06.00143704
28. Schönhofer B, Wenzel M, Geibel M, Köhler D. Blood transfusion and lung function in chronically anemic patients with severe chronic obstructive pulmonary disease. Crit Care Med. 1998;26(11):1824–1828. doi:10.1097/00003246-199811000-00022
29. Li J, Xiong Y, Li S, et al. Prevalence and risk factors of pulmonary embolism in COPD patients complicated with secondary polycythemia. Int J Chron Obstruct Pulmon Dis. 2024;19:2371–2385. doi:10.2147/COPD.S481905
30. Zhang J, DeMeo DL, Silverman EK, et al. Secondary polycythemia in chronic obstructive pulmonary disease: prevalence and risk factors. BMC Pulm Med. 2021;21(1):235. doi:10.1186/s12890-021-01585-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Six-Minute Walking Test and 30 Seconds Chair-Stand-Test as Predictors of Mortality in COPD – A Cohort Study
Höglund J, Boström C, Sundh J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2461-2469
Published Date: 4 October 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023
Can Treatable Traits Be the Approach to Addressing the Complexity and Heterogeneity of COPD?
Cazzola M, Rogliani P, Blasi F
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1959-1964
Published Date: 8 September 2023
Respiratory Infection Triggering Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:555-565
Published Date: 27 February 2024