Back to Journals » International Journal of General Medicine » Volume 14
Hematopoietic Stem-Cell Transplantation versus Immunosuppressive Therapy in Patients with Adult Acquired Severe Aplastic Anemia: A Cost-Effectiveness Analysis
Authors Zhang MX, Wang Q, Wang XQ
Received 12 March 2021
Accepted for publication 24 June 2021
Published 15 July 2021 Volume 2021:14 Pages 3529—3537
DOI https://doi.org/10.2147/IJGM.S310844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Meng-Xue Zhang,* Qian Wang,* Xiao-Qin Wang
Department of Hematology, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Qin Wang
Department of Hematology, Huashan Hospital, No. 12, Urumqi Middle Road, Shanghai, 200040, People’s Republic of China
Tel +86-21-52887102
Email [email protected]
Objective: Controversy remains regarding which therapy to initially select for severe aplastic anemia (SAA) patients aged 35– 50. This cost-effectiveness analysis aimed to use the Markov model to compare immunosuppressive therapy (IST) with hematopoietic stem-cell transplantation (HSCT) in age-stratified patients with SAA.
Methods: A cost-effectiveness analysis using a Markov model compared IST with HSCT in age-stratified patients with SAA. Baseline data were derived from a systematic literature review and collected from Huashan Hospital, Fudan University. The primary outcome was an incremental cost-effectiveness ratio (ICER).
Results: The HSCT strategy dominated in patients aged 18– 35 even though it was $146,970 more expensive than IST, and the ICER of HSCT to IST was $14,054.19/quality-adjusted life-year (QALY), which was less than the willingness-to-pay value of $25,397.57/QALY. The IST strategy dominated in patients aged 35– 50, because it was $72,009 less expensive than HSCT and yielded 3.24 QALYs more than HSCT. The model was vigorous in the sensitivity analyses of the key variables tested through the plausible ranges that were acquired from costing sources and previously published literature.
Conclusion: The preferred induction strategy for patients aged 18– 35 with SAA appears to be HSCT, and the preferred strategy for patients aged 35– 50 is IST, which minimizes costs while maximizing QALYs.
Keywords: severe aplastic anemia, hematopoietic stem cell transplantation, immunosuppressive therapy, cost-effectiveness, quality-adjusted life years
Introduction
Aplastic anemia (AA) is an immune-mediated disease involving hematopoietic failure.1 Severe aplastic anemia (SAA) progresses rapidly and has a high mortality. Standard frontline treatment for SAA patients is either hematopoietic stem-cell transplantation (HSCT) or immunosuppressive therapy (IST).
Acquired SAA is considered to result from the immune-mediated destruction of hematopoietic cells, and therefore, HSCT may essentially cure the disease. The overall survival rate of SAA patients receiving HSCT decreases with age due to the increasing possibility of graft failure and graft-versus-host disease (GVHD).2 The European Hematopoietic Stem Cell Transplantation Center guidelines state that sibling HSCT is the first choice of treatment for adolescent and young adult SAA patients and that patients between the ages of 35 and 50 should be carefully assessed for complications after transplantation. The long-term cure rate of human leukocyte antigen (HLA)-matched HSCT has reached 75–80% in recent years.3 The first-line treatment should be HSCT if patients under 35 have HLA-matched related donors. The upper age limit for HSCT as a first-line therapy remains controversial because the results vary extensively in diverse clinical studies. The British Committee for Standards in Haematology recommends an age limit of 50 for the use of HLA-contracted cell donor HSCT, and patients aged 35–50 need to be carefully assessed for comorbidities before deciding whether they are suitable for transplantation.4
IST suppresses immune function to reduce abnormal immune responses. The current standard IST first-line therapy is antithymocyte globulin (ATG) combined with cyclosporine (CSA), and age is not a limiting factor;5 however, a patient’s age remains a strong predictor of response and survival.6 In a randomized study, rabbit ATG was found to be inferior to horse ATG as a first treatment for SAA, as indicated by the hematologic response and survival.7 The thrombopoietin receptor agonist, eltrombopag, has shown significant activity as a single agent in the treatment of refractory patients with hematologic response rates of 40% to 50%.8 In a phase-2 trial, the addition of eltrombopag to standard IST was declared to be well tolerated and resulted in similar responses.9 However, there should be a prospective randomized trial of first-line therapy that compares IST with IST plus eltrombopag.10 IST is indicated for non-severe AA with blood transfusion dependence, minors lacking HLA-matched related donors, SAA patients with HLA-matched related donors aged >35, and patients aged >50.11 The overall survival rate with IST is generally high, with a 5-year survival rate of 60%–85%.12 There is no upper age limit for IST, but the mortality rates for patients over 60 are higher. IST does not cure SAA, and there are three major adverse consequences: no response, relapse, and clonal evolution.
HSCT offers the best chance of treatment, but it is costly and limited by the incidence of GVHD. The priority order of donor source for bone marrow transplantation is as follows: (1) HLA identical sibling, (2) HLA-matched unrelated donor, and (3) HLA-haploidentical donor if an HLA-matched unrelated donor is not rapidly available.13,14 The haplo-HSCT group has a lower incidence of secondary graft failure but higher incidence of acute GVHD and chronic GVHD.15 Post-transplantation cyclophosphamide as the sole GVHD prophylaxis is associated with low rates of acute and chronic GVHD in patients undergoing a peripheral blood stem-cell (PBSC) transplant for SAA using HLA-matched donors.16 Age at transplantation is not associated with survival, but grade II–IV acute GVHD risks are higher for patients aged 65 years or older. Also, chronic GVHD is lower with the GVHD prophylaxis regimens calcineurin inhibitor (CNI) + methotrexate and CNI alone or other agents compared with CNI + mycophenolate.17 Survival has remained unchanged in the past 15 years in patients with SAA over 40 undergoing an allogeneic HSCT. This is also true when correcting for confounding variables, such as a patient’s age, donor type, and in-vivo T-cell depletion compared with the total ATG patient population.18
IST is a first-line therapy that can induce a response in up to 75% of patients,19 but it also has a high relapse rate and can cause secondary clonal diseases, especially in young SAA patients. Therefore, the choice of treatment for patients aged 35–50 with SAA is clinically controversial. This study used clinical economics to compare the cost-effectiveness of two treatments for patients aged 35–50 with SAA and for a group of 18–35-year-old SAA patients simultaneously. This study also attempted to provide an objective reference for the clinical selection of treatment methods and to investigate the price threshold of the prioritized method, thereby decreasing patients’ medical expenses and improving the quality-adjusted life years (QALYs).
Methods
Patients
This study enrolled adult patients who had been diagnosed with SAA for the first time and had not received IST or HSCT. The study population was consistent with that of the literature on probabilistic sources. The age distribution of the patients was mostly concentrated in the range of 18–50. The patients were divided into two groups, the 18–35-year-old group and 35–50-year-old group, for analysis. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Huashan Hospital. Written informed consent was obtained from all participants.
The Structure of the Model
A Markov model was established for two interventions based on the relevant literature and clinical practice to perform a cost-effectiveness analysis of IST and HSCT for SAA. The incremental cost-effectiveness ratio (ICER) was the principal evaluation index. If the ICER is less than a certain threshold, the therapy is cost-effective; otherwise, it is not. The ICER threshold is conveyed as the willingness to pay (WTP), which reflects the economic burden of the patient’s willingness to bear a QALY for treating the disease. We typically used gross domestic product (GDP) per capita for comparison: if ICER < GDP per capita, the increased cost was completely worthwhile, and the therapy was cost-effective; if per capita GDP < ICER < 3 times per capita GDP, the increased cost was acceptable and the therapy was cost-effective; if ICER > 3 times per capita GDP, the added cost was not worthwhile, and the therapy was not cost-effective. Therefore, the WTP value of this study was set to three times the Chinese GDP per capita ($25,397.57).
We used TreeAge Pro 2011 software to build the Markov model to assess the cost-effectiveness of the two options. TreeAge Pro 2014 software is a professional analysis software for building decision trees and Markov models. Two cost-effectiveness analysis models (Figure 1A and B) with five states were created based on the relevant guidelines and clinical practice of IST and HSCT for SAA. These models intuitively reflect the mutual transformation association between the states. Patients that choose HSCT may be in one of five states of “healing/death/ineffective (still SAA)/short-term complications/long-term complications” during the first cycle (after treatment) and transitioning to other states in the second and subsequent cycles. Similarly, patients that choose IST may be in one of five states of “CR/PR/death/invalid (still SAA)/serious complications” in the first cycle (after treatment) and transition to other states in the second and subsequent cycles. The state of death cannot be transformed into any other state and is also known as the absorbing state. Transitions between several other states have different probabilities, and different states necessitate different medical costs. Each patient can only be in one state in any one cycle. The model cycle of both scenarios was set to 6 months. The model was run for 30 years (at which point most patients had died) to reflect the natural outcome of the disease and the life expectancy of the study population.
 |
Figure 1 The transitions between different states of the Markov model HSCT on the left (A) and IST on the right (B) and incremental-effectiveness scatter plot for (C) the 18–35 age group and (D) the 35–50 age group. Abbreviations: CR, complete remission; PR, partial remission; SAA, severe aplastic anemia. |
Data
The probability of conversion between the different states of the model was derived from an extensive literature search. The inclusion criteria were as follows: (1) the study time ranged from January 1, 1980, to August 1, 2018; (2) a research sample for the initial diagnosis of AA; (3) a sample population that had not received IST/HSCT treatment before; (4) total sample size >30 cases; and (5) studies dividing the sample population into HSCT and IST groups for comparison. HSCT included HLA-matched sibling transplantation, unrelated donor transplantation, and alternative donor HSCT. The exclusion criteria were as follows: (1) a study time frame that was earlier than January 1, 1980; (2) study-sample age range of <18 years; (3) total study-sample size of <30 cases; and (4) a sample population that had previously received HSCT/IST treatment. Accounting for expert advice and making certain assumptions based on the existing literature and clinical guidelines, we arranged the baseline value of the possibilities (Table 1).
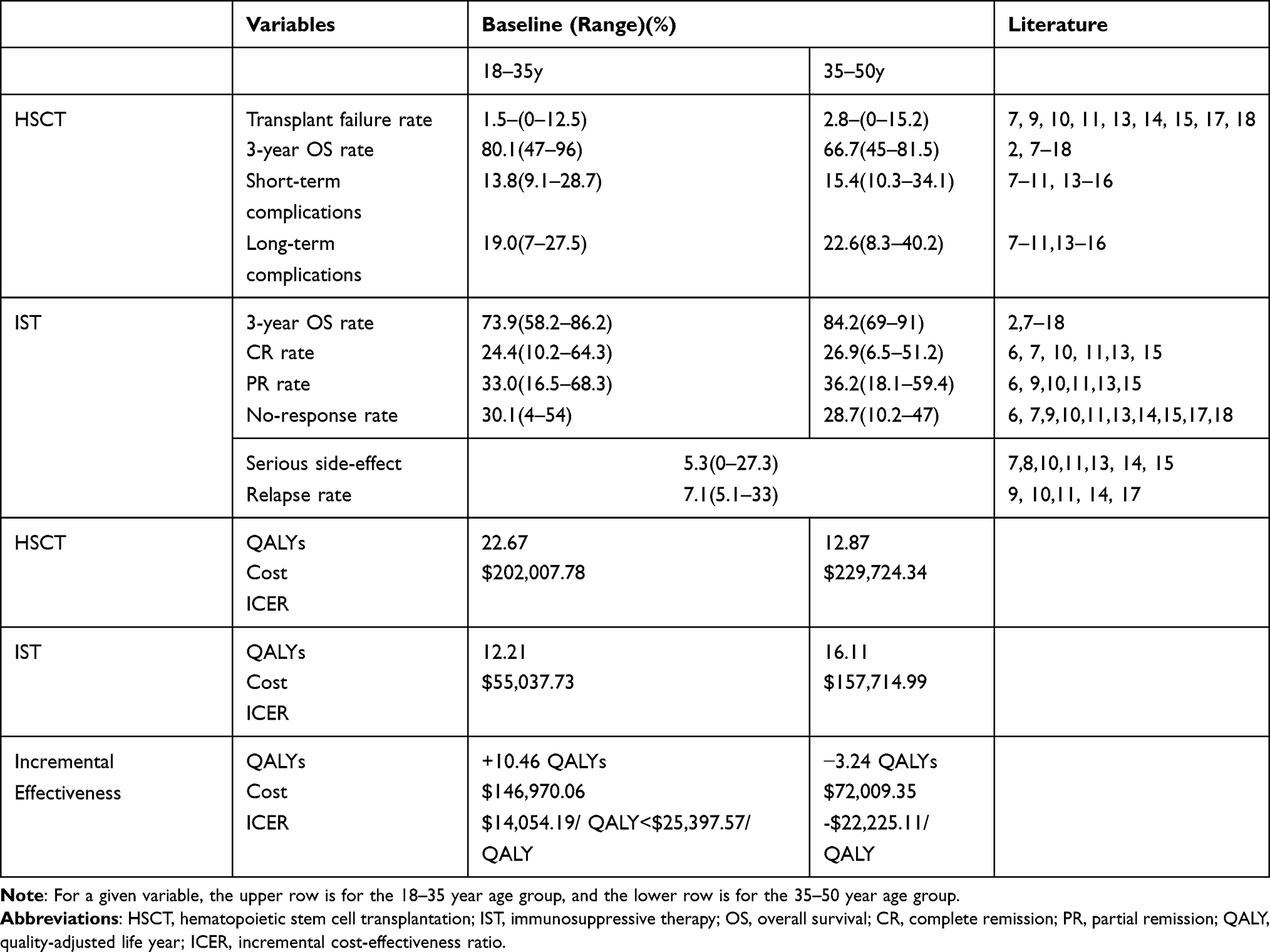 |
Table 1 Baseline Value of the Possibilities of HSCT and IST and Primary Outcomes of QALYs |
Cost
This study only considered direct medical costs from the perspective of China’s healthcare system. Based on the International Classification of Diseases (Tenth Revision) Code, patients over 18 years old admitted to Huashan Hospital, Fudan University, between January 1, 2009, and January 1, 2019, were selected according to their diagnosis. The screening conditions were limited to the first diagnosis of SAA in patients. The treatment cost and follow-up cost were calculated, and expert advice was consulted. We used the calculated median cost in the baseline analysis, and indirect costs, such as loss of labor capacity, were not included in this study (Table 2).
 |
Table 2 The Main Cost of the Treatment for SAA |
The health utility value is the weight of a certain health state comparative to the total health state. It is an index for assessing the satisfaction degree of a certain health condition and is a comprehensive index showing the health status of the individual. The values range from 0–1; death is scored as 0, while complete health is scored as 1. The health utility values used in this study were derived from the expert opinion: CR and survival with no complications were fundamentally equivalent to a complete health status, and consequently, their health utility value was 1. PR had a slightly lower health utility value of 0.9, while the health utility value of short-term complications and long-term complications was 0.5 and 0.6, respectively. The quality of life in patients with SAA and severe complications was greatly affected and had a health utility value of 0.3, and the health utility value of death was 0. Discounting is the process of converting the cost and health outcomes incurred at different times (years) into cost and health outcomes at the same “time point” at a certain interest rate. A 3% discount rate was used in this study.
This study used QALYs to evaluate the health outcomes of the two groups, referred to as the “effects” in the cost-effectiveness analysis. One QALY is equal to the expected life of the model simulation multiplied by the health utility value during that time.
All procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Results
Cost-Effectiveness Analysis
The 18–35 group and the 35–50 group generated very different conclusions based on the results of the 30-year simulation (Table 1). For the 18–35 group, HSCT had a QALY increment of 10.46 QALYs relative to IST, with a cost increase of $146,970.06 and an ICER of $14,054.19/QALY, which was less than the WTP value of $25,397.57. Therefore, the choice of HSCT was more cost-effective than IST for the 18–35 population. However, for the 35–50 group, the HSCT group’s QALY increment relative to the IST group was −3.24 QALYs, and the cost increase was $72,009.35. Therefore, HSCT was not a cost-effective option, while IST was a more cost-effective option for the 18–35 group.
According to the baseline examination of the Markov cohort simulation, there was always a large gap between the total cost of HSCT and IST, even with the extension of the follow-up period for the 18–35 group, but the increased effect of HSCT to IST (QALY) continued to grow. Therefore, the ratio of the cost difference to effect difference became progressively smaller (Table 3). As time elapsed, HSCT’s relatively high health resource input showed a better cost-effectiveness advantage. In the 35–50 group, the cost of IST was always lower and the QALYs were always greater, so IST always had an absolute advantage (Table 3).
 |
Table 3 Baseline Analysis of the Markov Cohort Simulation |
Probabilistic Sensitivity Analysis
The probabilistic sensitivity analysis assesses the influence of all model parameters on the analysis results by altering all the set model parameters at the same time. The analysis follows the standard of the Monte Carlo simulation, in which the individual can transfer to different states in each cycle according to the transition probability between states. The results are demonstrated in the incremental cost-effectiveness scatter plots (Figure 1C and D) through the simulation of a large number of cohort samples (the probability sensitivity analysis of this study for a Monte Carlo simulation of 1,000 sample sizes). The dotted line in the figure is the WTP threshold line, and the ICER results are distributed on either side of the threshold line. As seen in the figure, with a threshold of WTP = $25,397 in 65.9% of cases in the 18–35 group, HSCT was more cost-effective, and in 63.3% of cases in the 35–50 group, IST was more cost-effective.
Threshold Analysis
The threshold analysis evaluates when the cost-effectiveness optimal decision is altered to another scheme by changing the variables of the Markov model according to the probability range of the model. The examination (Table 4) showed that, for the 18–35 group, when the cost of transplantation was no higher than $129,714.29, HSCT was more cost-effective than IST and was the preferred treatment method from the perspective of health economics. Even if the cost of IST was reduced to 0, HSCT still had an advantage. However, when the transplant failure rate was as high as 18.6%, the mortality rate reached 41.2% within half a year after a successful transplant, or the IST no-response rate decreased to 1.36% the ideal decision became IST. For the 35–50 group, the cost of transplantation, failure rate of transplantation, and change in mortality during the half-year after transplantation did not change IST as the preferred treatment, but when the cost of IST increased to $89,147, the IST no-response rate reached 57.37%, or the relapse rate within half a year reached 46.84% the ideal decision changed to HSCT. This model is not sensitive to variations in utility values and discount rates.
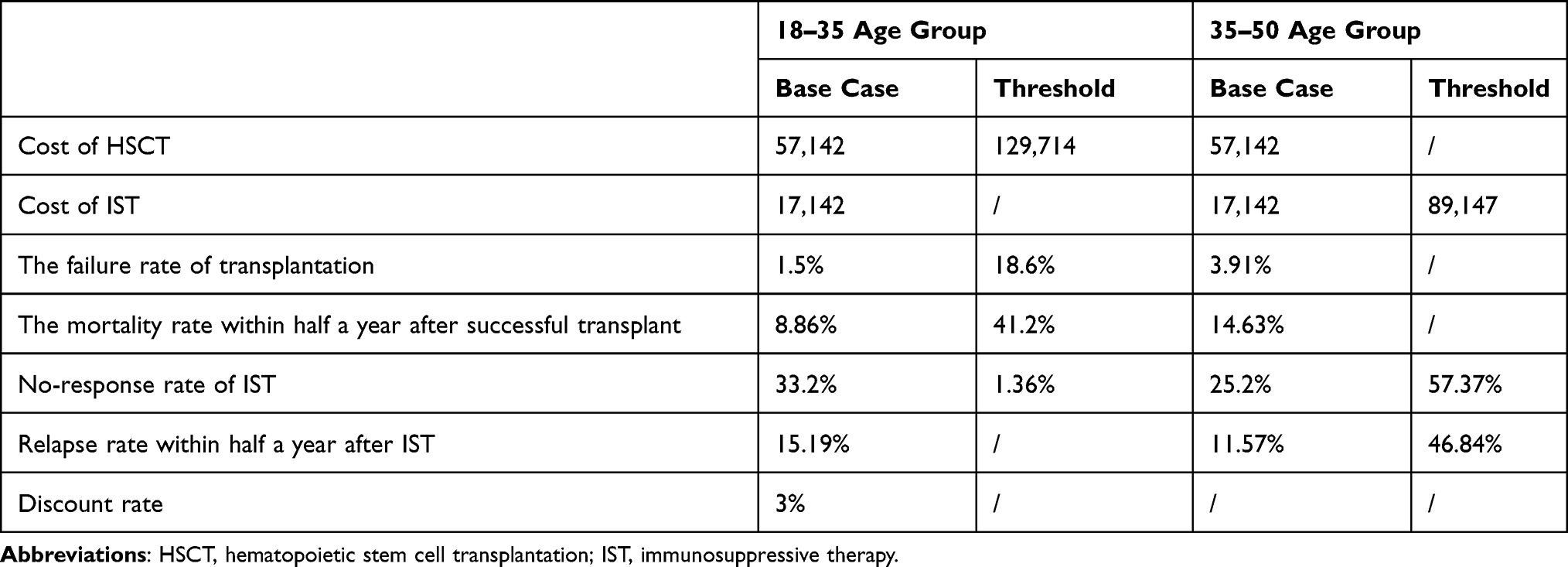 |
Table 4 Sensitivity Analyses for Age-Stratified Groups |
Discussion
IST and HSCT have been extensively approved in the treatment of SAA.20,21 The long-term survival rate of SAA patients has been significantly improved in recent years, but the two treatment methods have diverse limitations.22 IST does not cure SAA, it only allows patients to achieve complete or partial remission, and it may have three major adverse consequences: no response, relapse, and clonal evolution. HSCT costs more and is limited by the source of donors and acute and chronic GVHD.23 The current guidelines recommend that sibling HSCT is the treatment of choice for adolescent and young adult SAA patients, but the choice of treatment options for SAA patients aged 35–50 is clinically controversial, and there are no concise recommendations.
From the perspective of clinical economics, this study took the main factors, such as age, cost, and effect, into account to create a Markov model for a comprehensive analysis and to draw conclusions on the choice of treatment options. For patients aged 18–35 with SAA, HSCT is recommended given China’s current GDP. The cost of obtaining QALY is $14,054.19, which is less than the WTP value of $25,397.57, indicating that patients obtain more QALYs under an acceptable direct cost input. For patients aged 35–50 with SAA, the recommended option is IST, with more QALYs and a lower direct cost input. This conclusion was corroborated by the sensitivity analysis, and the same conclusion was attained using a Monte Carlo simulation to simulate 1,000 samples. We found that when the treatment cost doubles or the transplant failure rate, mortality, or IST relapse rate changes by more than five times the conclusion can be changed by adjusting different variables, which once again proves the conclusion of this study. If we can decrease the total cost of a particular treatment, we can achieve a better ICER and improve the efficiency of the health care provided. Similarly, increasing the success rate of a particular treatment and reducing the relapse rate are key methods for increased cost-effectiveness.
Previous comparisons of treatments for SAA have focused on outcomes such as the success/remission rate, overall survival rate, relapse rate, and event-free-survival rate.24 There are numerous studies comparing the outcomes of diverse treatments for different age groups, but there is no comparison of the cost-effectiveness of the treatments for SAA, and economic factors have not been included in these considerations.21,25–27 This study is the first cost-effectiveness analysis of SAA treatments. For patients with SAA that find it difficult to choose between the two main treatment methods, a cost-effectiveness analysis was performed on a younger patient group and an older patient group. It is concluded that HSCT is the first choice for younger patients and IST is preferred for older patients, which has great guiding value for clinical practice. The same applies in the US, age=40 is used as the cutoff for matched sibling HSCT up front for adults. Adults<40 do proceed to HSCT; adults >40 proceed to IST.28
It is also important to evaluate the treatment effect when assessing the effectiveness of a treatment regimen as well as to evaluate the cost of treatment and the cost of adverse events. For patients and the government, economic factors are very important and cannot be ignored. Often, clinicians pay more attention to the assessment of clinical effects, and it is easy to overlook the evaluation of adverse events or costs.29,30 A clinical decision made this way may have certain biases, but adverse events and costs are also significant factors to consider in clinical decision-making.31 For example, a cost-effectiveness evaluation of primary central nervous system lymphoma (PCNSL) treatment in 201232 concluded that young patients that selected high-dose methotrexate (MTX) chemotherapy combined with radiation therapy reduced their costs and improved their QALYs, and patients over the age of 60 were more suitable for chemotherapy because the cost of chemotherapy alone for the elderly was lower, while the QALYs acquired by the two treatment options were almost the same. This study provided suggestions with comprehensive considerations to help PCNSL patients choose a treatment option. In patients with SAA, the incidence and severity of adverse events associated with IST compared with those of HSCT greatly differ and the resulting costs are also very different. Consequently, this study takes both the effect of treatment and the direct costs of treatment into consideration.
There are some limitations to this study. First, the model assumes that the transition probabilities are equal in each cycle, but the transition probability may change over time. Also, HSCT requires informed consent from donors and recipients prior to treatment. Therefore, no randomized controlled trials have been completed to investigate this problem, so we selected high-quality studies with other designs that met the inclusion criteria as sources of data and performed a sensitivity analysis to recognize reliable sources. The health utility value parameters used in the models were also derived from expert advice and may not accurately reflect the patient’s quality of life because health utility values have not received sufficient attention and lack accurate and credible data sources.
Despite these limitations, this study investigated the cost-effectiveness of the two main treatments for SAA diagnosed for the first time, which can address a controversial area in SAA treatment and explore differences in treatment options across diverse age ranges. This study also confirmed that the most cost-effective choice for SAA patients aged 18–35 is HSCT, and IST is preferable for patients aged 35–50 because it maximizes QALYs while minimizing costs. The results of this study can provide significant reference information for clinicians and SAA patients.
Funding
This work was supported in part by grants from Shanghai Municipal Science and Technology Commission (#16ZR1404400).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Young NS, Longo DL. Aplastic anemia. N Engl J Med. 2018;379(17):1643–1656. doi:10.1056/NEJMra1413485
2. Gupta V, Eapen M, Brazauskas R, et al. Impact of age on outcomes after bone marrow transplantation for acquired aplastic anemia using HLA-matched sibling donors. Haematologica. 2010;95(12):2119–2125. doi:10.3324/haematol.2010.026682
3. Passweg JR, Marsh JCW. Aplastic anemia: first-line treatment by immunosuppression and sibling marrow transplantation. Hematology. 2010;2010(1):36–42. doi:10.1182/asheducation-2010.1.36
4. Dufour C, Paul V, Elisa C, et al. Similar outcome of upfront-unrelated and matched sibling stem cell transplantation in idiopathic paediatric aplastic anaemia. A study on behalf of the UK Paediatric BMT Working Party, Paediatric Diseases Working Party and Severe Aplastic Anaemia Working Party of EBMT. Br J Haematol. 2015;171(4):585–594.
5. Contejean A, Resche-Rigon M, Tamburini J, et al. Aplastic anemia in the elderly: a nationwide survey on behalf of the French reference center for aplastic anemia. Haematologica. 2019;104(2):256–262. doi:10.3324/haematol.2018.198440
6. Bacigalupo A, Oneto R, Schrezenmeier H, et al. First line treatment of aplastic anemia with thymoglobuline in Europe and Asia: outcome of 955 patients treated 2001–2012. Am J Hematol. 2018;93(5):643–648. doi:10.1002/ajh.25081
7. Scheinberg P, Nunez O, Weinstein B, et al. Horse versus rabbit antithymocyte globulin in acquired aplastic anemia. N Engl J Med. 2011;365(5):430–438. doi:10.1056/NEJMoa1103975
8. Scheinberg P. Recent advances and long-term results of medical treatment of acquired aplastic anemia. Hematol Oncol Clin North Am. 2018;32(4):609–618. doi:10.1016/j.hoc.2018.03.003
9. Assi R, Garcia-Manero G, Ravandi F, et al. Addition of eltrombopag to immunosuppressive therapy in patients with newly diagnosed aplastic anemia. Cancer. 2018;124(21):4192–4201. doi:10.1002/cncr.31658
10. Deeg HJ. More than one angle to target aplastic anemia? Cancer. 2018;124(21):4165–4167. doi:10.1002/cncr.31656
11. Killick SB, Bown N, Cavenagh J, et al. Guidelines for the diagnosis and management of adult aplastic anaemia. Br J Haematol. 2016;172(2):187–207. doi:10.1111/bjh.13853
12. Locasciulli A, Oneto R, Bacigalupo A, et al. Outcome of patients with acquired aplastic anemia given first line bone marrow transplantation or immunosuppressive treatment in the last decade: a report from the European Group for Blood and Marrow Transplantation (EBMT). Haematologica. 2007;92(1):11–18. doi:10.3324/haematol.10075
13. Bacigalupo A, Sica S. Alternative donor transplants for severe aplastic anemia: current experience. Semin Hematol. 2016;53(2):115–119. doi:10.1053/j.seminhematol.2016.01.002
14. Georges GE, Doney K, Storb R. Severe aplastic anemia: allogeneic bone marrow transplantation as first-line treatment. Blood Adv. 2018;2(15):2020–2028. doi:10.1182/bloodadvances.2018021162
15. Li Y, Duan F, Xiao H, et al. Therapeutic outcomes of haploidentical allogeneic hematopoietic stem cell transplantation in patients with severe aplastic anemia: a multicenter study. Transplantation. 2018;102(10):1724–1731. doi:10.1097/TP.0000000000002200
16. George B, Nisham PN, Devasia AJ, et al. Post-transplant cyclophosphamide as sole graft-versus-host disease prophylaxis is feasible in patients undergoing peripheral blood stem cell transplantation for severe aplastic anemia using matched sibling donors. Biol Blood Marrow Transplant. 2018;24(3):494–500. doi:10.1016/j.bbmt.2017.10.034
17. Rice C, Eikema DJ, Marsh JCW, et al. Allogeneic hematopoietic cell transplantation in patients aged 50Years or older with severe aplastic anemia. Biol Blood Marrow Transplant. 2019;25(3):488–495. doi:10.1016/j.bbmt.2018.08.029
18. Giammarco S, Peffault de latour R, Sica S, et al. Transplant outcome for patients with acquired aplastic anemia over the age of 40: has the outcome improved? Blood. 2018;131(17):1989–1992. doi:10.1182/blood-2017-09-807859
19. DeZern AE, Brodsky Robert A. Clinical management of aplastic anemia. Expert Rev Hematol. 2011;4(2):221–230. doi:10.1586/ehm.11.11
20. Kahn Q, Ellis RJ, Skikne BS, et al. A retrospective analysis of long-term survival in severe aplastic anemia patients treated with allogeneic bone marrow transplantation or immunosuppressive therapy with antithymocyte globulin and cyclosporin A at a single institution. Mil Med. 2002;167(7):541–545. doi:10.1093/milmed/167.7.541
21. Bacigalupo A, Giammarco S, Sica S. Bone marrow transplantation versus immunosuppressive therapy in patients with acquired severe aplastic anemia. Int J Hematol. 2016;104(2):168–174. doi:10.1007/s12185-016-2037-8
22. Arranz R, Otero M-J, Ramos R, et al. Clinical results in 50 multiply transfused patients with severe aplastic anemia treated with bone marrow transplantation or immunosuppressive therapy. Bone Marrow Transplant. 1994;13(4):383–387.
23. George B, Mathews V, Viswabandya A, et al. Immunosuppressive therapy and bone marrow transplantation for aplastic anaemia - the CMC experience. J Assoc Physicians India. 2015;63:36–40.
24. Ahn MJ, Choi JH, Lee YY, et al. Outcome of adult severe or very severe aplastic anemia treated with immunosuppressive therapy compared with bone marrow transplantation: multicenter trial. Int J Hematol. 2003;78(2):133–138. doi:10.1007/BF02983381
25. Doney K, Leisenring W, Storb R, et al. Primary treatment of acquired aplastic anemia: outcomes with bone marrow transplantation and immunosuppressive therapy. Ann Intern Med. 1997;126(2):107–115. doi:10.7326/0003-4819-126-2-199701150-00003
26. Viollier R, Passweg J, Gregor M, et al. Quality-adjusted survival analysis shows differences in outcome after immunosuppression or bone marrow transplantation in aplastic anemia. Ann Hematol. 2005;84(1):47–55. doi:10.1007/s00277-004-0930-3
27. Kim I, Yoon SS, Park S, et al. The treatment of severe aplastic anemia: outcomes of bone marrow transplantation and immunosuppressive therapy in a single institution of Korea. J Korean Med Sci. 2003;18(3):365–371. doi:10.3346/jkms.2003.18.3.365
28. Bacigalupo A. How I treat acquired aplastic anemia. Blood. 2017;129(11):1428–1436. doi:10.1182/blood-2016-08-693481
29. de Planque MM, Richel DJ, Fibbe WE, et al. Acquired severe aplastic anaemia in adults--a single centre study with 13 years follow-up. Neth J Med. 1990;37(3–4):103–110.
30. Peinemann F, Grouven U, Kroeger N, et al. First-line matched related donor hematopoietic stem cell transplantation compared to immunosuppressive therapy in acquired severe aplastic anemia. PLoS One. 2011;6(4):e18572. doi:10.1371/journal.pone.0018572
31. Marsh JCW. Making therapeutic decisions in adults with aplastic anemia. Hematology. 2006;2006(1):78–85. doi:10.1182/asheducation-2006.1.78
32. Prica A, Chan K, Cheung M. Combined modality therapy versus chemotherapy alone as an induction regimen for primary central nervous system lymphoma: a cost-effectiveness analysis. Neuro-Oncol. 2014;16(10):1384–1391. doi:10.1093/neuonc/nou057
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.