Back to Journals » Patient Preference and Adherence » Volume 15
Help-Seeking Preferences to Informal and Formal Source of Care for Depression: A Community-Based Study in Northwest Ethiopia
Authors Shumet S ![]() , Azale T, Abebaw DA
, Azale T, Abebaw DA ![]() , Tesfaw G
, Tesfaw G ![]() , Wondie M, Getinet Alemu W
, Wondie M, Getinet Alemu W ![]() , Amare T
, Amare T ![]() , Kassew T
, Kassew T ![]() , Mesafint G
, Mesafint G ![]()
Received 17 March 2021
Accepted for publication 11 June 2021
Published 6 July 2021 Volume 2021:15 Pages 1505—1513
DOI https://doi.org/10.2147/PPA.S311601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Shegaye Shumet,1 Telake Azale,2 Dessie Abebaw Angaw,3 Getachew Tesfaw,1 Messele Wondie,1 Wondale Getinet Alemu,1 Tadele Amare,1 Tilahun Kassew,1 Gebremeskel Mesafint4
1Department of Psychiatry, University of Gondar, Gondar, Ethiopia; 2Department of Health Education and Behavioral Science, University of Gondar, Gondar, Ethiopia; 3Department of Epidemiology and Biostatistics, University of Gondar, Gondar, Ethiopia; 4Mizan-Tapi University, College of Health Science, Department of Nursing, Mizan Aman, Ethiopia
Correspondence: Gebremeskel Mesafint
Mizan-Tapi University, College of Health Science, Department of Nursing, Mizan Aman, Ethiopia
Tel +251918209867
Email [email protected]
Background: Globally, 350 million people are suffering from depression. Many people suffering from depression use different sources of help for their problems. People with different mental health problems seek help from formal and/or informal sources. This gives crucial information on community beliefs and perception regarding their preference for help. This study helps to guide effective planning and provision of mental health services, and health policy of the country to explore the community’s preference to different sources of help.
Objective: The aim was to contrast patterns of formal and informal help-seeking preferences for depression among residents of Aykel town, Northwest Ethiopia.
Methods: This cross-sectional population-based study included 832 participants. We used a major depressive disorder case vignette and general help-seeking questionnaire (GHSQ) to assess preference to seek help. Study participants were selected by multistage cluster sampling technique. An independent sample t-test and analysis of variance test (ANOVA) was performed.
Results: A total of 656 subjects (78.8%) showed high propensity to intimate partner, and 655 (78.7%) of the study subjects had high propensity to mental health professional. The mean score of the residents’ preference to seek help from informal sources was 3.41± 0.60. The mean score of preference to seek help from formal sources was 3.18± 0.75. A total of 276 (33.2%) subjects showed high propensity to both informal and formal sources of help. The results also showed there was a mean score difference in preference for informal help between subjects with strong social support and low and moderate social support (P< 0.001).
Conclusion: The result suggests that the majority of the residents had a higher preference to seek help from informal sources than formal sources of care. Providing and strengthening both formal and informal sources of help in conjunction are crucial to get a more qualified and effective care for depressed patients.
Keywords: depression, preference to seek help, Ethiopia
Introduction
Depression is a major public health concern that affects more than 340 million people worldwide. Five mental disorders are in the top 10 leading causes of disability.1,2 Depression is one of the common mental disorders with an average prevalence of 12% globally.2 In the past 15 years, the magnitude of depression was increasing to 18.4%,1 and 40.5% of DALYs caused by mental illness accounted for depression.3 It affects all people in all age groups worldwide.4 Depression has high impact at the individual, family, and country level.2,5,6 At the individual level, depression can cause impairment in social and occupational functioning.7–9 Moreover, it increases the burden of other chronic medical illnesses such as HIV/AIDS, cardiac problems, diabetes mellitus, tuberculosis, and surgical illness.9,10 About 2.4% to 60% of life threatening illness burden in low income countries is associated with depression.11–15 The other trajectory consequences of depression are suicide8,16,17 and substance use.18,19
Early identification and intervention of depression can reduce the suffering of people, and prevent the morbidity and mortality rates of the affected individuals.20,21 It can also reduce long-term costs of mental health care service during the rehabilitation process.
As studies results have shown, there is variation among individuals in utilization and preference for mental health services.21–26 Therefore, to design appropriate planning and strengthening mental health services, it is important to know the communities’ preference to seek help and barriers that occur in the process. Despite different treatment modalities being available,27–29 nearly one half of individuals with depression seek formal help from health care1,2 professionals. Findings of earlier research revealed that the prevalence of formal help seeking behavior for depressive symptoms ranged from 33% to 55.6%.13,30,31
Socio-demographic variables such as female sex and younger age;6,32 clinical variables including co-morbid illnesses, perceived need of treatment, functional impairment, high level of depression;33,34 accessibility of the treatment;6,35 and white Americans36 were more frequently associated with help-seeking from different treatment areas.
Informal help is usually offered by friends, family, religious leaders (priests), or other non-health professionals. A study in five low and middle income countries showed that participants had higher support from informal help sources than formal help sources.5,37 Community based studies34,38 on formal and informal help preference among adults found that 55.6–63.1% of the participants preferred to seek help from informal sources such as friends and family when they were feeling “stress and depressed”. Therefore, assessing preferences of participants will help to understand and discover people’s dynamics in their choices of formal and informal help seeking for depression from different service providers. Additionally, it gives crucial information on communities’ beliefs and perception regarding their preference for help if they face depressive symptoms. In Ethiopia, there are studies on help seeking behavior for depression from health care providers12,14,19,39 and it is poorly detected by primary care clinicians.40 However, as per my knowledge there was no study which indicates the behaviors of the participants to the informal help sources. Therefore, this study considered the preference of the participants for both formal and informal help sources and this finding will help policy makers as an input to develop mental health service strategy by integrating formal and informal help sources. Because informal community health service is crucial at the initial point as a primary health care service, and people who prefer informal help sources as a first choice could be linked to the health professionals before their illnesses become worse. Thus, the purpose of this community survey was to assess preferences of Aykel town communities to formal and informal help sources for depressive symptoms in northwest Ethiopia.
Methods
Study Design and Setting
Community-based cross-sectional survey was employed between April and May 2015 at Aykel town, Northwest Ethiopia. In this town, around 18,507 residents were living. During the survey, there were two health posts, one health center and one primary hospital that provide health care services for the community in the town.
Study Participants and Sampling Procedure
A total of 832 participants were interviewed. Multi-stage cluster sampling technique was used to sample the participants. There were two kebeles in the town. The residents are huge in number with similar socio-demographic indicators in each Kebele (an administrative unit of Ethiopia, similar to a ward and consists of 5000 people). Therefore, simple random sampling (lottery method) technique was used to select one kebele. Inside this kebele, there are subdivisions of kebele to ketena. Therefore, twelve ketenas were included using lottery method. From the catchment area, 832 households were interviewed. Adult residents who age 18 years and above living in the catchment area were included for this study. Individuals with severe illness and unable to communicate were excluded from the study.
Data Collection Procedure and Tools
A structured questionnaire was used to assess the residents’ preference for informal and formal help sources, if they have depressive symptoms. It was designed through adopting from previously conducted study for mental health problems in Australia.41 The questionnaire was designed in English and was translated to Amharic, national language of Ethiopia, and back to English for its consistency. Data were collected by four trained public health professionals using the Amharic version of the questionnaire for a month. The training was given for data collectors regarding how to interview and explain unclear questions for the participants. Furthermore, they have been given awareness about ethical principles, including confidentiality/anonymity, data management and securing subjects’ informed consent for participation. All collected data were checked for completeness and consistency.
Socio demographic variables (sex, age, religion, marital status, ethnicity, educational status, and occupational status) were adopted from different literature.
Social support was measured using the Oslo 3-items social support scale with scores ranging from 3 to 14: 3–8=poor social support; 9–11= moderate social support; and 12–14=strong social support.42
General help seeking questionnaire (GHSQ) with major depressive disorder case vignette was used to measure preference for informal and formal source of help. Depression was presented for participants as a case vignette which meets Diagnostic Statistical Manual (DSM-5) criteria for major depressive disorder as shown in the Appendix. GHSQ is measured with likert type scale ranging from (1) “very unlikely” to (5) “very likely”. Participants were asked: “If you were feeling like symptoms described in the vignette, how likely it is, you would seek help from a list of people?” High scores (score of 4 or 5) for each source of help shows that a person had highest propensity to ask help; low score (≤3) indicates that the participants had low propensity to ask specific source of help.43 The mean scores of high and low propensity of each source of help were calculated. The sources of help were divided into three groups: formal help, close informal help and broad informal help. This category was adapted from an Italian study.37 The formal help group included any health professional (doctor, nurse, and public health professional), mental health professional (psychiatrist, psychologist, social worker and counselor) and traditional healers. Under the close informal help groups boyfriend, girlfriend, friend, father or mother, other relatives/family members were included. Religious related sources of help (holy water, priest), sorcerer were under the broad informal help category. In this study close informal and broad informal help category were considered as informal help sources. The sum of each source of help in the formal and informal category were computed and then divided by the number of sources of help in each category which resulted in the total score ranging from 1 to 5. The higher the score in each scale indicates the higher the likelihood that the participant prefers to seek this source of care. We have computed Cronbach’s Alpha to test the internal consistency of the scale, obtaining a score of 0.55. Cronbach Alpha indexes were also computed for each variable to test the internal consistency, and values ranged from 0.56 for the close informal help group to 0.69 for the formal help group.
Data Processing and Analysis
Data were entered in to EPI INFO 3.5.3 and then analyzed via STATA-14. Descriptive statistics (frequency, percent, mean and standard deviation) were used to summarize the data. Mean score and percentage estimate for specific informal and formal help preference were described. An independent sample T-test and analysis variance test (ANOVA) were performed to determine whether there was a difference in informal help scores between participants’ socio demographic characteristics.
Results
Personal and Socio-Economic Characteristics of the Residents
A total of 832 residents took part in the study with a response rate of 98.3%. More than half, 489 (58.8%) of the participants were males with the median age of 32 years (interquartile range= 10). Majority of the respondents, 698 (83.9%) were Orthodox Christianity, 365 (43.9%) had attended secondary education, and 243 (29.2%) of the participants were government employed workers. Nearly half, 406 (48.9%), of the respondents were single, and about 389 (46.8%) of the participants had moderate social support (Table 1).
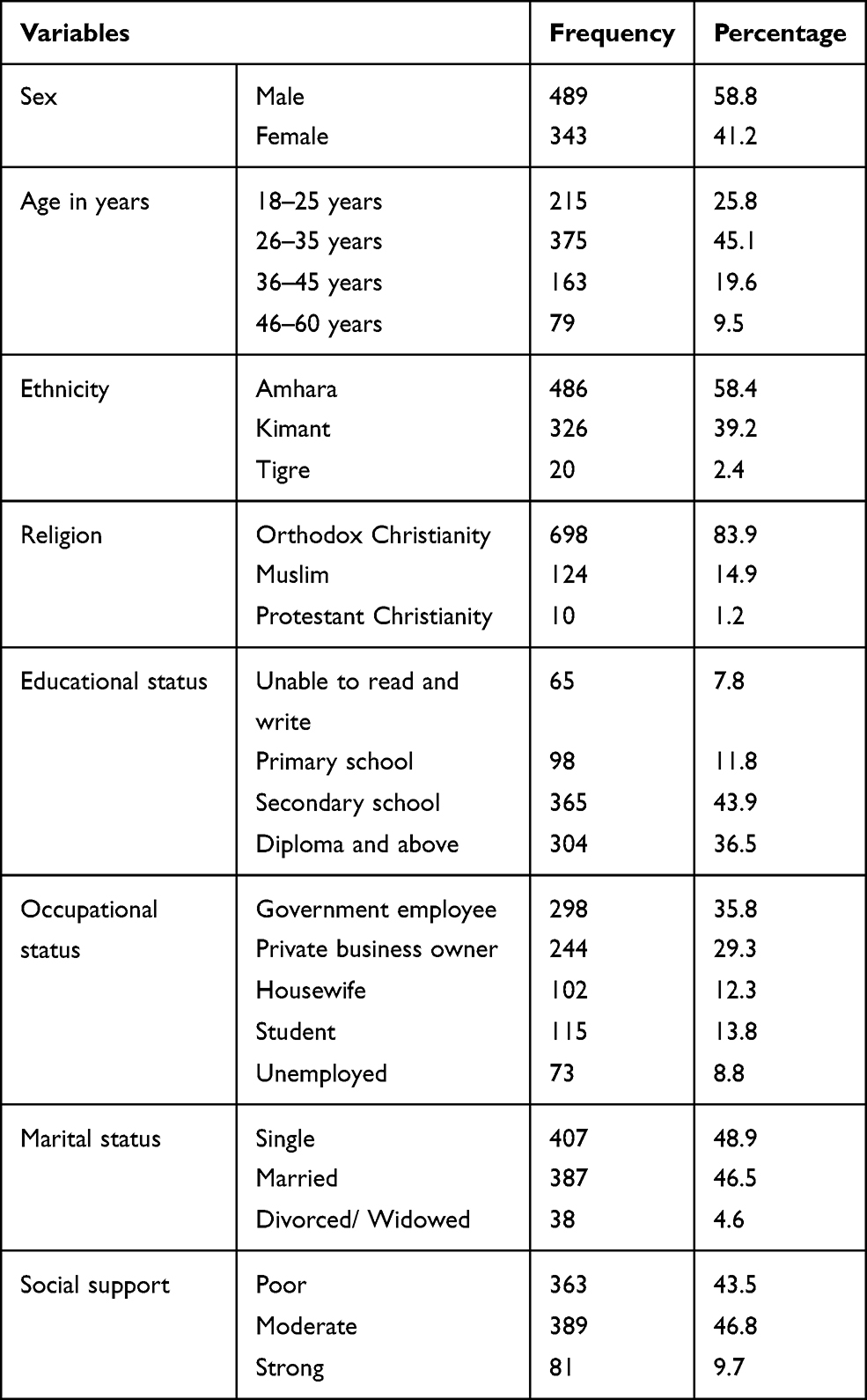 |
Table 1 Socio-Demographic Characteristics of Participants Residing in Aykel Town, Northwest Ethiopia, 2015 (n=832) |
Community Preference to Seek Help from Different Help Sources
The higher the score in each source of help indicates that the study participants have high preference to seek help. From informal sources of help, participants reported higher preference to seek help from intimate partner, parents, friends and a religious source of help than from other family members and sorcerer. From formal sources of care, participants reported higher propensity to seek help from mental health professionals (eg, psychiatrist, psychologist, social worker and counselor) than from general medical professionals or traditional healers.
Depending on the major depression case vignette, a total of 656 (78.8%) showed high propensity to intimate partner with the mean score of 3.96 (SD=1.14) followed by parents with mean score of 3.86±1.14, friends (mean score of 3.76±1.07) and religious sources (mean score of 3.86±1.30). About 812 (97.6%) of the participants had low propensity to seek help from sorcerer in broad informal help with mean score of 1.34±0.71. 655 (78.7%) of the study subjects had high propensity to mental health professional with a mean score of 4.00±1.09 (Table 2).
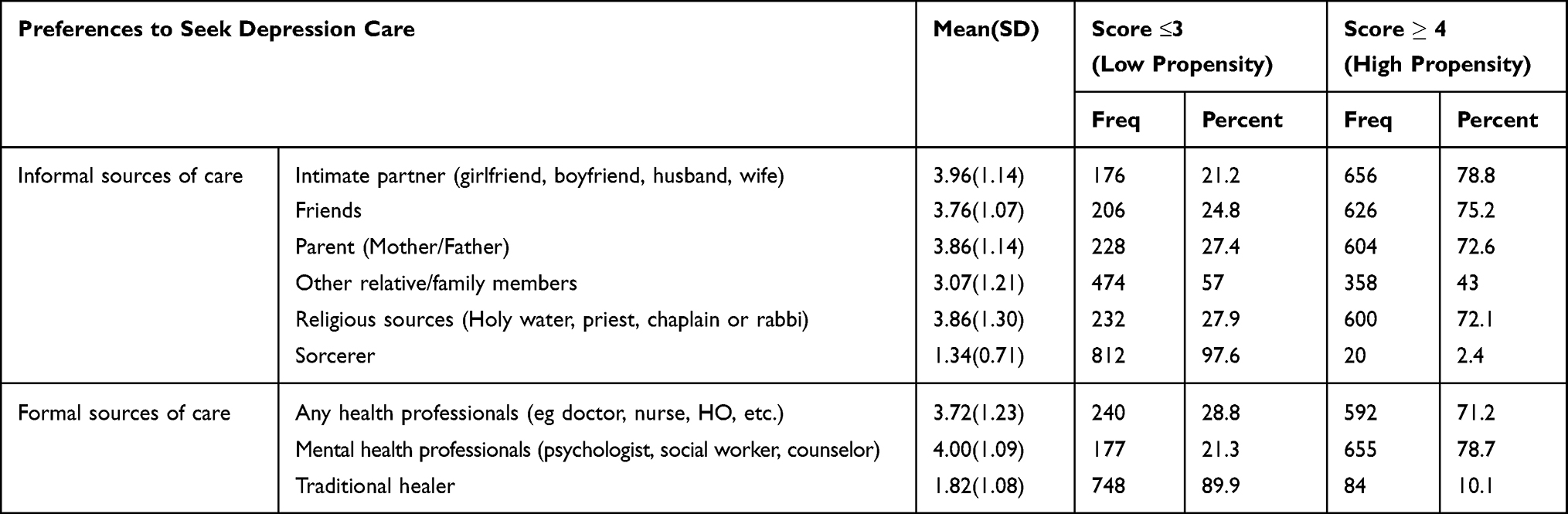 |
Table 2 Residents’ Preferences for Different Informal and Formal Sources of Help for Depression in Aykel Town, Northwest Ethiopia, 2015 (n=832) |
Total mean score of informal source of help was 3.41 (SD=± 0.60). The participants’ preference was higher for close informal help (3.67±0.78) than formal sources of help (3.18 ±0.75). The mean score of broad informal sources of help (religious leaders, sorcerer) was 2.6±0.76; this implies the subjects had a lower propensity than formal sources of help (Table 3).
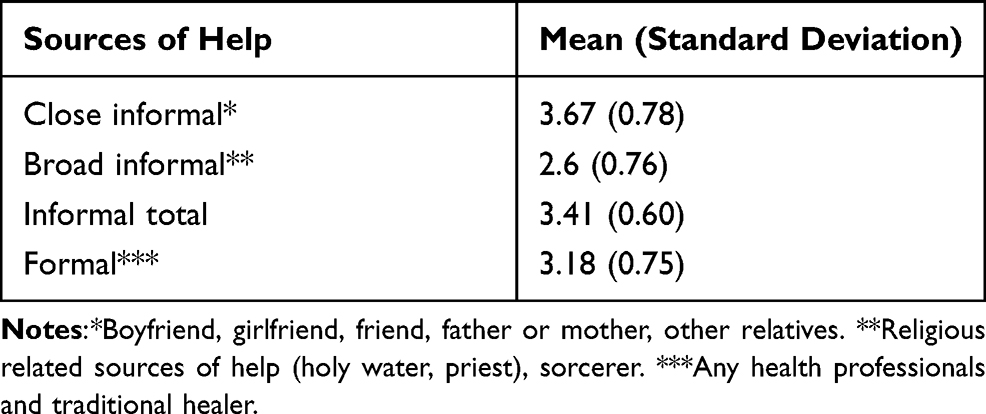 |
Table 3 Summary of Measures of Preferences to Informal and Formal Sources of Help for Depression |
A total of 276 (33.2%) subjects had high propensity to both informal and formal sources of help; 92 (11.1%) had high propensity to informal help and low to formal help whereas 62 (6.5%) of the subjects had low preference to informal help and high to formal help. Indeed, 85 (10.2%) of the study subjects had little propensity with mean score of nearly 2 or lower to both informal and formal sources of help.
In this study we found a significant difference in preference for informal sources of help between students and housewife or unemployed subjects. Students had lower propensity towards informal sources of help when they would encounter depressive symptoms than housewife and unemployed individuals (P=0.045). The result also demonstrated a significant mean score difference in preference for informal help sources between participants with strong social support and low and moderate social support (P<0.001). On the contrary, there was no mean score difference for informal help sources between sex, age, marital status, and educational status of the study participants (Table 4).
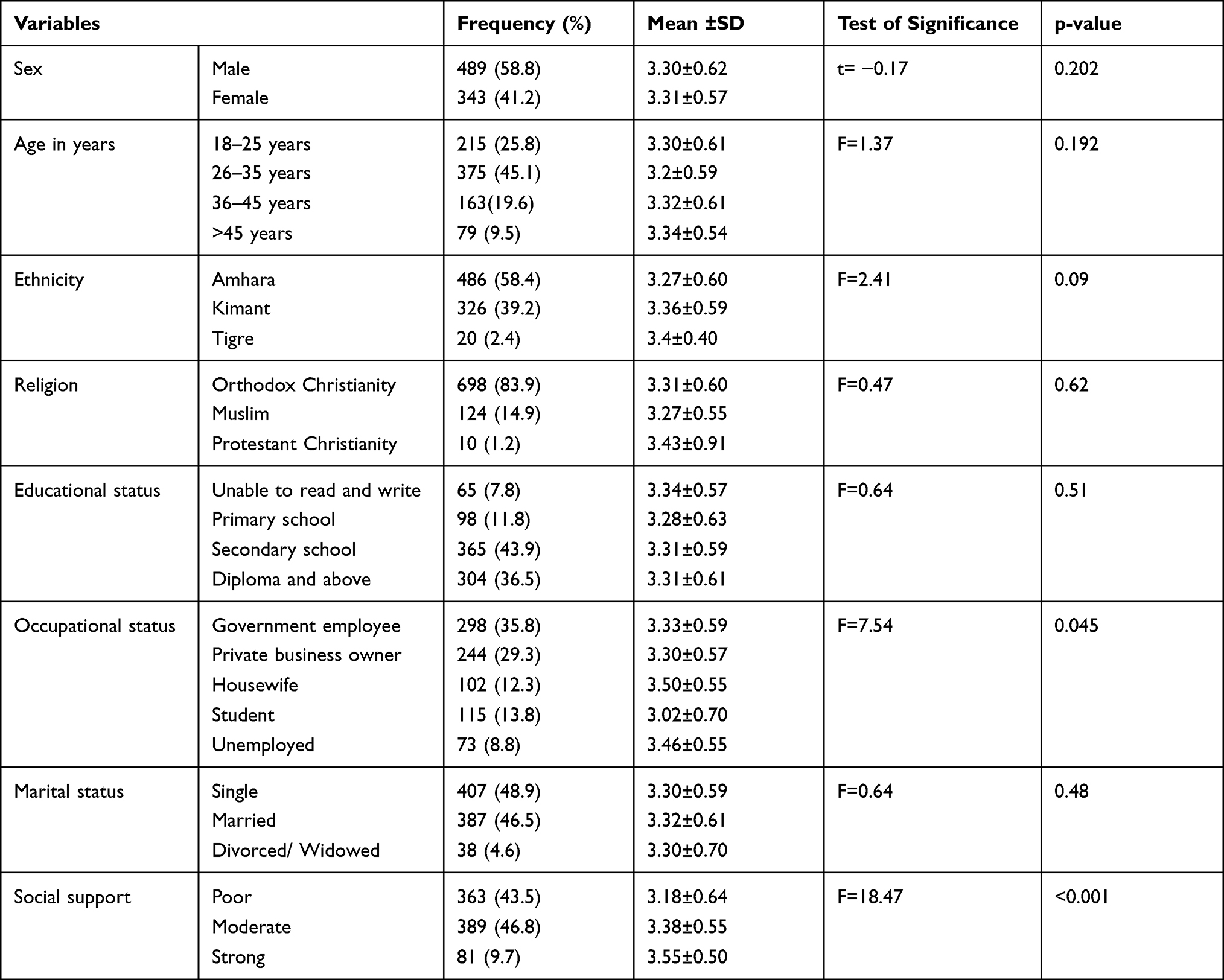 |
Table 4 Comparison of Socio Demographic Characteristics of Participants and Mean Scores of Preference to Informal Sources of Help, Northwest Ethiopia, 2015 (N=832) |
Discussion
Previous literature showed more than one in five community residents (20.5%) had depression in Ethiopia.19 We examined communities’ preference to seek help for depressive symptoms by presenting them a case vignette depicting an individual experiencing a major depressive disorder and asking them to report their preferences to seek help from formal and informal sources if they were having a similar situation.
More than three-fourths of the residents tended to prefer informal sources of help such as an intimate partner, friend, parents (father or mother), religious sources of help, and less likely to prefer sorcerer and other family members. The main reason could be these sources of help are usually available in nearby as required, and persons used easily for less severe of the problem.44 They might also use those sources of help as a bridge to formal and other broad sources of help such that in case of serious problems and need for professional help intimate partner, friends might facilitate the linkage to formal source of help.45 People’s propensity to source of help might also be related with illness casual belief. If people perceive depressive symptoms as due to adverse life events they might not prefer professional help.37
The fourth most preferred source of help was a mental health professional (psychiatrist, psychologist, social worker and counselor) that indicates professional help was considered an important source by more than 65% of the residents. Persons usually preferred the formal sources of help particularly for severe problems.38 This finding is in contrary to previous studies37,38,43 in which for young adults, family was relatively less important (21–31%) and GPs relatively more so (19–34%). People with physical illness causal belief might prefer professional help because they may think the problem could not improve by itself spontaneously. Though preference to informal help is its leading component, help-seeking should be promoted as a general attitude. Professional help is trusted if people know what trust in people and if they are aware of their feelings and can handle and communicate them.3,13 Therefore, indicating professional help as the real or best source of help can prove counterproductive. On the other hand, professional help needs to be publicized, and made more accessible to everyone and everywhere when needed. Professional help and reliable information about it should be more readily accessible in all settings for the community.14
Other relative/family members and sorcerer were substantially less preferred help-seeking sources by the residents. As study shows,46 if individuals have high support from friends and parents, they might have low preference for other family members. However, regarding low preference to sorcerer, study participants might not tell genuine information to the interviewers because study participants might be afraid of being stigmatized by the community. Regarding religious source of help (Holy water, priest, chaplain or rabbi), 70% of the study participants have high propensity to seek help if they have confronted similar situations in the case vignette. This finding is opposite with other studies.38,43 The possible reason for this difference might be socio-cultural, and population differences. People have understood depressive symptoms as less serious and not requiring treatment and therefore those suffering from depression might prefer religious sources of help rather than professional help. Most people in Ethiopia use traditional and religious methods for treating mental illness and look for modern treatment after they tried the local means.47 The other reason might be in developing countries like Ethiopia people might not afford the cost of modern treatment.
Concerning occupational status of the participants, students had lower propensity to seek help from informal sources if they would encounter depression than housewife and unemployed individuals (P=0.045). Majority of the students are young and they may consider depression is simple. As a result, they might cope up with the problem on their own. For example, a study conducted in Australia48 showed that participants reported that they do not like when people judged them or they feel that they are being judged. They prefer it when others think they are confident and in control. Preference to informal sources of help by unemployed participants might be related to inability to afford costs for professional help because this group of population might not have income for their health need. Housewife also might prefer from their intimate partner/couple to get any kind of help before they tried other options.
The result also demonstrated a significant mean score difference for informal help sources among subjects with strong social support and low and/or moderate social support (P<0.001). Social support has positive influence on individuals’ capacity to manage depression since supportive environment, for instance within family and peer domain are associated with symptom improvement.49
On the contrary, we did not obtain any mean score difference for informal sources of help between males and females, age, marital and educational status categories.
Limitation of the Study
We did not consider whether or not the participants have depression. Because participants’ preference to seek help might be different when they have depression or do not have depression.
The other limitation was we did not know the formal and informal help relation. Participants might seek help to formal help after talking to their family, parent, partner and other informal sources of help or in case of serious disorders.
Social desirability bias might be the other limitation of this study. Since data collection method was face-to-face interview which might lead individuals to respond socially acceptable answers during the interview process especially in case of sorcerer sources of help.
In addition, this study did not include many participants more than 60 years of age and future study needs to include this special population. This population might exhibit higher reluctance towards mental help-seeking, particularly for formal help sources.
Conclusion
This study has revealed that majority of the residents had higher preference to seek help from informal sources of care such as intimate partner, father or mother, friends and religious leaders than formal sources of care. There was mean score difference for informal sources across occupational status (student, housewife and unemployed), and degree of social support.
Though preference to informal help is its leading component, formal and informal help seeking should be promoted as a general attitude to get a more qualified and effective care for depressed patients. It is not clear whether informal and formal help are mutually exclusive or whether they are part of the same overall propensity to help-seeking. Although help seeking preference and attitude is not an actual behavior, it is an important issue in mental health for designing strategies to support the community.
Data Sharing Statement
All the data are included in the manuscript. The raw data generated and/or analyzed during the current study are available from the corresponding author on reasonable request [email protected].
Ethical Consideration
Ethical approval and clearance were obtained from the joint ethical review committee of the University of Gondar and Amanuel Mental Specialized Hospital Ethical Review Committee. A Formal letter of permission was also received from Aykel town administration. The aim of the study and the confidentiality issue was explained for the participants’. This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the participants. Personal identification was omitted to maintain confidentiality.
Acknowledgment
The authors acknowledge the University of Gondar and Amanuel Mental Specialized Hospital for funding the study. We extend our gratitude to data collectors, supervisors and study participants for their time and effort.
Author Contributions
All authors made a significant contribution to the conception, execution, acquisition of data, analysis and interpretation. Furthermore, all authors took part in drafting, revising or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the manuscript has been submitted; and agree to be accountable for all aspects of the works.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Keshavarz H, Fitzpatrick-Lewis D, Streiner D, Maureen R, Ali U, Shannon H. Screening for depression: a systematic review and meta-analysis. CMAJ Open. 2013;1(4):E159–67. doi:10.9778/cmajo.20130030
2. Depression WH. Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization; 2017:1–24.
3. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
4. World Health Organization. Mental health facing the challenges bsrfWEmc.
5. Jordans M, Rathod S, Fekadu A, et al. Suicidal ideation and behaviour among community and health care seeking populations in five low-and middle-income countries: a Cross-Sectional Study. Epidemiol Psychiatr Sci. 2018;27(4):393. doi:10.1017/S2045796017000038
6. Kohrt BA, Asher L, Bhardwaj A, et al. The role of communities in mental health care in low-and middle-income countries: a meta-review of components and competencies. Int J Environ Res Public Health. 2018;15(6):1279. doi:10.3390/ijerph15061279
7. Misganaw A, Melaku YA, Tessema GA, et al. National disability-adjusted life years (DALYs) for 257 diseases and injuries in Ethiopia, 1990–2015: findings from the global burden of disease study 2015. Popul Health Metr. 2017;15(1):28. doi:10.1186/s12963-017-0146-0
8. Duko B, Ayano G. Suicidal ideation and attempts among people with severe mental disorder, Addis Ababa, Ethiopia, Comparative Cross-Sectional Study. Ann Gen Psychiatry. 2018;17(1):23. doi:10.1186/s12991-018-0193-3
9. Reddy MS. Depression: the disorder and the burden. Indian J Psychol Med. 2010;32(1):1–2. doi:10.4103/0253-7176.70510
10. Srinivasan K, Isaacs AN, Villanueva E, Lucas A, Raghunath D. Medical attribution of common mental disorders in a rural Indian population. Asian J Psychiatr. 2010;3(3):142–144. doi:10.1016/j.ajp.2010.07.008
11. Menberu M, Mekonen T, Azale T, et al. Health care seeking behavior for depression in Northeast Ethiopia: depression is not considered as illness by more than half of the participants. Ann Gen Psychiatry. 2018;17(1):34. doi:10.1186/s12991-018-0205-3
12. Fekadu A, Alem A, Medhin G, et al. Utility of the concept of minor depressive disorder: evidence from a large rural community sample in a developing country setting. J Affect Disord. 2007;104(1–3):111–118. doi:10.1016/j.jad.2007.03.008
13. Rathod SD, De Silva MJ, Ssebunnya J, et al. Treatment contact coverage for probable depressive and probable alcohol use disorders in four low- and middle-income country districts: the PRIME cross-sectional community surveys. PLoS One. 2016;11(9):e0162038. doi:10.1371/journal.pone.0162038
14. Shumet S, Azale T, Ayano G, Abebaw D, Amare T, Getnet W. Intention to seek help for depression and associated factors among residents of Aykel Town, Northwest Ethiopia: Cross-Sectional Study. Int J Ment Health Syst. 2019;13(1):18. doi:10.1186/s13033-019-0274-y
15. Kebede D, Fekadu A, Alem A, Beyero T, Shibire T, Deyessa N. The distribution of mental disorders among an isolated island community in southern Ethiopia. Ethiop Med J. 2005;43(2):71–77.
16. Fekadu A, Medhin G, Selamu M, et al. Non-fatal suicidal behaviour in rural Ethiopia: a cross-sectional facility- and Population-Based Study. BMC Psychiatry. 2016;16(1):75. doi:10.1186/s12888-016-0784-y
17. Shibre T, Hanlon C, Medhin G, et al. Suicide and suicide attempts in people with severe mental disorders in Butajira, Ethiopia: 10 year follow-up of a population-based cohort. BMC Psychiatry. 2014;14(1):150. doi:10.1186/1471-244X-14-150
18. Mossie A, Kindu D, Negash A. Prevalence and severity of depression and its association with substance use in Jimma Town, Southwest Ethiopia. Depress Res Treat. 2016;2016:3460462. doi:10.1155/2016/3460462
19. Bifftu BB, Takele WW, Guracho YD, Yehualashet FA. Depression and its help seeking behaviors: a systematic review and meta-analysis of community survey in Ethiopia. Depress Res Treat. 2018;2018:1592596. doi:10.1155/2018/1592596
20. Christodoulou GN, Christodoulou NG. Early intervention in psychiatry. Early Interv Psychiatry. 2007;1(1):7–8. doi:10.1111/j.1751-7893.2007.00018.x
21. Wang PS, Aguilar-Gaxiola S, Alonso J, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet. 2007;370(9590):841–850. doi:10.1016/S0140-6736(07)61414-7
22. Boey KW. Help-seeking preference of college students in urban China after the implementation of the “open-door” policy. Int J Soc Psychiatry. 1999;45(2):104–116. doi:10.1177/002076409904500203
23. Chang DF, Tong H, Shi Q, Zeng Q. Letting a hundred flowers bloom: counseling and psychotherapy in the People’s Republic of China. J Ment Health Couns. 2005;27(2):104–116. doi:10.17744/mehc.27.2.hxfupdhht26b30a6
24. Chiu MY-L. Formal and informal help-seeking of Chinese families in a Hong Kong new town. 社會政策與社會工作學刊. 2002;6(1):221–240.
25. Guang-rong J, Ming W. A study on help-seeking hropensity of Chinese undergraduates. Chin J Clin Psychol. 2003.
26. Lin Y-N. Taiwanese university students’ perspectives on helping. Couns Psychol Q. 2002;15(1):47–58. doi:10.1080/09515070110104015
27. Arroll B, Macgillivray S, Ogston S, et al. Efficacy and tolerability of tricyclic antidepressants and SSRIs compared with placebo for treatment of depression in primary care: a meta-analysis. Ann Fam Med. 2005;3(5):449–456. doi:10.1370/afm.349
28. Cuijpers P, Donker T, van Straten A, Li J, Andersson G. Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychol Med. 2010;40(12):1943–1957. doi:10.1017/S0033291710000772
29. Cuijpers P, Geraedts AS, van Oppen P, Andersson G, Markowitz JC, van Straten A. Interpersonal psychotherapy for depression: a meta-analysis. Am J Psychiatry. 2011;168(6):581–592. doi:10.1176/appi.ajp.2010.10101411
30. Modabernia MJ, Tehrani HS, Fallahi M, Shirazi M, Modabbernia AH. Prevalence of depressive disorders in Rasht, Iran: a Community Based Study. Clin Pract Epidemiol Ment Health. 2008;4(1):20. doi:10.1186/1745-0179-4-20
31. Pérez-Zepeda MU, Arango-Lopera VE, Wagner FA, et al. Factors associated with help-seeking behaviors in Mexican older individuals with depressive symptoms: a Cross-Sectional Study. Int J Geriatr Psychiatry. 2013;28(12):1260–1269. doi:10.1002/gps.3953
32. Evans-Lacko S, Aguilar-Gaxiola S, Al-Hamzawi A, et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol Med. 2018;48(9):1560. doi:10.1017/S0033291717003336
33. Shi S, Lu Z, Zhu S. [Seeking behavior of patients with mental disorders and interfering factors]. Zhonghua Yi Xue Za Zhi. 2000;80(1):75–78. Chinese.
34. Oliver MI, Pearson N, Coe N, Gunnell D. Help-seeking behaviour in men and women with common mental health problems: Cross-Sectional Study. Br J Psychiatry. 2005;186(4):297–301. doi:10.1192/bjp.186.4.297
35. Fuller J, Edwards J, Procter N, Moss J. How definition of mental health problems can influence help seeking in rural and remote communities. Aust J Rural Health. 2000;8(3):148–153. doi:10.1046/j.1440-1584.2000.00303.x
36. Cabassa LJ, Zayas LH. Latino immigrants’ intentions to seek depression care. Am J Orthopsychiatry. 2007;77(2):231–242. doi:10.1037/0002-9432.77.2.231
37. D’Avanzo B, Barbato A, Erzegovesi S, et al. Formal and informal help-seeking for mental health problems. a survey of preferences of Italian students. Clin Pract Epidemiol Ment Health. 2012;8(1):47. doi:10.2174/1745017901208010047
38. Brown J, Evans-Lacko S, Aschan L, Henderson MJ, Hatch SL, Hotopf M. Seeking informal and formal help for mental health problems in the community: a secondary analysis from a psychiatric morbidity survey in South London. BMC Psychiatry. 2014;14(1):275. doi:10.1186/s12888-014-0275-y
39. Molla GL, Sebhat HM, Hussen ZN, Mekonen AB, Mersha WF, Yimer TM. Depression among Ethiopian adults: Cross-Sectional Study. Psychiatry J. 2016;2016:1468120. doi:10.1155/2016/1468120
40. Fekadu A, Medhin G, Selamu M, et al. Recognition of depression by primary care clinicians in rural Ethiopia. BMC Fam Pract. 2017;18(1):1–9. doi:10.1186/s12875-017-0628-y
41. Jorm AF, Wright A, Morgan AJ. Where to seek help for a mental disorder? National survey of the beliefs of Australian youth and their parents. Med J Aust. 2007;187(10):556–560. doi:10.5694/j.1326-5377.2007.tb01415.x
42. Dalgard OS, Bj S, Tambs K. Social support, negative life events and mental health. Br J Psychiatry. 1995;166(1):29–34. doi:10.1192/bjp.166.1.29
43. Rickwood D, Deane FP, Wilson CJ, Ciarrochi J. Young people’s help-seeking for mental health problems. Aust J Adv Ment Health. 2005;4(3):218–251. doi:10.5172/jamh.4.3.218
44. Jorm AF. Mental health literacy: empowering the community to take action for better mental health. Am Psychol. 2012;67(3):231. doi:10.1037/a0025957
45. Stanton J, Randal P. Doctors accessing mental-health services: an Exploratory Study. BMJ Open. 2011;1(1):e000017. doi:10.1136/bmjopen-2010-000017
46. Leavey G, Rothi D, Paul R. Trust, autonomy and relationships: the help-seeking preferences of young people in secondary level schools in London (UK). J Adolesc. 2011;34(4):685–693. doi:10.1016/j.adolescence.2010.09.004
47. Shibre T, Spångéus A, Henriksson L, Negash A, Jacobsson L. Traditional treatment of mental disorders in rural Ethiopia. Ethiop Med J. 2008;46(1):87–91.
48. Boyd CP, Hayes L, Nurse S, et al. Preferences and intention of rural adolescents toward seeking help for mental health problems. Rural Remote Health. 2011;11(1):122.
49. Heerde JA, Hemphill SA. Examination of associations between informal help-seeking behavior, social support, and adolescent psychosocial outcomes: a meta-analysis. Dev Rev. 2018;47:44–62. doi:10.1016/j.dr.2017.10.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.