Back to Journals » Infection and Drug Resistance » Volume 15
Helicobacter pylori Antibiotic Resistance in Egypt: A Single-Center Study
Authors Metwally M ![]() , Ragab R, Abdel Hamid HS, Emara N
, Ragab R, Abdel Hamid HS, Emara N ![]() , Elkholy H
, Elkholy H
Received 12 August 2022
Accepted for publication 28 September 2022
Published 11 October 2022 Volume 2022:15 Pages 5905—5913
DOI https://doi.org/10.2147/IDR.S386082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Mohamed Metwally,1 Raghda Ragab,1 Hasnaa S Abdel Hamid,2 Nashwa Emara,3 Hany Elkholy1
1Department of Hepatology, Gastroenterology and Infectious Diseases, Faculty of Medicine, Benha University, Benha, Qualubia, Egypt; 2Department of Microbiology and Immunology, Faculty of Medicine, Benha University, Benha, Qualubia, Egypt; 3Department of Histopathology, Faculty of Medicine, Benha University, Benha, Qualubia, Egypt
Correspondence: Mohamed Metwally, Hepatology, Gastroenterology, and Infectious Diseases Department, Benha University Hospital, PO Pox: 31518, Benha, Qualubia, Egypt, Tel +02 0106-4917959, Fax +02 013-3228631, Email [email protected]
Purpose: Helicobacter pylori (H. pylori) is the most common human bacterial infection worldwide, infecting approximately half of the world’s population. Although antibiotic use is indicated for H. pylori eradication, the recommended type of antibiotic varies from country to country according to the H. pylori resistance pattern; developing countries, such as Egypt, may have different patterns than developed countries. We evaluated the antibiotic resistance of H. pylori in Egypt.
Methods: This cross-sectional study included 134 adult patients with upper gastrointestinal (GI) complaints. Patients with a history of PPI during the last 2 weeks or antibiotics during the last 4 weeks before endoscopy were excluded. Upper GI endoscopies were performed and biopsies were collected for histopathology and H. pylori culture. Demographic, clinical, and endoscopic data were also collected. Antimicrobial susceptibility testing for H. pylori was performed for nine therapeutically relevant antibiotics using the Kirby–Bauer disc diffusion method.
Results: The H. pylori antibiotic resistance rates were as follows: moxifloxacin, 10%; doxycycline, 15%; levofloxacin, 20%; clarithromycin, 40%; azithromycin, 40%; erythromycin, 65%; rifampicin, 90%; amoxicillin, 95%; and metronidazole, 100%. Dual resistance rates were 40% for amoxicillin/clarithromycin, 40% for metronidazole/clarithromycin, and 95% for amoxicillin/metronidazole.
Conclusion: In Egyptian patients, H. pylori had > 90% resistance to metronidazole and amoxicillin; modest resistance to erythromycin, azithromycin, and clarithromycin; and low resistance to moxifloxacin, and levofloxacin (≤ 20%). Dual resistance was high for amoxicillin/clarithromycin and amoxicillin/metronidazole, which prefers using quinolones rather than clarithromycin or metronidazole for first-line treatment of H. pylori in Egypt.
Keywords: Helicobacter pylori antibiotic resistance, H. pylori culture, H. pylori treatment
Introduction
Helicobacter pylori (H. pylori) is the most widespread human pathogen, infecting about 50% of the global population.1 H. pylori is a major cause of peptic ulcers and a risk factor for gastric cancer and mucosa-associated lymphoid tissue (MALT) lymphomas.2 H. pylori may also be associated with extra-intestinal diseases, including immune thrombocytopenic purpura, refractory iron deficiency anemia, and vitamin B12 deficiency.3 The prevalence of H. pylori infection varies globally according to socioeconomic factors and levels of hygiene. In Egypt, the prevalence of H. pylori infection is high; the prevalence of H. pylori is up to 70% in dyspeptic patients.4
H. pylori is typically treated with a combination of 2–3 antibiotics and a proton pump inhibitor (PPI), taken concomitantly or sequentially, for periods ranging from 10 to 14 days. In clinical practice, the initial course of eradication therapy referred to as “first-line” therapy is usually the most successful.5 The success of eradication therapy largely depends on the rapid emergence of antibiotic-resistant strains of H. pylori. Antibiotic resistance is a constantly evolving process and the prevalence of H. pylori antibiotic resistance varies significantly from country to country and even between regions within the same country.6 The progressive loss of standard eradication therapy efficacy makes treating H. pylori more challenging than ever. Endoscopic guided antibiotic susceptibility testing may guide treatment after failure of second-line therapies.7 The last consensus for H. pylori management in Egypt recommended the same first- and second-line therapies as the international guidelines8; however, many studies recommend the identification of H. pylori antibiotic resistance. We aimed to evaluate the susceptibility and resistance of H. pylori to common antibiotics used in different treatment regimens.
Methods
This cross-sectional study included 134 adult patients with dyspepsia who attended the endoscopy unit of the Hepatology, Gastroenterology, and Infectious Diseases Department at Benha University Hospital between October 2018 and October 2020. The study protocol was approved by the Research Ethics Committee of Benha Faculty of Medicine. The study complies with the Declaration of Helsinki. All patients gave informed consent before inclusion in the study. Patients who received PPIs during the last 2 weeks or antimicrobial therapy during the last 4 weeks before endoscopy were excluded from the study. In addition, patients who refused to give informed consent were excluded.
Endoscopic findings were recorded and four gastric biopsies were collected. Two biopsy specimens were preserved with formalin solution for histopathological examination using hematoxylin–osin (H&E) staining. We also stained sections with modified Giemsa stain to confirm the diagnosis of H. pylori infection. Another two biopsies were cultured after homogenizing the samples with sterile glass rods under aseptic conditions. Culture media was prepared as a suspension of 39 g of Columbia blood agar base dissolved in one L of distilled water. The solution was boiled to completely dissolve the agar base and sterilized by autoclaving at 121°C for 15 minutes. After cooling, 5% sterile defibrinated blood was added to the solution. After adding two mL of distilled water to the H. pylori selective supplement vial and mixing gently, the supplement was added to 500 mL of Columbia blood agar base, mixed, and dispensed into sterile Petri dishes. A portion of each sample homogenate was inoculated into freshly prepared Columbia blood agar culture Petri dishes. All plates were incubated at 37°C under microaerophilic conditions in gas pack jars. The plates were inspected within 3–4 days. H. pylori colonies were identified with a urease test, colony morphology (circular, convex, translucent colonies about 2 mm in diameter), oxidase-positive test, catalase-positive test, and microscopic examination.
Antimicrobial susceptibility testing was performed for nine therapeutically relevant antibiotics using the Kirby–Bauer disc diffusion method according to the Clinical Laboratory Standards Institute guidelines (CLSI 2015). Zone sizes were measured and classified as sensitive and resistant (Table 1) according to the Clinical Laboratory Standards Institute guidelines (CLSI 2012).9
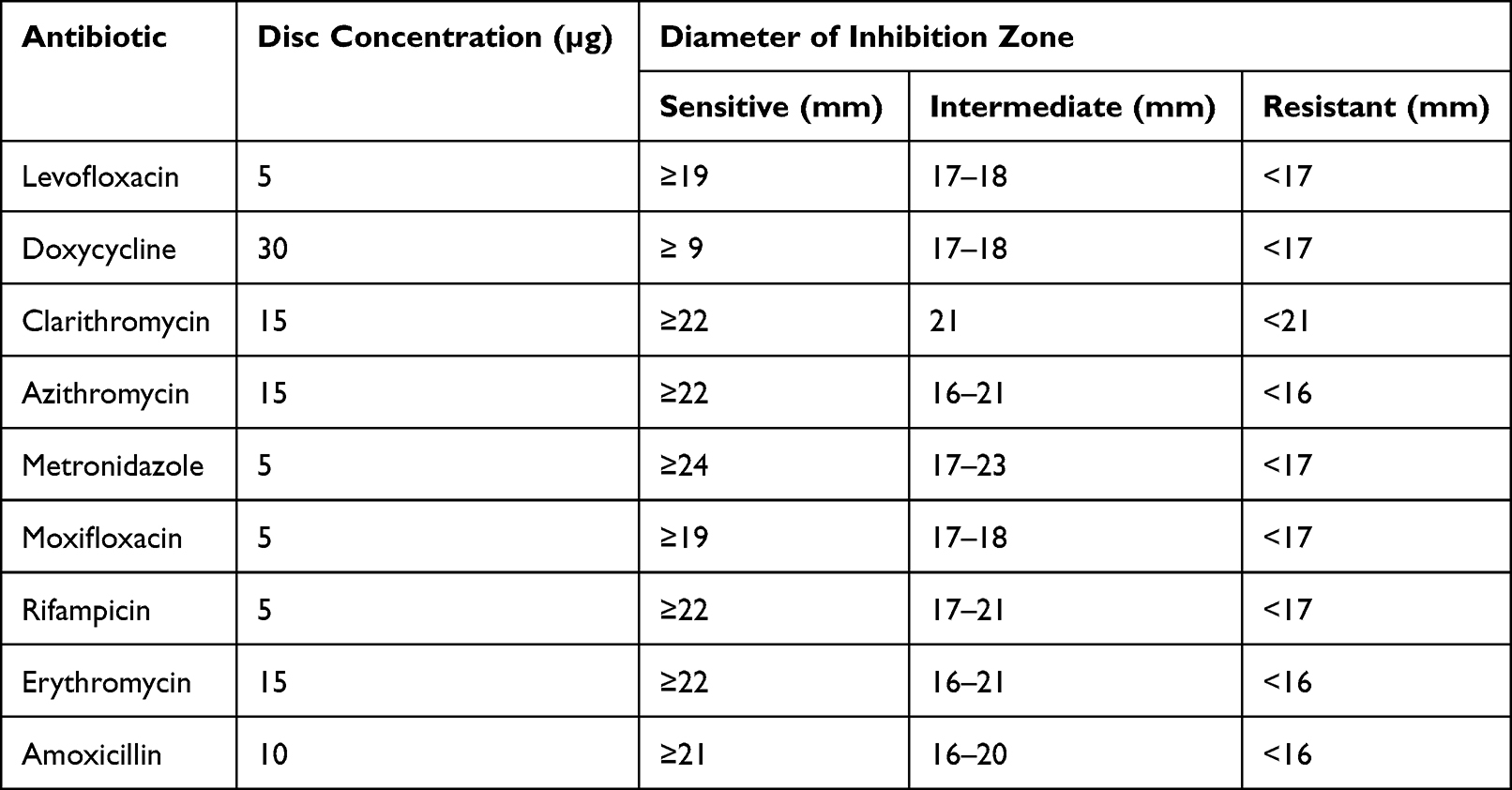 |
Table 1 Antibiotic Disk Concentrations and Diameters of the Zones of Inhibition |
Statistical Analyses
The sample size was calculated based on the American College of Gastroenterology guidelines, which recommend that antibiotics with a resistance prevalence of more than 20% should not be used for the treatment of H. pylori. To detect a resistance of 20% with a 95% confidence level and 10% confidence intervals, a minimum sample size of 61 patients was required. Based on an estimated culture sensitivity of 50%, a minimum of 122 H. pylori-positive samples were required.
Antibiotic resistance of H. pylori was calculated as a percentage (%) with a 95% confidence interval. Demographic, clinical, endoscopic, and histopathological variables were compared between culture positive and culture-negative patients. Two-tailed student t-test or Mann–Whitney test was used for comparison of continuous variables. Chi square test or Fisher’s exact test was used for dichotomous or categorical variables. Analyses were performed using SPSS program version 21.
Results
The study included 134 dyspeptic adult patients, consisting of 56 males (41.8%) and 78 females (58.2%). Abdominal pain, heartburn, nausea, vomiting, hematemesis, and melena were the main presenting symptoms followed by bloating, diarrhea, easy fatigability, and loss of weight (Table 2). Endoscopies showed that 71 patients (53%) had gastric erosions, 41 (30.6%) had endoscopic mucosal granularity, and 21 (15.7%) had gastric ulceration. Histopathological examinations revealed H. pylori in 121 of 134 (90.3%) patients. H. pylori was detected in the cocci form in 50/121 (41.3%) patients, cocco-bacilli was detected in 47/121 (38.3%) patients, and bacilli were detected in 24/121 (20.4%) patients (Table 3).
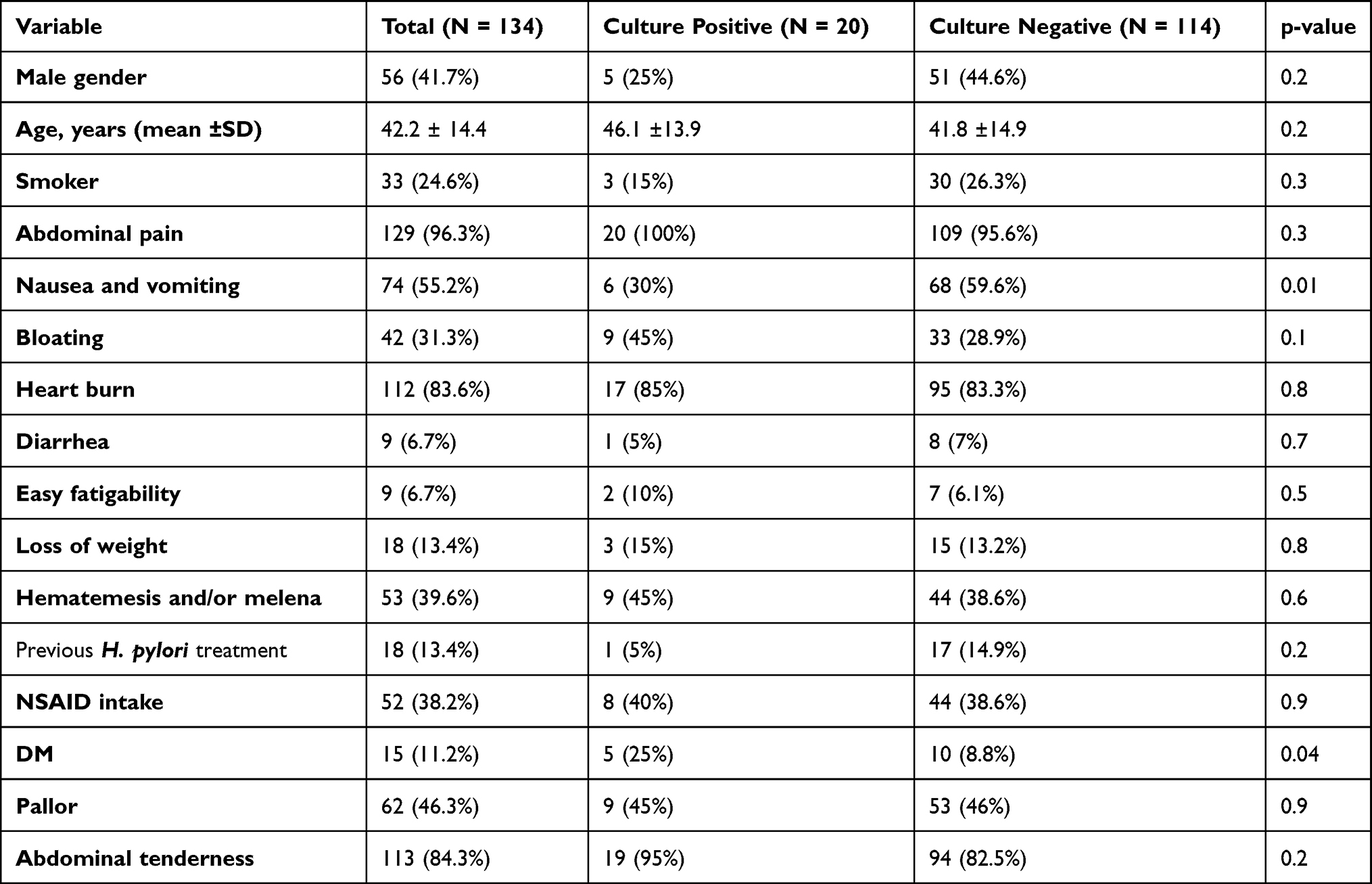 |
Table 2 Comparison of Demographic and Clinical Variables Between Culture-Positive and Culture-Negative Patients |
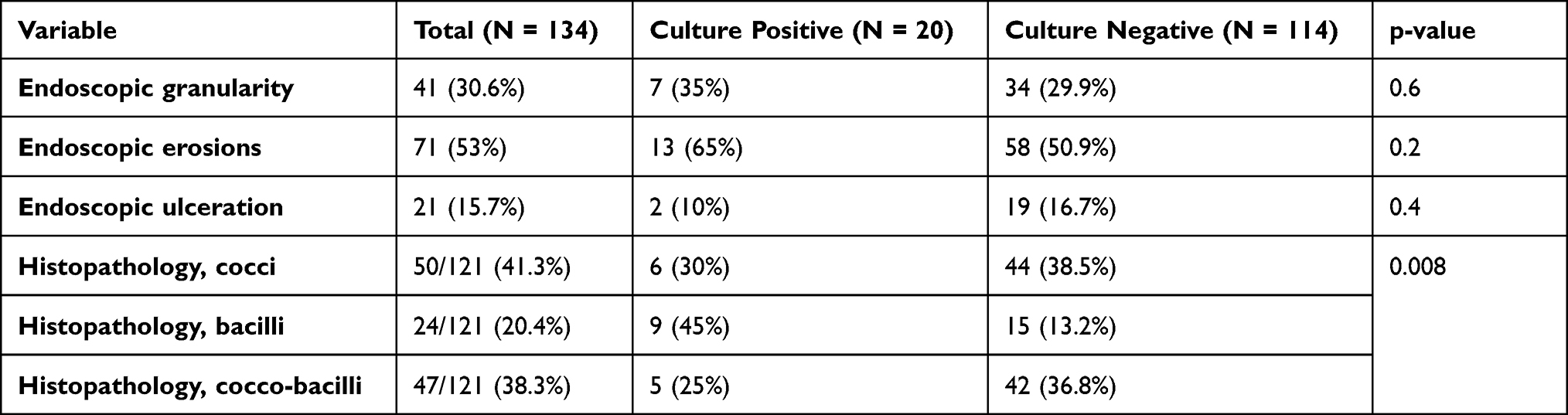 |
Table 3 Comparison of Endoscopic Findings and H. pylori Forms Between Culture-Positive and Culture-Negative Patients |
Twenty of the 134 biopsies had H. pylori-positive cultures (14.9%). All biopsies that tested H. pylori negative in histopathology examinations were also culture negative. The sensitivity and specificity of the culture method were 16.5% and 100%, respectively. The bacillary form of H. pylori was more cultivable (9/24, 37.5%) than the cocci (6/50, 12%) and cocco-bacilli (5/47, 10.6%) forms (P = 0.008) (Table 3). Diabetes mellitus (DM) was significantly associated with positive culture results (5/20, 25%) (P = 0.04) (Table 2). Only one case of culture-positive H. pylori had a history of H. pylori treatment (1/20, 5%) (Table 2).
After culturing the H. pylori, antibiotic susceptibilities were evaluated in positive strains. The resistance rates of the antibiotics were as follows: moxifloxacin, 10% (95% CI, 10 ± 13.2); doxycycline, 15% (95% CI, 15 ± 15.7); levofloxacin, 20% (95% CI, 20 ± 17.5); clarithromycin, 40% (95% CI, 40 ± 21.5); azithromycin, 40% (95% CI, 40 ± 21.5); erythromycin, 65% (95% CI, 65 ± 20.9); rifampicin, 90% (95% CI, 90 ± 13.2); amoxicillin, 95% (95% CI, 95 ± 9.6); and metronidazole, 100% (95% CI, 100 ± 4.4) (Figure 1).
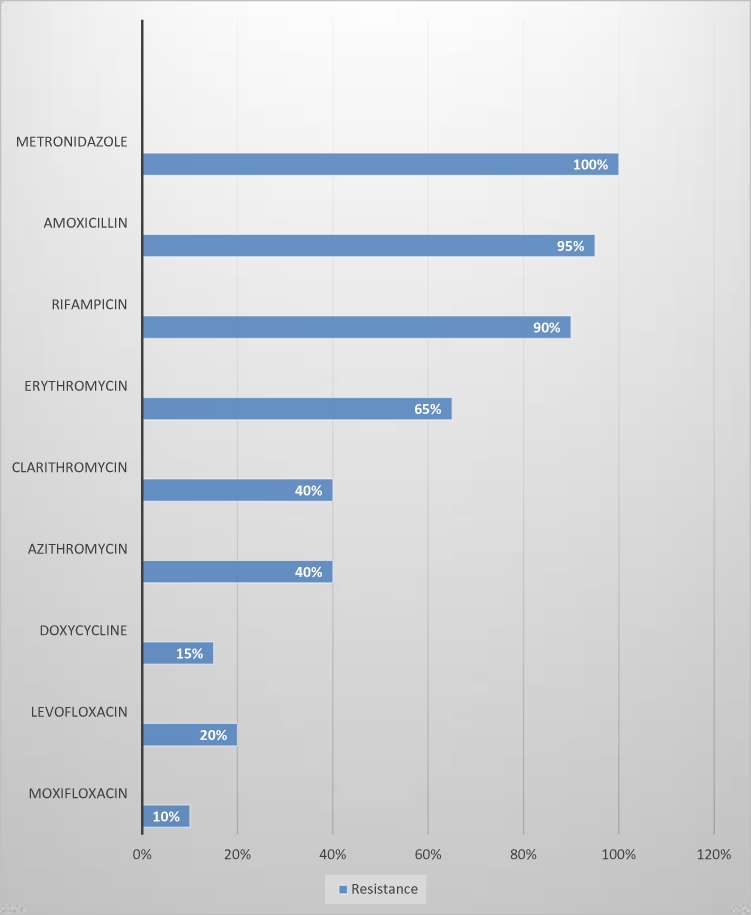 |
Figure 1 Antibiotic resistance rates. |
Multiple drug resistance rates were determined. Resistance to five antibiotics (clarithromycin, metronidazole, amoxicillin, doxycycline, and levofloxacin) was detected in 0/20 (0%) patients, resistance to clarithromycin, metronidazole, amoxicillin and doxycycline was detected in 2/20 (10%) patients, resistance to metronidazole, amoxicillin, doxycycline and levofloxacin was detected in 1/20 (5%), resistance to clarithromycin, metronidazole and amoxicillin was detected in 6/20 (30%), resistance to metronidazole, amoxicillin and levofloxacin was detected in 3/20 (15%), resistance to metronidazole and amoxicillin was detected in 7/20 (35%) (Figure 2). Simultaneous resistance to amoxicillin or metronidazole and clarithromycin, which were used as primary or secondary lines of treatment, was determined. Dual resistance to clarithromycin and amoxicillin was detected in 8/20 (40%) patients, and dual resistance to clarithromycin and metronidazole was detected in 8/20 (40%) patients (Figure 2).
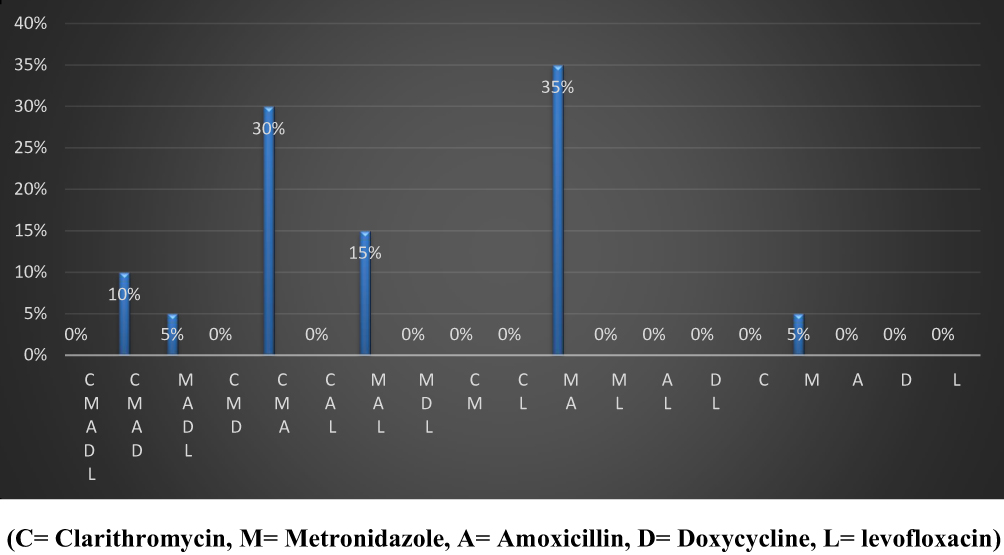 |
Figure 2 Multiple drug resistance of H. pylori to amoxicillin, metronidazole, levofloxacin, doxycycline, and clarithromycin. Abbreviations: C, clarithromycin; M, metronidazole; A, amoxicillin; D, doxycycline; L, levofloxacin. |
Discussion
H. pylori is one of the main pathogenic factors contributing to the occurrence and development of gastrointestinal diseases, such as chronic gastritis, peptic ulcers, gastric mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric cancer. Regimens, which combine PPIs and two antibiotics, are the first-line treatments for H. pylori eradication worldwide.10 However, eradication is seriously limited by the progressive increase in antibiotic resistance.
We detected H. pylori by histopathological examination of gastric biopsies in 90.3% of our dyspeptic patients. This high prevalence has been previously reported for developing countries and specifically for Egypt. A prevalence of 80% was reported by Khalifehgholi et al,11 and a prevalence of 90% in Egyptian adult patients was reported by Hunt et al.12 Other studies reported that the prevalence of H. pylori in Egypt was as high as 88.7%.13,14 On the other hand, the prevalence of H. pylori infection in our study was higher than the reported prevalence in Hispanics (22%) and East Asians (15%).15 The high frequency of H. pylori infection in developing countries is due to the low socioeconomic standards, bad sanitary conditions and water supplies, and increased home crowdedness, which facilitate transmission of H. pylori, especially intra-familial transmission.16
In this study, the sensitivity of the culture method for the detection of H. pylori was low (16.5%) compared with the sensitivity of histopathology; however, the specificity was 100%. Other studies reported higher sensitivity for the culture method. A study conducted at the Philippine General Hospital in 2004 revealed a 30% sensitivity.17 Another study measured a H. pylori culture sensitivity of 29.3% in Chinese patients.18 The differences in culture sensitivity may be attributed to variations in isolating the organism; success rates depend on the technical expertise of the microbiology laboratory, the adequacy of tissue sampling, the transport media and time, the culture media, and the incubation period.
The biopsies with the bacillary form of H. pylori were more likely to be positive in culture compared to other forms. This observation was reported by Eaton et al,19 who found that the bacillary form colonized well (100%) but the coccoid form did not colonize in any inoculated piglets. He considered the coccoid form of H. pylori a degenerative nonviable non-cultivable morphological phase. We also found an association between H. pylori culture-positive results and DM. This result is in accordance with a report by Perdichizzi et al showing that DM increased the incidence of H. pylori colonization.20 This increased colonization may be due to reduced gastric motility and chemical changes in the gastric mucosa following non-enzymatic glycosylation processes. Another explanation is that H. pylori is more prevalent in diabetic patients than in healthy individuals or non-diabetic patients.21
The antibiotic susceptibility results showed that the H. pylori cultures were the most resistant to metronidazole and amoxicillin. All of the isolated strains were resistant to metronidazole. This high resistance rate has been reported in many areas, especially in developing countries. A 100% metronidazole resistance rate was reported in Palestine22 and a 97.9% resistance rate was reported in Cameron.9 A high resistance rate was also reported also in China (90.6%) using both disk diffusion and the E-test.18 A moderate resistance rate was detected in France (58.6%)23 and Korea (27%).24 The high resistance rates may be due to the widespread use of metronidazole for other infectious diseases, such as parasitic intestinal infections and genital infections. Metronidazole is cheap and overused and is an over-the-counter drug in developing countries such as Egypt. The high resistance rate of metronidazole limits its use in the eradication of H. pylori. Point mutation or other genetic events play the main role in development of H. pylori antibiotic resistance. The gene mutations involved in resistance are rrn 23S in macrolides, rdxA, and frxA in metronidazole, gyraA in quinolones, rpoB in rifampins, plp 1 in amoxicillin and rrn 16S in tetracycline resistance.25
The H. pylori isolates from our study were also highly resistant to amoxicillin (95%). A high rate of amoxicillin resistance was also reported in Cameroon (97.14% using the disk diffusion method).9 Amoxicillin resistance varies widely in different geographical areas, ranging from 0% to 97%. A very low rate of resistance was reported in France (0% using PCR)23 and China (1.6% using E-test).26 Slightly higher resistance rates were detected in China18 (7.7% using the disk diffusion or E-test), Palestine (18%),22 Egypt (18.3% using PCR),27 Korea (20%),24 and Iran (30% using the E-test).28 The different amoxicillin resistance rates may be due to the different geographical areas or the different methods of testing resistance. Although the very high resistance rate in Egypt has not been previously reported, the high rate may be due to long-term misuse of antibiotics, leading to the emergence of resistant strains. The impact of amoxicillin resistance on H. pylori eradication is not known.
The resistance rate for clarithromycin in our study was 40%, which is in agreement with studies in China (44.4% using disk diffusion and E-tests)18 and Palestine (47%).22 Low rates of resistance were reported in Germany (10.9% using PCR)29 and Cameron (13.57% using disk diffusion).9 Clarithromycin resistance in H. pylori may be due to several point mutations in the peptidyl transferase region encoded in domain V of 23s rRNA, as reported by Abadi et al.30 Clarithromycin resistance may also be due to overuse for the treatment of infectious diseases, such as respiratory infections. The H. pylori samples in our study also exhibited high resistance to other macrolides. The resistance rate to azithromycin was 40% and the resistance rate to erythromycin was 65%. High resistance rates were reported in China for azithromycin by Shao et al (85.6%)26 and erythromycin by Brigitte et al (47.85%).9 The Egypt consensus guidelines recommend clarithromycin-based triple therapy as the first-line treatment for H. pylori.8 However, this recommendation should be reviewed, considering the high resistance rate.
Quinolones emerged as promising drugs in this study. The levofloxacin resistance rate was 20%. This rate is similar to the rates reported in Iran (28% using E-test),28 France (17.6% using PCR),23 and China (28.2% using disk diffusion and E-test).18 Zero resistance to levofloxacin was reported in Palestine22 and Cameron.9 Although levofloxacin and moxifloxacin are both quinolones, resistance to moxifloxacin was lower in our study (10%). Similar results were reported in Palestine (3%).22 Thus, moxifloxacin is one of the most effective drugs for the treatment of H. pylori, even before levofloxacin.
The resistance rate for doxycycline was 15% in our study. Similar results were reported in Iran (16%)28 and Korea (18%).24 However, lower rates were reported in France (0%),23 China (0.8%),18 and Germany (2.2%).29 These results support the use of doxycycline as a second-line therapy for H. pylori. Rifampicin had a very high resistance rate (90%). A high resistance rate for rifampicin was also reported in China (69.2%)18 and Iran (50%).28 However, very low resistance rates for rifampicin were reported by Brigitte et al (0%),9 Mégraud et al (1.2%),23 and Shao et al (2.8%).26
The resistance to two or more classes of antibiotics is considered multiple drug resistance. The multiple drug resistance rates in our study were 0% for five antibiotic types (clarithromycin, metronidazole, amoxicillin, doxycycline, and levofloxacin), 15% for four antibiotic types, 45% for three antibiotic types, and 35% for two antibiotic types. Amoxicillin or metronidazole and clarithromycin are used as first-line or second-line treatments for H. pylori. The simultaneous resistance rates to clarithromycin and amoxicillin and clarithromycin and metronidazole were both 40%. This finding explains the low eradication rate for these two regimens in Egyptian clinical trials.27 These results also raise the question regarding the value of these two regimens as first-line therapies in Egypt. Our results also support the use of doxycycline and moxifloxacin as second-line therapies.
The multiple drug resistance rates in our study were higher than the rates reported in Korea.24 In Korea, the multiple drug resistance rate to the same five drugs mentioned above was 42.9%; the dual drug resistance to clarithromycin and amoxicillin was 10% and dual drug resistance to clarithromycin and metronidazole was 8.6%. The high rate of multidrug resistance of H. pylori in our study was mostly due to cumulative antibiotic usage for various types of infections and the easy accessibility of antibiotics without prescriptions, which increased the resistance to common antibiotics in Egypt (amoxicillin and metronidazole) to a very high rate (>90%). Previous treatment failures and bacterial factors, such as mutations, can also explain the high resistance rates.31
One of the drawbacks of our study was that our estimation of sample size was based on the prevalence of H. pylori and the assumption of 50% sensitivity for the culture method. Unfortunately, the culture method in our study was less sensitive, which made the sample size for positive cultures smaller than our estimate. Another drawback of this study was the antibiotic susceptibility testing using only the disk diffusion method. Other recent and more accurate methods like PCR and E-test (Epsilometer test) are available. We chose to use the disk diffusion method because it is less expensive, more available, and applicable in developing countries.
Conclusions
The H. pylori samples in our study exhibited high resistance to metronidazole, amoxicillin, and rifampicin (above 90%), moderate resistance to erythromycin, azithromycin, and clarithromycin (40–65%), and low resistance to doxycycline, moxifloxacin, and levofloxacin (10–20%). Dual resistance was high for amoxicillin/clarithromycin and amoxicillin/metronidazole, which prefers using quinolones rather than clarithromycin or metronidazole for first-line treatment of H. pylori in Egypt.
Data Sharing Statement
Data are available on request through the corresponding author.
Funding
No funding was used in this study.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection—the Maastricht IV/Florence consensus report. Gut. 2012;61(5):646–664. doi:10.1136/gutjnl-2012-302084
2. Ohata H, Kitauchi S, Yoshimura N, et al. Progression of chronic atrophic gastritis associated with Helicobacter pylori infection increases risk of gastric cancer. Int J Cancer. 2004;109(1):138–143. doi:10.1002/ijc.11680
3. Liou J-M, Chen -C-C, Chen M-J, et al. Sequential versus triple therapy for the first-line treatment of Helicobacter pylori: a multicentre, open-label, randomised trial. Lancet. 2013;381(9862):205–213. doi:10.1016/S0140-6736(12)61579-7
4. Ghaith D, Elzahry M, Mostafa G, Mostafa S, Elsherif R, Ramzy I. Mutations affecting domain V of the 23S rRNA gene in Helicobacter pylori from Cairo, Egypt. J Chemother. 2016;28(5):367–370. doi:10.1179/1973947815Y.0000000067
5. Li B-Z, Threapleton DE, Wang J-Y, et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: systematic review and network meta-analysis. BMJ. 2015;351:h4052. doi:10.1136/bmj.h4052
6. Smith SM, O’Morain C, McNamara D. Antimicrobial susceptibility testing for Helicobacter pylori in times of increasing antibiotic resistance. World J Gastroenterol. 2014;20(29):9912–9921. doi:10.3748/wjg.v20.i29.9912
7. Cammarota G, Ianiro G, Bibbò S, et al. Culture-guided treatment approach for Helicobacter pylori infection: review of the literature. World J Gastroenterol. 2014;20(18):5205–5211. doi:10.3748/wjg.v20.i18.5205
8. Alboraie M, Elhossary W, Aly OA, et al. Egyptian recommendations for management of Helicobacter pylori infection: 2018 report. Arab J Gastroenterol. 2019;20(3):175–179. doi:10.1016/j.ajg.2019.09.001
9. Brigitte L, Mabeku K, Bille BE, et al. Broad spectrum resistance in Helicobacter pylori isolated from gastric biopsies of patients with dyspepsia in Cameroon and efflux-mediated multiresistance detection in MDR isolates. BMC Infect Dis. 2019;8:1–11.
10. Safavi M, Sabourian R, Foroumadi A. Treatment of Helicobacter pylori infection: current and future insights. World J Clin Cases. 2016;4(1):5. doi:10.12998/wjcc.v4.i1.5
11. Khalifehgholi M, Shamsipour F, Ajhdarkosh H, et al. Comparison of five diagnostic methods for Helicobacter pylori. Iran J Microbiol. 2013;5(4):396–401.
12. Hunt RH, Xiao SD, Megraud F, et al. Helicobacter pylori in developing countries. World gastroenterology organisation global guideline. J Gastrointestin Liver Dis. 2011;20(3):299–304.
13. Enany SM, Abdalla S, Ali K. The prevalence of Helicobacter pylori and resistance patterns in dyspeptic patients from Ismailia, Egypt. Suez Canal Univ Med J. 2005;8(1):87–92.
14. Gad YZ, Hassan AM. CagA Helicobacter pylori seropositivity in asymptomatic, apparently healthy, young adult Egyptian food handlers. Euroasian J hepato-Gastroentrol. 2012;2(1):20–23. doi:10.5005/jp-journals-10018-1025
15. Sonnenberg A, Turner KO, Genta RM. Low prevalence of Helicobacter pylori-positive peptic ulcers in private outpatient endoscopy centers in the United States. Am J Gastroenterol. 2020;115(2):244–250. doi:10.14309/ajg.0000000000000517
16. El-Sharouny E, El-Shazli H, Olama Z. Detection of Helicobacter pylori DNA in some Egyptian water systems and its incidence of transmission to individuals. Iran J Public Health. 2015;44(2):203–210.
17. Destura RV, Labio ED, Barrett LJ, et al. Laboratory diagnosis and susceptibility profile of Helicobacter pylori infection in the Philippines. Ann Clin Microbiol Antimicrob. 2004;3(1):1–6. doi:10.1186/1476-0711-3-25
18. Tang X, Chen X, Shen Y, et al. Primary antibiotic resistance of Helicobacter pylori among a Chinese Tibetan population. Future Microbiol. 2020;15(14):1353–1361. doi:10.2217/fmb-2020-0206
19. Eaton KA, Catrenich CE, Makin KM, Krakowka S. Virulence of coccoid and bacillary forms of Helicobacter pylori in gnotobiotic piglets. J Infect Dis. 1995;171(2):459–462. doi:10.1093/infdis/171.2.459
20. Perdichizzi G, Bottari M, Pallio S, Fera MT, Carbone M, Barresi G. Gastric infection by Helicobacter pylori and antral gastritis in hyperglycemic obese and in diabetic subjects. New Microbiol. 1996;19(2):149–154.
21. Hosseininasab Nodoushan SA, Nabavi A. The interaction of Helicobacter pylori infection and type 2 diabetes mellitus. Adv Biomed Res. 2019;8:15. doi:10.4103/abr.abr_37_18
22. Abdoh Q, Kharraz L, Ayoub K, et al. Helicobacter pylori resistance to antibiotics at the An-Najah National University Hospital: a cross-sectional study. Lancet. 2018;391:S32. doi:10.1016/S0140-6736(18)30398-2
23. Mégraud F, Alix C, Charron P, et al. Survey of the antimicrobial resistance of Helicobacter pylori in France in 2018 and evolution during the previous 5 years. Helicobacter. 2021;26(1):2–7. doi:10.1111/hel.12767
24. Park JY, Shin TS, Kim JH, Yoon HJ, Kim BJ, Kim JG. The prevalence of multidrug resistance of Helicobacter pylori and its impact on eradication in Korea from 2017 to 2019: a single-center study. Antibiotics. 2020;9(10):1–11. doi:10.3390/antibiotics9100646
25. Mégraud F, Lehours P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin Microbiol Rev. 2007;20(2):280–322. doi:10.1128/CMR.00033-06
26. Shao Y, Lu R, Yang Y, Xu Q, Wang B, Ye G. Antibiotic resistance of Helicobacter pylori to 16 antibiotics in clinical patients. J Clin Lab Anal. 2018;32(4):e22339. doi:10.1002/jcla.22339
27. Diab M, El-Shenawy A, El-Ghannam M, et al. Detection of antimicrobial resistance genes of Helicobacter pylori strains to clarithromycin, metronidazole, amoxicillin and tetracycline among Egyptian patients. Egypt J Med Hum Genet. 2018;19(4):417–423. doi:10.1016/j.ejmhg.2018.01.004
28. Hamidi S, Badmasti F, Sadeghpour Heravi F, et al. Antibiotic resistance and clonal relatedness of Helicobacter pylori strains isolated from stomach biopsy specimens in northeast of Iran. Helicobacter. 2020;25(2):1–8. doi:10.1111/hel.12684
29. Hofreuter D, Behrendt J, Franz A, et al. Antimicrobial resistance of Helicobacter pylori in an eastern German region. Helicobacter. 2021;26(1):1–6. doi:10.1111/hel.12765
30. Abadi AT, Taghvaei T, Ghasemzadeh A, Mobarez AM. High frequency of A2143G mutation in clarithromycin-resistant Helicobacter pylori isolates recovered from dyspeptic patients in Iran. Saudi J Gastroenterol Off J Saudi Gastroenterol Assoc. 2011;17(6):396–399. doi:10.4103/1319-3767.87181
31. Boyanova L, Hadzhiyski P, Kandilarov N, Markovska R, Mitov I. Multidrug resistance in Helicobacter pylori: current state and future directions. Expert Rev Clin Pharmacol. 2019;12(9):909–915. doi:10.1080/17512433.2019.1654858
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect and Safety of Helicobacter pylori Eradication Treatment Based on Molecular Pathologic Antibiotic Resistance in Chinese Elderly People
Gao C, Fan YH
Infection and Drug Resistance 2022, 15:3277-3286
Published Date: 22 June 2022
Prevalence of Helicobacter pylori Antibiotic Resistance in Patients Enrolled in Guangzhou, China
Deng R, Liu L, Xie W, Lu W, Liu Z, Wang Y
Infection and Drug Resistance 2023, 16:5033-5038
Published Date: 3 August 2023